Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
A Nomogram for Predicting Successful Weaning from Invasive Mechanical Ventilation Withdrawal in Patients with Chronic Obstructive Pulmonary Disease Complicated by Respiratory Failure
Authors Bao H, Zhu T, Li C, Huan J, Li L, Kong L, Chen Y, Shi L, Li C
Received 20 April 2026
Accepted for publication 12 June 2026
Published 23 June 2026 Volume 2026:21 618482
DOI https://doi.org/10.2147/COPD.S618482
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Hongzhu Bao,* Tianyi Zhu,* Chunhua Li, Jianbo Huan, Ling Li, Lingyu Kong, Yan Chen, Liang Shi, Congcong Li
Department of Respiratory and Critical Care Medicine, General Hospital of Northern Theater Command, Shenyang, Liaoning, 110013, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Congcong Li, Email [email protected]
Objective: To develop and validate a practical nomogram for predicting the success rate of invasive mechanical ventilation (IMV) weaning in patients with chronic obstructive pulmonary disease (COPD) complicated by acute hypercapnic respiratory failure.
Methods: A total of 159 eligible patients admitted between January 2020 and December 2024 were enrolled in this study, and they were randomly divided into a development cohort (n = 106) and a validation cohort (n = 53) at a 2:1 ratio. Least absolute shrinkage and selection operator (LASSO) regression and multivariate logistic regression were used to identify independent risk factors, which were used to construct a predictive nomogram. Model performance was evaluated using receiver operating characteristic (ROC) curves, calibration curves, and decision curve analysis (DCA), as well as through risk stratification validation.
Results: LASSO regression identified 5 candidate variables, and multivariate analysis confirmed that anxiety, pneumothorax, vasoactive drug use, and NT-proBNP were independent risk factors for weaning failure (all P < 0.05). The nomogram achieved excellent discriminative ability, with areas under the ROC curve (AUCs) of 0.942 (95% CI: 0.868– 1) in the development cohort and 0.982 (95% CI: 0.944– 1) in the validation cohort. The calibration curves indicated good consistency between the predicted and actual probabilities, and DCA demonstrated a favorable net clinical benefit. Using a cutoff value of 0.3, patients were effectively stratified into low-risk and high-risk groups by the nomogram, with significantly different weaning success rates between the cohorts (both P < 0.0001).
Conclusion: This study developed a simple, reliable, and clinically applicable nomogram for predicting IMV weaning success in COPD patients with respiratory failure. The nomogram might assist clinicians in implementing early risk stratification, optimizing weaning strategies, and improving clinical outcomes.
Plain Language Summary: In this study, a practical nomogram was developed to predict the weaning success of IMV in COPD patients with acute hypercapnic respiratory failure. This model can support clinical decision-making and facilitate individualized weaning strategies in the ICU. The key findings of this study are as follows:Anxiety, pneumothorax, vasoactive drug use, and NT-proBNP were identified as independent risk factors for weaning failure.The nomogram achieved good discrimination (AUC > 0.94) and calibration in both the development and validation cohorts.A cutoff value of 0.3 enabled effective risk stratification, with different weaning success rates between low- and high-risk groups.
Keywords: COPD, invasive mechanical ventilation, weaning, nomogram, risk prediction
Introduction
Chronic obstructive pulmonary disease (COPD) is an increasing global public health challenge, and it is a leading cause of morbidity and mortality worldwide.1–3 According to the Global Burden of Disease Study, COPD is the third leading cause of death globally,4 and it affected approximately 391.9 million people in 2019.5 It is associated with immense societal and economic burdens, which are driven by frequent exacerbations, frequent hospitalizations, and the need for long-term management.6 COPD is characterized by persistent respiratory symptoms and airflow limitation. Inhaled long-acting bronchodilators, steroids, and pulmonary rehabilitation are the standard treatment strategies.7,8 However, for patients with severe COPD, the occurrence of acute hypercapnic respiratory failure is inevitable, especially in those with infections.9 In this case, invasive mechanical ventilation (IMV), as a life-saving intervention, can stabilize patients during the acute phase and enable their recovery.10
However, withdrawing IMV, and thus liberating the patient from the ventilator, poses a considerable clinical dilemma. The weaning of IMV in patients with COPD and respiratory failure is a complex issue, which is accompanied by a high risk of failure.11 COPD patients often have difficulty breathing and have compromised respiratory muscle function because of airway obstruction and hyperinflation.12 COPD is also frequently comorbid with cardiovascular disease and malnutrition.13,14 As a consequence, compared with other patients, IMV in COPD patients may be prolonged, and the failure rate of IMV withdrawal may be higher. Previous studies have reported that failed weaning attempts are associated with a cascade of adverse outcomes, including prolonged ICU and hospital stays, increased risks of ventilator-associated pneumonia, and increased health care costs.15 More importantly, weaning failure is an independent predictor of increased mortality.15,16
Therefore, determining the optimal timing for weaning in COPD patients is challenging. The current decision-making often relies on a combination of clinical judgment and standardized weaning parameters, such as the rapid shallow breathing index (RSBI), maximal inspiratory pressure, and oxygenation measures.17,18 Conventional weaning indices such as RSBI, and maximal inspiratory pressure are widely used in clinical practice,19,20 however these parameters exhibit considerable variability and often lack sufficient predictive accuracy when used in isolation. Although several predictive models for weaning outcomes have been proposed, most have focused on general ICU populations rather than COPD-specific cohorts,21 and the existing literature on COPD weaning prediction remains limited. However, these parameters are variable and often exhibit insufficient predictive accuracy. An integrated and personalized predictive tool should be developed that can synthesize multiple types of relevant clinical data, standardize assessments, reduce the subjectivity of clinical judgment, and support more timely and confident decision-making, ultimately aiming to improve patient outcomes and optimize resource utilization.
To accurately predict the likelihood of successful weaning, in this study, we aimed to develop and validate a comprehensive nomogram for predicting the success rate of IMV withdrawal in patients with COPD complicated by respiratory failure. This practical, evidence-based tool will increase the precision and effectiveness of weaning management in this vulnerable patient group.
Patients and Methods
Research Subjects
In this retrospective study, we developed and validated a comprehensive nomogram for predicting the success rate of IMV withdrawal in patients with COPD complicated by respiratory failure. This study included adult patients (aged ≥18 years) who were diagnosed with COPD complicated by acute hypercapnic respiratory failure and who received IMV in the intensive care unit (ICU) of the Department of Respiratory and Critical Care Medicine, General Hospital of Northern Theater Command between January 1, 2020, and December 31, 2024. This study was approved by the hospital ethics committee, with the approval number Y (2025) No. 128.
The inclusion criteria were as follows: 1. COPD diagnosis was confirmed according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria,22 with preadmission history and spirometric criteria met (postbronchodilator FEV1/FVC < 0.70); and 2. Patients received IMV because of type II respiratory failure (the arterial blood gas assessment showing PaCO2 > 50 mmHg).
The exclusion criteria were as follows: 1. Tracheostomy; 2. Primary neuromuscular disease, irreversible neurologic impairment or cervical spinal cord injury; 3. Complicated with multiple organ failure (MOF); 4. Incomplete medical records; and 5. Age <18 years.
Procedures
First, from the hospital’s electronic medical records, we collected the relevant data of the patients who met the inclusion criteria, including baseline characteristics (sex, age, and smoking history), concomitant diseases (coronary heart disease, hypertension, diabetes, and chronic renal insufficiency), Acute Physiology and Chronic Health Evaluation II (APACHEII) scores within 24 h of admission, vital signs at admission (temperature, heart rate, blood pressure, and respiratory rate), laboratory examination results (total white blood cells, hemoglobin content, serum creatinine, serum albumin, NT-pro BNP, C-reactive protein, procalcitonin, and arterial blood gas analysis), preweaning clinical and ventilator parameters (coma before endotracheal intubation, vasoactive drug use after invasive mechanical ventilation, emotional anxiety, and ventilator-associated pneumonia or pneumothorax), and outcomes (success or failure of IMV withdrawal).
After admission, all patients underwent targeted symptomatic interventions based on comprehensive disease severity assessment; these interventions included anti-infective therapy, anti-inflammatory agents, bronchodilators, nutritional support, and multiorgan function protection. Invasive ventilation modes were tailored to the patients’ clinical status, which primarily included volume-assisted control ventilation (V-A/C), pressure-assisted control ventilation (P-A/C), and synchronized intermittent mandatory ventilation combined with pressure support ventilation (SIMV-PSV). The majority of patients were weaned from ventilation following a transition period with the PSV mode. In addition, timely extubation and weaning were implemented in patients who met the following criteria: 1. Clinical resolution of infection; 2. Clear consciousness and adequate cognitive responsiveness; 3. Hemodynamic stability; 4. Recovery to spontaneous breathing or significant improvement in spontaneous respiratory function, accompanied by reduced airway secretion; 5. Absence of electrolyte disturbance and acid–base imbalance; 6. Effective control of most predisposing factors for acute disease exacerbation or respiratory failure; and 7. Partial pressure of carbon dioxide (PaCO2) returning to the level typical in the stable remission phase, with a fraction of inspired oxygen (FiO2) ≤ 0.35.
Second, all included subjects were randomly divided into a development cohort and a validation cohort using a computer-generated random number list at a ratio of 2:1. The differences in subject demographics were determined to ensure comparability between the cohorts.
Outcomes
The primary outcome for the nomogram was successful withdrawal from IMV, which was defined as sustained spontaneous breathing without interventional ventilatory support for at least 48 hours following extubation. Weaning failure was defined as the need for reintubation and resumption of ventilatory support or occurrence of death within 48 hours of extubation. Specifically, weaning failure was define according to the following criteria: 1. Tachypnea with a respiratory rate > 30 breaths/min after weaning, indicating respiratory distress, or rapid shallow breathing index (RSBI) > 105; 2. An increase in heart rate of >20% above the baseline or an elevation in blood pressure of >20% above the baseline, which was accompanied by an arterial blood gas analysis assessment showing pH < 7.30 and SaO2 ≤ 88%, necessitating the resumption of invasive mechanical ventilation; and 3. Deterioration of consciousness, requiring the resumption of invasive mechanical ventilation.
Statistical Methods
Statistical analysis was performed using R software (version 4.2.1). Categorical variables are reported as frequencies (percentages), and they were compared using the chi-square test or Fisher’s exact test. Continuous variables are presented as medians with interquartile ranges (IQRs) or means ± standard deviations (SDs). These variables were compared using the Wilcoxon Mann‒Whitney U-test or Student’s t test, as appropriate.
Using least absolute shrinkage and selection operator (LASSO) regression (glmnet package in R), variable selection was performed to identify potential influencing factors in the development cohort. Using the multivariate logistic regression model, independent risk factors were determined from candidate variables, with P < 0.05 indicating the statistical significance of the variables, and the odds ratio (OR) and 95% confidence interval (CI) were calculated. Confounding factors included in the adjusted logistic regression model were selected based on the clinical relevance and univariate analysis results (P < 0.10 as the entry criterion). The final adjusted model included the following covariates: age, gender, diabetes, hypertension, pulmonary infection, coma, anxiety, pneumothorax, vasoactive drug, respiratory rate, hemoglobin level, D-dimer level, albumin level, creatinine level, and APACHE II score. The final multivariable model was used to construct the nomogram.
Using the data of the development cohort, model performance was evaluated with the rms package in R. The discriminative performance of the model was evaluated using the receiver operating characteristic (ROC) curve (pROC package in R). Furthermore, using decision curve analysis (DCA) and calibration curve analysis, the clinical net benefit of the nomogram was assessed across different threshold probabilities (rmda package in R) and model calibrations (rms package in R), respectively.
Model validation was performed in two steps. First, using an optimal cutoff point for the risk score for the model constructed using the data of the development cohort, patients in the validation cohort were stratified into low-risk and high-risk groups. Then, the success rate of IMV withdrawal between the high-risk and low-risk groups was compared using the chi-square (χ2) test, and a two-tailed P value of 0.05 was considered statistically significant, indicating that the actual success rate differed significantly between the high-risk and low-risk groups stratified by the model, which verified the effectiveness of risk stratification by the model.
Results
Basic Patient Information
A total of 159 patients with chronic obstructive pulmonary disease (COPD) complicated by respiratory failure who underwent invasive mechanical ventilation weaning were enrolled in this study. Among them, 130 patients were successfully weaned from the ventilator, and weaning failure was noted in 29 patients. For model establishment and validation, all patients were randomly divided into a development cohort (n = 106) and a validation cohort (n = 53) at a ratio of 2:1 (Figure 1).
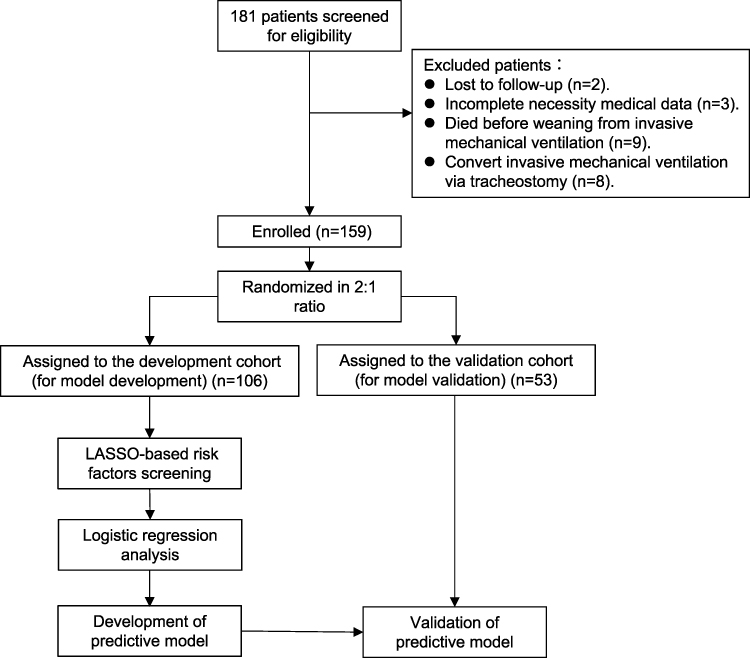 |
Figure 1 Flow chart of patient enrollment, grouping, and analysis. |
Baseline demographic, clinical, and laboratory data were compared between patients with successful weaning and those with a failed weaning attempt (Table 1). Significantly higher proportions of patients with a failed weaning attempt had diabetes, pulmonary infection, anxiety, pneumothorax, vasoactive drug administration, and coma (all P < 0.001). Significant between-group differences in temperature, respiratory rate, hemoglobin level, D-dimer level, albumin level, creatinine level, NT-proBNP level, and APACHE II score were detected (all P < 0.05).
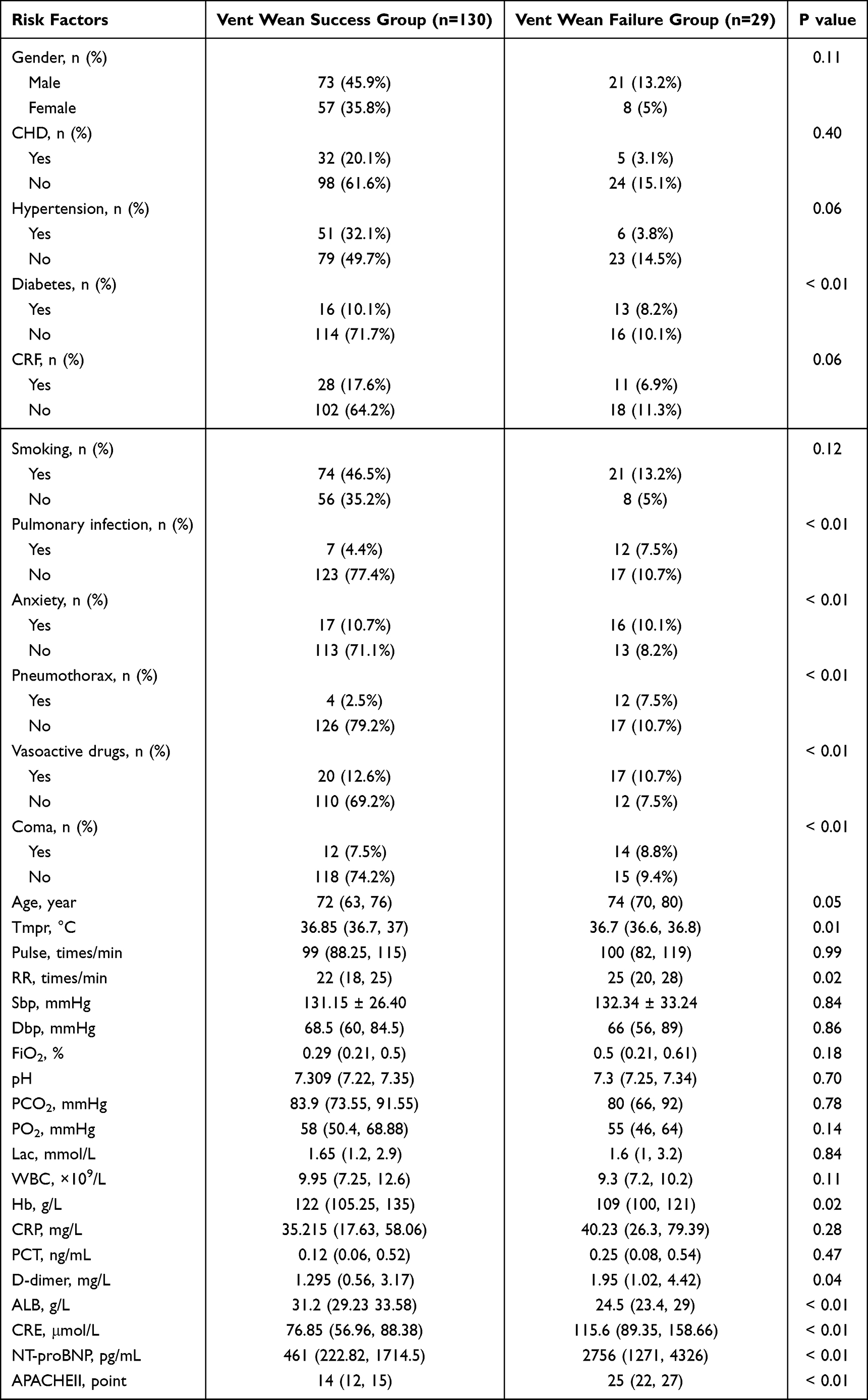 |
Table 1 Baseline Characteristics of Patients with Successful and Failed Ventilator Weaning |
Baseline characteristics were well-balanced between the development and validation cohorts (Table 2). No statistically significant differences were noted in demographic characteristics, comorbidities, vital signs, laboratory indicators, or APACHE II scores between the two cohorts (all P > 0.05), suggesting good comparability.
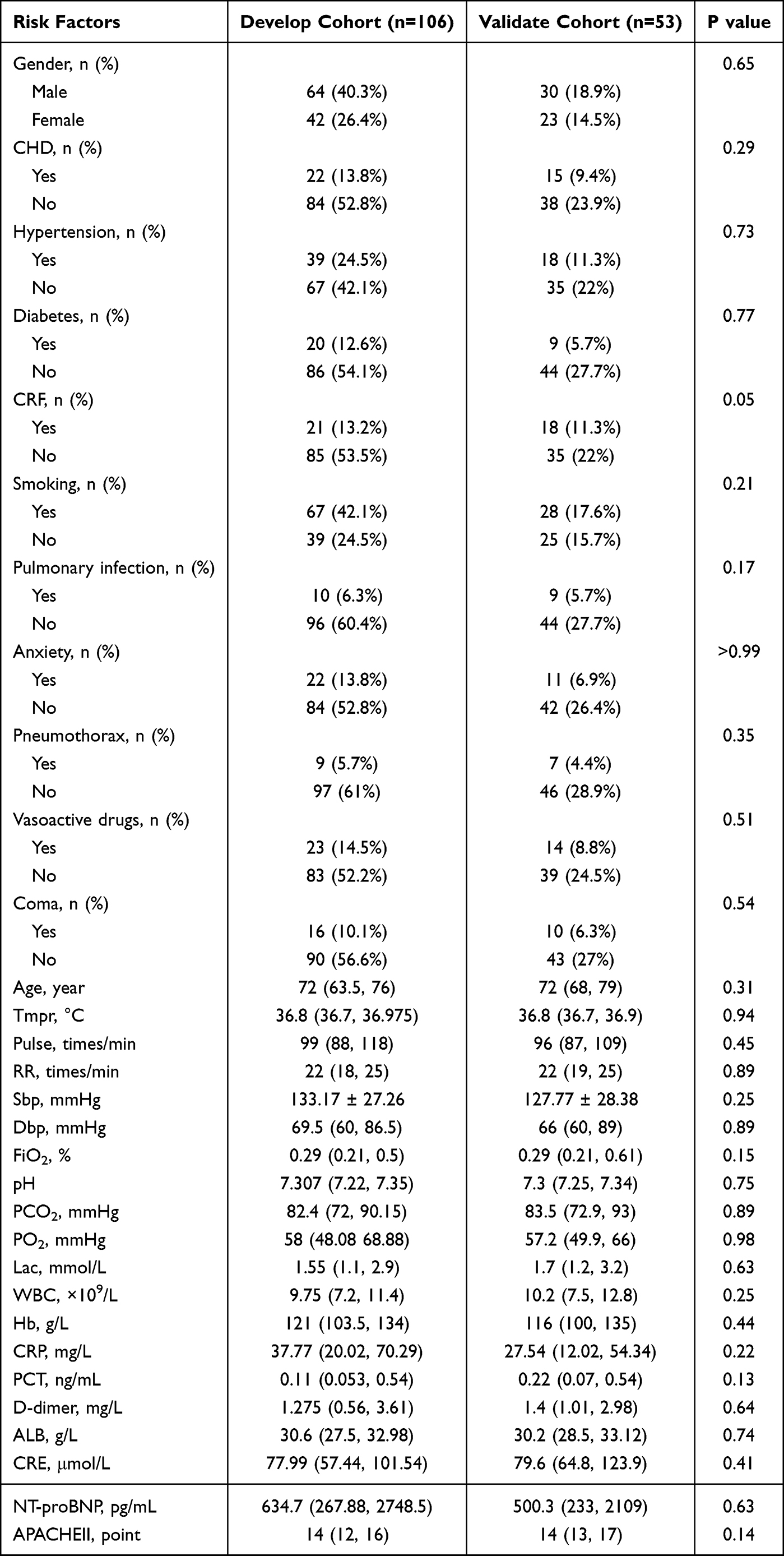 |
Table 2 Baseline Characteristics of Patients in the Development and Validation Cohorts |
Feature Selection Using LASSO Regression
LASSO regression was performed using the data of the development cohort to identify potential predictive factors for ventilator weaning failure (Figure 2A). Five-fold cross-validation was used to determine the optimal penalty parameter λ. The best model performance was achieved at λ.1 se = 0.022 (Figure 2B). Variables with nonzero coefficients were identified as candidate predictors to be included in further regression analysis. Under this parameter, LASSO regression ultimately revealed 5 variables, namely sex, NT-proBNP, anxiety, pneumothorax, and vasoactive drugs, with significant predictive value among all the candidate factors (Figure 2).
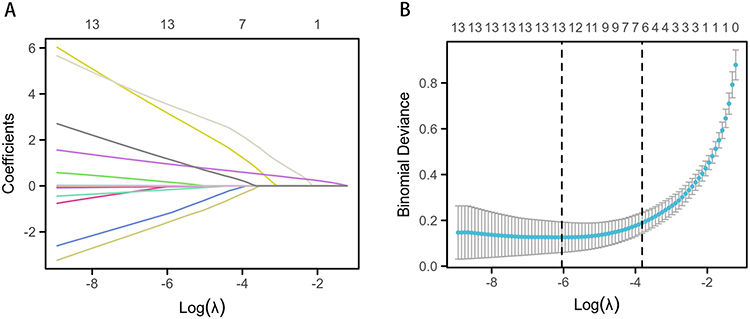 |
Figure 2 LASSO analysis of the development cohort. (A) Coefficient profiles of all candidate variables through LASSO regression. Each curve represents the trajectory of a single variable coefficient. (B) Five-fold cross-validation to determine the optimal penalty parameter λ (λ.1 se = 0.022). The left vertical dotted line indicates lambda.min (the optimal λ value with the minimum cross-validation error), and the right vertical dotted line indicates lambda.1se. |
Independent Risk Factors for Ventilator Weaning Failure
Univariate and multivariate logistic regression analyses were conducted using the data of the development cohort (Table 3). Univariate analysis revealed that anxiety, pneumothorax, vasoactive drug use, and NT-proBNP were significantly associated with weaning failure (all P < 0.05). With adjustment for confounding factors, multivariate analysis confirmed that anxiety (OR = 13.981; 95% CI: 2.136–91.521; P = 0.006), pneumothorax (OR = 39.126; 95% CI: 2.122–721.235; P = 0.014), vasoactive drug use (OR = 22.441; 95% CI: 3.372–149.358; P = 0.001), and NT-proBNP (OR = 1.000; 95% CI: 1.000–1.000; P = 0.017) were independent risk factors for invasive mechanical ventilation weaning failure.
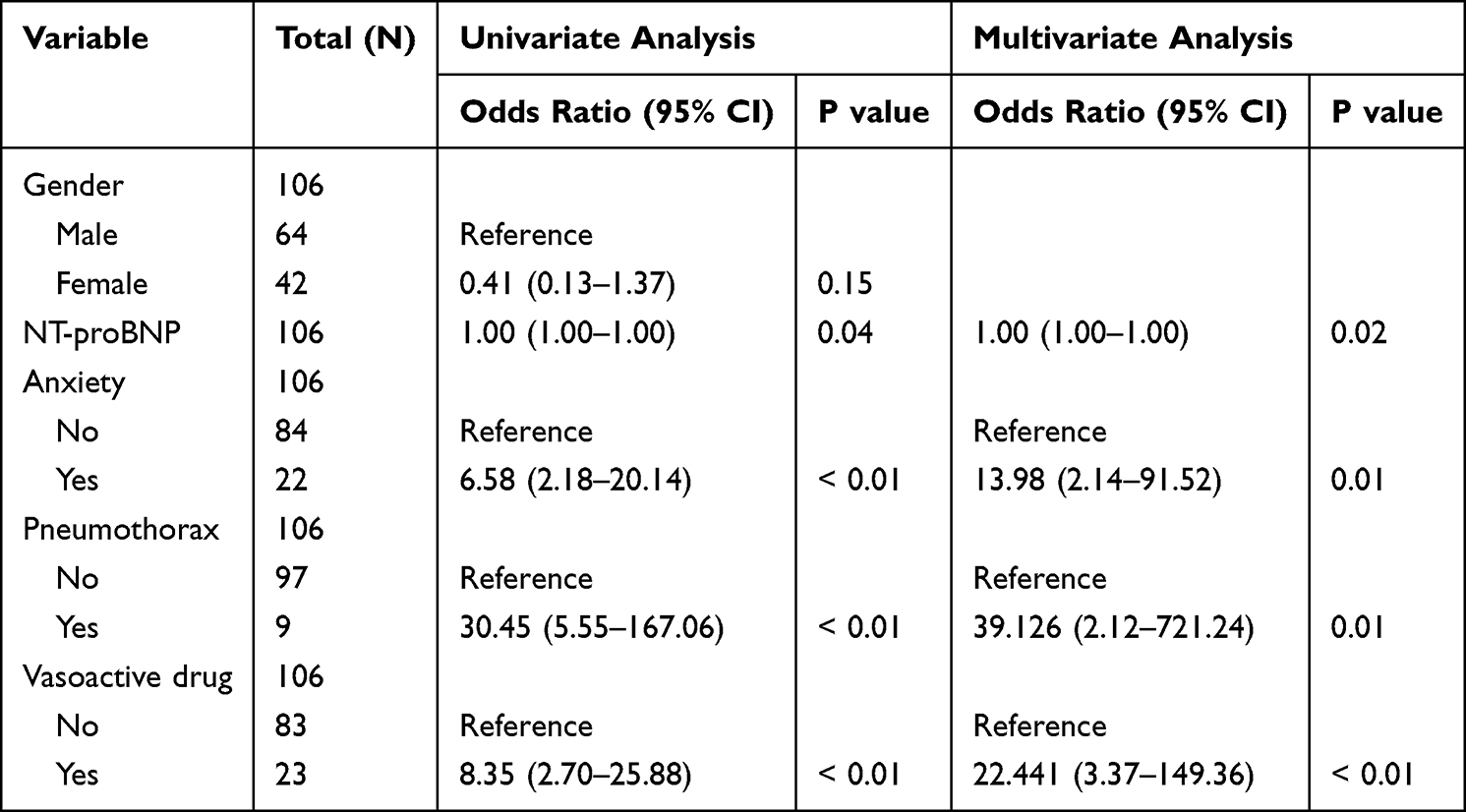 |
Table 3 Univariate and Multivariate Logistic Regression Analyses of Risk Factors for Invasive Mechanical Ventilation Weaning Failure in the Development Cohort |
Development and Performance Validation of the Predictive Nomogram
To predict the probability of successful weaning from invasive mechanical ventilation, a visual nomogram was constructed on the basis of the five risk factors from the development cohort (Figure 3).
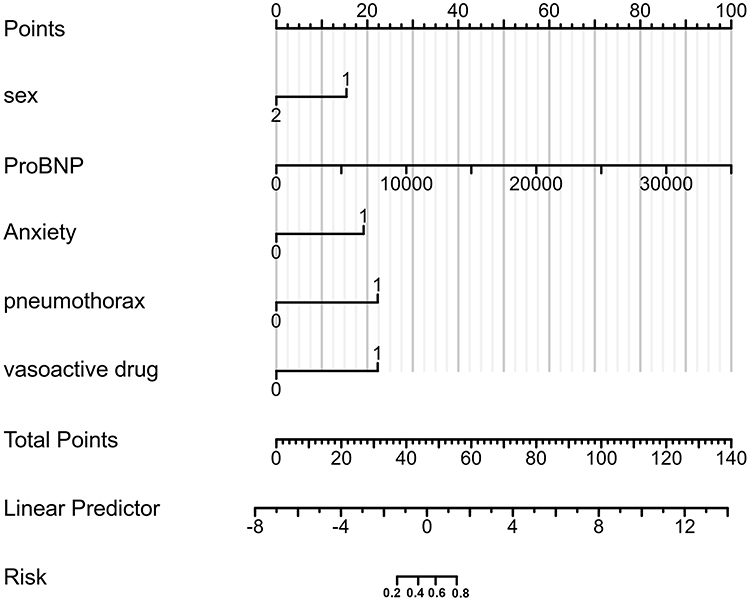 |
Figure 3 Nomogram for predicting the success rate of invasive mechanical ventilation weaning in the development cohort. The nomogram was constructed on the basis of five risk factors, namely, sex, anxiety, pneumothorax, vasoactive drug use, and NT-proBNP. The total points calculated from each variable can be used to estimate the individual probability of successful weaning. |
The discriminative ability of the nomogram was evaluated using receiver operating characteristic (ROC) curves. According to the area under the ROC curve (AUC), the nomogram exhibited favorable discriminative ability in both the development cohort (0.942, 95% CI: 0.868–1) (Figure 4A) and the validation cohort (0.982, 95% CI: 0.944–1) (Figure 4B). The calibration curves revealed excellent consistency between the nomogram-predicted probability and the actual weaning outcome in both cohorts (Figure 5A and B). Decision curve analysis (DCA) revealed that the nomogram conferred satisfactory net clinical benefit across a wide range of threshold probabilities, supporting its clinical utility in individualized risk assessment of ventilator weaning (Figure 5C and D).
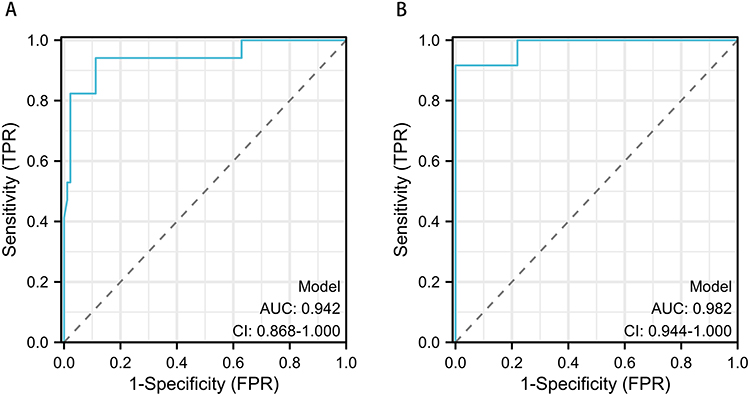 |
Figure 4 ROC curves of the predictive model in the development and validation cohorts. (A) ROC curve for the development cohort (AUC = 0.942; 95% CI: 0.868–1). (B) ROC curve for the validation cohort (AUC = 0.982, 95% CI: 0.944–1). Abbreviation: AUC, area under the curve. |
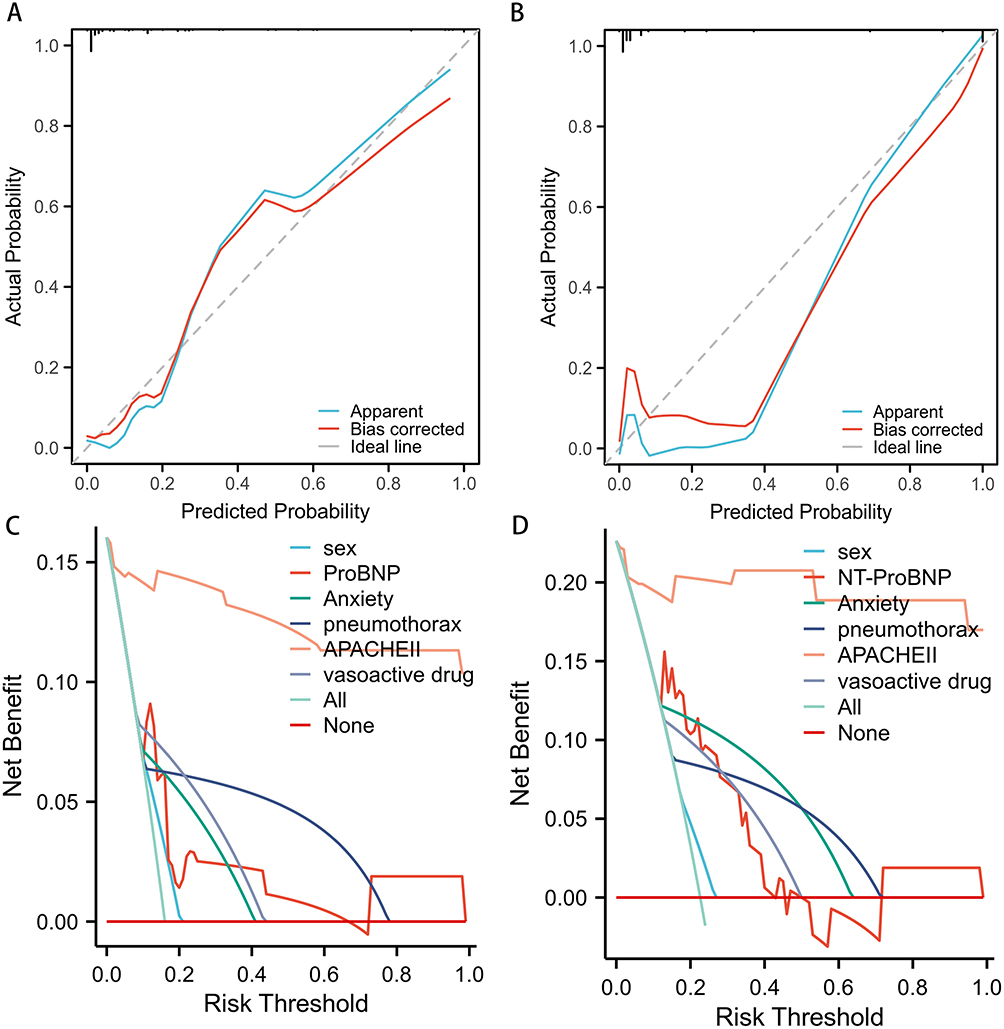 |
Figure 5 DCA and calibration curves of the predictive model for the development cohort and validation cohort. (A) Calibration curve of the development cohort: the ideal line represents perfect agreement between predicted and observed weaning success probability; the plotted smoothed curve close to the ideal line demonstrate that the model is well calibrated and predicted probabilities match actual clinical outcomes well. (B) Calibration curve of the validation cohort: satisfactory consistency between predicted and real weaning rates was observed. (C) DCA curve of the development cohort: the horizontal zero-line (None) stands for zero net clinical benefit (no patients receive weaning trial), the sloped all-intervention line (All) represents net benefit if all patients undergo ventilator weaning; the nomogram curve lying above the two reference lines across a wide threshold range indicates superior net clinical benefit from individualized weaning decision guided by this nomogram. (D) DCA curve of the validation cohort: the nomogram maintained positive net clinical value within clinically relevant probability thresholds. |
Validation of the Predictive Model for Risk Stratification
An optimal cutoff value of 0.3 for the risk score derived from the development cohort was applied to stratify patients into low-risk and high-risk groups. In the development cohort (n = 106), 16 patients were classified into the high-risk group, and 90 patients were classified into the low-risk group. As shown in Table 4, the weaning success rate was 12.50% (2/16) in the high-risk group and 96.67% (87/90) in the low-risk group, indicating a significant difference in the rate (χ2 = 71.47; P < 0.0001). In the validation cohort (n = 53), 14 patients were stratified into the high-risk group, and 39 were stratified into the low-risk group. The weaning success rate was 28.57% (4/14) in the high-risk group and 94.87% (37/39) in the low-risk group, with a statistically significant difference in the weaning rate (χ2 = 25.85; P < 0.0001). These results confirmed that the nomogram could effectively distinguish patients with high and low risks of weaning failure, demonstrating good stability and clinical applicability of the predictive model.
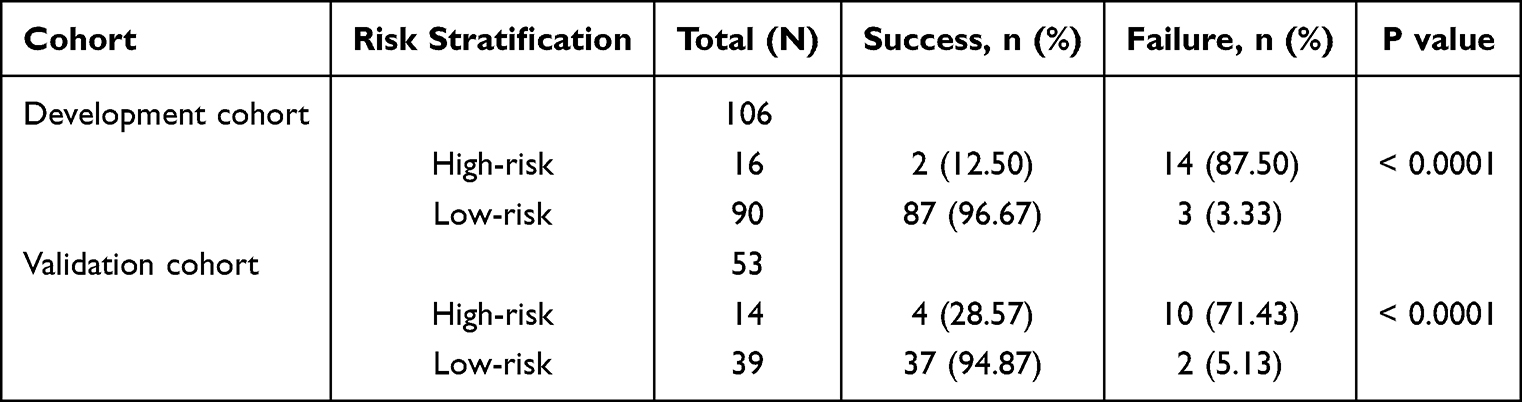 |
Table 4 Risk Stratification and Weaning Outcomes of the Development and Validation Cohorts |
Discussion
In this study, a practical nomogram for predicting the success rate of invasive mechanical ventilation weaning in patients with COPD complicated by respiratory failure was developed and validated. Through LASSO regression and multivariate logistic regression analyses, we identified anxiety, pneumothorax, vasoactive drug use, and NT-proBNP as the independent risk factors for weaning failure. The model showed excellent discrimination, calibration, and clinical net benefit, which were confirmed in both the development and validation cohorts. Furthermore, in the risk stratification analysis, a cutoff value of 0.3 was used to effectively distinguish low-risk and high-risk patients for weaning failure. Thus, the nomogram is a reliable and patient-specific risk assessment tool.
Weaning from invasive mechanical ventilation remains a critical and challenging step in the management of critically ill COPD patients. The early and accurate identification of high-risk individuals can help clinicians optimize weaning strategies, reduce the duration of mechanical ventilation, and decrease the incidence of complications such as ventilator-associated pneumonia and prolonged ICU stay.23,24 In the present study, patients with a failed weaning attempt had significantly higher rates of diabetes, pulmonary infection, anxiety, pneumothorax, and vasoactive drug administration; coma; higher APACHE II scores; and worse biochemical indicators, including lower serum albumin levels and higher creatinine and NT-proBNP levels. These findings are consistent with those of previous studies demonstrating that systemic inflammation, organ dysfunction, hemodynamic instability, and psychological distress are closely associated with difficult weaning.11,15,24 The strong association between anxiety and weaning failure may be mediated through several physiological pathways. Psychological stress activates the sympathetic nervous system, leading to increased catecholamine release and systemic oxygen consumption. In mechanically ventilated patients, anxiety can exacerbate patient-ventilator dyssynchrony, increase work of breathing, and promote respiratory muscle fatigue. Furthermore, anxiety and agitation often necessitate higher levels of sedation, which may delay the recovery of spontaneous respiratory drive and impair clearance of respiratory secretions.
By integrating multiple predictors from a statistical model, a nomogram, as a reliable and intuitive graphical calculation tool, can estimate an individualized probability of a clinical event.25 Our research identified key independent predictors associated with weaning success. These variables were used to construct a multivariate logistic regression model, which was transformed into a user-friendly nomogram. Anxiety was strongly predictive of weaning failure (OR = 13.981), which may be explained by increased oxygen consumption, respiratory muscle fatigue, and desynchrony between the patient and the ventilator (in agitated patients).26 Pneumothorax substantially increased the risk of weaning failure (OR = 39.126), as it directly impaired pulmonary compliance and gas exchange, making spontaneous breathing unsustainable. Vasoactive drug use (OR = 22.441) reflects persistent hemodynamic instability, inadequate tissue perfusion, and severe cardiovascular insufficiency, all of which impedes successful weaning. NT-proBNP was also independently associated with weaning failure, indicating that subclinical cardiac dysfunction and volume overload are important hidden barriers to ventilator liberation.27 The model had high discriminative ability, and risk stratification based on the cutoff value of 0.3 revealed that low-risk patients had a weaning success rate exceeding 94%, whereas high-risk patients had a success rate below 30%. This simple stratification can help clinicians make timely decisions regarding weaning attempts. It should be noted that NT-proBNP levels can be influenced by several confounding factors, including age, renal function, obesity, and concomitant cardiovascular medications. Future studies should incorporate more comprehensive cardiac assessment, including echocardiographic parameters, to better delineate the role of cardiac dysfunction in weaning failure.
This study has several strengths. First, it was conducted using the data of a well-defined cohort of COPD patients with acute hypercapnic respiratory failure, ensuring clinical homogeneity. Second, we used LASSO regression and strict internal validation to enhance model generalizability. Third, the nomogram encompasses readily available clinical and laboratory variables that do not require additional testing, supporting its easy clinical implementation. Fourth, we performed risk stratification validation, which further verified the clinical utility of the model. Numerous studies11,18,23,26,27 have linked anxiety, malnutrition, high RSBI, and weak respiratory muscle function to poor weaning outcomes. However, our work synthesized these factors into a simple, quantitative, and accessible nomogram, specifically for the COPD population. Our findings both confirm and extend previous knowledge.
Several limitations of this study should be acknowledged. First, this was a single-center retrospective study, with inherent selection bias and limited generalizability of the results. And the relatively small sample size, particularly the limited number of weaning failure cases, may affect model stability and contributed to the wide confidence intervals, indicating potential overfitting. To confirm its generalizability, the model requires external validation in prospective, multicenter cohorts, ensuring the inclusion of diverse patient populations and varying clinical practices. Second, although we included a range of clinical variables, other potentially significant factors such as detailed echocardiographic findings, nutritional indices (eg, albumin, prealbumin, body mass index), precise fluid balance data or biomarkers of inflammation were not systematically analyzed, and these should be included to further improve the predictive performance of the model. Especially, future studies should incorporate comprehensive cardiac assessment, including echocardiographic parameters, to better explore the role of cardiac dysfunction in weaning failure. Third, the definition of weaning success was based on a 48-hour period, which, although standard, may not capture all late failures. Long-term outcomes such as hospital mortality and rehospitalization were not evaluated. Finally, because the nomogram is a predictive tool, it can estimate probability and cannot replace comprehensive clinical judgment.
Conclusions
In this study, we developed a nomogram for predicting weaning success in COPD patients with acute hypercapnic respiratory failure. The model incorporates anxiety, pneumothorax, vasoactive drug use, and NT-proBNP, and it exhibits good discrimination, calibration, and clinical value in internal validation. It might serve as a supplementary tool to assist clinicians in identifying high-risk patients and informing weaning decisions, though it should not replace comprehensive clinical judgment. However, external validation in prospective, multicenter cohort is necessary before it can be recommended for clinical use. Future research should focus on the prospective external validation of this tool and investigate whether the implementation of this nomogram can improve patient outcomes.
Abbreviations
COPD, Chronic Obstructive Pulmonary Disease; ROC, Receiver Operating Characteristic; AUC, Area Under the Curve; DCA, Decision Curve Analysis; LASSO, Least Absolute Shrinkage and Selection Operator; CHD, Coronary Heart Disease; CRF, Chronic Renal Failure; RR, Respiratory Rate; SBP, Systolic Blood Pressure; DBP, Diastolic Blood Pressure; FiO2, Fraction of Inspired Oxygen; PCO2, Partial Pressure of Carbon Dioxide; PO2, Partial Pressure of Oxygen; Lac, Lactate; WBC, White Blood Cell; Hb, Hemoglobin; CRP, C-Reactive Protein; PCT, Procalcitonin; ALB, Albumin; CRE, Creatinine; NT-proBNP, N-Terminal Pro-B-Type Natriuretic Peptide; APACHE II, Acute Physiology and Chronic Health Evaluation II; OR, Odds Ratio; CI, Confidence Interval; IMV, Invasive Mechanical Ventilation; ICU, Intensive Care Unit; RSBI, Rapid Shallow Breathing Index; IQR, Interquartile Range; GOLD, Global Initiative for Chronic Obstructive Lung Disease; FEV1/FVC, Forced Expiratory Volume in 1 second/ Forced Vital Capacity; SaO2, Arterial Oxygen Saturation; MOF, Multiple Organ Failure.
Data Sharing Statement
The datasets during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The studies involving humans were approved by Ethics Committee of General Hospital of the Northern Theater Command. The studies were conducted in accordance with the Declaration of Helsinki and local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because (a) The risk to the subjects in the study is not greater than the minimum risk; (b) Exemption from informed consent will not have adverse effects on the health and rights of the subjects; (c) The privacy and personal identity information of the subjects are protected.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research was funded by Liaoning Provincial Natural Science Foundation Joint Fund (2023-MSLH-359).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–14. doi:10.1016/S0140-6736(22)00470-6
2. Valente D, Segreti A, Celeski M, et al. Electrocardiographic alterations in chronic obstructive pulmonary disease. J Electrocardiol. 2024;85:58–65. doi:10.1016/j.jelectrocard.2024.05.083
3. Li C, Zhu T, Ma D, Chen Y, Bo L. Complications and safety analysis of diagnostic bronchoscopy in COPD: a systematic review and meta-analysis. Expert Rev Resp Med. 2022;16(5):555–565. doi:10.1080/17476348.2022.2056023
4. Soriano JB, Kendrick PJ, Paulson KR. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet Resp Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
5. Adeloye D, Song P, Zhu Y, Campbell H, Sheikh A, Rudan I. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Resp Med. 2022;10(5):447–458. doi:10.1016/S2213-2600(21)00511-7
6. Zhou M, Wang H, Zeng X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2019;394(10204):1145–1158. doi:10.1016/S0140-6736(19)30427-1
7. Mathioudakis AG, Vestbo J, Singh D. Long-acting bronchodilators for chronic obstructive pulmonary disease: which one(S), how, and when? Clin Chest Med. 2020;41(3):463–474. doi:10.1016/j.ccm.2020.05.005
8. Shibata Y, Kawayama T, Muro S, Sugiura H. Management goals and stable phase management of patients with chronic obstructive pulmonary disease in the Japanese respiratory society guideline for the management of chronic obstructive pulmonary disease 2022 (6th edition). Respir Investig. 2023;61(6):773–780. doi:10.1016/j.resinv.2023.08.007
9. MacIntyre NR. Acute hypercapnic respiratory failure in COPD. Resp Care. 2023;68(7):973–982. doi:10.4187/respcare.10560
10. Gadre SK, Duggal A, Mireles-Cabodevila E, et al. Acute respiratory failure requiring mechanical ventilation in severe chronic obstructive pulmonary disease (COPD). Medicine. 2018;97(17):e487. doi:10.1097/MD.0000000000010487
11. Ye L, Yuan X, Li Y. Risk factors and predictive model for weaning failure in elderly patients with chronic obstructive pulmonary disease and type II respiratory failure. Am J Transl Res. 2025;17(7):5485–5492. doi:10.62347/KAAK3231
12. Fonseca J, Nellessen AG, Pitta F. Muscle dysfunction in smokers and patients with mild COPD: a systematic review. J Cardiopulm Rehabil. 2019;39(4):241–252. doi:10.1097/HCR.0000000000000400
13. Mai S, Nan Y, Peng L, Wu Y, Chen Q. Controlling nutritional status score in the prediction of cardiovascular disease prevalence, all-cause and cardiovascular mortality in chronic obstructive pulmonary disease population: NHANES 1999-2018. BMC Pulm Med. 2024;24(1):356. doi:10.1186/s12890-024-03175-7
14. Qu S, Zhu J. A nomogram for predicting cardiovascular diseases in chronic obstructive pulmonary disease patients. J Healthc Eng. 2022;2022:6394290. doi:10.1155/2022/6394290
15. Ionescu F, Zimmer MS, Petrescu I, et al. Extubation failure in critically Ill COVID-19 patients: risk factors and impact on in-hospital mortality. J Intensive Care Med. 2021;36(9):1018–1024. doi:10.1177/08850666211020281
16. Miura S, Butt W, Thompson J, Namachivayam SP. Recurrent extubation failure following neonatal cardiac surgery is associated with increased mortality. Pediatr Cardiol. 2021;42(5):1149–1156. doi:10.1007/s00246-021-02593-2
17. Al-Husinat L, Araydah M, Haddad F, et al. Ventilator weaning and extubation in acute brain injury: challenges and evidence-based approaches. Anaesth Crit Care. 2026;PA:101816.
18. Trivedi V, Chaudhuri D, Jinah R, et al. The usefulness of the rapid shallow breathing index in predicting successful extubation: a systematic review and meta-analysis. Chest. 2022;161(1):97–111. doi:10.1016/j.chest.2021.06.030
19. Wu Y, Qing Z, Wei N, Sun J, Dong L, Zhao K. Ventilation mode effect on weaning outcome in COPD with type II respiratory failure. Am J Transl Res. 2026;18(4):3057–3072. doi:10.62347/IOGD1818
20. Sun S, Pan L, Wang X, Zhao J. Diaphragmatic ultrasound in guiding weaning from invasive mechanical ventilation in patients with acute exacerbation of chronic obstructive pulmonary disease. Heart Lung. 2026;77:102692. doi:10.1016/j.hrtlng.2025.102692
21. Zhang F, Li L, Zhu T, Liu K. Construction of a nomogram to predict weaning-induced pulmonary edema in mechanically ventilated patients with cardiogenic respiratory failure. Front Med-Lausanne. 2025;12:1713050. doi:10.3389/fmed.2025.1713050
22. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
23. Jia Y, Kaul C, Lawton T, Murray-Smith R, Habli I. Prediction of weaning from mechanical ventilation using convolutional neural networks. Artif Intell Med. 2021;117:102087. doi:10.1016/j.artmed.2021.102087
24. Michels-Zetsche JD, Roser E, Ersoz H, et al. Indicators of different outcomes after prolonged weaning. Sci Rep-UK. 2025;15(1):35044. doi:10.1038/s41598-025-21370-2
25. Gafita A, Calais J, Grogan TR, et al. Nomograms to predict outcomes after (177)Lu-PSMA therapy in men with metastatic castration-resistant prostate cancer: an international, multicentre, retrospective study. Lancet Oncol. 2021;22(8):1115–1125. doi:10.1016/S1470-2045(21)00274-6
26. De Jong A, Capdevila M, Aarab Y, et al. Incidence, risk factors, and long-term outcomes for extubation failure in ICU in patients with obesity: a retrospective analysis of a multicenter prospective observational study. Chest. 2025;167(1):139–151. doi:10.1016/j.chest.2024.07.171
27. Liu J, Wang C, Ran J, et al. The predictive value of brain natriuretic peptide or N-terminal pro-brain natriuretic peptide for weaning outcome in mechanical ventilation patients: evidence from SROC. J Renin-Angio-Aldo S. 2021;22(1):1602243959.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Nomogram for Predicting Risk of Emergency Department Revisits in Chinese Older Patients
Fan L, Xue H, Wang Q, Yan Y, Du W
Risk Management and Healthcare Policy 2022, 15:2283-2295
Published Date: 6 December 2022
Integrated SIRI and Lipid Profile for Early Prediction of Bloodstream Infection in AML During Induction Chemotherapy
Luo G, Zeng S, Zhao H
Infection and Drug Resistance 2025, 18:6979-6990
Published Date: 27 December 2025
Development of a Risk Prediction Model for Preoperative Pre-Frailty in Elderly Patients with Gastric Cancer
Yin C, Yin M, Zhen J, Xue C, Zhu Z
Clinical Interventions in Aging 2025, 20:2763-2772
Published Date: 28 December 2025
Machine Learning Analysis of Risk Factors for Catheter-Associated Urinary Tract Infections in Stroke Patients and Their Impact on Healthcare Quality
Lu L, Li X, Cai D, Mei C, Hong X, Xie J
International Journal of General Medicine 2026, 19:591432
Published Date: 8 April 2026
Risk Stratification for ESBL-Producing Enterobacterales in Elderly Diabetic Patients with Urinary Tract Infections: A Multicenter Model to Support Empirical Antibiotic Decision-Making
Huang T, Qin J, Jiang X, Hu M, Wang J, Chen K, Yang F, Gu J, Wu H, Chen X
Infection and Drug Resistance 2026, 19:604463
Published Date: 1 May 2026