Back to Journals » Journal of Inflammation Research » Volume 19
A Novel Composite Bioscore Integrating Biomarkers, Clinical Scores, and Comorbidity Indices for Prognostic Stratification in Sepsis
Authors Țocu G ![]() , Mihailov R
, Mihailov R ![]() , Luțenco V, Dimofte F
, Luțenco V, Dimofte F ![]() , Ștefănescu BI
, Ștefănescu BI ![]() , Niculeț E
, Niculeț E ![]() , Mihailov OM, Țocu L, Stavăr Matei L
, Mihailov OM, Țocu L, Stavăr Matei L ![]()
Received 9 November 2025
Accepted for publication 6 February 2026
Published 23 February 2026 Volume 2026:19 579172
DOI https://doi.org/10.2147/JIR.S579172
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xin Du
George Țocu,1,2 Raul Mihailov,3 Valerii Luțenco,3 Florentin Dimofte,3 Bogdan Ioan Ștefănescu,3 Elena Niculeț,4 Oana Mariana Mihailov,5 Lavinia Țocu,6 Loredana Stavăr Matei5
1Department of Pharmaceutical Sciences, Faculty of Medicine and Pharmacy, “Dunărea de Jos” University, Galați, 800008, Romania; 2Clinical Department of Medical Laboratory Analysis, “Sf. Apostol Andrei” County Emergency Clinical Hospital, Galați, 800578, Romania; 3Department of Clinical Surgery, Faculty of Medicine and Pharmacy, “Dunărea de Jos” University, Galați, 800008, Romania; 4Department of Morphological and Functional Sciences, Faculty of Medicine and Pharmacy, “Dunărea de Jos” University, Galați, 800008, Romania; 5Department of Clinical Medicine, Faculty of Medicine and Pharmacy, “Dunărea de Jos” University, Galați, 800008, Romania; 6Department of Clinical Cardiology, “Sf. Apostol Andrei” County Emergency Clinical Hospital, Galați, 800578, Romania
Correspondence: Bogdan Ioan Ștefănescu, Department of Clinical Surgery, Faculty of Medicine and Pharmacy, “Dunarea de Jos” University, Galați, 800008, Romania, Email [email protected] Lavinia Țocu, Department of Clinical Cardiology, “Sf. Apostol Andrei” County Emergency Clinical Hospital, Galați, 800578, Romania, Email [email protected]
Background: Risk stratification in sepsis remains a major clinical challenge in hospital settings, where timely recognition of disease progression can critically influence outcomes. Traditional scoring systems, such as SOFA and APACHE II, are frequently applied but are limited by their complexity and inconsistent predictive accuracy. Integrating biological markers with clinical scores may enhance the early identification of patients with an unfavorable prognosis.
Objective: The objective of this investigation was to determine the prognostic performance of two composite scoring systems, BIO-S and BIO-SC, in predicting 28-day mortality among patients with sepsis or septic shock.
Methods: We conducted a retrospective single-center study including 125 adult surgical patients with sepsis or septic shock. BIO-S was calculated using procalcitonin (PCT), neutrophil-to-lymphocyte ratio (NLR), INR, and SOFA score, whereas BIO-SC extended this model by incorporating the Charlson Comorbidity Index (CCI). Both bioscores were calculated at admission and analyzed in relation to 28-day mortality and discharge status.
Results: Among the 125 patients included, 28-day all-cause mortality was 36% (n = 45). The BIO-SC score achieved the highest predictive accuracy for 28-day mortality (AUC = 0.942), surpassing BIO-S (AUC = 0.930), SOFA (AUC = 0.928), and APACHE II (AUC = 0.918). Both bioscores correlated strongly with discharge outcomes and were independent predictors of 28-day mortality (p < 0.001).
Conclusion: Integrating inflammatory biomarkers, organ dysfunction, and comorbidity burden into composite prognostic models such as BIO-S and BIO-SC significantly improves early mortality risk assessment and outcome prediction in sepsis, although external validation remains necessary.
Keywords: sepsis, septic shock, bioscore, biomarker, prognostic, risk stratification
Introduction
Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection, according to the Third International Consensus Definitions (Sepsis-3).1,2 Globally, it is estimated that 48.9 million cases occur each year, resulting in approximately 11 million deaths.3 The Surviving Sepsis Campaign reports mortality rates of 30–50% for sepsis and 50–60% for septic shock.4 The often subtle onset of sepsis and its heterogeneous clinical presentations make early recognition of severe cases and rapid initiation of therapy particularly challenging.5 Identifying patients at high risk and with unfavorable prognosis remains difficult, yet it is essential to improve survival through timely and appropriate therapeutic interventions.6 Despite advances in pathophysiological understanding and critical care management, sepsis-related mortality remains high, underscoring the urgent need for more accurate prognostic tools.7,8
Clinical assessment of sepsis commonly depends on severity scores, particularly the Sequential Organ Failure Assessment (SOFA) and the Acute Physiology and Chronic Health Evaluation II (APACHE II).9 As a component of the Sepsis-3 framework, SOFA provides a quantitative measure of organ failure and is recognized as a reliable prognostic indicator of mortality in patients with sepsis.10 However, its routine use is limited by the large number of parameters included, which may render it impractical in emergency departments,11 though it remains standard practice in the Intensive Care Unit (ICU). Although SOFA is more reliable than other tools, such as APACHE II or the Simplified Acute Physiology Score (SAPS) II, for predicting outcomes in intensive care, it does not always provide optimal accuracy for mortality prediction, and several studies have reported that its performance may be surpassed by biomarker-based scores or composite models.12 APACHE II, in use for over three decades as a benchmark of severity, integrates multiple acute physiological and chronic factors; however, its application at the bedside is relatively cumbersome and time-intensive.13 In addition, although APACHE II remains valid for short-term mortality prediction, it is not specific for sepsis and may underestimate acute organ dysfunction associated with severe infections.14 These shortcomings illustrate the limitations of conventional scores: some are complex or require numerous data points (restricting their use in emergency situations), while others fail to fully capture mechanisms critical for prognosis, such as immunosuppression or the impact of comorbidities.15
To address these challenges, research has increasingly focused on serum biomarkers with prognostic potential for outcome prediction in sepsis. Various biomarkers have been examined individually as potential indicators of sepsis severity, including procalcitonin (PCT) for bacterial infection, neutrophil-to-lymphocyte ratio (NLR) for systemic inflammation, and the International Normalized Ratio (INR) for sepsis-related coagulopathy. However, none of these biomarkers alone has provided sufficient predictive accuracy. Elevated PCT levels are linked with sepsis presence and infection severity, but their prognostic value for mortality remains modest. A recent study demonstrated that both PCT and C-reactive protein (CRP), interpreted separately, have limited utility in predicting 30-day mortality, showing no significant association with death in sepsis or septic shock.16 Likewise, NLR has been investigated as a prognostic marker, with some meta-analyses reporting that elevated values correlate with worse outcomes (hazard ratio ~1.6–1.7).11 Nevertheless, findings remain inconsistent, with other studies failing to confirm its predictive value.11 Similarly, an elevated INR reflects coagulopathy and possible disseminated intravascular coagulation, but by itself does not provide accurate prognostic information.17 The emerging consensus is that no single biomarker achieves adequate sensitivity and specificity for routine clinical use in diagnosing or prognosticating sepsis.18 The complexity and heterogeneity of the host response imply that multiple biological indicators are needed to reflect the full spectrum of disease mechanisms.19
In recent years, combining biomarkers with clinical scoring systems has been proposed as a strategy to enhance prognostic accuracy and improve outcome prediction in sepsis.20 Several studies have shown that adding laboratory markers to established scores improves mortality prediction. For example, incorporating serum lactate, PCT, or CRP values alongside SOFA led to a more accurate risk estimation than SOFA alone.21 Similarly, including parameters such as hypoalbuminemia or the inflammatory mediator heparin-binding protein (HBP) improved the predictive performance of SOFA-based models.22 A multicenter investigation further confirmed that merging clinical scores (SOFA with APACHE II) and biomarkers (eg, albumin) yields superior mortality prediction compared to either parameter individually.23 Pre-existing comorbidities also play a significant role: the Charlson Comorbidity Index (CCI), although less predictive on its own than severity scores,24 can complement them effectively. In a prospective cohort, a model combining PCT, SOFA, and CCI demonstrated the strongest prediction of 28-day mortality with an area under the curve (AUC) of 0.943, outperforming each factor individually.25 These findings suggest that aggregating information on infection and inflammation (PCT, NLR), organ dysfunction (SOFA), coagulation status (INR), and comorbidity burden (CCI) provides a more accurate representation of disease severity and prognosis in sepsis.
Based on these considerations, in the present study we developed two composite bioscores (BIO-S – BIOmarkers: PCT, NLR, INR + SOFA, and BIO-SC – BIOmarkers: PCT, NLR, INR + SOFA + CCI), intended to address the shortcomings of existing tools by offering greater accuracy in stratifying sepsis severity and predicting prognosis, with emphasis on short-term mortality. The BIO-S bioscore integrates four key elements: PCT (marker of bacterial infection), NLR (indicator of immune inflammatory response), INR (marker of coagulopathy), and the SOFA score (assessment of organ dysfunction). The BIO-SC bioscore extends BIO-S by adding the Charlson Comorbidity Index (CCI), thereby incorporating the impact of pre-existing chronic conditions on the outcome of septic patients.
This research sought to analyze the prognostic performance of two recently developed composite bioscores compared with conventional clinical tools in predicting 28-day mortality among surgical patients with sepsis or septic shock. By integrating inflammatory biomarkers with severity scores and comorbidity measures, these bioscores aim to enhance risk stratification and support more accurate prognostic assessment in sepsis management.
Materials and Methods
Study Design and Population
This retrospective, observational study included 125 adult patients admitted with sepsis or septic shock to the surgical wards of the “Sf. Apostol Andrei” County Emergency Clinical Hospital (Galați, Romania) between January 2020 and December 2021. As this was a retrospective cohort study, no a priori sample size calculation was performed. Instead, the study included all consecutive adult surgical patients with sepsis or septic shock who met the eligibility criteria during the study period, so the final sample size reflects the full eligible surgical case load of our center.
Diagnosis of sepsis and septic shock followed the Sepsis-3 criteria, with sepsis requiring an acute ≥2-point SOFA increase and septic shock requiring vasopressors to maintain MAP ≥65 mmHg and lactate >2 mmol/L despite adequate fluid resuscitation.1
Clinical and laboratory data were retrospectively extracted from the hospital electronic medical records and the Laboratory Information System (LIS), using anonymized identifiers and only after obtaining institutional ethics approval.
Inclusion criteria were: adult patients (≥18 years) admitted to surgical wards with confirmed sepsis or septic shock of surgical etiology (eg, postoperative peritonitis, intra-abdominal infection, or trauma-related sepsis) according to Sepsis-3 criteria at admission, availability of complete clinical and paraclinical data within the first 24 hours, and a 28-day follow-up period.
Exclusion criteria were: non-surgical sepsis cases, medical (non-operative) admissions, death within 72 hours of surgery, conservative (non-operative) management, prior antibiotic therapy exceeding 24 hours, ongoing chemotherapy, chronic dialysis, or immunosuppressive treatment.
Importantly, the exclusion of patients receiving ongoing chemotherapy or chronic dialysis referred only to active cytotoxic treatment and maintenance renal replacement therapy. Patients with a history of malignancy or chronic kidney disease not yet requiring dialysis remained eligible and were included in the cohort, and their chronic conditions were captured within the Charlson Comorbidity Index and comorbidity categories.
For each patient, clinical variables (SOFA score, APACHE II score, clinical status at admission), laboratory biomarkers (PCT, NLR, and INR), and comorbidity indices (Charlson Comorbidity Index, CCI) were recorded. SOFA and APACHE II scores were calculated at the time of surgical ward admission, prior to ICU transfer or initiation of vasopressor therapy. All biomarkers used to construct the bioscores (PCT, NLR, INR) were obtained at the time of surgical ward admission in the first 6 hours of admission. The Charlson Comorbidity Index (CCI) was calculated at surgical ward admission, based on documented pre-existing comorbidities. Comorbidities included cardiovascular disease (eg, hypertension, ischemic heart disease, heart failure), cerebrovascular disease (eg, stroke or transient ischemic attack), psychiatric disease (eg, epilepsy, dementia, bipolar disorder), metabolic disorders (eg, diabetes mellitus), chronic respiratory disease (eg, COPD), chronic kidney disease, chronic liver disease, and oncologic disease (solid tumors or hematological malignancies).
In this study, we analyzed only those biomarkers that were systematically recorded in the LIS for all included patients (procalcitonin, NLR, INR). Other biomarkers, such as lactate or presepsin, are not performed within the hospital’s clinical laboratory and are not automatically transmitted to the LIS. These analyses are carried out exclusively in the ICU at the bedside using point-of-care devices, without standardized integration into the clinical laboratory workflow.
The primary endpoint of the study was 28-day all-cause mortality among patients diagnosed with sepsis or septic shock. Mortality and survival status were determined based on hospital records and follow-up data obtained from outpatient visits or scheduled check-ups within 28 days after admission. Patients who survived beyond 28 days were censored at that time point for survival analysis.
All patients were screened for SARS-CoV-2 infection prior to surgical admission according to institutional protocols. No patients included in the final cohort had active COVID-19 infection at admission, and therefore COVID-related respiratory failure did not contribute to SOFA scores or outcomes.
The study was conducted and reported in accordance with the RECORD (REporting of studies Conducted using Observational Routinely-collected health Data) statement, which extends the STROBE guidelines for observational studies. The completed RECORD checklist is provided as Supplementary File 1.
Creation of the Bioscores
Starting from the premise that sepsis and septic shock involve quantifiable multisystemic dysfunctions, we developed two combined bioscores (BIO-S and BIO-SC). The biomarkers included in the bioscores were selected based on their biological relevance in sepsis pathophysiology and their routine availability in clinical laboratories. Therefore, this study focused on integrating widely measurable parameters into practical composite bioscores.
The BIO-S score was constructed by summing the point values obtained from four parameters (PCT, NLR, INR, and SOFA).
To ensure clinical plausibility and reproducibility, candidate categorical intervals for PCT, NLR and INR were initially defined based on pathophysiological severity patterns described in sepsis literature and on the empirical distribution observed in our cohort, then refined through ROC analysis. For PCT, categories (<0.5; 0.5–1.99; 2–9.99; 10–49.9; ≥50 ng/mL) followed established severity cut-offs frequently used to discriminate bacterial infection and sepsis severity.26,27 For NLR, categories (1–3.99; 4–5.99; 6–8.99; 9–17.99; >18) were chosen to reflect progressive systemic inflammatory response, consistent with ranges reported in previous sepsis studies.28,29 For INR, classes (<1.2; 1.2–1.49; 1.5–1.99; 2–4.99; ≥5) were designed to represent progressive stages of sepsis-associated coagulopathy, aligned with definitions used in sepsis-related coagulation scoring systems.30
Based on these intervals, BIO-S was formulated as follows:
- PCT – scored from 0 to 4 points (PCT: <0.5=0; 0.5–1.99=1; 2–9.99=2; 10–49.9=3; ≥50=4);
- NLR – scored from 0 to 4 points (NLR: 1–3.99=0; 4–5.99=1; 6–8.99=2; 9–17.99=3; >18=4);
- INR – scored from 0 to 4 points (INR: <1.2=0; 1.2–1.49=1; 1.5–1.99=2; 2–4.99=3; ≥5=4);
- SOFA score – full scoring adopted according to the original formula (values between 0 and 24 points).
Cut-off intervals were optimized using ROC curve analysis and the Youden index for 28-day mortality prediction. To ensure robustness and minimize potential overfitting, internal bootstrap validation (1000 iterations) was applied, yielding 95% confidence intervals that closely matched the apparent cut-offs. These thresholds demonstrated strong biological plausibility and consistency with prior evidence, supporting their stability within this cohort. The total BIO-S score ranged from 0 to 36 points.
The BIO-SC score represents an extension of the BIO-S score by adding a fifth element: the CCI (Charlson Comorbidity Index), quantified according to the original formula (values between 0 and 37), which integrates the severity and number of chronic comorbidities. Thus, BIO-SC reflects not only the acute severity of the septic process (through biomarkers and the SOFA score) but also the pre-existing comorbidity burden, resulting in values ranging from 0 to 73 points.
For clinical interpretability, BIO-S and BIO-SC risk categories (low, moderate, high) were defined using a combined approach: (I) the ROC-derived optimal cut-off (Youden index) for 28-day mortality to identify the transition to the high-risk stratum, and (II) Cox-derived hazard gradients, whereby each 1-point increase in BIO-S and BIO-SC increased the 28-day mortality hazard by approximately 28–29%. This procedure enabled clinically meaningful stratification of continuous scores into risk bands without relying on post-hoc mortality distribution.
Statistical Analysis
Statistical analyses were performed using SPSS software version 26.0 (IBM Corp., Armonk, NY, USA). Data distribution was assessed with the Kolmogorov–Smirnov and Shapiro–Wilk tests. Continuous variables were expressed as mean ± SD for normally distributed data or as median (interquartile range, IQR) for non-parametric data. Between-group differences were evaluated using the Student’s t-test or Mann–Whitney U-test, as appropriate, while categorical variables were compared using the χ2 or Fisher’s exact test. The prognostic performance of BIO-S and BIO-SC for predicting 28-day mortality was evaluated by receiver operating characteristic (ROC) curve analysis, with calculation of the area under the curve (AUC), sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). ROC-based optimal thresholds were subsequently verified using the Youden index (J = sensitivity + specificity − 1) for 28-day mortality. AUCs were compared between bioscores and conventional clinical scores (SOFA, APACHE II) using the DeLong test. Internal validation was performed via bootstrap resampling (1000 iterations) to estimate optimism-corrected AUCs and 95% CIs. Pearson’s correlation coefficients were used to examine linear associations between bioscores and discharge outcomes. Survival was analyzed using Kaplan–Meier curves based on risk categories (low, moderate, and high) defined by BIO-S and BIO-SC thresholds, with differences tested by the log-rank method. BIO-S and BIO-SC risk category thresholds were defined using ROC-derived optimal cut-offs (Youden index) for 28-day mortality. Proportional hazards Cox regression models were applied to assess the independent association of each score with 28-day mortality, reporting hazard ratios (HRs) and 95% confidence intervals (CIs). The initial multivariable model included BIO-S, BIO-SC, SOFA, APACHE II, septic shock status, age, sex, and the Charlson Comorbidity Index (CCI). Given that septic shock status may be collinear with severity scores and with the proposed bioscores, as it represents a clinical marker of acute severity, a backward stepwise elimination procedure was applied to reduce collinearity and informational overlap between variables and to retain only predictors with independent prognostic contribution. CCI was evaluated both as an independent covariate and as a component of the composite BIO-SC model. Model calibration was examined using the Hosmer–Lemeshow goodness-of-fit test, Brier score, and visual inspection of calibration plots comparing predicted versus observed 28-day mortality. All statistical tests were two-tailed, and p < 0.05 was considered statistically significant.
Results
The cohort included 125 patients, diagnosed at admission with sepsis (n = 35; 28%) or septic shock (n = 90; 72%). Out of the 125 patients, 70 (56%) were discharged in improved condition and 55 (44%) died. Among the deceased, 15 (12% of the total cohort; 42.9% of the sepsis group) were initially admitted with sepsis, and 40 (32% of the total cohort; 44.4% of the septic shock group) with septic shock. At 28 days, overall mortality reached 36% (45 out of 125 patients). The 28-day mortality was 31.43% (11 out of 35) among patients with sepsis and 37.78% (34 out of 90) among those with septic shock. The annual distribution of cases was 27 (21.6%) in 2020 and 98 (78.4%) in 2021, with the lower frequency in 2020 attributed to the onset of the COVID-19 pandemic, during which a significant decrease in surgical admissions was recorded. Age ranged between 22 and 89 years; the mean age (±SD) was 65.14±14.75 years overall, 64.77±15.68 in the sepsis group, and 65.28±14.46 in the septic shock group. Sex distribution indicated a male predominance (n=70; 56%) compared to female (n=55; 44%), while the place of residence was balanced (urban n=62; 50.4% vs rural n=63; 49.6%). Baseline demographic and clinical characteristics of the study population are summarized in Table 1.
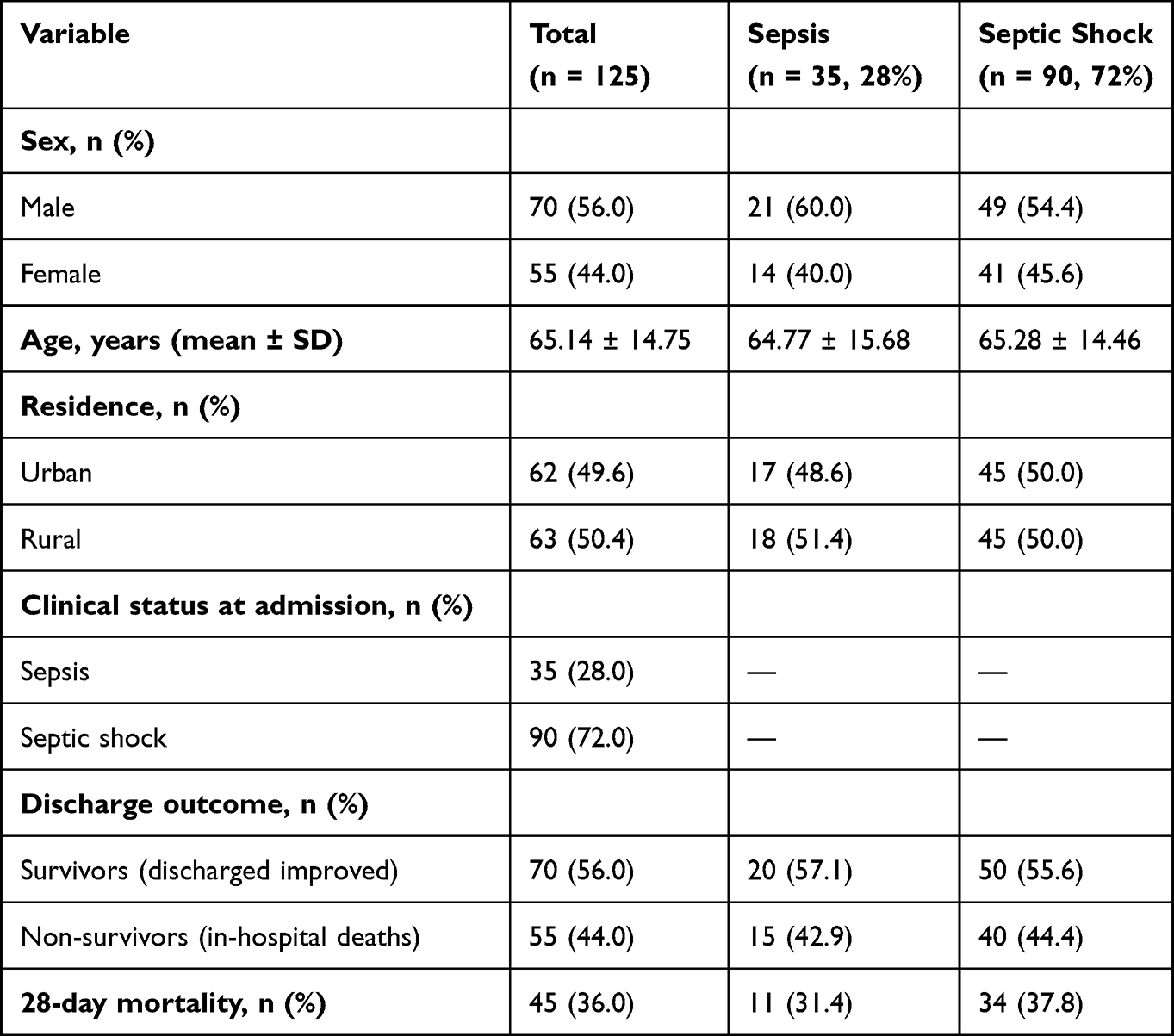 |
Table 1 Baseline Characteristics of the Study Population |
Chronic comorbidities were highly prevalent in this surgical sepsis cohort. The most common category was cardiovascular disease, present in 63 out of 125 patients (50.4%), followed by diabetes mellitus (30/125, 24.0%), oncologic disease (20/125, 16.0%), cerebrovascular disease (16/125, 12.8%), chronic kidney disease (16/125, 12.8%), chronic liver disease (16/125, 12.8%), psychiatric or neurologic disorders (13/125, 10.4%), and chronic respiratory disease (6/125, 4.8%). Only 18 patients (14.4%) had no recorded chronic comorbidities. When stratified by outcome, cardiovascular disease was present in 44.3% of survivors and 58.2% of non-survivors, while diabetes mellitus was documented in 22.9% versus 25.5%, respectively. Cerebrovascular disease occurred in 7.1% of survivors and 20.0% of non-survivors, and psychiatric/neurologic disorders in 7.1% versus 14.5%. Oncologic disease was identified in 11.4% of survivors and 21.8% of non-survivors, whereas chronic liver disease was present in 10.0% vs 16.4%, and chronic kidney disease in 12.9% vs 12.7%. Chronic respiratory disease was less frequent in both groups (2.9% vs 7.3%). Although cerebrovascular and oncologic comorbidities tended to be more frequent among non-survivors, no individual comorbidity category reached statistical significance in the survivors versus non-survivors comparison (all p > 0.05; Table 2).
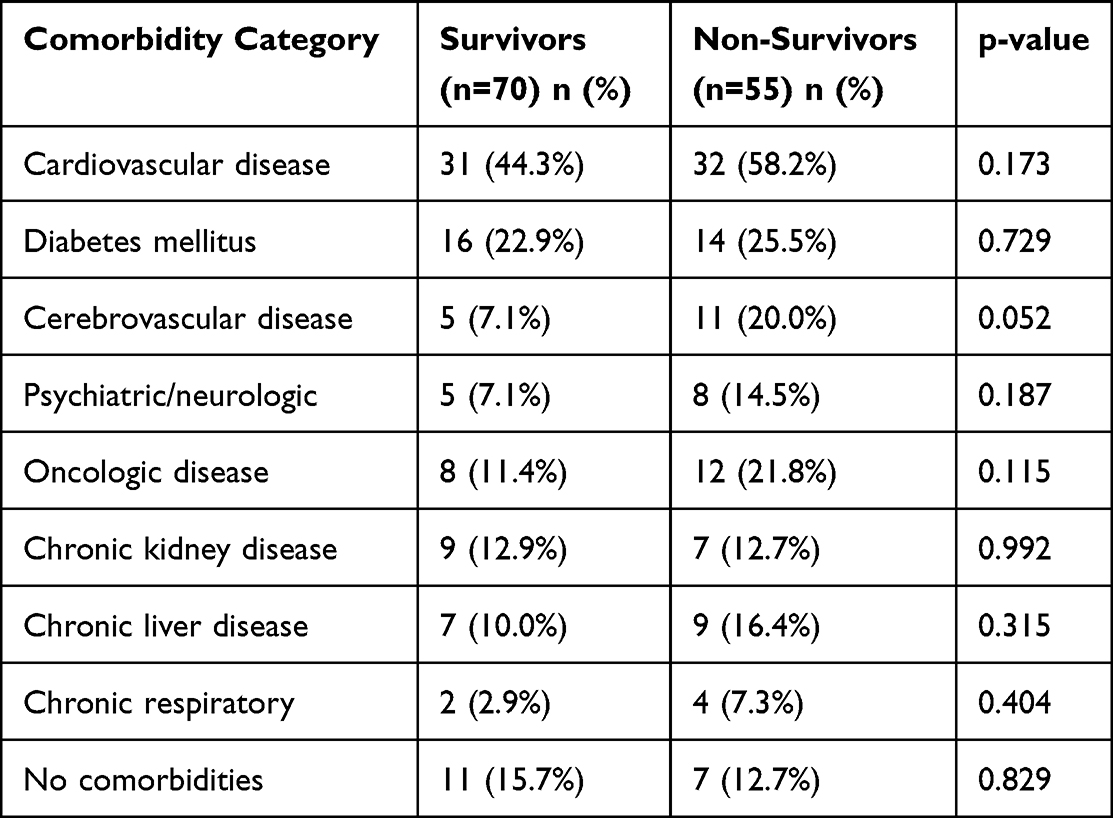 |
Table 2 Distribution of Chronic Comorbidities in the Survivors and Non-Survivors |
The majority of patients were admitted to the Department of General Surgery (n = 81, 64.8%), followed by Urology (n = 21, 16.8%), Thoracic Surgery (n = 9, 7.2%), Gynecology (n = 5, 4.0%), and smaller proportions from Vascular Surgery, Orthopedics, and Otorhinolaryngology (n = 3, 2.4% each). Regarding the anatomical site of infection, the most frequent localization was abdominal (n = 67, 53.6%), followed by urinary tract (n = 20, 16.0%), soft tissue or cutaneous/subcutaneous infections (n = 13, 10.4%), pulmonary (n = 11, 8.8%), anorectal (n = 6, 4.8%), pelvic/genital (n = 5, 4.0%), and ear–nose–throat (n = 3, 2.4%) sites. A detailed distribution of infection sites among survivors and non-survivors is presented in Table 3. This cohort consisted exclusively of surgical patients with sepsis or septic shock, which characterizes the present dataset as a derivation cohort rather than a validation cohort.
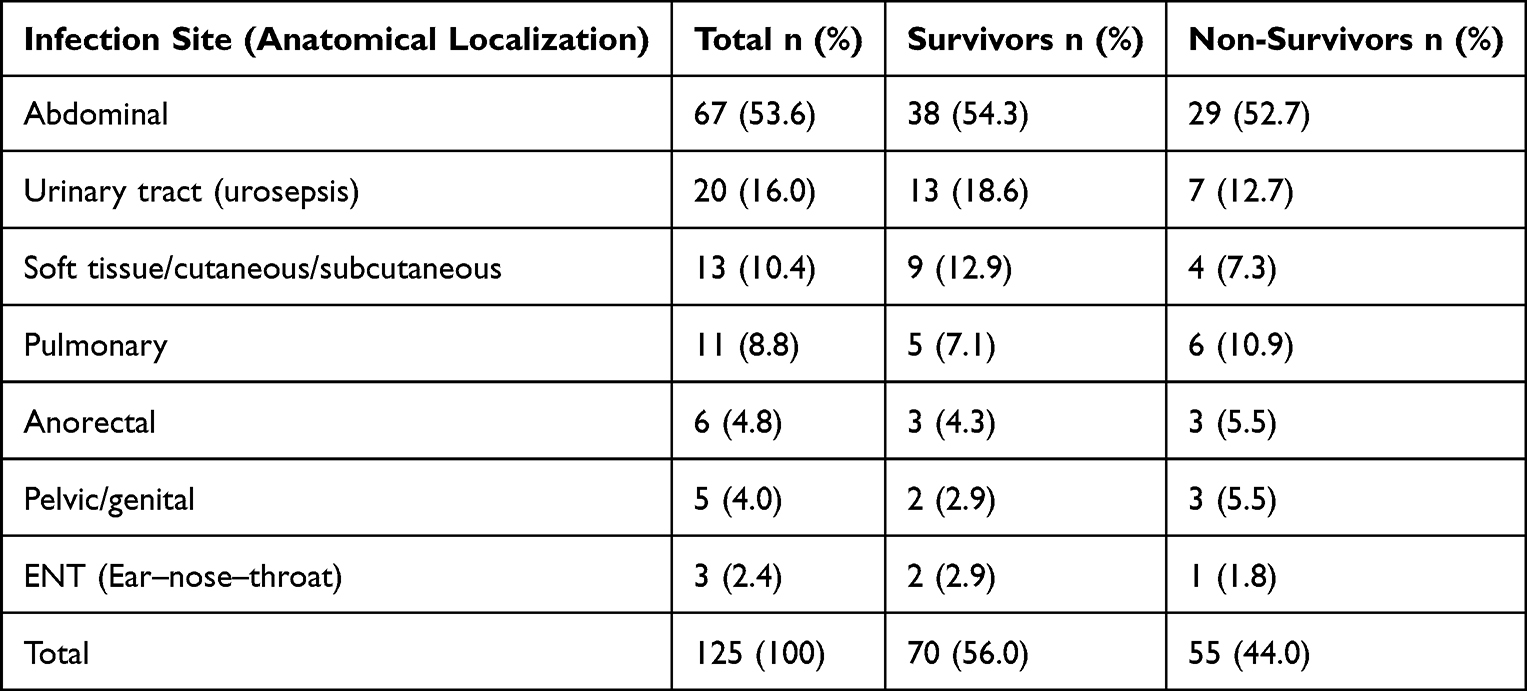 |
Table 3 Distribution of Infection Sites Among Survivors and Non-Survivors |
We analyzed the means and standard deviations of PCT, NLR, INR, and SOFA score at admission, in the total cohort and in both groups, as shown in Table 4. As SOFA values were non-normally distributed, we additionally report the median and interquartile range, which were 6 (IQR 3–9) for the overall cohort, 6 (IQR 2.5–9) in sepsis, and 6 (IQR 3–9) in septic shock.
 |
Table 4 Descriptive Statistics for the Biomarkers PCT, NLR, INR, and SOFA Score |
To assess the prognostic contribution of individual biomarkers, we also stratified patients by 28-day survival status. In addition to ROC-based analyses, we compared admission biomarker values between survivors and non-survivors. Median PCT levels at admission were similar in survivors and non-survivors (26.77 [IQR 8.78–42.48] vs 18.27 [IQR 9.09–32.77] ng/mL, p = 0.662), and the same held true for the neutrophil-to-lymphocyte ratio (11.21 [7.56–20.76] vs 12.15 [6.46–20.55], p = 0.750). By contrast, INR measured early in the postoperative or ICU stay was significantly higher in non-survivors than in survivors (2.39 [1.56–3.08] vs 1.51 [1.30–1.78], p < 0.001), supporting the prognostic relevance of sepsis-associated coagulopathy (Table 5). These findings are consistent with the ROC results, where PCT, NLR and especially INR displayed significant but individually imperfect prognostic accuracy, and they further underscore the rationale for integrating these markers into composite bioscores.
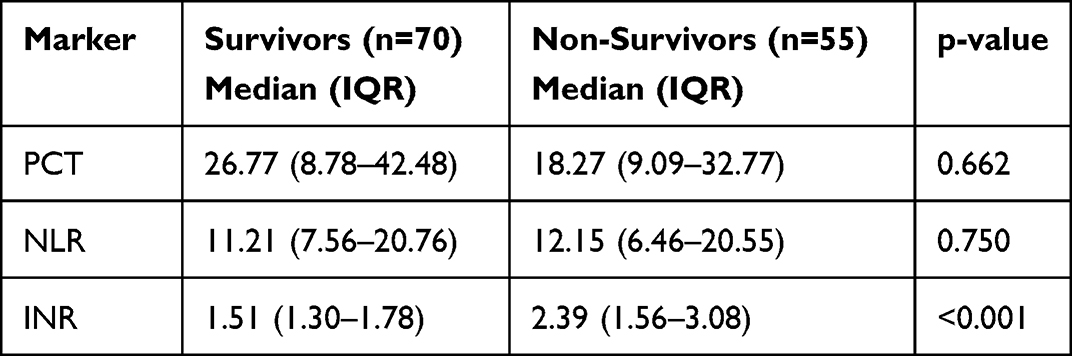 |
Table 5 Comparison of Individual Biomarkers Between Survivors and Non-Survivors |
Based on the score assigned to each patient according to the values of PCT, NLR, INR, and SOFA score, we calculated the final score, ie, the bioscore value per patient. We next determined the mean values of BIO-S and BIO-SC, which were markedly higher in patients with septic shock than in those with sepsis. At admission, the mean BIO-S reached 23.89 ± 4.34 in the septic shock group, compared to 12.68 ± 4.35 in the sepsis group (p < 0.001). Similarly, the BIO-SC score was much higher in patients with shock (28.41 ± 5.61 vs 16.2 ± 5.53 points in sepsis; p < 0.001). These descriptive data indicate a considerably higher initial severity in septic shock, captured by the elevated BIO-S and BIO-SC values, as shown in Table 6.
 |
Table 6 Descriptive Statistics for the BIO-S and BIO-SC Scores |
Table 7 and Figure 1 show the results of the ROC analysis evaluating the prognostic performance of the BIO-S score for predicting 28-day mortality, where a cut-off of 22 was identified for the entire cohort (AUC = 0.930; sensitivity = 0.945; specificity = 0.743). When analyzed separately by clinical severity, mortality prediction remained consistent, with optimal cut-offs of 12 for patients with sepsis (AUC = 0.943; sensitivity = 1.00; specificity = 0.850) and 24 for those with septic shock (AUC = 0.932; sensitivity = 0.900; specificity = 0.880).
 |
Table 7 Prognostic ROC Analysis of BIO-S for 28-Day Mortality |
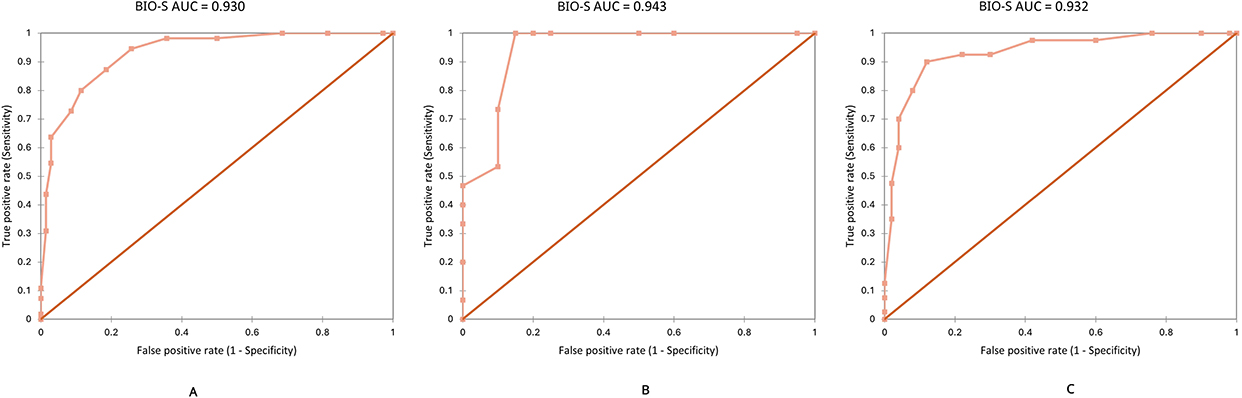 |
Figure 1 Prognostic ROC curves showing the AUC values of the BIO-S score for predicting 28-day mortality in all patients (A), in patients with sepsis (B), and in those with septic shock (C). |
Table 8 and Figure 2 present the results of the ROC analysis assessing the prognostic performance of the BIO-SC score for predicting 28-day mortality, where a cut-off of 28 was identified for the entire cohort (AUC = 0.942; sensitivity = 0.836; specificity = 0.914). When analyzed separately by clinical severity, mortality prediction remained consistent, with optimal cut-offs of 15 for patients with sepsis (AUC = 0.958; sensitivity = 0.867; specificity = 0.900) and 29 for those with septic shock (AUC = 0.947; sensitivity = 0.875; specificity = 0.900).
 |
Table 8 Prognostic ROC Analysis of BIO-SC for 28-Day Mortality |
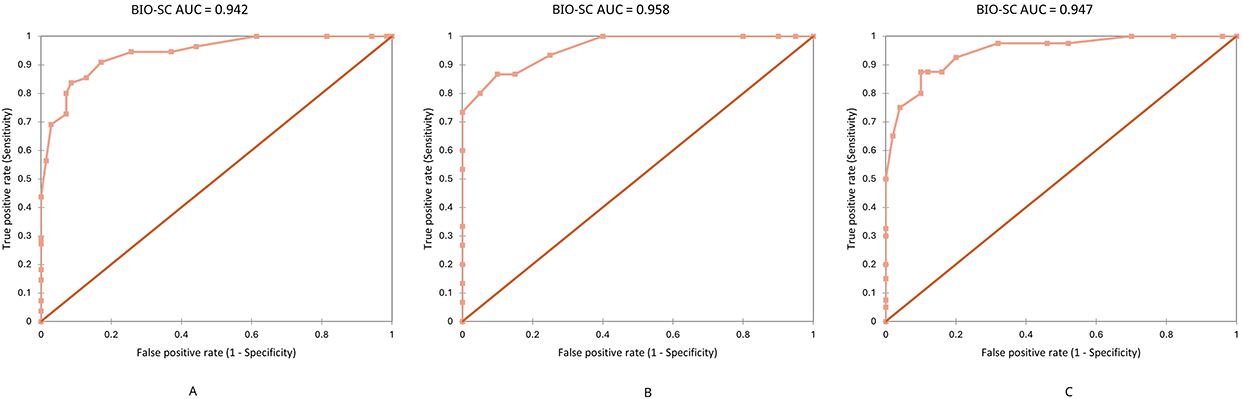 |
Figure 2 Prognostic ROC curves showing the AUC values of the BIO-SC score for pre-dicting 28-day mortality in all patients (A), in patients with sepsis (B), and in those with septic shock (C). |
The prognostic discrimination of the models was slightly attenuated in the aggregated cohort compared to analyses stratified by clinical severity, for both BIO-SC and BIO-S. Thus, for BIO-SC we obtained an AUC = 0.942 in the entire cohort, versus 0.958 in the sepsis group and 0.947 in the septic shock group; for BIO-S, AUC = 0.930 in the entire cohort, compared with 0.943 in the sepsis group and 0.932 in the septic shock group. These differences can be explained by case heterogeneity and cross-comparisons when pooling data (deaths from septic shock vs survivors from sepsis and vice versa), which reduce overall score separation—a typical “spectrum effect”. These findings support reporting AUC values and thresholds stratified by clinical severity (sepsis vs septic shock) and, optionally, estimating a stratum-standardized AUC, which more accurately reflects intra-group prognostic discrimination. Cut-off values were derived from ROC analysis, identifying the optimal balance between sensitivity and specificity. These thresholds were subsequently applied for Kaplan–Meier risk stratification and Cox regression to evaluate 28-day mortality prediction. Beyond predictive accuracy, model calibration was evaluated to assess the agreement between predicted and observed mortality probabilities.
Calibration analysis of the prognostic models (BIO-S and BIO-SC) confirmed good agreement between predicted and observed 28-day mortality. For BIO-S, the Hosmer–Lemeshow goodness-of-fit test yielded χ2=4.96 with 8 degrees of freedom (p=0.76) and a Brier score of 0.127. For BIO-SC, the Hosmer–Lemeshow statistic was χ2=6.66 (df=8, p=0.57) with a Brier score of 0.119, indicating adequate overall calibration for both models.
The prognostic performance analysis showed that both bioscores effectively predicted 28-day mortality, with higher AUC values reflecting increased mortality risk in patients with more severe disease. The obtained AUCs demonstrate high accuracy in differentiating mortality risk across severity levels, indicating that BIO-S and BIO-SC consistently stratify patients according to short-term outcomes. These findings emphasize the potential of both bioscores as practical tools for prognostic assessment and mortality prediction in sepsis.
We compared AUCs between the BIO-SC score and the other clinical scores using the DeLong statistical test (approximated by paired t-test), which showed significant differences between BIO-SC and the other scores used in practice. BIO-SC demonstrated a significantly higher AUC compared to BIO-S (p = 0.00026), SOFA (p = 1.37×10−6), and APACHE II (p = 1.80×10−15), confirming its superior performance in risk stratification and mortality prediction in patients with sepsis and septic shock (Table 9).
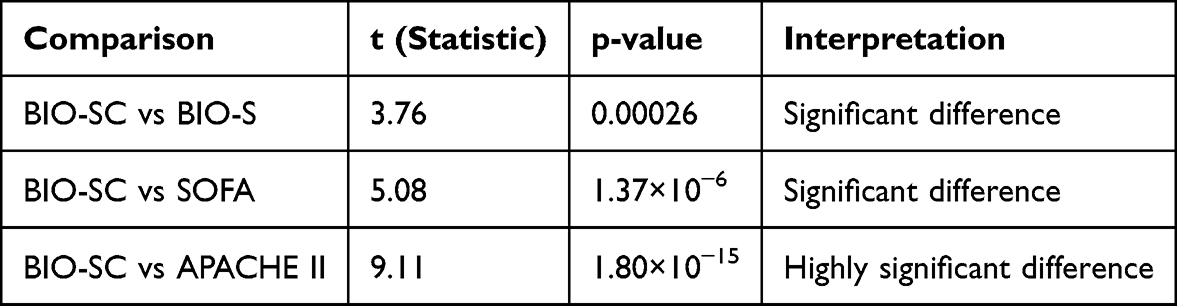 |
Table 9 Comparison of AUC Between the BIO-SC and BIO-S, SOFA, and APACHE II Using the DeLong Test |
Regarding prognostic value, strong correlations were observed between the BIO-S/BIO-SC scores and patient outcomes. Both BIO-S and BIO-SC were significantly associated with discharge status, with higher scores being linked to a greater likelihood of death. The Pearson correlation coefficient between BIO-S and survival was r = 0.739 (p < 0.001), and for BIO-SC r = 0.767 (p < 0.001), indicating a strong (and significant) positive correlation with mortality. In other words, patients who died had higher initial bioscore values, particularly BIO-SC, which showed the strongest correlation with discharge status. In addition, BIO-S and BIO-SC were found to correlate strongly with the existing SOFA and APACHE II scores, reflecting that they measure similar aspects of severity. For example, BIO-S showed the strongest correlation with the SOFA score (r ≈ 0.94), which is expected given that both primarily reflect acute organ dysfunction. BIO-SC demonstrated a somewhat weaker correlation with SOFA (r ≈ 0.83), consistent with the addition of the Charlson Comorbidity Index (CCI), which introduces chronic disease burden into the score and reduces direct collinearity with acute severity measures.
In the ROC analysis for predicting 28-day mortality, the composite bioscores BIO-SC and BIO-S demonstrated the highest predictive accuracies, with AUCs of 0.942 (95% CI: 0.913–0.971) and 0.930 (95% CI: 0.904–0.957), respectively. Both scores slightly outperformed the prognostic capacity of SOFA (AUC = 0.928; 95% CI: 0.895–0.961) and, to a greater extent, that of APACHE II (AUC = 0.918; 95% CI: 0.876–0.959). The differences between the AUCs of BIO-S, BIO-SC, SOFA, and APACHE II are illustrated in Figure 3. Individual ROC analyses for the main biomarkers included in the composite models showed that procalcitonin (PCT) had the highest individual prognostic accuracy (AUC = 0.872; 95% CI: 0.819–0.925), followed by NLR (AUC = 0.801; 95% CI: 0.742–0.859), and INR (AUC = 0.776; 95% CI: 0.711–0.841). Both composite bioscores and all individual biomarkers and conventional scores reached statistical significance (p < 0.05), with the composite models demonstrating the highest overall predictive accuracy through the integration of inflammatory, coagulation, and organ dysfunction parameters.
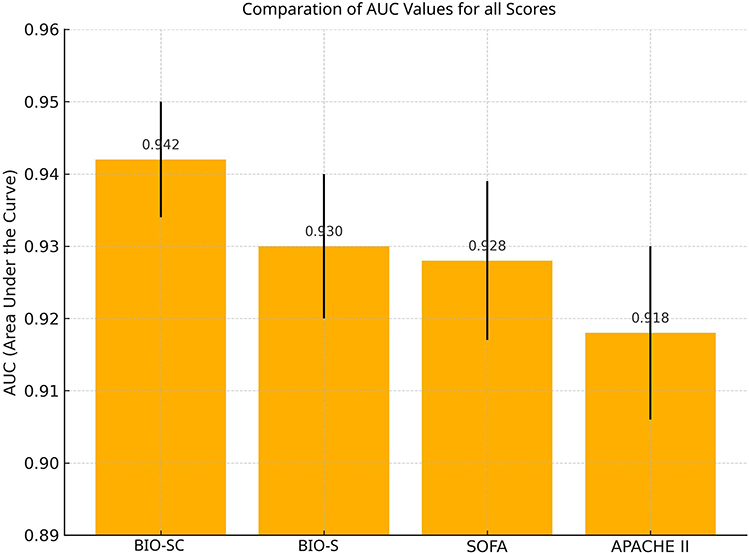 |
Figure 3 Comparison of AUC for all scores evaluated in the study. |
Multivariate Cox regression analysis identified BIO-S and BIO-SC as strong independent predictors of 28-day mortality (Table 10 and Figure 4). Each 1-point increase in BIO-S was associated with a 28% higher hazard of death (HR = 1.28, 95% CI: 1.11–1.48, p = 0.0006), while each additional point in BIO-SC increased mortality risk by 29% (HR = 1.29, 95% CI: 1.17–1.57, p = 0.0003). Among conventional clinical scores, only SOFA retained statistical significance (HR = 1.18, 95% CI: 1.02–1.36, p = 0.023), whereas APACHE II, age, sex, septic shock status, and CCI did not retain independent associations with mortality after inclusion of the composite bioscores and SOFA and were removed during the stepwise elimination process (all p > 0.05 for these variables in the initial model). This finding is consistent with the expected clinical collinearity between septic shock status, global severity scores, and the composite bioscores. These results demonstrate that BIO-S and BIO-SC provide superior prognostic value compared with traditional clinical scores.
 |
Table 10 Coefficients and Standard Errors (SE) for the BIO-S and BIO-SC Scores |
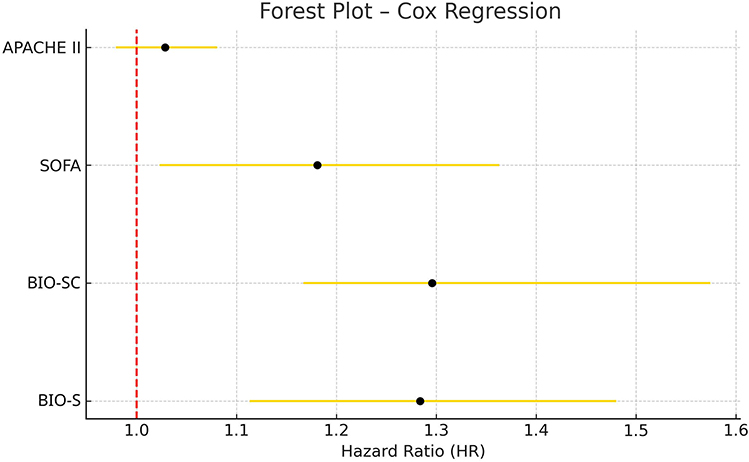 |
Figure 4 Forest plot diagram of Cox regression including the multivariable models BIO-S, BIO-SC, SOFA, and APACHE II. |
Risk stratification thresholds for BIO-S and BIO-SC were defined using ROC-derived optimal cut-offs (Youden index) for 28-day mortality, and the resulting low, moderate, and high-risk categories exhibited clear mortality gradients within the cohort (Tables 11 and 12).
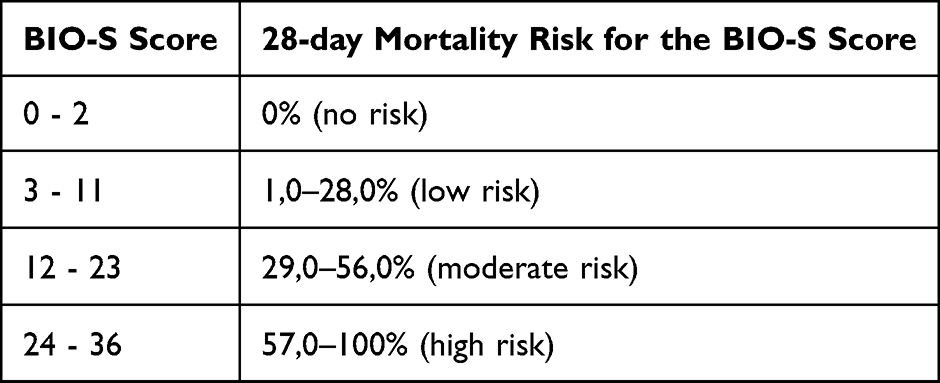 |
Table 11 Score and Risk Rate for the BIO-S Score |
 |
Table 12 Score and Risk Rate for the BIO-SC Score |
The 28-day survival analysis in the entire cohort, performed with Kaplan–Meier curves (Figures 5 and 6) based on risk groups defined by BIO-S and BIO-SC values, showed significant differences between risk categories (log-rank p < 0.001). Survival decreased progressively from low-risk to high-risk groups, confirming the value of risk stratification based on the bioscores. For example, patients classified as high-risk by BIO-S (score ≥ 24) had significantly reduced survival, with observed mortality ranging from 57–100%, compared with nearly 0% in the no-risk group (score 0–2). A similar pattern was seen with BIO-SC, where high-risk patients (score ≥ 29) had mortality between 59–100%, while those in the low-risk category (score 0–2) showed almost no deaths. These data clearly illustrate the ability of BIO-S and BIO-SC to stratify patients according to prognosis and to identify those at higher risk of adverse outcomes.
 |
Figure 5 Kaplan–Meier survival curves for 28-day mortality according to BIO-S risk stratification in patients with sepsis and septic shock. |
 |
Figure 6 Kaplan-Meier survival curves at 28 days according to BIO-SC risk stratifica-tion in patients with sepsis and septic shock. |
The newly developed BIO-S and BIO-SC scores have proven to be valuable tools in the prognostic assessment of patients with sepsis and septic shock. They demonstrate superior performance compared with classical scores such as SOFA and APACHE II in predicting 28-day mortality. BIO-SC, which integrates chronic comorbidities (CCI) alongside inflammatory biomarkers and organ dysfunctions, showed the best overall prognostic accuracy. Nevertheless, BIO-S, based on inflammatory biomarkers and SOFA, also demonstrated strong predictive ability, emphasizing the advantage of combining biological markers with severity scores. Overall, incorporating these bioscores into the evaluation of septic patients may enhance risk stratification and support clinical decision-making, highlighting their added prognostic value compared with traditional tools.
Discussion
Our investigation introduced and assessed two novel bioscores, BIO-S and BIO-SC, aimed at stratifying sepsis and septic shock patients. They demonstrated consistent prognostic value and outperformed conventional clinical scoring systems in predicting 28-day mortality and overall outcome accuracy. For example, BIO-SC achieved the highest area under the ROC curve (AUC = 0.942) for predicting 28-day mortality, closely followed by BIO-S (AUC = 0.930) and the SOFA score (0.928); in contrast, the APACHE II score had the weakest performance (AUC = 0.918). The superiority of the BIO-SC score over traditional clinical scores was further supported by the direct statistical analysis of differences between AUCs. The DeLong test highlighted significant differences in favor of BIO-SC, both compared to classical scores (SOFA, APACHE II) and compared to BIO-S (its version without CCI). Although the AUC differences between the proposed bioscores and SOFA were relatively small, the consistent trend was in favor of BIO-SC, suggesting that it captures additional prognostic factors beyond traditional scores. It is noteworthy that the differences with APACHE II were the most pronounced, indicating that composite scores based on biomarkers, organ dysfunction, and comorbidities may replace or even surpass older, more general models. This finding is consistent with recent literature showing that combining multiple biomarkers into a composite score can outperform classical scoring systems in predicting mortality in septic patients.23,25,31
The selection of biomarkers for the BIO-S and BIO-SC models was guided by their complementary pathophysiological roles and practical clinical availability. Procalcitonin (PCT) was included because it remains the most validated indicator of systemic bacterial infection and sepsis severity, reflecting cytokine-mediated activation of the CALC-1 gene during infection. The neutrophil-to-lymphocyte ratio (NLR) captures the dynamic balance between innate immune activation and adaptive immune suppression, serving as an integrative marker of immune dysregulation and cellular stress. INR reflects sepsis-induced coagulopathy, a frequent consequence of systemic inflammation and endothelial injury. Compared with fibrinogen or D-dimers, INR offers greater standardization, is routinely available in all hospital laboratories, and correlates directly with the degree of hepatic and endothelial dysfunction.
In addition to pathophysiological relevance, the selection of biomarkers also considered their standardized analytical availability within the laboratory workflow. In our center, these parameters (PCT, NLR, and INR) are processed in the clinical laboratory, automatically integrated into the LIS, and subjected to internal quality control procedures. By contrast, other biomarkers potentially useful in sepsis, such as lactate or presepsin, are measured selectively using point-of-care devices in the ICU, without LIS integration and without continuous quality control programs, which limits their use in retrospective models. In this regard, the absence of lactate or presepsin does not reflect a conceptual exclusion but rather the realities of local analytical infrastructure. For future research, other bioscore models may incorporate biomarkers such as lactate or presepsin, either alongside the current parameters or replacing some of them when the analytical infrastructure allows, although their inclusion should prioritize parameters processed in clinical laboratories with quality control systems in order to preserve the prognostic validity of the models.
From a practical perspective, CRP (although widely accessible) was excluded because of its limited specificity in bacterial infections and elevation in non-infectious inflammatory states, while novel biomarkers such as presepsin (PSP), although promising, are not yet available in our laboratory. Together, these markers address three major biological axes of the septic response: infection and inflammation (PCT), immune dysregulation (NLR), and coagulation–organ failure interaction (INR). Their integration within the BIO-S model, and subsequent expansion through comorbidity burden in BIO-SC, was designed to provide a multidimensional reflection of sepsis severity and mortality risk, rather than reliance on a single biomarker.
Indeed, the concept of combining multiple biomarkers to improve predictive accuracy is supported by numerous studies. For example, Liu et al reported that a simple bioscore combining procalcitonin (PCT), B-type natriuretic peptide (BNP), and lymphocyte percentage significantly increased the prognostic accuracy for postoperative sepsis (AUC = 0.914), surpassing each biomarker individually.32 Similarly, Gibot et al developed a bioscore based on three biomarkers (neutrophil CD64 index, PCT, and sTREM-1), which demonstrated high prognostic performance for sepsis outcomes, superior to any single marker, and validated these results in an external patient cohort.33 Sakyi et al proposed a bioscore composed of presepsin, PCT, and hs-CRP, evaluated in a case–control study on pediatric patients, where the AUCs were 0.787 (PCT), 0.784 (hs-CRP), and 0.748 (presepsin). Combined biomarkers modestly improved prognostic discrimination, with the pair PCT + hs-CRP showing the best predictive value (AUC = 0.801), while the triplet PCT + sCD14-ST + hs-CRP yielded a slightly lower AUC (0.770).34 Rondović et al monitored serum biomarkers at three time points (days 1, 3, and 5) and compared both individual biomarkers and clinical scores (SOFA, SAPS II, APACHE II) in an adult cohort with secondary sepsis. Presepsin predicted outcomes from day 1 (AUC = 0.670), and on day 3, presepsin, MPV, and lactate had AUCs of 0.716, 0.667, and 0.642, respectively. The composite bioscore (presepsin + MPV + lactate) on day 3 achieved an AUC of 0.820, outperforming both individual biomarkers and established clinical scores.35
By comparison, our bioscores showed high prognostic accuracy for 28-day mortality, comparable or superior to previous bioscore models, which often focused on early sepsis diagnosis rather than mortality prediction. Zhang et al proposed a composite model conceptually similar to BIO-SC, integrating CCI, SOFA, and PCT, which, in a cohort of 118 ICU patients with sepsis, proved superior to classical scoring systems and individual inflammatory markers. The individual AUCs were 0.712 (CCI), 0.801 (SOFA), and 0.889 (PCT), while the combined model (CCI + SOFA + PCT) reached an AUC of 0.943 (sensitivity 91.7% and specificity 83.0%) for 28-day mortality prediction.25 These results are remarkably close to our findings for BIO-SC (AUC = 0.942), providing convergent validation that integrating comorbidities (CCI) with severity scores and biomarkers (eg, PCT) increases the prognostic power for mortality.
Beyond their prognostic value, BIO-S and BIO-SC also correlated strongly with disease severity and organ dysfunction at admission. As expected, patients who presented with septic shock had significantly higher scores than those with non-shock sepsis, reflecting the close association between these bioscores and the extent of organ failure. In clinical application, BIO-S and BIO-SC reliably identified patients at higher risk of poor outcomes, serving as indicators of increased mortality risk. This ability to capture the severity of the underlying pathophysiological process highlights their usefulness as early indicators of increased mortality risk, supporting timely clinical prioritization. Notably, other multimarker approaches have also demonstrated prognostic relevance in relation to sepsis severity. For instance, a recent study combining pro-inflammatory cytokines (IL-6, IL-8) and heparin-binding protein (HBP), with or without albumin, showed improved prognostic accuracy compared with the SOFA score for predicting outcomes in sepsis and septic shock,36 further supporting the benefit of integrating multiple biological parameters to refine mortality risk prediction.
In our cohort, the individual biomarkers included in the bioscores showed heterogeneous associations with 28-day mortality when assessed separately. Admission procalcitonin (PCT) and neutrophil-to-lymphocyte ratio (NLR) did not differ significantly between survivors and non-survivors, reflecting substantial overlap in distribution between outcome groups, consistent with previous evidence that both markers demonstrate prognostic value at population level but limited stand-alone discrimination at the bedside.7,11,20 By contrast, INR values measured within the first hours after admission were markedly higher in non-survivors, highlighting the prognostic relevance of early sepsis-associated coagulopathy.17,21 Taken together, these findings reinforce the concept that no single biomarker provides sufficient prognostic discrimination, whereas integrating complementary biological dimensions of sepsis (infection, immune dysregulation, coagulation and comorbidity burden) into composite bioscores yields markedly improved risk stratification, in line with prior studies evaluating multimarker approaches.31–33,35
Interestingly, SOFA values at admission were similar between sepsis and septic shock patients in our cohort. This finding likely reflects the physiological profile of surgical sepsis, where non-cardiovascular organ dysfunction (renal, hepatic or respiratory) may already be present in severe sepsis without vasopressor requirement, whereas some shock patients may be admitted earlier with predominant cardiovascular compromise but limited multi-organ involvement. As SOFA is a composite score that integrates six organ systems, the cardiovascular component alone does not necessarily increase the total score in shock to a degree that separates it from severe sepsis.
Comparative analysis also indicated close relationships between our bioscores and existing clinical scores. BIO-S, in particular, correlated very strongly with the SOFA score (r ≈ 0.94), which was expected since both reflect acute organ dysfunctions. BIO-SC showed a somewhat weaker correlation with SOFA (r ≈ 0.83), but it surpassed BIO-S in correlation with patient outcome (discharge status, ie, survival/death). We observed that BIO-SC had a higher Pearson correlation coefficient with survival compared to BIO-S (r = 0.767 vs r = 0.739), meaning that including the Charlson Comorbidity Index (CCI) in the calculation of BIO-SC enhanced its prognostic relevance. Compared to BIO-S, the weaker correlation of BIO-SC with SOFA reflects the fact that SOFA captures only acute organ dysfunction, whereas BIO-SC incorporates baseline physiological vulnerability through comorbidities. This additional dimension explains why BIO-SC correlates more strongly with 28-day mortality despite a looser association with SOFA, as confirmed by the modest increase in AUC (from 0.930 to 0.942) and the higher Pearson correlation with outcome.
Although no single chronic disease category showed a statistically significant association with 28-day mortality, the cumulative burden of chronic illness contributed to overall prognosis. This effect is captured at the global level by comorbidity indices such as CCI and incorporated into composite models such as BIO-SC, providing prognostic information that is independent of acute organ dysfunction. While SOFA reflects short-term physiological failure, CCI captures chronic baseline vulnerability such as cardiovascular disease, diabetes, malignancy or renal impairment, all of which modulate a patient’s physiological reserve and ability to recover from sepsis. This is particularly relevant in elderly surgical patients, in whom mortality frequently reflects the combined impact of sepsis and pre-existing comorbidities rather than acute organ failure alone. By incorporating CCI, BIO-SC better discriminates patients with limited baseline reserve, thereby enhancing prognostic accuracy in cohorts where chronic disease burden is a major determinant of outcome. A recent study showed that in a significant proportion of fatal sepsis cases, pre-existing comorbidities contributed substantially to mortality, with death solely attributable to sepsis (in the absence of major comorbidities) being a rare event.37 Therefore, integrating CCI into BIO-SC aligns the score with the clinical reality of elderly patients with multiple diseases, enhancing the accuracy of mortality risk estimation. BIO-SC succeeds in more faithfully capturing vital risk, particularly in patients with comorbidities, compared to its version without CCI (BIO-S). Furthermore, other authors have also sought to improve prognostic prediction by including chronic factors alongside acute ones; for example, Shukeri et al derived a bioscore combining age, SOFA subscores for the central nervous system and liver, plus IL-6 at admission, achieving very good performance (AUC = 0.814) for predicting 30-day mortality,38 which highlights that enriching scores with comorbidity or immune response data can increase their prognostic capacity.
Another important finding is that both bioscores proved to be independent predictors of 28-day survival. In the multivariate Cox regression model (which included the bioscores simultaneously and accounted for clinical status, sepsis vs septic shock), only BIO-S and BIO-SC remained significant; each 1-point increase in these scores was associated with an approximate 28–29% increase in the hazard of death at 28 days. This aspect is particularly relevant: even after accounting for the presence of septic shock (a well-known major risk factor), the value of the BIO-S/BIO-SC scores added additional prognostic information. In other words, the bioscores can distinguish patients with more severe prognosis even within the same clinical category, for example identifying patients with septic shock at extremely high risk versus those with septic shock at moderate risk, or analogously within the sepsis group. This fine stratification capacity underscores the practical utility of the scores: they not only reflect severity (like SOFA) but also anticipate mortality risk more accurately than simply labeling a patient as “septic shock” or not. In the literature, increasing emphasis is placed on such stratification tools: Shukeri et al, for example, showed that their new bioscore (included in multivariate analysis) significantly improved the ability to predict mortality compared to usual scores, indicating that such a composite index captures risk beyond standard clinical factors.38
Early prognostic stratification provided by BIO-S and BIO-SC offers a structured overview of disease severity and expected outcomes, facilitating more consistent clinical decision-making without requiring additional diagnostic resources. In particular, the clinical implications are especially relevant for BIO-SC. Given its high specificity (0.914) at the optimal threshold (≥28), BIO-SC can function as an effective rule-in tool for identifying patients with substantially elevated mortality risk who may benefit from early ICU referral, intensified monitoring, or expedited source control. Conversely, patients classified in the low-risk BIO-SC category exhibited negligible 28-day mortality in our cohort, suggesting that BIO-SC may also inform de-escalation strategies by identifying low-risk surgical sepsis patients in whom aggressive or resource-intensive interventions can be safely avoided. This dual applicability, combining targeted escalation for high-risk patients and potential de-escalation in low-risk strata, underscores the added clinical value of BIO-SC beyond its discriminatory performance.
The advantage of BIO-S and BIO-SC is that they condense into a single value diverse patient information (clinical parameters, laboratory values, and comorbidity history), facilitating rapid communication between specialists and providing an overview of risk. Moreover, these scores could be integrated into hospital electronic systems as decision-support tools for sepsis management. Given their demonstrated accuracy, BIO-S and BIO-SC are well-suited to be included as key variables in advanced predictive algorithms for sepsis prognosis and outcome monitoring. Implementability is high: the scores rely only on standard tests and instruments, can be manually calculated or integrated into electronic health records (EHR), without advanced infrastructure or opaque algorithms. For instance, an automated alert system could be implemented to use bioscore values (together with other real-time parameters) to generate alarms of sepsis worsening before clinical decline becomes evident. Unlike opaque “black-box” prediction models, our scores have the advantage of clinical interpretability: physicians can easily understand which elements compose the score and how they contribute to risk, which could increase trust in computer-assisted decisions. In parallel, artificial intelligence and machine learning–based approaches may incorporate these bioscores or their component variables to enhance prognostic modeling and individualized risk stratification in sepsis, although such integration remains exploratory pending external validation.39,40 In essence, BIO-S and BIO-SC may represent a bridge between clinical score–based medicine and modern algorithmic approaches, combining high accuracy with ease of use in practice.
This study specifically focused on surgical sepsis, representing patients amenable to source control, a population often underrepresented in sepsis research but with high clinical relevance for perioperative decision-making. The analysis was intentionally centered on early evaluation, using parameters available at admission or within the first hours, to enhance the timeliness of prognostic assessment and therapeutic triage. The proposed bioscores (BIO-S and BIO-SC) integrate routinely available laboratory markers and clinical scores (PCT, NLR, INR, SOFA, CCI), thus capturing multidimensional aspects of inflammation, coagulopathy, organ dysfunction, and comorbidity burden. Their prognostic framework allows accurate estimation of 28-day mortality and risk stratification according to disease severity. The conclusions are reinforced by multiple complementary analyses (AUROC with confidence intervals, risk-category stratification, Kaplan–Meier survival curves, and Cox regression models), all supporting the same prognostic consistency and clinical relevance.
Given that the bioscores were developed in a homogeneous surgical sepsis population, the present dataset should be regarded as a model development (derivation) cohort. Consequently, broader validation in independent cohorts will be required to determine whether the prognostic thresholds identified in this study remain stable across different sepsis phenotypes.
The existence of actionable thresholds and easily interpretable risk categories (eg, BIO-S ≥ 24; BIO-SC ≥ 29) facilitates escalation of therapy and intensification of monitoring in appropriate patients. The results are consistent with the literature, which shows that composite models combining comorbidity, organ dysfunction, and inflammation outperform individual markers, while the single-center design with homogeneous protocols and Sepsis-3 definitions reduces inter-laboratory variability. Moreover, the low cost and reproducibility make them relevant even in resource-limited settings, supporting rapid bedside decisions.
The BIO-S and BIO-SC scores have proven to be valuable tools for prognostic risk stratification in surgical sepsis, demonstrating superior predictive power compared with conventional clinical scores. The inclusion of comorbidities in the BIO-SC model provided additional prognostic value for mortality prediction, emphasizing the major influence of pre-existing health status on sepsis outcomes. These findings have important clinical implications, paving the way for improved management of septic patients, either through the direct use of BIO-S and BIO-SC at the bedside or through the development of hybrid predictive models that integrate these bioscores with advanced clinical data analytics to more effectively anticipate and address this critical condition.
To assess the internal robustness of the proposed bioscores, a bootstrap validation procedure was performed with 1000 random resamples of the original dataset. The average optimism-adjusted AUC values for both BIO-S and BIO-SC differed by less than 0.02 from the apparent AUCs, confirming model stability and suggesting minimal overfitting. This internal validation supports the reproducibility of the findings within the present cohort.
Limitations and Future Directions
This study has several limitations that should be acknowledged. First, this is a single-center study restricted to surgical sepsis patients; therefore, the present cohort should be regarded as a model development dataset rather than a validation dataset. External multicenter validation, including medical ICU populations, will be required to confirm the reproducibility and stability of the proposed bioscore thresholds across different sepsis settings. A further limitation is that the optimal prognostic thresholds identified for BIO-S and BIO-SC were derived within the present cohort and may vary across external populations; therefore, threshold recalibration may be required during future validation. The predominance of abdominal sepsis and the frequent need for emergency surgical intervention may influence biomarker profiles differently than in non-surgical sepsis. Similar findings were reported by Liu et al, who analyzed postoperative sepsis and demonstrated the value of a biomarker-based bioscore in that specific context,32 whereas Yang et al observed distinct biomarker dynamics in mixed ICU cohorts.41 Second, the study period overlapped with the COVID-19 pandemic, when limited hospital access and delayed presentation often resulted in more severe disease at admission. This particular epidemiological context may have affected both patient characteristics and sepsis management, although the associations between bioscores and prognosis likely remain valid. Third, the cohort contained a relatively high proportion of patients with septic shock and a modest sample size, which may have attenuated the expected mortality gradient between sepsis and septic shock. Finally, the bioscore cut-off intervals were derived from both literature data and the distribution observed within this cohort, without external validation. While internal bootstrap validation supported the model’s robustness, external multicenter validation remains essential to confirm reproducibility and generalizability across diverse settings. It is worth noting that Gibot et al conducted external validation for their biomarker-based bioscore, confirming its robustness in an independent cohort.33
Despite these limitations, the study provides valuable preliminary evidence supporting the prognostic value of the BIO-S and BIO-SC scores in sepsis and septic shock. To establish their generalizability and clinical applicability, future prospective multicenter studies should include both surgical and medical ICUs and explore the potential need for recalibration in different patient populations (eg, varying comorbidity burdens or age profiles). Furthermore, expanding and refining the bioscore components through integration of novel molecular or genetic biomarkers, as well as analyzing dynamic trends over time rather than single admission values, could enhance predictive accuracy. In addition, integration with advanced computational approaches, such as AI-driven predictive algorithms, represents a promising direction for future validation and clinical implementation.
Conclusion
Individually, the biomarkers evaluated in this study, PCT, NLR and INR, as well as conventional severity scores such as SOFA and APACHE II, provided only limited and partially overlapping prognostic information, with sepsis-associated coagulopathy (reflected by INR) showing the clearest separation between survivors and non-survivors. However, when these parameters were integrated into composite bioscores, their prognostic performance improved substantially. The BIO-S score, which combines inflammatory biomarkers and organ dysfunction, and particularly the BIO-SC score, which additionally incorporates comorbidity burden through the Charlson Comorbidity Index, achieved high discriminatory power for short-term mortality and enabled clinically meaningful prognostic stratification in surgical sepsis.
These findings indicate that composite bioscores that aggregate infection, inflammation, coagulopathy, organ dysfunction and chronic vulnerability offer a more comprehensive depiction of sepsis severity than single biomarkers or traditional scores alone. In this context, BIO-S and especially BIO-SC can be regarded as practical decision-support tools for early prognostic assessment in surgical patients with sepsis or septic shock, helping to identify high-risk individuals who may benefit from early ICU referral and low-risk patients in whom resource-intensive interventions may be avoided. External multicenter validation will be required to confirm the generalizability of these bioscores and to refine their thresholds across different sepsis populations.
Data Sharing Statement
The information will be granted access to under reasonable request from the corresponding author.
Ethics Approval
This retrospective observational study was approved by the Ethics Committee of the “Sf. Apostol Andrei” County Emergency Clinical Hospital, Galați, Romania (registration number: 25060/05.10.2022). The database, including patients admitted between January 2020 and December 2021, was accessed and anonymized only after obtaining ethical approval. The Ethics Committee waived the requirement for individual informed consent due to the retrospective and non-interventional nature of the study. All procedures were performed in accordance with national regulations and the principles of the Declaration of Helsinki.
Author Contributions
George Țocu: Conceptualization, Methodology, Formal analysis, Writing – original draft, Supervision. Raul Mihailov: Data curation, Software, Validation, Visualization, Writing – review and editing. Valerii Luțenco: Methodology, Formal analysis, Data curation, Validation, Writing – review and editing. Florentin Dimofte: Supervision, Project administration, Methodology, Validation, Writing – review and editing. Bogdan Ioan Ștefănescu: Data curation, Formal analysis, Validation, Visualization, Writing – review and editing. Elena Niculeț: Methodology, Data curation, Validation, Writing – review and editing. Oana Mariana Mihailov: Formal analysis, Validation, Visualization, Writing – review and editing. Lavinia Țocu: Data curation, Software, Visualization, Writing – review and editing. Loredana Stavăr Matei: Project administration, Supervision, Validation, Writing – review and editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–21. doi:10.1001/jama.2016.0287
2. Gauer R, Forbes D, Boyer N. Sepsis: diagnosis and management. Am Fam Physician. 2020;101(7):409–418.
3. Tocu G, Stefanescu BI, Serban C, et al. Correlation between serum procalcitonin levels and 28-day mortality in patients with surgical sepsis and septic shock. Chirurgia. 2023;118(2):161–169. doi:10.21614/chirurgia.2838
4. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med. 2021;49(11):e1063–e1143. doi:10.1007/s00134-021-06506-y
5. Lutenco V, Beznea A, Mihailov R, et al. Literature review of prognostic factors in secondary generalized peritonitis. Life. 2025;15(6):880. doi:10.3390/life15060880
6. Wu R, Jiang H, Mao G, et al. Sepsis prognosis-related scoring standards: a comprehensive review. Biotarget. 2022;5:3. doi:10.21037/biotarget-21-5
7. Tocu G, Mihailov R, Serban C, Stefanescu BI, Tutunaru D, Firescu D. The contribution of procalcitonin, C-reactive protein, and interleukin-6 in the diagnostic and prognostic of surgical sepsis: observational and statistical study. J Multidiscip Healthc. 2023;16:2351–2359. doi:10.2147/JMDH.S422359
8. Duncan CF, Youngstein T, Kirrane MD, Lonsdale DO. Diagnostic challenges in sepsis. Curr Infect Dis Rep. 2021;23(10):22. doi:10.1007/s11908-021-00765-y
9. Li D, Wei Y, Zhang C, et al. Value of SOFA score, APACHE II score, and WBC count for mortality risk assessment in septic patients: a retrospective study. Medicine. 2025;104(17):e42464. doi:10.1097/MD.0000000000042464
10. Do SN, Dao CX, Nguyen TA, et al. Sequential organ failure assessment (SOFA) score for predicting mortality in patients with sepsis in Vietnamese intensive care units: a multicentre, cross-sectional study. BMJ Open. 2023;13(3):e064870. doi:10.1136/bmjopen-2022-064870
11. Wu H, Cao T, Ji T, Luo Y, Huang J, Ma K. Predictive value of the neutrophil-to-lymphocyte ratio in the prognosis and risk of death for adult sepsis patients: a meta-analysis. Front Immunol. 2024;15:1336456. doi:10.3389/fimmu.2024.1336456
12. Zhou H, Lan T, Guo S. Prognostic prediction value of qSOFA, SOFA, and admission lactate in septic patients with community-acquired pneumonia in the emergency department. Emerg Med Int. 2020;2020:7979353. doi:10.1155/2020/7979353
13. Soares M, Dongelmans DA. Why should we not use APACHE II for performance measurement and benchmarking? Rev Bras Ter Intensiva. 2017;29(3):268–270. doi:10.5935/0103-507X.20170043
14. Huang CT, Ruan SY, Tsai YJ, Ku SC, Yu CJ. Clinical trajectories and causes of death in septic patients with a low APACHE II score. J Clin Med. 2019;8(7):1064. doi:10.3390/jcm8071064
15. McCarthy SL, Stewart L, Shaikh F, Murray CK, Tribble DR, Blyth DM. Prognostic value of Sequential Organ Failure Assessment (SOFA) score in critically ill combat-injured patients. J Intensive Care Med. 2022;37(11):1426–1434. doi:10.1177/08850666221078196
16. Schupp T, Weidner K, Rusnak J, et al. C-reactive protein and procalcitonin during the course of sepsis and septic shock. Ir J Med Sci. 2024;193(2):457–468. doi:10.1007/s11845-023-03385-8
17. Schupp T, Weidner K, Rusnak J, et al. Diagnostic and prognostic significance of the prothrombin time/international normalized ratio in sepsis and septic shock. Clin Appl Thromb Hemost. 2022;28:10760296221137893. doi:10.1177/10760296221137893
18. Seidlitz S, Hölzl K, von Garrel A, et al. AI-powered skin spectral imaging enables instant sepsis diagnosis and outcome prediction in critically ill patients. Sci Adv. 2025;11(8):eadw1968. doi:10.1126/sciadv.adw1968
19. Turgman O, Schinkel M, Wiersinga WJ. Host response biomarkers for sepsis in the emergency room. Crit Care. 2023;27(1):97. doi:10.1186/s13054-023-04367-z
20. Ryoo SM, Han KS, Ahn S, et al. The usefulness of C-reactive protein and procalcitonin to predict prognosis in septic shock patients: a multicenter prospective registry-based observational study. Sci Rep. 2019;9(1):6579. doi:10.1038/s41598-019-42972-7
21. Tan R, Ge C, Yang Z, et al. Prediction of poor prognosis in patients with sepsis-induced coagulopathy. Medicine. 2025;104(19):e42709. doi:10.1097/MD.0000000000042709
22. Han X, Dou Q, Zhu Y, et al. Heparin-binding protein-enhanced quick SOFA score improves mortality prediction in sepsis patients. Front Med Lausanne. 2022;9:926798. doi:10.3389/fmed.2022.926798
23. Li W, Wang M, Zhu B, Zhu Y, Xi X. Prediction of median survival time in sepsis patients by the SOFA score combined with different predictors. Burns Trauma. 2020;8:tkz006. doi:10.1093/burnst/tkz006
24. Cui Y, Wang T, Bao J, Tian Z, Lin Z, Chen D. Comparison of Charlson’s weighted index of comorbidities with the chronic health score for the prediction of mortality in septic patients. Chin Med J. 2014;127(14):2623–2627. doi:10.3760/cma.j.issn.0366-6999.20132684
25. Zhang X, Wang Q, Luo X, Lei Y, Huang X. Prognostic value of Charlson weighted index of comorbidities combined with Sequential Organ Failure Assessment score and procalcitonin in patients with sepsis. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019;31(11):1335–1339. doi:10.3760/cma.j.issn.2095-4352.2019.11.005
26. Mearelli F, Fiotti N, Giansante C, et al. Derivation and validation of a biomarker-based clinical algorithm to rule out sepsis from noninfectious systemic inflammatory response syndrome at emergency department admission: a multicenter prospective study. Crit Care Med. 2018;46(5):736–742. doi:10.1097/CCM.0000000000003206
27. Zhang Z, Smischney NJ, Zhang H, et al. Development and validation of a novel sepsis prognostic model based on red blood cell distribution width, platelet count, and neutrophil-to-lymphocyte ratio. Sci Rep. 2022;12(1):20002. doi:10.1038/s41598-022-24079-4
28. Gül M, Demir F, Gündüz RC, et al. The predictive value of neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios in pediatric patients with sepsis. BMC Pediatr. 2023;23(1):334. doi:10.1186/s12887-023-04056-5
29. Barteková M, Kuricová K, Bolek T, et al. Diagnostic and prognostic potential of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in sepsis and septic shock. Bratisl Lek Listy. 2021;122(7):474–488. doi:10.4149/BLL_2021_076
30. Iba T, Levy JH, Warkentin TE, et al. Coagulopathy of sepsis: pathophysiology, diagnostic approaches, and treatment. Clin Appl Thromb Hemost. 2022;28:10760296221077115. doi:10.1177/10760296221077115
31. Song J, Moon S, Park DW, et al. Biomarker combination and SOFA score for the prediction of mortality in sepsis and septic shock: a prospective observational study according to the Sepsis-3 definitions. Medicine. 2020;99(12):e20495. doi:10.1097/MD.0000000000020495
32. Liu Z, Chen J, Liu Y, et al. A simple bioscore improves diagnostic accuracy of sepsis after surgery. J Surg Res. 2016;200(1):290–297. doi:10.1016/j.jss.2015.07.022
33. Gibot S, Béné MC, Noel R, et al. Combination biomarkers to diagnose sepsis in the critically ill patient. Am J Respir Crit Care Med. 2012;186(1):65–71. doi:10.1164/rccm.201201-0037OC
34. Sakyi SA, Enimil A, Adu DK, et al. Individual and combined bioscore model of presepsin, procalcitonin, and high sensitive C-reactive protein as biomarkers for early diagnosis of paediatric sepsis. Heliyon. 2020;6(9):e04841. doi:10.1016/j.heliyon.2020.e04841
35. Rondović G, Šurbatović M, Djordjević D, et al. Composite bioscore is superior to routine biomarkers and established scoring systems in predicting mortality in adult critically ill patients with secondary sepsis. Vojnosanit Pregl. 2021;78(11):1173–1184. doi:10.2298/VSP200312044R
36. Feng L, Liu S, Wang J, et al. The performance of a combination of heparin-binding protein with other biomarkers for sepsis diagnosis: an observational cohort study. BMC Infect Dis. 2024;24(1):755. doi:10.1186/s12879-024-09666-6
37. Thomas-Rüddel DO, Fröhlich H, Schwarzkopf D, Bloos F, Riessen R. Sepsis and underlying comorbidities in intensive care unit patients: analysis of the cause of death by different clinicians—a pilot study. Med Klin Intensivmed Notfmed. 2024;119(2):123–128. doi:10.1007/s00063-023-01037-4
38. Shukeri WFW, Md-Ralib A, Mat-Nor MB. Derivation of a new bioscore for predicting mortality in sepsis. Int Med J Malays. 2019;18(1):81–87. doi:10.31436/imjm.v18i1.216
39. Tocu G, Lisă EL, Tutunaru D, et al. The potential of artificial intelligence in the diagnosis and prognosis of sepsis: a narrative review. Diagnostics. 2025;15(17):2169. doi:10.3390/diagnostics15172169
40. Luțenco V, Tocu G, Guliciuc M, et al. New horizons of artificial intelligence in medicine and surgery. J Clin Med. 2024;13(9):2532. doi:10.3390/jcm13092532
41. Yang Y, Xie J, Guo F, et al. Combination of C-reactive protein, procalcitonin and sepsis-related organ failure score for the diagnosis of sepsis in critical patients. Ann Intensive Care. 2016;6(1):51. doi:10.1186/s13613-016-0153-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Correlation and Prognostic Assessment of Low T3 Syndrome and Norepinephrine Dosage for Patients with Sepsis: A Retrospective Single-Center (Cohort) Study
Zhang J, Fu S, Liu F, Wan J, Wu S, Jiang G, Tao W, Zhou W, Qian K
International Journal of General Medicine 2022, 15:4837-4847
Published Date: 10 May 2022
Identifying Potential Effective Diagnostic and Prognostic Biomarkers in Sepsis by Bioinformatics Analysis and Validation
Huang X, Tan J, Chen X, Zhao L
International Journal of General Medicine 2022, 15:6055-6071
Published Date: 6 July 2022
Impaired Circulating Antibody-Secreting Cells Generation Predicts the Dismal Outcome in the Elderly Septic Shock Patients
Xu H, Li T, Zhang X, Li H, Lv D, Wang Y, Huo F, Bai J, Wang C
Journal of Inflammation Research 2022, 15:5293-5308
Published Date: 13 September 2022
Integrated Analysis Identified TGFBI as a Biomarker of Disease Severity and Prognosis Correlated with Immune Infiltrates in Patients with Sepsis
Shi M, Wei Y, Guo R, Luo F
Journal of Inflammation Research 2024, 17:2285-2298
Published Date: 15 April 2024
Lactate-Modified Prognostic Nutritional Index (LPNI) and Its Association with ICU Mortality in Patients with Sepsis: A Retrospective Cohort Study
Li X, Qian S, Chen H, Yuan X, Xia X, Gao X, Chen G
Journal of Inflammation Research 2026, 19:604786
Published Date: 28 May 2026