Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
A Prospective Observational Study Evaluating the PRogression Of BronchiEctasis in COPD Patients - Results from the PROBE - COPD Study
Authors Venkitakrishnan R ![]() , Sudheendranath A, Vijay A, Ramachandran D, Cleetus M
, Sudheendranath A, Vijay A, Ramachandran D, Cleetus M ![]() , Somson HT, John S
, Somson HT, John S
Received 3 October 2025
Accepted for publication 9 March 2026
Published 24 March 2026 Volume 2026:21 571906
DOI https://doi.org/10.2147/COPD.S571906
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Rajesh Venkitakrishnan,1 Athulya Sudheendranath,2 Anand Vijay,1 Divya Ramachandran,1 Melcy Cleetus,1 Hasha Thankam Somson,1 Susan John3
1Department of Pulmonary Medicine, Rajagiri Hospital, Aluva, Kochi, Kerala, India; 2Department of Pulmonary Medicine, Pushpagiri Institute of Medical Sciences and Research Centre, Tiruvalla, Kerala, India; 3Department of Clinical Epidemiology, Rajagiri Hospital, Aluva, Kochi, Kerala, India
Correspondence: Rajesh Venkitakrishnan, Department of Pulmonary Medicine, Rajagiri Hospital, Aluva, Kochi, Kerala, India, Tel +91-9745501976, Email [email protected]
Background: Bronchiectasis is increasingly recognised in individuals suffering from chronic obstructive pulmonary disease (COPD) and is associated with adverse outcomes. However, data on its temporal course and risk factors for progression in advanced COPD remain limited.
Objective: The study aimed to assess the progression of bronchiectasis in stage E COPD patients over one-year, identify factors contributing to its advancement, and compare clinical outcomes between patients diagnosed with bronchiectasis and those without the condition.
Methods: Patients with stage E COPD underwent high-resolution CT (HRCT) and were classified according to whether bronchiectasis present or absent at baseline. All participants were followed for 12 months, with quarterly clinical evaluation, six-monthly sputum culture, spirometry, and repeat HRCT at one-year. Progression of bronchiectasis, decline in lung function, exacerbations, hospitalisations, and mortality were assessed. Predictors of progression were explored using univariate analysis.
Results: Of the 104 patients, 33 (31.7%) had bronchiectasis at baseline. At one-year, 22 of these (66.67%) showed radiological progression and 8 (24.2%) remained stable Among the 71 without bronchiectasis, new bronchiectasis developed in 37 (52.1%). Frequent exacerbations (≥ 2/year) occurred more often in patients with bronchiectasis compared to those without (84.8% vs. 75.8%, P=0.023). Hospitalisation rates were also higher in the bronchiectasis group (60.6% vs. 35.2%, P< 0.001).
Conclusion: Bronchiectasis was present in one-third of stage E COPD patients at baseline, and more than half of those without bronchiectasis developed new lesions during follow-up. COPD patients with bronchiectasis had higher exacerbation frequency, hospitalisations, and greater progression of disease, underscoring its role as a poor prognostic marker in advanced COPD.
Plain Language Summary: Bronchiectasis is common in advanced COPD and often progresses rapidly. In the PROBE-COPD study, patients with bronchiectasis had more exacerbations, hospitalizations, and worse outcomes, underscoring its role as a poor prognostic marker. Progression of bronchiectasis over time occurs in severe COPD patients. Presence of bronchiectasis may be looked upon as a prognostic phenotype.
Keywords: COPD, bronchiectasis, exacerbations
Introduction
Bronchiectasis is a long-standing airway disorder marked by permanent dilation of the bronchi resulting from chronic inflammation and infection, and it commonly occurs alongside chronic obstructive pulmonary disease (COPD). Radiologic bronchiectasis is detected in a substantial proportion of COPD patients, about half of those with moderate-to-severe COPD in some studies.1 The coexistence of bronchiectasis in COPD (sometimes termed “COPD–bronchiectasis overlap”) carries significant clinical implications. Individuals with this overlap typically exhibit more severe disease characteristics, including greater sputum production and a higher frequency of acute exacerbations and hospitalisations.2 They also suffer worse long-term outcomes; it has been noted that the presence of bronchiectasis in COPD has been associated with a ~2.5-fold increase in all-cause mortality risk.3 These observations underscore bronchiectasis as a marker of a high-risk COPD phenotype with poorer prognosis.
COPD is increasingly recognised as a heterogeneous disease, characterised by substantial variability in symptoms, prognosis, and response to therapy among patients.4 This recognition has led to intensified efforts to define clinically relevant phenotypes that could support more tailored treatment approaches.5,6 Among the proposed strategies, thoracic CT imaging has gained attention for its ability to identify structural lung abnormalities associated with distinct disease patterns.7 Features such as emphysematous changes, airway wall thickening,8 and bronchiectasis9 are considered important radiological markers with potential relevance in phenotyping COPD.7,10 Within this framework, bronchiectasis may serve not only as a comorbidity but also as a defining phenotype of COPD with prognostic relevance.
Despite its importance, the natural course of bronchiectasis in COPD remains incompletely understood. It is unclear whether bronchiectasis changes in COPD are static or progressively worsen over time. Recent longitudinal evidence suggests that bronchiectasis can indeed evolve. In one long-term study of COPD patients, roughly one-third showed either enlargement of existing lesions or development of new bronchiectasis over several years.11 In addition, the study identified multiple determinants of bronchiectasis progression, notably ongoing purulent sputum production, a high burden of severe exacerbations leading to hospitalisation, and recurrent sputum isolation of pathogenic microorganisms.11 Such findings imply that ongoing airway infection and inflammation in COPD may drive the worsening of bronchiectasis. However, data on the short-term progression of bronchiectasis, particularly in the highest-risk COPD subgroups, are scarce.
The 2023 GOLD guidelines introduced a new “Stage E” category for COPD, denoting patients with frequent or severe exacerbations (consolidating the former GOLD C and D groups).12 These Stage E patients represent a specially vulnerable cohort in whom bronchiectasis might be expected to progress. We hypothesised that given the structural damage and higher inflammatory burden, Stage E COPD patients with bronchiectasis might be more symptomatic, might have more frequent exacerbations and worse clinical outcomes than those without bronchiectasis. Further, given the frequent infective exacerbations in Stage E COPD patients, bronchiectasis might be expected to progress in them over time. The present PROBE–COPD study (PRogression Of BronchiEctasis in COPD) was designed to prospectively observe Stage E COPD patients over one-year to characterise the course of bronchiectasis and identify factors predictive of its progression. Preliminary findings indicate that even within one-year, a subset of patients exhibit radiographic bronchiectasis progression or new-onset bronchiectasis, reaffirming that structural airway damage can worsen over short time frames. Moreover, Stage E patients with bronchiectasis experienced poorer clinical outcomes during follow-up, compared to Stage E patients those without bronchiectasis.2
Accordingly, the objectives of the PROBE–COPD study were to evaluate the one-year evolution of bronchiectasis in stage E COPD, determine risk factors for progression, and assess differences in clinical outcomes between Stage E patients with versus without bronchiectasis.
Objectives
The primary objective was to identify the course (progression, stability or new occurrence) of bronchiectasis in stage E COPD patients at one-year follow-up.
Secondary objectives were to assess the difference in clinical outcomes (exacerbation rate, hospitalisation rate, pneumonia, mortality etc) in stage E COPD patients with bronchiectasis and those without bronchiectasis during the same follow-up period, to identify the proportion of patients with stage E COPD having bronchiectasis, to spell out the prevalence and microbial aetiology of lower respiratory tract colonisation with potentially pathogenic microorganisms in COPD patients with bronchiectasis and compare the results with patients not having bronchiectasis.
Materials And Methods
Study Design and Settings
This study was a single-centre, longitudinal, prospective, observational cohort study conducted in the Department of Pulmonary Medicine, Rajagiri Hospital, Chunangamveli, Aluva, a tertiary care institution in Central Kerala, India. Both outpatients and inpatients were enrolled.
Study Duration
The study was conducted between March 2022 to September 2023. Recruitment was carried out over six months (March 2022 to September 2022), with each patient followed up for 12 months from the last date of enrolment.
Sample Size
Based on the study by Arram et.al,13 (“Bronchiectasis in COPD patients”), the percentage of bronchiectasis in patients with severe COPD was 62.2%. Applying 15% relative precision and a 95% confidence interval (CI) the minimum required sample size was calculated as 104.
Where:
P = Prevalence bronchiectasis in COPD = 62.2%
1-P = 37.8%
Relative precision = 15% of P = 9.33
1-a/2: Desired Confidence level = 1.96 at 95% CI
Sampling Strategy
Consecutive sampling was employed. All patients ≥ 18 years of age presenting to the department (inpatients or outpatient) with newly or previously diagnosed stage E COPD and who had undergone HRCT thorax were screened. Enrolment continued until the required sample size was reached, based on inclusion and exclusion criteria.
Inclusion Criteria
- COPD was diagnosed based on the criteria outlined in the 2023 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines
- HRCT-confirmed bronchiectasis (for the COPD with bronchiectasis subgroup)
- Willingness to complete one-year follow-up at the study centre
Patients with COPD and bronchiectasis were required to satisfy all three criteria. Patients without bronchiectasis had to meet inclusion criteria 1 and 3 but not criterion 2.
Exclusion Criteria
- Pre-existing bronchiectasis of a known aetiology other than COPD.
- History of pulmonary mycobacterial disease.
- Isolated asymptomatic bronchiectasis restricted to a single pulmonary segment.
- Pre-existing lung disease other than COPD.
- Immunodeficiency states or active malignancy.
Patients meeting even a single exclusion criterion were not enrolled.
Recruitment and Follow-Up
Ethical clearance was obtained from the Institutional Ethics Committee before the commencement of the study. Eligible patients presenting during the recruitment period were enrolled after screening. Demographic and clinical data were collected using a structured proforma with a unique study ID. Records were maintained in a password-protected system. All patient identifiers were removed prior to data entry. Patients were followed up for 12 months. The BRICS Score was used to measure radiological bronchiectasis severity and bronchiectasis severity index (BSI) for clinical as well as radiological severity. Clinical outcomes (exacerbations, hospitalisations, pneumonia, mortality) and microbiological data were recorded. Figure 1 depicts the patient flow through recruitment and follow-up.
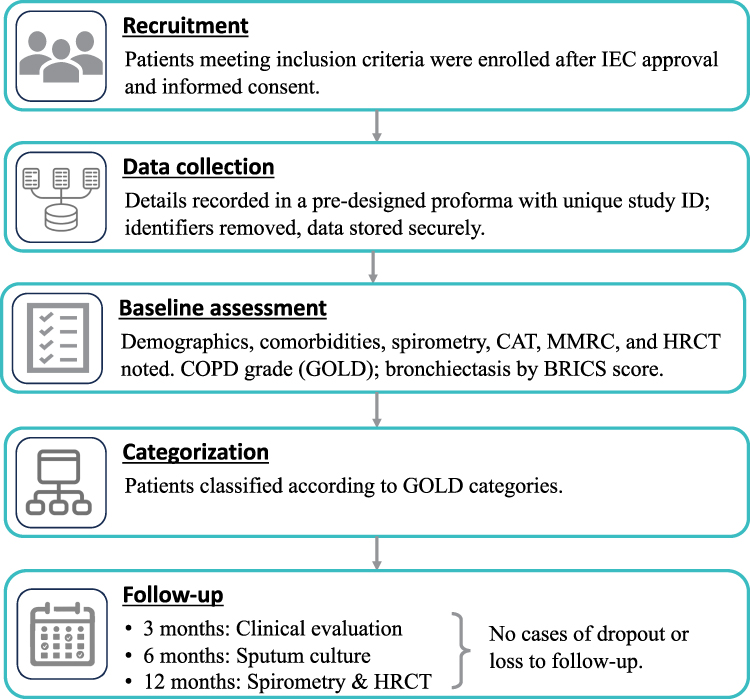 |
Figure 1 Study flow diagram. |
Statistical Analysis
Data analysis was conducted using SPSS software (version 26; IBM Corp., Armonk, NY, USA). Descriptive statistics were presented as frequencies and percentages for categorical variables, while continuous data were summarised using mean and standard deviation. Group-wise comparisons were performed with the chi-square test for categorical parameters and the independent samples t-test for continuous measures. Univariate analysis was carried out to explore associations between baseline variables and outcomes. Time-to-event variables, including exacerbation-free survival, were evaluated using Kaplan–Meier curves and compared with Log rank testing. Cox proportional hazards regression analysis was employed to calculate hazard ratios along with corresponding 95% confidence intervals for factors associated with clinical outcomes. Statistical significance was defined as a two-sided P value of less than 0.05.
Ethical Considerations
The Institutional Ethics Committee approved the study protocol (letter no RAJH/2022/040). As no additional investigations or treatment interventions were undertaken beyond routine clinical care, the committee waived the requirement for an additional written informed consent. All data were anonymised, and the study involved no additional risk or financial burden for participants. The study complies with the Declaration of Helsinki with regards to the ethical standards.
Results
A total of 104 patients with category E COPD were evaluated in this study, of whom 33 (31.73%) had bronchiectasis on baseline CT chest, while 71 showed no evidence of bronchiectasis. Figure 1 summarises the recruitment of study subjects.
Baseline Characteristics
The mean age of participants was 71.58 ± 8.099 years (range 44–92 years). The majority (76.92%, 80 out of 104) of participants fell within the 61–80 years age group. Of the 104 study subjects, 93 were male (89.42%) and 11 were female. At least one comorbidity was present in 90 patients, whereas 14 patients (13.4%) did not have any comorbid conditions. Out of the 33 with bronchiectasis, 28 patients (84.84%) had at least one medical comorbidity compared to 87.32% (62 out of 71) in subjects without bronchiectasis. Current or former smoking status was reported in 89 of the 104 patients (85.57%). The non-smokers included patients with COPD due to biomass exposure (COPD-P), patients with COPD due to infections (COPD-I) etc. Occasional or regular alcohol intake was noted in 61 patients (58.65%).
All the baseline characters have been summarised in Table 1. A higher proportion of patients in the bronchiectasis group had taken prior pneumococcal and influenza vaccinations. Dyslipidaemia as a comorbidity was more frequently encountered in the non-bronchiectasis COPD patients. The percentage of patients with FEV1 <50%, CAT score >10 and frequent exacerbations ≥2 annually) were significantly higher in the bronchiectasis group.
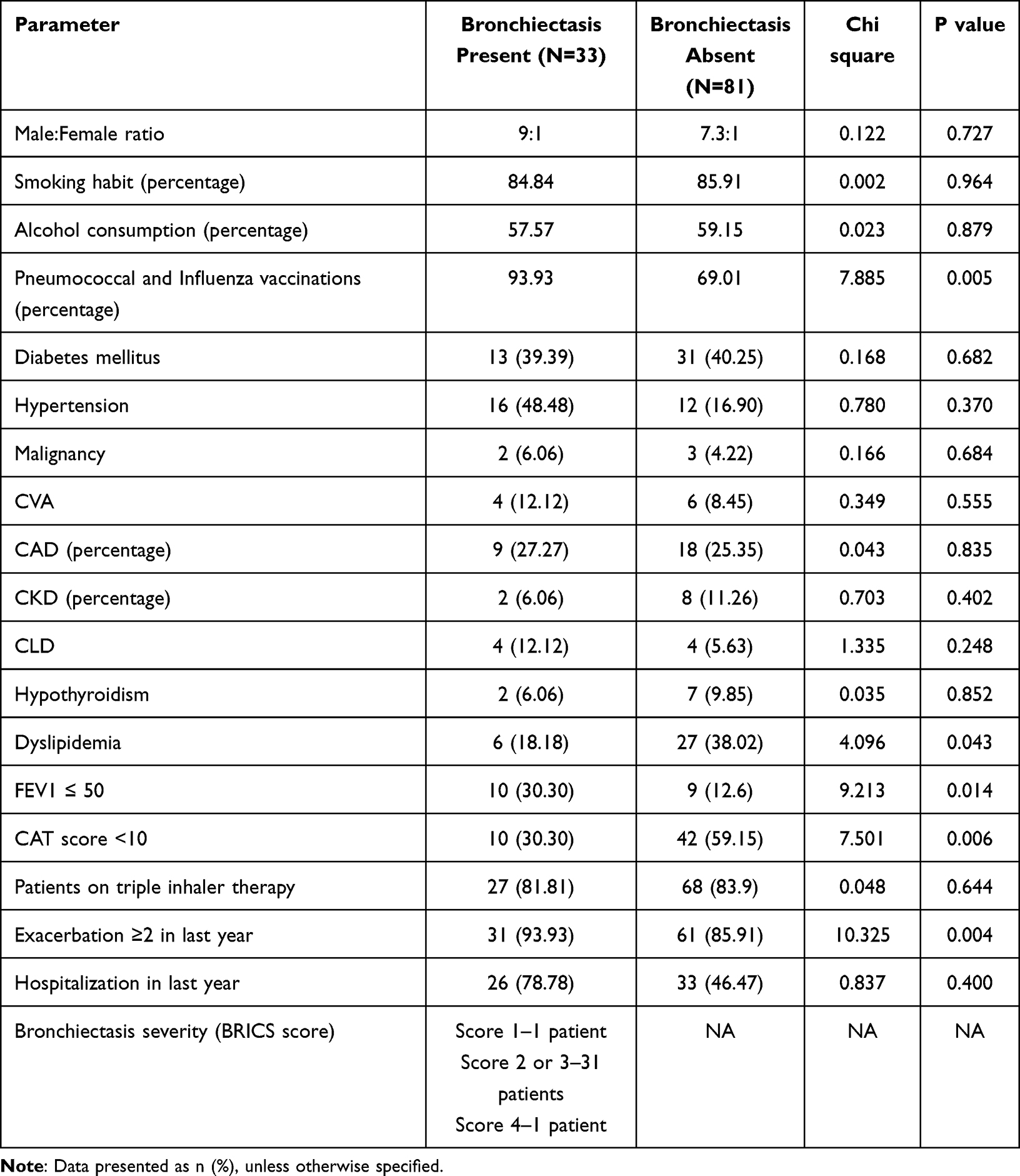 |
Table 1 Baseline Characteristics of COPD Patients with and without Bronchiectasis |
Baseline Extent and Severity of Bronchiectasis
Among the 33 patients who had bronchiectasis in the initial CT, 18 patients (54.55%) had unilateral bronchiectasis and 15 had bilateral bronchiectasis. In 11 patients (33.3%), a single lobe was affected. Twelve patients (36.3%) had involvement of two lobes and eight patients (24.2%) had involvement of three lobes. Four and five lobes were affected in one patient each. A BRICS score of one was observed in one patient (3.03%). Thirty-one patients (93.94%) had a score of 2–3. A score of four was noted in one patient (3.03%).
Follow-Up Data
Over the one-year follow-up period, out of the 33 patients who had bronchiectasis in the initial HRCT, 28 patients (84.84%) had ≥2 exacerbations. In those without bronchiectasis, 55 patients (75.75%) had ≥2 exacerbations in the one-year study period. The observed difference between the two groups reached statistical significance (χ2 = 6.890; P=0.023).
The median time to first exacerbation was significantly shorter in patients with bronchiectasis (2.0 months, 95% CI: 1.42, 2.58) compared to those without bronchiectasis (5.0 months, 95% CI: 4.39, 5.61; P<0.001). This indicates that bronchiectasis patients experienced their first exacerbation much earlier during follow-up. The Cox proportional hazards model demonstrated a significantly greater hazard of first exacerbation over 12 months in patients with bronchiectasis (HR = 4.72, 95% CI: 2.87, 7.74, P<0.001), exceeding four times that observed in patients without bronchiectasis (Figure 2). In those patients with bronchiectasis, 20 patients (60.6%) had at least two hospital admissions during the one-year follow-up and in those without bronchiectasis, only 25 patients (35.2%) had two or more hospital admissions. This result is statistically significant with a p-value of 0.001 and a chi-square value of 10.374.18 patients (54.54%) had ICU admissions, whereas of the patients without bronchiectasis, 24 patients (33.80%) had ICU admissions. This is a statistically significant result with a chi-square value of 5.700 and a p-value of 0.017. Respiratory failure was observed in 14 patients (42.42%) with bronchiectasis and 24 patients (33.80%) without bronchiectasis, which is not statistically significant. Broad-spectrum or reserve antibiotics (Carbapenem, piperacillin-tazobactam, polymyxin, ceftazidime or aztreonam) were used in 30 patients (90.90%) with bronchiectasis and 63 patients (88.73%) without bronchiectasis, which is not statistically significant. Gram-negative bacilli were isolated in 11 patients (33.33%) with bronchiectasis and 15 patients (21.12%) without bronchiectasis, which is also not statistically significant. There were 4 and 7 isolates of Pseudomonas in each group respectively. Other organisms included H.influenza in 2 cases without bronchiectasis and 4 cases with bronchiectasis. Outcome variations according to bronchiectasis status are presented in Figure 3.
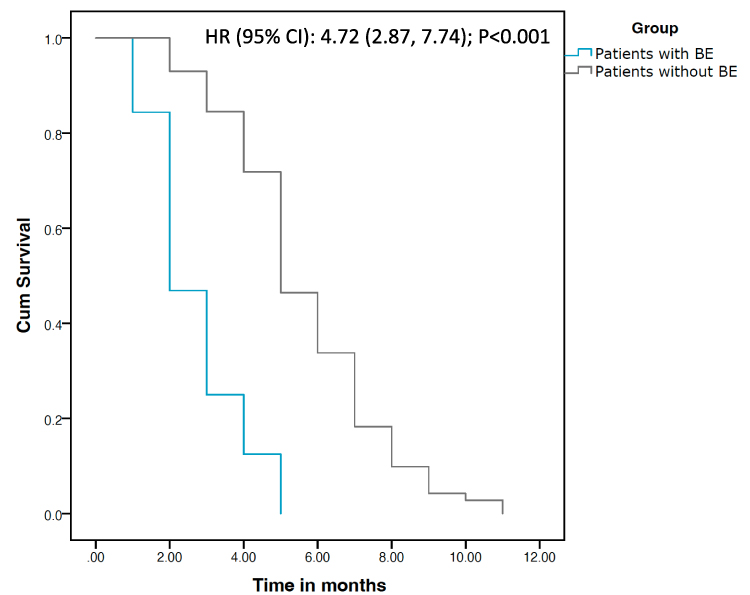 |
Figure 2 Kaplan–Meier curves showing exacerbation-free survival over 12 months in patients with bronchiectasis and without bronchiectasis. Abbreviations: BE, bronchiectasis; HR, hazard ratio. |
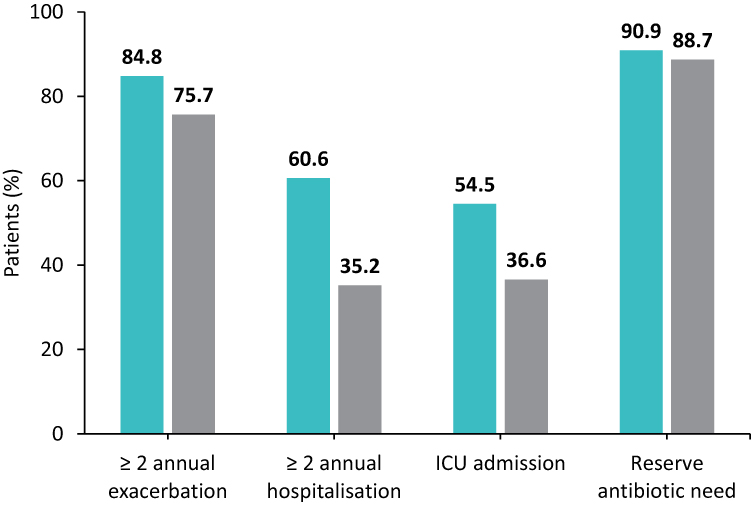 |
Figure 3 Differences in clinical outcomes in patients with and without bronchiectasis over one year follow up. Green bars indicate patients with bronchiectasis and greay bars represent those without bronchiectasis. Abbreviation: ICU, intensive care unit. |
Course of Bronchiectasis
Among the 104 study subjects, 100 patients completed a one-year follow-up period. Three patients in the bronchiectasis group and one in the group without bronchiectasis expired during the follow-up period. In the 33 patients who had bronchiectasis in the initial HRCT thorax, the follow-up CT at one year showed stable lesions in eight patients (24.24%). The lesion showed an increase in extent in 22 patients (66.67%). This included both an increase in the extent of the pre-existing lobes (six patients - 18.18%) as well as extension to an uninvolved lobe (16 patients - 48.48%). In the 71 patients without bronchiectasis in the initial CT, new bronchiectasis developed in 37 patients (52.11%), whereas no bronchiectasis was noted in the one-year follow-up CT in 33 patients (46.47%). Figure 4 summarises the temporal course of bronchiectasis in COPD patients as observed after the one-year follow-up.
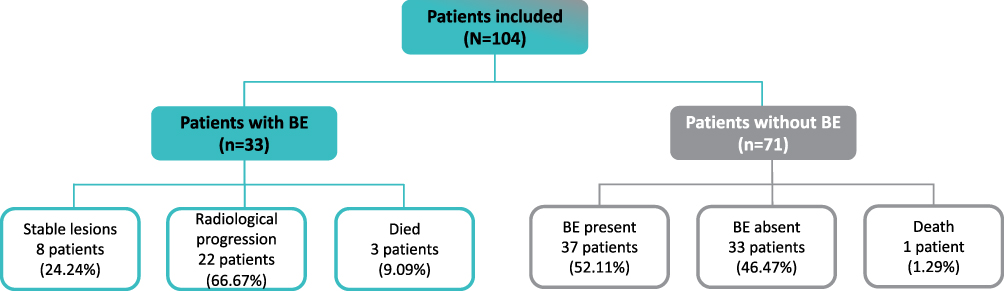 |
Figure 4 Temporal course of bronchiectasis in COPD patients after the one-year follow-up period. |
Patients with higher grades of dyspnoea (MMRC ≥2) had approximately 3.3 times higher odds of progression compared to those with MMRC <2, suggesting that greater baseline symptom burden was associated with a higher likelihood of progression in this dataset. Similarly, isolation of potentially pathogenic microorganisms (PPM) from sputum or bronchioloalveolar lavage and exacerbation rate were also risk factors for progression of bronchiectasis. (Table 2).
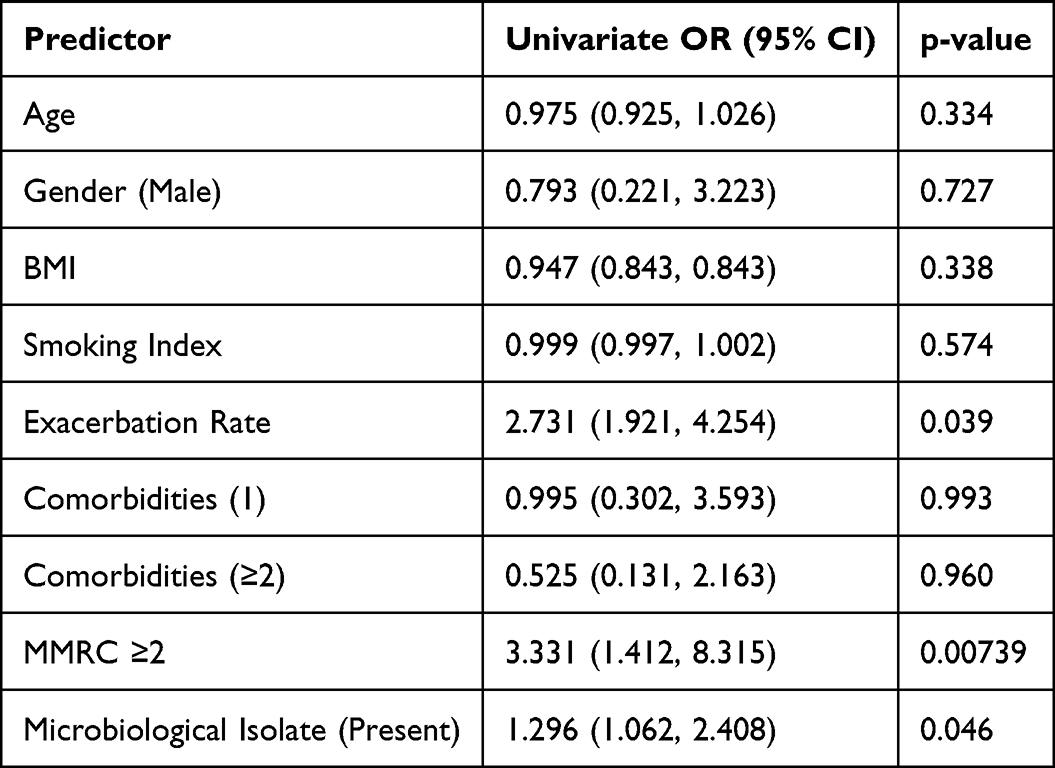 |
Table 2 Risk Factors Associated with Progression of Bronchiectasis |
Discussion
In this prospective observational study, we evaluated 104 patients with stage E COPD and found that 33 individuals (31.73%) had evidence of bronchiectasis at baseline. Reported rates of bronchiectasis among COPD populations vary widely across studies, ranging from as low as 4% to as high as 72%, depending on geography, disease severity, and study methodology. For example, Martínez-García and colleagues observed the occurrence of bronchiectasis in 53.3% of moderate-to-severe COPD patients at baseline.11 Similarly, In a study involving 69 patients with COPD, Arram et al observed a bronchiectasis prevalence of 47.8%, with a clear gradient across severity - 31.3% in moderate COPD compared with 62.2% in severe disease.13 In other cohorts, including a UK study involving patients with acute exacerbations, prevalence rates of up to 69% have been reported, with the majority of cases classified as minor or mild in severity (minor 40%, mild 29%, moderate 22%, and severe 8%).13–15 Patel et al also reported bronchiectasis prevalence in half of a moderate-to-severe COPD cohort.16 Such variability underscores the influence of patient selection, regional differences, and disease severity on prevalence estimates. In our series, the prevalence of 31.7% lies toward the lower end of this reported spectrum.
The coexistence of bronchiectasis in COPD is commonly associated with a more severe clinical presentation. They tend to be older, heavy smokers, have lower body mass index, and are more likely to be chronic mucus secretors and to carry a higher burden of comorbidities.14,16,17 These patients also experienced greater symptom load, more severe airflow obstruction,17 and worse exercise tolerance. The most consistent feature across studies is a higher frequency and severity of exacerbations, a relationship first highlighted by Patel et al and subsequently confirmed in multiple cohorts.13,14,16–18 Nonetheless, not all data are concordant. Jairam et al found that CT-based features such as emphysema and airway thickening were stronger independent predictors of adverse outcomes, while severe bronchiectasis was not independently linked to hospitalisation or death.19 Similarly, a Brazilian study reported that HRCT findings of bronchiectasis did not correlate with worse obstruction, in contrast to emphysema, which showed stronger associations.18 This study has the demerit that CT scans were obtained for reasons other than the intention to detect bronchiectasis. In similar lines, a Brazilian study suggested that airway findings in COPD patients by HRCT do not correlate with worse airway obstruction,18 but emphysema does.
In the landmark study by Martínez-García et al11 reported that over follow-up, bronchiectasis remained absent in 27.3% of patients, remained stable in 36.4%, progressed in 16.9%, and newly developed in nearly 20%. Our findings align with the reports that bronchiectasis in COPD is dynamic and progressive. Among the 33 patients with baseline bronchiectasis, follow-up CT after one year demonstrated stable disease in only 24.2%, whereas 66.7% showed worsening, either through increased involvement within the same lobes or extension to new lobes. Of the 71 patients without initial bronchiectasis, over half (52.1%) developed new lesions during follow-up, further supporting the concept of structural airway deterioration over time. Collectively, these results highlight that bronchiectasis represents a clinically meaningful phenotype of COPD with a tendency to progress, especially in high-risk patients such as those classified as Stage E.
Limitations of the Study
This study has certain limitations; however, careful measures were taken to minimise their potential impact on the results and conclusions.
- The number of patients recruited into the study has been small, considering the fact that this is a single-centre study that spanned a limited time frame. However, we have been able to meet the required minimum sample size.
- A substantial proportion of the study subjects belonged to the male gender which might question the extrapolation of these results to female COPD patients. However, it may be noted that most Indian studies on COPD have a male preponderance and hence the study results may be generalizable to Indian COPD population.
- Post-tuberculosis bronchiectasis is common in India. Since we have excluded post-tuberculosis patients to avoid patients with any known aetiology of bronchiectasis, it may limit the extension of the results to post tuberculosis COPD patients. However, the proportion of this patients is small compared to the overall global COPD burden.
- The temporal evolution of bronchiectasis in COPD patients beyond the one-year follow-up period has not been studied. Prospective studies spanning for longer period is advocated to study this aspect.
Conclusions
The occurrence of bronchiectasis in stage E COPD patients in our study was 31.73%. COPD patients with bronchiectasis had more severe airflow limitation, more frequent exacerbations, more frequent hospitalisations and higher symptom burden. At baseline, among the patients with bronchiectasis, 54.55% had unilateral bronchiectasis and 45.45% had bilateral bronchiectasis. In 11 patients (33.33%), a single lobe was affected, and in 12 patients (36.36%), two lobes were affected. During the one-year follow-up period, frequency of exacerbations, need for ICU care and need for reserve antimicrobials were higher in COPD patients with bronchiectasis. One-year follow-up of CT scan showed stable Bronchiectasis lesions in 24.24% and an increase in extent in 66.67%. In patients without bronchiectasis in the initial CT, new bronchiectasis developed in 52.11% patients. These results prove that our hypothesis (stage E COPD patients with bronchiectasis might be more symptomatic, might have more frequent exacerbations and worse clinical outcomes than those without bronchiectasis; bronchiectasis might be expected to progress in Stage E COPD patients over time) is true.
Take Home Messages
Bronchiectasis is common in advanced COPD and is associated with increased exacerbations, hospitalisations, and worse outcomes. Its presence may therefore represent a prognostic marker. Progression of bronchiectasis occurs in patients with severe COPD, supporting the need for active screening in this population for both predictive and therapeutic considerations.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Martínez-García MÁ, Soler-Cataluña JJ, Donat Sanz Y, et al. Factors associated with bronchiectasis in patients with COPD. Chest. 2011;140(5):1130–11. doi:10.1378/chest.10-1758
2. Kawamatawong T, Onnipa J, Suwatanapongched T. Relationship between the presence of bronchiectasis and acute exacerbation in Thai COPD patients. Int J Chron Obstruct Pulmon Dis. 2018;13:761–769. doi:10.2147/COPD.S139776
3. Martínez-García MA, de la Rosa Carrillo D, Soler-Cataluña JJ, et al. Prognostic value of bronchiectasis in patients with moderate-to-severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;187(8):823–831. doi:10.1164/rccm.201208-1518OC
4. Decramer M, Janssens W, Miravitlles M. Chronic obstructive pulmonary disease. Lancet. 2012;379(9823):1341–1351. doi:10.1016/S0140-6736(11)60968-9
5. Han MK, Agusti A, Calverley PM, et al. Chronic obstructive pulmonary disease phenotypes: the future of COPD. Am J Respir Crit Care Med. 2010;182(5):598–604. doi:10.1164/rccm.200912-1843CC
6. Miravitlles M, Calle M, Soler-Cataluña JJ. Clinical phenotypes of COPD: identification, definition and implications for guidelines. Arch Bronconeumol Engl Ed. 2012;48(3):86–98. doi:10.1016/j.arbres.2011.10.007
7. Bafadhel M, Umar I, Gupta S, et al. The role of CT scanning in multidimensional phenotyping of COPD. Chest. 2011;140(3):634–642. doi:10.1378/chest.10-3007
8. Mair G, Maclay J, Miller JJ, et al. Airway dimensions in COPD: relationships with clinical variables. Respir Med. 2010;104(11):1683–1690. doi:10.1016/j.rmed.2010.04.021
9. Martínez-Garcia MÁ, Selma-Ferrer MJ, Navarro-Soriano C, Muñoz-Reina A. Bronchiectasis phenotype in COPD patients. Clin Pulm Med. 2015;22(3):123–127. doi:10.1097/CPM.0000000000000089
10. Lynch DA, Austin JH, Hogg JC, et al. CTdefinable subtypes of chronic obstructive pulmonary disease: a statement of the Fleischner Society. Radiology. 2015;277(1):192–205. doi:10.1148/radiol.2015141579
11. Martínez-García MÁ, de la Rosa-Carrillo D, Soler-Cataluña JJ, et al. Bronchial infection and temporal evolution of bronchiectasis in patients with chronic obstructive pulmonary disease. Clin Infect Dis. 2021;72(3):403–410. doi:10.1093/cid/ciaa069
12. Case MA, Boorman EP, Ruvalcaba E, et al. Guideline alignment and medication concordance in COPD. CHEST Pulm. 2024;2(1):100017. doi:10.1016/j.chpulm.2023.100017
13. Arram EO, Elrakhawy MM. Bronchiectasis in COPD patients. Egypt J Chest Dis Tuberc. 2012;61(4):307–312. doi:10.1016/j.ejcdt.2012.07.001
14. Gatheral T, Kumar N, Sansom B, et al. COPD-related bronchiectasis; independent impact on disease course and outcomes. COPD J Chronic Obstr Pulm Dis. 2014;11(6):605–614.
15. Chen YH, Sun YC. Bronchiectasis as a comorbidity of chronic obstructive pulmonary disease: implications and future research. Chin Med J. 2016;129(17):2017–2019. doi:10.4103/0366-6999.189071
16. Patel IS, Vlahos I, Wilkinson TM, et al. Bronchiectasis, exacerbations indices, and inflammation in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2004;170(4):400–407. doi:10.1164/rccm.200305-648OC
17. Steward JI, Maselli DJ, Anzueto A, et al. Clinical impact of CT radiological feature of bronchiectasis in the COPDGene cohort. Am J Respir Crit Care Med. 2012;185:A3656.
18. da Silva SM, Paschoal IA, De Capitani EM, et al. COPD phenotypes on computed tomography and its correlation with selected lung function variables in severe patients. Int J Chron Obstruct Pulmon Dis. 2016;11:503–513. doi:10.2147/COPD.S90638
19. Jairam PM, van der Graaf Y, Lammers JW, Mali WP, de Jong PA. PROVIDI Study group. Incidental findings on chest CT imaging are associated with increased COPD exacerbations and mortality. Thorax. 2015;70(8):725–731. doi:10.1136/thoraxjnl-2014-206160
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
FIDEPOC: Consensus on Inspiratory Flow and Lung Deposition as Key Decision Factors in COPD Inhaled Therapy
González-Torralba F, Baloira A, Abad A, Fuster A, García-Rivero JL, García-Sidro P, Márquez-Martín E, Palop M, Soler N, Velasco JL
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1005-1015
Published Date: 4 May 2022
Effect of Recent Exacerbation History on the Efficacy of Once-Daily Single-Inhaler Fluticasone Furoate/Umeclidinium/Vilanterol Triple Therapy in Patients with Chronic Obstructive Pulmonary Disease in the FULFIL Trial
Panettieri Jr RA, Camargo CA Jr, Cheema T, El Bayadi SG, Fiel S, Vila TM, Jain RG, Midwinter D, Thomashow B, Ludwig-Sengpiel A, Lipson DA
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2043-2052
Published Date: 1 September 2022
Efficacy of mRNA and Inactivated Whole Virus Vaccines Against COVID-19 in Patients with Chronic Respiratory Diseases
Kwok WC, Leung SHI, Tam TCC, Ho JCM, Lam DCL, Ip MSM, Ho PL
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:47-56
Published Date: 19 January 2023
Use of Remote Cardiorespiratory Monitoring is Associated with a Reduction in Hospitalizations for Subjects with COPD
Polsky M, Moraveji N, Hendricks A, Teresi RK, Murray R, Maselli DJ
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:219-229
Published Date: 3 March 2023
Exacerbations and Real-World Outcomes After Single-Inhaler Triple Therapy of Budesonide/Glycopyrrolate/Formoterol Fumarate, Among Patients with COPD: Results from the EROS (US) Study
Strange C, Tkacz J, Schinkel J, Lewing B, Agatep B, Swisher S, Patel S, Edwards D, Touchette DR, Portillo E, Feigler N, Pollack M
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2245-2256
Published Date: 12 October 2023