Back to Journals » Patient Preference and Adherence » Volume 16
Health Priorities in Chronic Obstructive Pulmonary Disease Patients with Multimorbidity: A Qualitative Study
Authors Cai M, Cui M, Nong Y, Qin J, Mo S
Received 8 June 2022
Accepted for publication 25 August 2022
Published 13 September 2022 Volume 2022:16 Pages 2521—2531
DOI https://doi.org/10.2147/PPA.S377832
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Mengqian Cai,1 Miaoling Cui,1 Ying Nong,2 Jinlian Qin,1 Sucai Mo1
1Department of Nursing, the First Hospital Affiliated of Guangxi Medical University, Nanning, People’s Republic of China; 2Respiratory Medicine, the First Hospital Affiliated of Guangxi Medical University, Nanning, People’s Republic of China
Correspondence: Miaoling Cui, Tel + 86 138 7813 4966, Email [email protected]
Purpose: To explore the health priorities of patients with multimorbidity in COPD and the factors as to why their condition is prioritized.
Methods: This qualitative study was conducted from February to April 2022 at a hospital in China. A specially selected sample of 18 patients completed a general information sheet and face-to-face interviews. The Colaizzi method was used to analyze the data.
Results: Participants reported their experience which fell into three themes: disease burden, health perception and views of others. In addition, participants explained that health knowledge from short videos on mobile apps influenced them, which in turn influenced their ranking.
Conclusion: Our findings suggested that health priorities of patients with multimorbidity in COPD manifest differently. Specifically, our findings suggested that patients’ health priorities are most influenced by disease burden, health perception, and the opinions of those around them. Nursing staff should fully understand each patients’own perspectives and provide them with personalized support.
Keywords: chronic obstructive pulmonary disease, health priorities, multimorbidity, multiple chronic conditions, qualitative research
Introduction
Multiple chronic conditions (MCCs) refers to the presence of two or more chronic diseases in the same patient.1 About one-third of adults worldwide are multimorbidity cases,2 and data from the China Health and Aging Report (CHALRS)3,4 shows that the prevalence of multimorbidities among middle-aged and elderly people in China has reached 53.8%. Research evidence5,6 shows that chronic obstructive pulmonary disease (COPD), an inflammatory airway disease with high rates of disability and death, is expected to be the third leading cause of death worldwide by 2030. With the fifth-highest disease burden, the disease will place an additional burden on patients’ health and finances. COPD exists as a comorbidity with an incidence of 80% ~ 90% accompanying cardiovascular disease, gastroesophageal reflux disease, osteoporosis or depression.7,8 COPD has become one of the major public health problems.9 Guidelines and expert consensus are still oriented towards single-disease treatment,10 which is inapplicable and can easily lead to an increased risk of multiple medication and treatments conflicting for patients.11
Despite the growing number of COPD patients in China, there is currently little research in healthcare services on the phenomenon of multimorbidity in COPD. Existing research focuses on disease classification and quantitative statistics, paying little attention to patients’ own experiences or recognizing multimorbidity. A growing number of studies have found12,13 that there are different emphases on multimorbidity treatment between doctors and patients in the treatment process, and that active attention should be paid to patients’ ideas. This has gradually developed into an ambiguous concept related to health priorities14,15 which has not yet developed into a universally accepted definition. When caring for patients with multimorbidity, health priorities should be the core focus to achieve patient-centered care. Emerging evidence suggests that prioritizing health concerns as well as considering patients’ cultural value preferences in patients with multiple health problems are useful methods in clarifying patients’ most emerging problems in order to provide better care.16 However, relevant studies remain scarce, mostly taking place in Europe and North America focusing on diabetes and arthritis,17,18 but COPD patients’ perceptions are largely unexplored. This study aims to identify and describe the characteristics and reasons why Chinese COPD patients with multimorbidity prioritize their MCCs. Our findings from this study will contribute to the understanding of patients’ multimorbidity experiences and decisions in the Asian context and expand the scope of current investigations on health priorities.
Methods
Design
A qualitative descriptive design was used to conduct semi-structured interviews with COPD patients attending the hospital’s Integrated Respiratory Care and Chronic Disease Management outpatient at a tertiary referral and the teaching hospital in Guangxi Zhuang Autonomous Region, China, to explore their health priorities. The target population included patients with multimorbidity at several regional levels, including Nanning, Guilin and Liuzhou, which are geographically close to each other. The population included a variety of employment and educational backgrounds.
Samples and Settings
The participants recruitment was based on the principle of maximal differentiation to fully consider the representativeness of the respondents, including diseases varieties, the number of diseases, and severity of diseases. Participants were asked to meet the following inclusion criteria: (1) a clear diagnosis of COPD in the hospital HIS system visit record and at least one other chronic disease confirmed; (2) a diagnostic basis: COPD met the diagnostic criteria of the GOLD 2020 guidelines and other chronic diseases met the criteria of the WHO International Classification of Diseases, which contains 14 common categories of chronic diseases: hypertension, dyslipidemia, diabetes, cancer, lung disease, liver disease, heart disease, stroke, kidney disease, digestive system disease, psychiatric-related problems, memory disease, arthritis/rheumatoid and asthma; (3) a lack of cognitive deficits, unimpeded communication with the investigator; (4) informed consent and voluntary cooperation with this study. Those with severe illness or severe cognitive impairment or mental illness that prevented them from cooperating were excluded. The sample amount ultimately collected was based on the saturation of information from the interview data. All interviews were conducted from February–April 2022. This study was conducted in accordance with the Declaration of Helsinki and received ethics approval from the First Affiliated Hospital of Guangxi Medical University Medical Ethics Committee (2021KY-E-116).
Data Collection
The study adopted a semi-structured in-depth interview method to collect data. Before the interviews, the researcher obtained basic information about the interviewees on the hospital HIS system, including various types of disease diagnosis, disease duration and treatment plan, etc. The researcher contacted participants for an interview one weeks later by phone, at a mutually convenient date. The interview was conducted in a quiet and comfortable meeting room. The interviewer was introduced to the participant by the professional nurses for chronic respiratory disease management. The purpose of the study and the time required was explained to the participant before the interview. Each participant spent approximately five minutes to complete the informed consent form and the population general information sheet, which contained information such as name, age, education, place of residence and occupation.
This study was evidence-based and a research team was established with experts who had been engaged in the management of chronic respiratory diseases for more than 20 years and had extensive clinical experience. The team members were trained in a professional qualitative research course. An initial interview outline was formed with literature review and group discussion and then two participants were pre-interviewed to determine the interview schedule in conjunction with the interview results.
Each interview started with the same open question: How is your health recently? The main interview questions to the participants are the following: (1) Do you currently have any other problems? (2) Which problem do you usually pay more attention to? Can you tell us why? (3) If you were to rank these issues, which issue would be first and which would be second? Or are they all equally important? Can you tell us the reasons for your decision? In addition, we asked the following subquestions: (1) How have these illnesses affected you? (2) Where do you usually learn about the problems you mentioned? (3) What are your thoughts and feelings about you health? During the interview, the interviewer recorded keywords and phrases, paying attention to non-verbal communication: expression, tone of voice, intonation, body posture, etc. Participants were encouraged to talk freely about all topics. Each interview lasted from 30 to 40 minutes.
Analysis of Information
In this study, data saturation was reached at interview 18. Two researchers independently transcribed the audio recordings into transcript within 24 hours after each interview. The first author checked the content of the two transcripts, and if there were differences, repeated listening to the recordings to avoid bias as much as possible.
The interview data were analyzed using the Colaizzi’s method.19 Two researchers independently read the transcript word-for-word, coded the recurring meaningful phrases, summarized and extracted the coded ideas, and formulated the themes. The third researcher participated in the copy-by-copy comparison of the data and recorded the controversial contents.
The researchers engaged in group discussions to organize and analyze the themes again, listened to the experts’ opinions on the themes and the parts that were in disagreement and listened back uniformly to correct the analysis results after the analysis was completed to ensure the accuracy and precision of the results. Finally, the results were returned to the interviewees for verification of the authenticity of the content. As this was the first study to explore the health priorities of the Chinese population, the first author translated the citations and subject matter from Chinese to English, and an author with bilingual (Chinese/English) expertise oversaw the entire transcription process to ensure the accuracy of the content.
Results
Sample Characteristics
A total of 18 COPD patients participated, 77.78% male (n=14) and 22.22% female (n=4), aged 46–77 (64.7±8.8) years, with a multimorbidity duration of 0.5–15 years (Table 1). The study included patients with different combinations of chronic diseases, 33.3% of the sample had only one chronic disease, 44.4% of the sample had a combination of two or three chronic conditions and 22.3% of the sample had a combination of more than three chronic conditions, with the most common comorbidity being hypertension (50.0%), followed by diabetes (27.8%) (Table 2).
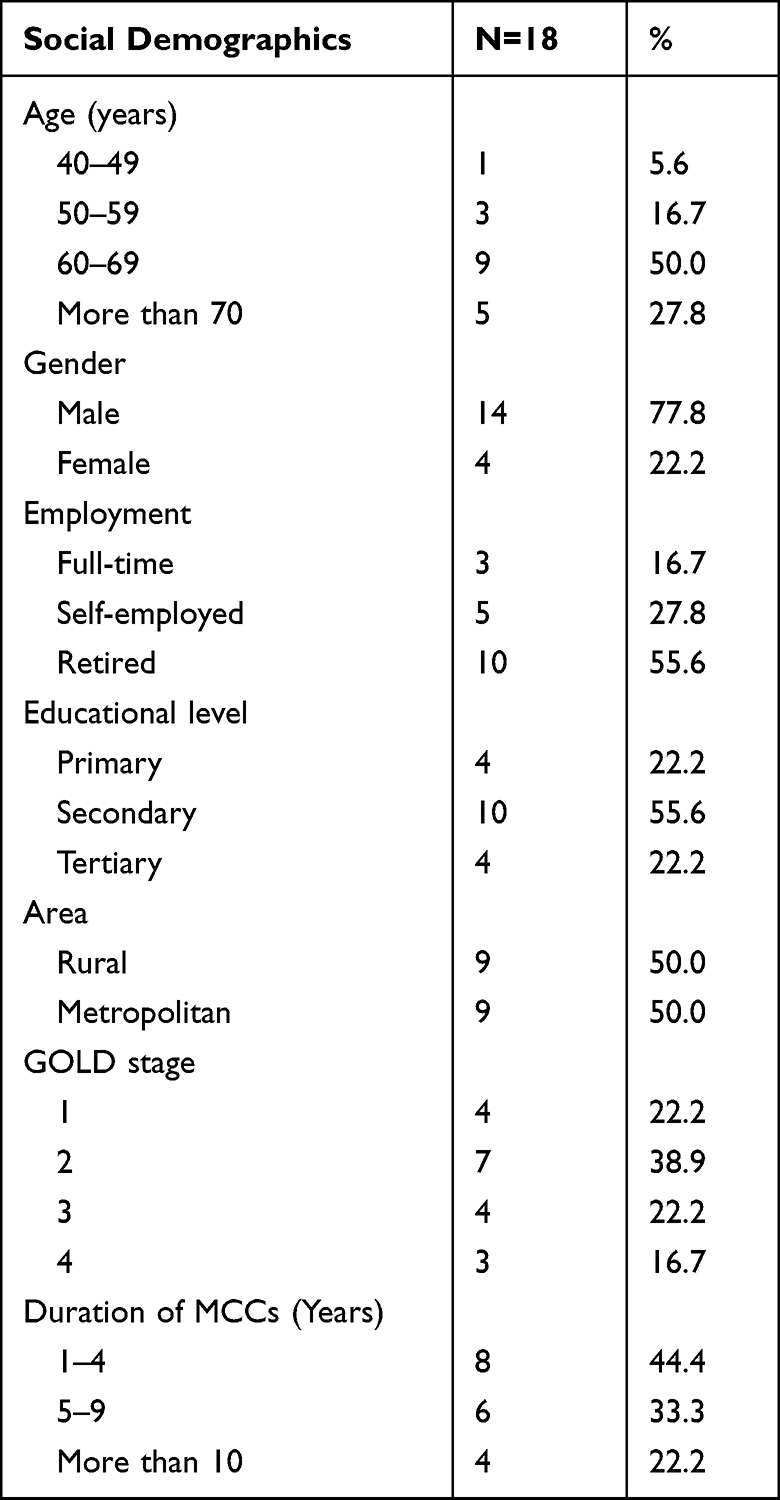 |
Table 1 Sample Characteristics |
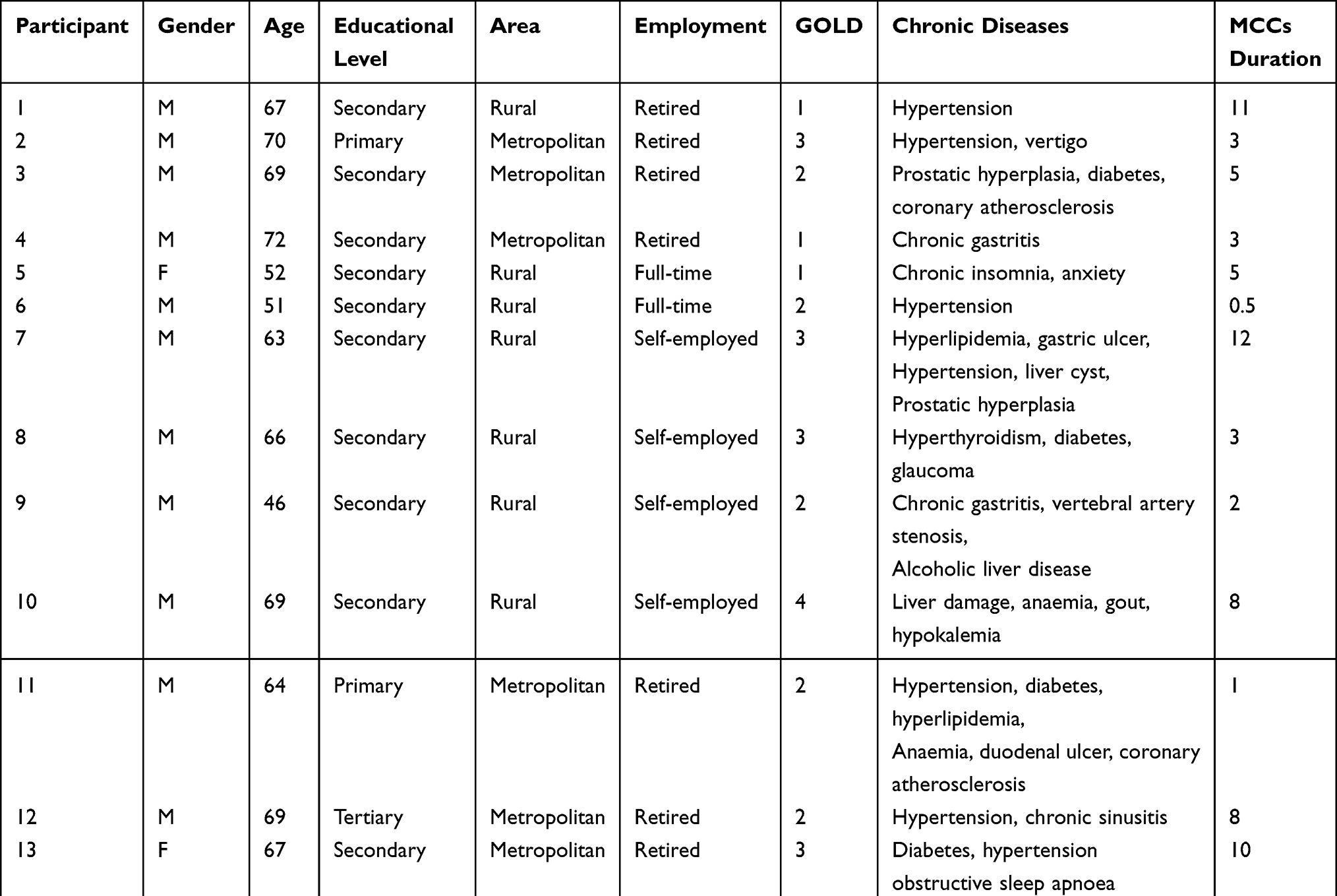 |
Table 2 Characteristics of Individual Participants |
Due to the variability in the number of co-existing conditions among respondents, this study focuses on the top two chronic conditions self-reported by patients. The results showed that 61.1% of participants ranked COPD as their top problem; 11.1% gave the highest priority to hypertension, and secondary priority problems included COPD (22.2%), hypertension (27.8%), chronic gastritis (11.1%), diabetes (5.6%), anaemia (5.6%), coronary atherosclerosis (5.6%), chronic insomnia (5.6%), chronic sinusitis (5.6%), vertebral artery stenosis (5.6%), alcoholic liver disease (5.6%) and obstructive sleep apnoea hypoventilation syndrome (5.6%). Table 3 presents a list of the health priority ranking of the participants.
 |
Table 3 Participants’ Self-Reported Ranking of Health Priorities |
Overview of the Main Themes
This interview was used to elicit data that would further explain the factors influence condition priorities. All findings were summarized into three themes (Table 4).
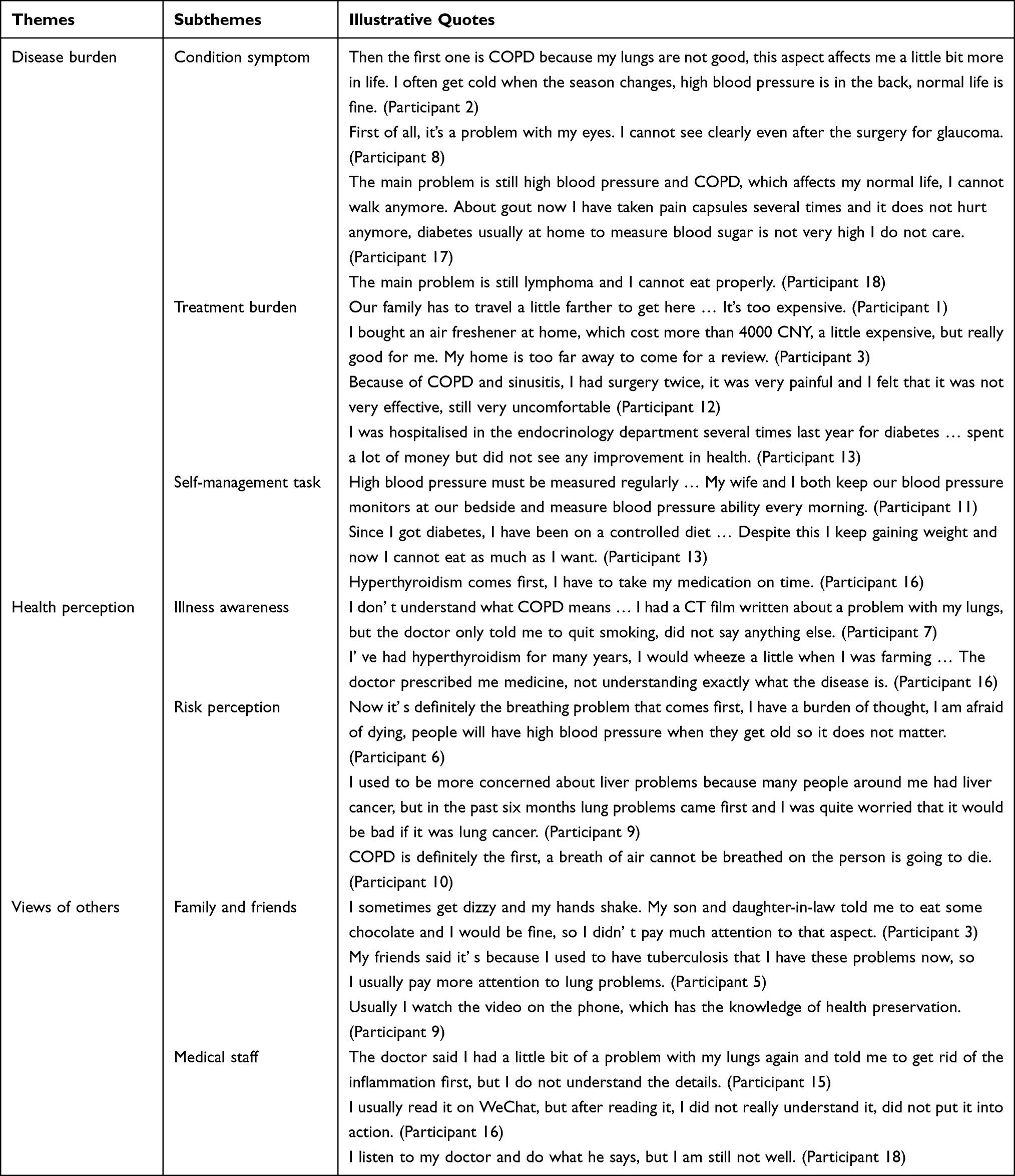 |
Table 4 Characteristics of Health Priorities of Patients with Multimorbidity in COPD |
Theme 1: Disease Burden
Sub-Theme 1: Condition Symptom
Many participants mentioned that they experienced multiple adverse symptoms. A common observation was that participants tended to prioritize symptomatic disease over asymptomatic disease.
The main problem is breathing. Now I have no strength to walk, I cannot walk, and when I walk, I will wheeze. Everything else does not matter. I do not get dizzy with high blood pressure, and gastritis usually does not flare up even if do not eat spicy or sour things. (Participant 7)
Regarding some diseases that did not have a direct adverse effect on daily life, some participants did not include them in their health priorities.
The first one was poor breathing and the second one was sinusitis. I have not even felt normal and uncomfortable physically since my bronchial surgery. The sinusitis makes my nose run backward a lot and affects my sleep. Regarding hypertension, I do not feel any very direct effect, so I am not too concerned. (Participant 12)
Sub-Theme 2: Treatment Burden
The burden of treatment on participants was a significant influence on health priorities. The majority of respondents in the sample experiencing greater financial stress for their first-priority disease.
My lupus erythematosus costs thousands of dollars in the hospital, and I do not have that much money to do farm work at home. (Participant 15)
Medical portability influenced participants’ decision-making such as drug allocation and transportation issues.
My hometown does not have inhaled drugs, I need to come here every month to get medicine, sometimes there is no medicine in the pharmacy. It’s a lot of trouble for me to come all the way here. (Participant 5)
Sub-Theme 3: Self-Management Task
The majority of participants described top-priority diseases that required self-management in their daily lives.
With COPD I need to use my inhaled medication on time, just like I have to eat three meals a day, one day without interruption. (Participant 2)
They believe that through self-management and exercise they can improve their health status, therefore devote more attention to these diseases.
I do pursed lips breathing every day. I think I still need to strengthen the exercise, so that the body will be comfortable (Participant 10)
Theme 2: Health Perception
Sub-Theme 1: Illness Awareness
The level of illness awareness was low in this sample of participants. Some participants were unable to accurately describe the name and symptoms of the disease, simply interpreted some diseases as organ problems.
I just have lung problems. The name is too long to remember, the obstruction sounds serious. I cannot sleep if I have something on my mind, so I guess it’s insomnia. (Participant 5)
Sub-Theme 2: Risk Perception
Participants had different opinions about disease risk. Some participants felt that the presence of poor prognosis and disease risk should be at the top of the list, and If left unattended, it can be a serious threat to life.
The first one is my lung problem. I used to be more concerned about high blood pressure, but it does not matter, just take medication on time, because high blood pressure does not kill people. People can be bad if they cannot breathe. (Participant 14)
Theme 3: Views of Others
Sub-Theme 1: Family and Friends
As China is traditional family-oriented society, the respondents’ preference to follow the advice of friends and relatives around them when faced with the treatment of multiple illnesses is likely to have been an important factor influencing the participants’ preferred view of their illness.
Actually, I should put the cough at the top of my list, but my friends around me are also more concerned about high blood pressure and high blood sugar, and that’s what we are used to thinking. (Participant 11)
Sub-Theme 2: Medical Staff
In addition, information asymmetry between patients and doctors may influence respondents’ illness perception, resulting in changes in health priorities. One example was a participant diagnosed diabetes who reported thinking he was just hypoglycemic, therefore, not taking it seriously.
I think I heard the doctor say I might have diabetes, I did not pay attention to it, I just have a little thirsty at night. (Participant 3)
Some respondents mentioned the opinions of medical professionals about their multiple diseases, but there was no clear in-depth discussion of health priorities between them.
The doctor said that stomach problems are not easily cured and it is useless to rush, so I am more concerned. (Participant 4)
This study also found that the mobile new media is gradually becoming a new channel for some people to acquire knowledge about diseases, affecting the priority of patients to treat diseases.
I often look at it on my phone, there are doctors who lecture on TikTok; COPD is the former bronchitis and emphysema, but hypertension is not much to see. (Participant 1)
Discussion
The current study used a qualitative interview approach to discover the health priorities of patients with multimorbidity in COPD. The findings of this study can contribute to the growing literature on the management of MCCs based on the Asian context, and more specifically, this study adds to the existing evidence on the perspectives of COPD patients with multimorbidity in China. It focuses on understanding how and why patients prioritize various conditions, tapping into the participants’ rich experiences. In our participant sample, fewer patients were able to consider multiple categories of their illnesses on the same position, and conditions were subject to the phenomenon of prioritization, in line with previous studies.20 The results of the present study showed disease burden, health perception and the views of others are the most important factors influencing the health priorities of COPD patients with multimorbidity.
According to our analysis, disease burden was an important factor influencing the priority of the condition, which was consistent with previous studies.21 COPD patients with multimorbidity occur in clusters, with an average number of approximately 3.9,22 and some Chinese scholars have shown23 that the burden of medical care and the need for medical consultation for elderly patients with multimorbidity in China is high, which was in agreement with this study. Participants’ stories revealed much distress in coping with MCCs, with respondents having complex conditions and up to eight co-existing diseases, causing damage to multiple organs and systems, which was similar with other studies.24 Our analysis also suggests that participants generally agreed that economic pressure is an important issue. If the reimbursement ratio of medical insurance can be further improved, it can solve many of the patients’ worries. It is necessary for health care professionals to speak up for patients through professional information dissemination platforms and seek improvements in social attention and policy support in the future.
Health perception refers to patients’ understanding and awareness of the disease, attention to its prognosis and related life expectations.25 The more patients know about the disease, the more likely they are to actively cooperate and receive better COPD care. Our participants attach great importance to the risk and prognosis of diseases. However, the respondents have a low level of awareness of their own diseases and lack the proper understanding of diseases. This situation will lead to patients missing the early recognition and treatment of the disease, so as to delay the disease. Consequently, we cannot eliminate the patient’s worry and fear of the disease, and this increases the psychological burden on them. These findings emphasize that an individual’s perception of disease influences his priority coping goals and health outcomes. It is suggested that medical staff carry out personalized communication and education to make patients correctly aware of their health risks, and then take active measures to prevent them. This is an important consideration for future work.
Unlike other research, we also found the participants referred more to the perspectives of family and friends and less to medical personnel when considering health priorities, which may be related to the traditional Chinese cultural environment. This is a study based on the Chinese population, where family-centered Confucianism, filial piety and patriarchal decision-making are more fully respected among people. Therefore, we should strengthen the publicity and education of family members in clinical work, inform them of the importance of their participation in the disease management of patients with multimorbidity, encourage family members to participate, and maximize the role of family in disease management. In addition, our participants seek health knowledge mainly on the internet. The impact caused by the rise of short-form social media such as TikTok and WeChat has spread to the medical field, impacting the Chinese traditional medical consultation model. The health care accounts on short video platform are mostly non-professional, lacks high-quality medical content. Unscientific health information can easily mislead audiences and delays in medical.26 Patients with multimorbidity face the need of health knowledge in various aspects. It is essential for medical staff to deliver accurate health information, the researchers should also actively carry out health education activities, strengthen the “Internet+” medical education and popularization services, and realize the multimedia of health science popularization. This will be one of our future research directions.
Previous research has noted27 that as a subjective experience, patients may inherently prioritize certain illnesses over others and change this prioritization over time. One study28 found that there was only 54.9% agreement between patients and physicians on health priorities and that an excessive focus on patients’ personal priorities may lead to poor disease outcomes, which is an important consideration for future work. However, there is still a paucity of research on patient health priorities and a lack of enough supportive evidence.29 The literature on MCCs management in China are few reported.30,31 Researchers should focus on the illness experience of patients with multimorbidity, help them improve their illness perceptions and construct patient-centered pathways for multimorbidity management. Overall, clarifying patient health priorities enables physicians to understand patient value preferences and help patients to view their illnesses objectively and scientifically. Medical staff should translate traditional clinical thinking, confirm communication about the importance and priority of multiple issues and actively integrate patient health priority perspectives with disease treatment concepts to provide personalized support for patients with multimorbidity.
Strengths and Limitations
This is the first qualitative study published in Chinese mainland on patients with multimorbidity in COPD. Using a qualitative design, this study explains the health priorities of patients with multimorbidity in COPD. Participants varied in demographics, clinical characteristics, and perspectives. A discussion based on health priorities demonstrates what is really going on inside the minds of the respondents.
One of the main limitations in this study was that participants’ burden of disease scores were not assessed using a professional assessment tool and lacked objective data for comparison, which may have made the results more subjective. All participants had different types of additional diseases. However, they were all recruited at a Centre for Integrated Respiratory Care and Chronic Disease Management Clinic, and the interviewer was introduced to the participant by the professional nurses for chronic respiratory disease management. Because all participants came from a single hospital in southern China, assessment may be more consistent, but the study may not be representative of other regions of China. Future studies should expand recruitment and explore prioritizing classification in other multimorbidity regional clusters will help to address this issue. In addition, our analysis of the priorities of patients with multimorbidity was conducted during a period. There is a trajectory of change in health priorities, and the findings generated in this study need to be further explored through both qualitative and quantitative research methods.
Conclusion
In conclusion: COPD patients with multimorbidity have distinctive health priorities. There is a widespread phenomenon of heavy treatment burden, low illness perception, and lack of access to professional information. With the aging of China’s population, the phenomenon of “multiple diseases in one body” among COPD patients has become increasingly prominent. It is suggested that healthcare professionals should pay attention to the issues. By understanding the patients’ health priorities, professionals can better develop individualized interventions and realize person-centered multimorbidity management. Therefore, future researchers should expand the assessment of health priorities to provide insights from different perspectives such as health outcomes, symptoms, and treatment. The next step in this study will be to explore whether clustering of different chronic diseases exists in China, and to gather information from patients with other types of multimorbidities and their health care workers. This will help to achieve dynamic analysis and comparison over time and to clearly identify factors related to patients’ health priorities.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Consent for Publication
The informed consent form included a statement that the patients agreed to their interviews to be used in anonymised publication.
Funding
This study was supported by the Guangxi Medical and Health Research Program (grant number: Z20190780) and the First Affiliated Hospital of Guangxi Medical University Nursing Clinical Research Climbing Program Innovation Project (grant number: YYZS2020027).
Disclosure
All authors declare no conflict of interest.
References
1. National Institute for Health and Care Excellence. Multimorbidity: clinical assessment and management [EB/OL]; 2016. Available from: https://www.nice.org.uk/guidance/ng56.
2. Hajat C, Stein E. The global burden of multiple chronic conditions: a narrative review. Prev Med Rep. 2018;12:284–293. doi:10.1016/j.pmedr.2018.10.008
3. Zhao YH, Wang YF, Chen XX, China Health and Retirement Longitudinal Study [EB/OL]; 2019. Available from: http://charls.pku.edu.cn/Public/ashelf/public/uploads/document/public_documents/application/china-health-retirement-report.pdf.
4. Ya W, Lu Y, Zhang R, et al. Multimorbidity status of the elderly in China-research based on CHARLS data. Chin J Dis Control Prev. 2019;23(4):426–430.
5. García-Olmos L, Alberquilla A, Ayala V, et al. Comorbidity in patients with chronic obstructive pulmonary disease in family practice: a cross-sectional study. BMC Fam Pract. 2013;14:11. doi:10.1186/1471-2296-14-11
6. Hansen NS, Ängquist L, Lange P, et al. Comorbidity Clusters and Healthcare Use in Individuals With COPD. Respir Care. 2020;65(8):1120–1127. doi:10.4187/respcare.07136
7. García-Olmos L, Alberquilla A, Ayala V, et al. Comorbidity in patients with chronic obstructive pulmonary disease in family practice: a cross sectional study. BMC Fam Pract. 2013;14(14):11.
8. Hansen NS, Ängquist L, Lange P, et al. Comorbidity clusters and healthcare use in individuals with COPD. Respir Care. 2020;65(8):1120–1127.
9. Chubachi S, Sato M, Kameyama N, et al. Identification of five clusters of comorbidities in aI longitudinal Japanese chronic obstructive pulmonary disease cohort. Respir Med. 2016;117:272–279. doi:10.1016/j.rmed.2016.07.002
10. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease 2020 report[EB/OL]; 2019. Available from: https://goldcopd.org/gold-reports/.
11. Hughes LD, McMurdo ME, Bet G, et al. Guidelines for people not for diseases: the challenges of applying UK clinical guidelines to people with multimorbidity. Age Ageing. 2013;42(1):62–69. doi:10.1093/ageing/afs100
12. Eckerblad J, Theander K, Ekdahl A, et al. To adjust and endure: a qualitative study of symptom burden in older people with multimorbidity. Appl Nurs Res. 2015;28(4):322–327. doi:10.1016/j.apnr.2015.03.008
13. Richardson LM, Hill JN, Smith BM, et al. Patient prioritization of comorbid chronic conditions in the Veteran population: implications for patient-centered care. SAGE Open Med. 2016;4:2050312116680945. doi:10.1177/2050312116680945
14. Feder SL, Kiwak E, Costello D, et al. Perspectives of patients in identifying their values-based health priorities. J Am Geriatr Soc. 2019;67(7):1379–1385. doi:10.1111/jgs.15850
15. Fried TR, Tinetti M, Agostini J, et al. Health outcome prioritization to elicit preferences of older persons with multiple health conditions. Patient Educ Couns. 2011;83(2):278–282. doi:10.1016/j.pec.2010.04.032
16. Cheraghi-Sohi S, Morden A, Bower P, et al. Exploring patient priorities among long-term conditions in multimorbidity: a qualitative secondary analysis. SAGE Open Med. 2013;1:205031211350395. doi:10.1177/2050312113503955
17. Mc NK, Breken BD, Alzubaidi HT, et al. Health professional perspectives on the management of multimorbidity and polypharmacy for older patients in Australia. Age Ageing. 2017;46(2):291–299. doi:10.1093/ageing/afw200
18. Grant RW, Ashburner JM, Hong CS, et al. Defining patient complexity from the primary care physician’s perspective: a cohort study. Ann Intern Med. 2011;155(12):797–804. doi:10.7326/0003-4819-155-12-201112200-00001
19. Colaizzi P. Psychological Research as the Phenomenologists View It. New York: Oxford University Press; 1978:4827.
20. Cheng C, Bai J, Yang CY, et al. Patients’experiences of coping with multiple chronic conditions: a qualitative descriptive study. J Clin Nurs. 2019;28(23–24):4400–4411. doi:10.1111/jocn.15022
21. Sathanapally H, Sidhu M, Fahami R, et al. Priorities of patients with multimorbidity and of clinicians regarding treatment and health outcomes: a systematic mixed studies review. BMJ Open. 2020;10(2):e033445. doi:10.1136/bmjopen-2019-033445
22. Triest F, Franssen F, Reynaert N, et al. Disease-Specific Comorbidity Clusters in COPD and Accelerated Aging. J Clin Med. 2019;8(4):548. doi:10.3390/jcm8040511
23. Yan W, Wang JP, Zhang HB, et al. Challenges and solutions for elderly patients with multimorbidity during receiving management in China. Chine General Practice. 2018;21(3):261–264.
24. Houben-Wilke S, Triest F, Franssen F, et al. Revealing methodological challenges in chronic obstructive pulmonary disease studies assessing comorbidities: a narrative review. Chronic Obstr Pulm Dis. 2019;6(2):166–177.
25. NIH National Heart Lung and Blood Institute. COPD learn more breathe better® program.[EB/OL]. 2018; Available from: https://www.nhlbi.nih.gov/health/educational.
26. Lin Y, Ye X. Analysis of the operation status and development of health care accounts on TIKTOK. Chin J Hosp Admin. 2020;36(12):1045–1048.
27. Beverly EA, Wray LA, Chiu C-J, et al. Older Adults‘ Perceived Challenges With Health Care Providers Treating Their Type 2 Diabetes and Comorbid Conditions. Clin Diabetes. 2014;32(1):12–17. doi:10.2337/diaclin.32.1.12
28. Déruaz-Luyet A, N’Goran AA, Pasquier J, et al. Multimorbidity: can general practitioners identify the health conditions most important to their patients? Results from a national cross-sectional study in Switzerland. BMC Fam Pract. 2018;19(1):66. doi:10.1186/s12875-018-0757-y
29. Salisbury C, Man MS, Bower P, et al. Management of multimorbidity using a patient-centred care model: a pragmatic cluster-randomised trial of the 3D approach. Lancet. 2018;392(10141):41–50. doi:10.1016/S0140-6736(18)31308-4
30. Wang JF, Zhang ZH, Cui Y, et al. AnaIysis on combinations of muhimorbidity in the eidey in shanghai comnlunities and the influence factors. Griatr Health Care. 2017;23(2):97–101.
31. Wu TT, Lu Y, Ai DD, et al. Comorbidity management model in elderly in China based on the theory of complexity science. Chine General Practice. 2019;22(34):4197–4201.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development of an Electronic Tool to Assess Patient Preferences in Geriatric Polypharmacy (PolyPref)
Eidam A, Roth A, Frick E, Metzner M, Lampert A, Seidling HM, Haefeli WE, Bauer JM
Patient Preference and Adherence 2022, 16:1733-1747
Published Date: 23 July 2022
Satisfaction and Adherence of COPD Patients to a Conventional Training Associated with Functional Exercises and to a Conventional Training Isolated: A Qualiquantitative Study
Grigoletto I, de Lima FF, Eto DA, Suzuki NNV, Uzeloto JS, Ramos EMC
Patient Preference and Adherence 2022, 16:2759-2772
Published Date: 11 October 2022
Frequency and Correlates of Multimorbidity Among the Oldest Old: Study Findings from the Representative “Survey on Quality of Life and Subjective Well-Being of the Very Old in North Rhine-Westphalia (NRW80+)”
Hajek A, König HH
Clinical Interventions in Aging 2023, 18:41-48
Published Date: 11 January 2023
Factors Affecting Patient Adherence to Inhalation Therapy: An Application of SEIPS Model 2.0
Ma J, Sun X, Wang X, Liu B, Shi K
Patient Preference and Adherence 2023, 17:531-545
Published Date: 3 March 2023
A Qualitative Study on Distributed Leadership in Integrated Care: Exploring the Experiences of Elderly Multimorbid Patients with GP Collaboration
Braut H, Storm M, Mikkelsen A
Journal of Multidisciplinary Healthcare 2023, 16:3167-3177
Published Date: 26 October 2023