Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 14
Barriers and Facilitators to Successful Intensive Adherence Counseling in Rural Northern Uganda: An Exploratory Interview with HIV-Positive Clients Using the COM-B Framework
Authors Beja H ![]() , Daisy N, Edek MT, Kobusinge V, Akaki O, Owachgiu IO, Udho S
, Daisy N, Edek MT, Kobusinge V, Akaki O, Owachgiu IO, Udho S ![]()
Received 17 October 2022
Accepted for publication 16 November 2022
Published 21 November 2022 Volume 2022:14 Pages 553—563
DOI https://doi.org/10.2147/HIV.S393093
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Humphrey Beja,1 Nakayiwa Daisy,2 Micheal Tonny Edek,1 Veronic Kobusinge,1 Oscar Akaki,3 Innocent Ocitti Owachgiu,1 Samson Udho1
1Department of Midwifery, Faculty of Nursing & Midwifery, Lira University, Lira, Uganda; 2Department of Psychiatry, Faculty of Medicine, Lira University, Lira, Uganda; 3Department of Environmental Health & Disease Control, Faculty of Public Health, Lira University, Lira, Uganda
Correspondence: Samson Udho, Department of Midwifery, Faculty of Nursing & Midwifery, Lira University, P.O Box 1035, Lira, Uganda, Tel +256 785 588 257, Email [email protected]
Purpose: Intensive adherence counseling (IAC) was introduced as a strategy to enhance adherence to antiretroviral therapy (ART) among HIV clients with non-suppressed viral loads. There has been sub-optimal viral load suppression among HIV clients in Uganda enrolled in IAC. However, there is a scarcity of literature on the barriers and facilitators of successful IAC. We aim to explore the barriers and facilitators to successful IAC among HIV-positive clients seeking care in public health facilities in rural northern Uganda.
Patients and Methods: This was an exploratory qualitative study conducted among 15 purposively sampled HIV-positive clients enrolled in IAC in public health facilities offering ART services in northern Uganda. We conducted in-depth interviews using semi-structured interview guides based on the capability, opportunity, motivation, and behavior (COM-B) framework for behaviour change. Data were analyzed using the deductive thematic approach of Braun and Clarke following the COM-B framework.
Results: The majority of the participants were females (60%), married (53%), and attained primary education (47%). Barriers to successful IAC were Capability – alcoholism and promiscuity, Opportunity – stigma and discrimination, delayed viral load result, shortage of food, and heavy workload; and Motivation – deteriorating health and lack of incentives. Facilitators to successful IAC were Capability – good knowledge of ART, good memory, and reminder alerts; Opportunity – availability of ART, social support, availability of ART, prolonged ART refill, and good counseling; and Motivation – desire to live longer and healthy and the desire to fulfill dreams and goals.
Conclusion: Successful implementation of IAC needs to consider the context of the person in care thus the need to strengthen individualized IAC sessions. HIV care providers can adopt the COM-B framework to perform individualized IACs and use the information to strengthen the counseling sessions.
Keywords: barriers, facilitators, HIV, intensive adherence counseling
Introduction
HIV/AIDS remains a global public health challenge with 38 million people living with HIV, 1.7 million HIV new infections, and 690,000 AIDS-related deaths.1 Sub-Saharan Africa is still disproportionately affected by HIV/AIDS with 25.6 million people living with HIV, 730,000 HIV new infections, and 300,000 AIDS-related deaths.1 In Uganda, there are still 1.4 million people living with HIV, 38,000 HIV new infections, and 22,000 AIDS-related deaths.2 The prevalence of HIV in Uganda among adults, aged 15 to 49 years, is estimated at 5.4%.2
Uganda has made substantial progress in the fight against HIV/AIDS following the adoption and implementation of the UNAIDS 90–90-90 targets.3 In Uganda, 91% of people are aware of their HIV status of which 90% are on HIV treatment, and of which, 82% are virally suppressed.2 Viral load non-suppression is the only UNAIDS 2020 target that was not achieved by Uganda. HIV-positive clients are said to be virally non-suppressed when their viral load exceeds 1000 copies/mL.3 Viral load non-suppression among HIV-positive clients is usually because of nonadherence to antiretroviral therapy (ART). Non-adherence to ART may be intentional or unintentional.4 Intentional non-adherence to ART is the active process whereby the patient chooses to deviate from the treatment regimen while unintentional nonadherence is the passive process in which the patient may be careless or forgetful about adhering to the treatment regimen.4 Non-adherence to ART is associated with drug resistance which leads to treatment failure and ultimately HIV/AIDS-related morbidity and mortality.
Adherence to ART may be influenced by individuals’ capability to adhere to ART, the opportunity to adhere to ART, or intrinsic motivation to remain adherent to medication.5 Barriers to ART adherence refer to factors that prevent HIV-positive clients from adhering to their antiretroviral medication while facilitators are factors that enable HIV-positive clients to adhere to their antiretroviral medication as prescribed by the healthcare provider.4 Intensive adherence counseling (IAC) has been adopted by the Ministry of Health of Uganda as one of the strategies to address non-adherence to ART. IAC is the continued and repeated process that involves a structured assessment of the current level of ART adherence, exploring the specific barriers the patient must overcome, assisting patients to identify solutions to the barriers, and developing an individualized adherence intervention.3
Previous studies found IAC to be associated with enhanced viral load suppression among HIV-1 clients who were previously non-suppressed.6–8 Conversely, evidence from other contexts indicates that there are sub-optimal HIV-1 viral load suppression rates following the IAC program.9–12 Informal interactions with HIV healthcare providers in the context of rural northern Uganda also indicated that some HIV-positive clients remain virally non-suppressed even after IAC. This could be attributed to the weak healthcare systems in such contexts which undermines harnessing the benefits of IAC. Unfortunately, there is a paucity of literature explaining why IAC is ineffective in achieving HIV-1 viral load suppression in such contexts.11 A structured exploration of the barriers and facilitators to successful IAC using the Capacity, Opportunity, and Motivation, for Behavior (B) change framework (COM-B framework) from the perspective of HIV-positive clients, may yield valuable information that may inform the design of interventions to harness the full potential of IAC as found in previous studies.6–8 Therefore, the purpose of this study was to explore the barriers and facilitators to successful IAC among HIV-positive clients seeking care in public health facilities in rural northern Uganda.
The COM-B Theoretical Framework
We adopted the COM-B framework which is composed of four components, namely, Capability (C), Opportunity (O), Motivation (M), and Behavior (B) hence the name, the COM-B framework.5,13 Capability is all the knowledge, skills, and abilities to adhere to a behavior.5,13 Opportunity refers to all the factors that lie outside the individual that prompt or make them adhere to a particular behavior while motivation refers to all the internal processes that influence decision making for behavior change.5,13 The model proposes that for one to perform a particular behavior, one must feel they are both psychologically and physically able to do so, have the social and physical opportunity to engage in the behavior, and want or need to carry out the behavior more than other competing behaviors.5,13 The barriers and facilitators to viral load suppression among HIV-positive clients enrolled in the IAC program were identified using the COM-B framework. The framework is illustrated in Figure 1.
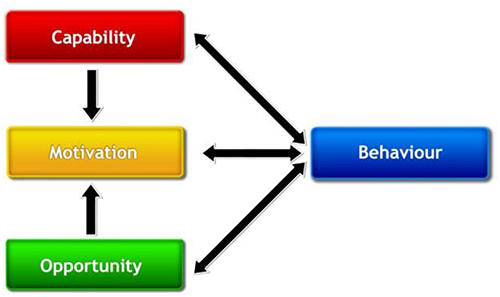 |
Figure 1 COM-B framework of understanding behavior change. Notes: Reproduced with permission from Michie, (S), van Stralen, (M)M. and West, (R) The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implementation Sci 6, 42 (2011). License: http://creativecommons.org/licenses/by/2.0. |
Methods
Study Design and Setting
We conducted a qualitative descriptive study in March 2021 to explore the barriers and facilitators to successful intensive adherence counselling (IAC) among HIV-positive clients in rural northern Uganda. The study was performed from a constructivist point of view and it was conceptualized by BH, DN, VK, OA, and IOO in consultation with SU.
The study was conducted in the ART clinic of Ogur and Amach Health Center (H/C) IV which records high volume of HIV-positive clients enrolled into IAC. These healthcare facilities are located in Lira District, northern Uganda which is located approximately 342 kilometers by road to Kampala, the capital city of Uganda. In Uganda, the provision of ART services starts from Health Center III and above. Lira District has two Health Center IV and five Health Center III. The ART clinics in Ogur and Amach H/C IV have the highest number of HIV-positive clients enrolled into IAC. The health facilities run from Monday to Friday from 8:00 to 17:00 Hours and they offer IAC at least once per week. Each of the ART clinics has at least one clinical officer, two nurses, two counselors, and other auxiliary staff.
Study Participants and Sampling Criteria
The study was conducted among HIV-positive clients seeking care in Amach and Ogur Health Center IV in Lira District, northern Uganda. We purposively recruited 15 participants who spoke to the research aims and had the experience of the phenomenon under scrutiny.3 The principle of information power was used to estimate the sample size.4 We sampled HIV-positive clients aged 18 years and above, enrolled in IAC, and who could speak either Lango or the English language. We excluded HIV-positive clients who were enrolled in IAC for less than one week and those enrolled for more than a week but never had a session of IAC. Clients who were busy at the time of data collection were excluded from the study.
Recruitment of Participants
A client linkage facilitator helped the research assistants to identify and recruit the eligible study participants at each of the health facilities. Some of the participants were identified by the research assistants during their interactions at the health facilities. Upon identifying the eligible prospective participants, the research assistants explained the purpose, benefits, and risks of participating in the study to the prospective participants. Out of the 18 eligible prospective participants approached, 15 consented to participate in the study and were recruited in the study. The venue and time of conducting the in-depth interview were arranged with the participants at their convenience.
Data Collection
We conducted face-to-face in-depth interviews (IDI) using a semi-structured interview guide with open-ended questions based on the COM-B framework to explore the barriers and the facilitators to successful IAC. The interview guides were developed by HB and SU and were pilot tested among HIV-positive clients who were not included in the study and revisions were made accordingly. The interview guide had five sections comprising socio-demographic characteristics of the study participants and the four components of the COM-B framework. Each component of the interview guide had a different trigger question based on the COM-B framework. The interviews were conducted by trained research assistants who asked open-ended questions to elicit information for each of the sections based on the interview guide (Appendix 1). The interviews were conducted in Lango (local dialect) and English language in a private setting within the health facility or the participants’ homes. The interviews lasted for 30 to 45 minutes and they were audio-recorded using an audio recorder while field notes were also taken on the body language and feelings of the participant at the time of data collection.
Data Analysis
Data were transcribed verbatim by two research assistants and the transcripts were verified against the audio recordings by SU and HB to clarify any unclear information before permitting the data clerks to conduct the next sets of interviews. We conducted the deductive thematic analysis as described by Braun and Clarke.14 Semantic manual data coding was independently done by SU and HB in accordance with the COM-B domains of capability, opportunity, motivation, and behaviors. Discrepancies in codes were resolved through consultation involving SU and HB. Iterative group discussions were held with other authors, MTE, VK, OA, DN, and IOO to agree on which responses were barriers and facilitators to successful IAC. Data were presented as direct quotes while providing a contextual explanation of the barriers and facilitators to successful IAC among the study participants.
Scientific Rigor and Trustworthiness
Five strategies and principles of credibility, dependability, confirmability, transferability, and reflexivity were used to ensure and maintain rigor and trustworthiness in our study.15 Credibility was maintained by restating and summarizing information during the interviews and taking field notes on body language during the interviews by the research assistants. Dependability and confirmability were ensured by audio-recording of interviews against which findings and interpretations were crossed-checked. Group discussions in moments of disagreement during data analysis also ensured the dependability and confirmability of our data. Transferability was maintained by identifying participants who could fully express themselves and making a thick description of the study methods. As recommended as part of primary qualitative research, we reflected on how our backgrounds and positions might have influenced our conceptualization, data collection, analysis, and interpretation of data. HB, MTE, VK, and IOO are undergraduate midwifery students who have had some clinical exposure with care of HIV-positive clients in rural settings. DA and OA are undergraduate psychiatry and public health students with minimal exposure to the care of HIV-positive clients. SU is a certified nurse-midwife with seven years of clinical and classroom teaching and three years of active clinical care of patients including HIV-positive clients in low-resource settings. We are therefore somewhat aware of what hinders HIV-positive clients from receiving optimal care and we are sympathetic to the challenges HIV-positive clients go through while enrolled on ART. The research team maintained reflexivity by recording, discussing, and challenging established assumptions about the study contexts.
Ethical Considerations
The study was conducted under the 2013 Declaration of Helsinki. The study protocol was reviewed and cleared by Gulu University Research and Ethics Committee (GUREC) (GUREC-2021-168). The protocol was cleared for data collection in Uganda by Uganda National Council for Science and Technology (RESCLEAAR/01). Administrative clearance was further obtained from the office of the District Health Officer of Lira District and the Hospital administration of Ogur and Amach Health Center IV. Written informed consent was obtained from all participants to participate in the study and publish this data. Privacy and confidentiality were maintained throughout the study by not including identifiable information in addition to conducting the interviews in a private space. All the recorded materials and transcripts were password protected and kept under lock and key by SU while all the data clerks signed nondisclosure agreements of the data collected.
Results
Socio-Demographic Characteristics of Study Participants
We conducted a total of 15 in-depth interviews with HIV-positive clients. The age of the participants ranged from 19 to 59 years, the majority of the participants were subsistence farmer (73%), females (60%), and married (53%) while 47% had attained primary level education. Table 1 describes the study participants.
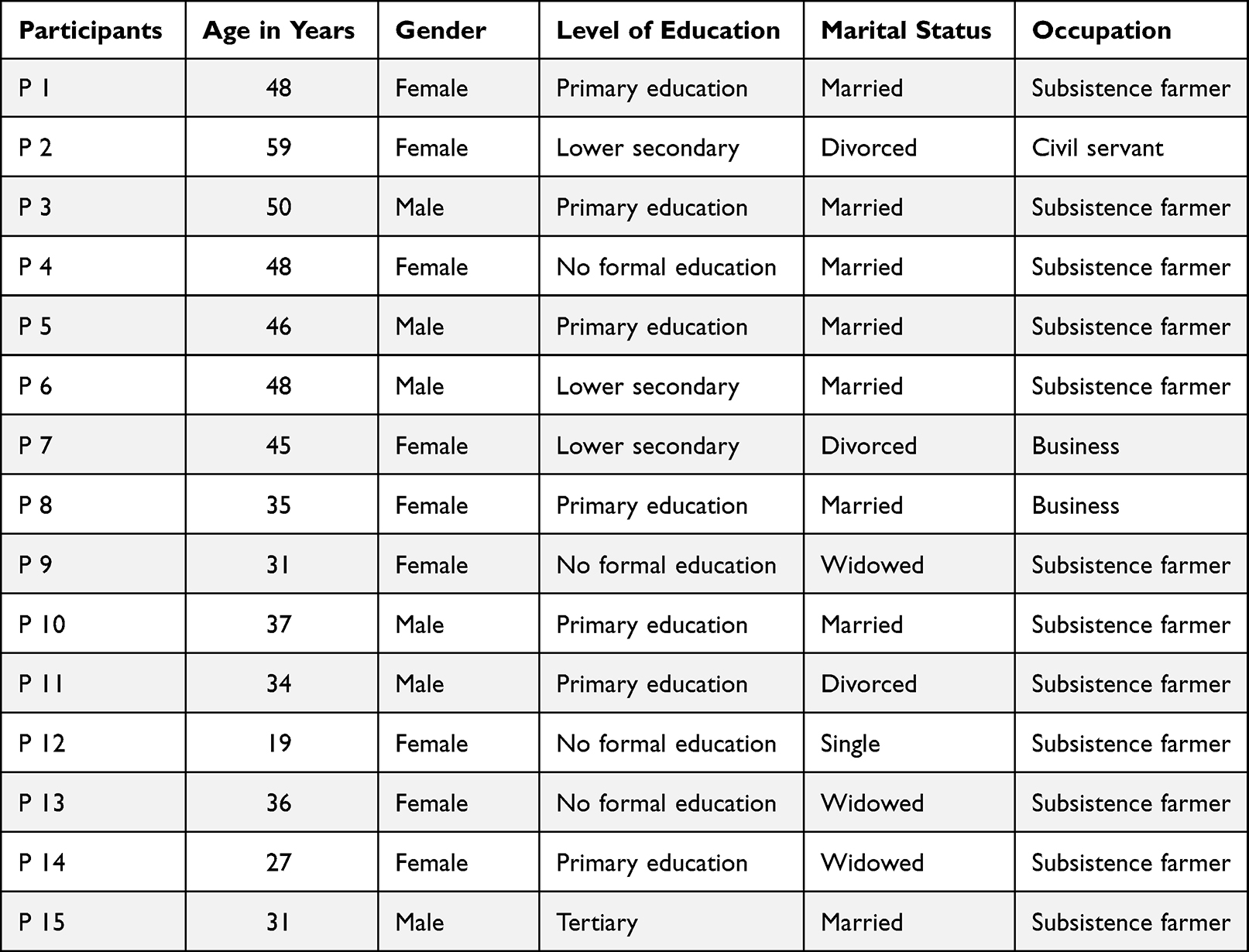 |
Table 1 Description of the Study Participants |
Barriers and Facilitators to Successful IAC Among HIV-Positive Clients
We structured the barriers and facilitators to successful IAC around the three domains of the COM-B framework as shown in Figure 2.
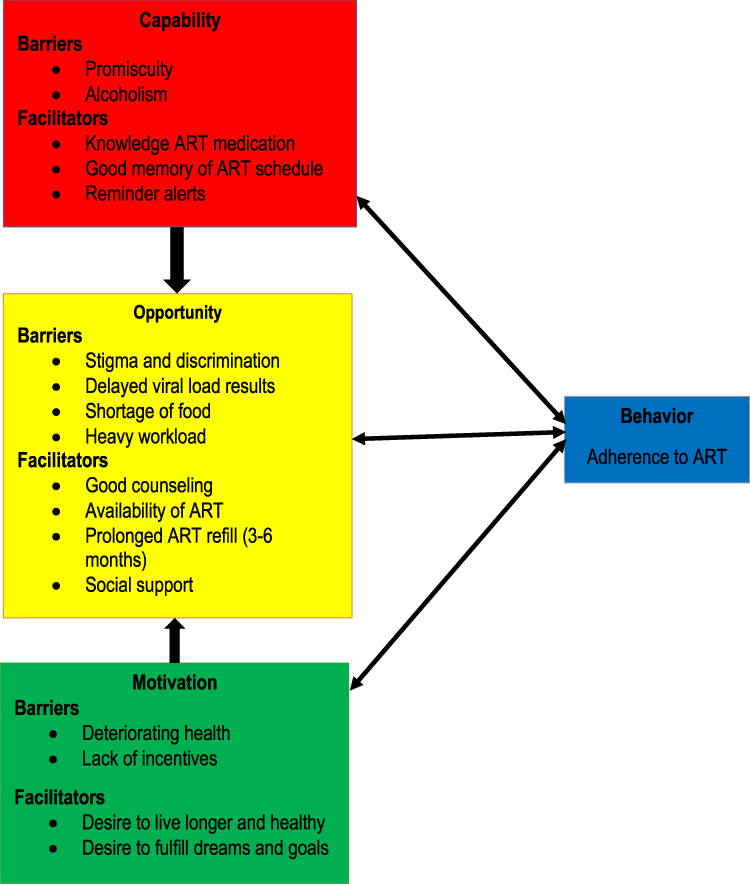 |
Figure 2 Barriers and facilitators to successful intensive adherence counseling. |
The factors that negatively affected any components of the COM-B framework were classified as barriers and those that positively affected the components were regarded as facilitators.
Capacity
We explored the capacity (physical and psychological) of HIV-positive clients enrolled in intensive adherence counseling (IAC) to adhere to antiretroviral therapy (ART) while enrolled in IAC. The majority of the study participants expressed that promiscuity was at the center of their non-adherence to ART and unsuppressed viral load while enrolled in IAC. Respondents reported that promiscuity interfered with their routine of taking medication because of fear of disclosing their HIV-positive status to their new sexual partners which compelled them to leave their medication behind in case they were moving in with the new sexual partner. This is typified by a response from one of the study participants.
First of all, I want to say that what leads to a lack of medication adherence is that If I am a man who doesn’t have a wife and I’m living with HIV, when it reaches a point that I am supposed to take my medication but you find the focus is on following a woman that you had been talking to and sometimes you end up not coming back in case that woman allows to accommodate you that night. So once you go it means you’ll miss your medication because you have forgotten it at home. Participant 3
Some participants reported that alcoholism was a major barrier to successful IAC. This was because they could forget their medication as prescribed since they are drunk while others were taken up in the business of selling alcohol. Sometimes they have a hang-over which makes them lose the appetite to take their medicine in fear for side effects as narrated by these respondents.
What I was doing that made me default my treatment was alcohol. Sometimes I get drunk and I would forget to take the medication and at times I would sleep out of home and which means that I have moved without my medication. Sometimes I am even too angry to even take my medicines because of alcohol. Participant 5
The problem is that when you have very many people at home [the customers] who have come to take alcohol you don’t get time to take the medication, their presence would not give me time to cook and also to take my medication because from the training we have received they told us that you should eat and you should take the medication at the right time that you were told to do so. Participant 4
On the other hand, one of the key facilitators to successful IAC among the study participants was adequate knowledge about how to take their medicines. The participants’ good knowledge was attributed to the quality of counseling offered during the IAC sessions where they were taught how to take their medicines and manage the common side effects of the medicines.
When I enrolled in AIC, the counselor started teaching me how to swallow the drugs and encouraging me to keep taking ARVs and that I may live up to old age, also telling me that many people are taking ARVs. So nowadays I take my drugs, unlike those days. Participant 15
Some of the study participants suggested that their good memory of medication schedules was a major facilitator of successful IAC. Although reminders can sometimes be helpful to trigger a memory of when to take medication, it was also very important that one has the intrinsic capacity to recall their medication schedules to avoid missing their pills.
……once I wake up in the morning after brushing, the first thing that I do is check in this my phone (showing the phone) to ensure it is 8:00 hours. Once I haven’t taken my medicine I cannot engage myself in any activities. Even if I move away I have it in my head that there is something that I need to do, something is missing that I haven’t done and I can easily remember when it is time for my medication, and at once I run to where my tin for the medicine is placed and swallow my medicine. Even if I was in the garden, I can take a bicycle to rush for the medicine…. Participant 8
Opportunity
When we explored the opportunities for successful IAC, we found that the majority of the respondents had a heavy workload which left them exhausted to a point where they could not take their medicines. Most of the study participants were subsistence farmer and it is plausible that the hectic garden work left most of them tired. This is exemplified by a quote from one of the study participants.
…. too much work makes it difficult for me to remain strong enough to keep taking the medicines as prescribed. Sometimes when I am in the garden, I even forget to take my medicine even if I had not intended to miss it. It’s not that we are not supposed to work but you have to do something that does not overpower your energy. Participant 5
Stigma and discrimination were major barriers to successful IAC among the study participants. Although IAC sessions are supposed to incorporate aspects of coping with stigma and discrimination, it appeared that most of the study participants had not yet developed sufficient coping mechanisms to a point where the stigma and discrimination directed at them affected their adherence to their medicines hence returning unsuppressed viral load results.
In my environment especially in my home, the thing that affects me negatively are the neighbors who sometimes come to my home and they begin abusing me that I am useless. Sometimes they come and tell me that you are very sick, why are you still using or digging this garden, this garden belongs to me so they end up having a land wrangle with me on the garden which belongs to me, so such things make me sad and sometimes I feel like refusing to take my medication. Participant 6
My blood brother abuses me, saying I have HIV and that I am going to die, that I should not struggle for land with him. This hurts me and sometimes makes me forget to take my medicine. Participant 10
The participants also added that delayed viral load results kept most of them guessing whether they were performing well in the IAC program. This left most of them discouraged and they started to lose focus on taking their medication.
Sometimes our viral load takes a long time to come back and sometimes we are not given making us stay relaxed not knowing whether the result is good or not. I think it would be a good thing for us to be regularly updated about how we are doing on treatment as soon as our results are back. Participant 5
The majority of the study participants indicated that lack of food was a major reason for their non-adherence to medication while on the IAC program. Most ART regimens are best taken with a meal to lessen the side effects. If the clients did not anticipate having a meal, they shied away from taking their medicine for fear of the side effects.
The only thing that I feel is missing that should have helped us in attending this training successfully is that sometimes we feel very hungry, in our houses of course sometimes we don’t get things to eat… that make it very difficult to take the medication in the right way and also when you come for this training the whole day without anything to eat, it’s a lot of discomforts. Participant 6
On the other hand, quality counseling played a key role in ensuring that these participants remain adherent to their medication while on the IAC program. This was attributed to the great work being done by the counselors and others healthcare workers at the facility who availed them of all the relevant information they needed to remain adherent to their medicine.
After joining this program [IAC program], the very many thoughts I used to think about are no more because I was properly advised to forget the past and focus on my health, and I am glad I did so. Participant 6
Some of the participants also credited their success in the IAC program to the availability of ART within the health facility at all times. In recent years, ART has become one of the most readily available medicines in public health facilities in Uganda. This has ensured that all HIV-positive clients get constant ART refills. In some instances, the clients also get prolonged ART refills for up to three to six months when they achieve viral load suppressions.
….the medications are never out of stock. What I want to say is that God should continue blessing the work of our leaders…… we’re receiving our medication and I have some remaining at home….we get the medications for full five or six months in advance. Participant 4
The presence of social support was a major boost to successful IAC for most of the study participants. The support came from family members, peers, and friends in form of encouragement, material giving, and positive affirmation of their HIV-positive status.
I have friends and I am a member of a group for communal digging. It is only myself who is living positively, the rest of the group members are not. They lend me money which I use to buy clothes and food which I can cook. My friends don’t talk ill of me, they encourage me to keep on taking my drugs. Participant 12
Motivation
The primary motivational barrier to successful IAC was deteriorating health while enrolled in the IAC program. The IAC program by design is meant for HIV-positive clients who have not achieved viral load suppression and are, therefore in a poor health state. The absence of improvement while enrolled in the program made some of them lose hope and begin to default on their medication hence unsuppressed viral load.
I felt demotivated, I was feeling so sick and when I went to the hospital for a checkup I found that the results were not good and I even had other infections. I felt like maybe I should discontinue taking ARVs, sit back, and wait for death. Participant 1
In addition, the majority of the study participants also indicated that the lack of incentive to remain adherent to ART while enrolled in the IAC program also prompted some of them to lose the moral to remain adherent to their medicine. Previous HIV programs had initiated simple incentives such as giving porridge to HIV-positive clients when they come for routine care, but that has stopped since those programs have scaled-down. This is explicated by a response from one of the participants.
What is the reward for not defaulting treatment anyway? If they were giving us small gifts for not defaulting our treatment, maybe people like me would not still have high levels of the virus in their blood. I would work harder so that I get the gift. I remember when they used to give us porridge for attending the training, [IAC sessions], many people were coming for the training. Participant 1
Conversely, most of the study participants indicated that the desire to live longer and be healthy was a major driving force in their success while enrolled in the IAC program. This was attributed to the fact that most of them had children to look after and they feared that when they were deceased, no one would step up to take care of their children. In addition, they felt that staying on medication relieved them from a lot of body pains.
I am also doing that for the sake of my life because I want to live longer and healthy so that when I’m among people I don’t look like one who is living positively. Participant 5
The most important reason why I will never stop taking my medication or stop attending this training session is that I want to stay alive. My family is still young and I cannot afford to leave them alone at this time. Participant 6
Some of the participants remained in treatment so that they could live to fulfill their dreams and goals in life. It was interesting to note that the rural status of these participants did not hold back some of them from having big ambitions in life and becoming exemplary to other HIV-positive clients. This was typified by a response from one of the study participants.
Pertaining myself looking ahead of my life as I am taking my medication I feel that I should stay long and do so many things in life so that I become a good example that once you take your medication well you get that opportunity to fulfill your dreams in life. Participant 8
Discussion
We aimed to explore the barriers and facilitators to successful IAC among HIV-positive clients seeking care in public health facilities in rural northern Uganda using the COM-B framework. We found that the barriers to successful IAC were alcoholism, promiscuity, stigma and discrimination, delayed viral load result, shortage of food, heavy workload, deteriorating health, and lack of incentives. The facilitators to successful IAC included good knowledge of ART, good memory, reminder alerts, availability of ART, social support, availability of ART, prolonged ART refill, good counseling, desire to live longer and healthy, and the desire to fulfill dreams and goals. Our results shed light on why the IAC program intended to help HIV-positive clients achieve viral load suppression has had mixed outcomes in previous studies.
Capacity-Related Barriers to Successful IAC
We found that the capacity-related barriers to successful IAC were majorly promiscuity and alcoholism. These results can be attributed to the single-marital status of some of the participants, and reports of unstable family relationships. It could also be attributed to the low educational levels of our study participants which may undermine their risk perceptions. The results of our study are similar to the results of related previous studies which found that alcoholism and promiscuity can undermine adherence to ART.16–19 During IAC, attempts should be made by the counselors to explore the history of alcoholism and promiscuity among HIV-positive clients enrolled in IAC, and efforts should be made to address the problem with the clients.
Opportunity-Related Barriers to Successful IAC
Our study found that the major opportunity-related barriers to successful IAC are stigma and discrimination, shortage of food, delayed viral load results, and heavy workload. These results are plausible because all these are critical external factors that disturb HIV-positive clients psychologically to appoint where they may become non-adherent to their drugs hence unsuppressed viral load due to forgetfulness, anger, and fear of taking their drugs on an empty stomach. Our studies are similar to the results of previous studies conducted in Uganda,19,20 Eswatini,18 and a systematic review on barriers and facilitators to ART adherence in sub-Saharan Africa21 which showed that stigma and discrimination, shortage of food, delayed viral load results, and heavy workload can lead to non-adherence to ART hence unsuppressed viral load. We encourage HIV service providers to avail viral load results to HIV-positive clients as soon as they are ready so that they may know whether what they are currently doing to remain on treatment is working.
Motivation-Related Barriers to Successful IAC
We found that the deteriorating health of HIV clients enrolled in IAC and lack of incentives were the two major motivation-related barriers to unsuppressed viral load while enrolled in IAC. HIV-positive clients are typically expected to start improving health-wise once they are started on ART accompanied by good counseling such as those offered during IAC. Therefore, it is conceivable that some may get discouraged and stop taking their drugs altogether once they do not see an immediate improvement in their health hence continued unsuppressed viral load. Meanwhile, the absence of incentives for HIV-positive clients enrolled in IAC may directly lead to a loss of motivation to remain adherence to medication hence unsuppressed viral load. Our findings are identical to the results of studies that found that incentives cap motivate HIV-positive clients to remain adherent to their medications.22,23 Results of our study suggest that healthcare facilities through their non-governmental partners should identify small but meaningful incentives to motivate HIV-positive clients enrolled in IAC to remain focused on taking their drugs to achieve viral load non-suppression.
This study has some limitations. The results of this study may not be generalizable to other contexts which are not identical to that of this study because of its qualitative nature. Additionally, we only elicited views of HIV-positive clients on barriers and facilitators to successful IAC; we do not have views of healthcare providers involved in direct service delivery to these clients to give alternative perspectives on barriers and facilitators to successful IAC. Nevertheless, the findings of our study are highly informative because of the use of the COM-B framework which enabled us to systematically explore the barriers and facilitators to successful IAC.
Conclusion
Successful implementation of IAC has many individual-level barriers and facilitators that need to be contextually explored and considered during service delivery. The results of our study give insight into why implementation of IAC has had conflicting outcomes across settings and what should be considered to improve the implementation of the program. We recommend individualized IAC to give sufficient time to explore individual-level barriers and facilitators during IAC to enhance IAC outcomes.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We acknowledge all those who accepted to participate in this study and the staff at Ogur and Amach Health Center IV. We thank our research assistants, Gabriel Obura and Vicky Atim for the great work done during data collection, transcription, and translation. We also acknowledge the technical support and mentorship offered by Prof. Celestino Obua, Assoc. Prof. Edward Kumakech, Dr. Moses Ochan, and Professor Elialilia S. Okello during the data analysis and drafting of the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Research reported in this publication was supported by the Fogarty International Center (US Department of State’s Office of the US Global AIDS Coordinator and Health Diplomacy [S/GAC] and the President’s Emergency Plan for AIDS Relief [PEPFAR]) of the National Institutes of Health under Award Number R25TW011210. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
The authors declare that they have no competing interests.
References
1. UNAIDS Data. UNAIDS 2020 global report; 2020.
2. Uganda AIDS commission. Fact sheet 2020; 2020. Available from: https://uac.go.ug/sites/default/files/Reports/2019%20Uganda%20Fact%20Sheet_0.pdf.
3. Ministry of Health. Consolidated guidelines for the prevention and treatment of HIV and AIDS in Uganda; 2018.
4. Hugtenburg JG, Timmers L, Elders PJ, Vervloet M, van Dijk L. Definitions, variants, and causes of nonadherence with medication: a challenge for tailored interventions. Patient Prefer Adherence. 2013;7:675. doi:10.2147/PPA.S29549
5. Michie S, Van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6(1):1–12. doi:10.1186/1748-5908-6-42
6. Fox MP, Berhanu R, Steegen K, et al. Intensive adherence counselling for HIV‐infected individuals failing second‐line antiretroviral therapy in Johannesburg, South Africa. Trop Med Int Health. 2016;21(9):1131–1137. doi:10.1111/tmi.12741
7. Pius A, Josephine NN, Erick S, et al. Influence of intensified adherence counselling on viral load suppression of people receiving antiretroviral therapy at a health centre IV in southwestern Uganda: a qualitative study. AIDS Res Ther. 2021;18(1):1–7. doi:10.1186/s12981-021-00372-w
8. Lukyamuzi Z, Etajak S, Katairo T, et al. Effect and implementation experience of intensive adherence counseling in a public HIV care center in Uganda: a mixed-methods study. BMC Infect Dis. 2021;21(1):1–15. doi:10.1186/s12879-021-06862-6
9. Nasuuna E, Kigozi J, Babirye L, Muganzi A, Sewankambo NK, Nakanjako D. Low HIV viral suppression rates following the intensive adherence counseling (IAC) program for children and adolescents with viral failure in public health facilities in Uganda. BMC Public Health. 2018;18(1):1–9. doi:10.1186/s12889-018-5964-x
10. Birungi J, Cui Z, Okoboi S, et al. Lack of effectiveness of adherence counselling in reversing virological failure among patients on long‐term antiretroviral therapy in rural Uganda. HIV Med. 2020;21(1):21–29. doi:10.1111/hiv.12790
11. Bvochora T, Satyanarayana S, Takarinda KC, et al. Enhanced adherence counselling and viral load suppression in HIV seropositive patients with an initial high viral load in Harare, Zimbabwe: operational issues. PLoS One. 2019;14(2):e0211326. doi:10.1371/journal.pone.0211326
12. Ndikabona G, Alege JB, Kirirabwa NS, Kimuli D. Unsuppressed viral load after intensive adherence counselling in rural eastern Uganda; a case of Kamuli district, Uganda. BMC Public Health. 2021;21(1):1–13. doi:10.1186/s12889-021-12366-4
13. Michie S, Atkins L, West R. The behaviour change wheel: a guide to designing interventions. Great Britain: Silverback Publishing; 2014.
14. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
15. Denzin NK, Lincoln YS. The Sage Handbook of Qualitative Research.
16. Moucheraud C, Stern AF, Ahearn C, et al. Barriers to HIV treatment adherence: a qualitative study of discrepancies between perceptions of patients and health providers in Tanzania and Uganda. AIDS Patient Care STDS. 2019;33(9):406–413. doi:10.1089/apc.2019.0053
17. Sileo KM, Kizito W, Wanyenze RK, et al. Substance use and its effect on antiretroviral treatment adherence among male fisherfolk living with HIV/AIDS in Uganda. PLoS One. 2019;14(6):e0216892. doi:10.1371/journal.pone.0216892
18. Becker N, Cordeiro LS, Poudel KC, Sibiya TE, Sayer AG, Sibeko LN. Individual, household, and community level barriers to ART adherence among women in rural Eswatini. PLoS One. 2020;15(4):e0231952. doi:10.1371/journal.pone.0231952
19. Bukenya D, Mayanja BN, Nakamanya S, Muhumuza R, Seeley J. What causes non-adherence among some individuals on long term antiretroviral therapy? Experiences of individuals with poor viral suppression in Uganda. AIDS Res Ther. 2019;16(1):1–9. doi:10.1186/s12981-018-0214-y
20. Ajuna N, Tumusiime B, Amanya J, Awori S, Rukundo GZ, Asiimwe JB. Social networks and barriers to ART adherence among young adults (18–24 years) living with HIV at selected primary health facilities of South-Western Uganda: a Qualitative Study. HIV/AIDS. 2021;13:939.
21. Croome N, Ahluwalia M, Hughes LD, Abas M. Patient-reported barriers and facilitators to antiretroviral adherence in sub-Saharan Africa. AIDS. 2017;31(7):995. doi:10.1097/QAD.0000000000001416
22. Foster C, McDonald S, Frize G, Ayers S, Fidler S. “Payment by Results”—financial incentives and motivational interviewing, adherence interventions in young adults with perinatally acquired HIV-1 infection: a pilot program. AIDS Patient Care STDS. 2014;28(1):28–32. doi:10.1089/apc.2013.0262
23. Haberer JE, Sabin L, Amico KR, et al. Improving antiretroviral therapy adherence in resource‐limited settings at scale: a discussion of interventions and recommendations. J Int AIDS Soc. 2017;20(1):21371. doi:10.7448/IAS.20.1.21371
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Factors Influencing ART Adherence Among Persons Living with HIV Enrolled in Community Client-Led Art Delivery Groups in Lira District, Uganda: A Qualitative Study
Isabirye R, Opii DJ, Opio Ekit S, Kawomera A, Lokiru L, Isoke R, Ssenkaali J, Puleh SS
HIV/AIDS - Research and Palliative Care 2023, 15:339-347
Published Date: 15 June 2023
Barriers and Facilitators to Health-Care Provider Payment Reform – A Scoping Literature Review
Ndayishimiye C, Tambor M, Dubas-Jakóbczyk K
Risk Management and Healthcare Policy 2023, 16:1755-1779
Published Date: 7 September 2023
Barriers and Facilitators to Utilization of Community Drug Distribution Points Among People Living with HIV in Bushenyi District, South-Western Uganda: A Qualitative Study
Oyet D, Niyonzima V, Akol G, Onyait E, Twinomugisha D, Kawala Wambera D, Wakida EK, Obua C
HIV/AIDS - Research and Palliative Care 2023, 15:633-640
Published Date: 16 October 2023
Planning for Hospital Discharge for Older Adults in Uganda: A Qualitative Study Among Healthcare Providers Using the COM-B Framework
Owokuhaisa J, Schwartz JI, Wiens MO, Musinguzi P, Rukundo GZ
Journal of Multidisciplinary Healthcare 2023, 16:3235-3248
Published Date: 2 November 2023
Older Adult Perspectives on Statin Continuation and Discontinuation in Primary Cardiovascular Disease Prevention: A Mixed-Methods Study
Brunner L, Mooser B, Spinewine A, Rodondi N, Aubert CE
Patient Preference and Adherence 2024, 18:15-27
Published Date: 3 January 2024