Back to Journals » Patient Preference and Adherence » Volume 16
Satisfaction and Adherence of COPD Patients to a Conventional Training Associated with Functional Exercises and to a Conventional Training Isolated: A Qualiquantitative Study
Authors Grigoletto I ![]() , de Lima FF
, de Lima FF ![]() , Eto DA, Suzuki NNV, Uzeloto JS, Ramos EMC
, Eto DA, Suzuki NNV, Uzeloto JS, Ramos EMC
Received 7 April 2022
Accepted for publication 2 August 2022
Published 11 October 2022 Volume 2022:16 Pages 2759—2772
DOI https://doi.org/10.2147/PPA.S367088
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Naifeng Liu
Isis Grigoletto,1 Fabiano Francisco de Lima,2 Daniele Akemi Eto,1 Natália Narumi Voltareli Suzuki,1 Juliana Souza Uzeloto,1 Ercy Mara Cipulo Ramos1
1Department of Physical Therapy, São Paulo State University (UNESP), Faculty of Science and Technology, Presidente Prudente, São Paulo, Brazil; 2Department of Physical Therapy, Speech and Occupational Therapy, School of Medicine, University of São Paulo (USP), São Paulo, São Paulo, Brazil
Correspondence: Isis Grigoletto, Department of Physical Therapy, São Paulo State University (UNESP), Faculty of Science and Technology, 305, Roberto Simonsen St, Presidente Prudente, SP, 19060-900, Brazil, Tel +55 18 3229 5821, Email [email protected]
Purpose: To verify, through quali-quantitative analysis, the satisfaction and adherence of patients with Chronic Obstructive Pulmonary Disease (COPD) to the insertion of functional circuit training into conventional training.
Patients and Methods: 23 patients with COPD from a randomized clinical trial were invited to participate in a quali-quantitative analysis after the training finalization, divided into FTG (Functional Training Group) and CTG (Conventional Training Group). A total of 21 patients participated [(FTG: n=10; 65.80± 7.31 years; FEV1/FVC: 56.44± 12.67%) and CTG (n=11; 70.36± 7.02 years; FEV1/FVC: 55.89± 8.20)]. For the qualitative evaluation, focus groups were performed, using a previously developed script. Adherence was verified by the presence in the training sessions that were prescribed, and the quantitative analysis was performed using questionnaires with multiple-choice questions (evaluation of the aspects that can interfere in a training). The participants were asked to define a grade between zero and ten regarding the aspects of the training (satisfaction).
Results: In both groups, there was similar adherence (p=0.965) and satisfaction (p=0.341). The qualitative analysis identified seven themes and 17 codes, representing factors related to satisfaction and negative aspects, as follows: factors associated with satisfaction: self-efficacy management, physical and psychosocial improvement, interpersonal relationships, and proposed exercises. Negative aspects: pains, comorbidities, beliefs, and personal demotivation. In the quantitative analysis, was verified that an increase in the symptoms, the distance between home and training center, and personal problems were not factors that interfered in the adherence of the participants (p< 0.05).
Conclusion: Similar satisfaction and adherence of patients with COPD were observed in the FTG and CTG and patients from FTG reported higher fatigue.
Keywords: Chronic Obstructive Pulmonary Disease, physical exercise, patient satisfaction, patient adherence, qualitative research, quantitative evaluation
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is characterized by airflow limitation, respiratory symptoms,1 functional limitations,2 and associated comorbidities.1 According to the World Health Organization (WHO), by 2030, COPD will be the third cause of death in the world.3
The need to insert patients with COPD into a Pulmonary Rehabilitation Program (PRP) to control the disease and improve or maintain their clinical status is well defined in the literature.4–6 Further, PRPs have several interventions and one of them is physical exercise, considered grade “A” evidence in the treatment of these patients.7 Aerobic and resistance training (conventional training) are conventional modalities of physical training used in PRPs,2,8,9 that increase muscle strength, functional capacity, quality of life, and reduce dyspnea.4–6
Even though the benefits of physical training during PRP for COPD patients,5,9 the adherence and conclusion rate of these programs are still poor.10,11 Due to that, several qualitative and quantitative studies have sought to understand the reasons for these facts, some of which are personal compromises, and changes in routine and work.12,13 Studies have shown that body mobility limitation14 and the monotony of the PRPs15 are barriers to adherence, which are associated with exercise intolerance, which can influence negatively the treatment adhesion.10,12,13,15
Functional exercise is considered a modality of exercise that includes muscle work and coordinated multi-joint movements with dynamic exercises, simulating routine activities.16 Preview study showed that functional exercises promote functional benefits to COPD.17,18 Sewell et al performed a physical training program composed of aerobic and home training associated with functional exercises, which promoted physical benefits to COPD patients. Although, no adherence analysis was performed.18
Hence, considering that functional exercise is a different modality that simulates routine activities (eg: simulating drying the back, sweeping the floor, and tying a shoe), is more dynamic than the conventional ones (aerobic training in cycle ergometers and static strength exercises),18 and that exercise programs with multiple modalities can produce higher adherence than programs with poor exercises varieties,19 the functional training associated to the conventional training could be an alternative to improve treatment adherence to the physical training in patients with COPD.
Also considering that functional exercises in a circuit format can promote an increase in muscle strength,20 functional capacity,18 and quality of life,17,18 this may be an interesting and viable alternative to the cited problems.
Qualitative analysis, searching for attitudes related to human behavior, demonstrates that the investigation of satisfaction with the subject’s treatment is extremely important,21 not only investigating the disease, but searching for the meaning for these patients, and their characteristics and way of living, in all contexts.22
Quantitative studies differ from qualitative regarding the methodology to data collection and the analysis and interpretation of the variables.23 While quantitative data is submitted to multivariate analysis and techniques for statistical predictions, qualitative studies promote deep participation of the participants that consequently produce a specific knowledge related to these individuals’ experiences, which can be an important key to understanding their feelings and beliefs about a specific treatment program.23
Thus, from this analysis, we could understand the factors involved in the process of disease acceptance to the proposed treatment, making it possible to develop new strategies to improve adherence and satisfaction. Therefore, the present study aimed to verify the satisfaction and adherence of patients with COPD to the insertion of a functional circuit into conventional training and compare this with isolated conventional training.
Materials and Methods
Sample Selection
This study is a secondary analysis composed of a convenience sample from a prior randomized clinical trial (RCT).24 From July 2018 to January 2020, patients with COPD were recruited to participate in physical training to decrease their disease symptoms, through invitations at doctor’s offices, health centers, and hospitals. The inclusion criteria of this study were: (1) patients with COPD diagnosed according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD); (2) clinically stable patients without exacerbations or changes in medications for at least 30 days; (3) patients who did not use long-term oxygen therapy at home; (4) patients without pathological conditions that prevented the performance of physical activity; (5) absence of severe or unstable heart disease and (6) patients that did not have been included in another structured exercise program.
After agreeing to participate, the patients were randomized into training groups. Thirty-five patients with COPD were randomized into: Functional Training Group (FTG) [11 patients], Conventional Training Group (CTG) [12 patients], and Usual Care Group (UCG) [12 patients]. Twenty-three patients from this randomized clinical trial were invited to participate in qualitative and quantitative analysis (only patients from FTG and CTG - because this qualitative study is a secondary analysis that was restricted only to verify and compare the satisfaction and adherence of the exercise training groups).
Twenty-one of these patients participated in the present study, which consisted of focus groups (FTG: 10 patients and CTG: 11 patients) to collect the qualitative data and questionnaires to collect the quantitative data. All patients of these training (FTG and CTG) were invited to participate in these evaluations, only one patient of FTG did not perform the quali-quantitative evaluation due to personal problems, and all patients of CTG participated.
The randomized allocation sequence of the RCT related to this study was performed by a researcher who was not involved in the recruitment, evaluation, or patient training. An online platform (www.sealedenvelope.com) and concealed brown envelopes were used. The randomization process was carried out in blocks defined a priori. Evaluators were blinded to the allocation of participants to interventions. The training was supervised by trained physiotherapists not involved in the randomization process or evaluations. In the qualitative and quantitative evaluation, the moderator was blinded to the participants’ training allocation.
The sample size of the RCT was determined based on a prior study, based on the primary physical activity of daily life variable. Considering this variable, the sample size was 25 individuals in each group.24 Nonetheless, it is reasonable to reinforce that the present study is a secondary analysis with a convenient sample of this study.24
This work complies with the Declaration of Helsinki and was approved by the Research Ethics Committee of the Faculty of Sciences and Technology of UNESP, Campus of Presidente Prudente, SP, Brazil (CAAE: 77909317.2.0000.5402) and the patients signed the Consent Form. This study was registered at ensaiosclinicos.gov.br (ID: RBR-3zmh3r).
Training Groups
The FTG performed 24 sessions of aerobic and resistance training combined with a functional circuit (Supplementary Material - Circuit of functional exercises), and the CTG performed 24 sessions of aerobic and resistance training. UCG performed only conventional respiratory physiotherapy. All the training sessions were conducted by physiotherapists with experience in COPD physical training. The training protocol was previously published elsewhere.24
The patients performed aerobic training on a treadmill (Movement LX170/LX 3.0, Brazil) for 30 minutes, with the prescription determined by the Six-Minute Walk Test (6MWT).25,26 The initial intensity of the training was defined as 80% of the speed achieved in the 6MWT.5 The patients were required to maintain their dyspnea between values four and six (moderate intensity) on a Borg Scale4 during the training.27 If the values on the Borg Scale were less than four, a 5% increase in training intensity was applied in the next session.
In the resistance training, conventional weight machines (Ipiranga, Brazil) were used, and knee flexion and extension and elbow flexion were performed. The load prescription was defined according to the One Maximum Repetition Test (1MR).28,29 The training intensity was between 60% and 80% of the 1MR test, with three series of 10 repetitions, and an increase of 5% in the load for every four sessions performed.4 This training was carried out according to the recommended protocol for COPD.4
In the functional training, patients performed the conventional training (aerobic and resistance combined) and functional exercises in a circuit form, that simulated the Activities of Daily Living (Supplementary material- Circuit of functional exercises), which were developed according to prior identification of the main routine activities are limited in patients with COPD (to this identification, patients not related to this study were interviewed). The patients were required to perform each exercise for two minutes and thirty seconds and maintain their dyspnea between four and six on the Borg Scale.4 If the values were less than four, the patients were asked to increase the exercise speed and if the values were above six, they were asked to decrease the speed. Sticks, balls, chairs, cones, hula hoops, stairs, and ramps were used for this training. In general, the functional exercises simulated the following tasks: drying the back; sweeping the floor; tying a shoe; passing a squeegee on the floor; picking up objects in high and low places; squatting; walking on uneven ground using ramps and stairs; standing up and sitting in a chair; changing clothes; simulate the avoidance of obstacles during gait and picking up objects. The functional exercises are present in more detail in the supplementary material - Circuit of functional exercises.
The training program lasted eight weeks, three times per week, with a session duration of 60 minutes. Global stretches were performed before each session. The CTG performed aerobic and resistance training in three sessions per week and the FTG performed aerobic and resistance training in two sessions per week and functional and resistance training in one session.
Adherence Evaluation
To evaluate adherence, each individual’s presence in the sessions was counted. Adherence was determined as the presence in six weeks of training, in other words, 18 sessions, this number has been defined as necessary to represent adherence to treatment in patients with COPD by a previous guideline.30 We also assigned an adherence score to each individual based on the proportion of attending sessions that were prescribed: high adherence (>85% of the prescribed sessions), moderate adherence (35–85% of the prescribed sessions), and low adherence (<35% of the prescribed sessions), according to Oates et al.31
Qualitative Evaluation
After the finalization of the training groups, the patients were invited to participate in a focal group to collect qualitative and quantitative data. Focus groups were conducted by a researcher using a previously developed script, with open questions (Supplementary material - Qualitative evaluation questions). The moderator was female, a Ph.D. student, with previous experience in physical training and qualitative research. A second researcher was present in the focus groups to detail notes of the participant’s answers. The patients had previous contact with the moderator and before participation, all patients were informed about the aims of the study and how it would be accomplished.32,33
The focus groups were performed in a classroom at the university where the research was conducted. The focal group meetings were recorded using a recording device (OLYMPUS / VN-8100PC, Tokyo, Japan) and transcribed verbatim.
Figure 1 presents the flowchart of the study.
 |
Figure 1 Flowchart of the study. Abbreviations: FTG, Functional Training Group; CTG, Conventional Training Group. |
Following the methods for qualitative studies that allow a limited number of patients in a focus group,32,33 the patients in this study were divided into four focus groups. Four patients from the FTG participated in the first focus group of the FTG evaluation, and five from the CTG participated in the first focal group of the CTG evaluation. After that, another six patients from the FTG participated in another focus group to qualitatively evaluate the functional training associated with the conventional training and six from the CTG participated in a focus group to evaluate the conventional training isolated. The data were collected until no new information was obtained (saturation point).32,33
Quantitative Evaluation
After the finalization of the focus groups, participants answered a quantitative questionnaire (developed by the authors) with multiple-choice questions, related to reasons to seek medical assistance, which medical specialist sought, and possible reasons that interfered with attendance at training sessions. This questionnaire was developed by the researchers based on previous qualitative studies related to patients’ satisfaction and adherence to pulmonary rehabilitation programs,11,34 in other words, was developed and applied based on a preview of patients’ beliefs and experiences in pulmonary rehabilitation. In that way, we formulated these multiple-choice questions only to understand our patients’ profiles and to verify if the aspects presented in these questionnaires were relevant to them.
Participants were asked to define a grade between 0 (zero) and 10 (ten) related to training aspects, such as structure offered, relationship with the therapists, training offered, materials used, the process of evaluation, and general satisfaction.
Analysis of Qualitative and Quantitative Data
Qualitative data were analyzed using content analysis, related to a systematic analysis of the description of the phenomena, which allows researchers to improve their understanding of the data, by refining words into fewer categories related to the content obtained in the focus groups.35
The transcriptions of the focus groups were analyzed by three independent researchers who identified and classified categories related to the research question. The analysis was developed by the categorization, organization, and compaction of the data. After this analysis a triangulation was performed, which consisted of a discussion about the differences in the results, to reach a consensus, identifying themes which include the codes (demonstrate the main points reported by the patients). Subsequently, the results were forwarded to 10% of the participants to confirm whether the results were following the focus groups, and the patients confirmed this. The focus groups ranged from 16 to 51 minutes.
For quantitative data analysis, we used the Shapiro–Wilk test to verify the normality of data, the Student t test for independent data to compare the groups regarding the continuous data (data expressed as mean and standard deviation), and the Chi-square test for categorical data analysis (data expressed in absolute numbers). The statistical software SPSS 23.0 version was used, and the level of significance was set at 5%.
Results
In total, 21 patients participated in the evaluation process: FTG [n=10 (6 men)] and CTG [n=11 (6 men)]. Table 1 shows the anthropometric and spirometric characteristics of the groups, the data are expressed as mean and standard deviation. The mean presence of the patients in the sessions was 19 sessions (79.16%) in both groups. Seventy percent of the patients from the FTG presented moderate adherence and 30% of the patients presented high adherence. While the patients from the CTG presented 72% of moderate adherence and 27% of high adherence.
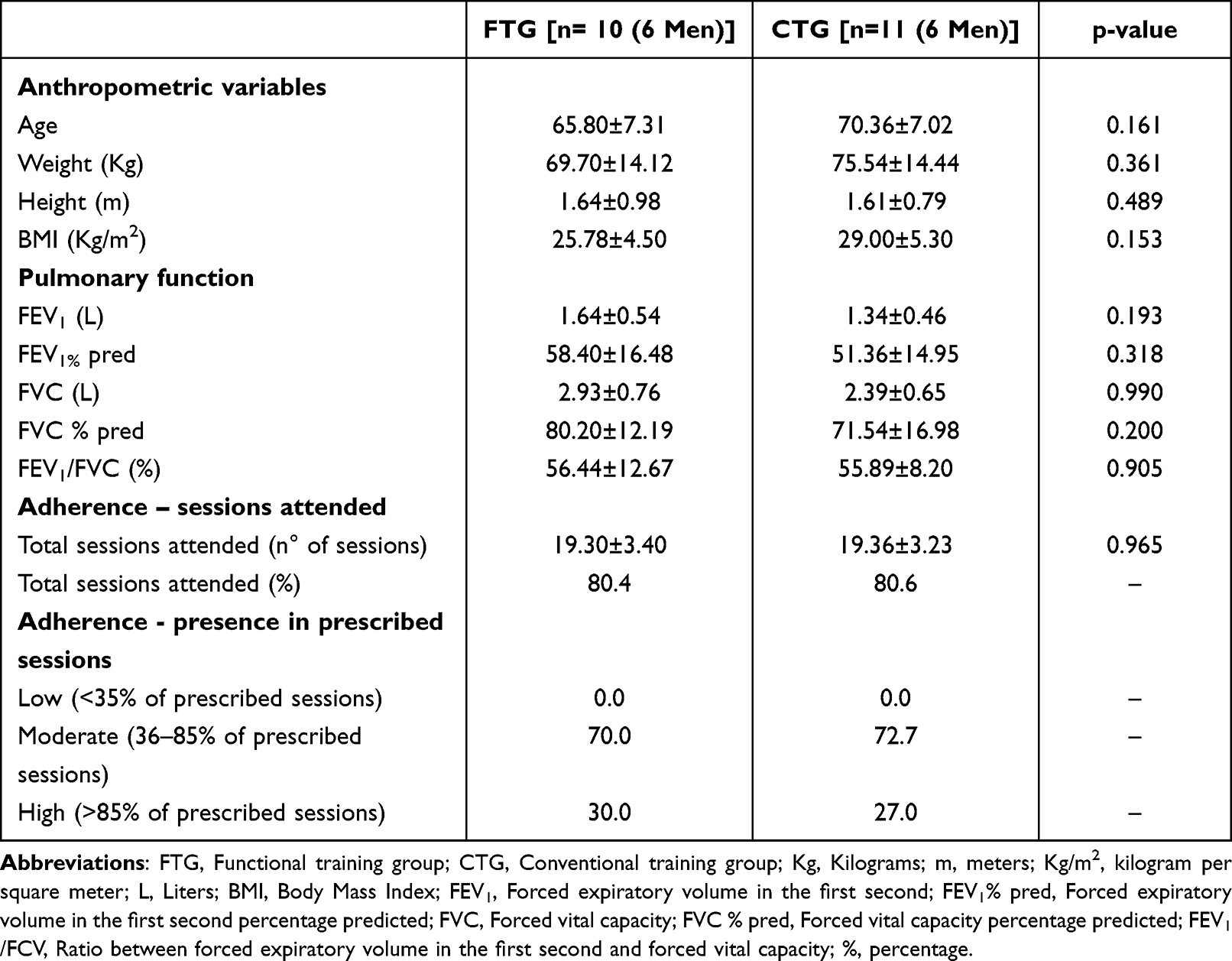 |
Table 1 Anthropometric and Spirometric Characteristics of the Groups. Data Expressed as Mean and ± Standard Deviation or in Percentage (%) |
Table 2 shows each question and answer on the quantitative questionnaire, with questions related to the specialty sought and possible reasons that interfered with attendance at training sessions, also it is possible to verify the number of patients that answered each question in both groups.
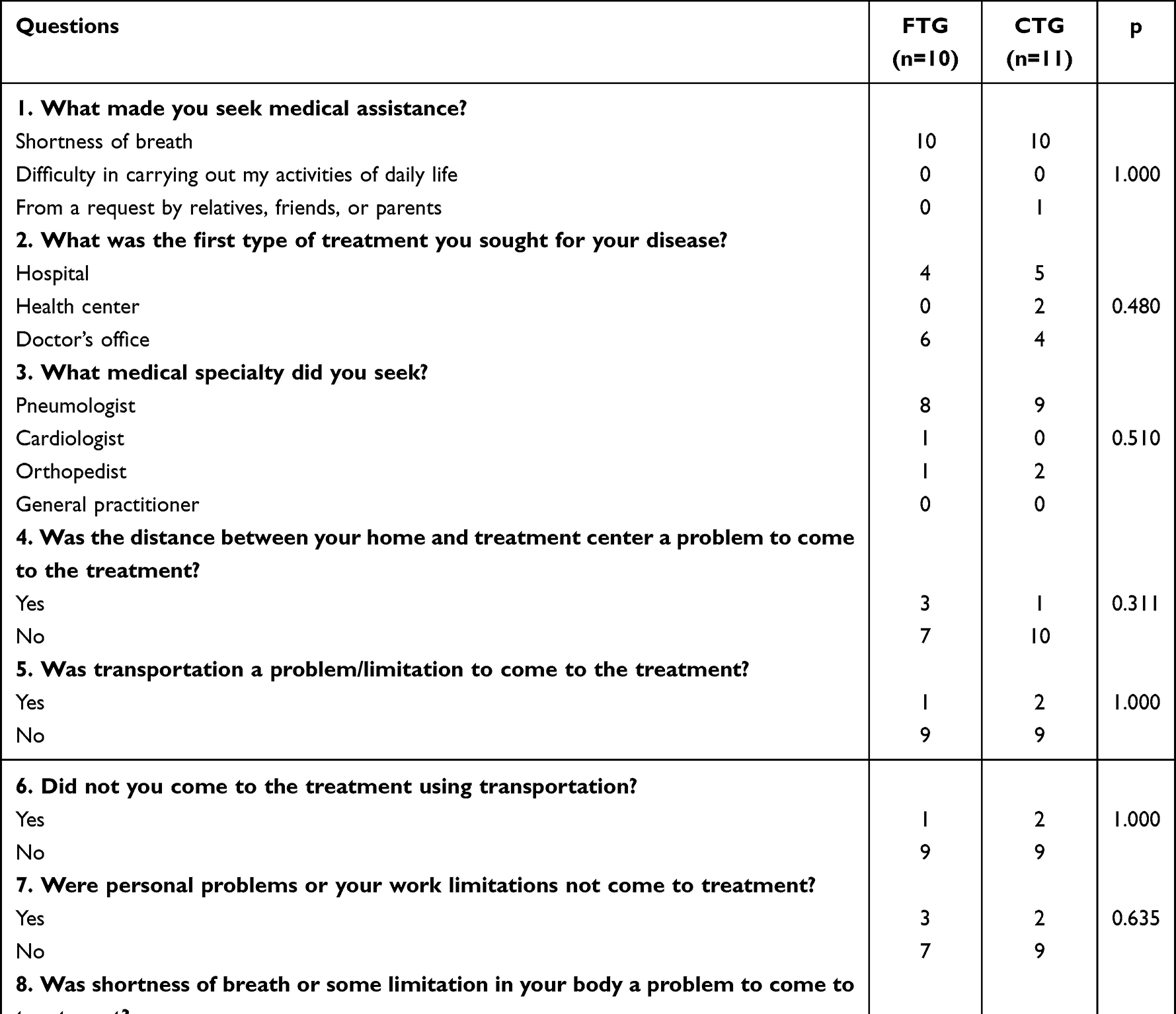 |
Table 2 Subjects’ Answers to Quantitative Questionnaire |
Table 2 shows there were no statistical differences between groups. The majority of the patients sought medical assistance due to shortness of breath, at a doctor’s office or hospital with a pneumology specialist. Furthermore, the distance between home and the treatment center, transportation, problems related to an increase in respiratory symptoms, and personal problems were not limiting factors to attending the treatment.
Figure 2 presents the grades defined concerning training aspects, with no statistical differences between groups (FTG and CTG): structure offered (p=0.439), relationship with the therapists (p=1.000), training offered (p=0.19), materials used (p=0.90), the process of evaluation (p=0.614), and general satisfaction with the training offered (p=0.341). The grades are expressed as median.
 |
Figure 2 Quantitative analysis of satisfaction of the subjects with the training. Abbreviations: FTG, Functional Training Group; CTG, Conventional Training Group. |
Qualitative analysis identified seven themes according to the codifications: 1) “knowledge about the disease and treatments”; 2) “perceived benefits from the treatment”; 3) “satisfaction with the treatment”; 4) “complications during the treatment”; 5) “suggestions”; 6) “possible reasons to leave the treatment”; 7) “perceptions during the treatment”.
Theme 1 - Knowledge About the Disease and Treatments
This theme contains all information obtained about the patients’ prior knowledge of the diseases before beginning the treatment. The transcription demonstrates that patients did not have previous knowledge about the available treatments for disease management and they started to gain this after the therapist’s knowledge transmission (Code 1). They learned to control the disease symptoms, such as dyspnea (Code 2).
Theme 2 - Perceived Benefits from the Treatment
This theme is related to patients’ perceptions about improvements in physical (Code 1) and psychosocial aspects (Code 2). The patients reported benefits from the treatment, such as improvement in physical aspects, decrease in dyspnea, improved quality of sleep, and daily activities of life, such as taking a bath, walking, and cleaning the house. Further, they reported improvements in psychosocial aspects, such as decreased anxiety and distress due to the disease.
Theme 3 - Satisfaction with the Treatment
In this theme, the reports related to the proposal of exercise type (Code 1), the relationship between COPD patients (Code 2), and therapists (Code 3) during the treatment, the desire for continuity in treatment (Code 4), and treatment indication to other patients (Code 5), were considered for satisfaction with the proposed treatment. The reports on this theme demonstrated general satisfaction with the offered treatment. Regarding the proposed exercises, the CTG showed great satisfaction with the treadmill in aerobic training, while the FTG patients (seven patients) reported more fatigue during the functional circuit training when compared to aerobic and resistance training. The relationship between patients and therapists, the opportunity of creating new friendships with patients with the same disease, and the therapist’s attention and concern for them were reported by patients.
Theme 4 - Complications During Treatment
This theme contains information related to complications during the training (Code 1). Comorbidities, such as heart and orthopedic problems were reported.
Theme 5 - Suggestions
Questions related to patient suggestions to improve the training, such as altering the intensity (Code 1) and frequency of training (Code 2) are in this theme. The patients suggested alterations in training intensity and frequency. The CTG suggested that the intensity and repetitions in the resistance training could be higher. The FTG reported that the session frequency was adequate.
Theme 6 - Possible Reasons to Leave the Treatment
This theme contains information related to possible reasons that interfere with attendance for treatment, such as health complications during the treatment (Code 1), beliefs (Code 2), and personal motivation (Code 3). A couple of patients reported difficulty in the exercises due to previous disease pain, these were determined as health complications. The beliefs, like being scared of performing the exercises on the treadmill and fear of the health professionals wearing white clothes were reported as possible reasons to leave the treatment.
Theme 7 - Perceptions During the Treatment
Finally, this theme presents information about the patients’ positive (Code 1) and negative impressions (Code 2) during the training. In the CTG the patients reported they liked the proposed exercises, as positive perceptions. In the FTG one subject reported the functional circuit was good due to their high blood pressure and dyspnea during aerobic training as in the functional training their blood pressure was lower.
Regarding negative perceptions, the CTG patients reported high fatigue on the treadmill. In the FTG, the majority of the patients affirmed that some functional exercises were difficult to perform, due to fatigue and dyspnea, such as exercises that simulated “tying shoes” and “getting dressed”.
The themes, codes, and transcriptions are presented below in Table 3.
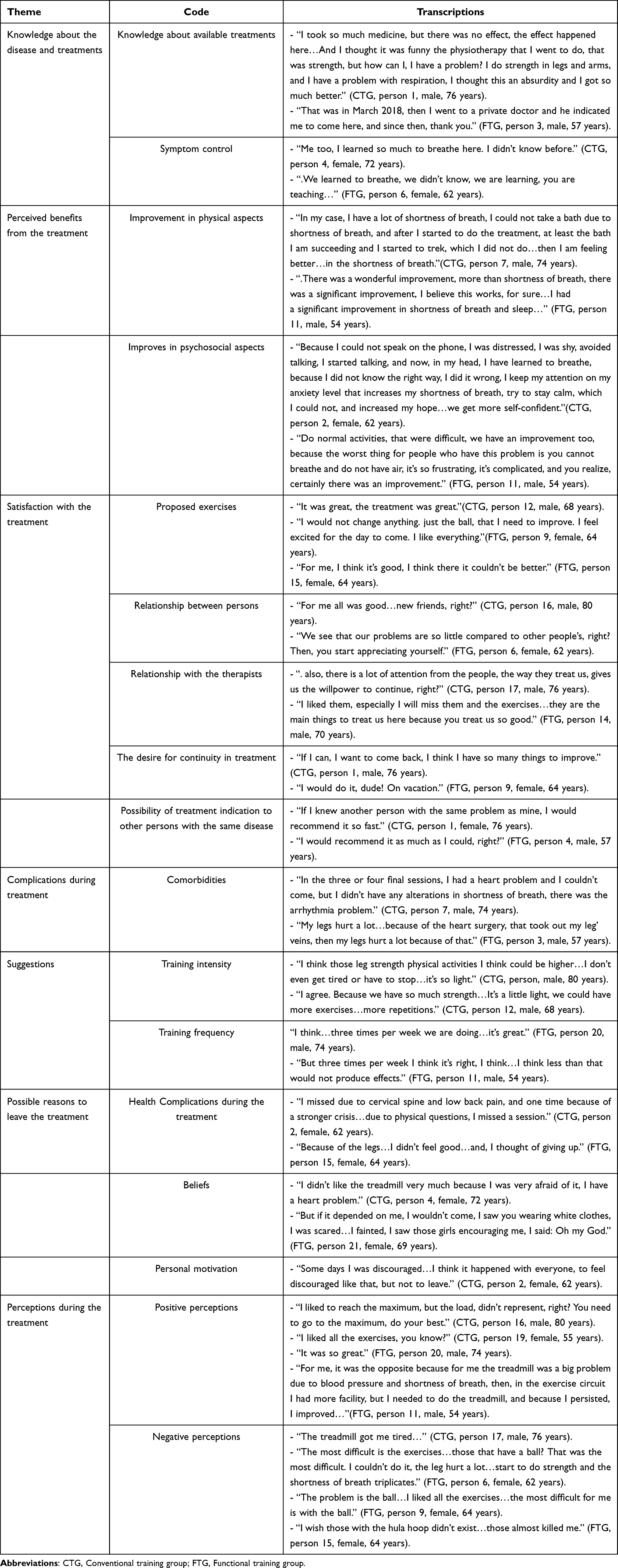 |
Table 3 Themes, Codes, and Transcriptions Were Obtained from Focus Groups |
Discussion
The addition of circuit training to conventional training (aerobic and resistance combined) led to great satisfaction and adherence of COPD patients, in the same way as the isolated conventional training. Patients from the functional training associated with the conventional training experienced more fatigue than the patients submitted to the conventional training isolated. Also, the following positive factors related to satisfaction, such as learning about disease management, improvement in physical and psychosocial conditions, the possibility of interpersonal relationships, and some details of the proposed exercises were reported. Although, negative aspects such as pain, comorbidities, beliefs, and personal motivation were also pointed out.
Both groups adhered to the training, considering that the FTG and the CTG had an average presence of 19 sessions and that the patients from these groups had moderate adherence (>70% of the patients attended the prescribed sessions) and high adherence (>27% of the patients attended the prescribed sessions) we can affirm that both training had a great influence on the adherence to the treatment. Great adherence to physical training programs is extremely important to this population, that can experience beneficial gains in exercise training programs.30,31
Conventional training is commonly prescribed in patients with COPD, considering the benefits obtained, such as improvement in dyspnea, functional capacity, routine activities, and quality of life.4–6,33,36 These improvements were reported by patients in both groups, evidencing the satisfaction with the treatment. Psychosocial improvements, such as a reduction in anxiety levels, were perceived by patients as benefits obtained from the training.37
Complaints about the difficulty of disease management are common in patients with COPD, especially dyspnea control.37 It is reasonable that patients with COPD started to deal with the disease with strategies learned during the treatment,34,35 considering that improvement in disease control leads to a better social life and quality of life.11 Which is following the reports of the patients in the present study since they mentioned improvement in disease control and how good this aspect was for them.
Interpersonal relationships were demonstrated as positive aspects by the patients in both training groups. This is a factor that can influence the adherence and satisfaction of patients with COPD in a physical training program. Relationships between the patients with the same disease are considered a positive aspect, considering the complicity, sharing the same feelings, as well as the advice and reassurance among the patients,13,34 it is also a place to form new friendships. Moreover, the relationship with the therapists is a positive aspect reported by patients that positively influences satisfaction with treatment, considering demonstrations of confidence, support, and attention to the patients by the therapists.13,34,36,37
In the Desveaux et al study,30 the participants from physical training in a PRP demonstrated satisfaction with structured training programs, with adequate equipment that allowed the correct performance of the exercises,36 which is following reports of the patients in the present study, considering the satisfaction with the proposed exercises in both groups.
In the CTG, there was a preference for aerobic training, and the patients suggested that the resistance training intensity could be higher. Therefore, we suggest that the resistance training intensity may be higher than imposed in the present study (from 60% to 80% Maximum Repetition - MR) in samples with similar perceptions.
In the FTG, the patients reported high fatigue during functional exercises, this may be justified by the fact that functional exercises simultaneously work several body structures, promoting balance between the upper and lower parts of the limbs and trunk, and consequently better neuromuscular activation and higher musculoskeletal adaptation,38 as well as simulating routine activities,18 which the patients have difficulty performing due to the characteristics of the disease.39 In addition, the functional exercises were formulated by the most difficult activities to execute, reported by patients with COPD.
The exercises in the FTG that simulated “tying shoes” and “getting dressed” were considered very difficult to accomplish due to dyspnea. This may be explained by the fact that the exercise that simulates “tying shoes” leads to shallow, rapid, and irregular breathing with lower values of oxygen saturation.40 In addition, the exercise that simulates “getting dressed” promotes higher minute ventilation and, consequently, a decrease in oxygen saturation and hypoxemia, which could explain the increase in dyspnea during these exercises.41 These results are following another study, which verified that patients with COPD have difficulty in performing exercises that simulate daily activities with trunk flexion and movements with upper limbs.42
Pain during the exercises, such as fatigue after training, and associated comorbidities are negative aspects, considering factors that influence subject adherence43–45 and training satisfaction, bearing in mind that pain from prior conditions and associated comorbidities are factors that interfere in the participation of these patients in physical training.11,14,43 However, even though these are negative points, they did not interfere with the adherence and satisfaction of the patients with the training offered.
Previous studies have verified that questions related to personal demotivation create psychosocial barriers that interfere with the adherence of patients with COPD to physical training.43,44 In the present study this fact was reported by some patients with personal demotivation to attend the sessions. Besides this, the beliefs before the treatment, that the patients were not capable of performing the proposed exercises, are factors that may create negative influences. On the other hand, studies indicate that after starting physical training in PRP, patients become more confident and overcome their expectations related to prior beliefs.11,34 Therefore, since the satisfaction and adherence of patients to the training were similar between the groups, the insertion of a functional circuit into conventional training, could be an alternative form of training to perform routine activities, which the patients find difficult to execute.
As limitations of the present study, we can mention the fact that the patients who performed functional training were only submitted to conventional training in isolation, while the patients of the other group did not perform any session with functional exercises, thus, the patients did not experience both training types, and so, they could not perform comparisons between the training methods. Further, even though qualitative research generally has small sample sizes, we present the size of our sample and the time of the focus groups as possible limitations, which should be considered when our results would be translated into clinical practice. Added to that, despite that the questionnaire was developed by the research team based on previous studies,11,34 the questionnaire was not validated. Finally, the patient’s dropout can be considered a limitation of our study, although, it is reasonable to explain that many recruited patients had distance and transport difficulty to attend the spirometry evaluation, which made them decline to perform the spirometry.
As a suggestion to future studies, we highlight the possibility of COPD patients performing one or two sessions of a functional exercise program associated with conventional training and another day of only conventional training isolated, to verify the beliefs and satisfaction of the patients that experienced both training.
As clinical implications in this study, considering the satisfaction and adherence of the participants to this type of training, we mention the possibility of inserting a functional circuit associated with a conventional training into treatments for patients with COPD in outpatient clinics, rehabilitation centers, and hospitals, when the therapist aims to work on the execution of routine activities.
Conclusion
Patients with COPD presented great satisfaction and adherence to the insertion of a functional circuit into conventional training. Although the patients reported high fatigue during functional exercises, the satisfaction and adherence were similar to isolated conventional training.
Abbreviations
COPD, Chronic Obstructive Pulmonary Disease; FTG, Functional training group; CTG, Conventional training group; FEV1/FCV, Ratio between forced expiratory volume in the first second and forced vital capacity, WHO, World Health Organization; PRP, Pulmonary Rehabilitation Program; UCG, Usual Care Group; Kg, Kilogram; m, meters; Kg/m2, kilogram per square meter; L, Liters; BMI, Body Mass Index; FEV1, Forced expiratory volume in the first second; FEV1% pred, Forced expiratory volume in the first second percentage predicted; FVC, Forced vital capacity; FVC % pred, Forced vital capacity percentage predicted; MR, Maximum Repetition.
Data Sharing Statement
The datasets used and/or analyzed during the study are available from the corresponding author on reasonable request.
Acknowledgements
The authors would like to thank all the volunteers, São Paulo State University (UNESP) for allowing the development of this research. I.G; F.F.L and E.M.C.R were supported by: grant #2017/10925-2, grant #2017/10145-7 and #2018/18239-3, São Paulo Research Foundation (FAPESP) and the CAPES. This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Burki NK, Lee LY. Mechanisms of dyspnea. Chest. 2010;138(5):1196–1201. doi:10.1378/chest.10-0534
2. Lacasse Y, Martin S, Lasserson TJ, Goldstein RS. Meta-analysis of respiratory rehabilitation in chronic obstructive pulmonary disease. A Cochrane systematic review. Eura Medicophys. 2007;43(4):475–485.
3. World Health Organization; 2018 Chronic respiratory diseases. https://www.who.int/respiratory/copd/en/.
4. Garvey C, Bayles MP, Hamm LF, et al. Pulmonary rehabilitation exercise prescription in chronic obstructive pulmonary disease: review of selected guidelines: an official statement from the American association of cardiovascular and pulmonary rehabilitation. J Cardiopulm Rehabil Prev. 2016;36(2):75–83. doi:10.1097/HCR.0000000000000171
5. Maltais F, Decramer M, Casaburi R, et al. An official American Thoracic Society/European Respiratory Society statement: update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2014;189(9):e15–62. doi:10.1164/rccm.201402-0373ST
6. Leite MR, Ramos EM, Kalva-Filho CA, et al. Effects of 12 weeks of aerobic training on autonomic modulation, mucociliary clearance, and aerobic parameters in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:2549–2557. doi:10.2147/COPD.S81363
7. Barreiro E, Bustamante V, Cejudo P, et al. Guidelines for the evaluation and treatment of muscle dysfunction in patients with chronic obstructive pulmonary disease. Arch Bronconeumol. 2015;51(8):384–395. doi:10.1016/j.arbr.2015.04.027
8. Ries AL, Bauldoff GS, Carlin BW, et al. Pulmonary rehabilitation: joint ACCP/AACVPR evidence-based clinical practice guidelines. Chest. 2007;131(5 Suppl):4s–42s. doi:10.1378/chest.06-2418
9. Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–64. doi:10.1164/rccm.201309-1634ST
10. Jones AW, Taylor A, Gowler H, O’Kelly N, Ghosh S, Bridle C. Systematic review of interventions to improve patient uptake and completion of pulmonary rehabilitation in COPD. ERJ Open Res. 2017;3(1):1. doi:10.1183/23120541.00089-2016
11. Hayton C, Clark A, Olive S, et al. Barriers to pulmonary rehabilitation: characteristics that predict patient attendance and adherence. Respir Med. 2013;107(3):401–407. doi:10.1016/j.rmed.2012.11.016
12. Keating A, Lee A, Holland AE. What prevents people with chronic obstructive pulmonary disease from attending pulmonary rehabilitation? A systematic review. Chron Respir Dis. 2011;8(2):89–99. doi:10.1177/1479972310393756
13. Fischer MJ, Scharloo M, Abbink JJ, et al. Participation and drop-out in pulmonary rehabilitation: a qualitative analysis of the patient’s perspective. Clin Rehabil. 2007;21(3):212–221. doi:10.1177/0269215506070783
14. Keating A, Lee AL, Holland AE. Lack of perceived benefit and inadequate transport influence uptake and completion of pulmonary rehabilitation in people with chronic obstructive pulmonary disease: a qualitative study. J Physiother. 2011;57(3):183–190. doi:10.1016/S1836-9553(11)70040-6
15. Dourado VZ, Tanni SE, Antunes LC, et al. Effect of three exercise programs on patients with chronic obstructive pulmonary disease. Braz J Med Biol Res. 2009;42(3):263–271. doi:10.1590/S0100-879X2009000300007
16. Fragoso ACBL. A influência do treinamento funcional e core training na execução das atividades diárias de um grupo de indivíduos na cidade de Fraiburgo, SC. Unoesc Ciência ACBS. 2014;5(1):15–24.
17. Egan CDB, Blake C, Fullen BM, et al. Short term and long term effects of pulmonary rehabilitation on physical activity in COPD. Respir Med. 2012;106(12):1671–1679. doi:10.1016/j.rmed.2012.08.016
18. Sewell L, Singh SJ, Williams JEA, Collier R, Morgan MDL. Can individualized rehabilitation improve functional Independence in elderly patients with COPD? Chest. 2005;128(3):1194–1200. doi:10.1378/chest.128.3.1194
19. Sylvester BDSM, McEwan D, Wolf SA, et al. Variety support and exercise adherence behavior: experimental and mediating effects. J Behav Med. 2016;39(2):214–224. PMID: 26546241. doi:10.1007/s10865-015-9688-4
20. Kamahara K, Homma T, Naito A, et al. Circuit training for elderly patients with chronic obstructive pulmonary disease: a preliminary study. Arch Gerontol Geriatr. 2004;39(2):103–110. doi:10.1016/j.archger.2004.01.004
21. Green JTN. Qualitative Methods for Health Research. Vol. 3. London: Sage; 2004:26.
22. Pinto J, Martin-Nogueras AM, Morano MTA, TE Macedo, Arenillas JIC, Troosters T. Chronic obstructive pulmonary disease patients’experience with pulmonary rehabilitation: a systematic review of qualitative research. Chron Respir Dis. 2013;10(3):141–157. doi:10.1177/1479972313493796
23. Gemeda FT. The basis of distinction between qualitative and quantitative research in social science: reflection on ontological, epistemological and methodological perspectives. Ethip J Educ Sci. 2010;6(1):97–108.
24. de Lima FF, Camillo CA, Grigoletto I, et al. Effects of combining functional exercises with exercise training on daily physical activities and functionality in patients with COPD: a protocol for a randomized clinical trial. Trials. 2019;20(1):680. doi:10.1186/s13063-019-3780-y
25. Zainuldin R, Mackey MG, Alison JA. Prescription of walking exercise intensity from the 6-minute walk test in people with chronic obstructive pulmonary disease. J Cardiopulm Rehabil Prev. 2015;35(1):65–69. doi:10.1097/HCR.0000000000000074
26. Rodrigues A, Di Martino M, Nellessen AG, Hernandes NA, Neder JA, Pitta F. Is the six-minute walk test a useful tool to prescribe high-intensity exercise in patients with chronic obstructive pulmonary disease? Heart Lung. 2016;45(6):550–556. doi:10.1016/j.hrtlng.2016.08.005
27. Wen H, Gao Y, An JY, Chen QL, Zheng JP. [Evaluation of exercise intensity for pulmonary rehabilitation in patients with chronic obstructive pulmonary disease - 中重度慢性阻塞性肺疾病患者肺康复运动强度的评估]. Zhonghua Jie He He Hu Xi Za Zhi. 2007;30(1):27–30. Chinese.
28. Anunciação PG, Poton R, Szytko A, Polito MD. Comportamento cardiovascular após o exercício resistido realizado de diferentes formas e volumes de trabalho. Rev Bras Med Esporte. 2012;18(2):117–121. doi:10.1590/S1517-86922012000200011
29. Nicolino J, Ramos D, Leite MR, et al. Analysis of autonomic modulation after an acute session of resistance exercise at different intensities in chronic obstructive pulmonary disease patients. Int J Chron Obstruct Pulmon Dis. 2015;10:223–229. doi:10.2147/COPD.S64345
30. National Clinical Guideline Centre 2010 Chronic obstructive pulmonar disease: management of chronic obstructive pulmonar disease in adults in primary and secondary care. Accessed 06 October 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK65039/
31. Oates GRNS, Ott C, Scarinci IC, Schumann C, Parekh T, Dransfield MT. Adherence to pulmonary rehabilitation in COPD: a qualitative exploration of patient perspectives on barriers and facilitators. J Cardiopulm Rehabil Prev. 2019;39(5):344–349. doi:10.1097/HCR.0000000000000436
32. Mellion LR, Tovin MM. Grounded theory: a qualitative research methodology for physical therapy. Physiother Theory Pract. 2002;18(3):109–120. doi:10.1080/09593980290058490
33. Cutcliffe JR. Methodological issues in grounded theory. J Adv Nurs. 2000;31(6):1476–1484. doi:10.1046/j.1365-2648.2000.01430.x
34. Meis JJ, Bosma CB, Spruit MA, et al. A qualitative assessment of COPD patients’ experiences of pulmonary rehabilitation and guidance by healthcare professionals. Respir Med. 2014;108(3):500–510. doi:10.1016/j.rmed.2013.11.001
35. Elo S, Kyngas H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
36. Desveaux L, Rolfe D, Beauchamp M, Goldstein R, Brooks D. Participant experiences of a community-based maintenance program post-pulmonary rehabilitation. Chron Respir Dis. 2014;11(1):23–30. doi:10.1177/1479972313516880
37. Witcher CS, McGannon KR, Hernandez P, et al. A qualitative exploration of exercise among pulmonary rehabilitation participants: insight from multiple sources of social influence. Respir Care. 2015;60(11):1624–1634. doi:10.4187/respcare.04120
38. Cassemiro BM, Lemes ÍR, Figueiredo MP, Vanderlei FM, Pastre CM, Netto Júnior J. Effects of functional resistance training on muscle strength and musculoskeletal discomfort. Fisioter Mov. 2017;30(2):347–356. doi:10.1590/1980-5918.030.002.ao15
39. Wheaton AG, Cunningham TJ, Ford ES, Croft JB. Employment and activity limitations among adults with chronic obstructive pulmonary disease--United States, 2013. MMWR Morb Mortal Wkly Rep. 2015;64(11):289–295.
40. Velloso M, Stella SG, Cendon S, Silva AC, Jardim JR. Metabolic and ventilatory parameters of four activities of daily living accomplished with arms in COPD patients. Chest. 2003;123(4):1047–1053. doi:10.1378/chest.123.4.1047
41. Tangri S, Woolf CR. The breathing pattern in chronic obstructive lung disease during the performance of some common daily activities. Chest. 1973;63(1):126–127. doi:10.1378/chest.63.1.126
42. Barusso MS, Gianjoppe-Santos J, Basso-Vanelli RP, Regueiro EM, Panin JC, Di Lorenzo VA. Limitation of activities of daily living and quality of life based on COPD COMBINED CLASSIFICATION. Respir Care. 2015;60(3):388–398. doi:10.4187/respcare.03202
43. Blackstock FC, ZuWallack R, Nici L, Lareau SC. Why don’t our patients with chronic obstructive pulmonary disease listen to us? The enigma of nonadherence. Ann Am Thorac Soc. 2016;13(3):317–323. doi:10.1513/AnnalsATS.201509-600PS
44. Rodgers S, Dyas J, Molyneux AW, Ward MJ, Revill SM. Evaluation of the information needs of patients with chronic obstructive pulmonary disease following pulmonary rehabilitation: a focus group study. Chron Respir Dis. 2007;4(4):195–203. doi:10.1177/1479972307080698
45. Harrison SL, Lee AL, Elliott-Button HL, et al. The role of pain in pulmonary rehabilitation: a qualitative study. Int J Chron Obstruct Pulmon Dis. 2017;12:3289–3299. doi:10.2147/COPD.S145442
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Health Priorities in Chronic Obstructive Pulmonary Disease Patients with Multimorbidity: A Qualitative Study
Cai M, Cui M, Nong Y, Qin J, Mo S
Patient Preference and Adherence 2022, 16:2521-2531
Published Date: 13 September 2022
Factors Affecting Patient Adherence to Inhalation Therapy: An Application of SEIPS Model 2.0
Ma J, Sun X, Wang X, Liu B, Shi K
Patient Preference and Adherence 2023, 17:531-545
Published Date: 3 March 2023
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
The Use of Antibiotics for Uncomplicated Urinary Tract Infections in Adult Women: Qualitative Findings From the SCOUT Trial
Munné-Barellas B, Monfà R, Llor C, Garcia-Sangenís A, Miranda-Jiménez C, Morros R, Moragas A, Alvarez-Greciano P, Leiva A, Lozano-Del Hoyo ML, Sánchez-Calavera MA, Marín-Cañada J, Sánchez-Ruano R
Patient Preference and Adherence 2025, 19:2673-2685
Published Date: 31 August 2025
A Phenomenological Qualitative Study of Primary Informal Caregiver of Chinese Patients with Advanced Stage COPD: An In-Depth Exploration of Experiences and Needs
Ren X, Li F, Gao T, Xu X, Sun L, Liu S, Liu Y, Wang F
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:514685
Published Date: 20 March 2026