Back to Journals » Journal of Inflammation Research » Volume 18
A Prognostic Nomogram Combining Postoperative SII and PIV Improves Long-Term Survival Prediction in NSCLC
Authors Yu Q ![]() , Zheng L, Iqbal M, Xiang J
, Zheng L, Iqbal M, Xiang J ![]() , Tang J
, Tang J
Received 29 August 2025
Accepted for publication 6 November 2025
Published 22 December 2025 Volume 2025:18 Pages 17911—17926
DOI https://doi.org/10.2147/JIR.S559530
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Felix Marsh-Wakefield
Qian Yu,1,2 Leliang Zheng,3 Majid Iqbal,3 Juanjuan Xiang,2,3 Jingqun Tang1,2
1Department of Thoracic Surgery, The Second Xiangya Hospital, Central South University, Changsha, Hunan, 410013, People’s Republic of China; 2Hunan Key Laboratory of Early Diagnosis and Precise Treatment of Lung Cancer, The Second Xiangya Hospital, Central South University, Changsha, Hunan, 410013, People’s Republic of China; 3NHC Key Laboratory of Carcinogenesis and the Key Laboratory of Carcinogenesis and Cancer Invasion of the Chinese Ministry of Education, Cancer Research Institute, School of Basic Medical Science, Central South University, Changsha, Hunan, People’s Republic of China
Correspondence: Jingqun Tang, Department of Thoracic Surgery, The Second Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China, Email [email protected]
Purpose: Systemic inflammation plays a crucial role in the progression and prognosis of non-small cell lung cancer (NSCLC), yet the prognostic value of perioperative inflammatory markers remains underexplored.
Patients and methods: We retrospectively analyzed 243 patients who underwent resection (2015– 2019) at The Second Xiangya Hospital. Five inflammatory indices—neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic immune-inflammation index (SII), systemic inflammation response index (SIRI), and pan-immune-inflammation value (PIV)—were calculated from pre- and postoperative blood counts, and their changes (Δ values) were derived. Prognostic markers were identified using receiver operating characteristic (ROC) curve analysis, Cox regression, least absolute shrinkage and selection operator (LASSO), and stepwise selection. A nomogram was developed in a training cohort and internally validated using a 70/30 hold-out split from the same center.
Results: Postoperative SII and PIV, along with their perioperative changes (ΔSII and ΔPIV), showed superior prognostic performance compared to preoperative values. The final nomogram (POST_SII, POST_PIV, clinical tumor-node-metastasis stage, smoking history, preoperative albumin, age, and gender) achieved a concordance index (C-index) of 0.85 in the training cohort, with area under the curve (AUCs) of 0.86, 0.89, and 0.94 at 1-, 3-, and 5-year, and a C-index of 0.80 with AUCs of 0.74, 0.85, and 0.90 in the validation cohort. The model surpassed TNM and clinical models and showed greater net clinical benefit in decision-curve analysis.
Conclusion: Postoperative SII and PIV are strong inflammatory predictors of survival after NSCLC resection. A nomogram integrating these markers with clinical variables provides accurate, individualized risk stratification.
Keywords: nomogram, survival prediction, systemic immune-inflammation index, pan-immune-inflammation value, postoperative prognosis
Introduction
Non-small cell lung cancer (NSCLC) is one of the most prevalent malignancies worldwide, accounting for approximately 18.7% of total cancer deaths.1 Surgical resection is the primary curative treatment for NSCLC; however, the postoperative prognosis varies significantly.2 While traditional staging systems, such as TNM staging, provide prognosis estimates, they primarily focus on anatomical tumor characteristics and fail to fully capture the complex biological processes underlying tumor progression, including the patients’ systemic immune-inflammatory status and dynamic perioperative changes.3
Mounting evidence highlights the pivotal role of systemic inflammation in tumor initiation, progression, and metastasis.4,5 Inflammatory markers, including the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR), have been extensively linked to poor prognosis in cancers.6 However, most NSCLC prognostic nomograms have been derived from preoperative/baseline variables (clinicopathologic features and inflammatory measures), with postoperative and perioperative dynamics remaining under-represented.7,8 Surgical stress elicits a systemic inflammatory response, transient immune disequilibrium, and metabolic reprogramming that remodel the tumor microenvironment (TME) and dampen immune surveillance in the early postoperative period. Accordingly, capturing perioperative inflammatory dynamics may yield prognostic signals that are stronger and more clinically actionable than those provided by preoperative indices alone.9
In this study, we conducted retrospective study to comprehensively investigate the association between dynamic perioperative immune-inflammatory indices and survival. By quantifying both preoperative baseline and postoperative changes in inflammatory markers, this model seeks to enhance the precision of long-term survival prediction in NSCLC patients. The successful implementation of such a dynamic prognostic tool could significantly advance personalized medicine by enabling more stratified risk assessment and tailored therapeutic interventions.
Methods
Patients and Participants
This retrospective study included a total of 243 patients with non-small cell lung cancer (NSCLC) who underwent curative-intent surgical resection at The Second Xiangya Hospital of Central South University between January 2015 and December 2019. All patients were pathologically confirmed to have NSCLC and completed comprehensive clinical evaluations both preoperatively and postoperatively.
Inclusion Criteria: ① Patients with histopathologically confirmed NSCLC who received their initial diagnosis and underwent surgical resection at our institution; ② Availability of complete clinical, pathological, and imaging data, including peripheral blood test results within 3–5 days before and after surgery; ③ Availability of complete follow-up information on overall survival (OS).
Exclusion Criteria: ① Death within 30 days after surgery. ② Presence of chronic respiratory diseases (eg, bronchial asthma, chronic obstructive pulmonary disease, interstitial pulmonary fibrosis) or other severe comorbidities deemed by the attending physician to significantly impair surgical tolerance or long-term prognosis; ③ History of malignancies other than NSCLC; ④ Presence of clinically confirmed acute infections (eg, pneumonia, urinary tract infection, skin and soft tissue infections) within one month prior to surgery, or administration of antibiotics due to infection during the same period.
OS and Follow-Up
Overall survival (OS) was defined as the interval from the date of surgery to the date of death from any cause or the last follow-up. Patients who remained alive at the last follow-up were censored at 60 months. The follow-up duration was calculated from the date of surgery to the date of last contact or death.
Clinical Information
Clinical data were obtained from the hospital’s electronic medical record system, outpatient follow-up records, and regular postoperative surveillance. The following variables were collected: gender, age, smoking history, body mass index (BMI), surgery type, clean node number, tumor location, lobe number, histology, clinical tumor-node-metastasis stage (cTNM stage), T stage, lymph node metastasis, and pathological features including pleural invasion, neural invasion, vascular invasion, and programmed death-ligand 1 expression (PD-L1 expression). The PD-L1 status was retrieved from pathology reports and recorded as the tumor proportion score (TPS, %).
Inflammatory Indices and Calculation
Peripheral blood samples collected within 3–5 days before and 3–5 days after surgery were used to assess routine hematological parameters, including neutrophil count (NEU), lymphocyte count (LYM), monocyte count (MON), platelet count (PLT), and serum albumin level (ALB). Based on these values, five systemic inflammation-based composite indices were calculated as follows:
Neutrophil-to-lymphocyte ratio (NLR) = NEU / LYM
Platelet-to-lymphocyte ratio (PLR) = PLT / LYM
Systemic immune-inflammation index (SII) = (PLT × NEU) / LYM
Systemic inflammation response index (SIRI) = (NEU × MON) / LYM
Pan-immune-inflammation value (PIV) = (NEU × PLT × MON) / LYM
Each index was calculated at two timepoints: preoperatively and postoperatively, denoted respectively by the prefixes PRE_ (eg, PRE_SII) and POST_ (eg, POST_PIV). In addition, delta values (Δ) were derived to reflect perioperative changes, defined as the difference between postoperative and preoperative values (eg, ΔSII = POST_SII − PRE_SII). These Δ values were used to assess dynamic alterations in systemic inflammation during the perioperative period and to explore their potential prognostic implications.
Statistical Analysis
Continuous variables were presented as mean ± standard deviation and compared using the Student’s t-test or the Wilcoxon rank-sum test, as appropriate. Categorical variables were summarized as counts and percentages and compared using the chi-squared test. Five inflammation-based composite indices (NLR, PLR, SII, SIRI, and PIV) were derived from preoperative (PRE_) and postoperative (POST_) peripheral blood values, including neutrophils (NEU), lymphocytes (LYM), monocytes (MON), platelets (PLT), and albumin (ALB). Perioperative changes (Δ values) were calculated as POST_ minus PRE_ (eg, ΔSII = POST_SII − PRE_SII). All patients (N = 243) were randomly divided into a training cohort (70%) and a validation cohort (30%). Unless otherwise specified, all modeling procedures were performed in the training cohort.
In the training cohort, conventional receiver operating characteristic (ROC) curves were first used to determine the optimal cutoff values of each inflammation index using the Youden index, which were then applied to stratify patients into high- and low-risk groups for Kaplan–Meier survival analysis. Prognostic performance of individual indices was further evaluated using time-dependent ROC curves (TIMEROC) and Harrell’s concordance index (C-index). Subsequently, univariate Cox regression was performed to identify clinical variables associated with overall survival (OS). Each significant clinical variable (P < 0.05) was then individually included in multivariate Cox regression with each inflammation index to examine the independent prognostic value of each index. The area under the curve (AUC) and C-index were used to compare the discriminative performance of these multivariate models. Based on these analyses, four optimal indices (POST_SII, POST_PIV, ΔSII, and ΔPIV) were selected for model construction. To further explore potential non-linear associations between each inflammation-based index and overall survival, restricted cubic spline (RCS) functions with four knots were fitted in univariable Cox proportional hazards models. Hazard ratios (HRs) and 95% confidence intervals (CIs) were plotted across the range of each continuous variable, and log-likelihood ratio tests were used to assess evidence of non-linearity.
All clinical variables with statistical significance in univariate Cox analysis, along with the selected four inflammation indices, were subjected to least absolute shrinkage and selection operator (LASSO) regression with the λ.1se criterion to reduce collinearity and avoid overfitting. The retained variables were further refined by stepwise multivariate Cox regression to determine the final predictors for model development.10 Age and gender were included in the model based on clinical relevance, regardless of statistical significance. Three hierarchical prognostic models were constructed: the TNM model (cTNM stage only), the Clinical model (cTNM plus clinical predictors), and the Nomogram model (Clinical model plus POST_SII and POST_PIV) (Table 1). Model performance was evaluated using time-dependent AUC and Harrell’s C-index. Calibration plots and Kaplan–Meier curves were used to assess predictive accuracy and survival stratification. Decision curve analysis (DCA) was performed to assess clinical utility at 1, 3, and 5 years. Reclassification performance was further compared across models using net reclassification improvement (NRI) and integrated discrimination improvement (IDI), with the TNM model as the reference. The proportional hazards (PH) assumption for the final multivariable Cox model was assessed using Schoenfeld residuals and log–log survival plots to ensure that the PH assumption was not violated.
 |
Table 1 Model Characteristics |
To address potential bias from a single 70/30 split and assess robustness, we applied two procedures using the final seven-variable Cox model (Smoking History, cTNM stage, Preoperative Albumin, POST_SII, POST_PIV, Age, and Gender): (i) 5-fold cross-validation in the training cohort and (ii) 100 repeated 70/30 random splits of the full cohort. Discrimination was summarized by Harrell’s C-index and time-dependent AUCs at 1, 3, and 5 years; AUCs were estimated with Uno’s method, and time points with insufficient events or at-risk subjects were treated as NA and excluded from averaging. Results are reported as mean ± standard deviation across folds or splits.
All statistical analyses were conducted using R software (version 4.3.2), and a two-sided P value < 0.05 was considered statistically significant. The study design and patient selection process are summarized in Supplementary Figure 1.
Results
Patient Baseline Characteristics
The study included the retrospective analysis of 243 patients with NSCLC who underwent curative-intent surgical resection at the Second Xiangya Hospital of Central South University from January 2015 and December 2019. The characteristics of the patients were displayed in Table 2. The mean age was 58.0 ± 9.9 years, and the cohort included 152 (62.6%) males and 91 (37.4%) females. Prognosis was retrospectively evaluated through an analysis of varied 5-year survival rates. Among these 243 patients, 137 patients were alive at the last follow-up, while 106 patients had passed away (Table 2). Compared with the survival group, the death group showed significantly different distribution in gender (75.5% male vs 24.5% female, P < 0.001), smoking history (54.7% smokers vs 45.3% non-smokers, P < 0.001), and adenocarcinoma histology (62.3% vs 37.7% non-adenocarcinoma, P = 0.007). In the death group, advanced clinical stage (cTNM stage II–III: 66% vs 34%, P < 0.001), higher T stage (P < 0.001), and more frequent lymph node metastasis (P < 0.001) were more often seen, indicating a more advanced disease state.
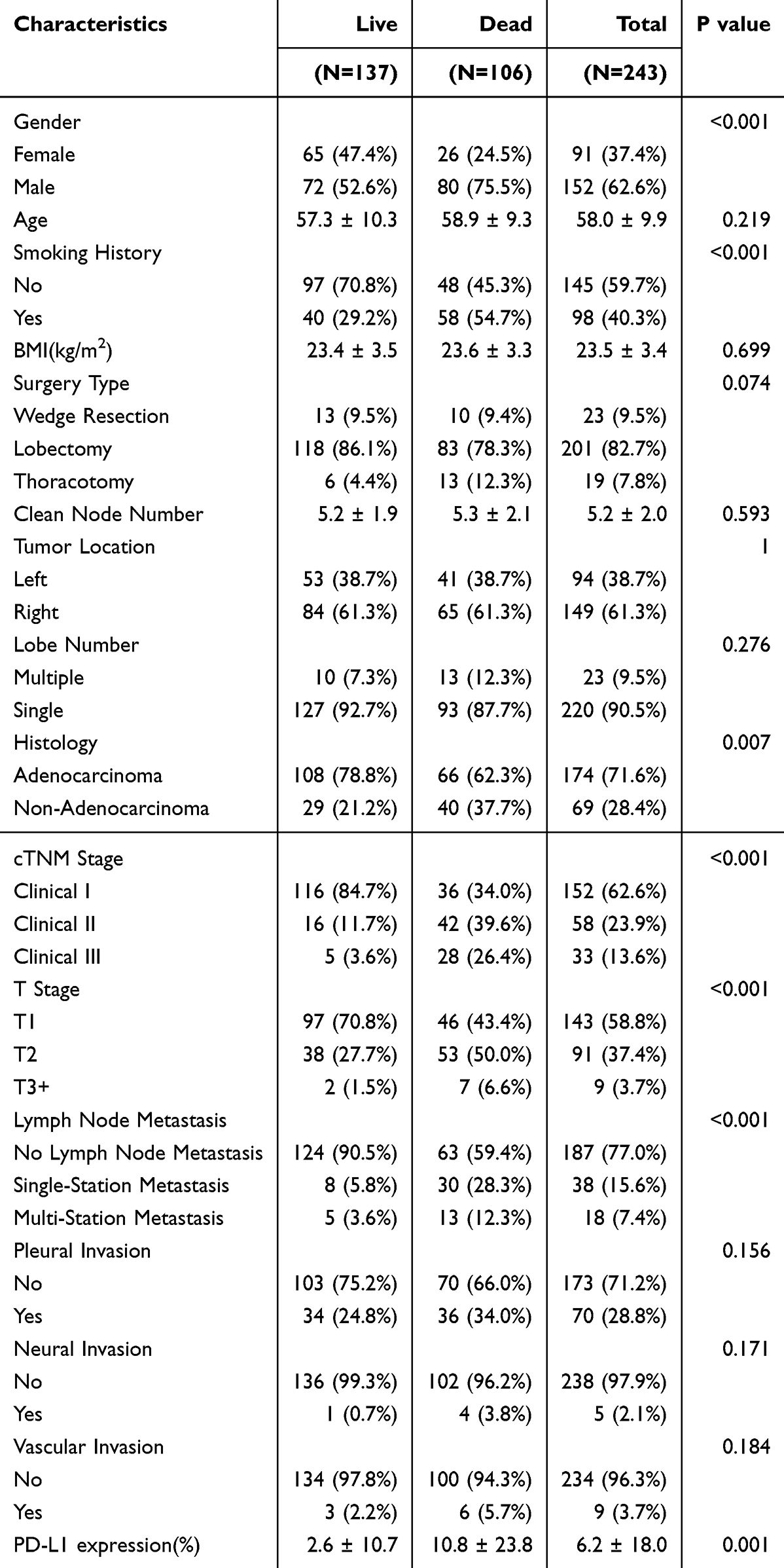 |
Table 2 Clinical Characteristics |
We specifically evaluate the difference in systemic immune-inflammation indices (Table 3). Indicators from peripheral blood demonstrated that the death group had significantly elevated preoperative levels of neutrophil (P = 0.013), platelet (P = 0.016), and monocyte (P = 0.001), along with reduced albumin levels (P = 0.009). The immunohistochemical test showed that the death group had notably increased PD-L1 expression levels (10.8 ± 23.8 vs 2.6 ± 10.7, P = 0.001). This indicates that the baseline inflammation status might negatively influence the postoperative prognosis of lung cancer patients, while immune nutritional status has positive impacts.
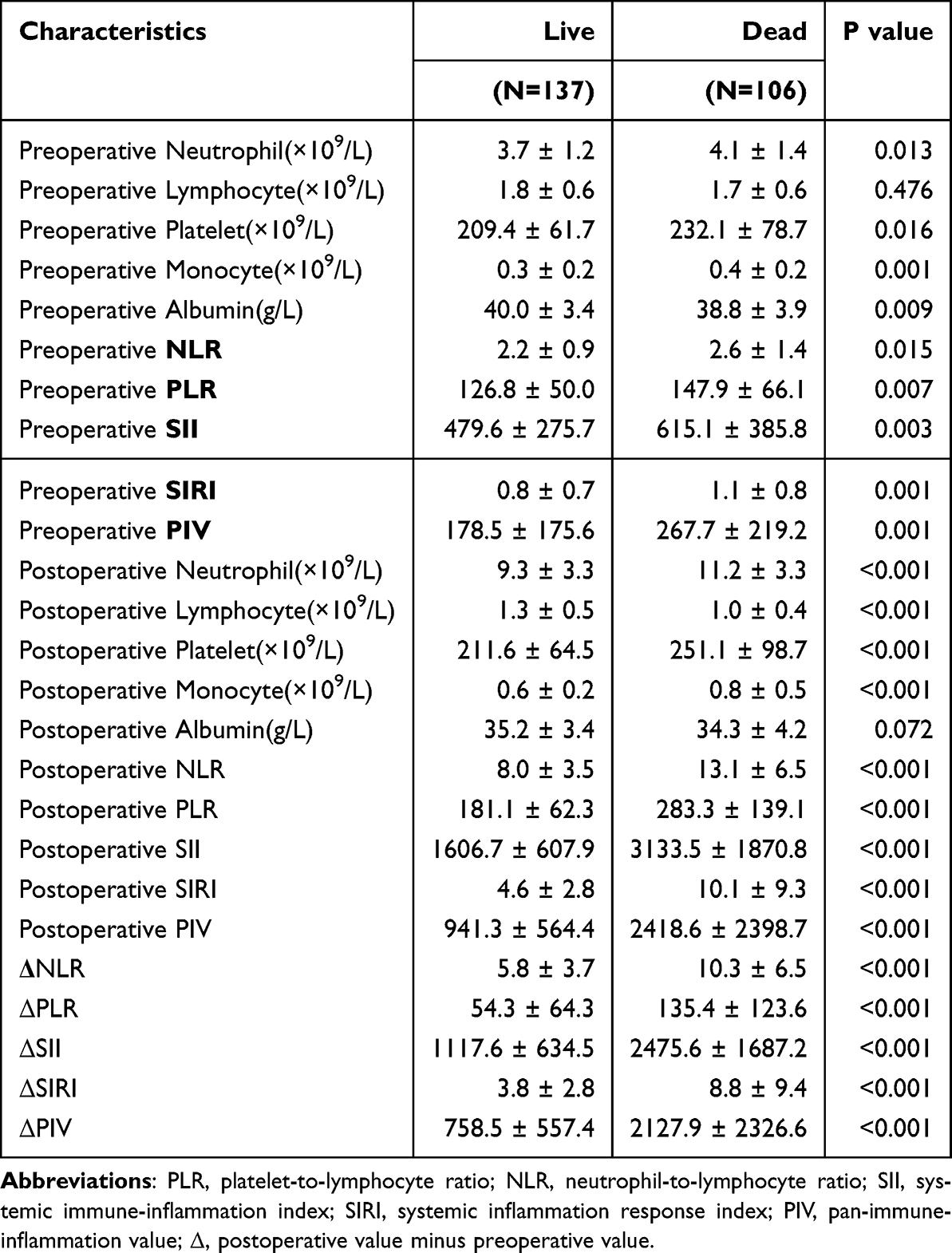 |
Table 3 Inflammation-Related Indices’ Characteristics |
After the operation, systemic inflammation is commonly seen in most patients, which is a usual response to surgical trauma. After the operation, the patients showed increased neutrophils and decreased lymphocytes and albumin. Compared to the survival group, the death group had significantly increased levels of neutrophils (P < 0.001), platelets (P < 0.001), and monocytes (P < 0.001), along with notably reduced levels of lymphocytes (P < 0.001). This indicates that the occurrence of inflammation after operation might negatively influence the postoperative prognosis of lung cancer patients. Several established inflammation indices are recognized as superior prognostic indicators compared to single inflammatory cell counts. Consistent with this, we revealed significantly higher preoperative and postoperative levels of five inflammatory indices, including NLR, PLR, SII, SIRI, and PIV, in the death group than in the survival group (Table 3). Importantly, the postoperative and Δ (change) values of these indices revealed greater differences between the two groups than their preoperative values, underscoring the significance on prognosis of perioperative inflammatory status. These results suggest that heightened inflammatory activity, particularly when sustained postoperatively or rising perioperatively, is closely linked to adverse long-term prognosis.
Inflammation-Based Indices as Predictors of Long-Term Survival
We subsequently examined the prognostic performance of these preoperative, postoperative, and Δ (post-pre) inflammation-related indices using time-dependent ROC curves and the concordance index (C-index). After determining optimal cutoff values via ROC analysis (Youden’s index), we conducted univariate Cox regression for clinical variables and each inflammation marker. Significant clinical variables (P < 0.05) and individual inflammation markers were then included in multivariate Cox models. To reduce overfitting, the cohort (N = 243) was randomly split into a training set (70%, n = 170) and a testing set (30%, n = 73). All model development and cutoff determination were conducted solely in the training set.
As an initial screening step, 15 inflammatory markers were assessed for overall prognostic performance using time-dependent AUCs and Harrell’s C-index. Patients were dichotomized into high and low groups according to ROC-derived cut-off values for each inflammatory index (Supplementary Figure 2). POST_PIV, POST_SII, ΔPIV, and ΔSII consistently demonstrated the highest AUCs and C-index values (Figure 1A), indicating superior discriminative ability for overall survival.
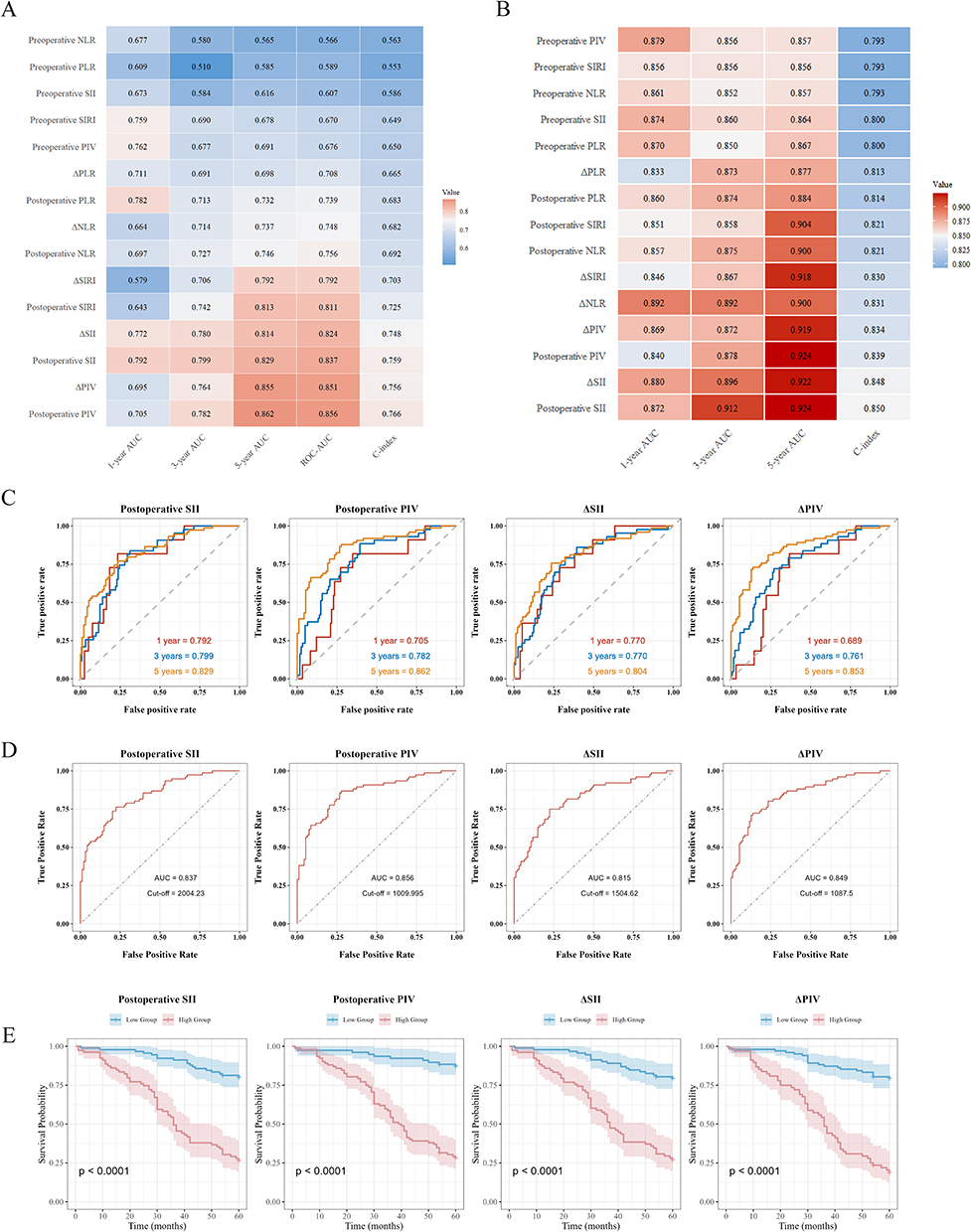 |
Figure 1 Prognostic evaluation of inflammation-based indices. (A) Heatmap showing AUCs and C-index of 15 inflammation markers for overall survival. (B) AUCs and C-index of Cox models incorporating each marker with significant clinical variables. (C) Time-dependent ROC curves of POST_SII, POST_PIV, ΔSII, and ΔPIV at 1-, 3-, and 5-year follow-up. (D) Standard ROC curves and cutoff values for the four selected markers. (E) Kaplan-Meier survival curves for high- and low-risk groups based on each marker’s cutoff (log-rank P < 0.0001). |
To better contextualize these findings, we first performed univariate Cox regression analysis on clinical variables, identifying several factors significantly associated with overall survival, including Gender, Smoking History, cTNM stage, T stage, Histology, Lymph Node Metastasis, PD-L1 expression, and Preoperative Albumin (P < 0.05) (Table 4). These clinical predictors were then incorporated into multivariate models with each inflammation marker. As shown in Figure 1B and detailed in Table 5, POST_PIV (HR = 7.87, P < 0.001), POST_SII (HR = 6.87, P < 0.001), ΔPIV (HR = 5.32, P < 0.001), and ΔSII (HR = 5.98, P < 0.001) remained independent predictors for poor survival in multivariate analysis after adjusting for relevant clinical confounders.
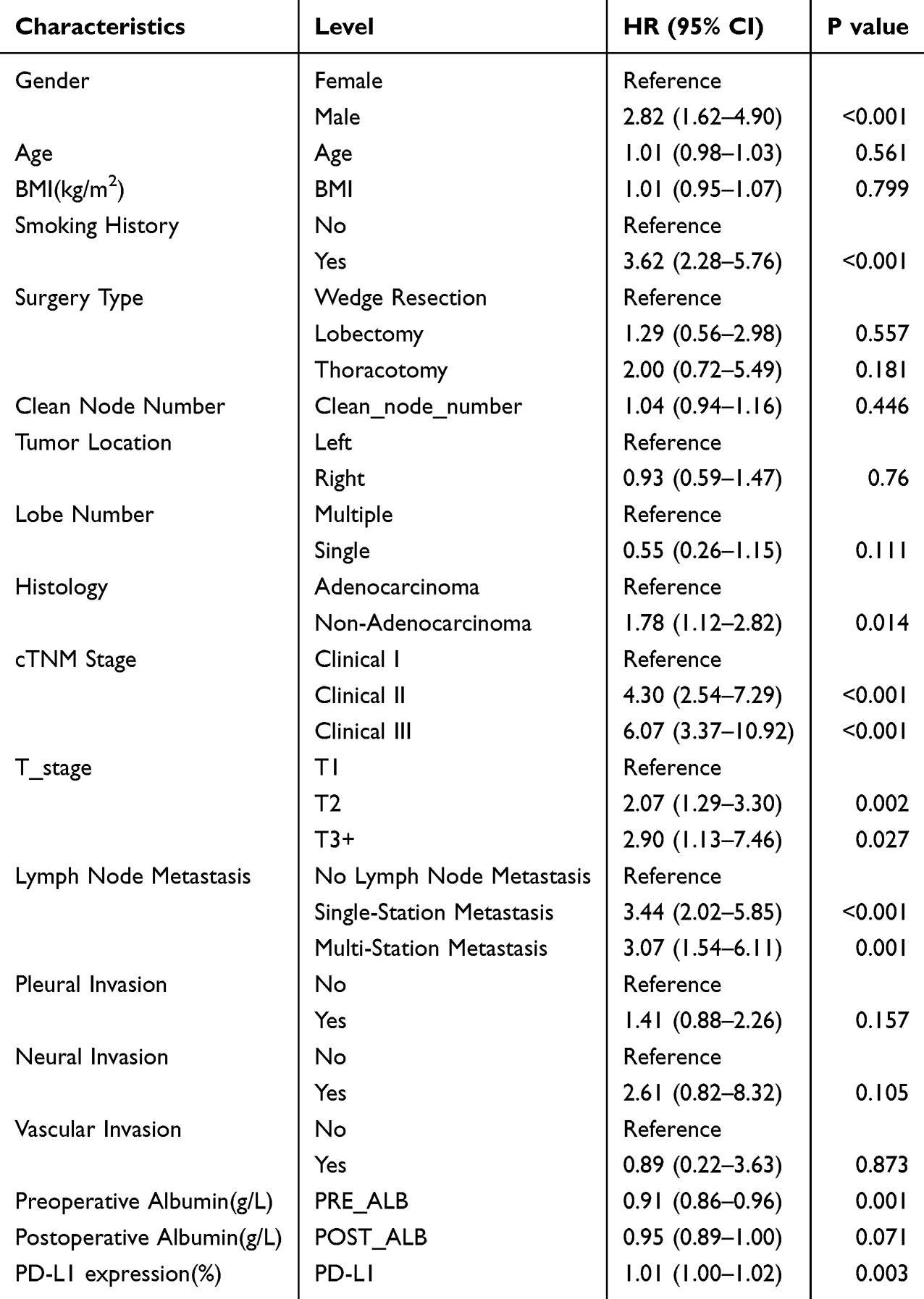 |
Table 4 Univariate Cox Regression for Clinical Characteristics |
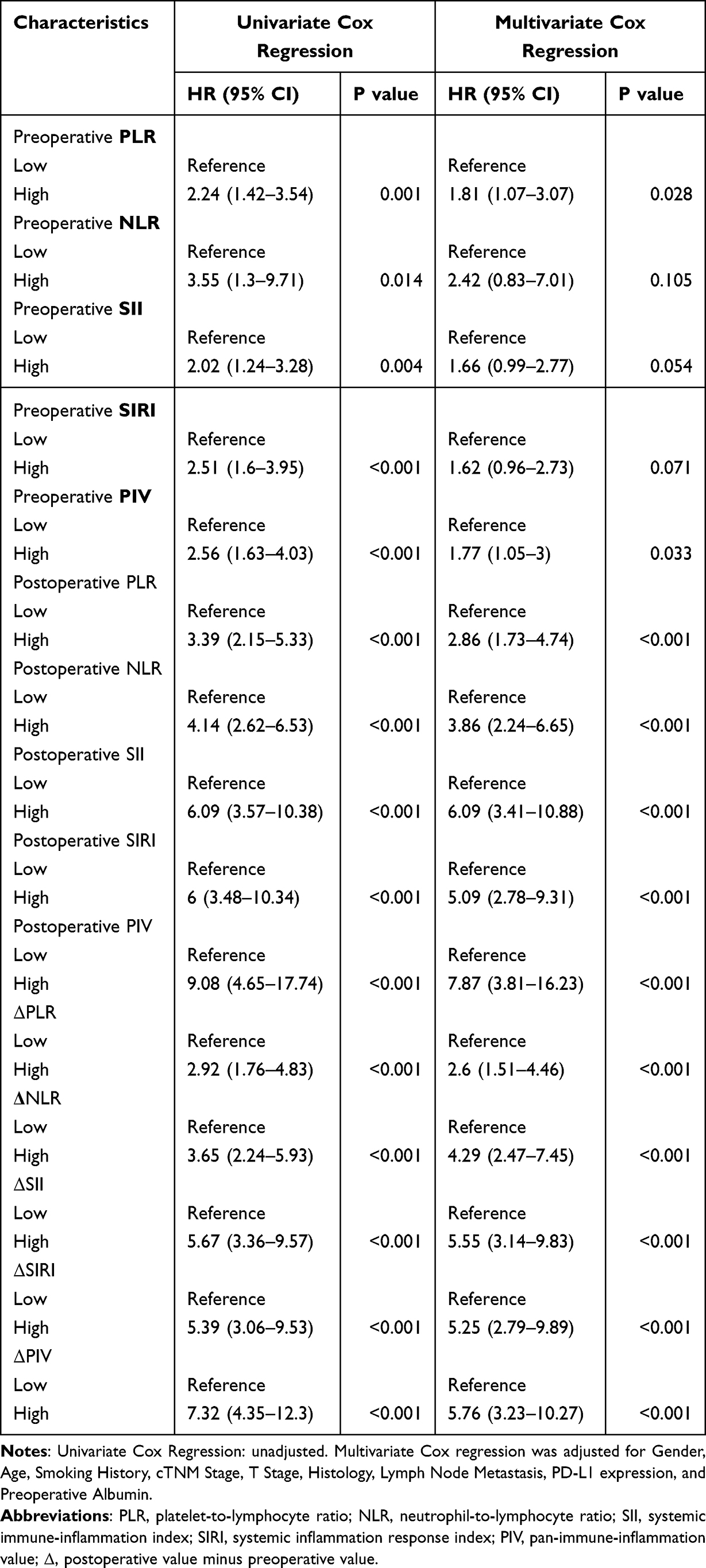 |
Table 5 Inflammatory Index Univariate and Multivariate Cox Regression |
Time-dependent ROC analysis (Figure 1C) further confirmed their temporal predictive stability, with POST_SII yielding AUCs of 0.753, 0.796, and 0.828 at 1-, 3-, and 5-year, respectively. Standard ROC analysis (Figure 1D) further revealed these four indices with high overall discriminative ability. Using their ROC-derived optimal cutoffs derived from the training cohort (2004.23 for POST_SII, 1174.825 for POST_PIV, 1504.62 for ΔSII, and 1116.705 for ΔPIV), Kaplan-Meier curves stratified patients into high/low-risk groups, showing significantly shorter survival in high-risk groups (log-rank P < 0.0001; Figure 1E). Additionally, restricted cubic spline (RCS) analysis in univariable Cox models revealed significant non-linear associations for all inflammation-based indices with overall survival (all P for non-linearity < 0.05). These curves demonstrated that the risk of death did not increase in a strictly linear fashion but exhibited a threshold or plateau effect for certain markers, with sharp risk escalation beyond specific value ranges (Supplementary Figure 3). These findings highlight the prognostic superiority of dynamic and postoperative inflammatory markers, suggesting that systemic inflammation after surgery may more accurately reflect underlying disease aggression and long-term outcomes in NSCLC.
Prognostic Evaluation of Clinical and Inflammatory Variables
The four optimal inflammatory markers (POST_SII, POST_PIV, ΔSII, ΔPIV) and significant clinical variables identified from univariate Cox analysis (P < 0.05) were subjected to LASSO regression. Using the λ min criterion, 11 variables were retained (Figure 2A and B). To further refine the model, we further applied stepwise multivariate Cox regression based on these LASSO-selected variables, yielding a final model with five core predictors: Smoking History (HR = 2.65, 95% CI: 1.61–4.34), cTNM Stage (Stage II: HR = 2.95, 95% CI: 1.68–5.18; Stage III: HR = 2.78, 95% CI: 1.49–5.20), Preoperative Albumin (HR = 0.9, 95% CI: 0.84–0.96), POST_SII (HR = 3.02, 95% CI: 1.59–5.73), and POST_PIV (HR = 3.71, 95% CI: 1.66–8.27). Age and Gender were forcibly retained due to their known clinical relevance and potential impact on stratification in external populations, despite statistical non-significance (Age: HR = 1.018, P = 0.19; Gender [Male]: HR = 0.949, P = 0.894) (Figure 2C). All variables met the proportional hazards assumption (all P > 0.05) (Supplementary Figure 4).
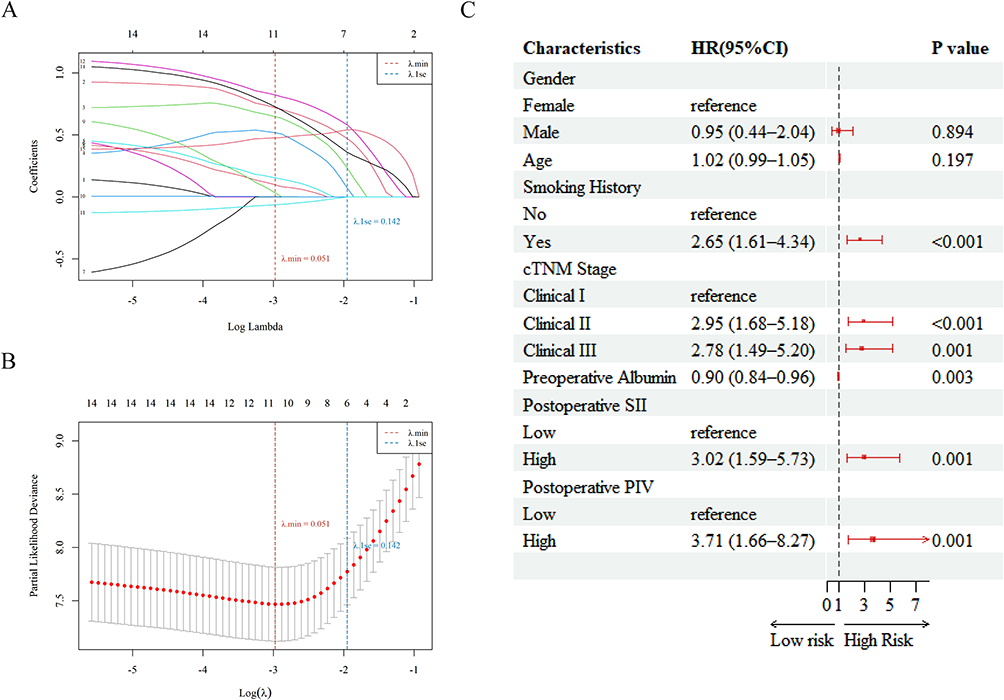 |
Figure 2 Selection and Confirmation of Prognostic Variables Using LASSO and Cox Regression. Feature selection and model refinement for prognostic variable identification. (A) LASSO coefficient profiles of the 12 variables with the penalty parameter (λ) selected via 10-fold cross-validation. (B) Partial likelihood deviance plotted against log (λ); six variables were retained at λ.1se. (C) Forest plot of the final multivariate Cox regression model. Gender and age were forcibly included due to clinical relevance, while five variables were statistically significant: smoking history, cTNM stage, preoperative albumin, postoperative SII, and postoperative PIV. |
A prognostic nomogram integrating these predictors was constructed in the training cohort (N = 170) (Figure 3A). The nomogram demonstrated strong predictive performance, with C-index of 0.85 and AUCs of 0.86, 0.89, and 0.94 at 1-, 3-, and 5-year, respectively (Figure 3B). Calibration curves showed strong agreement between predicted and observed survival probabilities at 1-, 3-, and 5-year (Figure 3D). Validation in the testing cohort (n = 73) maintained robust performance (C-index of 0.80 and AUCs of 0.74, 0.85, and 0.90 at 1-, 3-, and 5-year) (Figure 3C and E). Kaplan–Meier curves based on total nomogram points stratified patients into distinct risk groups with significantly different survival outcomes (Figure 3F and G).
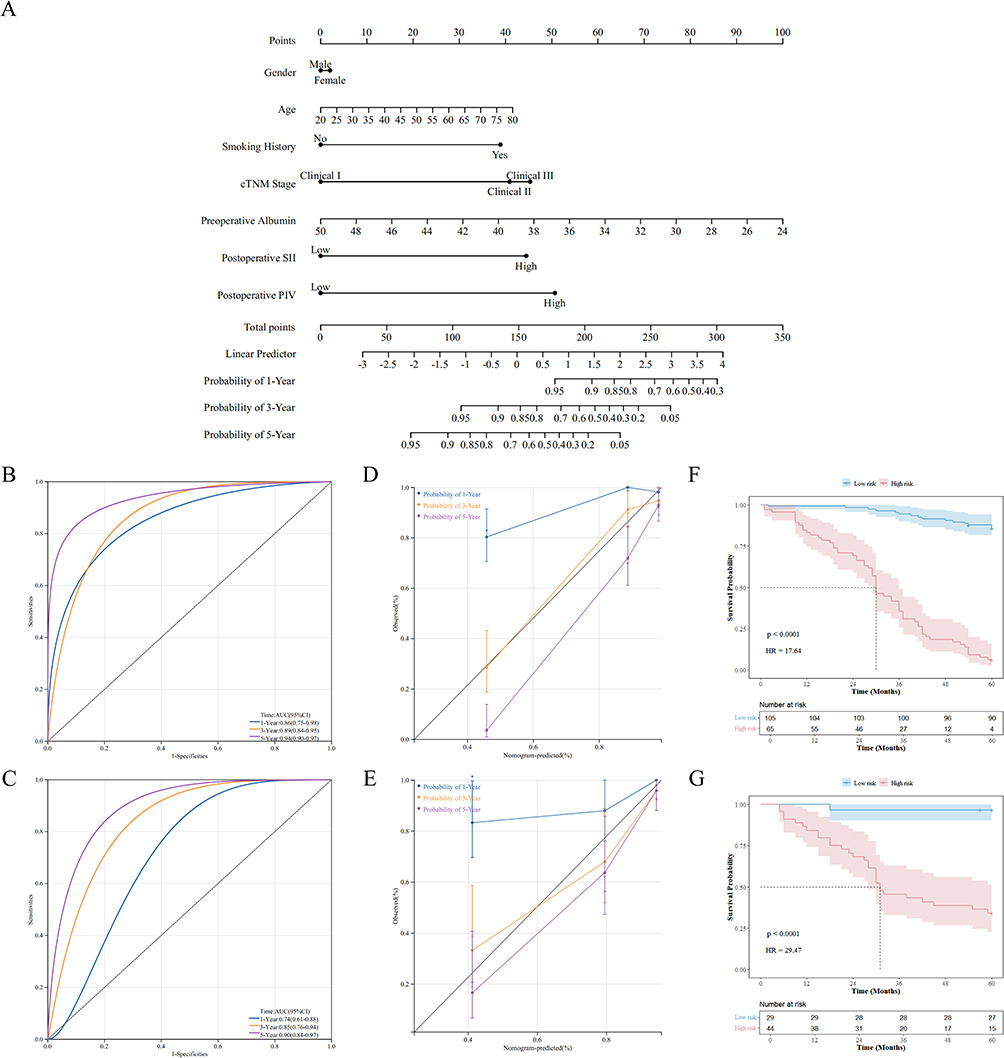 |
Figure 3 Construction and Validation of the Prognostic Nomogram. (A) Nomogram integrating seven variables (Gender, Age, Smoking History, cTNM stage, Preoperative Albumin, Postoperative SII, Postoperative PIV) for 1-, 3-, and 5-year survival prediction in the training cohort. (B and C) Time-dependent ROC curves at 1-, 3-, and 5-year in the training (B) and validation (C) cohorts. (D and E) Calibration plots for 1-, 3-, and 5-year survival prediction in the training (D) and validation (E) cohorts. (F and G) Kaplan–Meier survival curves stratified by total risk score in the training (F) and validation (G) cohorts. |
Decision curve analysis (DCA) demonstrated a significantly superior net clinical benefit of the nomogram versus TNM and clinical variables-only models across threshold ranges of 0.05–0.5 in both the training and validation cohorts. (Figure 4). Although Age and Gender were not statistically significant, their removal led to subtle changes in DCA curves, especially in the validation cohort, indicating potential instability. Their inclusion may thus enhance the nomogram’s robustness and generalizability. (Supplementary Figure 5).
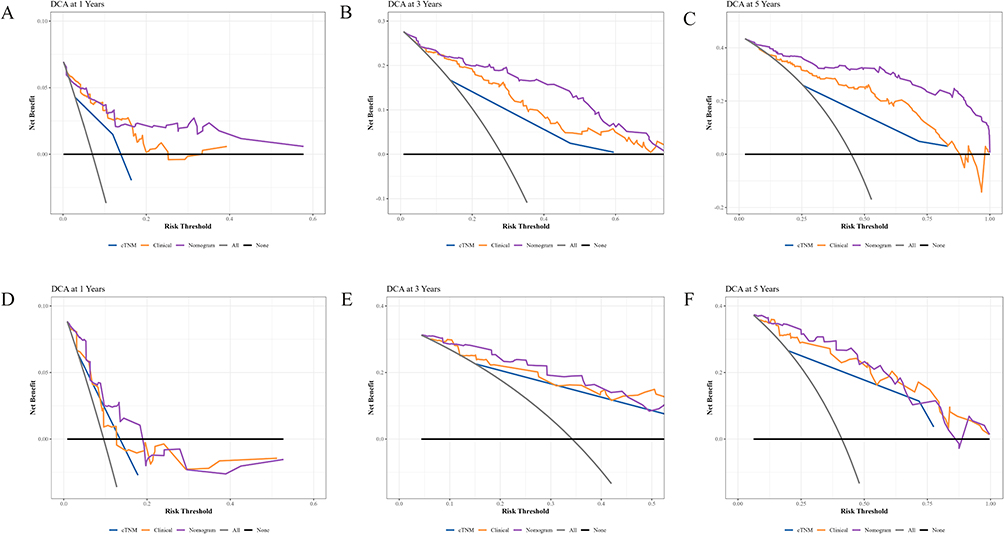 |
Figure 4 Decision Curve Analysis (DCA) for Evaluating Clinical Net Benefit of the Nomogram Model. (A–C) DCA curves for predicting 1-, 3-, and 5-year survival in the training cohort. (D–F) DCA curves for predicting 1-, 3-, and 5-year survival in the validation cohort. The nomogram model consistently showed superior net clinical benefit compared with TNM and clinical-only models across a wide range of threshold probabilities. |
To mitigate potential random selection bias and assess robustness, two complementary internal resampling procedures were conducted. In 5-fold cross-validation of the training cohort, refitting the final seven-variable Cox model in each fold yielded a C-index of 0.85 ± 0.03 and time-dependent AUCs of 0.78 ± 0.29, 0.88 ± 0.04, and 0.93 ± 0.06 at 1, 3, and 5 years, respectively (Supplementary Table 1). Across 100 repeated 70/30 random splits of the full cohort, discrimination remained consistent (mean C-index 0.80 ± 0.03; AUCs 0.76 ± 0.11 / 0.84 ± 0.04 / 0.89 ± 0.04 at 1/3/5 years), aligning with the single hold-out validation (validation C-index 0.80; AUCs 0.74 / 0.85 / 0.90) (Supplementary Table 2).
To further quantify the model’s added predictive value, we compared the nomogram with the TNM and clinical models using Net Reclassification Improvement (NRI) and Integrated Discrimination Improvement (IDI) (Table 6). In the training cohort, the nomogram demonstrated significantly higher NRI and IDI at all time points (all P < 0.01). In the validation set, although improvements were more modest, significant gains in both metrics were still observed at 3- and 5-years. Similar trends were observed in the full cohort analysis. These findings further underscore the superior prognostic capacity of the nomogram over conventional models.
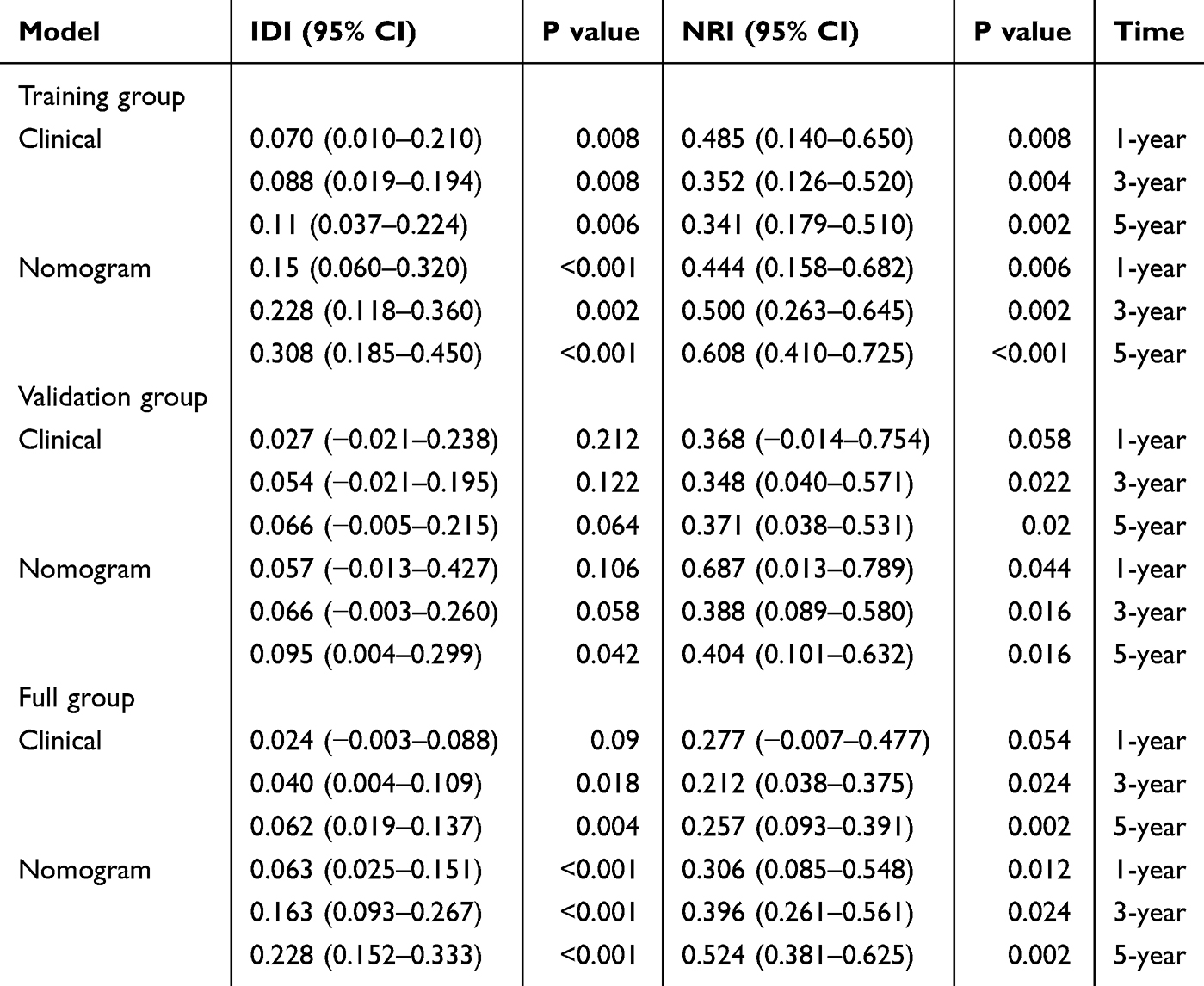 |
Table 6 NRI and IDI of the Nomogram and Clinical Model in Survival Prediction Compared with TNM Stage |
Discussion
Inflammation and immune dysregulation have long been recognized as critical drivers of cancer initiation, progression, and metastasis.11,12 While tumor-associated inflammation exhibits paradoxical tumor-suppressive and -promoting effects, baseline inflammatory indices provide valuable insight into pre-existing immune status.13 Our study demonstrated that perioperative inflammatory dynamics, particularly POST_SII, POST_PIV, ΔSII and ΔPIV, provide superior prognostic stratification compared to preoperative baselines in postoperative NSCLC patients. These dynamic indicators outperformed preoperative baselines in predicting long-term survival with enhanced discrimination, improved classification capacity and consistent robustness.
In NSCLC, prognostic significance of systemic inflammation-based biomarkers, such as the NLR, PLR, SII, and PIV, have been elucidated.14–17 The high levels of postoperative systemic inflammation is a usual response to surgical stress, determined by the magnitude of injury.18 The association between baseline inflammatory indicators with cancer prognosis has highlighted the important role of patients’ intrinsic immune reserve in determining clinical outcomes. Baseline inflammation indicators refer to inflammation-related biomarkers assessed before disease onset, prior to therapeutic intervention, or in a healthy state. The elevations of ΔSII and ΔPIV signifies failed immunological resolution, aligning with clinical observations where persistent postoperative inflammation and associated complications lead to a poor recovery, persistent disability or death.19
Surgical trauma provokes a coordinated systemic inflammatory response and a transient period of immune disequilibrium that can remodel the tumor microenvironment and attenuate antitumor surveillance in the early postoperative window. Mounting evidence suggests that surgical stress activates the neuroendocrine–immune axis, leading to catecholamine and glucocorticoid release that suppress cytotoxic T- and NK-cell activity while expanding myeloid-derived suppressor cells (MDSCs) and regulatory T cells.20,21 Concurrently, neutrophil extracellular traps (NETs) and platelet activation promote circulating tumor cell adhesion and metastatic niche formation, whereas elevated IL-6, IL-8, and TNF-α drive persistent STAT3 and PI3K/AKT/mTOR signaling that facilitates epithelial–mesenchymal transition (EMT) and immune evasion.22,23 Oxidative stress and metabolic reprogramming further amplify this immunosuppressive milieu by impairing lymphocyte proliferation and effector function.23 Collectively, these cascades create a transient but biologically permissive environment in which residual tumor cells can survive, resist immune clearance, and disseminate. Neutrophil predominance, lymphocyte suppression, and platelet or monocyte activation, together with perioperative metabolic reprogramming and cytokine fluxes, provide a mechanistic basis for why postoperative composites such as POST_SII and POST_PIV, and their perioperative deltas, outperform static baselines.24 These dynamics more faithfully reflect the shifting host–tumor balance immediately after resection, when micrometastatic progression and early recurrence risk may be determined.
While prior research has applied postoperative inflammation-based models in gastric and colorectal cancers,25,26 our work adds to the growing body of evidence supporting the prognostic value of postoperative inflammatory markers in NSCLC. Furthermore, restricted cubic spline (RCS) analyses revealed nonlinear associations between individual inflammatory indices and survival risk, though the overall risk trend remained consistent, reinforcing the robustness of our final multivariable model. Beyond assessing single markers, we developed a comprehensive nomogram that integrates immune–inflammatory responses, nutritional and physiologic status, and tumor burden.27 By incorporating dynamic postoperative metrics that capture real-time host–tumor interactions, the nomogram advances risk stratification beyond static baselines. Clinically, it supports risk-adapted postoperative care: high-risk patients should undergo intensified surveillance with early MDT review and targeted perioperative optimization (nutrition rehabilitation and/or inflammation control), whereas low-risk patients can maintain standard follow-up intervals. Internal robustness was further supported by five-fold cross-validation in the training cohort and 100 repeated 70/30 random splits in the full cohort, which yielded concordant performance (Supplementary Tables 1–2). This multidimensional approach addresses limitations of existing models that neglect the impact of surgical injury.
Nonetheless, this study has certain limitations. It is based on a single-center retrospective cohort with a moderate sample size, which may introduce selection bias and limit generalizability. Center-specific perioperative pathways and laboratory platforms may also influence inflammatory indices and outcomes, contributing to spectrum and selection bias. Accordingly, we will undertake multicenter prospective validation and update the model as needed. Although postoperative inflammatory indices remained independently associated with survival after adjustment for available clinical covariates, other perioperative factors—such as anesthesia/analgesia strategies and postoperative complications—were not consistently standardized in the records and may contribute to residual confounding. We therefore consider these results hypothesis-generating and suitable for prospective confirmation. In addition, perioperative blood draws were performed within a 3–5-day window before and after surgery, which could introduce timing variability in the measured indices. Future protocols will fix sampling days to reduce temporal variability and evaluate short-term kinetics of SII/PIV. Internal robustness was supported by 5-fold cross-validation and 100 repeated 70/30 splits, but this does not substitute for external (including temporal) validation and formal calibration. Finally, inflammation-based indices are surrogate markers of immune status and do not directly delineate the molecular pathways linking inflammation to tumor progression and recurrence. Future studies will integrate tissue and circulating biomarkers with prospectively collected perioperative data to elucidate mechanisms and refine the model across histologic subtypes and treatment contexts.
Conclusion
POST_SII and POST_PIV were identified as the most robust inflammatory predictors of overall survival in resected NSCLC. A prognostic nomogram integrating postoperative inflammatory markers (POST_SII and POST_PIV) with clinical variables (smoking history, cTNM stage, preoperative albumin, age, and gender) demonstrated superior predictive performance compared with TNM and clinical models in resected NSCLC. This model provides a practical tool for individualized postoperative risk stratification and warrants external validation.
Data Sharing Statement
The raw clinical datasets used and/or analyzed during the current study are publicly available in the OMIX database under accession number OMIX011524. All code used for data processing and statistical analysis is accessible via GitHub at: https://github.com/Yuki3885/inflammatory-Rdata.
Ethics Approval and Informed Consent
The study was approved by the Ethics Committee of The Second Xiangya Hospital of Central South University (approval No. Z0933-01). Written informed consent was obtained from all participants prior to enrollment. The research was conducted in accordance with the Declaration of Helsinki.
Author Contributions
Qian Yu contributed to conceptualization and methodology, performed data curation, formal analysis, and investigation, prepared visualization, drafted the original paper (writing – original draft), and contributed to writing – review and editing. Leliang Zheng assisted with data curation and formal analysis, contributed to investigation and visualization, and participated in writing – review and editing. Majid Iqbal contributed to validation and writing – review and editing. Juanjuan Xiang assisted with validation and project administration, and contributed to writing – review and editing. Jingqun Tang provided supervision, funding acquisition, and resources, and critically revised the paper (writing – review and editing), and served as guarantor of the work.
All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Clinical Key Specialty Major Scientific Research Project (Z2023003); Key Research and Development Program of Hunan (2019SK2253), National Natural Science Foundation of Changsha (kq2208299, kq2403084), the National Natural Science Foundation of Hunan (2025JJ50173).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Yano T, Okamoto T, Fukuyama S, Maehara Y. Therapeutic strategy for postoperative recurrence in patients with non-small cell lung cancer. World J Clin Oncol. 2014;5(5):1048–1054. doi:10.5306/wjco.v5.i5.1048
3. Guo L, Li J, Wang J, et al. Prognostic role of dynamic changes in inflammatory indicators in patients with non-small cell lung cancer treated with immune checkpoint inhibitors-a retrospective cohort study. Transl Lung Cancer Res. 2024;13(8):1975–1987. doi:10.21037/tlcr-24-637
4. Nøst TH, Alcala K, Urbarova I, et al. Systemic inflammation markers and cancer incidence in the UK biobank. Eur J Epidemiol. 2021;36(8):841–848. doi:10.1007/s10654-021-00752-6
5. Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):e493–503. doi:10.1016/S1470-2045(14)70263-3
6. Lei Y, Cao C, Tang R, Liu Y. Peripheral blood inflammatory biomarkers neutrophil/ lymphocyte ratio, platelet/lymphocyte ratio and systemic immune-inflammation index/albumin ratio predict prognosis and efficacy in non-small cell lung cancer patients receiving immunotherapy and opioids. BMC Cancer. 2025;25(1):664. doi:10.1186/s12885-025-14060-9
7. Tamburini N, Aramini B, Potenza I, et al. Prognostic significance of preoperative neutrophil-to-lymphocyte ratio in lung carcinoid patients after receiving curative surgery. A multicentre study. Front Oncol. 2025;15:1585433. doi:10.3389/fonc.2025.1585433
8. Akcam TI, Tekneci AK, Turhan K, et al. Prognostic value of systemic inflammation markers in early stage non-small cell lung cancer. Sci Rep. 2025;15(1):33886. doi:10.1038/s41598-025-08683-y
9. Chen Z, Zhang P, Xu Y, et al. Surgical stress and cancer progression: the twisted tango. Mol Cancer. 2019;18(1):132. doi:10.1186/s12943-019-1058-3
10. Wang S, Zhao M, Gao Z, et al. A survival nomogram involving nutritional-inflammatory indicators for cervical cancer patients receiving adjuvant radiotherapy. J Cancer. 2024;15(17):5773–5785. doi:10.7150/jca.100564
11. Coussens LM, Werb Z. Inflammation and cancer. Nature. 2002;420(6917):860–867. doi:10.1038/nature01322
12. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–674. doi:10.1016/j.cell.2011.02.013
13. Shalapour S, Karin M. Pas de deux: control of anti-tumor immunity by cancer-associated inflammation. Immunity. 2019;51(1):15–26. doi:10.1016/j.immuni.2019.06.021
14. Guo W, Cai S, Zhang F, et al. Systemic immune-inflammation index (SII) is useful to predict survival outcomes in patients with surgically resected non-small cell lung cancer. Thorac Cancer. 2019;10(4):761–768. doi:10.1111/1759-7714.12995
15. Lei W, Wang W, Qin S, Yao W. Predictive value of inflammation and nutritional index in immunotherapy for stage IV non-small cell lung cancer and model construction. Sci Rep. 2024;14(1):17511. doi:10.1038/s41598-024-66813-4
16. Liu W, Zhang T, Li L, Zou J, Xu C. Assessing the prognostic value of the neutrophil-to-lymphocyte ratio in stage I non-small-cell lung cancer with complete resection. Can Respir J. 2022;2022:6837872. doi:10.1155/2022/6837872
17. Zhai WY, Duan FF, Lin YB, et al. Pan-immune-inflammatory value in patients with non-small-cell lung cancer undergoing neoadjuvant immunochemotherapy. J Inflamm Res. 2023;16:3329–3339. doi:10.2147/JIR.S418276
18. Furák J, Németh T, Lantos J, et al. Perioperative systemic inflammation in lung cancer surgery. Front Surg. 2022;9:883322. doi:10.3389/fsurg.2022.883322
19. Bain CR, Myles PS, Martin C, et al. Postoperative systemic inflammation after major abdominal surgery: patient-centred outcomes. Anaesthesia. 2023;78(11):1365–1375. doi:10.1111/anae.16104
20. Wang Z, Zhao Y, Zhang L. Emerging trends and hot topics in the application of multi-omics in drug discovery: a bibliometric and visualized study. Curr Pharm Anal. 2024;21(1):20–32. doi:10.1016/j.cpan.2024.12.001
21. Keshavarzmotamed A, Mousavi V, Masihipour N, et al. Regulating miRNAs expression by resveratrol: novel insights based on molecular mechanism and strategies for cancer therapy. Curr Mol Pharmacol. 2024;17(1):1–21. doi:10.2174/0118761429249717230920113227
22. Liu Y, Zhang S, Liu K, Hu X, Gu X. Advances in drug discovery based on network pharmacology and omics technology. Curr Pharm Anal. 2024;21(1):33–43. doi:10.1016/j.cpan.2024.12.002
23. Singh J, Luqman S, Meena A. Carvacrol as a prospective regulator of cancer targets/signalling pathways. Curr Mol Pharmacol. 2023;16(5):542–558. doi:10.2174/1874467215666220705142954
24. Li G, Wan Y, Jiao A, et al. Breaking boundaries: chronic diseases and the frontiers of immune microenvironments. Med Res. 2025;1(1):62–102. doi:10.1002/mdr2.70007
25. Sun J, Yang R, Wu H, Li L, Gu Y. Prognostic value of preoperative combined with postoperative systemic immune-inflammation index for disease-free survival after radical rectal cancer surgery: a retrospective cohort study. Transl Cancer Res. 2024;13(1):371–380. doi:10.21037/tcr-23-1289
26. Lin JX, Wang ZK, Huang YQ, et al. Dynamic changes in pre- and postoperative levels of inflammatory markers and their effects on the prognosis of patients with gastric cancer. J Gastrointest Surg. 2021;25(2):387–396. doi:10.1007/s11605-020-04523-8
27. Iasonos A, Schrag D, Raj GV, Panageas KS. How to build and interpret a nomogram for cancer prognosis. J Clin Oncol. 2008;26(8):1364–1370. doi:10.1200/JCO.2007.12.9791
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy of the Systemic Immune-Inflammation Index and Prognosis Nutritional Index for the Diagnosis of Venous Thromboembolism in Gastrointestinal Cancers
Zhang L, Fang Y, Xing J, Cheng H, Sun X, Yuan Z, Xu Y, Hao J
Journal of Inflammation Research 2022, 15:4649-4661
Published Date: 15 August 2022
Nomogram Based on Preoperative Fibrinogen and Systemic Immune-Inflammation Index Predicting Recurrence and Prognosis of Patients with Borrmann Type III Advanced Gastric Cancer
Wang H, Yin X, Ma K, Wang Y, Fang T, Zhang Y, Xue Y
Journal of Inflammation Research 2023, 16:1059-1075
Published Date: 12 March 2023
Predictive Value of Pan-Immune Inflammation Value and Systemic Immune-Inflammation Index for Identifying Coronary Vulnerable Plaques: New Insights from Optical Coherence Tomography in Acute Coronary Syndrome Patients
Ji J, Wei X, Xue B, Wan D, Wu L, Liu H
Journal of Inflammation Research 2024, 17:10371-10382
Published Date: 4 December 2024
Analysis of Risk Factors and Development of a Predictive Model for Prognosis in Early-Stage Rectal Cancer Patients
Zhang CT
International Journal of General Medicine 2025, 18:3961-3968
Published Date: 16 July 2025
Prognostic Nomogram for Hepatocellular Carcinoma Patients with High Systemic Immune-Inflammation Index: Validation in Surgical and Immunotherapy Cohorts and Exploration of Immune Microenvironment Mechanisms
Wang X, Hu Z, Ding J, Zheng S, Wei B, Zhou Y, Wang S
Journal of Hepatocellular Carcinoma 2026, 13:588390
Published Date: 30 March 2026