Back to Journals » Journal of Pain Research » Volume 16
A Pilot Study for Effectiveness of Non-Pharmacological versus Pharmacological Treatment Strategies for Lumbar Disc Herniation: A Pragmatic Randomized Controlled Trial
Authors Kim D, Kim ES, Lee YJ ![]() , Lee JY
, Lee JY ![]() , Park KS, Jung SY, Yang C
, Park KS, Jung SY, Yang C ![]() , Han CH
, Han CH ![]() , Ha IH
, Ha IH ![]()
Received 12 May 2023
Accepted for publication 12 August 2023
Published 18 September 2023 Volume 2023:16 Pages 3197—3216
DOI https://doi.org/10.2147/JPR.S421148
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Doori Kim,1 Eun-San Kim,1 Yoon Jae Lee,1 Jee Young Lee,2 Kyong Sun Park,3 So Young Jung,4 Changsop Yang,5 Chang-Hyun Han,6,7 In-Hyuk Ha1
1Jaseng Spine and Joint Research Institute, Jaseng Medical Foundation, Seoul, 06110, Republic of Korea; 2Department of Korean Internal Medicine, Integrative Cancer Center, Cha Ilsan Medical Center, Goyang-si, Gyeonggi-do, Republic of Korea; 3Jaseng Hospital of Korean Medicine, Seoul, 06110, Republic of Korea; 4Clinical Research Coordinating Team, Korea Institute of Oriental Medicine, Daejeon, 34054, Republic of Korea; 5Clinical Medicine Division, Korea Institute of Oriental Medicine, Daejeon, Republic of Korea; 6Korean Convergence Medical Science, University of Science & Technology (UST), School of Korea Institute of Oriental Medicine, Daejeon, 34054, Republic of Korea; 7KM Science Research Division, Korea Institute of Oriental Medicine, Daejeon, 34054, Republic of Korea
Correspondence: In-Hyuk Ha, Jaseng Spine and Joint Research Institute, Jaseng Medical Foundation, 540 Gangnam-daero, Gangnam-gu, Seoul, 06110, Republic of Korea, Tel +82-2-2222-2740, Fax +82-2-2222-2737, Email [email protected] Chang-Hyun Han, KM Science Research Division, Korea Institute of Oriental Medicine, 1672 Yuseong-daero, Yuseong-gu, Daejeon, 34054, Republic of Korea, Tel +82-(0)42-868-9498, Fax +82-(0)42-869-2775, Email [email protected]
Purpose: We aimed to compare the efficacy, safety, and cost-effectiveness of non-pharmacological- and pharmacological treatment strategies for Lumbar disc herniation (LDH) in pragmatic clinical settings.
Patients and Methods: This study was a pilot, two-armed, parallel pragmatic randomized controlled trial. Thirty patients aged 19– 70 years with a numeric rating scale (NRS) score ≥ 5 for sciatica and confirmed LDH on magnetic resonance imaging (MRI) were included. Participants were assigned in a 1:1 ratio to non-pharmacological (non-Phm) or pharmacological (Phm) treatment group. They were treated for 8 weeks and a total follow-up period was 26 weeks after randomization. Non-Phm treatment included acupuncture, spinal manual therapy, etc., Phm included medication, injection, nerve block, etc., The primary outcome was a numeric rating scale (NRS) of radiating leg pain. NRS for low back pain, Oswestry disability index, visual analog scale, Fear-Avoidance Beliefs Questionnaire, patient global impression of change, Short Form-12 Health Survey, version 2, 5-level European Quality of Life-5 dimensions (EQ-5D) were also measured. Linear mixed model was used to evaluated the difference in change of outcomes from baseline between two groups. An economic evaluation was conducted using incremental cost-effectiveness ratios.
Results: There was no significant difference between the two groups in the intervention period, but non-Phm group showed significantly greater degree of improvement in follow-up of Week 14. Difference in the NRS for sciatica and ODI were 1.65 (95% CI 0.59 to 2.71, p=0.003) and 8.67 (95% CI 1.37 to 15.98, p=0.21), respectively in Week 14. The quality-adjusted life year (QALY) value calculated by EQ-5D and Short Form-6 Dimension were 0.006 (95% CI − 0.012 to 0.024, p=0.472) and 0.015 (95% CI − 0.008 to 0.038, p=0.195) higher in non-Phm group than in Phm group. The cost was lower in non-Phm group than in Phm group (Difference: − 682, 95% CI − 3349 to 1699, p=0.563).
Conclusion: We confirmed that the non-Phm treatment could be more cost-effective treatments than Phm treatments and feasibility of a large-scale of main study in future.
Keywords: conservative treatment, intervertebral disc displacement, low back pain, sciatica
Introduction
Lumbar disc herniation (LDH) is one of the most common causes of low back pain (LBP) and radiating leg pain (sciatica).1 The prevalence of sciatica vary from 1.6% in the general population to 43% in specific working populations.2 Most cases of sciatica caused by acute LDH show favorable outcomes and resolve within 2 weeks to 3 months.3,4 However, in some cases, LDH becomes a chronic condition of lifelong experience with LBP.5
Conservative treatment should be the first-line therapy for sciatica; nonetheless, the best method of conservative treatment remains unclear, with guidelines differing in their recommendations.4 The American College of Physicians (ACP) recommends that non-pharmacological treatments, such as superficial heat treatment, massage, acupuncture, and spinal manipulation, should be selected for patients with LBP with or without sciatica.6 Among these various non-pharmacological treatments, there are many differences between guidelines for acupuncture and manual therapy. Korea guidelines7 recommend acupuncture and spinal manual therapy with high grade level of evidence. It suggested that acupuncture, electroacupuncture, and spinal manual therapy are helpful in improving pain and overall symptoms in patients with LDH. However, the United Kingdom (UK) guidelines8 recommend manual therapy only alongside an exercise program and against acupuncture. The Danish guidelines9 also state that acupuncture has low-quality evidence.
On the other hand, harms and serious adverse events for these non-pharmacological therapies have not been reported.6 In an RCT study on manual therapy for the neck, adverse events related to the musculoskeletal system and nervous system were observed in 5 patients (9.3%) in the intervention group, but all were mild or moderate side effects.10 In a systemic review of acupuncture treatment for a LDH patient, adverse events were reported in two trials, one reported no adverse events, and one reported local haematoma.11
The recommendations for invasive treatment also vary widely depending on guidelines. Some recent guidelines6,9 do not recommend epidural injections or facet joint injections, whereas the UK guidelines8 recommend epidural injections for patients with severe sciatica. The United States (US) guidelines12 also strongly recommend epidural injections for the management of sciatica or LDH. It suggested that transforaminal epidural steroid injections provide short-term (2–4 weeks) pain relief in LDH patients. Epidural injection is associated with serious adverse events such as plegia, spinal cord injury, dural hemorrhage, paralysis, stroke, and dural punctures, although the incidence rate is low.13–15
Meanwhile, nevertheless medication is one of the most frequently used treatments for back pain and neuropathic patients,16,17 major guidelines tend to place less emphasis on medication treatments.18 The ACP6 recommends that pharmacological treatment should be considered only when patients have inadequate response to non-pharmacological therapy. NSAIDS, one of the representative medication, is associated with slight pain and functional improvement, but has a high possibility of adverse events such as abdominal pain, gastrointestinal bleeding/perforation, dizziness, and headache.6 Opioids are also associated with nausea and vomiting, and have long-term adverse events such as addiction and abuse. Several guidelines caution that opioids should be used only in carefully selected patients for a short duration.19,20
Nevertheless, there are several guidelines that recommend medication. UK guidelines state that non-steroidal anti-inflammatory drugs (NSAIDS) should be considered for managing LBP, the lowest effective dose should be prescribed for the shortest possible time, considering potential harm.8 Another guideline from NICE offered a choice of amitriptyline, duloxetine, gabapentin or pregabalin as initial treatment for neuropathic pain.21
In the other hand, medication such as opioids and epidural injections are widely used in real-world clinical practice. Opioid use is highly common and has been increasing in Canada and the US.22,23 In South Korea, 78.5% of patients with LDH were prescribed non-opioid analgesics, and 4% were prescribed opioid analgesics.24 In addition, nerve blocks were used in > 14% of the patients with LBP,24 while 10%–11% of the patients used injection therapy.25 This indicates that active pharmacotherapy, including nerve blocks, is commonly used in real-world clinical practice, regardless of the recommendations in clinical practice guidelines.
Evidently, relevant high-quality clinical studies are necessary to address conflicting opinions among guidelines and gaps between recommendations and the real-world. South Korea has a dual healthcare system with Western and Korean medicine, and Korean Medicine doctors (KMDs) can independently use acupuncture or manual therapy. In addition, patients can select treatment methods according to their preferences and medical conditions. Thus, it is appropriate to compare the two-treatment strategy in real-world clinical settings.
Therefore, in this study, we aimed to exploratory compare the efficacy and cost-effectiveness of non-pharmacological and active pharmacological treatment strategies based on pragmatic clinical settings and evaluate the feasibility of conducting a large-scale clinical trial. This study hypothesized that non-pharmacological treatment would be more cost-effectiveness than pharmacological treatment. The results of this study will be useful information for patients and clinicians who have to choose the treatment options.
Materials and Methods
Study Design and Setting
This was a pragmatic randomized controlled, parallel-grouped pilot study. In a spine specialty hospital of Korean medicine in South Korea, 30 patients were selected and randomly assigned to a non-pharmacological treatment (Non-Phm) group and a pharmacological treatment (Phm) group at a 1:1 ratio (15 participants per group). The patients underwent treatment for a total of 8 weeks, with two sessions a week, and followed up after 9, 13, and 26 weeks from randomization. Patient recruitment was conducted from July to December 2021, and the last follow-up ended in June 2022.
Before commencing the clinical study, the investigator held a one-on-one briefing session with the study participants to provide sufficient explanation of the information on the clinical study (effects, adverse events, and matters related to patient safety), and obtained the signed consent form from all participants. Timelines of the clinical study was shown in Supplementary Table 1.
All documents related to this study, including the protocol, were approved by the Institutional Review Board of the Jaseng Hospital of Korean Medicine before the initiation of patient recruitment (JASENG 2021–02-015). The protocol was registered at Clinicaltrials.gov (NCT04833270) and cris.nih.go.kr (KCT0006113). This study was conducted in accordance with the Declaration of Helsinki.
Participants
In this study, men and women between the ages of 19 and 70 years who had an average numeric rating scale (NRS) score ≥5 for radiating leg pain (sciatica) for three consecutive days and who were confirmed with LDH on magnetic resonance imaging (MRI) that could account for the radiating pain in the leg were included. If the grade of disc herniation on MRI was “protrusion” or higher, it was judged to be LDH. The MRI reading was performed by a radiologist. Whether the patient’s symptoms were due to LDH findings on MRI was judged by a Korean medicine doctor with more than 2 years of clinical experience. As for disease codes of LDH, M51 for the seventh revision of the Korean standard classification of disease (KCD-7) was used. The KCD-7 is the Korean version mapping of the International Classification of Disease and Causes of Death-10 (ICD-10). Those who were diagnosed with specific critical conditions that may cause low back pain or radiating leg pain (spine metastasis of malignancy, acute fracture of the spine, or spine dislocation); those who were taking steroids, immunosuppressants, psychotropic medications, or any other medication that may affect the results of this study; and those who had undergone lumbar spinal surgery within the last 3 months were excluded from this study. The inclusion and exclusion criteria for the eligibility of the participants are presented in Supplementary Material 1.
Intervention
In this study, the treatment strategy for each group was determined in advance but not the specific treatment methods. The treatment was conducted based on the assigned strategy; however, the details of the actual treatment were determined and implemented based on the decisions of the clinician according to the patient’s condition. All treatment details are recorded in detail in the case report form (CRF).
Non-Phm Treatment Group
In the Non-Phm group, the patients underwent a total of 16 sessions of treatment, twice a week for 8 weeks, in principle; however, the actual frequency was determined after considering the patient’s condition and the clinician’s judgment. Typical Korean medicine with Non-Phm treatments include acupuncture, electroacupuncture, and spinal manual therapy. The acupoints used in acupuncture treatment, depth of needle insertion, frequency of stimulation and intensity with a needle for electroacupuncture therapy, and type of manual were selected according to the clinical judgment of the KMD.
Phm Group
Active Phm treatment strategies include the prescription of medications, injections and nerve blocks. However, considering that there are almost no cases where only a drug prescription is made in actual clinical practice, physical therapy, such as transcutaneous electrical nerve stimulation (TENS) and interferential current therapy (ICT), can be performed together if necessary. During the 8-week intervention period, three sessions of nerve blocks and two drug prescriptions per week were recommended; nonetheless, the actual procedure, drug prescription, and number of prescription days were determined at the discretion of the responsible clinician.
Outcomes
Primary and Secondary outcomes
The primary outcome of this study was the NRS of radiating leg pain. The NRS is a numeric pain scale for the objective representation of subjective pain felt by individual patients, and the intensity of pain over the past week was evaluated. The patient selects a number from 0 to 10 that best represents the current level of pain and discomfort (0 representing no pain and 10 representing the worst pain and discomfort imaginable).26,27
For secondary outcomes, the NRS score for LBP, Oswestry disability index (ODI),28,29 visual analog scale (VAS) for LBP and radiating pain,27 Fear-Avoidance Beliefs Questionnaire (FABQ),30 patient global impression of change (PGIC),31,32 Short Form-12 Health Survey, version 2 (SF-12 v2),33 5-level European Quality of Life-5 dimensions (EQ-5D-5L) [9, 10, and credibility and expectancy were measured. All questionnaires used in this study were verified validity and reliability. Detailed descriptions for each outcome and timelines are presented in Supplementary Material 2.
In addition, changes in the severity of disc herniation on MRI was investigated, and the pathological state of disc herniation was classified into a total of four types (desiccated or bulging; protrusion; extrusion; and sequestration or migration) for each of the baseline and Week 27 follow-up time points. Regardless of the level of the spine, if any of the levels had a corresponding finding, it was considered present; otherwise, it was absent.
Resource Utilization Measurements
In addition to the intervention conducted within the trial, the utilization of healthcare services related to LBP and radiating leg pain was surveyed at each visit of the participants. For the survey, a questionnaire that was separately developed for this purpose with structured questions to assess formal or informal medical costs, non-medical costs, time costs, and costs of productivity loss was used. Formal medical costs refer to costs incurred in using the services of healthcare providers, while informal medical costs include costs of purchasing healthy functional food and medical devices. Non-medical costs include costs incurred while using healthcare services, such as transportation costs, the time the patient spent, and fee of the paid caregiver. The cost of productivity loss refers to the cost of economic loss caused by (i) not being able to participate in labor or (ii) reduced work productivity owing to illness.
For medications (drugs prescribed for a current medical condition or as a rescue medication), the types and doses of prescribed drugs were surveyed; further, for all treatments, the information on the cost per treatment was collected. The expenses identified from the survey were considered non-reimbursement and copayment, and the payer reimbursement was calculated using the cost of payer reimbursement corresponding to the age and gender of the patient with the applicable condition from the 2019 Health Insurance Review and Assessment Service - National Patient Sample data.34
Transportation costs were also investigated through patient surveys; time costs were estimated through a survey on the time taken for patients to receive treatment and then by individual substitution of the standard wage corresponding to the age and gender of the patient from the 2021 Survey Report on Labor Conditions by Employment Type.35
Productivity loss was surveyed using the Work Productivity and Activity Impairment–Specific Health Problem (WPAI–SHP) questionnaire.36 WPAI–SHP allows the assessment of absenteeism (work time missed), presenteeism (impairment while working), overall work productivity loss (absenteeism + presenteeism), and activity impairment (impairment in regular activities) due to specific health problems in the past week.37,38 In this study, to consider productivity loss and opportunity costs for the self-employed and household tasks, as well as the productivity loss for paid workers under employment, overall work productivity loss was applied for paid workers under employment, and activity impairment was applied for other participants to calculate WPAI. The cost of economic loss due to productivity loss was estimated by multiplying the WPAI obtained through patient surveys and the standard wage applicable to the age and gender of the patient.35
For all costs, the inflation rate in the healthcare price index was applied to convert to the amount representative of the price as of 2022. For exchange rates, the average exchange rate from January–June 2022, based on a bank in South Korea, which was 1234.31 won, was applied39 and expressed in US dollars.
Sample Size Estimation
There has been no previous study comparing the effectiveness of Non-Phm and active Phm in patients with LDH, which could have provided a basis for calculating the target sample size of this study. As a pilot study to evaluate the feasibility of a follow-up study, this study allocated 12 participants to each group, which was considered the minimum number necessary for a pilot study;40 further, considering a dropout rate of 20%, 15 participants were to be allocated to each group. Therefore, a total of 30 patients were recruited for this study.
Randomization
Participants who were determined to be eligible based on the inclusion and exclusion criteria and signed the Informed consent form for this clinical study were assigned to two groups at a ratio of 1:1 (15 participants each) using a randomization table The randomization table was created in advance by a statistician using R studio 1.1.463 (© 2009–2018 RStudio, Inc., Boston, Massachusetts, United States). The random sequence was generated by block randomization, and the size of one block was randomly set between 2 and 4. The generated randomization results were sealed in an opaque envelope and stored in a double-locked cabinet, and the screening researcher of each study institute opened the randomization envelope for each patient to proceed with the group assignment. The randomization number assigned to each study participant was recorded on the electronic chart.
Blinding
Owing to the nature of interventions in this study, blinding was not possible; therefore, this study was conducted as an open-label study, while assessor blinding was applied. An assessor who did not participate in the process of intervention in this study was blinded to the group allocation and performed the assessment in a separate place before the intervention.
Data Management and Monitoring
The electronic CRF (e-CRF) based on the internet-based clinical research management systems operated by the Korean Centers for Disease Control and Prevention was used in this study. Before the commencement of the study, training was held for the investigators in their respective institutions on the developed standard operating procedures and e-CRF input guidelines. The data entered into the e-CRF were locked and concealed from all investigators except for the person in charge of data management. In addition, monitoring was conducted five times in total to ensure the safety of participants and integrity of the study data.
Statistical Analysis
In this study, intention-to-treat (ITT) analysis was conducted as the primary analysis. For handling missing data, a mixed model for repeated measures was used in the case of the linear mixed model (LMM), which is a primary analysis. An area under the curve comparison, a secondary analysis, was performed after replacing the missing data with multiple imputations. For sensitivity analysis, we initially planned to present the per-protocol (PP) analysis results for patients who received >12 sessions of treatment during the 8-week intervention period; all but one patient underwent >12 treatment sessions, and this patient, who had only baseline values, was excluded from LMM analysis. Therefore, the analysis results of the ITT and PP analysis sets were the same; hence, they are not presented separately.
The sociodemographic characteristics of the study participants and treatment expectancy were evaluated for each group. Continuous variables were expressed in terms of mean (standard deviation) or median (quartile), and the differences between the two groups were tested by using independent t-test or Wilcoxon-rank sum test depending on the distribution of samples. Categorical variables were expressed using frequencies (%), and the differences between the two groups were compared using the chi-square test or Fisher’s exact test.
Regarding the outcome measures in this clinical study, the difference in changes in continuous outcomes from baseline levels for each timepoint between the two groups was evaluated. Regarding primary analysis, an LMM was used, with baseline values of each outcome used as covariates and the group as the fixed factor. In addition, the areas under the curve from randomization to the last week of the follow-up period were calculated to compare the total changes in outcome values in the two groups. Effect size for primary and secondary outcomes were also calculated for Week 9 and Week 13.
The significance level was set to 0.05 for all statistical analyses, and SAS 9.4 (© SAS Institute, Inc., Cary, NC, USA) or R studio 1.1.463 (© 2009–2018 RStudio, Inc., Boston, Massachusetts, United States) was used for the statistical analyses.
Economic Evaluation
In this study, cost-effectiveness was compared between the Non-Phm- and Phm groups through economic evaluation. The primary outcome for economic evaluation was the incremental cost-effectiveness ratio (ICER) of the Non-Phm group to the Phm group. ICER was calculated by dividing the difference in cost between the two groups by the difference in the quality-adjusted life year (QALY) value. The values of QALY were calculated with EQ-5D-5L and short-form six dimensions (SF-6D). Missing data were replaced by multiple imputations using the Markov chain Monte Carlo method. The uncertainty of cost-effectiveness was estimated by bootstrapping the cost and QALY, and the probability that the Korean medicine Non-Phm would be cost-effective as a function of willingness to pay (WTP) was determined using the cost-effectiveness acceptability curves. All analyses were conducted from societal perspectives, including the cost of productivity loss. The threshold for WTP was set at $24,710 based on the reported amount in South Korea.41
Two types of sensitivity analyses were performed. First, we modified the calculation method for the production loss. In the primary analysis, the overall work impairment of all patients, including participants who were not paid workers, was calculated. In the sensitivity analysis, it was considered that income loss due to time and productivity loss occurred only for employed patients, and the loss for all patients who were not paid workers under employment was calculated as 0 US dollars. Second, a cost-effectiveness analysis for ODI was conducted. Differential ODI was calculated using the difference between the baseline and the last follow-up time point for each group.
Adverse Events
In this study, all adverse events (AEs) that occurred during the clinical trial were investigated and recorded. AEs were collected through patient complaints or observations, and the occurrence of AEs was compared between the two groups in terms of frequency.
The causality between each treatment method and the AE that occurred was categorized into six levels (1 = definitely related, 2 = probably related, 3 = possibly related, 4 = probably not related, 5 = definitely not related, and 6 = unknown). The severity of AEs was classified into three levels following the Spilker AE classification system [Mild (1): did not impair the participant’s normal activities of daily living (ADLs), caused minimal discomfort, and required no additional treatment; moderate (2): significantly impaired the participant’s normal ADLs and may have required treatment, but they were resolved after treatment; severe (3): severely impaired the participant’s normal ADLs, required intense treatment, and left sequelae].
Results
Participants
From May 2021 to December 2021, a total of 172 patients underwent the screening process. Among those who were recruited, 30 patients were enrolled and randomly assigned to the Non-Phm and Phm groups. In the Non-Phm group, one participant withdrew consent after the first visit, and another patient withdrew consent after 7 weeks of treatment. No participants dropped out in the Phm group. Consequently, ITT analysis was conducted on a total of 29 patients (n = 14 in the Non-Phm group; n = 15 in the Phm group). As all 29 participants underwent >12 sessions of treatment, PP analysis was not conducted separately (Figure 1).
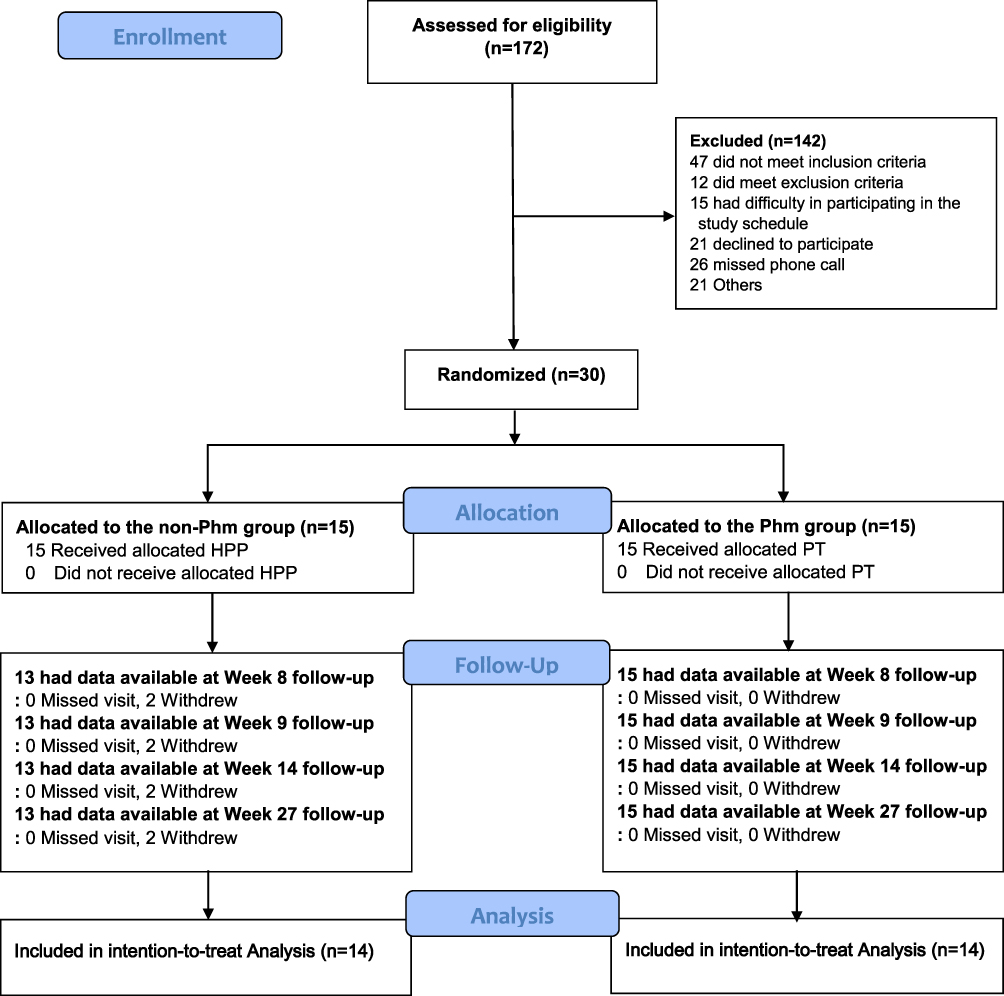 |
Figure 1 Flowcharts of participants. Of the total 172 patients screened, 30 who met the inclusion criteria and agreed to participate in the study were enrolled. Intention-to treat analysis was performed in 15 patients in the Phm group and 14 patients in the non-Phm group. Abbreviations: Phm, pharmacological treatment; non-Phm, non-pharmacological treatment; |
Baseline Characteristics
The baseline characteristics of the study participants are outlined in Table 1. The proportion of females in the Non-Phm group and Phm group was 60.0% and 46.7% respectively (p=0.714), and the mean age was 45.2 ± 14.2 and 49.1 ± 8.7 (p=0.369). There were 5 (33.3%) and 7 (46.7%) patients who were recommended for spinal surgery (p=0.709), and 1 (6.7%) and 2 (13.3%) had spinal surgery (p=1.000). On MRI, 4 (26.6%) and 5 (33.3%) patients showed more than extrusion findings on disc herniation. There were no outcomes and characteristics that showed significant differences between the two groups at baseline.
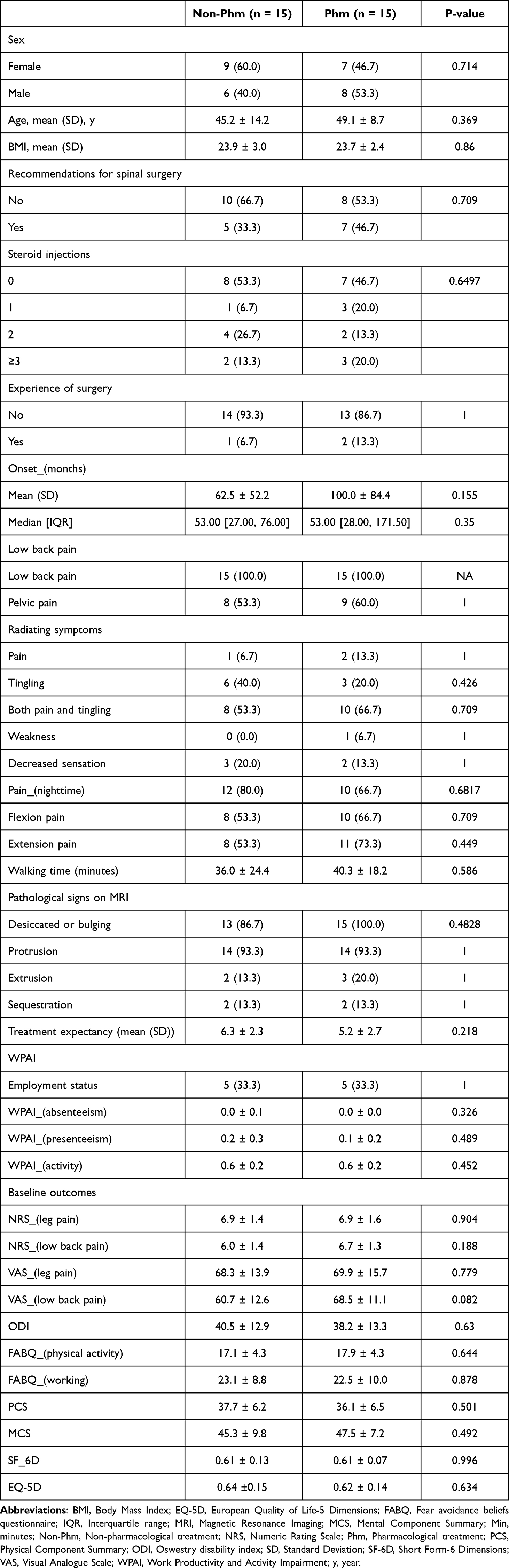 |
Table 1 Baseline Characteristics of Participants by Randomized Group |
Treatments and Compliance Rate
All patients in the Non-Phm group underwent a session of acupuncture, electroacupuncture, and spinal manual therapy. Acupuncture was performed within an average of 14.7 ± 3.9 times per person; the Shinsu acupoint was the most frequently used point in the acupuncture treatment. All patients in the Phm group received drug prescriptions, nerve blocks, and physical therapy. Regarding physical therapy, ICT and ultrasound were the most frequently used. Among medications, aceclofenac was prescribed to all patients for an average of 53.9 ± 12.4 days per patient (Supplementary Table 2).
The average number of visits in the non-Phm group was 14.7 ± 3.9, and the average compliance rate was 92.1% (out of a total of 16 visits). The average number of visits in the Phm group was 15.2 ± 1.3, and the average compliance rate was 95.0%. In addition, the number of days the Phm group actually took the drug was 49.7 ± 7.9 days with the average compliance rate of 83.6%.
Primary and Secondary Outcomes
The NRS score for radiating leg pain, which was the primary outcome, showed no significant difference between the two groups at Week 9, the primary endpoint. However, at Week 14 in the follow-up period, the Non-Phm group showed a significantly greater improvement (difference: −0.56, 95% CI −1.62 to 0.50, p=0.003). Both NRS and VAS scores for LBP and radiating leg pain showed a greater improvement in the Phm group at Week 9—immediately after completion of the 8-week intervention (NRS in Phm group: 2.91, 95% CI 2.10 to 3.71; NRS in Non-Phm group: 3.25, 95% CI 2.39 to 4.10; VAS in Phm group: 27.71, 95% CI 18.81 to 36.60; VAS in Non-Phm group: 32.55, 95% CI 23.11 to 42.00). At Week 14 in the follow-up period, superior improvement was achieved in the Non-Phm group, but the difference was not significant (Difference of NRS: 0.75, 95% CI −0.43 to 1.93, p=0.208; Difference of VAS: 9.92, 95% CI −4.46 to 24.31, p=0.175). Regarding the ODI score, the Non-Phm group showed superior improvement at all time points of Weeks 9, 14, and 27; at Week 14 in the follow-up period, the difference was significant (Difference 8.67, 95% CI 1.37 to 15.98, p=0.021). Quality of life as measured using EQ-5D and SF-12 also continued to be superior in the Non-Phm group, but the difference between the two groups was not significant. (Table 2, Supplementary Table 3, and Figure 2).
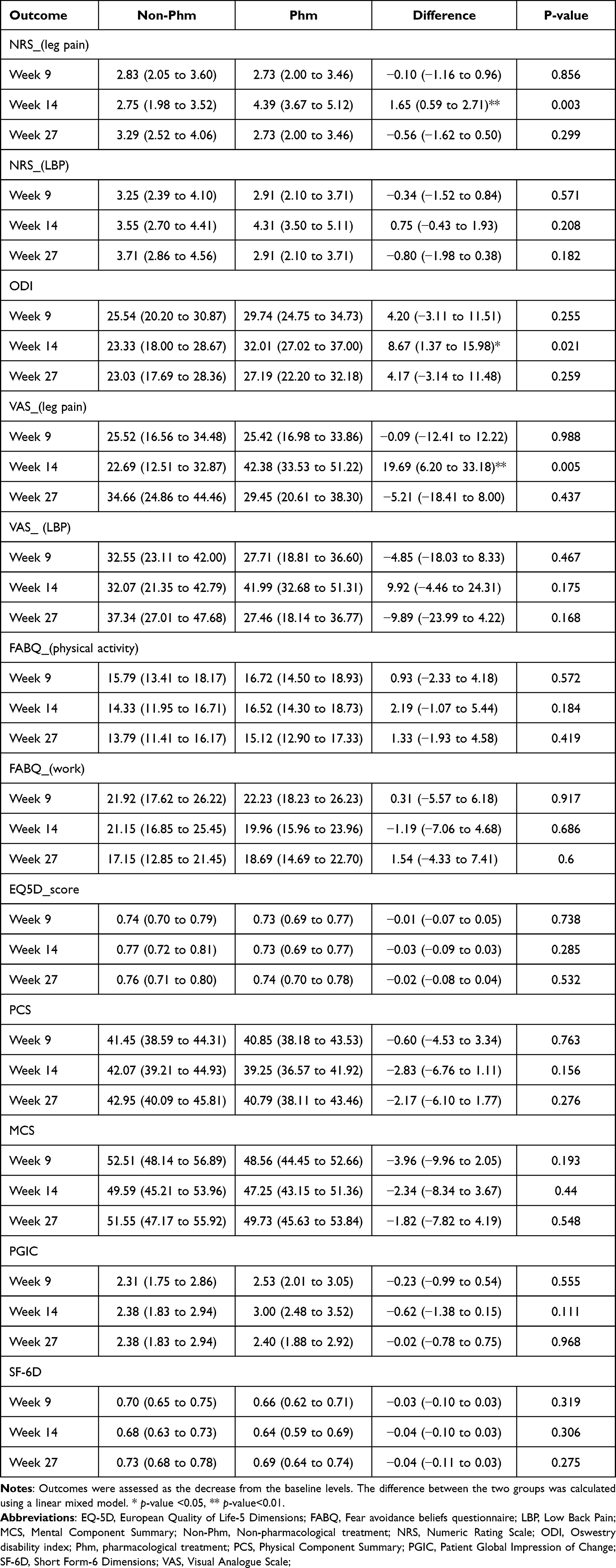 |
Table 2 Primary and Secondary Outcomes According to Treatment and Endpoint |
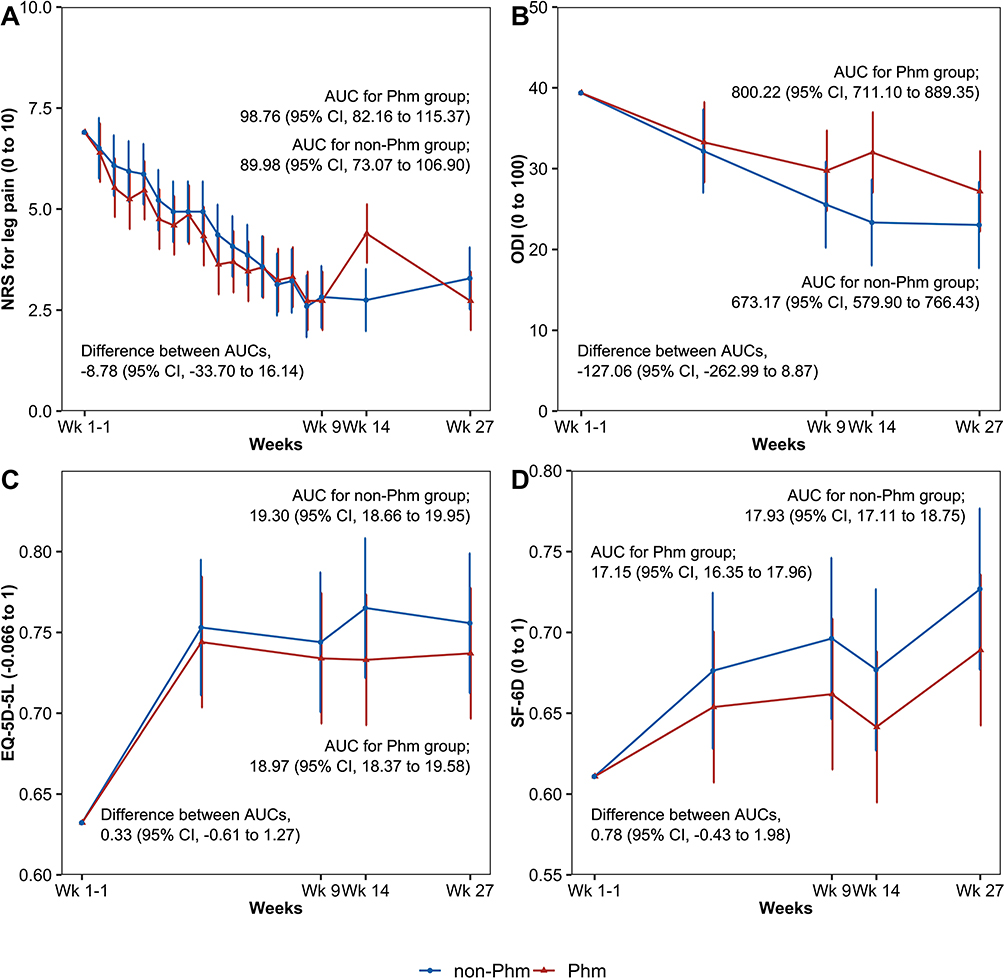 |
Figure 2 Changes in outcomes over time. (A) Changes of NRS for leg pain, (B) Changes of ODI, (C) Changes of EQ-5D-5L, (D) Changes of SF-6D. Abbreviations: NRS, Numeric Rating Scale; ODI, Oswestry Disability Index; EQ-5D-5L, 5-level European Quality of Life-5 dimensions; SF-6D, Short Form-6 Dimension; AUC, Area Under Curve; Phm, Pharmacological treatment; non-Phm, non-pharmacological treatment; Wk, Week; CI, Confidence Interval. |
The AUC analysis, which calculated the cumulative outcome for 26 weeks—the total duration of the follow-up—revealed no outcome that showed a significant difference between the Non-Phm and Phm groups (Table 3). However, the Non-Phm group showed greater improvement than did the Phm group in the following outcomes: NRS for leg pain, VAS for leg pain, FABQ, physical activity, ODI, EQ-5D, Physical Component Summary, Mental Component Summary, and SF-6D.
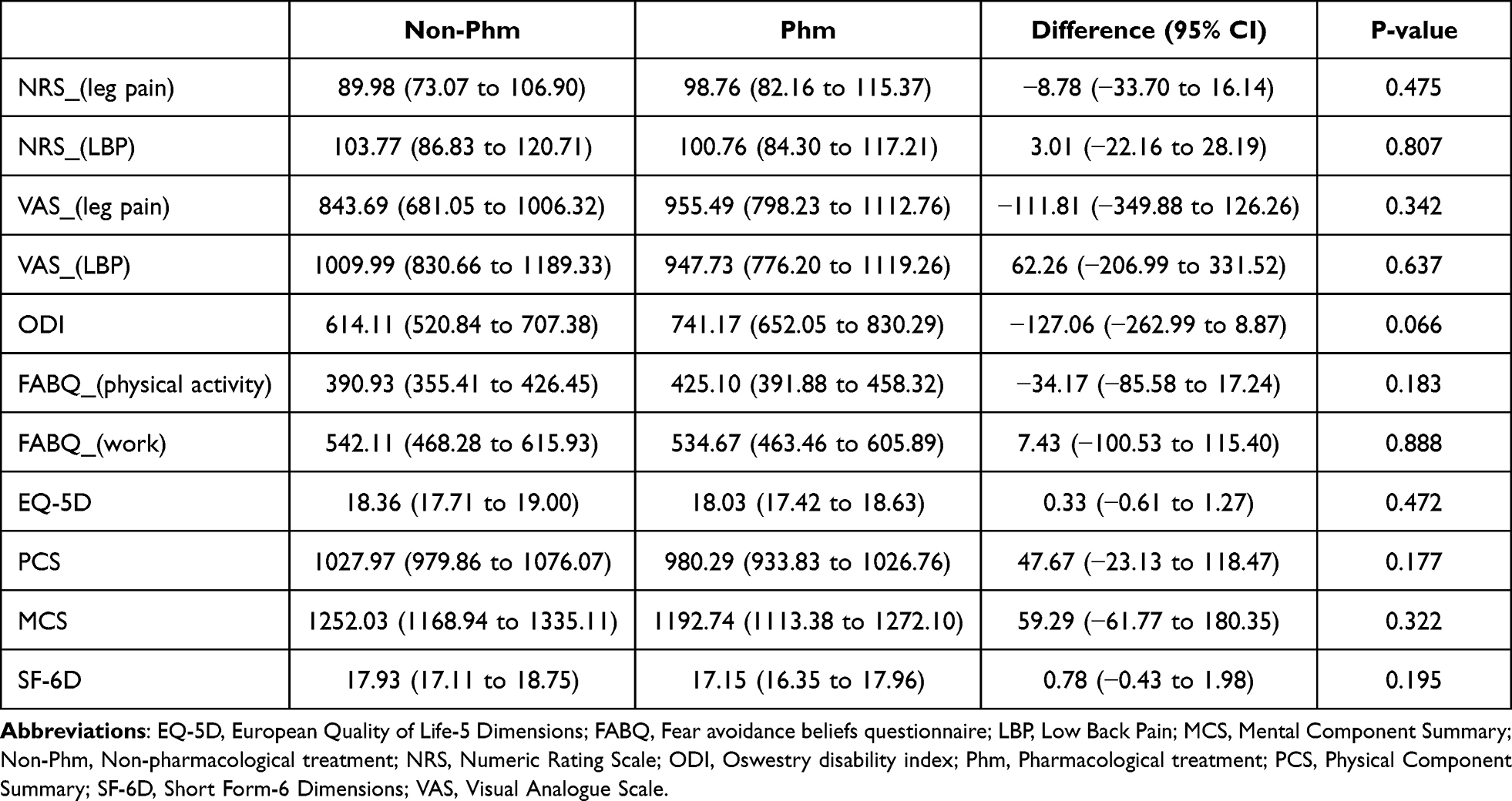 |
Table 3 Area Under the Curve of Outcomes According to Treatment |
The effect size was calculated as the difference between baseline and week 9 and baseline and week 14 values (Supplementary Table 4). As a result of the analysis, the effect size of NRS for leg pain was 0.03 and 0.85 in Week 9 and Week 13, respectively, that of NRS for LBP was 0.05 and 0.56, and that of ODI was 0.35 and 0.88, respectively. Overall, the effect size of Week 13 was calculated larger than that of Week 9, and in particular, the effect sizes of NRS for leg pain, ODI, VAS for leg pain and PCS at Week 13 were very high (0.85, 0.88, 0.90, and 0.76, respectively).
MRI Changes
All patients who participated in this clinical trial underwent MRI scans at screening, but at the last follow-up of Week 26, 10 patients in Non-Phm group and 12 patients in Phm group underwent MRI scans. MRI analysis was performed only for patients who had MRI scans at both baseline and follow-up. As a result, all all three patients (two in the Phm group and one in the Non-Phm group) who showed sequestration or migration at baseline resolved (Supplementary Table 5). There were 3 patients (25.5%) in the Phm group only at baseline with extrusion findings on MRI, and the same was observed at Week 26. At baseline, 10 patients (100.0%) in the Non-Phm group and 11 patients (91.7%) in the Phm group showed protrusion, and at Week 26, 9 (90.0%) and 11 (91.7%), respectively.
Adverse Events
A total of nine cases of AEs were observed in seven patients, of which, six AEs were “Definitely not related” to the intervention in terms of causality and three AEs were “Possibly related” to the intervention. All three “possibly related” AEs occurred in the Phm group, and the symptoms of AEs were gastritis, nausea, and headaches. The severity of all AEs that occurred during the study was mild (Supplementary Table 6).
Economic Evaluation
The cost analysis of the two groups revealed that the Non-Phm group spent $378 (95% CI: 21 to 765) more in medical costs than the Phm group did, but saved $97 (95% CI: −274 to 76) and $964 (95% CI: −3742 to 1175) in non-medical costs and productivity loss cost, respectively, compared to the Phm group. Consequently, in terms of the total cost, the Non-Phm group spent $7907 (95% CI 6498–9604) and the Phm group spent $8589 (95% CI: 6717–10,772), indicating that the Non-Phm group spent $682 (95% CI: –3349 to 1699) less for healthcare utilization in total. The difference in QALY between the two groups was 0.006 (95% CI: –0.012 to 0.024) in terms of EQ-5D and 0.015 (95% CI: −0.008 to 0.038) in terms of SF-6D, indicating that the value of QALY in the Non-Phm group was larger (Table 4). The healthcare costs and resource utilization during the intervention- and follow-up periods are summarized in Supplementary Table 7.
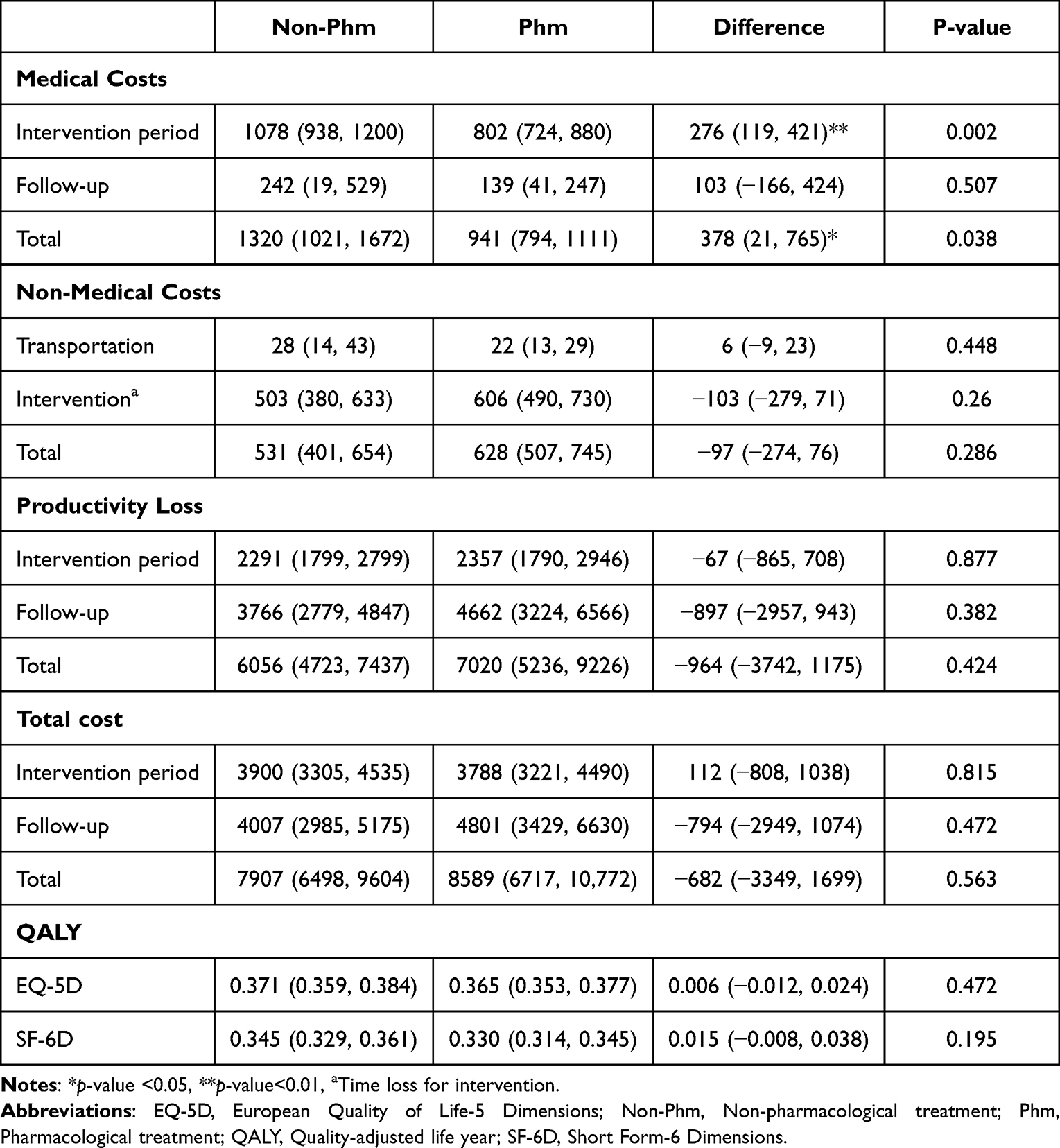 |
Table 4 Comparisons of Costs and QALY Between the Two Groups |
Table 5 shows the economic evaluation results of Non-Phm compared with Phm. From a societal perspective, the Non-Phm group showed a higher QALY and lower cost than the Phm group did, confirming that Non-Phm was a dominant option. Based on the analysis of WTP, the probability of Non-Phm being the cost-effective option was 75.9% in terms of EQ-5D and 80.2% in terms of SF-6D. The cost-effectiveness plane and cost-effectiveness acceptability curves are shown in Figure 3.
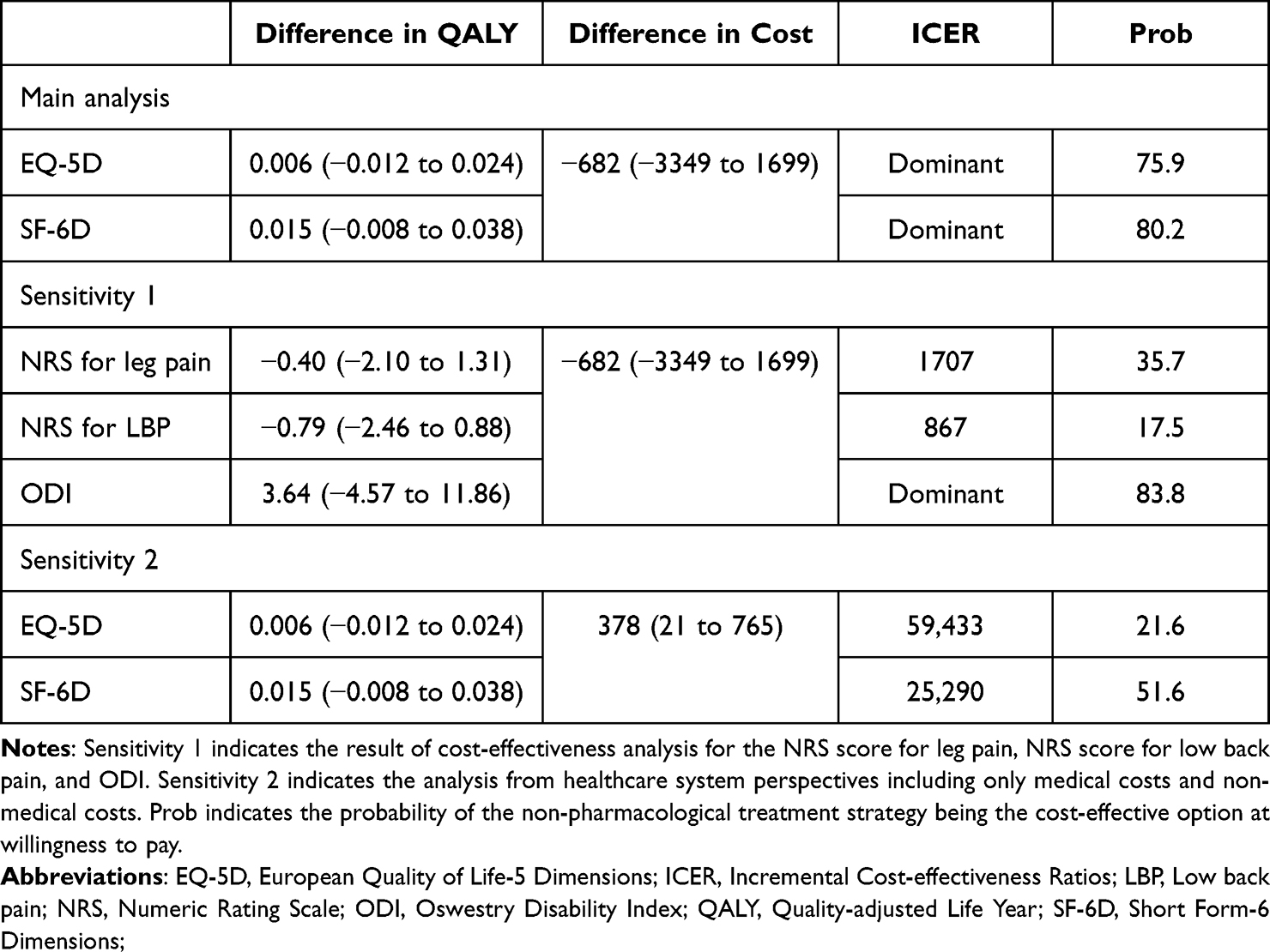 |
Table 5 Economic Evaluation Results |
 |
Figure 3 Comparison of cost-effectiveness of non-pharmacological and pharmacological treatments in terms of societal perspective. (A) Cost-effectiveness plane, (B) Cost-effectiveness acceptability curves. Abbreviations: EQ-5D-5L, 5-level European Quality of Life-5 dimensions; SF-6D, Short Form-6 Dimension. |
Discussion
Currently, there are multiple treatment options for patients with LDH, with inconsistencies among guidelines for conservative treatment of LDH and a gap between treatment practice in real-world clinical settings and the guidelines. This pilot study was conducted to evaluate the feasibility of a clinical study comparing Non-Phm and Phm for patients with non-acute LDH. At the time of follow-up, 1 month after the intervention, the degree of improvement in ODI and NRS score of radiating leg pain was significantly greater in the Non-Phm than in the Phm group.
There are various treatment options for Non-Phm treatment strategies, but there are often conflicting guidelines for acupuncture and manual therapy, especially for acupuncture. Meanwhile, in Korea, many back pain patients use Korean medicine, and acupuncture and spinal manipulation are representative Non-Phm treatments used by Korean medicine doctors. Therefore, in this study, among Non-phm treatment strategies, acupuncture and manual therapy were selected and compared with Phm treatment.
The primary outcome of this study was NRS for leg pain, and besides this, both NRS and VAS are used to assess leg and back pain. Both NRS and VAS are validated outcomes to assess pain severity. However, there is a difference that NRS can be asked verbally, and VAS should be evaluated by looking at the paper. For convenience, this study allowed telephone surveys at the f/u, but VAS is an item that cannot be surveyed over the phone. Therefore, it is decided to primary outcome as NRS, not VAS. In addition, the use of both scales was to see whether the two outcomes showed similar results, that is, to improve the reliability of the results. In this study, the reliability of the results was demonstrated by the two outcomes showing similar results and directions.
Based on the baseline characteristics of the 30 participants in this study, 40% were recommended for spinal surgery, 30% showed extrusion or sequestrated discs on MRI findings, and the NRS score for radiating leg pain was approximately 7 points, indicating that patients with severe LDH participated in this clinical trial. Additionally, the onset median value of the patients was 53 months in both groups, indicating many patients with chronic conditions of LDH.
The changes in the NRS score of radiating leg pain during the 8-week intervention period showed gradual improvement in both groups, but the improvement in the Phm group tended to be slightly greater. However, in the Phm group, the pain worsened at Week 14 and then improved again. Accordingly, at Week 14 in the follow-up period, the improvement in the Non-Phm group was significantly greater. Looking at the minimal clinically important differences (MCID) for major outcomes, there were previous studies where the MCID for NRS of back pain ranged from 1 to 2.3, and for NRS of leg pain ranged from 1 to 1.6 and ODI ranged from 10 to 12.8. In this study, at Week 14, the difference in NRS of leg pain between the two groups was 1.65 (95% CI 0.59 to 2.71), and the difference in ODI was 8.67 (95% CI 1.37 to 15.98).42–45 Therefore, the difference in NRS is judged to be a significant difference beyond the MCID between the two groups, and the ODI difference is also judged to be large, ranging from 67% to 87% of the MCID.
Meanwhile, ODI showed a slightly different pattern from the pain outcomes, with excellent improvement in the Non-Phm group throughout the intervention and follow-up periods. ODI in the non-Phm group continuously decreased during the follow-up period as well as during the intervention period, but in the Phm group, it also worsened at Week 14 and then improved again. Functional disability may be expected to improve once pain reduces, but this is not necessarily the case in real-world clinical practice. Pain and physical functions are associated with various factors such as biomechanical and psychosocial factors.46,47 One study that analyzed the correlation between pain, functional disability, and quality of life for 195 patients who used primary care for the management of LBP in Spain concluded that improvement in pain resulted in little improvement in functional disability and quality of life.47 Therefore, careful consideration of the most important outcome measure between pain and functional disability, which more accurately reflects the status of a patient’s improvement and can serve as a primary outcome, is crucial.
In addition, quality of life also improved overall in both groups, and the Non-Phm group showed an overall trend of higher quality of life scores during the intervention and follow-up periods than did the Phm group. LBP is associated with quality of life in various aspects such as pain, psychological factors, and societal factors.48 A large-scale cross-sectional survey study conducted in France49 indicated that LBP correlated with low quality of life. Assessment of quality of life is important in identifying patients’ needs and establishing treatment goals and plans; additionally, it is instrumental as an outcome evaluating treatment effects.50 Of note, the findings of this study indicated that Non-Phm showed a significant improvement in functional disability and quality of life compared to Phm. However, as this is a pilot study with a small sample size, whether Non-Phm is more effective in improving physical function and quality of life than the pain itself will need to be clarified in a large-scale main trial, which will be conducted later.
Meanwhile, the pain- and function-related outcomes of the Phm group improved up to the end of the intervention period, worsened considerably at Week 14 in the follow-up period, and improved again at Week 27 in the follow-up period. The worsening at Week 14 is thought to be caused by the discontinuation of medication that suppressed pain during the intervention period. To examine the reason for the improvement at Week 27, healthcare utilization by patients between Weeks 14 and 27 was investigated (Supplementary Table 8); six people in the Phm group sought additional medical care, and their average NRS and ODI scores at Week 14 were higher than those who did not seek additional healthcare service, indicating that patients who had little improvement or whose conditions exacerbated availed additional medical care. Nonetheless, the difference in improvement between the groups with and without healthcare utilization was not large, indicating that the improvement at Week 27 was not due to additional healthcare utilization between Weeks 14 and 27. Whether this pattern is a specific characteristic of the participants in this study or a general characteristic of Phm will need to be investigated in future studies planned for a larger number of patient samples.
Furthermore, MRI scans were examined at baseline and at the final follow-up timepoint. A comparison of the MRI findings at baseline revealed no significant difference between the groups. There were missing data at the time of follow-up, rendering comparison before and after the intervention challenging. However, analysis of patients with MRI findings both at baseline and after intervention revealed that sequestration-migration of disc herniation on MRI findings observed in all three patients resolved during the follow-up period. As important changes were observed on MRI in this way, in-depth research and considerable discussion will be needed in advance to leverage the changes on MRI findings in the main trial that will be conducted later.
An assessment and analysis of AEs in the Phm group revealed three AEs (gastritis, nausea, and headaches) possibly related to the intervention. NSAIDs, such as aceclofenac, were the main prescription drugs used in the Phm group during the intervention period, and pregabalin and a combination of tramadol and acetaminophen were prescribed to all patients. Tramadol, an opioid, is known to lead to abuse and misuse51 and cause side effects such as gastrointestinal symptoms, including constipation and nausea, and neurologic symptoms, including dizziness and headaches.52 NSAIDs are also reported to be associated with headaches and heartburn.52 In this study, although the AEs were not severe, they were observed at a high percentage of 20% in the Phm group. Therefore, when prescribing medications, the possible side effects and benefits of the drug must be carefully considered.
Additionally, economic evaluation alongside the pilot randomized controlled trial was conducted. Cost analysis revealed that medical cost, including the cost of the intervention, was high in the Non-Phm group. Among the treatments received by the Phm group, medication costs were low, and the cost of nerve blocks was relatively high. However, 11 of 15 patients in the Phm group received nerve blocks, and a total of 15 sessions of nerve blocks were performed. If more nerve blocks were performed, the medical cost result would have been different. In the Non-Phm group, although the medical costs were higher, the cost of productivity loss was lower, resulting in a slightly lower total cost. Furthermore, as QALY was higher in this group, Non-Phm was a more dominant option than Phm in terms of societal perspectives. However, the number of samples was too small to conduct economic evaluation alongside this pilot study; therefore, further verification is required on the reliability of the economic evaluation results. More reliable results may be obtained in a future large-scale clinical trial.
There are some limitations to this study. First, although our objective was to compare the Non-Phm and active Phm groups, physical therapy, such as TENS and ICT, was used in the active pharmacological treatment group. This decision was made in consideration of the fact that in the real world, patients with LDH rarely receive only pharmacological treatment without physical therapy.24 Besides, there are conflicting guidelines for nerve block, etc. Therefore, we wanted to compare the effects of non-pharmacological treatment with active pharmacological treatment including injection or nerve block, rather than simply medication prescription. However, active pharmacological treatment was not performed in the Phm group because the physician in charge of Phm treatment in this study was conservative in his treatment. Therefore, it is questionable whether the Phm group reflected the real world well. In further study, to better reflect the real world, we will consider a method of receiving treatment at an external institution rather than in trial institution. In additions, although we investigated the detailed information of treatment used in each group, types of nerve blocks and medications used for blocks were not investigated. This point will be supplemented to collect more detailed information about treatment in the main study. Lastly, due to the small number of subjects in this study, care must be taken in the interpretation and generalization of our study results. Again, due to the small number of participants, subgroup analysis on various baseline factors such as surgical and injection experience was not conducted in this study. It is expected that more reliable conclusions and interpretations will be possible through a large-scale main study and various results will be derived through subgroup analysis of various factors.
Nevertheless, in a situation where conflicting guidelines for pharmacological treatment exist and various AEs for pharmacological treatment are reported, this study showed the possibility of comparative advantage of certain non-pharmacological treatments. In addition, this study tried to increase the external validity of the results by reflecting the real-world clinical practice as much as possible. Finally, by successfully completing the pilot study, we were able to confirm the feasibility of the main large-scale study and decide to conduct the main study. The findings of this study can be useful information for patients and clinicians who have to choose the treatment options. If this superiority of non-pharmacological treatment is confirmed once again through the main large-scale study, it will be possible to provide a new treatment option that is less harmful to many LDH patients.
Conclusion
It is confirmed that Non-Phm treatment could be more cost effective than Phm treatment. Further large-scale studies will be conducted. The findings of this study can be useful information for patients and clinicians who have to choose the treatment options.
Abbreviations
EQ-5D, European Quality of Life-5 Dimensions; FABQ, Fear avoidance beliefs questionnaire; MRI, Magnetic Resonance Imaging; Non-Phm, Non-pharmacological treatment; NRS, Numeric Rating Scale; Phm, Pharmacological treatment; ODI, Oswestry disability index; SF-6D, Short Form-6 Dimensions; VAS, Visual Analogue Scale; WPAI, Work Productivity and Activity Impairment.
Data Sharing Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy/ethical restrictions.
Funding
This research was funded by the Korea Institute of Oriental Medicine (KIOM), Republic of Korea (grant number: KSN1823211).
Disclosure
The author reports no conflicts of interest in this work.
References
1. Goupille P, Jayson MI, Valat J-P, Freemont AJ. The role of inflammation in disk herniation-associated radiculopathy. Elsevier. 1998;28:60–71.
2. Konstantinou K, Dunn KM. Sciatica: review of epidemiological studies and prevalence estimates. Spine. 2008;33(22):2464–2472. doi:10.1097/BRS.0b013e318183a4a2
3. Legrand E, Bouvard B, Audran M, Fournier D, Valat JP. Sciatica from disk herniation: medical treatment or surgery? Joint Bone Spine. 2007;74(6):530–535. doi:10.1016/j.jbspin.2007.07.004
4. Vroomen PC, de Krom MC, Slofstra PD, Knottnerus JA. Conservative treatment of sciatica: a systematic review. Clin Spine Surgery. 2000;13(6):463–469.
5. Axén I, Leboeuf-Yde C. Trajectories of low back pain. Best Pract Res Clin Rheumatol. 2013;27(5):601–612. doi:10.1016/j.berh.2013.10.004
6. Qaseem A, Wilt TJ, McLean RM, Forciea MA. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166(7):514–530. doi:10.7326/M16-2367
7. Goo B, M-g J, Kim E-J, et al. Korean Medicine Clinical Practice Guidelines for Lumbar Herniated Intervertebral Disc in Adults: based on Grading of Recommendations Assessment, Development and Evaluation (GRADE). MDPI. 2022;246.
8. Bernstein IA, Malik Q, Carville S, Ward S. Low back pain and sciatica: summary of NICE guidance. BMJ. 2017;356.
9. Stochkendahl MJ, Kjaer P, Hartvigsen J, et al. National Clinical Guidelines for non-surgical treatment of patients with recent onset low back pain or lumbar radiculopathy. Eur Spine J. 2018;27(1):60–75. doi:10.1007/s00586-017-5099-2
10. Lee J, Cho J-H, Kim K-W, et al. Chuna manual therapy vs usual care for patients with nonspecific chronic neck pain: a randomized clinical trial. JAMA network open. 2021;4(7):e2113757–e2113757. doi:10.1001/jamanetworkopen.2021.13757
11. Tang S, Mo Z, Zhang R. Acupuncture for lumbar disc herniation: a systematic review and meta-analysis. Acupuncture in Medicine. 2018;36(2):62–70. doi:10.1136/acupmed-2016-011332
12. Manchikanti L, Knezevic NN, Navani A, et al. Epidural interventions in the management of chronic spinal pain: American Society of Interventional Pain Physicians (ASIPP) comprehensive evidence-based guidelines. Pain Phys. 2021;24(S1):27.
13. Eworuke E, Crisafi L, Liao J, et al. Risk of serious spinal adverse events associated with epidural corticosteroid injections in the Medicare population. Reg Anesth Pain Med. 2021;46(3):203–209. doi:10.1136/rapm-2020-101778
14. Schneider B, Zheng P, Mattie R, Kennedy DJ. Safety of epidural steroid injections. Expert Opin Drug Saf. 2016;15(8):1031–1039. doi:10.1080/14740338.2016.1184246
15. El-Yahchouchi CA, Plastaras CT, Maus TP, et al. Adverse event rates associated with transforaminal and interlaminar epidural steroid injections: a multi-institutional study. Pain Med. 2016;17(2):239–247. doi:10.1111/pme.12896
16. Chou R. Pharmacological management of low back pain. Drugs. 2010;70:387–402. doi:10.2165/11318690-000000000-00000
17. de Campos TF. Low back pain and sciatica in over 16s: assessment and management NICE Guideline [NG59]. J Physiother. 2017;63(2):120. doi:10.1016/j.jphys.2017.02.012
18. Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368–2383. doi:10.1016/S0140-6736(18)30489-6
19. Chou R, Deyo R, Friedly J. Noninvasive Treatments for Low Back Pain. Comparative Effectiveness Review. Prepared Pacific Northwest Evidence Based Practice Center Under Contract. 2016:57.
20. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain—United States, 2016. JAMA. 2016;315(15):1624–1645. doi:10.1001/jama.2016.1464
21. Health NIf, Excellence C. Neuropathic pain in adults: pharmacological management in non-specialist settings (clinical guideline CG173); 2019.
22. Deyo RA, Von Korff M, Duhrkoop D. Opioids for low back pain. BMJ. 2015:4;350.
23. Martell BA, o’Connor PG, Kerns RD, et al. Systematic review: opioid treatment for chronic back pain: prevalence, efficacy, and association with addiction. Ann Intern Med. 2007;146(2):116–127. doi:10.7326/0003-4819-146-2-200701160-00006
24. Ahn Y-J, Shin J-S, Lee J, et al. Evaluation of use and cost of medical care of common lumbar disorders in Korea: cross-sectional study of Korean Health Insurance Review and Assessment Service National Patient Sample data. BMJ open. 2016;6(9):e012432. doi:10.1136/bmjopen-2016-012432
25. National Evidence-based Healthcare Collaborating Agency. 요통에 대한 주사치료의 임상적 효과. [Clinical effectiveness of injection therapy for low back pain]; 2010. Available from: https://www.neca.re.kr/SKIN_DIR/doc.html?fn=7960020130215112452.pdf&rs=/upload/synap/202308/.
26. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: visual analog scale for pain (vas pain), numeric rating scale for pain (nrs pain), mcgill pain questionnaire (mpq), short‐form mcgill pain questionnaire (sf‐mpq), chronic pain grade scale (cpgs), short form‐36 bodily pain scale (sf‐36 bps), and measure of intermittent and constant osteoarthritis pain (icoap). Arthritis Care Res. 2011;63(S11):S240–S252.
27. Karcioglu O, Topacoglu H, Dikme O, Dikme O. A systematic review of the pain scales in adults: which to use? Am J Emerg Med. 2018;36(4):707–714. doi:10.1016/j.ajem.2018.01.008
28. Jeon C-H, Kim D-J, Kim D-J, Lee H-M, Park H-J. Cross-cultural adaptation of the Korean version of the Oswestry Disability Index (ODI). J Korean Society Spine Surgery. 2005;12(2):146–152. doi:10.4184/jkss.2005.12.2.146
29. Kim D-Y, Lee S-H, Lee H-Y, et al. Validation of the Korean version of the Oswestry disability index. Spine. 2005;30(5):E123–E127. doi:10.1097/01.brs.0000157172.00635.3a
30. Cha Y-J, Kim K. Reliability and validity of the Korean version of the fear of daily activities questionnaire for patients with low back pain. J Korea Contents Assoc. 2011;11(5):224–232. doi:10.5392/JKCA.2011.11.5.224
31. Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113(1–2):9–19. doi:10.1016/j.pain.2004.09.012
32. Dworkin RH, Turk DC, Wyrwich KW, et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. j Pain. 2008;9(2):105–121. doi:10.1016/j.jpain.2007.09.005
33. Kim S-H, M-W J, Ahn J, Ock M, Shin S, Park J. Assessment of psychometric properties of the Korean SF-12 v2 in the general population. BMC Public Health. 2014;14(1):1–7. doi:10.1186/1471-2458-14-1086
34. Kim L, Kim J-A, Kim S. A guide for the utilization of health insurance review and assessment service national patient samples. Epidemiol Health. 2014;36:e2014008. doi:10.4178/epih/e2014008
35. Ministry of Employment and Labor. 2019. 년 고용형태별근로실태조사 보고서 [2019 Survey Report on Labor Conditions by Employment Type]. Available from: http://laborstat.moel.go.kr/lsm/bbs/selectBbsList.do?bbsYn=Y?answerSn=0&bbsId=LSS108&bbsSn=0&leftMenuId=0010001100116&menuId=0010001100116115&pageIndex=1&searchCtgryCode=004&subCtgryCode=004.
36. Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics. 1993;4(5):353–365. doi:10.2165/00019053-199304050-00006
37. Prasad M, Wahlqvist P, Shikiar R, Shih Y-CT. A review of self-report instruments measuring health-related work productivity. Pharmacoeconomics. 2004;22(4):225–244. doi:10.2165/00019053-200422040-00002
38. DOMINGUES RB, PICON IS, VESCOVi J, et al. Assessment of Work Productivity and Activity Impairment (WPAI) questionnaire for migraine with the help of a smartphone app. Arq Neuropsiquiatr. 2020;78(8):468–472. doi:10.1590/0004-282x20200004
39. Woori bank. Available from: https://spot.wooribank.com/pot/Dream?withyou=FXXRT0016.
40. Julious SA. Sample size of 12 per group rule of thumb for a pilot study. Pharm Statistics. 2005;4(4):287–291. doi:10.1002/pst.185
41. National Evidence-based Healthcare Collaborating Agency. 의료 의사결정의 비용-효용성에 관한 아시아 공동 연구 [A Joint Asian Study on Cost-Utility in Healthcare Decision-Making]; 2012. https://www.neca.re.kr/SKIN_DIR/doc.html?fn=8382720130701160912.pdf&rs=/upload/synap/202309/.
42. Hägg O, Fritzell P, Nordwall A. The clinical importance of changes in outcome scores after treatment for chronic low back pain. Eur Spine J. 2003;12(1):12–20. doi:10.1007/s00586-002-0464-0
43. Lauridsen HH, Hartvigsen J, Manniche C, Korsholm L, Grunnet-Nilsson N. Responsiveness and minimal clinically important difference for pain and disability instruments in low back pain patients. BMC Musculoskelet Disord. 2006;7(1):1–16. doi:10.1186/1471-2474-7-82
44. Copay AG, Glassman SD, Subach BR, Berven S, Schuler TC, Carreon LY. Minimum clinically important difference in lumbar spine surgery patients: a choice of methods using the Oswestry Disability Index, Medical Outcomes Study questionnaire Short Form 36, and pain scales. Spine J. 2008;8(6):968–974. doi:10.1016/j.spinee.2007.11.006
45. Carreon LY, Bratcher KR, Canan CE, Burke LO, Djurasovic M, Glassman SD. Differentiating minimum clinically important difference for primary and revision lumbar fusion surgeries. J Neurosurg Spine. 2013;18(1):102–106. doi:10.3171/2012.10.SPINE12727
46. Grönblad M, Hupli M, Wennerstrand P, et al. Intercorrelation and test-retest reliability of the Pain Disability Index (PDI) and the Oswestry Disability Questionnaire (ODQ) and their correlation with pain intensity in low back pain patients. Clin J Pain. 1993;9(3):189–195. doi:10.1097/00002508-199309000-00006
47. Kovacs FM, Abraira V, Zamora J, et al. Correlation between pain, disability, and quality of life in patients with common low back pain. Spine. 2004;29(2):206–210. doi:10.1097/01.Brs.0000107235.47465.08
48. Snelgrove S, Liossi C. Living with chronic low back pain: a metasynthesis of qualitative research. Chronic Illn. 2013;9(4):283–301. doi:10.1177/1742395313476901
49. Husky MM, Ferdous Farin F, Compagnone P, Fermanian C, Kovess-Masfety V. Chronic back pain and its association with quality of life in a large French population survey. Health Qual Life Outcomes. 2018;16(1):195. doi:10.1186/s12955-018-1018-4
50. Wood-Dauphinee SL. Assessment of back-related quality of life: the continuing challenge. Spine. 2001;26(8):857–861. doi:10.1097/00007632-200104150-00005
51. Woodcock J. A difficult balance--pain management, drug safety, and the FDA. N Engl J Med. 2009;361(22):2105–2107. doi:10.1056/NEJMp0908913
52. Carter GT, Duong V, Ho S, Ngo KC, Greer CL, Weeks DL. Side effects of commonly prescribed analgesic medications. Phys Med Rehabil Clin N Am. 2014;25(2):457–470. doi:10.1016/j.pmr.2014.01.007
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Druggable Genome-Wide Mendelian Randomization Identifies Distinct Therapeutic Targets for Low Back Pain, Intervertebral Disk Degeneration, and Sciatica
Sun A, Li Z, Du Y, Liu H, Zhan Q, Liu Z
Journal of Pain Research 2025, 18:5769-5780
Published Date: 4 November 2025
Non-Pharmacological and Pharmacological Treatments for Non-Acute Lumbar Disc Herniation: A Protocol for a Multicenter Pragmatic Trial
Kim D, Lee YJ, Yang C, Ahn YJ, Kim S, Lee Y, Cho HW, Han CH, Ha IH
Journal of Pain Research 2025, 18:7167-7178
Published Date: 26 December 2025