")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Barriers and Facilitators to Health-Care Provider Payment Reform – A Scoping Literature Review
Authors Ndayishimiye C , Tambor M , Dubas-Jakóbczyk K
Received 9 May 2023
Accepted for publication 4 August 2023
Published 7 September 2023 Volume 2023:16 Pages 1755—1779
DOI https://doi.org/10.2147/RMHP.S420529
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Costase Ndayishimiye,1,2 Marzena Tambor,2 Katarzyna Dubas-Jakóbczyk2
1Doctoral School of Medical and Health Sciences, Jagiellonian University Medical College, Krakow, Poland; 2Health Economics and Social Security Department, Institute of Public Health, Jagiellonian University Medical College, Krakow, Poland
Correspondence: Costase Ndayishimiye, Doctoral School of Medical and Health Sciences, Jagiellonian University Medical College, ul. św. Łazarza 16, Krakow, 31-530, Poland, Tel +48579143137, Email [email protected]
Background: Changes to provider payment systems are among the most common reforms in health care. They are important levers for policymakers to influence the health system performance. The aim of this study was to identify, systematize, and map the existing literature on the factors that influence health-care provider payment reforms.
Methods: A scoping review was conducted. Literature published in English between 2000 and 2022 was systematically searched in five databases, relevant organizations, and journals. Academic publications and grey literature on health-care provider payment reform and the factors influencing reform were considered. An inductive thematic analysis was applied to map the barriers and facilitators that influence payment reforms.
Results: The study included 51 publications. They were divided into four categories: empirical studies (n=17), literature reviews (n=6), discussion/policy papers (n=18), and technical reports/policy briefs (n=9). Most of the studies were conducted in developed economy countries (n=36). The most frequently reformed payment method was fee-for-service (n=37), and the newly implemented methods included bundled payments (n=16), pay-for-performance (n=15), and diagnosis-related groups (n=11). This study identified 43 sub-themes on barriers to provider payment reforms, which were grouped into eight main themes. It identified 51 sub-themes on facilitators, which were grouped into six themes. Barriers include stakeholder opposition, challenges related to reform design, hurdles in implementation structures, insufficient resources, challenges related to market structures, legal barriers, knowledge and information gaps, and negative publicity. Facilitators include stakeholder involvement, complementary reforms/policies, relevant prior experience, good leadership and management of change, sufficient resources, and external pressure to introduce reform.
Conclusion: The factors that influence health-care payment reforms are often contextual and interrelated, and encompass a variety of perspectives, including those of patients, providers, insurers, and policymakers. When planning reforms, one should anticipate potential barriers and devise appropriate interventions.
Registration: The study was registered with the Open Science Framework.
Keywords: barriers, facilitators, health care provider, health reform, payment reform
Introduction
Health-care systems are constantly evolving to better meet the changing health needs of the population and to adapt to external pressures. Hence, reforms are an integral part of every health-care system. They can be defined as a sustained process of fundamental change in national health policy or institutional arrangements, often led by the government, to improve the functioning and performance of the health sector and ultimately the health status of the population.1,2 Health system reform can be a complex process. Some authors describe it as a cycle that should go through six stages: defining the problem, setting the agenda, developing plans, formulating solutions, implementing them, and evaluating the results.3,4 At the same time, it can be considered as a process that operates at different policy levels, including systemic (changing the institutional arrangements for regulating, financing, and delivering services); programmatic (setting system priorities); organizational (concerned with service provision); and instrumental (generating institutional intelligence to improve system performance).5 The scope of reform may vary depending on how many aspects of the health-care system have changed and how much these changes deviate from past practices.6
Several factors can influence the process of health reform and determine its success.7,8 As stated in institutional theory9–11 and modified for primary care reform,12,13 there are three main pressures and influences for health-care reform. These include coercive influences (laws, regulations, and policies), normative factors (professional influences and culture), mimetic factors (presence of trailblazers and successful leaders), and readiness for change in practice (perceptions and attitudes). The empirical evidence from the analysis of health-care reforms in 60 countries points to four sets of factors that can influence the success of reforms: the incremental approach (“acorn to oak tree principle”), use of IT and good-quality data (“data to information to intelligence principle”), involvement of relevant stakeholders (“many hands principle”), and putting the patient at the center of proposed changes (“patient as preeminent player principle”).7
Provider payment system reforms are one of the most common reforms in health care today.14,15 This involves, first of all, changes in the mechanisms used to transfer funds to health-care providers (provider payment methods), as well as alterations in supporting elements such as contracting, information management, and accountability mechanisms.15 Ideally, payment systems help achieve health policy goals by incentivizing necessary medical services for patients, supporting the quality of care, promoting equity, and at the same time, enabling efficient use of resources. To achieve such goals, a variety of payment methods can be used, ranging from those that rely on available/used inputs, to methods based on outputs (services provided), and even mechanisms that reward health outcomes.16,17 Each of them creates different incentives for health-care providers. The payments, whether determined prospectively or retrospectively, fixed or variable, can also shift the financial risk between providers and payers.17 Thus, policymakers consider them one of the most important levers through which they can influence health system performance.16
The literature is replete with systematic assessments of the impact of specific provider payment methods on health system and/or patient outcomes.18–20 A recent review focused on factors that influence the design, implementation, and adaption of value-based payment (VBP) models at the provider level.21 The authors applied Greenhalgh et al’s22 framework on the diffusion of innovations in service organizations to classify facilitators and inhibitors to VBP models. Unlike previous research, our study identifies, synthesizes, and maps the literature on barriers and facilitators to provider payment reforms more broadly. Since we do not restrict the type of payment method and take an inductive approach to mapping factors influencing reform, our study covers a full range of factors that affect various provider payment methods. By following the general goals of scoping reviews,23 we explore the breadth of existing evidence, build a knowledge base, identify potential research gaps, and provide implications for further research.
Methods
The scoping review followed the methodological guidelines developed by Peters and colleagues (2015, 2017, and 2020).23–25 The process involves the following five steps: 1. Defining specific research questions; 2. Identification of relevant documents; 3. Study selection; 4. Data extraction; and 5. Data analysis and presentation of results. The study protocol was registered with the Open Science Framework (OSF) registries.26
Defining the Review Questions
The general research question is as follows: “What are the barriers and facilitators of health-care provider payment reform?” The specific review questions (RQ) are as follows:
- RQ1 – What types of literature on barriers and facilitators of provider payment methods can be identified?
- RQ2 – What types of payment reforms have been analyzed (including. ie, payment method, provider type, scope of reform)?
- RQ3 – What factors (barriers and facilitators) have been described as influencing health-care provider payment reforms?
Identifying Relevant Literature
We searched five databases: 1. Medline via PubMed, 2. Web of Science, 3. Scopus, 4. Business Source Complete via EBSCO, 5. Google Engine. The searches were conducted from 08 November 2022 to 24 January 2023. A combination of relevant keywords and synonyms from four main topics was used, namely “factor” AND “health care provider” AND “payment” AND “reform”. They were searched in titles and abstracts. Table 1 shows the search query for the databases, including all keywords and synonyms used. The search strategy was developed using an iterative approach and tested in advance in Scopus, PubMed, and Web of Science. To complement the search in the databases, we conducted a manual search of the grey literature on the websites of (non-)government agencies, organizations, and research institutes that are active in this research field. In addition, references of the already included publications were scanned to find additional studies of interest to the research. As part of the Supplementary Materials, details of the search strategies for Scopus, Web of Science, PubMed, Business Source Complete, and Google Engine Search are presented in respective Tables S1-S5, while the list of manually searched organizations and journals can be found in Tables S6 and S7, respectively.
 |
Table 1 Search Strategy and Keywords in Databases |
Selection of Studies
The retrieved records were deduplicated in Mendeley Reference Manager and then imported into Rayyan Desktop27 for a two-stage screening. The first stage is title and abstract screening, and the second stage is full-text screening. In each stage, two independent researchers (CN and KDJ or MT) randomly screened 10% of the retrieved records, compared and discussed the results. Since the two researchers achieved a high level of agreement (over 85%), the remaining data was screened by one researcher (CN). The screening of the full texts was conducted based on pre-defined inclusion and exclusion criteria. Studies that addressed health-care provider payment reform and included an analysis of factors (barriers and/or facilitators) were considered. These were peer-reviewed empirical publications, policy briefs, theoretical papers, technical reports, books, chapters, or dissertations published in full text in English between 2000 and 2022. Conversely, studies were excluded from our analysis if they focused on other types of health-care reform (eg, evaluating other aspects of purchasing without analyzing payment methods), if they did not provide information on factors that influence provider payment reform, if they were not the appropriate types of publications (eg, conference abstracts, commentaries, letters to the editor, erratum, etc.), or if the full texts were in a different language.
Data Extraction
The data were extracted using an Excel template. It consists of three main parts related to the three specific questions of the review: 1. information on the included publication (reference, year, country, objective, and type of publication); 2. data on provider payment method reform (objective of reform, year, provider concerned, payment method, scope of reform, and reform phase in which the factor assessment was conducted); 3. information on the factors identified as influencing payment reform, either as facilitators, barriers, or both. The included publications were classified into four main categories: empirical studies (original, based on primary data, published in peer-reviewed journals); discussion/policy papers (published in peer-reviewed journals); literature reviews (published in peer-reviewed journals); and technical reports/policy briefs (eg, briefs published by advocacy organizations). For the classification of payment methods, the authors utilized two parameters: whether the payment rate was determined retrospectively or prospectively, and whether it was based on input (resources used or available), output (service provided), or outcome (health outcomes).17,28 For the classification of reforms, the authors adapted the OECD classification16 by coding whether the reform modified the existing payment method, introduced an additional payment method to the existing one, or replaced the existing method with a new one. Three reform phases were applied, namely: 1. planning, 2. implementation, and 3. assessment. Data mining involved randomly extracting a 10% sample of the studies by two independent investigators, CN and KDJ or MT, who are the authors of this study. The results were compared, and any discrepancies were discussed to ensure consistency. The two independent investigators achieved a high level of agreement, surpassing 85%. The remaining data was processed by one researcher (CN).
Data Analysis, Summary, and Presentation of Results
Both quantitative and qualitative (thematic analysis) methods were used for data analysis. Data on factors influencing reform were thematically analyzed and grouped inductively (manually). This was done in six steps: 1. we read and reread the data and noted initial ideas (familiarized ourselves with the data); 2. we coded initial features of interest (initial codes); 3. we grouped the codes into potential themes; 4. we reviewed these themes; 5. we refined the specifics of each theme; and 6. we produced the report in relation to the question under investigation.29 This inductive, data-driven approach resulted in mapping the factors described as barriers or facilitators to provider payment methods based on the most prevalent themes/sub-themes. Naturally, the same factor (eg, providers’ attitude) may act as a barrier (providers’ opposition) or facilitator (providers’ support). However, our approach was to map the existing evidence based on the descriptions provided by the authors of the included studies. The overall presentation of results follows the Preferred Reporting Items for Systematic reviews and Meta-Analyses extended checklist for scoping reviews – PRISMA-Scr,30 supported by appropriate tabular and graphical presentations.
Results
Search results
Search results in five databases yielded 10,835 publications. Deduplication in Mendeley resulted in 5690 articles, out of which 128 remained after a screening process based on titles and abstracts. Forty-two publications were included after a full-text evaluation, based on predefined inclusion criteria. Of the 89 excluded articles, 41 analyzed factors affecting other types of health-care reforms, 29 studies were excluded because they did not analyze factors impeding and/or facilitating health-care provider payment reform, 14 studies were excluded because they were the wrong publication types (mainly commentaries and conference abstracts), and five studies were excluded because the full text was not accessible to us (we requested the authors for full texts, but we did not receive a response from them). The results of manual searches of selected organizations and journals yielded three studies, while reference checks yielded nine additional studies. A total of 51 publications were included in the final synthesis (refer to Figure 1). Information on all the included studies is presented in Table 2.
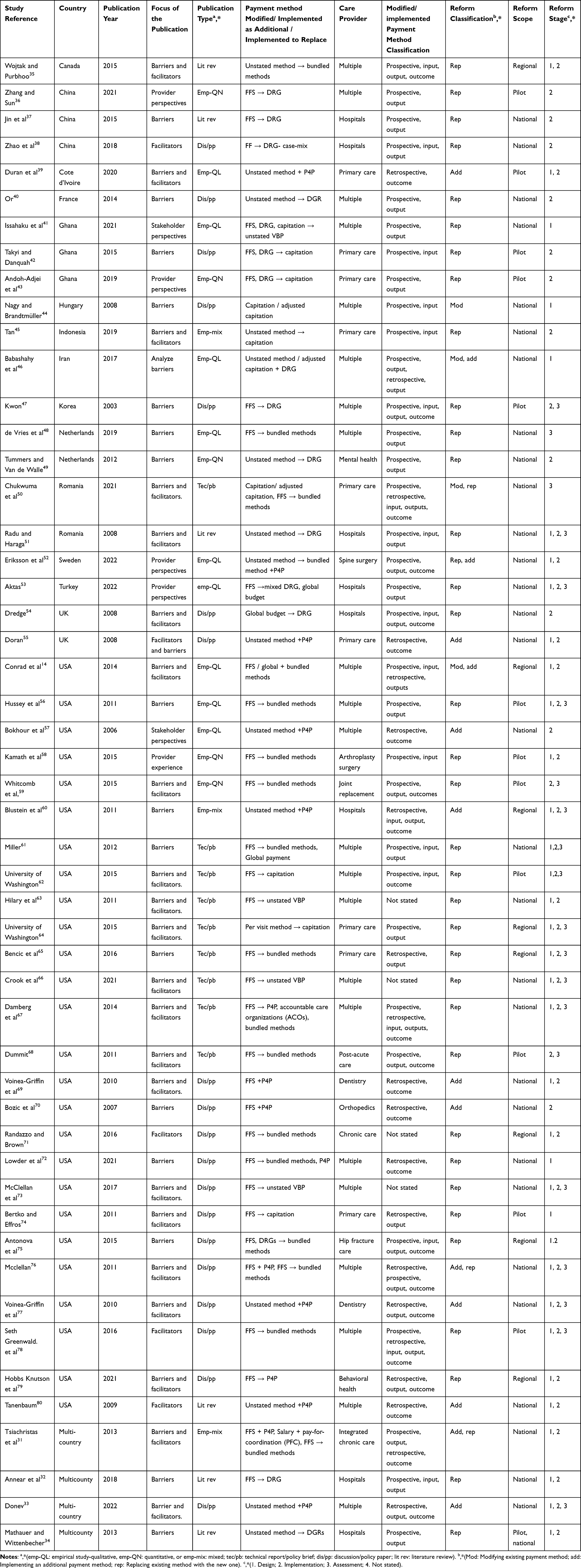 |
Table 2 General Overview of the Included Publications |
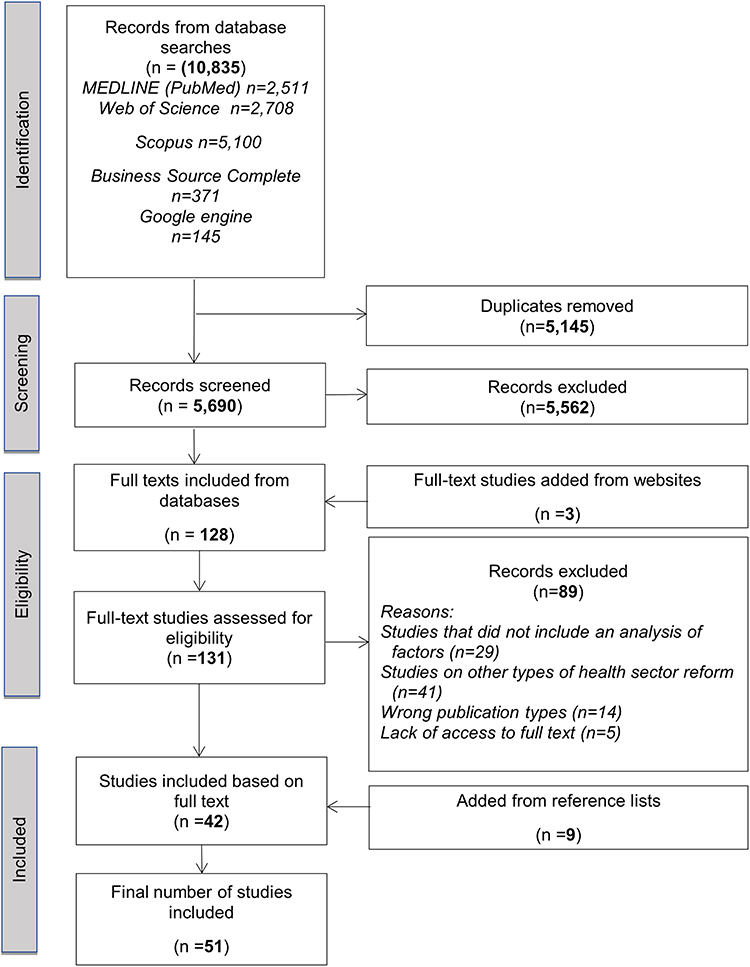 |
Figure 1 Presentation of the results following the PRISMA flowchart. |
Overview of the Included Publications
Most studies were published from 2010 onward (n=43/51, 84.3%). In terms of publication type, discussion/policy papers were consistently high (n=18/51), followed by empirical studies (n=17/51), technical reports/policy briefs (n=9), and literature reviews (n=6/51) (Figure 2).
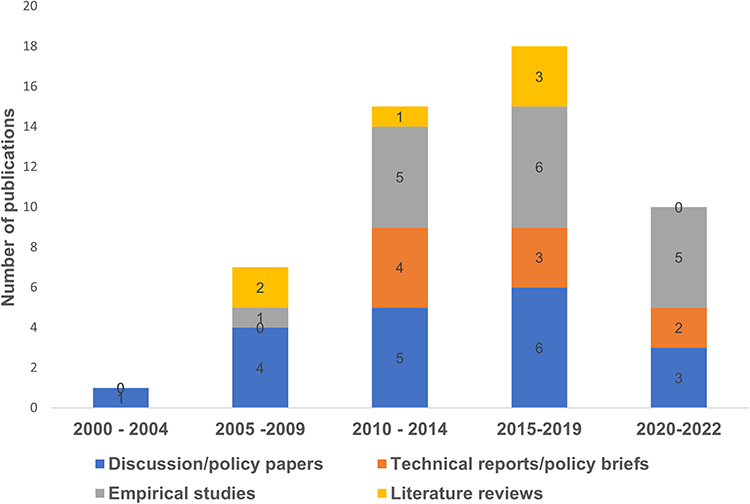 |
Figure 2 Included study types and publication period on a 5-year scale, starting with the oldest included study published in 2000 and ending with the most recent published studies in 2022. Publications include discussion/policy papers (blue), technical reports/policy briefs (Orange), empirical studies (grey), and literature reviews (yellow). |
In terms of geographic distribution (Figure 3), 47/51 were conducted in individual countries, with the United States (USA) accounting for more than half of them (n=26/47). Consequently, most studies (n=27/47) were from North America, followed by nine from Europe, seven from Asia, and four from Africa. Thus, the majority of studies were from developed economies (n=36/47), while a few (n=11/47) were from developing economies.
 |
Figure 3 Study regions from which the included publications originated. Results are shown from left to right, starting with studies covering single countries from America (blue), Europe (green), Asia (yellow), and Africa (dark), and studies covering multiple countries (red). |
The four studies31–34 covered more than one country. The first31 included Austria, France, England, the Netherlands, and Germany. The aim was to provide an overview of payment systems implemented to promote chronic disease integration. This was done by identifying facilitators and barriers to their implementation and assessing how stakeholders perceived their success. A second cross-national study32 examined experiences of using Diagnosis-Related Groups (DRGs) in three Asian countries: Japan, Korea, and Thailand. This study focuses on technical issues and implementation challenges. Another study33 looked at the experiences and factors of performance-based payment in Southeastern European countries, while the last study34 provided a comprehensive overview of DRG-based hospital payment systems in low- and middle-income countries. It examines design and implementation issues as well as related challenges in these countries.
In the vast majority of studies (44/51), the focus was on analyzing the factors (barriers and/or facilitators) that influence provider payment reform. In the remaining seven studies, the focus was more on the perspective of providers and/or other stakeholders regarding payment. These studies also included an analysis of barriers and/or facilitators. Of the 17 empirical studies, the majority (9/17) used a qualitative approach, primarily conducting interviews with various stakeholders involved in provider payment reform. For discussion/policy papers (18/51), the authors often relied on desk research and/or described experiences/opinions regarding a specific reform. However, in many cases, the methods used were not clearly presented or were only vaguely mentioned.
Regarding payment methods that were modified or implemented, almost one-third of studies reported adopting bundled payments (n=16/51). These methods were more commonly used for multiple providers (n=8/16) and specialties (n=7/16), such as surgery and chronic conditions. Pay-for-performance (P4P) programs were the second most commonly implemented schemes (n=15/51), used in a variety of provider settings (multiple n=6, primary care (PHC) n=4, specialist n=4, hospital n=1). 22% (n=11/51) of studies focused on DRGs, which were mostly used for hospitals (n=7/11). Additionally, 18% (n=9/51) of studies reported on capitation payments, which were more commonly associated with PHC (n=6/9).
The majority of studies (35/51) focused on reforms where existing payment methods were completely replaced by new ones, while in 13 studies, new methods were added to the existing ones. FFS was the most frequently changed payment method (72%, n=37/51). With regard to the scope and stage of reforms, the majority of studies focused on national-level provider payment reforms (n=30/51). Most of the included publications focused on the design and/or implementation of the reform (n=49/51), with over a third of them also including an evaluation (n=20/51).
Of the 51 publications included, only 47 provided details on the type of payment method implemented. Twenty-seven of these 47 were prospective, 13 were retrospective, and the remaining seven were a combination of both retro and prospective methods. There was also a wide variety in the classification of methods based on input, output, and outcome measures. Eight of the 47 publications used methods that were based on input, output, and outcome. Additionally, 14 publications used methods that were based solely on output, while seven used methods that were solely based on outcome. In general, outcome measures were used in more than half of the publications (n=24/47).
Mapping of the Barriers and Facilitators
The mapping of factors influencing provider payment reforms in the 51 studies included in the review revealed a variety of themes, which were sometimes interrelated or overlapping. The factors identified were often contextual and presented from a variety of perspectives, including patients, providers, insurers, and policymakers. We identified 43 subthemes of barriers, which we grouped into eight main themes (Table 3), and 51 subthemes of facilitators, which were grouped into six themes (Table 4).
 |
Table 3 Barriers to Provider Payment Reform |
 |
Table 4 Facilitators to Provider Payment Reform |
The first major theme of barriers to provider payment reforms was stakeholder opposition or reluctance, as reported in 27 out of the 51 included studies. Most examples (96.29%, n=26/27) related to provider opposition, although the reasons for opposition varied. 51.85% (n=14/27) of studies indicated that provider resistance was related to unsatisfactory incentives (eg, insufficient or misaligned incentives), while 37.03% (n=10/27) attributed provider resistance to being held accountable for outcomes they cannot control (eg, health outcomes that are more dependent on patient behavior). The latter was evident in payment systems that focused on meeting specific performance metrics, for which providers were rewarded or penalized. Examples of such systems include P4P programs and bundled payments. Provider resistance or reluctance was also evident when a payment method challenged their professional values (ie, professional ethics/clinical autonomy, cited by 37.03%, n=10/27), or they were reluctant to adopt new payment models because they were more familiar with the existing payment model (cited by 18.51%, n=5/27). Similarly, but generally across a wide range of stakeholders, 22.22% of studies (n=6/27) mentioned hesitancy when a new payment initiative was proposed, whereas previous attempts at reform had failed. An example of this can be seen in the Netherlands, where multiple stakeholders, such as insurers, PHC providers, and hospitals, expressed a lack of trust due to the failure of a previous shared savings program.48
Thirty-three studies mentioned obstacles related to the design features of the reform (second major theme). Many barriers were related to specific payment reforms, such as the implementing P4P and bundled payments. The majority of design problems arose because standards and/or benchmarks (quality, cost, risk balance, etc.) were not available (48.48%, n=16/33), or because there were numerous, ambiguous, or unreconciled indicators/measures (eg, performance/outcomes) (24.24%, n=8/33). Reform initiatives that were administratively and operationally complex and not tailored to the local context (eg, social, cultural, or political) were also less likely to succeed (21.21%, n=7/33), as evidenced in different countries, including the USA,59 Côte d’Ivoire,39 and Iran.46 Some challenges were noted when the proposed reform required a partial or complete transformation of health-care delivery (n=3/33). One example is bundled payment for hip fractures in the USA, which required a change in the care delivery process.75 Other barriers also occurred when payment reforms differed between health plans and providers (n=3/33). An evaluation of episodes of care for low-volume Medicaid providers in Tennessee found that different design features, such as practice qualification standards and reporting measures, resulted in significant variations among payers. These differences discouraged many providers from participating.65
In 18 studies, the obstacles were related to the implementation structure of the payment system. These issues were related to confusion caused by conflicts and/or administrative mismatches among the main actors (mentioned in 50%, n=9/18) or due to the fragmented structure of the implementation system (in 33.33%, n=6/18). The aforementioned barriers were documented in various instances, such as the implementation of VBP in health care in Ghana,41 capitation systems in PHC in Indonesia,45 performance-based financing in Côte d’Ivoire,39 and bundled payments in the home care system in Ontario.35 One-third of the papers (n=6/18) also mentioned challenges that arose when implementation structures needed to be adapted to the unique characteristics of payment reform initiatives (eg, to address racial and ethnic disparities, equity, and language barriers). An example of this was when the state of Massachusetts revised its implementation structures to introduce a new approach that used P4P specifically to address racial and ethnic disparities in hospital care for Medicaid patients.60 Some payment reforms have also been hampered by delays caused by lengthy regulatory, administrative, and/or bureaucratic processes (mentioned in five papers).
Barriers related to insufficient resources and capacity were cited in 16 studies. In more than half of these studies (n=9/16), the barriers were associated with the need for new infrastructure (eg, IT, and multi-stakeholder friendly systems). Many papers (n=7/16) also linked this to limited funding/budgetary constraints (eg, extra resources for new costs for data, indicators, staff training, additional payments, etc.), while about a third of the papers (n=5/16) mentioned the need to hire new human resources (service providers, additional staff, IT personnel, etc.). The latter was worse in reform areas where human resources were already unevenly distributed, eg, rural areas more so than urban areas. Regional inequities were reported, for example, in Indonesia, when policies were developed to introduce capitation payments for PHC.45
Sixteen studies mentioned challenges related to the structure of the health market. 43.75% (n=7/16) mentioned barriers that arose because the market environment was unable to engage different stakeholders. Such barriers occurred when the market structure for certain payment reforms, such as the bundled method, was unable to handle multiple stakeholders from both the public and private sectors (eg, because public and private markets operated under different systems). About one-third of the studies (n=5/16) reported barriers related to participating providers having too small number of populations (ie, low volume providers). A quarter of the studies (n=4/16) reported barriers related to competing stakeholder priorities in the market (n=4/16). Additionally, a few papers identified barriers related to market structure that gave advantages to the largest payers, ultimately limiting the efforts of smaller plans with smaller market share (mentioned by two studies).
Challenges related to the legal/regulatory framework were mentioned in 11 studies. In approximately half of the studies (n=5/11), the implementation of provider payment reform was hindered by a mismatch between the level of autonomy of central and decentralized entities (eg, a lack of decentralized fiscal autonomy). For example, the lack of autonomy of decentralized entities hindered the design and implementation of performance-based financing (PBF) in Côte d’Ivoire.39 In more than a third (n=4/11), the obstacles arose from competing health policy and political priorities. In the USA, for example, the implementation of payment reforms to improve the quality of care and political efforts to contain the rise in health-care costs were at odds. This was evident in certain laws, such as the “Patient Referral Law”, also known as the “Stark Act”, which restricts financial relationships between hospitals and physicians.76 Some legal and regulatory hurdles also restricted the right to collect and share data (eg, personal data). Such laws interfered with the implementation of the VBP to address social determinants of health in the USA.66 Other payment reforms have been hampered by requiring substantial amendments to national health-care legislation. In Romania, for example, the introduction of a new payment method for PHC providers necessitates an amendment to the health reform law. This law permits only capitation and FFS as acceptable payment methods under the social security system.50
The last two major themes of barriers included knowledge/information gaps and negative publicity (mentioned in 11 and 4 studies, respectively). Knowledge or information gaps were mostly (72.72%, n=8/11) due to insufficient knowledge about the payment reform initiative (eg, among providers), different levels of information (ie, information asymmetry among stakeholders, mentioned by 36.36% n=4/11) or lack of specific knowledge among stakeholders, eg, IT/data illiteracy (mentioned in two studies). Some payment reforms were also affected by negative media coverage and advertising. For example, negative media coverage increased opposition among some providers to the capitation reform introduced by the Ghana National Health Insurance Scheme.43 Similarly, in the Netherlands, it amplified providers’ voices opposing DRGs, ultimately leading to significant opposition to the introduction of this payment method.49
In terms of factors facilitating health-care provider payment reforms, the first major theme is stakeholder support and engagement (mentioned in 31 studies). In 58.06% (or n=18/31) of these studies, great emphasis was placed on actions aimed to engage various stakeholders. Support from larger stakeholders (eg, the Ministry of Health and provider associations) was one of the most principal factors mentioned in 11 studies. In 35.48% (n=11/35) and 32.25% (n=10/35) of studies, respectively, reforms were enabled by high-level engagement of politicians/political parties and policymakers, as well as government interest in creating a sense of urgency for payment reform. For example, the Dutch government exerted more pressure for bundled payments for birth care and provided subsidies through its Ministry of Health for knowledge and tool development as well as for specific payment (infra)structures.48 A number of studies (n=10/35) also found that clear mechanisms related to factors such as leadership, alignment of goals and incentives, shared norms and values, and relationships among stakeholders facilitated the success of payment reforms. Some studies reported that trust among actors and the achievement of a consensus on reform, as well as communication among them, were particularly beneficial for the successful implementation of reforms. In addition, reforms were facilitated by a coherent alliance structure between local and central actors during implementation and others were enabled by the involvement of trusted neutral bodies that facilitated both the design and implementation process. Despite previous barriers focused on provider resistance, the willingness of providers to accept the new payment system was identified as a key factor in the success of some reforms (n=5/31). In addition, transparency in reform negotiations was also cited as crucial for the success of payment reforms.
In 17 studies, it was found that the availability of complementary measures/policies facilitated payment reforms. In 41.17% of these studies (n=7/17), payment reforms were facilitated by a favorable market, social, legislative, and regulatory environment that aligned with the reform goals. In 35.29% (n=6/17) of the studies, reforms were facilitated by complementary changes in other health policies or simultaneous efforts in the health-care marketplace. Another 35.29% of studies pointed to specific and meaningful policies addressing ethical issues related to professionalism, patient-physician relationship, access to care, and patient autonomy. In 29.41% (n=5/17) of cases, reforms were supported by federal or state legislation encouraging payment innovation. Other facilitators included pre-existing measures and policies, such as antitrust measures to prevent the exercise of health-care market power, measures against anti-competitive behavior by large providers, and the existence of regulatory mechanisms for robust competition between payers and providers. Typical examples can be found in some countries, such as the USA, where there have been many complementary policies and measures. These include the Patient Protection and Affordable Care Act, commonly known as Obamacare, as well as various measures to prevent anti-competitive behavior and the exercise of market power.61 Hungary's health sector has long prioritized equity in all health reform proposals. This has subsequently proved helpful in enabling related payment reform, for example, the introduction of a risk-adjusted capitation system.44 Other areas of health policy have also facilitated payment reform for providers in other countries, such as the introduction of case-based DRGs in hospitals in Romania.51
Another major theme of facilitators for payment reforms is prior relevant experience and know-how, as highlighted in 14 studies. About half of the studies (n=6/14) indicated that conducting a pilot project/feasibility study before full implementation of the actual reform facilitated reform initiatives. For example, in the Netherlands, bundled payment for integrated chronic disease care was initially piloted for type 2 diabetes, which proved successful. It was later approved for nationwide implementation for diabetes, asthma, chronic obstructive pulmonary disease (COPD), and vascular disease.48 Similarly, 42.85% of studies reported building reform on existing lessons learned or infrastructure, while 35.71% related to a long history of progressive health reform innovations. For example, the implementation of P4P in Massachusetts was successful due to its long history of health policy innovation and collaboration among different stakeholders. A system was already in place with hospitals, government payers, experts, and various committees (eg, quality and cost advisory boards).60 More than a third of the studies (n=5/14) reported that reform was facilitated by the fact that there was already an existing team and staff (ie, stability of the workforce), that the participating organizations had relevant experience, that they built on early partnerships already in place or that they built on and learned from best practices (ie, benchmarking). Also, previous experience with legal, social, and regulatory conditions was found to be helpful in implementing payment reforms, as reported in some studies (21.42%, or n=3). For example, a study of value-based reforms in six states across three regions of the USA found that prior experience in dealing with federal and state laws, such as the Patient Protection and Affordable Care Act, guided reform initiatives in many contexts, particularly in response to local market requirements.14
In 14 studies, the availability of sufficient resources was indicated as a facilitator for payment reform. In 50.0% of these studies (n=7/14), sufficient resources were cited as adequate infrastructure, 42.85% (n=6/14) related to software/IT systems (eg, electronic health records, data tools (cost, outcome measures)), 35.71% related to adequately trained IT staff, and 28.57% (n=5/14) related to data sharing and privacy mechanisms. In several other studies, it was purely related to financial factors, such as additional reform funding (grants, sponsorship, loans, etc.) and external investment that enabled an increase in needed resources (mentioned in 35.71%, n=5/14 and 28.57%, n=4/14 of studies, respectively).
Good-quality leadership and management of change at the provider level was described as important facilitators of payment reforms in 14 studies. The top five subthemes for this factor included 1) having a leader who is instrumental in building and maintaining cohesive stakeholder relationships (cited in 50% of studies, n=7/14), 2) flexibility and stable leadership that is able to analyze market conditions and stakeholder engagement and change priorities over time (cited in 35.71%, n=5/14), 3) appropriate leadership across reform initiatives to share best practices and find solutions to challenges (cited in 28.57%, n=4/14), 4) timely and consistent feedback management (cited in 28.57%, n=4/14), and 5) ability to retain key staff or replace departing staff in a timely manner (eg, physician attrition) (21.42%, n=3/14).
A few payment reforms were adopted and implemented due to external pressures, as mentioned by two studies. For example, the Macedonian Ministry of Health introduced P4P for hospitals despite opposition from physicians. This decision was influenced by the growing international debate and interest in this payment mechanism.33 The adoption of reform was also related to shifts in political interests in favor of health reform due to upcoming presidential elections, parliamentary votes, and so on. One example is the Medicare P4P program, which received massive support from the 2008 presidential candidates and their parties.80
Discussion
Summary of Results
In our study, we identified, synthesized, and mapped the existing literature on barriers and facilitators to health-care provider payment reform. We reviewed 51 studies published between 2000 and 2022, mostly from developed economies, with a strong representation from the USA (50.98%, n=26/51). FFS was the most commonly replaced and/or supplemented method (72%, n=37/51), while newly introduced methods included bundled payments (n=16), pay-for-performance (n=15), and diagnosis-related groups (n=11). Forty-seven of the 51 publications that provided details on the type of payment method implemented, the majority were prospective (n=27/47) and generally based on outcome measures (n=24/47).
The barriers to provider payment reform can be categorized into eight main themes: stakeholder opposition, challenges related to reform design, hurdles in implementation structures, insufficient resources, challenges related to market structure, legal barriers, knowledge and information gaps, and negative publicity. The facilitators are grouped into six main themes: stakeholder involvement, complementary reforms/policies, relevant prior experience, good leadership and management of change, sufficient resources, and external pressure to introduce reform. The factors influencing payment reforms (barriers and facilitators) are often interconnected and can be context-dependent.
Comparison with the Literature
The study’s findings, while narrowly focused on health-care provider payment reform, are consistent with the majority of the existing literature on facilitators and barriers to health-care reform in general.7–12 The findings underscore the enormous importance of stakeholder engagement. This is consistent with previous studies,7,21 particularly the “principle of many hands”, which has been cited as one of the key success factors of health reforms.7
The key stakeholders in payment reforms are the providers themselves, payers, insurers, government agencies (eg, the Ministry of Health), physicians’ associations, and patients/citizens. We found that the existing literature on barriers mainly focuses on the reluctance or resistance of providers and physician associations to reform. The strategy of involving stakeholders (eg, providers) early on in understanding the objectives of a reform program and their role in planning and implementation has proven successful in a number of health reform initiatives in avoiding individual and institutional resistance.41,71 Stakeholder involvement and greater participation can help establish consensus and ultimately facilitate the successful implementation of reforms.
Our study found that patients are the least involved stakeholders in health-care provider payment reforms. This is consistent with previous research indicating a lack of community and patient involvement in health reforms in general.12 In particular, it is consistent with the findings of researchers such as Doran, who found that patient involvement in the development of P4P systems was extremely limited.55 On the other hand, the literature discusses the recognition of patients as important stakeholders in health reform,81–83 particularly the successful reform principle of placing patients at the center of proposed changes.7 Some researchers suggest that patient participation in today’s health-care decision-making processes could be strengthened at both the individual and collective levels.81,82
Many of the themes and subthemes in our review align with the existing literature on three types of influences and pressures modelled in previous research on institutional change theory in health-care reform.12,13 The first is coercive pressure, which originally stems from political influence and associated legitimacy.9,12 It includes laws, regulations, and policies as determinants of change. In line with this, our study found that government support, political commitment from politicians, or their political parties are important for a successful payment reform process. We also found that reform is more likely to succeed if there are already well-established, complementary laws, regulations, and policies in place in the health sector. In addition, we found that political influence on reform can also come from outside the health system, eg, when political interests shift to support reform. This is consistent with coercive influences, according to which both formal and non-formal pressures can be external or imposed directly by organizations on which one depends on and/or by cultural expectations in society.9
The second category of factors falls under normative influences, which are mainly due to professionalization.9,13 It is defined as the collective struggle of members of a profession to define and control the conditions and methods of their work, as well as to establish a cognitive basis and legitimacy for their professional autonomy.9 In our study, several factors are associated with this category, particularly barriers to remuneration reform that arise when the proposed reform conflicts with health-care providers’ professional values, such as ethics, autonomy, and their traditional or habitual ways of practicing health care. As mentioned earlier, some of these factors can lead to resistance or reluctance among health-care providers.
Importantly, the normative nature of influences highlights two aspects of professionalization. The first is education (eg, in-service training programs), and the second is the establishment and development of professional networks.9 Regarding the first aspect, it can help to close the knowledge gap that hinders the proper implementation of payment reform, as indicated by our study. We found that stakeholders may face knowledge gaps, eg, IT/data illiteracy (eg, inability to enter data into the database, inability to use EMRs, etc.). Therefore, the first aspect is particularly helpful in acquiring the specific skills needed to implement payment reform. The second aspect, building networks, is one of the most crucial factors, as professional networks can help share information, including best practices, and learn from each other, all of which contribute to the success of payment reform. However, we have found that stakeholders’ interests can compete and conflict. This is consistent with the findings of previous studies on barriers and facilitators to health-care reform, eg Levesque et al,12 which show that members of networks may clash with their priorities, eg when the goals of some stakeholders in the networks (eg the government) and medical professional associations clash. These associations always strive to preserve the professional autonomy of their members.
The third category is mimetic influences, under which researchers such as Levesque et al12 contend that the presence of innovators and champions (ie, successful leaders) who can play a key role in a multidisciplinary team significantly contributes to the success of health reform. The authors suggest that including providers in this role helps to reduce physician resistance to reform by giving more weight to the voice of their medical profession. In many ways, these findings are consistent with the results of our study. For example, we found that health-care providers may resist reform initiatives in which they are not involved in organizing. Moreover, this overall perspective on the presence of successful leaders aligns with our research findings, which indicate that good-quality leadership and change management at the provider level are crucial in enabling payment reform. Proactive change management is particularly important because change can occur at any time and at any level. When introducing payment reform, it is essential for everyone on the team to understand the reasons behind the change, the expected benefits, and how it will impact their respective roles. They also need to be aware of the impact their interactions with others on the team can have. This means rethinking workflows, developing customized communication plans for each stakeholder, and carefully monitoring and managing team dynamics (such as addressing negative employee attitudes and resolving conflicts). Apart from innovators and champions, which are considered crucial factors, uncertainty is also recognized as a powerful force in mimetic processes, often stimulating imitation.9 This is broadly consistent with our finding that the adoption of payment reforms can be influenced by international interest in health-care change (ie, imitation of what is being done abroad). The mimetic process also suggests modeling organizations on others when there is a poor understanding of a change, when goals are ambiguous, or when the environment creates symbolic uncertainty.9 In our study, we also found that the success of payment reforms is enhanced by building on and learning from best practices (ie, benchmarking). This is also consistent with our other findings on the many barriers to payment reform that stem from hurdles in the design of reforms and implementation structures (eg, goals that are not embedded in the local context, ambiguous metrics, etc.). Benchmarking is, thus, a crucial factor in overcoming such challenges.
As in previous studies,12 we indicate that health-care reforms are more effectively implemented when providers are more receptive to reform, meaning they have positive perceptions and attitudes. However, this is rarely the case due to their inertia in changing their past practices.64 We found in our study that providers resist payment reform not only because they are unwilling to change their usual practices but also because they believe they will be exposed to risks they cannot control (eg, certain quality metrics and outcomes). Strong resistance can arise when the risks they are held accountable for lead to unsatisfactory incentives (eg, misaligned incentives and financial penalties). This is the case with most P4P systems, which have their roots in economic theory and behavioral psychology.84 These systems require providers to align their behavior with specific performance indicators, particularly in terms of quality. Some providers complain that the quality is highly dependent on patients’ adherence to physician recommendations (screening, treatment, lifestyle, etc.). They argue that they are unfairly penalized for patient behavior that is beyond their control.55,57,61,65 Similar concerns may arise with other payment arrangements, such as bundled payments, because they often involve financial risks for providers.
Finally, but largely consistent with previous studies,14,21,62,85 we found that sufficient resources (eg, additional funding, infrastructure, etc.) are an undeniable factor in facilitating provider payment reform. Previous researchers, such as Leao et al,21 have found that sufficient infrastructure and advanced health information technology are key factors in the design, implementation, and applicability of VBP models. This is consistent with most of our findings, which indicate that payment reforms require adequate health information systems infrastructure and the associated costs (eg, IT tools, data, etc.). It is also emphasized in the “principle of data to information to intelligence” described by Braithwaite et al.7 However, the increasing need for health information technology may also pose challenges for implementing provider payment reform, such as the introduction of complex metrics and standards.
Overall, our study has shown that despite some country- and/or region-specific characteristics of health system organization (eg, Europe vs the USA) and resulting payment policies, the issue of factors influencing provider payment reforms is to some extent universal in nature. For example, the issue of stakeholder involvement was mentioned (either as a barrier or facilitator) in studies from 20 different countries across all regions represented in the included publications (ie, North America, Europe, Asia, and Africa).
Strengths and Limitations
To the best of the authors’ knowledge, this study is the first to identify and map the factors that have influenced diverse provider payment method reforms worldwide. Using an inductive, data-driven approach to map barriers and facilitators allowed for the inclusion of a variety of perspectives and provided a comprehensive overview of the existing evidence. Because we included all methods of paying providers (including P4P programs), we were not able to capture the specifics of reform or implementation of a particular method well. In addition, we focus on payment methods rather than solely on changes related to payment systems. This includes supporting elements such as contracting, information management, and accountability. Some factors may be context-specific, eg, specific to systems with many payers. Furthermore, only English-language publications were considered, and the quality of the studies was not assessed. The latter is consistent with the methodological guidelines for conducting scoping reviews.24
Implications of the Study
Our findings suggest that there is a paucity of empirical research focused on identifying the barriers and facilitators to provider payment reforms, especially outside the context of the USA. This is consistent with issues raised by other authors48 about the need to plan and conduct primary data research on factors that can support the successful implementation of reforms in various health-care settings. Further research could focus more on analyzing specific types of factors, such as stakeholder involvement, including patient/citizen participation in the design of provider payment reforms, or on the implementation of specific payment methods. Further research is also needed on integrating these types of reforms into the broader context of health-care system and addressing significant current challenges (eg, health-care workforce shortages;86,87 digitalization;86,88,89 changing models of care87,90). Future research on the factors that influence the success of reform may help in developing guidelines for a more evidence-based approach. The identified and mapped major themes of factors influencing reforms can serve as a starting point for research aimed at ranking the importance and level of priority of various types of determinants. This can lead to the development of a tool for evaluating reforms in health-care provider payment. Such a tool can assist policymakers in assessing potential barriers and devising suitable strategies to mitigate their negative impacts on the reform process.
Conclusions
The main barriers and facilitators to payment reform are interrelated. The same factor can act as a barrier or facilitator, depending on its characteristics. Although specific factors can be highly contextual, there are many commonalities in payment reforms worldwide. High levels of stakeholder engagement and support, government commitment, and political support, existing complementary health reform, sufficient resources and capacity, proactive change management, and previous experience in implementing reforms are all examples of facilitators. Barriers include strong resistance (usually from health-care providers), political unwillingness to reform, lack of appropriate IT systems and infrastructure, knowledge gaps, and legal, regulatory, and ethical challenges. These factors may affect different stages of reform – design, implementation, evaluation, or multiple stages simultaneously. More primary data research is needed on the specific factors that influence health-care provider payment reforms. A research gap exists, particularly in developing economies.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sein T. Health Sector Reform: Issues and Opportunities. World Health Organization/SEA/HMM/Meet; 2000.
2. Lambo E, Sambo LG. Health sector reform in sub-Saharan Africa: a synthesis of country experiences. East Afr Med J. 2003;80(6 Suppl):S1–20. doi:10.4314/eamj.v80i6.9308
3. Knill C, Tosun J. Policy making. In: Caramani D editor. Comparative Politics. Oxford University Press; 2008:495–519. doi:10.4324/9780203109823-25
4. Roberts MJ, Hsiao W, Berman P, Reich MR. The Health-Reform Cycle. Get Heal Reform Right a Guide to Improv Perform Equity. 2009. doi:10.1093/acprof:oso/9780195371505.003.0002
5. Frenk J. Dimensions of health system reform. Health Policy (New York). 1994;27(1):19–34. doi:10.1016/0168-8510(94)90155-4
6. Roberts MJ, Hsiao W, Berman P, Reich MR. Getting Health Reform Right: A Guide to Improving Performance and Equity. Oxford University Press; 2008; doi:10.1093/acprof:oso/9780195371505.001.0001
7. Braithwaite J, Mannion R, Matsuyama Y, et al. Accomplishing reform: successful case studies drawn from the health systems of 60 countries. Int J Qual Heal Care. 2017;29(6):880–886. doi:10.1093/intqhc/mzx122
8. Rechel B, Ahmedov M, Akkazieva B, Katsaga A, Khodjamurodov G, McKee M. Lessons from two decades of health reform in Central Asia. Health Policy Plan. 2012;27(4):281–287. doi:10.1093/heapol/czr040
9. DiMaggio PJ, Powell WW. The iron cage revisited: institutional isomorphism and collective rationality in organizational fields. Am Sociol Rev. 1983;48(2):147–160. doi:10.2307/2095101
10. Meyer JW, Rowan B. Institutionalized organizations: formal structure as myth and ceremony. Am J Sociol. 1977;83(2):340–363. doi:10.1086/226550
11. Scott WR, Ruef M, Mendel PJ, Caronna CA. Institutional Change and Healthcare Organizations: From Professional Dominance to Managed Care. University of Chicago Press; 2000.
12. Levesque J-F, Haggerty JL, Hogg W, et al. Barriers and facilitators for primary care reform in Canada: results from a deliberative synthesis across five provinces. Healthc Policy. 2015;11(2):44.
13. Levesque J-F, Pineault R, Provost S, et al. Assessing the evolution of primary healthcare organizations and their performance (2005-2010) in two regions of Québec province: Montreal and Montérégie. BMC Fam Pract. 2010;11(1):95. doi:10.1186/1471-2296-11-95
14. Conrad DA, Grembowski D, Hernandez SE, Lau B, Marcus‐smith M. Emerging lessons from regional and state innovation in value‐based payment reform: balancing collaboration and disruptive innovation. Milbank Q. 2014;92(3):568–623. doi:10.1111/1468-0009.12078
15. Delbanco SF, Anderson KM, Major CE, Kiser MB, Toner BW. Promising Payment Reform: risk-Sharing with Accountable Care Organizations. Commonw Fund. 2011;1530:1–33.
16. OECD. Better Ways to Pay for Health Care. OECD Health Policy Studies; 2016.
17. Langenbrunner J, Cashin C, O’Dougherty S. Designing and Implementing Health Care Provider Payment Systems: How-to Manuals. World Bank Publications; 2009.
18. Mathes T, Pieper D, Morche J, Polus S, Jaschinski T, Eikermann M. Pay for performance for hospitals. Cochrane Database Syst Rev. 2019;7(7):CD011156. doi:10.1002/14651858.CD011156.pub2
19. Jia L, Meng Q, Scott A, Yuan B, Zhang L. Payment methods for healthcare providers working in outpatient healthcare settings. Cochrane Database Syst Rev. 2021;1(1):CD011865. doi:10.1002/14651858.CD011865.pub2
20. Agarwal R, Liao JM, Gupta A, Navathe AS. The Impact Of Bundled Payment On Health Care Spending, Utilization, And Quality: a Systematic Review. Health Aff. 2020;39(1):50–57. doi:10.1377/hlthaff.2019.00784
21. Leao DLL, Cremers H-P, van Veghel D, Pavlova M, Hafkamp FJ, Groot WNJ. Facilitating and Inhibiting Factors in the Design, Implementation, and Applicability of Value-Based Payment Models: a Systematic Literature Review. Med Care Res Rev. 2023;107755872311609. doi:10.1177/10775587231160920
22. Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Q. 2004;82(4):581–629. doi:10.1111/j.0887-378X.2004.00325.x
23. Peters MDJ, Marnie C, Tricco AC, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. 2020;18(10):2119–2126. doi:10.11124/JBIES-20-00167
24. Peters MDJ, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. JBI Evid Implement. 2015;13(3):141–146.
25. Peters MDJ, Godfrey C, McInerney P, Baldini Soares C, Khalil H, Parker D. Scoping reviews. Joanna Briggs Inst Rev Man. 2017;2015:1–24.
26. Ndayishimiye C, Tambor M, Dubas-Jakóbczyk K. Barriers and facilitators of healthcare provider payment reform. Open Science Framework (OSF); November 2022. doi:10.17605/OSF.IO/Y75RE
27. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-A web and mobile app for systematic reviews. Syst Rev. 2016;5(1):1–10. doi:10.1186/s13643-016-0384-4
28. WHO EMRO. Type of Indicators; 2014. https://www.emro.who.int/child-health/research-and-evaluation/indicators/Type-of-indicators.html.
29. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
30. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
31. Tsiachristas A, Dikkers C, Boland MRS, Rutten-van Mölken MPMH. Exploring payment schemes used to promote integrated chronic care in Europe. Health Policy (New York). 2013;113(3):296–304. doi:10.1016/j.healthpol.2013.07.007
32. Annear PL, Kwon S, Lorenzoni L, et al. Pathways to DRG-based hospital payment systems in Japan, Korea, and Thailand. Health Policy (New York). 2018;122(7):707–713. doi:10.1016/j.healthpol.2018.04.013
33. Donev DM. Pay-for-performance and tools for quality assurance in health care. South East Eur J Public Heal. 2022;2022(Special Issue 1):NA. doi:10.11576/seejph-5115
34. Mathauer I, Wittenbecher F. Hospital payment systems based on diagnosis-related groups: experiences in low- and middle-income countries. Bull World Health Organ. 2013;91(August):746–756A. doi:10.2471/BLT.12.115931
35. Wojtak A, Purbhoo D . Perspectives on Advancing Bundled Payment in Ontario’s Home Care System and Beyond. Healthc Q. 2015;18 1 :18–25. doi:10.12927/hcq.2015.24248
36. Zhang L, Sun L, et al. Impacts of diagnosis-related groups payment on the healthcare providers’ behavior in China: A cross-sectional study among physicians. Risk Manag Healthc Policy. 2021;14():2263–2276. doi:10.2147/RMHP.S308183
37. Jin P, Biller-Andorno N, Wild V, et al. Ethical Implications of Case-Based Payment in China: A Systematic Analysis. Dev World Bioeth. 2015;15(3):134–142. doi:10.1111/dewb.12055
38. Zhao C, Wang C, Shen C, Wang Q . Diagnosis-related group (DRG)-based case-mix funding system, a promising alternative for fee for service payment in China. Biosci Trends. 2018;12(2):109–115. doi:10.5582/bst.2017.01289
39. Duran D, Bauhoff S, Berman P et al. The role of health system context in the design and implementation of performance-based financing: evidence from Cote d’Ivoire BMJ Glob Heal. 2020;5(e002934):1–10. doi:10.1136/bmjgh-2020-002934
40. Or, Z. Implementation of DRG Payment in France: issues and recent developments.Health Policy (New York). 2016;117(2) :146–150 doi:10.1016/j.healthpol.2014.05.006
41. Issahaku Y, Thoumi A, Abiiro GA, Ogbouji O, Nonvignon J. Is value-based payment for healthcare feasible under Ghana’s National Health Insurance Scheme? Heal Res Policy Syst. 2021;19(1):145. doi:10.1186/s12961-021-00794-y
42. Takyi E, Danquah, A. Rolling Out the capitation payment system in Ghana: Lessons from the pilot implementation in Ashanti Region. SSRN. 2015. https://dx.doi.org/10.2139/ssrn.2641605
43. Andoh-Adjei F-X, Nsiah-Boateng E, Asante, FA, van der Velden, K, Spaan, E. Provider preference for payment method under a national health insurance scheme: a survey of health insurance-credentialed health care providers in Ghana. PLoS One. 2019;14(8). doi:10.1371/journal.pone.0221195
44. Nagy B, Brandtmüller Á. Implementing Risk Adjusted Capitation Payments with Health Care Reforms in Hungary. Competitio. 2008;7(2):147–160. doi:10.21845/comp/2008/2/8
45. Tan SY. Bureaucratic autonomy and policy capacity in the implementation of capitation payment systems in primary healthcare: comparative case studies of three districts in Central Java, Indonesia. J Asian Public Policy. 2019;12(3):330–350. doi:10.1080/17516234.2018.1459150
46. Babashahy S, Baghbanian A, Manavi S, Sari AA, Manesh AO, Ronasiyan R. Towards Reforming Health Provider Payment Methods: Evidence from Iran. Heal SCOPE. 2017;(6)1:e33575 doi:10.5812/jhealthscope.33575
47. Kwon S.Payment system reform for health care providers in Korea. Health Policy Plan.2003;18(1):84–92.doi:10.1093/heapol/18.1.84
48. de Vries EF, Drewes HW, Struijs JN, Heijink R, Baan CA. Barriers to payment reform: experiences from nine Dutch population health management sites. Health Policy (New York). 2019;4149(1–9). doi:10.1016/j.healthpol.2019.09.006
49. Tummers LG, Van de Walle S. Explaining health care professionals’ resistance to implement Diagnosis Related Groups:(No) benefits for society, patients and professionals. Health Policy (New York). 2012;108(2–3):158–166. doi:10.1016/j.healthpol.2012.08.024
50. Chukwuma, A, Comsa, R, Chen, D, Gong, E. Provider Payment Reforms for Improved Primary Health Care in Romania. Health Nutrition and Population, World Bank.Washingt, DC,August 2021.
51. Radu C-P, Haraga S. The Romanian model of hospital financing reform. J Public Health (Bangkok). 2008;16(3):229–234. doi:10.1007/s10389-007-0170-9
52. Eriksson T, Levin L-Å, Nedlund, A-C. The introduction of a value-based reimbursement programme-Alignment and resistance among healthcare providers. Int J Health Plann Manage. 2022;1–20. doi:10.1002/hpm.3574
53. Aktas P. Physician perspectives on the implications of the diagnosis-related groups for medical practice in Turkey: A qualitative study. Int J Health Plann Manage. 2022;37(3):1769–1780. doi:10.1002/hpm.3445
54. Dredge, R. Payment by Results as a lever for NHS reforms. J Manag Mark Healthc. 2008; 1(4):375–381 doi:10.0.4.155/mmh.2008.1.4.375
55. Doran, T Lessons from early experience with pay for performance . Dis Manag Heal Outcomes; 2008 16 2 69–77 doi:10.2165/00115677-200816020-00001
56. Hussey PS, Ridgely MS, Rosenthal MB. The PROMETHEUS bundled payment experiment: slow start shows problems in implementing new payment models. Health Aff. 2011;30(11):2116–2124. doi:10.1377/hlthaff.2011.0784
57. Bokhour BG, Burgess JFJ, Hook, JM et al. Incentive implementation in physician practices: A qualitative study of practice executive perspectives on pay for performance. Med Care Res Rev. 2006;63(1 Suppl):73S–95S. doi:10.1177/1077558705283645
58. Kamath AF, Courtney PM, Bozic KJ, Mehta, S, Parsley, BS, Froimson, MI, et al. Bundled payment in total joint care: survey of AAHKS membership attitudes and experience with alternative payment models. J Arthroplasty. 2015; 30(12):2045–2056 doi:10.1016/j.arth.2015.05.036
59. Whitcomb WF, Lagu T, Krushell RJ et al, et al. Experience with designing and implementing a bundled payment program for total Hip replacement. Jt Comm J Qual Patient Saf. 2015;41(9):406–413. doi:10.1016/s1553-7250(15)41052-9
60. Blustein J, Weissman, JS, Ryan, AM, Doran, T. Analysis Raises Questions On Whether Pay-For-Performance In Medicaid Can Efficiently Reduce Racial And Ethnic Disparities. Health Aff. 2011;30(6):1165–1175. doi:10.1377/hlthaff.2010.1022
61. Miller, HD. Ten Barriers to Healthcare Payment Reform And How to Overcome Them.
62. University of Washington.Robert Wood Johnson Foundation Payment Reform Evaluation Project Development of Models for Comprehensive Payment Reform in Vermont Green Mountain Care Board; 2015.
63. Hilary K, Johnson Foundation RW, Academy Health. Facilitators and Barriers to Payment Reform :Market-Based, Governmaental, Organizational, and Design Considerations. 2021.
64. University of Washington . Transforming Payment for Oregon’s Community Health Centers through an Alternative Payment Methodology; 2015.
65. Bencic S, Cabral L, Friedman A et al. Payment Reform in Diverse Practice Settings: Making Patient-Centered Medical Homes and Episodes of Care Work for Low-Volume Medicaid Providers in Tennessee.Woodrow Wilson School of Public and International Affairs, Princeton University;2016.
66. Crook, HL, Zheng, J, Bleser, WK, Whitaker, RG, Masand, J, Saunders, RS. How Are Payment Reforms Addressing Social Determinants of Health ?Policy Implications and Next Steps; 2021.
67. Damberg CL, Sorbero ME, Lovejoy, SL, Martsolf, GR, Raaen, L, Mandel, D. Measuring Success in Health Care Value-Based Purchasing Programs: Findings from an Environmental Scan, Literature Review, and Expert Panel Discussions. Rand Heal Q. 2014;4(3):9.
68. Dummit, LA.Medicare’s Bundling Pilot: Including Post-Acute Care Services Washington, DC: National Health Policy Forum;2011.
69. Voinea-Griffin A, Rindal DB, Fellows JL, Barasch A, Gilbert GH, Safford MM. Pay-for-performance in dentistry: what we know. J Healthc Qual. 2010;32(1):51–58. doi:10.1111/j.1945-1474.2009.00064.x
70. Bozic, KJ, Smith, AR, Mauerhan, DR. Pay-For-Performance in Orthopedics. Implications for Clinical Practice. J Arthroplasty. 2007;22(6 SUPPL):8–12. doi:10.1016/j.arth.2007.04.015
71. Randazzo, G, Brown, Z. Transitioning from volume to value: A strategic approach to design and implementation. Nurs Adm Q. 2016;40(2):130–136. doi:10.1097/NAQ.0000000000000153
72. Lowder, JL, Barker, MA, Ferzandi, T et al. Developing an Advanced Alternative Payment Model for Stress Urinary Incontinence. Female Pelvic Medicine & Reconstructive Surgery.2021;27(4):217–222. doi:10.1097/SPV.0000000000000997
73. Mcclellan, MB, Feinberg, DT, Bach, PB et al. Payment Reform for Better Value and Medical Innovation. A Vital Direction for Health and Health Care.National Academiy of Medicine;2017.
74. Bertko J, Effros, R. Increase the Use of “Bundled” Payment Approaches. Rand Heal Q. 2011; 1 (3): 15.
75. Antonova, E, Boye, ME, Sen, N, O’Sullivan, AK, Burge, R, et al. Can Bundled Payment Improve Quality and Efficiency of Care for Patients with Hip Fractures? J Aging Soc Policy. 2015;27(1):1–20. doi:10.1080/08959420.2015.970844
76. Mcclellan M. Reforming Payments to Healthcare Providers : The Key to Slowing Healthcare Cost Growth While Improving Quality ?J Econ Perspect. 2011;25(2):69–92. doi:10.1257/jep.25.2.69
77. Voinea-Griffin A, Rindal DB, Fellows JL, Barasch, A, Gilbert, GH, Safford, MM, et al. Pay-for-performance in dentistry: what we know. J Healthc Qual. 2010;32(1):51–58. doi:10.1111/j.1945-1474.2009.00064.x
78. Seth Greenwald, A, Bassano, A, Wiggins, S et al.Alternative reimbursement models: Bundled payment and beyond. J Bone Jt Surg - Am Vol. 2016; 98(e45) :1–7. doi:10.2106/JBJS.15.01174
79. Hobbs Knutson, K, Wennberg, D, Rajkumar, D.Driving Access and Quality: A Shift to Value-Based Behavioral Health Care. Psychiatr Serv. 2021; 72(8) : 943–950. doi:10.1176/appi.ps.202000386
80. Tanenbaum SJ . Pay for performance in Medicare: evidentiary irony and the politics of value. J Health Polit Policy Law. 2009;34(5):717–746. doi:10.1215/03616878-2009-023
81. Van de Bovenkamp, HM,:Trappenburg, MJ, Grit, KJ.Patient participation in collective healthcare decision making: the Dutch model. Heal Expect. 2010; 13 (1): 73–85. doi:10.1111/j.1369-7625.2009.00567.x
82. Baggott R, Forster R. Health consumer and patients’ organizations in Europe: towards a comparative analysis. Heal Expect. 2008;11(1):85–94.
83. World Health Organization. Implementing Citizen Engagement within Evidence-Informed Policy-Making: An Overview of Purpose and Methods. World Health Organization; 2022.
84. Kohn A. Punished by rewards: The trouble with gold stars, incentive plans, A’s, praise, and other bribes. New York; 1993.
85. Braithwaite J, Matsuyama Y, Mannion R, Johnson J, Bates DW, Hughes C. How to do better health reform: a snapshot of change and improvement initiatives in the health systems of 30 countries. Int J Qual Heal Care. 2016;28(6):843–846.
86. Chibuzor M, Arikpo I, Aquaisua E, et al. Implementation of health workforce information systems: a review of eight sub-Saharan country experiences. J Public Health. 2021;43(Suppl 1):i27–i40. doi:10.1093/pubmed/fdaa263
87. WHO Regional Office for Europe. Health and Care Workforce in Europe: Time to Act. World Health Organization. Regional Office for Europe; 2022.
88. Institute of Medicine. Digital Infrastructure for the Learning Health System: The Foundation for Continuous Improvement in Health and Health Care: Workshop Series Summary. Washington, DC: The National Academies Press; 2011. doi:10.17226/12912
89. Ndayishimiye C, Lopes H, Middleton J. A systematic scoping review of digital health technologies during COVID-19: a new normal in primary health care delivery. Health Technol. 2023;13(2):273–284. doi:10.1007/s12553-023-00725-7
90. World Health Organization. Continuity and Coordination of Care: A Practice Brief to Support Implementation of the WHO Framework on Integrated People-Centred Health Services. World Health Organization; 2018.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.