Back to Journals » International Journal of General Medicine » Volume 18
A Multi-Algorithm Machine Learning Model for Predicting the Risk of Preterm Birth in Patients with Early-Onset Preeclampsia
Authors Xu Y ![]() , Zu Y
, Zu Y ![]() , Zhang Y
, Zhang Y ![]() , Liang Z, Xu X, Yan J
, Liang Z, Xu X, Yan J
Received 15 February 2025
Accepted for publication 29 June 2025
Published 4 August 2025 Volume 2025:18 Pages 4195—4207
DOI https://doi.org/10.2147/IJGM.S521763
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Yanhong Xu,1,* Yizheng Zu,2,* Ying Zhang,1,* Zewei Liang,1 Xia Xu,1,3– 5 Jianying Yan1,3– 5
1College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University Fujian Maternity and Child Health Hospital, Fuzhou, Fujian, People’s Republic of China; 2The Affiliated Changzhou Second People’s Hospital of Nanjing Medical University, Changzhou, Jiangsu, People’s Republic of China; 3Fujian Clinical Research Center for Maternal-Fetal Medicine, Fuzhou, Fujian, People’s Republic of China; 4Laboratory of Maternal-Fetal Medicine, Fujian Maternity and Child Health Hospital, Fuzhou, Fujian, People’s Republic of China; 5National Key Obstetric Clinical Specialty Construction Institution of China, Fuzhou, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xia Xu, College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University Fujian Maternity and Child Health Hospital, No. 18 Daoshan Road, Gulou District, Fuzhou, Fujian, People’s Republic of China, Email [email protected] Jianying Yan, College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University Fujian Maternity and Child Health Hospital, No. 18 Daoshan Road, Gulou District, Fuzhou, Fujian, People’s Republic of China, Email [email protected]
Purpose: To analyze the risk factors for preterm birth in patients with early-onset preeclampsia (EOPE) based on multi-algorithm machine learning and to construct a predictive model to explore the predictive value of the model.
Methods: A retrospective analysis was conducted on 442 EOPE patients from a single tertiary center, divided into preterm birth (< 37 weeks, n=358) and term-born (≥ 37 weeks, n=84) groups. Univariate analysis, random forest importance assessment, lasso regression combined with multivariate regression analysis were used for feature evaluation. Eight machine learning models were trained (70% data) and validated (30% data). A Stacking ensemble model was constructed, and SHapley Additive exPlanations (SHAP) was used for feature interpretation.
Results: The area under the receiver operating characteristic curve (AUROC) for predicting preterm birth in EOPE patients using Logistic Regression, Gaussian Naive Bayes, Extreme Gradient Boosting (XGBoost), Light Gradient Boosting Machine, Support Vector Machine (SVM), Gradient Boosting Decision Tree (GBDT), Multi-Layer Perceptron, and Elastic Net were 0.763, 0.712, 0.821, 0.832, 0.821, 0.842, 0.784, and 0.763, respectively. The Stacking model (XGBoost+GBDT+SVM) achieved superior performance (AUROC=0.865). Three independent risk factors were identified: fetal growth restriction (aOR=3.50, p = 0.047), serum cystatin C (aOR=11.27, p = 0.018), and C-reactive protein (aOR=1.37, p < 0.001). SHAP analysis revealed GBDT as the top contributor to Stacking predictions, with microalbunminuria (GBDT, XGBoost) and age (SVM) being the most influential features.
Conclusion: Machine learning models can serve as reliable assessment tools for predicting the risk of preterm birth in patients with EOPE. The ensemble prediction model demonstrates the best predictive performance, helping obstetricians identify high-risk patients and perform early intervention to improve perinatal outcomes.
Keywords: machine learning, preterm birth, early-onset preeclampsia, clinical prediction model
Introduction
Preeclampsia (PE) is a serious obstetric complication with an incidence of 2%-8%,1 and it represents one of the primary contributors to preterm birth (delivery before 37 weeks) and low birth weight infants (<2500g).2–4 as well as a major contributor to maternal and perinatal mortality. Despite extensive research, the underlying pathophysiological mechanisms of PE remain incompletely understood, and current effective treatment options remain limited primarily to pregnancy termination.5,6
This clinical challenge is further complicated by the recognition that PE manifests differently depending on gestational timing at onset. PE is divided into early-onset preeclampsia (EOPE) (occurring before 34 weeks of gestation) and late-onset preeclampsia (occurring at 34 weeks of gestation or later). The two subtypes show significant differences in clinical significance, long-term prognosis, treatment response, and pathological mechanisms.7,8 Patients with EOPE experience earlier onset during critical fetal organ development.9,10 Its pathophysiological hallmarks, including placental hypoperfusion, thyroid dysfunction, and systemic inflammation, create a unique risk environment that disproportionately contributes to global preterm birth rates and associated complications.11–13 While numerous risk factors for preterm birth in general PE populations have been identified, including maternal age, history of preterm birth, multiple pregnancies, and various maternal comorbidities,14–16 the distinct risk profile of EOPE remains understudied. Emerging evidence highlights the pivotal role of inflammatory mediators (CRP, fractalkine, MIP-1β) and angiogenic imbalances (sFlt-1/PlGF ratio) in PE pathogenesis. These biomarkers not only reflect systemic inflammation linked to placental dysfunction but also correlate with adverse outcomes like intrauterine growth restriction and preterm premature rupture of membranes.6,17–19
Previous studies have shown that early screening for preterm birth in pregnant women can reduce its incidence.12,20 Therefore, there is an urgent need for an accurate predictive model in clinical practice to assess the risk of preterm birth in EOPE. In recent years, machine learning algorithms have been widely applied in the medical field with good performance. Compared to logistic regression algorithms, the advantages of machine learning lie in its ability to handle high-dimensional data and its self-learning capabilities.21 Recent work by Kawakita et al employed machine learning, including XGBoost, to predict preterm PE using biomarkers available before 23 weeks. While demonstrating the utility of computational approaches, their model focused exclusively on early gestation and general PE, leaving unaddressed the individualized assessment and predictive models for the risk of preterm birth in women with EOPE.14 Therefore, through a retrospective study, we aim to explore the associated high-risk factors for preterm birth in PE, compare the predictive capabilities of eight machine learning algorithms for the risk of preterm birth in patients with EOPE, and attempt to construct a risk assessment tool with optimal performance to guide early intervention, aiming to improve pregnancy outcomes.
Materials and Methods
Study Subjects and Data Collection
We conducted a retrospective study on pregnant women who received prenatal care and were hospitalized for delivery at Fujian Maternity and Child Health Hospital from January 2012 to January 2023. All data were sourced from the electronic medical record system of Fujian Maternity and Child Health Hospital, totaling 4571 cases of PE patients. Inclusion criteria: (1) diagnosed with PE; (2) PE diagnosis gestational age ≥ 28 weeks and ≤ 34 weeks; (3) age ≥ 18 years. Exclusion criteria: (1) multiple pregnancies; (2) stillbirth or malformation; (3) incomplete clinical data. Based on the inclusion and exclusion criteria, a total of 442 cases of EOPE patients were included in the study. They were divided into two groups based on whether the gestational age at delivery was term-born birth group (≥ 37 weeks) or preterm birth group (< 37 weeks).
Based on current relevant research and clinical practice,2,6,14,15,17,18 we selected 62 potential predictive factors that may affect the risk of preterm birth in EOPE patients. All variables included: demographic and clinical characteristics (8 variables), such as age, height, pre-pregnancy BMI, gravidity, parity, gestational age at PE diagnosis, systolic blood pressure at diagnosis of PE, and diastolic blood pressure at diagnosis of PE. Past medical history and complications (17 variables): family history of hypertension, scarred uterus, pregnancy with assisted reproductive technology, history of abortion, history of preterm birth, history of cervical surgery, history of pelvic surgery, pre-pregnancy diabetes, thyroid disease, autoimmune diseases, genital tract malformations, aspirin use during pregnancy, fetal growth restriction (FGR), gestational diabetes mellitus (GDM), intrahepatic cholestasis of pregnancy (ICP), polyhydramnios, oligohydramnios. Relevant biochemical indicators tested (37 variables): hemoglobin (HB), alkaline phosphatase (ALP), total cholesterol (TC), triglycerides (TG), serum glucose (GLU), serum calcium (Ca), serum magnesium (Mg), creatine kinase (CK), creatine kinase isoenzyme (CK-MB), lactate dehydrogenase (LDH), creatinine (Cr), urea, uric acid (UA), carbon dioxide binding capacity (CO2CP), serum cystatin C (Cys-C), microalbunminuria (MAU), alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transferase (GGT), cholinesterase (CHE), C-reactive protein (CRP), total bile acids (TBA), total bilirubin (TBIL), direct bilirubin (DBIL), indirect bilirubin (IBIL), ferritin (FER), albumin (ALB), globulin (GLO), platelet (PLT), fibrin degradation products (FDP), thrombin time (TT), activated partial thromboplastin time (APTT), high-density lipoprotein (HDL), low-density lipoprotein (LDL), serum kalium (K), serum natrium (Na). All the above biochemical indicators were the most recent results before the diagnosis of PE.
We also analyzed 18 maternal and infant perinatal outcomes, including placental adhesion, placental abruption, spontaneous premature rupture of membranes, fetal distress, postpartum hemorrhage, cesarean section delivery, neonatal gestational age, neonatal weight, neonatal length, 1-minute Apgar score, placental weight, umbilical cord length, umbilical cord torsion, small for gestational age (SGA), Severe SGA, and low birth weight infants, asphyxia neonatorum and neonates admitted to NICU.
Data Preprocessing
None of the variables in this study exceeded the 30% missingness threshold, with the majority (85%) demonstrating missing rates below 5%. Missing values were handled using multiple imputation with chained equations. Continuous variables were standardized and categorical variables were encoded to maintain data integrity throughout the preprocessing pipeline.
Model Establishment and Validation
We first use univariate analysis, random forest importance assessment combined with lasso regression to select feature variables. All data in this study are randomly divided into a training set and a validation set in a 7:3 ratio. We optimize the model hyperparameters using 5-fold cross-validation combined with grid search. 8 machine learning algorithms are used to build models, including Logistic Regression (LR), Gaussian Naive Bayes (GNB), Extreme Gradient Boosting (XGBoost), Light Gradient Boosting Machine (LightGBM), Support Vector Machine (SVM), Gradient Boosting Decision Tree (GBDT), Multi-Layer Perceptron (MLP), and Elastic Net (EN). 7 metrics are used to evaluate the models (training set and validation set), including sensitivity, specificity, accuracy, precision, F1 score, area under the receiver operating characteristic curve (AUROC) and area under the precision-recall curve (AUPRC). To achieve better predictive performance, a stacking algorithm is used to construct an ensemble model. The SHapley Additive exPlanations (SHAP) method is used for interpretability analysis of the model, revealing the contribution of each feature variable to the model.
Statistical Analysis
We use SPSS 26.0 and Python 3.7 for data organization and analysis. Quantitative data are expressed as mean ± standard deviation (SD), and t-tests or non-parametric tests are used for analysis based on whether the data follow a normal distribution. Qualitative data are expressed as cases (%), and chi-square tests or Fisher’s exact probability method are used for analysis. A p value of < 0.05 is considered statistically significant.
Results
Baseline Characteristics
According to the inclusion and exclusion criteria, our study included a total of 442 patients with EOPE, of which 358 cases (81.00%) experienced preterm birth. Baseline data such as age, history of abortion, aspirin use during pregnancy, FGR, ALP, TC, TG, UA, Cys-C, MAU, ALT, AST, GGT, CRP, TBA, and TT were significantly higher in the preterm birth group compared to the term-born group (p < 0.05); while Ca and ALB were significantly lower in the preterm birth group than in the term-born group (p < 0.01) (Table 1).
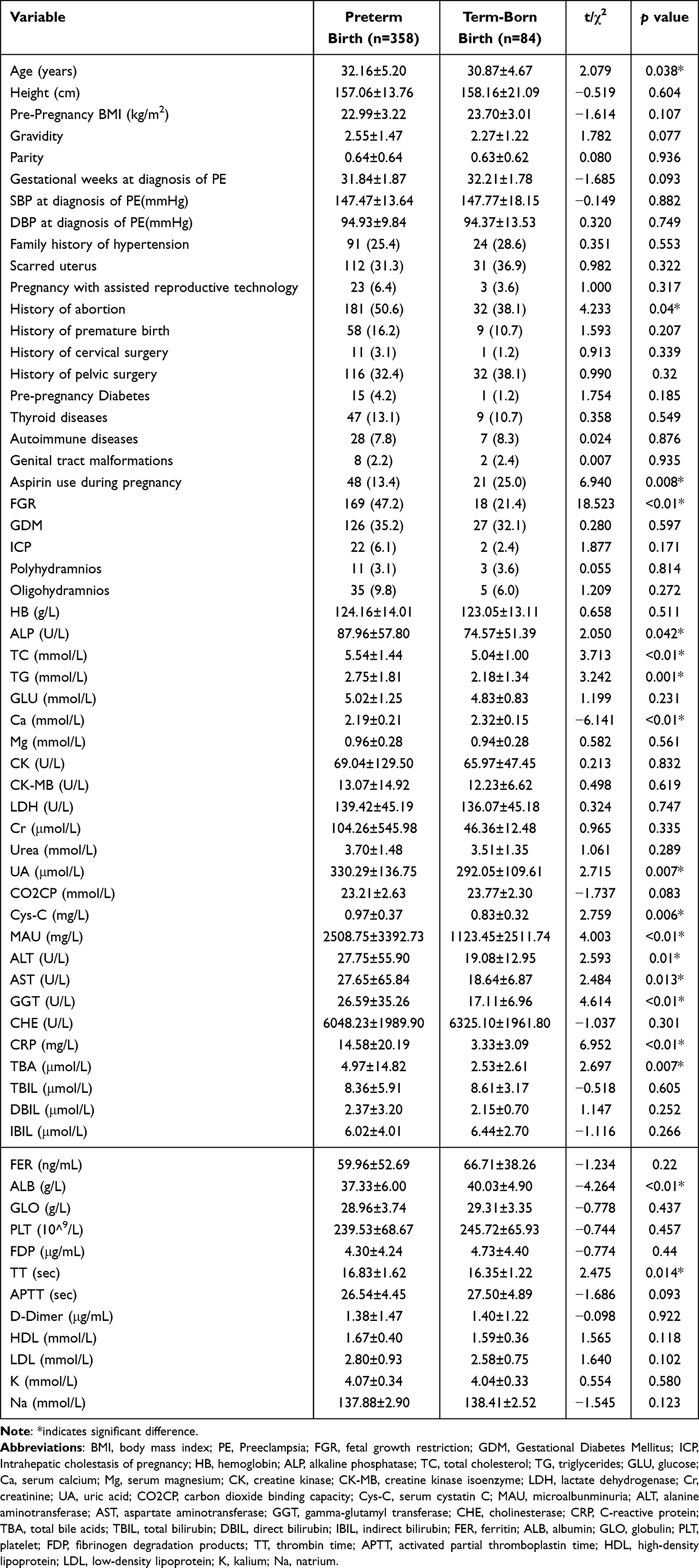 |
Table 1 Baseline Characteristics of 442 Patients in PE |
The incidence of perinatal outcomes such as placental abruption, fetal distress, cesarean section delivery, SGA, severe SGA, low birth weight infants, and neonates admitted to NICU was significantly higher in the preterm birth group compared to the term-born group (p < 0.01). Indicators such as neonatal gestational age, neonatal weight, neonatal length, 1-minute Apgar score, and placental weight were significantly lower in the preterm birth group than in the term-born group (p < 0.01) (Table 2).
 |
Table 2 Analysis of Perinatal Outcomes in 442 Patients of PE |
Variable Selection
Based on the 18 variables with p < 0.05 from the univariate analysis mentioned above, a random forest model was established, and feature importance ranking was conducted (Figure 1A). To streamline the number of variables, lasso regression was further applied to the 18 variables for selection (Figure 1B and C). The dashed line corresponds to lambda.min (the lambda at which the mean squared error is minimized), and based on this dashed line, the optimal number of variables was determined to be 9. Therefore, the subsequent model will include the top 9 variables ranked by random forest importance assessment, namely MAU, Cys-C, age, CRP, Ca, aspirin use during pregnancy, ALB, FGR and ALP. Multivariate logistic regression analysis of the nine variables identified three independent risk factors significantly associated with preterm birth in PE. FGR showed an adjusted odds ratio of 3.501 (95% CI 1.016–12.064, p = 0.047), Cys-C demonstrated an adjusted odds ratio of 11.265 (95% CI 1.509–84.106, p = 0.018), and CRP had an adjusted odds ratio of 1.374 (95% CI 1.151–1.641, p < 0.001). These associations were visually represented in the forest plot (Figure 1D).
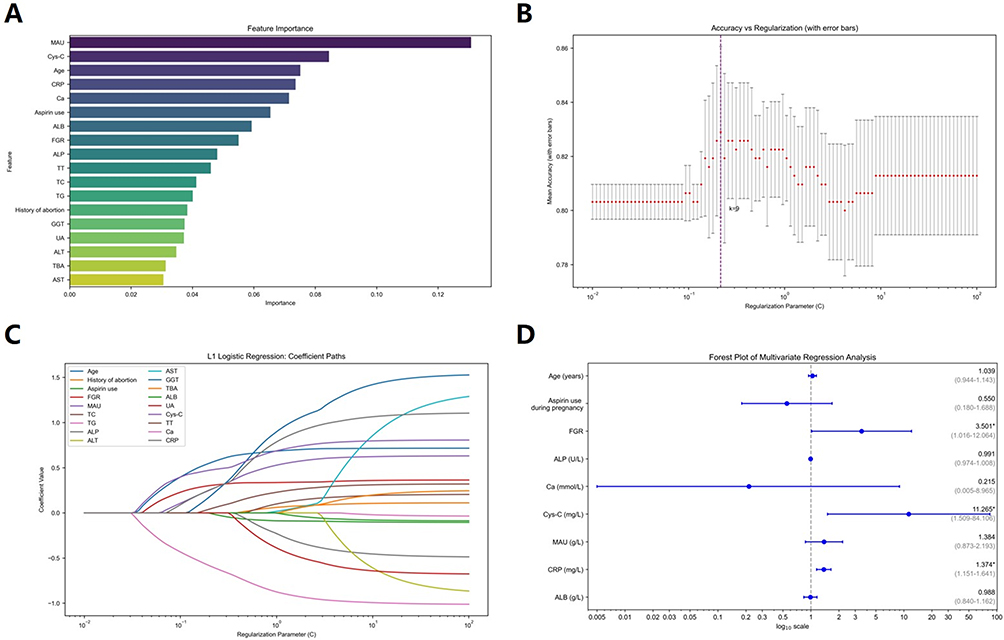 |
Figure 1 Variable selection for the prediction model. (A) Importance ranking of feature variables in the random forest model for preterm birth risk in patients with early-onset preeclampsia. (B) Variables selected by Lasso regression, with the dashed line representing the lambda that yields the minimum mean of the target parameters, under which the model achieved the best performance. (C) Variation characteristics of LASSO regression coefficients. (D) Forest plot displaying adjusted odds ratios with 95% confidence intervals for independent risk factors associated with preterm birth in preeclampsia patients. *P<0.05. Abbreviations: MAU, microalbunminuria; Cys-C, serum cystatin C; CRP, C-reactive protein; Ca, serum calcium; ALB, albumin; FGR, fetal growth restriction; ALP, alkaline phosphatase; TT, thrombin time; TC, total cholesterol; TG, triglycerides; GGT, gamma-glutamyl transferase; UA, uric acid; ALT, alanine aminotransferase; TBA, total bile acids; AST, aspartate aminotransferase. |
Training Set and Validation Set Data
A total of 442 patients were randomly divided into a training set (n=310) and a validation set (n=132) in a 7:3 ratio. The training set was used for model construction, while the validation set was used to evaluate the performance of the trained model. There were no significant statistical differences in the included variables and perinatal outcomes between the two groups (Tables 3 and 4).
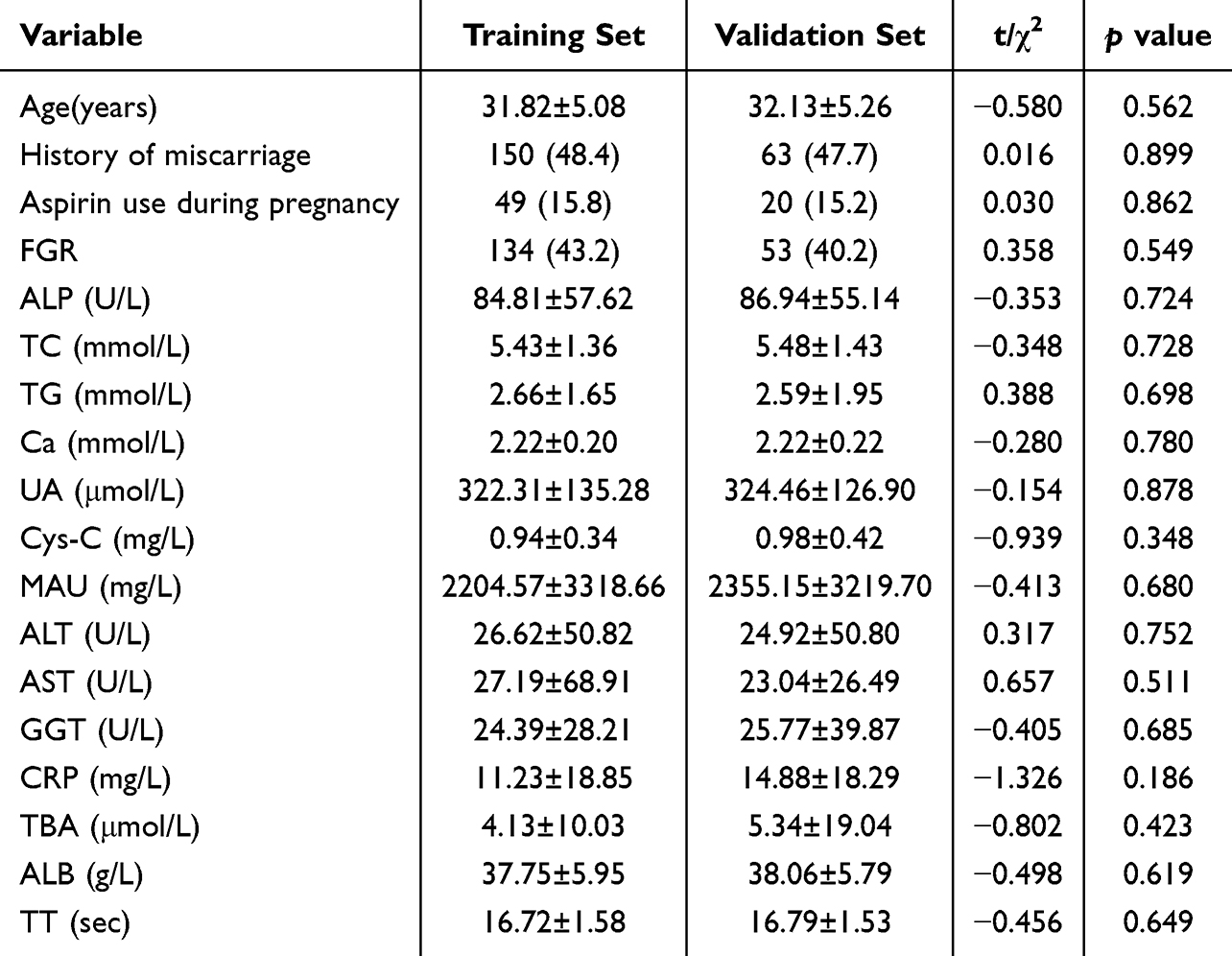 |
Table 3 Comparison of Each Variable Included in the Training and Validation Sets |
 |
Table 4 Comparison of Perinatal Outcomes in the Training and Validation Sets |
Prediction Model Construction and Evaluation
In the training set, the AUROC for predicting preterm birth in EOPE patients based on LR, GNB, XGBoost, LightGBM, SVM, GBDT, MLP, and EN were 0.842, 0.754, 0.854, 0.987, 0.887, 0.984, 0.865, and 0.843, respectively; the AUPRC were 0.954, 0.913, 0.937, 0.997, 0.964, 0.996, 0.961, and 0.954, respectively (Figure 2A and C).
 |
Figure 2 Performance comparison of different machine learning models. (A) ROC curves of 9 models on the training set. (B) ROC curves of 9 models on the validation set. (C) PRC curves of 9 models on the training set. (D) PRC curves of 9 models on the validation set. (E) Heatmap of evaluation metrics for 9 models on the training set. (F) Heatmap of evaluation metrics for 9 models on the validation set. Abbreviations: ROC, receiver operating characteristic curve; PRC, precision-recall curve; LR, logistic regression; GNB, Gaussian Naive Bayes; XGBoost, extreme gradient boosting; LightGBM, light gradient boosting machine; SVM, support vector machine; GBDT, gradient boosting decision tree; MLP, multi-layer perceptron; EN, elastic net. |
In the validation set, the AUROC for predicting preterm birth in EOPE patients based on LR, GNB, XGBoost, LightGBM, SVM, GBDT, MLP, and EN were 0.763, 0.712, 0.821, 0.832, 0.821, 0.842, 0.784, and 0.763, respectively; the AUPRC were 0.932, 0.913, 0.959, 0.963, 0.951, 0.964, 0.937, and 0.932, respectively (Figure 2B and D).
Among all single algorithm models, LightGBM in the training set had the best sensitivity (0.952), specificity (0.967), accuracy (0.955), precision (0.992), and F1 score (0.971) (Table 5); MLP in the validation set had the best sensitivity (0.881), specificity (0.652), accuracy (0.841), precision (0.923), and F1 score (0.901) (Table 5, Figure 2E and F).
 |
Table 5 Performance Comparison of Different Machine Learning Models |
Model Fusion
After stacking model fusion, a total of 247 different model combinations were output. The combinations were ranked based on the size of the AUROC on the validation set, listing the top 5 combinations. Among them, the joint prediction of “XGBoost” + “GBDT” + “SVM” achieved the maximum AUROC of 0.865 (Table 6 and Figure 2).
 |
Table 6 Comparison of the Performance of the Different Combinations of Stacking Ensemble Models |
SHAP Value of Different Models
The SHAP plot of the best Stacking model shows the contribution of three individual models (GBDT, SVM, XGBoost) to the final prediction results of Stacking. The results indicate that among the three models, GBDT contributes the most to the prediction results of the Stacking model (Figure 3A). To examine the clinical relevance of different variables in different models, we output the SHAP plots of the three individual models (GBDT, SVM, XGBoost) that make up the best Stacking model, analyzing the contribution of the nine feature variables included in the model to each model. The results show that in the GBDT model, MAU contributes the most to the prediction results of the model (Figure 3B); in the SVM model, age contributes the most to the prediction results of the model (Figure 3C); in the XGBoost model, MAU contributes the most to the prediction results of the model (Figure 3D).
 |
Figure 3 SHAP value of different models on the selected feature set. (A) SHAP value of the best Stacking model. (B) SHAP value of GBDT on selected feature set. (C) SHAP value of SVM on selected feature set. (D) SHAP value of XGBoost on selected feature set. Abbreviations: SHAP, shapley additive explanation; GBDT, gradient boosting decision tree; SVM, support vector machine; XGBoost, extreme gradient boosting; FGR, fetal growth restriction; MAU, microalbunminuria; Ca, serum calcium; Cys-C, serum cystatin C; ALB, albumin; CRP, C-reactive protein; ALP, alkaline phosphatase. |
Discussion
EOPE presents with high risks of adverse outcomes, especially preterm birth, necessitating close monitoring and early intervention.22,23 This study systematically evaluated the predictive performance of multiple machine learning models for preterm birth risk in EOPE. The ensemble model combining XGBoost, GBDT and SVM demonstrated superior predictive accuracy (AUROC=0.865) compared to individual algorithms. Moreover, we identified nine clinically significant predictors, among which FGR, serum Cys-C, and CRP emerged as independent risk factors. These findings provided both methodological and clinical advancements in EOPE management.
With the development of advanced algorithms like artificial intelligence and data mining, machine learning applications in preterm birth clinical diagnosis, prognosis assessment, and precision treatment have gained research focus.24–26 Sun et al used various machine learning models to predict preterm birth, finding the RF model performed best (AUROC=0.885, accuracy=0.816), aiding clinicians in early intervention.1 As most predictive models lack external validation, Liu et al employed the NVSS database with four models (Logistic, Adaptive lasso, Bootstrap forest, Boosting trees), all showing high accuracy (AUROC>0.7). Their nomogram using nine risk factors also achieved AUROC=0.704, demonstrating good generalizability.27 Kawakita et al predicted preterm birth risk in PE patients before 37 weeks using data before 23 weeks, with XGBoost performing best (AUROC=0.749).14 The optimal models in the aforementioned studies are inconsistent with this study, likely due to differences in the population scope and ethnic variations.
In this study, multiple machine learning models were established, with the GBDT model outperforming the other seven models in predicting the risk of preterm birth in EOPE, achieving an AUROC of 0.842. A Stacking algorithm was used to construct an ensemble model, showing that the combined prediction performance of “XGBoost” + “GBDT” + “SVM” was superior to that of individual models, with an AUROC reaching 0.865. Furthermore, our study elucidates key risk factors for preterm birth in EOPE through comprehensive analysis. Nine clinically significant variables were incorporated into the predictive model, which collectively captured the syndromic nature of EOPE progression from placental origin to systemic complications.28 Notably, placental insufficiency markers (FGR), renal dysfunction indicators (Cys-C), and systemic inflammation (CRP) were three independent risk factors.
FGR emerged as the strongest anatomical predictor (aOR=3.501). This reflects the hallmark placental insufficiency of EOPE, where defective spiral artery remodeling reduces uteroplacental perfusion compared to normal pregnancies. The resulting hypoxia triggers compensatory mechanisms that accelerate placental aging and prostaglandin release, predisposing to preterm labor.29,30 Cys-C demonstrated the most pronounced biochemical association (aOR=11.265). As a sensitive glomerular filtration marker, elevated levels indicate renal endothelial damage—a key feature of EOPE’s systemic vasculopathy.31,32 CRP showed a dose-dependent relationship (aOR=1.374 per mg/L). This acute-phase reactant quantifies the systemic inflammation that characterizes severe EOPE. CRP’s dual role in both disrupting trophoblast function and stimulating myometrial contractility explains its predictive persistence.33–35 Beyond these primary predictors, other model variables like MAU (reflecting glomerular endothelial injury), advanced maternal age (associated with vascular senescence), hypocalcemia (linked to vascular smooth muscle dysfunction), and low albumin (indicating capillary leakage) further delineate EOPE’s multisystem pathophysiology. Aspirin use, though protective in some contexts, may signal high-risk pregnancies requiring intensified monitoring, while elevated ALP likely reflects placental ischemia or hepatic involvement. Together, these biomarkers provide a holistic representation of EOPE’s heterogeneous mechanisms contributing to preterm birth.6,15,18,28,32
The model’s clinical utility in this study lies in transforming standard biomarkers into preterm birth risk predictions without requiring additional tests. By incorporating routinely measured EOPE parameters, it enables risk stratification during clinical evaluation. This approach facilitates identification of patients who may benefit from tailored interventions based on their specific risk profiles. The ensemble method demonstrates enhanced predictive capability compared to individual models. Further validation across diverse clinical environments and potential integration with electronic health records warrant investigation to assess practical implementation.
Despite providing important findings, this study has some limitations. First, the data were sourced from a single hospital, and the sample size was relatively small, which may affect the external generalizability of the results. Although we made every effort to incorporate the clinical relevant variables with a lower rate of missing data, we acknowledge that some potentially important predictors may not have been captured in our dataset. Additionally, although we used multiple imputation to handle missing data, potential biases cannot be completely ruled out. Future research should consider expanding the sample size and conducting multi-center validation to enhance the credibility and applicability of the findings. Furthermore, the lack of long-term follow-up prevents us from assessing the long-term status of mothers and newborns. Therefore, subsequent research should focus on establishing a more comprehensive risk assessment model to further optimize the prediction and intervention strategies for preterm birth risk in EOPE patients.
Conclusion
In summary, this study systematically analyzed the clinical characteristics of EOPE patients and their relationship with preterm birth risk, identifying key biomarkers and independent risk factors, and establishing effective predictive models. These findings provide important references for clinical decision-making, with the hope of reducing preterm birth risk and improving maternal and infant outcomes in future clinical practice. Further research should focus on external validation and optimization of this model for broader application.
Data Sharing Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding authors.
Ethics Approval and Consent to Participate
The studies involving humans were approved by Ethics Committee of Fujian Maternity and Child Health Hospital (2025KY012). The data analysis procedures followed the guidelines in the Declaration of Helsinki. Patient consent was waived by the Ethics Committee as this study involved anonymized retrospective data analysis, ensuring no breach of confidentiality. The medical records used in this study were obtained from previous clinical diagnosis and treatment, and will not cause physical and mental pain to patients, affect the safety and health of patients, increase the economic burden of patients and their families, and exemption from informed consent will not adversely affect the rights and health of patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Fujian Provincial Health Technology Project (2024ZD01005), Joint Funds for the innovation of science and Technology, Fujian province (2020Y9134), Joint Funds for the innovation of science and Technology, Fujian province (2020Y9401), National Key Clinical Specialty Construction Program of China (Obstetric), Fujian Provincial Natural Science Foundation of China (2024Y0035), Startup Fund for scientific research, Fujian Medical University (2024QH2047).
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Docheva N, Arenas G, Nieman KM, Lopes-Perdigao J, Yeo K-TJ, Rana S. Angiogenic biomarkers for risk stratification in women with preeclampsia. Clin Chem. 2022;68(6):771–781. doi:10.1093/clinchem/hvab281
2. Alvestad S, Husebye ESN, Christensen J, et al. Folic acid and risk of preterm birth, preeclampsia, and fetal growth restriction among women with epilepsy: a prospective cohort study. Neurology. 2022;99(6):e605–e615. doi:10.1212/WNL.0000000000200669
3. Li X, Zhang W, Lin J, et al. Preterm birth, low birthweight, and small for gestational age among women with preeclampsia: does maternal age matter? Pregnancy Hypertens. 2018;13:260–266. doi:10.1016/j.preghy.2018.07.004
4. An H, Jin M, Li Z, et al. Impact of gestational hypertension and pre-eclampsia on preterm birth in China: a large prospective cohort study. BMJ Open. 2022;12(9):e058068. doi:10.1136/bmjopen-2021-058068
5. Jung E, Romero R, Yeo L, et al. The etiology of preeclampsia. Am J Obstet Gynecol. 2022;226(2S):S844–S866. doi:10.1016/j.ajog.2021.11.1356
6. MacDonald TM, Walker SP, Hannan NJ, Tong S, Kaitu’u-Lino TJ. Clinical tools and biomarkers to predict preeclampsia. EBio Medicine. 2022;75:103780. doi:10.1016/j.ebiom.2021.103780
7. Jia Y, Lu W, Xie H, et al. Upregulation of siglec-6 induces mitochondrial dysfunction by promoting GPR20 expression in early-onset preeclampsia. J Transl Med. 2024;22(1):674. doi:10.1186/s12967-024-05505-z
8. Liu Y, Du L, Gu S, et al. Identification of the role of DAB2 and CXCL8 in uterine spiral artery remodeling in early-onset preeclampsia. Cell Mol Life Sci. 2024;81(1):180. doi:10.1007/s00018-024-05212-4
9. Huang Z, Sun L, Gao Y, et al. Exploration of the molecular characteristics and potential clinical significance of shared immune-related genes between preterm preeclampsia and term preeclampsia. BMC Pregnancy Childbirth. 2024;24(1):543. doi:10.1186/s12884-024-06526-8
10. Villalain C, Herraiz I, Dominguez-Del Olmo P, Angulo P, Ayala JL, Galindo A. Prediction of delivery within 7 days after diagnosis of early onset preeclampsia using machine-learning models. Front Cardiovasc Med. 2022;9:910701. doi:10.3389/fcvm.2022.910701
11. Farias-Jofre M, Romero R, Galaz J, et al. Blockade of IL-6R prevents preterm birth and adverse neonatal outcomes. EBioMedicine. 2023;98:104865. doi:10.1016/j.ebiom.2023.104865
12. Creswell L, Rolnik DL, Lindow SW, O’Gorman N. Preterm birth: screening and prediction. Int J Womens Health. 2023;15:1981–1997. doi:10.2147/IJWH.S436624
13. de Paula Eduardo JAF, de Rezende MG, Menezes PR, Del-Ben CM. Preterm birth as a risk factor for postpartum depression: a systematic review and meta-analysis. J Affect Disord. 2019;259:392–403. doi:10.1016/j.jad.2019.08.069
14. Kawakita T, Martins JG, Diab YH, Nehme L, Saade G. Derivation and validation of prediction of preterm preeclampsia using machine learning algorithms. Am J Perinatol. 2024. doi:10.1055/a-2495-3600
15. Nilsson EE, Winchester P, Proctor C, Beck D, Skinner MK. Epigenetic biomarker for preeclampsia-associated preterm birth and potential preventative medicine. Environ Epigenet. 2024;10(1):dvae022. doi:10.1093/eep/dvae022
16. Huang C, Long X, van der Ven M, Kaptein M, Oei SG, van den Heuvel E. Predicting preterm birth using electronic medical records from multiple prenatal visits. BMC Pregnancy Childbirth. 2024;24(1):843. doi:10.1186/s12884-024-07049-y
17. Wang Y, Li B, Zhao Y. Inflammation in preeclampsia: genetic biomarkers, mechanisms, and therapeutic strategies. Front Immunol. 2022;13:883404. doi:10.3389/fimmu.2022.883404
18. Feng W, Luo Y. Preeclampsia and its prediction: traditional versus contemporary predictive methods. J Matern Fetal Neonatal Med. 2024;37(1):2388171. doi:10.1080/14767058.2024.2388171
19. Pala S, Atilgan R, Ilhan N. High amniotic fluid fractalkine and MIP-1beta levels are associated with intrauterine growth restriction: a prospective cohort study. Turk J Med Sci. 2024;54(1):280–290. doi:10.55730/1300-0144.5789
20. Hezelgrave NL, Suff N, Seed P, et al. Comparing cervical cerclage, pessary and vaginal progesterone for prevention of preterm birth in women with a short cervix (SuPPoRT): a multicentre randomised controlled trial. PLoS Med. 2024;21(7):e1004427. doi:10.1371/journal.pmed.1004427
21. Ngiam KY, Khor IW. Big data and machine learning algorithms for health-care delivery. Lancet Oncol. 2019;20(5):e262–e273. doi:10.1016/S1470-2045(19)30149-4
22. Rahman L, Anwar R, Mose JC. Maternal and neonatal outcome among women with early-onset preeclampsia and late-onset preeclampsia. Hypertens Pregnancy. 2024;43(1):2405991. doi:10.1080/10641955.2024.2405991
23. Serra B, Mendoza M, Scazzocchio E, et al. A new model for screening for early-onset preeclampsia. Am J Obstet Gynecol. 2020;222(6):608e1–608e18. doi:10.1016/j.ajog.2020.01.020
24. Sun Q, Zou X, Yan Y, et al. Machine learning-based prediction model of preterm birth using electronic health record. J Healthc Eng. 2022;2022:9635526. doi:10.1155/2022/9635526
25. Sharifi-Heris Z, Laitala J, Airola A, Rahmani AM, Bender M. Machine learning approach for preterm birth prediction using health records: systematic review. JMIR Med Inform. 2022;10(4):e33875. doi:10.2196/33875
26. Zhang Y, Lu S, Wu Y, Hu W, Yuan Z. The prediction of preterm birth using time-series technology-based machine learning: retrospective cohort study. JMIR Med Inform. 2022;10(6):e33835. doi:10.2196/33835
27. Liu Y, Liu J, Shen H. Machine learning model-based preterm birth prediction and clinical nomogram: a big retrospective cohort study. Int J Gynaecol Obstet. 2025;169(1):332–340. doi:10.1002/ijgo.16036
28. Erez O, Romero R, Jung E, et al. Preeclampsia and eclampsia: the conceptual evolution of a syndrome. Am J Obstet Gynecol. 2022;226(2S):S786–S803. doi:10.1016/j.ajog.2021.12.001
29. Colson A, Sonveaux P, Debieve F, Sferruzzi-Perri AN. Adaptations of the human placenta to hypoxia: opportunities for interventions in fetal growth restriction. Hum Reprod Update. 2021;27(3):531–569. doi:10.1093/humupd/dmaa053
30. Check J, Shuster C, Hofheimer J, et al. Preeclampsia, fetal growth restriction, and 24-month neurodevelopment in very preterm infants. JAMA Network Open. 2024;7(7):e2420382. doi:10.1001/jamanetworkopen.2024.20382
31. Alshannag F, Zaki RMM, Hemida E, ElBakry MMM, Noureldeen AFH. Endostatin and cystatin C as potential biomarkers for early prediction of preeclampsia. ACS Omega. 2023;8(45):42776–42786. doi:10.1021/acsomega.3c05586
32. Goodbred AJ, Langan RC. Chronic kidney disease: prevention, diagnosis, and treatment. Am Fam Physician. 2023;108(6):554–561.
33. Guan X, Fu Y, Liu Y, et al. The role of inflammatory biomarkers in the development and progression of pre-eclampsia: a systematic review and meta-analysis. Front Immunol. 2023;14:1156039. doi:10.3389/fimmu.2023.1156039
34. Puttaiah A, Kirthan JPA, Sadanandan DM, Somannavar MS. Inflammatory markers and their association with preeclampsia among pregnant women: a systematic review and meta-analysis. Clin Biochem. 2024;129:110778. doi:10.1016/j.clinbiochem.2024.110778
35. Gigase FAJ, Boekhorst M, Suleri A, et al. Maternal immune activation during pregnancy and obstetric outcomes: a population-based cohort study. BJOG. 2025. doi:10.1111/1471-0528.18191
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Machine Learning-Based Mortality Risk Prediction Model in Patients with Sepsis
Zhang Y, Li C, Ji Y, Wei B, Guo S, Mei X, Wang J
Journal of Inflammation Research 2025, 18:6427-6437
Published Date: 19 May 2025
Comparison of Interpretable Machine Learning Models Using Systemic Inflammation Index to Predict Preterm Birth in Gestational Diabetes Mellitus
Pang Q, Peng L, Wu J, Wang Y, Zhang R, Liu Z, Jiang L
International Journal of Women's Health 2026, 18:541610
Published Date: 10 February 2026
Construction and Validation of Active Case-Finding Tool in Community Participants with Chronic Obstructive Pulmonary Disease Using an Interpretable Machine Learning Approach
Tian H, Wu F, Sun C, Deng Z, Zhou Y, Ran P
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:589883
Published Date: 16 June 2026