Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
A Multi-Disciplinary Approach to the Management of Chemotherapy-Induced Nausea and Vomiting in Breast Cancer
Authors Chen F, Cao K, Zhao X, Xia L, Liu M, Jiang Y
Received 29 April 2026
Accepted for publication 24 June 2026
Published 9 July 2026 Volume 2026:22 620981
DOI https://doi.org/10.2147/TCRM.S620981
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Fang Chen,1 Kai Cao,2 Xiaoyan Zhao,2 Liping Xia,2 Meng Liu,2 Yifan Jiang2
1Department of Nursing, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2Division of Thyroid Breast Surgery, Department of Surgery, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Yifan Jiang, Division of Thyroid Breast Surgery, Department of Surgery, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310003, People’s Republic of China, Email [email protected]
Abstract: Chemotherapy is a cornerstone of comprehensive breast cancer treatment. However, its non-specific cytotoxic effects frequently involve the gastrointestinal tract, leading to a spectrum of digestive adverse reactions, including chemotherapy-induced nausea and vomiting (CINV), anorexia, diarrhea, and constipation. These symptoms not only compromise patients’ quality of life but may also impair treatment adherence. In severe cases, they can necessitate dose reduction or treatment discontinuation. This review systematically examines the epidemiology, pathophysiology, and classification of gastrointestinal adverse reactions associated with breast cancer chemotherapy, with a focus on CINV management strategies. These strategies include pharmacological prophylaxis, individualized risk assessment, non-pharmacological interventions, and the use of standardized assessment tools. Based on the available evidence, we discuss the transition from an experience-based nursing model to a predictive one. We also emphasize the importance of patient education, psychological support, and family involvement, and highlight specific considerations for breast cancer patients. This review provides a systematic, evidence‑based reference for the clinical care of CINV in breast cancer to optimize gastrointestinal symptom management and improve treatment outcomes and quality of life for these patients.
Keywords: breast cancer, chemotherapy, adverse effect, chemotherapy-induced nausea and vomiting, clinical management, nursing
Introduction
Breast cancer is one of the most common cancers in the world, with approximately 2.3 million newly diagnosed cases and 670,000 related deaths reported in 2022.1 With continuous improvements in screening techniques and systemic therapies, the survival of breast cancer patients has been significantly prolonged. Unfortunately, survivors may experience significant adverse side effects from breast cancer diagnosis and cancer directed therapies. Among all treatment related adverse side effects, gastrointestinal toxicity, particularly chemotherapy‑induced nausea and vomiting (CINV), is the most common.2 It affects approximately 70%-80% of patients receiving chemotherapy.3,4 CINV severely compromises quality of life and treatment compliance, and may even lead to dose reduction or treatment discontinuation.5,6
This review synthesizes the evidence base for optimal CINV management in breast cancer patients. We describe the pathophysiology, risk factors, and evidence-based prevention and treatment strategies for CINV management. We adopt a multidisciplinary perspective, integrating evidence from oncology, clinical pharmacy, nursing, psychology, nutrition, and integrative oncology. By synthesizing both pharmacologic and non-pharmacologic strategies across these disciplines, we aim to provide a comprehensive framework for multidisciplinary teams managing CINV in breast cancer care.
Methodology
A literature search was conducted in PubMed, Web of Science, and Cochrane Library from inception to December 2025. The search strategy combined terms related to breast cancer (“breast cancer” OR “breast neoplasm” OR “mammary cancer”), chemotherapy‑induced nausea and vomiting (“CINV” OR “nausea” OR “vomiting” OR “anti-emetic”), and management (“clinical management” OR “prevention” OR “treatment” OR “guideline” OR “non‑pharmacological” OR “integrative oncology”). We included peer-reviewed clinical studies, guidelines, systematic reviews, meta-analyses, and relevant narrative reviews focusing on CINV management in breast cancer patients. No language restrictions were applied. Two authors independently screened the literature and resolved disagreements through discussion. The findings were thematically synthesized and are presented across the following sections.
Epidemiology
The global burden of breast cancer shows significant geographic and temporal variations, which is closely linked to socioeconomic development, lifestyle factors and healthcare access.7,8 Specifically, women in transitioned countries tend to have higher incidence rates compared with those in transitioning countries (54.1 vs 30.8 per 100,000, respectively). However, they experience lower mortality (11.3 vs 15.3 per 100,000, respectively) due to better access to early detection and advanced treatments.1,9
Burden and Management of Chemotherapy in Breast Cancer
Chemotherapy is a standard part of curative breast cancer treatment. For decades, anthracyclines, taxanes, and alkylating agents have formed the backbone of systemic therapy for both early and advanced breast cancer. However, current chemotherapeutic regimens do not distinguish between cancer cells and normal cells. This non-specific targeting of rapidly dividing cells frequently affects the gastrointestinal tract.2 This damage attacks the gastrointestinal mucosa and triggers signals to the medullary vomiting center. Therefore, chemotherapy-induced gastrointestinal (GI) toxicities is one of the most common side effects associated with these treatments.10 Approximately 70–80% of patients receiving chemotherapy are at risk of developing Chemotherapy-induced nausea and vomiting (CINV).3 It can reduce quality of life and treatment adherence, and may even lead to dose reduction or treatment discontinuation. In addition to nausea and vomiting, patients may experience a range of other distressing symptoms such as anorexia, diarrhea, abdominal pain, constipation, and weight loss. These symptoms collectively lead to difficulty eating, social isolation, reduced confidence in treatment, and even avoidance of therapy. Therefore, effective management of CINV is essential to optimize treatment outcomes in breast cancer patients. Clinical management of CINV should integrate symptom assessment, pharmacotherapy, and psychological support.
Emetogenic Risk Classification of Breast Cancer Chemotherapy Regimens
Chemotherapy plays an important role in the comprehensive treatment, making it critical to evaluate the emetogenic risk of routine breast cancer chemotherapy regimens. According to the expected vomiting rate in the absence of anti-emetic prophylaxis, the emetogenicity of breast cancer chemotherapy regimens are stratified into four emetogenic risk tiers: high emetogenic chemotherapy (HEC, >90%), moderate emetogenic chemotherapy (MEC, 30–90%), low emetogenic chemotherapy (LEC, 10–30%), and minimal emetogenic chemotherapy (<10%) (Table 1).
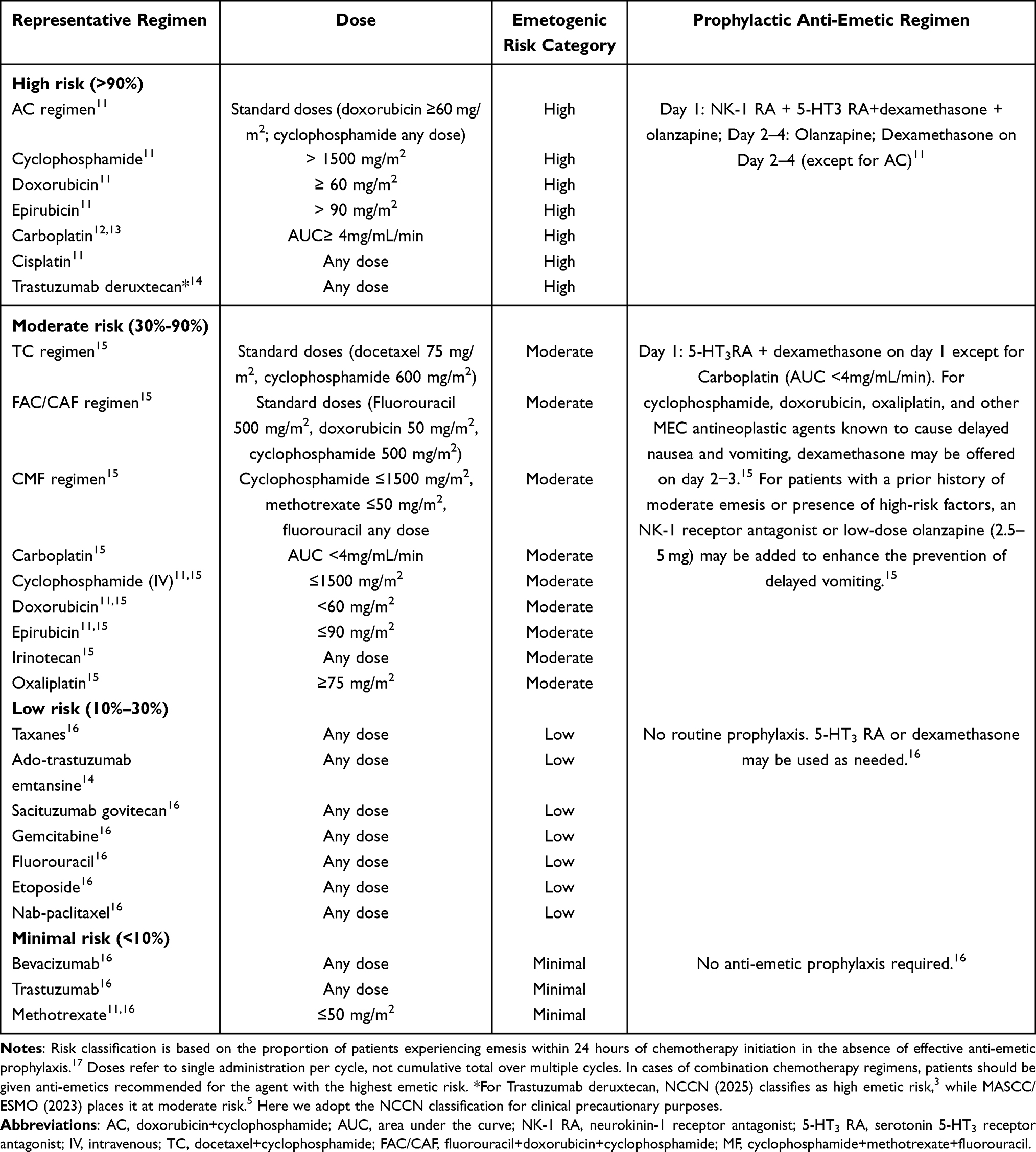 |
Table 1 Emetogenic Risk Classification and Recommended Anti-Emetic Prophylaxis for Intravenous Chemotherapy Agents |
In breast cancer, the anthracycline plus cyclophosphamide (AC) combination is a classic HEC regimen.11 However, not all regimens containing an anthracycline or cyclophosphamide are HEC. The emetogenic risk of a single-agent depends on the specific drug and its dose. For cyclophosphamide, only when used as a single agent at doses exceeding 1500 mg/m2 is it classified as HEC. Other HEC regimens include carboplatin AUC ≥4, carmustine>250 mg/m2, cisplatin, dacarbazine, doxorubicin≥60 mg/m2, epirubicin>90 mg/m2, ifosfamide≥2 g/m2 per dose, mechlorethamine, and streptozocin.18 Notably, the classification of trastuzumab deruxtecan (T-DXd) remains discordant across guidelines. It is listed as a MEC agent in the MASCC and ESMO guidelines for the appropriate use of anti-emetic drugs whereas the NCCN guidelines regard it as a HEC agent.12,15 For all HEC regimens, current guidelines recommend a four-drug anti-emetic combination (NK1 antagonist, 5-HT3 antagonist, dexamethasone, and olanzapine). However, for patients receiving the AC regimen, dexamethasone is recommended only on day 1 of chemotherapy, whereas for non-AC HEC regimen such as cisplatin, a 4-day dexamethasone schedule is used.
In addition, a broad range of regimens are classified as moderate emetogenic risk (MEC), with TC (docetaxel plus cyclophosphamide) being most commonly used. In one study, standard anti-emetic prophylaxis (5‑HT3 receptor antagonist plus dexamethasone) achieved a complete response (CR) rate of 87% for the TC regimen.17 However, this finding has yet to be validated in larger, real‑world populations. For patients who still experience CINV after TC, aprepitant as second‑line rescue therapy still achieves a CR in 52.2% of cases.17 Other MEC regimens include carboplatin AUC<4, cyclophosphamide ≤1500 mg/m2, doxorubicin <60 mg/m2, and epirubicin ≤90 mg/m2.18 Taxanes are classified as low emetogenic risk (LEC), for which guidelines recommend either dexamethasone or a 5-HT3antagonist as a single agent.19 Nevertheless, some patients may still experience nausea, highlighting the need for individualized assessment. Vinca alkaloids pose minimal emetogenic risk and do not require routine anti-emetic prophylaxis.19
Special Considerations for CINV Management in Breast Cancer
Relying on emetogenic risk classification alone is insufficient for managing CINV in breast cancer patients. Although information is now readily available, many patients still lack adequate knowledge about CINV.20 Most patients do not know the risk classification of their CINV. And their knowledge of the role and adverse reactions of chemotherapy regimens is vague. Consequently, clinical interventions should prioritize proactive prevention and careful assessment. Moreover, breast cancer patients often experience multiple symptoms simultaneously that require additional considerations. Studies have shown that nausea is more distressing than vomiting for breast cancer patients.21 Current anti-emetic drugs control vomiting relatively well but are less effective against nausea,21 suggesting the need to assess nausea as an independent clinical indicator. A randomized controlled trial (J-FORCE) demonstrated that adding olanzapine 5mg to standard anti-emetic therapy significantly reduced both acute and delayed nausea in patients receiving cisplatin-based or AC chemotherapy.22 Furthermore, gastrointestinal symptom cluster including nausea, vomiting, and decreased appetite is most prominent in the early cycles of chemotherapy, while fatigue, cognitive, and psychosocial symptom clusters persist or even worsen in later cycles or after treatment completion.23 This dynamic pattern suggests that clinical interventions could be implemented in phases: focusing on gastrointestinal symptom management in the early cycles, and continuing to monitor psychological and functional status in subsequent cycles. Finally, clinical decisions should also consider individual patient risk factors, such as younger age, female sex, and a prior history of CINV.
Individual Risk Factors
Clinicians and nurses should identify individual risk factors for CINV, including younger age, female sex, expectancy of CINV, prior nausea or vomiting, history of morning sickness, anxiety and use of non-steroidal anti-inflammatory drugs.24,25 These factors are associated with an increased incidence of nausea and vomiting. For high-risk patients, enhanced preventive measures may be considered, such as extending the duration of anti-emetic therapy or adding olanzapine. Preliminary evidence from a prospective study suggested that risk-stratified management, which applies enhanced measures to intermediate- and high-risk patients, may reduce the incidence of nausea and vomiting and improve quality of life scores.26 However, larger, well-designed trials are needed to confirm these findings.
Assessment Tool for CINV
To enable timely adjustment of anti‑emetic regimens, it is essential to accurately distinguish among the three main types of CINV: anticipatory, acute, and delayed.27 These types differ in both their timing and their response to anti‑emetic therapy. Acute vomiting occurs within 24 hours after chemotherapy. It usually begins 1–2 hours after drug administration and peaks at 4–6 hours. Delayed vomiting appears more than 24 hours after chemotherapy. It most commonly peaks at 48–72 hours and can last up to 6–7 days. Anticipatory nausea and vomiting (ANV) develop before the next chemotherapy cycle begins, often triggered by poorly controlled CINV in a previous cycle. Therefore, accurate differentiation of these three types is necessary to guide precise, individualized regimen adjustments. Delayed nausea and vomiting deserves particular attention. Its onset occurs after patients have been discharged, making it difficult for patients to report symptoms to healthcare providers in a timely manner. Consequently, delayed CINV is often significantly underestimated in clinical practice. Moreover, due to its prolonged duration, delayed vomiting poses continuous challenges to patients’ nutritional intake, fluid‑electrolyte balance, and self‑care capacity at home. If not properly managed, it substantially increases patient distress and the risk of treatment discontinuation. Therefore, periodic assessments of this phase should be actively conducted rather than passively waiting for patient complaints.
For accurate assessment of CINV, a combination of three validated tools is recommended (Table 2). MASCC anti-emesis tool (MAT) to evaluate the severity of acute and delayed nausea and vomiting.28 Morrow assessment of nausea and emesis (MANE) to identify anticipatory nausea and vomiting, the prevention of which relies on adequate control of CINV in previous cycles. And functional living index-emesis (FLIE) to quantify the impact of CINV on patients’ daily functioning and quality of life.29 Together, these tools enable comprehensive assessment of symptom control, functional impact, and all phases of CINV. Specifically, MANE can be used before the chemotherapy cycle to assess anticipatory risk, MAT during the cycle to document acute and delayed symptoms, and FLIE after the cycle to evaluate functional impact.
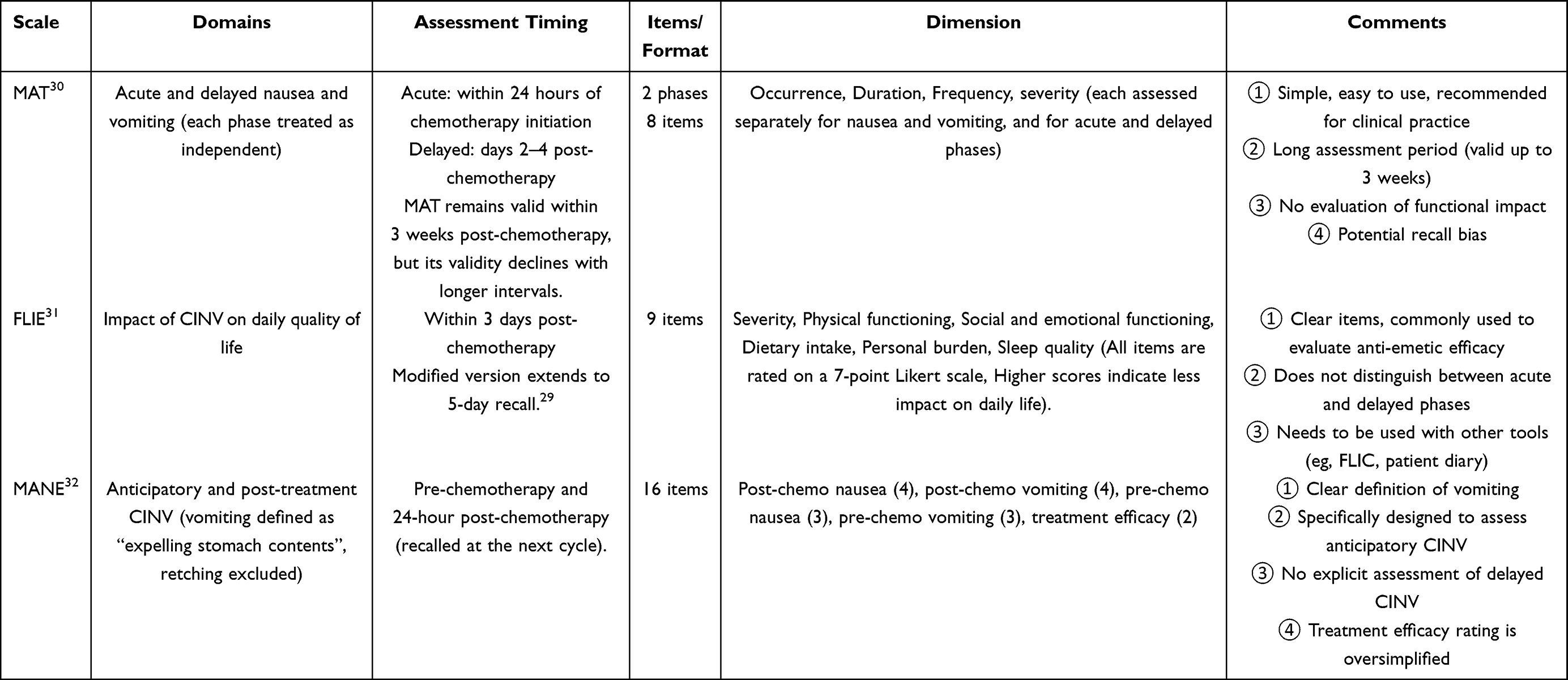 |
Table 2 Comparison of Commonly Used CINV Assessment Tools |
Pharmacologic Prevention
Currently, anti-emetic drugs are widely used in chemotherapy patients and can reduce the incidence of vomiting in patients to about 20%.33 First, nurses can help doctors assess the emetogenic risk level of the chemotherapy regimen. For patients receiving highly emetogenic chemotherapy (HEC), a three-drug combination consisting of an NK1 receptor antagonist (RA), a 5-HT3 RA, and dexamethasone has long been the standard of care. More recently, guidelines have been updated to include the anti-psychotic agent olanzapine.19 By blocking multiple receptors, including 5-HT3 and dopamine, olanzapine has demonstrated particular efficacy in controlling the delayed phase of chemotherapy-induced nausea and vomiting (CINV). This was clearly evidenced by the 2019 J-Force trial, a randomized controlled study in patients receiving cisplatin-based chemotherapy.22 It showed that adding olanzapine (5 mg on days 1–4) to the standard triplet regimen significantly improved delayed-phase control, achieving a complete response rate of 79% compared to 66% in the placebo group. While mild sedation is a common adverse effect, more recent evidence suggests that a reduced dose of 2.5mg provides comparable anti-emetic efficacy with significantly less daytime somnolence. These findings support the use of a lower starting dose or bedtime administration in clinical practice to optimize the balance between efficacy and tolerability.
Integrative Oncology for CINV in Breast Cancer Patients
Non‑pharmacologic prevention is an essential component of comprehensive CINV management, encompassing behavioral interventions, physical therapies, dietary guidance, health education, psychological support, and symptom monitoring. These integrated interventions have been shown to effectively reduce gastrointestinal symptoms and improve patients’ self‑efficacy and quality of life.
Behavioral Interventions
Behavioral interventions are now a well‑established component of supportive care for CINV in breast cancer patients, particularly for preventing anticipatory nausea and vomiting.34 Evidence indicates that these symptoms are closely associated with pre‑chemotherapy anxiety.35 Standard anti-emetics effectively control the physiological aspects of CINV by targeting neurotransmitter pathways such as 5‑HT3 and NK1 receptors. However, they have limited efficacy against the psychological dimension including conditioned nausea and anxiety‑driven symptoms. Behavioral interventions work through cognitive, emotional, and conditioned learning pathways, offering a different mechanism of action.
Relaxation and Cognitive‑Behavioral Strategies
Cognitive-behavioral interventions have been shown to effectively reduce CINV.36 Among these, progressive muscle relaxation training (PMRT) is the most thoroughly studied method. Given that anxiety is a significant risk factor for CINV, the anti-emetic effect of PMRT may be partly mediated through anxiety reduction. Indeed, Tan et al showed that PMRT significantly reduced anxiety levels, improved quality of life, and achieved better control of nausea and vomiting.37
Adding guided imagery to PMRT provides additional benefit. A randomized trial by Yoo et al in newly diagnosed breast cancer patients found that this combined intervention reduced episodes of anticipatory and post‑chemotherapy nausea and vomiting and improved quality of life at six‑month follow‑up.38 Charalambous et al also reported that the combination of guided imagery and progressive muscle relaxation significantly reduced retching, anxiety, and depression.39
Music therapy offers a low‑intensity, easily scalable option. A meta‑analysis by Wei et al showed that music interventions reduced the incidence of CINV and decreased the severity of delayed vomiting.40 Based on this evidence, NCCN recognizes music as an acceptable adjunct to standard anti-emetic therapy for CINV, including anticipatory symptoms.41
Notably, even brief, nurse‑led interventions can be effective. Hunter et al compared a 20‑minute mindfulness relaxation (higher intensity) versus relaxing music (lower intensity) in a predominantly female chemotherapy population (85% breast cancer patients). Both interventions significantly reduced nausea at the midpoint of chemotherapy compared with standard care (mindfulness relaxation: OR = 0.44, 95% CI 0.20–0.93; relaxing music: OR = 0.40, 95% CI 0.20–0.93), indicating good feasibility for implementation.42
Taken together, these findings suggest that relaxation and cognitive-behavioral strategies may be useful adjuncts to pharmacotherapy, particularly for psychological symptoms. However, the strength of recommendation varies across intervention types.
Systematic Desensitization
For patients who develop more severe anticipatory symptoms, a different behavioral approach may be recommended. Systematic desensitization is a behavioral therapy based on classical conditioning. The patient first learns to relax and is then gradually exposed to stimuli that typically trigger nausea or vomiting, such as chemotherapy-related environments, smells, or images. This process reduces the conditioned response over time.
For patients who have developed anticipatory nausea and vomiting, systematic desensitization is currently the best behavioral intervention. A meta-analysis by Kobayashi et al showed that systematic desensitization significantly improved anticipatory CINV compared with control groups, with risk ratios of 0.60 for nausea and 0.54 for vomiting.43 However, the analysis also noted that most included studies had a high or unclear risk of bias, and adverse events were not consistently reported. Therefore, despite its strong theoretical rationale and promising preliminary evidence, systematic desensitization requires further high-quality randomized controlled trials before routine clinical implementation.
Individual Differences and Personalized Interventions
Responses to behavioral interventions vary considerably among patients. Emerging evidence suggests that individual differences in sensory perception and autonomic reactivity may predict which patients are most likely to benefit from a given behavioral intervention. Chemotherapy-induced side effects are associated with increased autonomic nervous system activity and heightened individual stress reactivity. Notably, individuals with high “absorption” traits or heightened sensitivity are at greater risk of developing side effects but may also be more responsive to guided imagery and relaxation-based interventions.44 These findings indicate that behavioral interventions should be matched to a patient’s psychological characteristics. Such personalization is likely to yield better outcomes than applying a standard intervention to all patients, though this has yet to be tested in prospective studies.
Stepped-Care Strategy
Based on the available evidence, a stepped‑care strategy is a practical approach in clinical settings.45 For patients with mild anxiety or early conditioned nausea, low-intensity, easily scalable interventions such as PMRT or music therapy may be offered as first-line behavioral support. For patients who develop clear anticipatory nausea and vomiting, referral for systematic desensitization should be considered. This strategy avoids over-treatment while ensuring that patients with refractory symptoms receive appropriately intensive behavioral therapy.
Physical Therapies
Acupoint Stimulation
Acupoint stimulation is recommended by the National Comprehensive Cancer Network (NCCN) guidelines as a complementary intervention for CINV. In particular, auricular acupressure combined with acupoint pressing has been shown to effectively reduce the incidence of delayed nausea and vomiting.
In traditional Chinese medical theory, the meridian system is a network of channels through which the life-energy known as “Qi” flows.46 Neiguan (PC6) is located on the Pericardium Channel of Hand Jueyin and is closely associated with the functions of the stomach, heart, and chest. Stimulating PC6 helps harmonize stomach Qi and relieve nausea and vomiting. In auricular therapy, the ear acts as a microsystem that reflects the entire body, with specific points corresponding to areas such as the spleen, stomach, and sympathetic nervous system. These theoretical foundations provide a traditional medical basis for the use of acupoint stimulation in managing CINV in breast cancer patients.
Modern molecular biological studies showed that the anti-emetic mechanism of acupoint stimulation involves multiple neuro-endocrine pathways.47,48 Stimulating a surface point such as PC6 activates Aβ and C afferent fibers.49 These fibers transmit signals through the spinal cord to the vomiting center and the chemoreceptor trigger zone (CTZ) in the brainstem, and also to higher centers like the cerebral cortex. This signal transmission induces endorphinergic cells to release endorphins. Endorphins then suppress the excitability of the CTZ, thereby reducing the triggering of vomiting signals. At the same time, stimulation of the periaqueductal gray matter in the midbrain leads to the release of enkephalins. In addition, activation of the hypothalamic-pituitary axis prompts the pituitary gland to secrete β-endorphin and adrenocorticotropic hormone (ACTH).50 Together, these endogenous opioid peptides and hormones then modulate the serotonin (5-HT) neurotransmitter system, thereby exerting a central anti-emetic effect.51 Furthermore, acupoint stimulation activates the vagus nerve and modulates the brain-gut axis, thereby improving gastrointestinal motility and secretory function.52
Auricular acupuncture therapy appears to have a beneficial effect on CINV. Analyses showed that auricular stimulation reduces the risk of nausea and vomiting.53,54 Notably, it is effective in both the acute and delayed phases after chemotherapy, with particularly pronounced efficacy in the delayed phase.55 Furthermore, auricular therapy reduces the incidence of belching, acid regurgitation, and appetite loss (OR=0.33), and significantly alleviates constipation.56 A separate meta‑analysis of acupressure at the PC6 point reported significant reductions in acute nausea (SMD = –0.39) and delayed nausea (SMD = –0.51).57 However, the included trials generally had small sample sizes and a high risk of bias, which limits the strength of this evidence.
The benefit of acupoint stimulation may be more pronounced in specific patient populations. For patients receiving highly emetogenic chemotherapy but unable to follow guideline‑consistent anti-emetic regimens for economic or personal reasons, a portable, non‑invasive device for acupoint stimulation may improve complete response rates and quality‑of‑life scores for nausea and vomiting.
In summary, acupoint stimulation as an adjunct to conventional anti-emetic regimens has definite clinical value. It helps alleviate chemotherapy‑induced gastrointestinal adverse reactions, such as nausea, vomiting, loss of appetite, and constipation. Future research should focus on optimizing stimulation parameters, defining the best timing of intervention, and validating its standardized application in cancer supportive care through large, multi-center trials.
Exercise
Exercise is a potentially useful non-pharmacologic intervention for preventing and reducing CINV symptoms in breast cancer patients receiving chemotherapy. Different types of exercise, including yoga, aerobic and resistance training, and respiratory training have been shown to effectively alleviate CINV.
Multiple studies have reported benefits of yoga for CINV management. A systematic review of 20 randomized controlled trials suggested that six styles of yoga improved short-term treatment-related complications, including nausea and vomiting.58 These findings were further supported by a randomized controlled study showing that a 12-week yoga intervention significantly reduced nausea and vomiting at the 6-month follow-up in breast cancer patients.59 Moreover, Selvan et al demonstrated that yoga also alleviated the frequency and severity of nausea, anticipatory nausea, and vomiting.60
Similarly, aerobic exercise may represent an option for helping patients to control these symptoms as well. Patients receiving moderate-to-high intensity aerobic exercise combined with resistance training had significantly lower rates of nausea and vomiting.61 Notably, patients in the higher-intensity exercise program also required fewer chemotherapy dose adjustments and returned to work earlier. In contrast, even a home‑based program consisting of five 30‑minute sessions of low‑to‑moderate physical activity per week was also associated with less decline in cardiorespiratory fitness, less nausea and vomiting, and better physical function.62
Beyond the benefits of sustained exercise, even a single exercise can also provide immediate relief. An observational study of 38 breast cancer patients undergoing chemotherapy demonstrated that energy increased and nausea decreased immediately after a single session of endurance or resistance training.63 These findings challenge the prevailing dogma that exercise should be avoided during treatment. Instead, patients should be encouraged to exercise even if they experience nausea during chemotherapy.
In addition, Respiratory training has also been shown to be effective in reducing CINV in breast cancer patients. A randomized controlled trial demonstrated that a 6‑day respiratory exercises significantly reduced the frequency of nausea, vomiting, and retching, decreased nausea severity, and improved functional status.64
It should be noted that exercise should be delivered or supervised by trained professionals to avoid unintended harm, particularly in patients at risk of nausea or vomiting. According to the American College of Sports Medicine (ACSM) guidelines, cancer patients are recommended to perform at least 90 minutes of moderate‑intensity aerobic exercise per week, along with strength training twice weekly.65 However, these recommendations should be tailored to each patient’s condition to offer most benefits. For example, when a patient experiences moderate nausea or vomiting, temporarily reducing exercise intensity or duration may help prevent symptom aggravation. In cases of severe nausea or vomiting, exercise may be suspended until gastrointestinal symptoms resolve.
Dietary and Nutritional Guidance
Dietary and nutritional management is an essential component of supportive care for breast cancer patients undergoing chemotherapy. As highlighted by Belluomini et al, despite advances in anti-emetic drugs, approximately 30% of adult patients still experience CINV, which can lead to electrolyte imbalance, anorexia, and treatment interruption.66 Early and individualized nutritional counseling has been shown to effectively reduce the severity of nausea and vomiting, optimize patient outcomes, and is both safe and feasible.67 Based on current evidence, the following principles should guide dietary and nutritional advice for breast cancer patients during chemotherapy.
General Principles
Patients should eat a small, light meal 1–2 hours before chemotherapy and avoid undergoing treatment on an empty stomach or in an overly full state. Five to six small meals per day are recommended to reduce the gastrointestinal load per meal and lower the likelihood of triggering nausea. In addition, patients should avoid lying down immediately after eating to prevent gastroesophageal reflux that may exacerbate nausea.
Nutrient Recommendations
For protein, guidelines recommend a daily intake of at least 1.0 to 1.5 g/kg of body weight to maintain lean body mass and prevent sarcopenia.68 This is particularly important for breast cancer patients, as increased catabolism and reduced appetite during chemotherapy often lead to insufficient protein intake. Regarding carbohydrates and fats, daily energy intake should consist of approximately 55% carbohydrates, mainly complex carbohydrates such as whole grains, oats, and brown rice, while fats, primarily monounsaturated and polyunsaturated fatty acids, should be less than 30%. A daily intake of five to nine servings of vegetables and fruits is recommended, with each serving equivalent to about 150 grams of fruit or 75 grams of vegetables. Moreover, the daily diet should include garlic and cruciferous vegetables such as broccoli and cabbage. As for fluids and electrolytes, patients with CINV are prone to dehydration and electrolyte disturbances. Therefore, patients should be encouraged to drink small amounts of warm water, light salt water, or oral rehydration solution at frequent intervals, avoiding large volumes at one time that may trigger nausea.
Special Dietary Components
A meta-analysis by Lin et al reported that ginger capsules combined with standard anti‑emetic drugs were associated with a reduced incidence of grade 3 acute nausea and severe vomiting, with acceptable safety.69 Therefore, ginger supplementation starting before chemotherapy may be considered as an adjunct to standard anti-emetics, though optimal dosing and potential drug interactions warrant further investigation. Additionally, a daily intake of 2 to 2.2 grams of omega‑3 fatty acids, specifically EPA and DHA, can improve appetite, food intake, and weight maintenance.70 Their anti‑inflammatory properties help reduce inflammation and counteract cachexia.
In summary, nutritional education and support are integral components of comprehensive management. Dietary and nutritional guidance for breast cancer patients during chemotherapy should be individualized. Based on adequate energy and protein intake, a small‑meal, light‑and‑easy‑to‑digest eating pattern is recommended, along with appropriate supplementation of evidence‑based dietary components such as ginger and omega‑3 fatty acids.
Discussion
For a long time, the clinical management of CINV has largely adopted a passive model in which symptoms are treated after they occur. This model has very limited efficacy in controlling CINV in patients with breast cancer, particularly for delayed nausea and vomiting and anticipatory nausea and vomiting. Once severe CINV develops, even intensified interventions often fail to achieve complete control, frequently leading to chemotherapy dose reduction or treatment discontinuation. Therefore, CINV management should shift from reactive treatment to proactive prevention, from hospital‑based to community‑extending care, and from single‑modality pharmacotherapy to multi-modal integrated management.71 However, realizing this shift requires healthcare system support, including adequate staffing, patient education infrastructure, and remote monitoring tools.
In clinical practice, two long-underestimated issues contribute to poor CINV control. First, underreporting of symptoms is common. Most patients regard nausea and vomiting as an inevitable accompaniment of chemotherapy and choose to endure symptoms for fear of increasing the burden on healthcare providers or causing treatment adjustments. Second, adherence to anti-emetic therapy after discharge is poor. Patients often take their medication only after symptoms have already developed, which defeats the fundamental principle that anti-emetics should be used prophylactically. Inadequate symptom‑related knowledge and weak self‑management skills among patients are important reasons for impaired long‑term quality of life.72 Accordingly, healthcare professionals should provide systematic health education. They need to clearly tell patients that CINV is preventable and manageable. They should also instruct patients to report symptoms promptly and teach simple non-pharmacologic approaches, such as dietary modifications, acupressure, and relaxation training. By doing so, self‑management can be integrated into the entire post‑discharge rehabilitation process.
Among all types of CINV, delayed CINV and anticipatory CINV are the most difficult to manage and represent the most prominent unmet needs of breast cancer patients. Delayed CINV typically occurs 24–120 hours after discharge, when patients are no longer under direct medical supervision. Patients often tolerate symptoms at home without seeking help. By the time they present for medical attention, they may already have developed loss of appetite, dehydration, or electrolyte disturbances. These complications significantly increase long‑term physical exhaustion and nutritional risk. Routine follow‑up telephone calls 48–72 hours after discharge, or daily symptom recording using an electronic patient‑reported outcome (ePRO) system may enable dynamic monitoring and timely regimen adjustment. However, relevant large-scale implementation research remains limited. Anticipatory CINV is essentially a conditioned reflex. It arises from the association between a poorly controlled vomiting experience in a previous chemotherapy cycle and environmental cues related to treatment. Once this reflex is established, conventional anti-emetic drugs become largely ineffective. Therefore, the most effective preventive strategy is to achieve complete control of acute and delayed symptoms in every cycle, thereby preventing the formation of the conditioned association. For patients who have already developed anticipatory CINV, systematic desensitization and cognitive‑behavioral therapy (CBT) are the most evidence‑based interventions. Simply escalating anti-emetic drug types or doses is not sufficient. As international guidelines consistently emphasize, psychosocial intervention is an indispensable component of symptom management for breast cancer survivors. Accordingly, establishing a standardized psychological referral pathway may improve outcomes for patients with anticipatory CINV, although cost-effectiveness data are limited.
Current clinical practice mainly relies on the emetogenic risk classification of chemotherapy regimens to guide anti-emetic strategies. However, this framework fails to account for the substantial interindividual variability in treatment response. Treatment‑related toxicities in breast cancer exhibit significant individual susceptibility, influenced by host factors such as age, menopausal status, and psychological state.24 Therefore, beyond risk classification, clinicians should identify high-risk individuals before chemotherapy and implement intensified interventions, such as combining pharmacotherapy with early behavioural intervention. In this way, anti-emetic management may shift from a regimen-based approach to precise stratification and individualized care.
Non‑pharmacological interventions such as music therapy, relaxation training, and mindfulness training are safe, low‑cost, and complement pharmacotherapy. However, their application is limited by wide variation in study designs and a lack of standardization, which makes it difficult to draw definitive conclusions about their effectiveness. Another related and distinct challenge is resource limitation. In routine clinical practice, it is often unclear who should deliver these interventions and how to ensure patient adherence. Given these practical constraints, a stepped-care model offers a viable solution. Under this model, all patients receive basic self-administered support, including health education and music resources. Patients at intermediate or high risk receive brief relaxation training provided by nurses. Only those with anticipatory symptoms or refractory CINV are referred to specialists for systematic desensitization or cognitive-behavioral therapy. This approach allocates limited resources efficiently by matching intervention intensity to symptom severity, while maintaining accessibility for the majority of patients. Although this stepped-care model is theoretically sound, its clinical and cost-effectiveness have yet to be rigorously evaluated.
Multidisciplinary collaborative care of CINV management should also incorporate family support and cultural factors. Many patients adopt passive coping strategies after discharge because they do not want to increase the burden on their families. At the same time, their need for family support increases during peak symptom periods. Healthcare professionals should therefore actively educate family members about the impact of CINV and the importance of their involvement, helping to build a stable support system at home. Cultural differences in symptom reporting also matter. Chinese patients often describe symptoms indirectly, using terms like “poor appetite” or “stomach discomfort” rather than explicitly reporting nausea and vomiting. To avoid underestimation of symptoms, clinicians should minimize technical jargon, use open-ended questions, and consider culturally adapted assessment tools.
Future research should prioritize the development of individualized risk prediction tools, real‑world implementation strategies for non-pharmacologic interventions, standardized mobile health monitoring, and culturally tailored education and care models. These approaches would enable multidisciplinary collaborative care of CINV management and improve treatment adherence and long‑term quality of life in breast cancer patients.
We acknowledge that this review is not entirely comprehensive. The field of CINV management is evolving rapidly, and despite our efforts to provide a broad synthesis of evidence, several emerging areas could not be fully covered due to limited evidence. These include individualized risk prediction models based on artificial intelligence and machine learning, as well as wearable devices for real-time symptom monitoring. These emerging areas are promising and deserve further research to advance the future of CINV care.
Conclusions
CINV management in breast cancer patients should be guided by the emetogenic risk stratification of chemotherapy regimens and fully consider individual risk factors. The combination of pharmacologic and non-pharmacologic interventions can minimize the impact of gastrointestinal toxicity on treatment delivery and quality of life. Nevertheless, there is still considerable work ahead in the management of CINV. A substantial proportion of patients continue to experience delayed or anticipatory nausea and vomiting, underreport symptoms, or show poor adherence to anti-emetic regimens. These challenges frequently result in suboptimal response to current anti-emetic regimens and, in severe cases, chemotherapy interruption. Future advances will likely require developing novel agents with distinct mechanisms of action, integrating non-pharmacologic options more effectively into routine clinical practice, and establishing individualized risk prediction tools with remote monitoring to improve ou-of-hospital symptom management. Addressing these unmet needs will be critical to improving CINV management and sustaining treatment adherence.
Data Sharing Statement
Data availability is not applicable to this article as no new data were created or analyzed in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Zhejiang Province Traditional Chinese Medicine Science and Technology Program (2024ZL090).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Kim J, Harper A, McCormack V, et al. Global patterns and trends in breast cancer incidence and mortality across 185 countries. Nat Med. 2025;31(4):1154–14. doi:10.1038/s41591-025-03502-3
2. Akbarali HI, Muchhala KH, Jessup DK, Cheatham S. Chemotherapy induced gastrointestinal toxicities. Adv Cancer Res. 2022;155:131–166. doi:10.1016/bs.acr.2022.02.007
3. Henson LA, Maddocks M, Evans C, Davidson M, Hicks S, Higginson IJ. Palliative care and the management of common distressing symptoms in advanced cancer: pain, breathlessness, nausea and vomiting, and fatigue. J Clin Oncol. 2020;38(9):905–914. doi:10.1200/JCO.19.00470
4. Piccioni AL. Out-patient management of nausea and vomiting in multiday therapy of acute myeloid leukemia in the elderly. Use of granisetron in slow-release transdermal formulation. Clinical case. Recenti Prog Med. 2019;110(3):10e–13e. doi:10.1701/3132.31185
5. Chen W, Zhao Y, Dai Y, Nie K. Gastrointestinal inflammation plays a critical role in chemotherapy-induced nausea and vomiting. Eur J Pharmacol. 2022;936:175379. doi:10.1016/j.ejphar.2022.175379
6. Jordan K, de Azambuja E, García Del Barrio MÁ, et al. Going beyond the 2023 MASCC and ESMO guideline update for the prevention of chemotherapy- and radiotherapy-induced nausea and vomiting. Eur J Cancer. 2025;222:115451. doi:10.1016/j.ejca.2025.115451
7. Zhang J, Lu Y, Zhang N, et al. Global burden of female breast cancer and its association with socioeconomic development status, 1990-2044. Cancer Rep. 2023;6 Suppl 1(Suppl 1):e1827. doi:10.1002/cnr2.1827
8. Arnold M, Morgan E, Rumgay H, et al. Current and future burden of breast cancer: global statistics for 2020 and 2040. Breast. 2022;66:15–23. doi:10.1016/j.breast.2022.08.010
9. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
10. Qi Y, Li H, Guo Y, Cao Y, Wong CL. Symptom clusters in breast cancer patients receiving adjuvant chemotherapy: a systematic review. J Clin Nurs. 2024;33(12):4554–4567. doi:10.1111/jocn.17479
11. Herrstedt J, Celio L, Hesketh PJ, et al. 2023 updated MASCC/ESMO consensus recommendations: prevention of nausea and vomiting following high-emetic-risk antineoplastic agents. Support Care Cancer. 2023;32(1):47. doi:10.1007/s00520-023-08221-4
12. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: antiemesis. Version 2.2024. Plymouth Meeting, PA: National Comprehensive Cancer Network; 2024.
13. Berger MJ, Ettinger DS, Aston J, et al. NCCN guidelines insights: antiemesis, version 2.2017. J Natl Compr Canc Netw. 2017;15(7):883–893. doi:10.6004/jnccn.2017.0117
14. Jordan K, Chan A, Gralla RJ, et al. Emetic risk classification and evaluation of the emetogenicity of antineoplastic agents-updated MASCC/ESMO consensus recommendation. Support Care Cancer. 2023;32(1):53. doi:10.1007/s00520-023-08220-5
15. Scotté F, Schwartzberg L, Iihara H, et al. 2023 updated MASCC/ESMO Consensus recommendations: prevention of nausea and vomiting following moderately emetic risk antineoplastic agents. Support Care Cancer. 2023;32(1):45. doi:10.1007/s00520-023-08222-3
16. Olver I, Clark-Snow R, Ruhlmann CH, et al. 2023 updated MASCC/ESMO consensus recommendations: controlling nausea and vomiting with chemotherapy of low or minimal emetic potential. Support Care Cancer. 2023;32(1):37. doi:10.1007/s00520-023-08223-2
17. Llombart-Cussac A, Ramos M, Dalmau E, et al. Incidence of chemotherapy-induced nausea and vomiting associated with docetaxel and cyclophosphamide in early breast cancer patients and aprepitant efficacy as salvage therapy. Results from the Spanish breast cancer group/2009-02 study. Eur J Cancer. 2016;58:122–129. doi:10.1016/j.ejca.2016.01.015
18. Navari RM, Ruddy KJ, LeBlanc TW, et al. Avoidable acute care use associated with nausea and vomiting among patients receiving highly emetogenic chemotherapy or oxaliplatin. Oncologist. 2021;26(4):325–331. doi:10.1002/onco.13620
19. Herrstedt J, Clark-Snow R, Ruhlmann CH, et al. 2023 MASCC and ESMO guideline update for the prevention of chemotherapy- and radiotherapy-induced nausea and vomiting. ESMO Open. 2024;9(2):102195. doi:10.1016/j.esmoop.2023.102195
20. Cheng J, Xu J, Shi R, Zhu W, Lu M, Mao Y. Chemotherapy-induced nausea and vomiting symptom experience in patients with non-small-cell lung cancer: a qualitative study. Medicine (Baltimore). 2025;104(47):e45097. doi:10.1097/MD.0000000000045097
21. Yeo W, Mo FKF, Yip CCH, et al. Quality of life associated with nausea and vomiting from anthracycline-based chemotherapy: a pooled data analysis from three prospective trials. Oncologist. 2021;26(12):e2288–e2296. doi:10.1002/onco.13978
22. Hashimoto H, Abe M, Tokuyama O, et al. Olanzapine 5 mg plus standard anti-emetic therapy for the prevention of chemotherapy-induced nausea and vomiting (J-FORCE): a multicentre, randomised, double-blind, placebo-controlled, Phase 3 trial. Lancet Oncol. 2020;21(2):242–249. doi:10.1016/S1470-2045(19)30678-3
23. Hsu HT, Lin KC, Wu LM, et al. Symptom cluster trajectories during chemotherapy in breast cancer outpatients. J Pain Symptom Manag. 2017;53(6):1017–1025. doi:10.1016/j.jpainsymman.2016.12.354
24. Mosa ASM, Hossain AM, Lavoie BJ, Yoo I. Patient-related risk factors for chemotherapy-induced nausea and vomiting: a systematic review. Front Pharmacol. 2020;11:329. doi:10.3389/fphar.2020.00329
25. Mukoyama N, Yoshimi A, Goto A, et al. An analysis of behavioral and genetic risk factors for chemotherapy-induced nausea and vomiting in Japanese subjects. Biol Pharm Bull. 2016;39(11):1852–1858. doi:10.1248/bpb.b16-00440
26. Clemons M, Bouganim N, Smith S, et al. Risk model-guided antiemetic prophylaxis vs physician’s choice in patients receiving chemotherapy for early-stage breast cancer: a randomized clinical trial. JAMA Oncol. 2016;2(2):225–231. doi:10.1001/jamaoncol.2015.3730
27. Alves RB, Rebouças CV, Yamada AMTD, Cruz FJSM. Prevalence of anticipatory nausea and vomiting in breast cancer patients undergoing highly emetogenic chemotherapy. Rev Assoc Med Bras. 2024;70(4):e20230937. doi:10.1590/1806-9282.20230937
28. Matsuda Y, Okita K, Furuhata T, et al. Evaluation of the validity of chemotherapy-induced nausea and vomiting assessment in outpatients using the Japanese version of the MASCC antiemesis tool. Support Care Cancer. 2015;23(11):3331–3339. doi:10.1007/s00520-015-2780-z
29. Martin AR, Pearson JD, Cai B, Elmer M, Horgan K, Lindley C. Assessing the impact of chemotherapy-induced nausea and vomiting on patients’ daily lives: a modified version of the functional living index-emesis (FLIE) with 5-day recall. Support Care Cancer. 2003;11(8):522–527. doi:10.1007/s00520-003-0482-4
30. Molassiotis A, Coventry PA, Stricker CT, et al. Validation and psychometric assessment of a short clinical scale to measure chemotherapy-induced nausea and vomiting: the MASCC anti-emesis tool. J Pain Symptom Manag. 2007;34(2):148–159. doi:10.1016/j.jpainsymman.2006.10.018
31. Martin AR, Carides AD, Pearson JD, et al. Functional relevance of antiemetic control. Experience using the FLIE questionnaire in a randomised study of the NK-1 antagonist aprepitant. Eur J Cancer. 2003;39(10):1395–1401. doi:10.1016/s0959-8049(03)00299-5
32. Morrow GR. A patient report measure for the quantification of chemotherapy induced nausea and emesis: psychometric properties of the Morrow assessment of nausea and emesis (MANE). Br J Cancer Suppl. 1992;19:S72–S74.
33. Babu G, Saldanha SC, Kuntegowdanahalli Chinnagiriyappa L, et al. The efficacy, safety, and cost benefit of olanzapine versus aprepitant in highly emetogenic chemotherapy: a pilot study from South India. Chemother Res Pract. 2016;2016:3439707. doi:10.1155/2016/3439707
34. Morrow GR, Asbury R, Hammon S, et al. Comparing the effectiveness of behavioral treatment for chemotherapy-induced nausea and vomiting when administered by oncologists, oncology nurses, and clinical psychologists. Health Psychol. 1992;11(4):250–256. doi:10.1037//0278-6133.11.4.250
35. Rodríguez M. Individual differences in chemotherapy-induced anticipatory nausea. Front Psychol. 2013;4:502. doi:10.3389/fpsyg.2013.00502
36. Samami E, Shahhosseini Z, Hamzehgardeshi Z, Elyasi F. Psychological interventions in chemotherapy-induced nausea and vomiting in women with breast cancer: a systematic review. Iran J Med Sci. 2022;47(2):95–106. doi:10.30476/ijms.2020.86657.1660
37. Tan L, Fang P, Cui J, Yu H, Yu L Effects of progressive muscle relaxation on health‑related outcomes in cancer patients: a systematic review and meta‑analysis of randomized controlled trials. Complement Ther Clin Pract. 2022;49:101676.
38. Yoo HJ, Ahn SH, Kim SB, Kim WK, Han OS. Efficacy of progressive muscle relaxation training and guided imagery in reducing chemotherapy side effects in patients with breast cancer and in improving their quality of life. Support Care Cancer. 2005;13(10):826–833. doi:10.1007/s00520-005-0806-7
39. Charalambous A, Giannakopoulou M, Bozas E, Marcou Y, Kitsios P, Paikousis L. Guided imagery and progressive muscle relaxation as a cluster of symptoms management intervention in patients receiving chemotherapy: a randomized control trial. PLoS One. 2016;11(6):e0156911. doi:10.1371/journal.pone.0156911
40. Wei TT, Tian X, Zhang FY, Qiang WM, Bai AL. Music interventions for chemotherapy-induced nausea and vomiting: a systematic review and meta-analysis. Support Care Cancer. 2020;28(9):4031–4041. doi:10.1007/s00520-020-05409-w
41. Molassiotis A, Affronti ML, Fleury M, Olver I, Giusti R, Scotte F. 2023 MASCC/ESMO consensus anti-emetic guidelines related to integrative and non-pharmacological therapies. Support Care Cancer. 2023;32(1):30. doi:10.1007/s00520-023-08225-0
42. Hunter JJ, Maunder RG, Sui D, et al. A randomized trial of nurse-administered behavioral interventions to manage anticipatory nausea and vomiting in chemotherapy. Cancer Med. 2020;9(5):1733–1740. doi:10.1002/cam4.2863
43. Kobayashi M, Kako J, Iba A, et al. Non‑pharmacological treatments for anticipatory nausea and vomiting during chemotherapy: a systematic review and meta‑analysis of the clinical practice guidelines for antiemesis 2023. Int J Clin Oncol. 2024;29(7). doi:10.1007/s10147
44. Zachariae R, Paulsen K, Mehlsen M, Jensen AB, Johansson A, von der Maase H. Chemotherapy-induced nausea, vomiting, and fatigue--the role of individual differences related to sensory perception and autonomic reactivity. Psychother Psychosom. 2007;76(6):376–384. doi:10.1159/000107566
45. Affronti ML, Lee J, Molassiotis A, et al. MASCC 2023 patient-centered anti-emetic guidelines and education statements: an evidence-based and consensus resource for patients. Support Care Cancer. 2024;32(6):335. doi:10.1007/s00520-024-08543-x
46. Wenxi YU, Lina T, Hongtao LI, Yonggang W, Zan S. Neiguan (PC6) acupoint stimulation for preventing chemotherapy-induced nausea and vomiting: a cost-effective supplement in guideline-inconsistent chemotherapy-induced nausea and vomiting prophylaxis subgroup. J Tradit Chin Med. 2024;44(3):581–585. doi:10.19852/j.cnki.jtcm.20240402.005
47. Takahashi T. Mechanism of acupuncture on neuromodulation in the gut--a review. Neuromodulation. 2011;14(1):8–12. doi:10.1111/j.1525-1403.2010.00295.x
48. Takahashi T. Effect and mechanism of acupuncture on gastrointestinal diseases. Int Rev Neurobiol. 2013;111:273–294. doi:10.1016/B978-0-12-411545-3.00014-6
49. Zhao ZQ. Neural mechanism underlying acupuncture analgesia. Prog Neurobiol. 2008;85(4):355–375. doi:10.1016/j.pneurobio.2008.05.004
50. Pan B, Castro-Lopes JM, Coimbra A. Activation of anterior lobe corticotrophs by electroacupuncture or noxious stimulation in the anaesthetized rat, as shown by colocalization of Fos protein with ACTH and beta-endorphin and increased hormone release. Brain Res Bull. 1996;40(3):175–182. doi:10.1016/0361-9230(96)00011-1
51. Zhang X, Jin HF, Fan YH, Lu B, Meng LN, Chen JD. Effects and mechanisms of transcutaneous electroacupuncture on chemotherapy-induced nausea and vomiting. Evid Based Complement Alternat Med. 2014;2014(1):860631. doi:10.1155/2014/860631
52. Lu M, Chen C, Li W, Yu Z, Xu B. EA at PC6 promotes gastric motility: role of brainstem vagovagal neurocircuits. Evid Based Complement Alternat Med. 2019;2019:7457485. doi:10.1155/2019/7457485
53. Alhusamiah B, Almomani J, Al Omari A, et al. The effectiveness of P6 and auricular acupressure as a complimentary therapy in chemotherapy-induced nausea and vomiting among patients with cancer: systematic review. Integr Cancer Ther. 2024;23:15347354241239110. doi:10.1177/15347354241239110
54. Issac A, Nayak SG, Halemani K, Mishra P, Chand G. Acupressure on chemotherapy-induced nausea and vomiting among breast cancer patients: a systematic review and meta-analysis. Asian Pac J Cancer Prev. 2024;25(10):3421–3428. doi:10.31557/APJCP.2024.25.10.3421
55. Shen G, Ren D, Zhao F, et al. Effect of adding electroacupuncture to standard triple anti-emetic therapy on chemotherapy-induced nausea and vomiting: a randomized controlled clinical trial. J Clin Oncol. 2024;42(34):4051–4059. doi:10.1200/JCO.24.00099
56. Chen K, Zhang N, Ye T. Effectiveness of auricular acupoint therapy on chemotherapy-induced gastrointestinal reaction in breast cancer patients: a systematic review and meta-analysis. Holist Integ Oncol. 2024;3(1):67. doi:10.1007/s44178-024-00147-z
57. Xiao C, Qin M, Xia H, Xing Q, Wang D, Qian W. Effects of PC6 acupressure on acute and delayed nausea and vomiting induced by chemotherapy in patients with malignant neoplasm: a meta-analysis. Support Care Cancer. 2023;31(9):510. doi:10.1007/s00520-023-07976-0
58. Neelam K, Mani S, Chellappan K. Yoga for treatment-related complications in patients with breast cancer: a systematic review of randomized control trials. Curr Cancer Ther Rev. 2025;21(5):721–733. doi:10.2174/0115733947307543240725101158
59. Jong MC, Boers I, Schouten van der Velden AP, et al. A randomized study of yoga for fatigue and quality of life in women with breast cancer undergoing (Neo) adjuvant chemotherapy. J Altern Complement Med. 2018;24(9–10):942–953. doi:10.1089/acm.2018.0191
60. Selvan P, Hriso C, Mitchell J, Newberg A. Systematic review of yoga for symptom management during conventional treatment of breast cancer patients. Complement Ther Clin Pract. 2022;48:101581. doi:10.1016/j.ctcp.2022.101581
61. Van Waart H, Stuiver MM, van Harten WH, et al. Effect of low-intensity physical activity and moderate- to high-intensity physical exercise during adjuvant chemotherapy on physical fitness, fatigue, and chemotherapy completion rates: results of the PACES randomized clinical trial. J Clin Oncol. 2015;33(17):1918–1927. doi:10.1200/JCO.2014.59.1081
62. Van Waart H, Stuiver MM, van Harten WH, et al. Recruitment to and pilot results of the PACES randomized trial of physical exercise during adjuvant chemotherapy for colon cancer. Int J Colorectal Dis. 2018;33(1):29–40. doi:10.1007/s00384-017-2921-6
63. Johnsson A, Demmelmaier I, Sjövall K, Wagner P, Olsson H, Tornberg ÅB. A single exercise session improves side-effects of chemotherapy in women with breast cancer: an observational study. BMC Cancer. 2019;19(1):1073. doi:10.1186/s12885-019-6310-0
64. Vinolo-Gil MJ, Martín-Valero R, Martín-Vega FJ, Rodríguez-Huguet M, Perez-Cabezas V, Gonzalez-Medina G. Respiratory physiotherapy intervention strategies in the sequelae of breast cancer treatment: a systematic review. Int J Environ Res Public Health. 2022;19(7):3800. doi:10.3390/ijerph19073800
65. Campbell KL, Winters-Stone KM, Wiskemann J, et al. Exercise guidelines for cancer survivors: consensus statement from international multidisciplinary roundtable. Med Sci Sports Exerc. 2019;51(11):2375–2390. doi:10.1249/MSS.0000000000002116
66. Belluomini L, Avancini A, Sposito M, et al. Integrating nutrition, physical exercise, psychosocial support and anti-emetic drugs into CINV management: the road to success. Crit Rev Oncol Hematol. 2024;201:104444. doi:10.1016/j.critrevonc.2024.104444
67. James S, Oppermann A, Schotz KM, et al. Nutritional counseling during chemotherapy treatment: a systematic review of feasibility, safety, and efficacy. Curr Oncol. 2024;32(1):3. doi:10.3390/curroncol32010003
68. Limon-Miro AT, Lopez-Teros V, Astiazaran-Garcia H. Dietary guidelines for breast cancer patients: a critical review. Adv Nutr. 2017;8(4):613–623. doi:10.3945/an.116.014423
69. Lin CY, Huang SH, Tam KW, Huang TW, Gautama MSN. Efficacy and safety of ginger on chemotherapy-induced nausea and vomiting: a systematic review and meta-analysis of randomized controlled trials. Cancer Nurs. 2025;48(6):455–466. doi:10.1097/NCC.0000000000001355
70. Hébuterne X, Lemarié E, Michallet M, de Montreuil CB, Schneider SM, Goldwasser F. Prevalence of malnutrition and current use of nutrition support in patients with cancer. JPEN J Parenter Enteral Nutr. 2014;38(2):196–204. doi:10.1177/0148607113502674
71. Warr D. Bringing it all together in the treatment of CINV: application of current knowledge into routine clinical practice. Support Care Cancer. 2018;26(Suppl 1):29–33. doi:10.1007/s00520-018-4117-1
72. Archer W, Ashlock LAR, Chapman JA, Gonzalez JM, Mazur K, Pifer K. Using follow-up telephone calls to identify obstacles to prevention and treatment of chemotherapy-induced nausea and vomiting. Clin J Oncol Nurs. 2023;27(6):644–652. doi:10.1188/23.CJON.644-652
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cost-Effectiveness Analysis of the Oncotype DX Breast Recurrence Score® Test in Node-Negative Early Breast Cancer
Berdunov V, Millen S, Paramore A, Griffin J, Reynia S, Fryer N, Brown R, Longworth L
ClinicoEconomics and Outcomes Research 2022, 14:619-633
Published Date: 19 September 2022
Advice from One Patient to Another: Qualitative Analysis of Patients’ Perspectives About Chemotherapy Initiation
Malinowski C, Paredes E, Housten AJ, Chavez-MacGregor M
Patient Preference and Adherence 2022, 16:3283-3289
Published Date: 14 December 2022
Dietary Behavior and Its Association with Nutrition Literacy and Dietary Attitude Among Breast Cancer Patients Treated with Chemotherapy: A Multicenter Survey of Hospitals in China
Tang H, Wang R, Yan P, Zhang W, Yang F, Guo S, Li T, Yi L, Bai X, Lin S, Zhang Y, Shang L
Patient Preference and Adherence 2023, 17:1407-1419
Published Date: 9 June 2023
Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives
Wang J, Wu SG
Breast Cancer: Targets and Therapy 2023, 15:721-730
Published Date: 20 October 2023
Cost-Effectiveness Analysis of the Oncotype DX Breast Recurrence Score® Test from a US Societal Perspective
Berdunov V, Cuyun Carter G, Laws E, Luo R, Russell CA, Campbell S, Abdou Y, Force J
ClinicoEconomics and Outcomes Research 2024, 16:471-482
Published Date: 4 June 2024