Back to Journals » Advances in Medical Education and Practice » Volume 14
A Comparative Study of Traditional Technique Guide versus Virtual Reality in Orthopedic Trauma Training
Authors Lamb A, McKinney B, Frousiakis P, Diaz G ![]() , Sweet S
, Sweet S
Received 12 November 2022
Accepted for publication 20 August 2023
Published 4 September 2023 Volume 2023:14 Pages 947—955
DOI https://doi.org/10.2147/AMEP.S395087
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Ashley Lamb,1 Brandon McKinney,1 Petros Frousiakis,1 Graal Diaz,2 Stephan Sweet1
1Orthopedic Surgery, Community Memorial Hospital, Ventura, CA, USA; 2Research Department-Graduate Medical Education, Community Memorial Healthcare System, Ventura, CA, USA
Correspondence: Graal Diaz, Research Department-Graduate Medical Education, Community Memorial Hospital, 147 N. Brent Street, Ventura, CA, 93003, USA, Email [email protected]
Background: Medical and surgical education is an expansive field fraught with many challenges. Technology such as virtual reality could be a new venue that can offer a solution to improve surgical training.
Objective: The objective of this prospective, blinded study was to evaluate virtual reality as a training model for orthopedic surgery and surgical training at large.
Methods: Fourth-year medical students with novice skills volunteered to participate in this observer-blinded 1:1 randomized controlled trial. They had no prior experience in tibia intramedullary nail (IMN) surgery. They were randomized into traditional technique guide education and virtual reality. The participants were timed on their mock surgery, and a blinded observer was utilized to subjectively grade their performance throughout the procedure using the Global Assessment 5-point Rating Scale and Procedure-Specific Checklist.
Results: Thirty-eight participants were recruited and randomized into virtual reality (19) and traditional (19) groups. There were trends in all categories favoring the virtual reality group. The VR group had improved time to completion (9.6 minutes vs 12.2 minutes, P = 0.034) and reduced need for corrections within the mock procedure (2.2 vs 2.5; P = 0.05).
Conclusion: Virtual reality training was more effective than traditional training in learning and completing the steps of the tibia IMN surgery for novice medical students. Virtual reality training may be a useful method to augment orthopedic education and surgical training.
Keywords: surgical training, virtual reality, traditional surgical training, operating room, mock procedures, comparative study
Introduction
Surgical training for orthopedic residents can be hampered by limited training opportunities outside of the operating room. Passive learning tools such as standard guide techniques are often used as training modalities. However, technological advances are changing the face of medicine, and surgical training is at the forefront of innovation. These advances are designed to improve patient care and care delivery including advancing types and availability of surgical techniques. In today’s world, these advances transcend bedside to medical education. Innovations are designed to improve knowledge delivery in an expansive field and combat the challenges specific to surgery and medical education. In some cases, technology is borrowed from other arenas of daily living and re-purposed. This includes virtual reality (VR), first developed in the mid-1980s by Jaron Lanier.1 He initially worked to develop a multi-sensory stimulation tool to target the entertainment field. This technology was also being investigated in the science realm within NASA.1,2
Literature Review
Virtual reality can create a microenvironment that allows for training experiences aimed at increasing perceptual fidelity. It can also improve users’ performance by lowering the cognitive load in completing a task through the development of muscle memory.1 A recent meta-analysis of 45 VR studies showed that VR is a feasible and effective adjunct to traditional surgical training.2 This can have significant advances for the surgical specialties in medicine.
As surgical complexity increases, surgeons learning new techniques need more exposure and practice. The number of cases to reach proficiency varies. For orthopedic surgeries, the number of cases can range from 20 to 30 for simple hip fractures,3 to 170 cases for knee arthroscopy.4 A recent review published a few years ago in the Journal of Surgery evaluating the readiness of general surgery residents for independent practice after completing a 5-year training program found that residents need to be more universally ready to independently perform core procedures on graduation. They estimated that this could reach up to one-third of graduates needing supervision.5 In a randomized, double-blinded trial evaluating virtual reality training for gallbladder removal, general surgery residents with VR training were 29% faster. Additionally, residents without VR training were five times more likely to injure the gallbladder or burn non-targeted tissue.5 As a new training modality, VR could offer the solution to improving collaboration, surgical training, and proficiency.6 There is ongoing research in this field, and a recent small, randomized control trial of 20 participants reviewed the use of VR to teach the surgical technique for tibial shaft fractures. This research found that VR training allowed for 20% faster completion.6,7
When discussing virtual reality, many different types of platforms can be used. Monitors with interactive surgical instruments versus immersive virtual reality present a completely different experience. While there are a few studies on monitored virtual reality, completely immersive virtual reality surgical training, which incorporates audio, visual, and proprioceptive tactile feedback, needs to be better studied throughout the literature. While sizable data exist for training with simulators for arthroscopy and general surgery procedures, there are limited virtual reality training modalities specifically studying orthopedic trauma training.
Tibia intramedullary nailing (IMN) is a standard trauma procedure for tibia shaft fractures, which was commonly taught using passive tools such as standard guides. Tibia IMN is a core competency orthopedic residents need to demonstrate proficiency for graduation to independent practice as outlined by ACGME. It incorporates the basic skills and principles utilized in many other orthopedic procedures. The fundamental principles are essential, but individual cases can be complex based on fracture and injury patterns. Failure of proper positioning can lead to fracture reduction outside of acceptable alignment tolerances, injury to the articular cartilage, or cortical perforation.8
Methods
A completely immersive audio, visual, tactile, proprioceptive feedback virtual reality platform was developed by Osso VR Inc. Within this technology, trainees place goggles on their faces that block out reality and the user’s view is a virtual operating room (Figure 1). Two sensors allow the trainee to operate within a safe boundary that has been pre-dictated and free of obstacles. Both hands are given controllers with movements tracked by the sensors allowing the trainee to use accurate movements to simulate the surgery, hammering while using the mallet, for example. This allows the trainee to feel immersed entirely within the virtual operating room and get the most out of the training experience. The module developed allows the trainee to simulate a tibia IMN surgery learning the basic steps, instrumentation, and proper technique. Visual clues throughout the module give instructions on the step-by-step order of the surgery (Figure 2). This allows both a visual and kinesthetic learning platform to digest the information.
 |
Figure 1 Virtual reality operating room as visualized by the participant. |
 |
Figure 2 VR participant is instructed on each step of the procedure. |
The traditional technique guide cohort was provided with the standard industry surgical technique guide to learn the steps of the tibia intramedullary nailing. Participants were allowed to study the standard industry surgical technique guide for as long as needed. The second cohort was provided with the virtual reality platform. This platform utilized a virtual module to learn the steps of the tibia intramedullary nailing procedure. Participants in the virtual reality group were allowed to use the module and run through the mock surgery as often as needed. Immediately after completing the technique guide study or the virtual reality module, participants were tested objectively on their comprehension of the procedure. Model tibia bones were used for the simulation of the intramedullary nail insertion. The instruments provided on a simulated OR table were identical to the layout demonstrated in the virtual reality module (Figures 3–5).
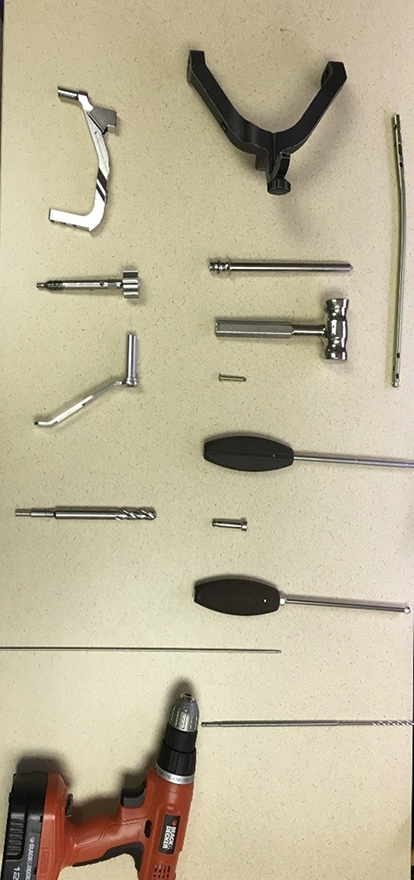 |
Figure 3 Standardized operating room back table for tibia IMN, mirroring virtual reality back table. |
 |
Figure 4 Participant completing virtual reality module. |
 |
Figure 5 Participant completing mock surgical procedure. |
Evaluation of Skills
The participants were timed on their mock surgery. A blinded observer (surgeon evaluator) subjectively graded their performance throughout the procedure, evaluating proficiency, timing, and the number of errors. This was standardized for both cohorts using an adapted Global Assessment 5-point Rating Scale.6 Using the Global Assessment 5-point scale, participants were awarded between 1 and 5 points for each category. One represented poor performance, and five had high scores (Table 1 and Table 2). Participants were also evaluated using the Procedure-Specific Checklist: 1-point for every step performed correctly and 0-points if the step was performed incorrectly or not. A pre-survey was provided prior to and a post-survey was provided after the mock surgery that evaluated the participants’ experience, including satisfaction, confidence, applicability, and overall interest. Survey questions were adapted from Blumstein et al validated questionnaire on current motivation8 (Appendix 1). Surgeon evaluators were provided with this chart before the procedure and instructed to rate the performance during the mock operation of tibia IMN. The monotonic relationship of each variable was analyzed by comparing the two cohorts using two non-parametric methods: Kendall’s Tau-b and Spearman’s Rho. These methods are similar and lead to the same inferences. All participants completed a written consent, which included permission to take photographs (Figures 4 and 5) to be used for publication. The Internal Review Board (IRB) at Community Memorial Healthcare System in Ventura, California, approved this study. This was an unfunded study.
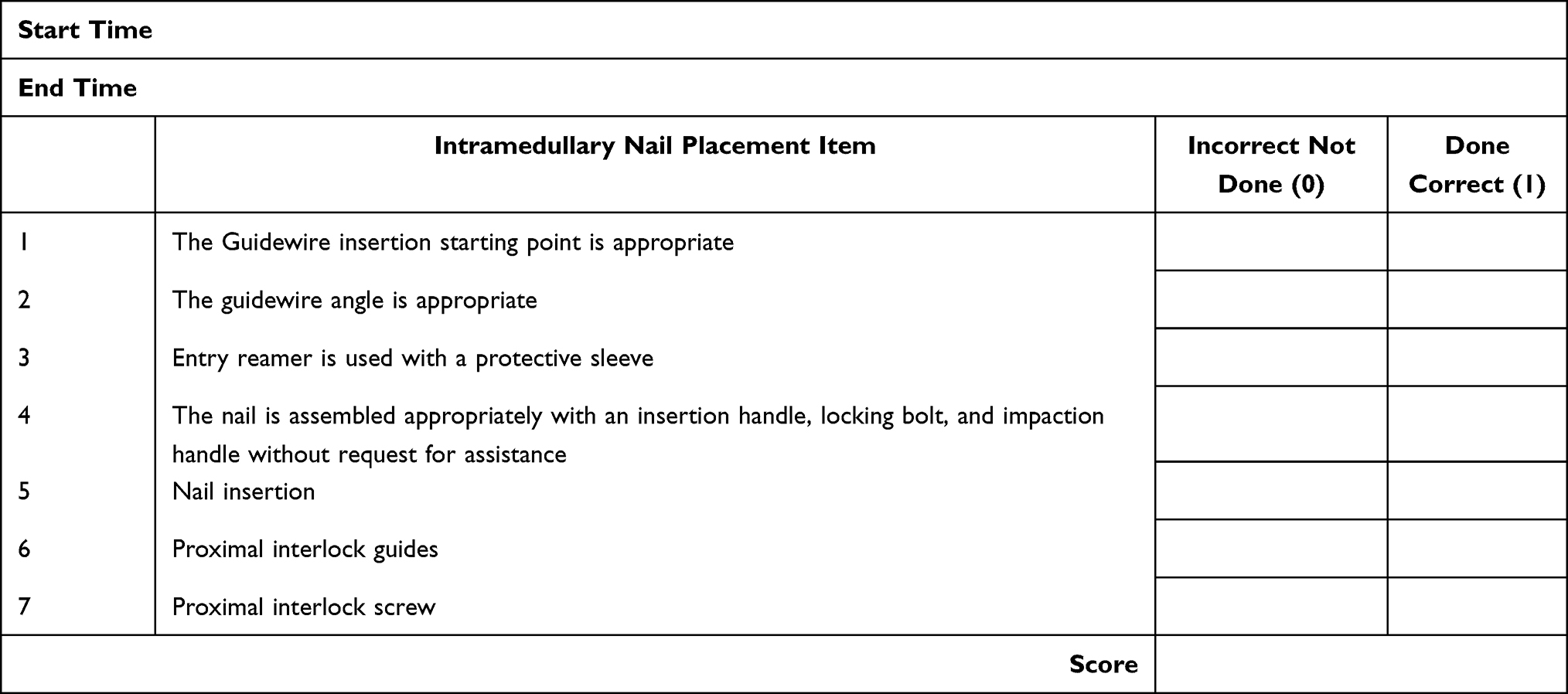 |
Table 1 Global Assessment 5-Point Rating Scale |
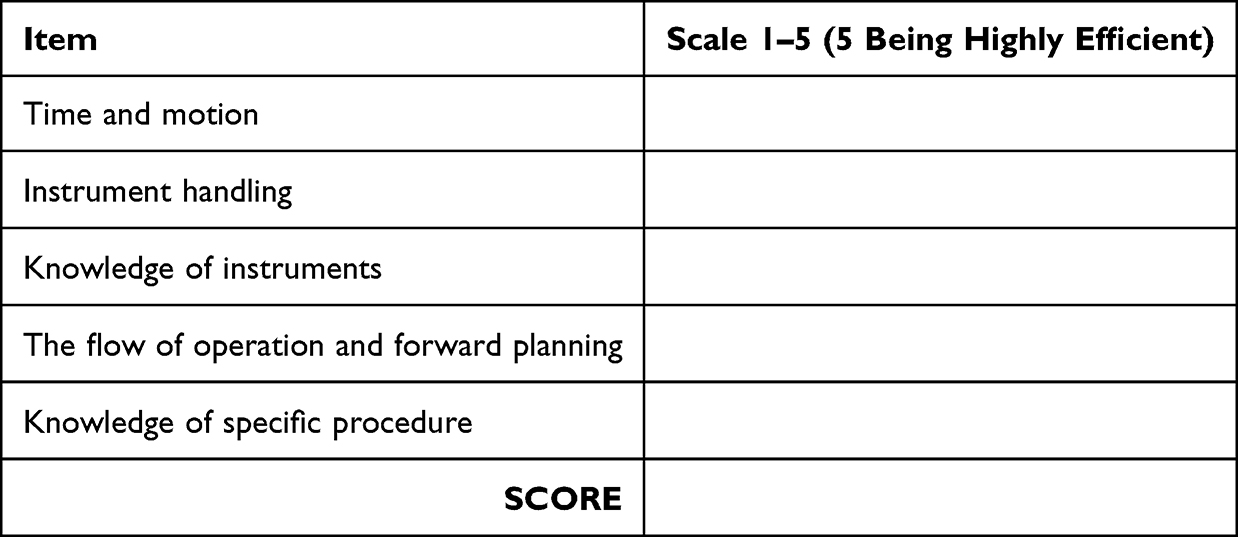 |
Table 2 Procedure-Specific Checklist Description |
Results
Thirty-eight participants were recruited and randomized into VR (19) and traditional technique guides (19). All 38 participants completed the learning phase and mock surgery. There were trends in most categories favoring the virtual reality group. However, no statistically significant difference in any of the objective evaluation metrics (Table 3, procedure specific overall % correct, 73% vs 68% and Table 4, overall objective performance, 2.81 vs 2.68) or subjective evaluation metrics (Table 5, the mean difference in all questions was 0.21) was noted. Spearman’s rho and Kendall’s tau analyses demonstrated a statistically significant (p < 0.05) difference in favor of the virtual reality group in regard to time to completion and number of redirections within the mock procedure (Table 6 and Table 7). Evaluation of training times (NS), procedure times (P-value= 0.02), and the number of redirects (P-value= 0.05) showed that virtual reality participants performed at a higher level compared with the technique guide-training group (Table 8).
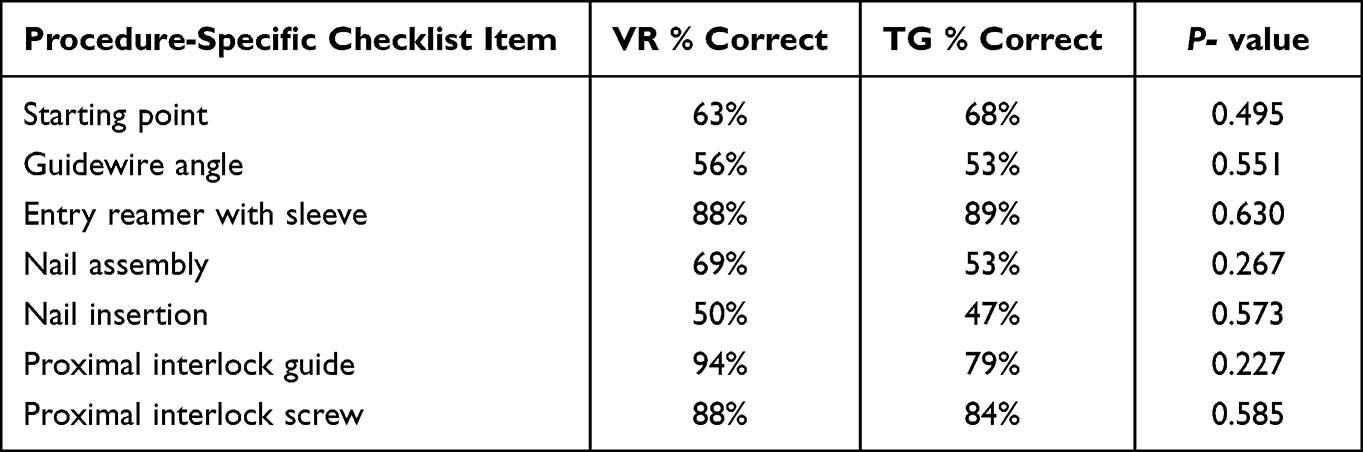 |
Table 3 Procedure-Specific Checklist Performance by Group |
 |
Table 4 Objective Evaluation Performance by Group |
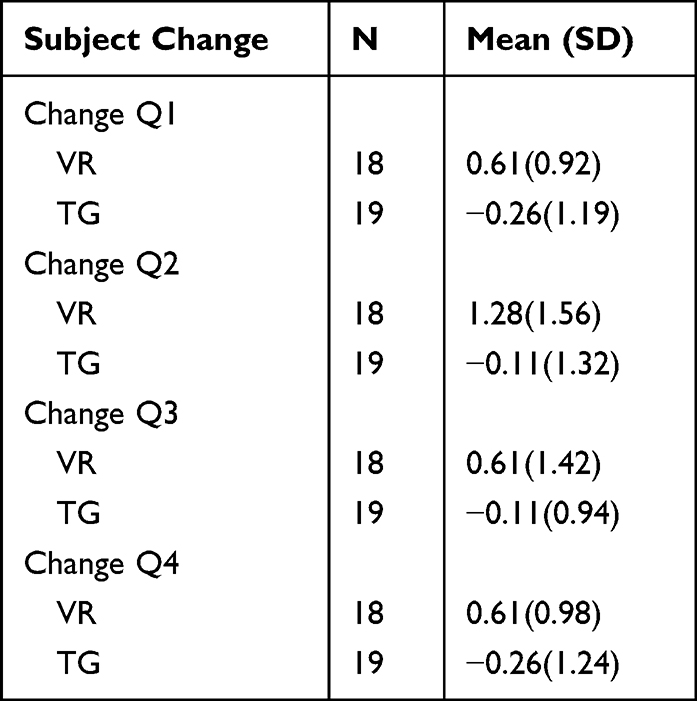 |
Table 5 Group Statistics on All Four-Subject Questions |
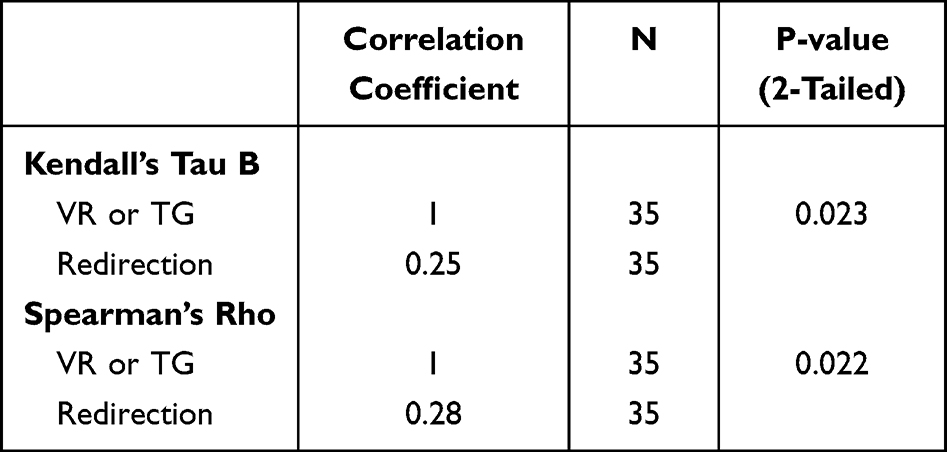 |
Table 6 Number of Redirections |
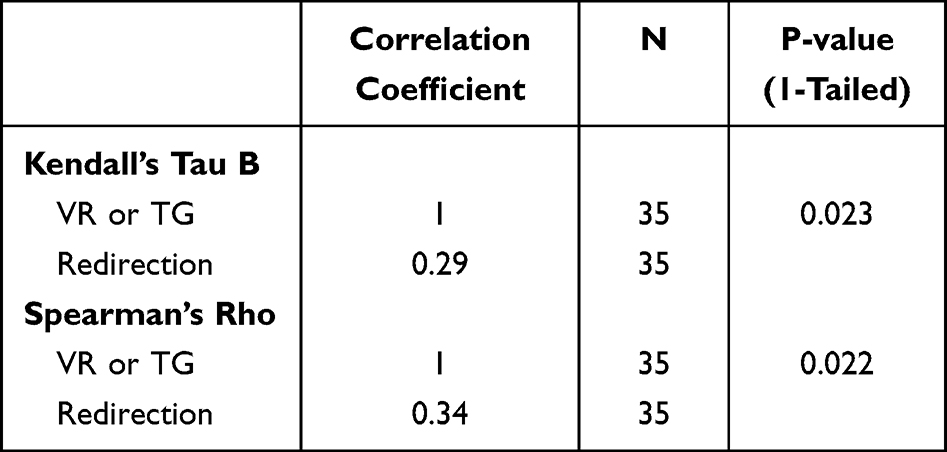 |
Table 7 Completion Time |
 |
Table 8 Training and Procedure Times and Number of Redirects |
Discussion
This prospective, blinded study aimed to evaluate virtual reality as a training model for orthopedic surgery and surgical training at large. Our study demonstrated a statistically significant (p < 0.05) difference in favor of the virtual reality group regarding time to completion and the number of redirections within the mock procedure. Using virtual reality for training allowed the operating surgeon more independence during the mock procedure. They required fewer redirections, which indicates improved knowledge regarding the required steps for successful completion.
Improved operating times are linked with patient outcomes and are associated with overall operating costs. Although the link between virtual reality’s improved operating room times has not been studied, the theoretical improvements based on current working clinical knowledge could translate to decreased surgical site infections, lower overall morbidity and mortality, and cost reduction. More research is needed to validate virtual reality training before actual operations to determine if there is a significant difference in patient outcomes.
There is significant variability in learning styles and preferences. This is one of the obstacles physician educators face.9,10 There are innumerable training manuals for visual learners and lectures that can be utilized for audio-based learners; however, procedure-based subspecialties need additional kinesthetic training to develop psychomotor skills. This cannot be obtained through stationary and passive learning. Although this is obtained during repetitive surgical procedures, virtual reality offers a bridge between the books and the operating room. It allows additional opportunities to develop the manual skills needed to become a proficient surgeon.11 Virtual reality limits the patient risk of trial and error of novice surgeons and may lessen surgical complications. That is, this is an important training opportunity for the future. The learning curve for different surgeries is variable among surgeons. Complexity and type of surgery can affect a surgeon’s proficiency. Some surgeons can be better at certain surgical modalities. VR can level the playing field by providing a safe learning environment to explore and develop skills on an individualized learning need.
Virtual reality may provide many theoretical applications and advantages to training and practicing surgeons. This modality can provide access to simulated procedures in uncommon cases. VR can refresh the steps of a surgical procedure or provide mock surgical situations such as complications or critical thinking scenarios. This technology can be developed to increase exposure to aspects of intraoperative complications that develop critical thinking in high-pressure situations before the occurrence.1,2,4,12 This can include mock intraoperative complications followed by experimental corrections with immediate critical feedback. In theory, this could improve surgeon response and reactivity to prompt recognition of complications and prior experience to navigate the next steps without delay. As supported by our subjective survey, virtual reality improves overall confidence with the procedure; this can be extrapolated to surgical complications and hopefully improved decision-making in the operating room. Having additional exposure and problem-solving through virtual reality can equip the surgeon, which could translate to mitigating complications. It can be a training tool for disseminating new surgical techniques beyond residency. VR can improve surgeon competence and proficiency, ultimately improving patient care.12,13
The main limitation of our study is the sample size, which may be the reason why we have several non-significant results. Another limitation of our study is the use of medical students rather than surgical residents. Medical students offer a more accurate review of the performance possibilities of VR, as they have no significant prior surgical training experience. This is a more accurate testing cohort for this model. Additionally, the volume of medical students interested in volunteering has limited the total number in each of our cohorts. Testing on a larger scale using medical school classes or other venue options will need to be conducted to improve sample size and the powered study. In addition, students’ prior differences in drill handling skills were controlled with the initial drill readiness training administered at the beginning of the study. Due to the novice nature of the medical students and the variability of exposure to power tools or drill use, equal time was spent in each student’s orientation regardless of training modality. This included drill chucking and unchucking the drill, familiarizing with trigger use, and forward and reverse operation of the drill. The study needs to address long-term comprehension of the surgery and maintenance of the information over a period of time. There are also challenges in using head-mounted displays, which were very well described in a recent study by Doughty et al.13 A future study focusing on the technical and human factor limitations, we believe, will make VR’s viability in teaching surgical navigation more impactful.
Conclusion
Virtual reality is an engaging training modality gaining support for routine use in surgical training. Our results and outcomes are similar to Blumstein et al recently published trial of the exact modality. Although similar, our study had an increased cohort size, standardization of the back table, and collection of subjective data from participants. This randomized, blinded trial demonstrated that VR improved performance specifically in regard to time to completion and the number of redirections within the mock procedure validating the legitimacy and effectiveness of virtual reality as a surgical training tool.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Araujo SE, Delaney CP, Seid VE, et al. Short-duration virtual reality simulation training positively impacts performance during laparoscopic colectomy in animal model: results of a single-blinded randomized trial: VR warm-up for laparoscopic colectomy. Surg Endosc. 2014;28(9):2547–2554. doi:10.1007/s00464-014-3500-3
2. Suresh D, Aydin A, James S, Ahmed K, Dasgupta P. The role of augmented reality in surgical training: a systematic review. Surg Innov. 2022. PMID: 36412148. doi:10.1177/15533506221140506
3. Bartlett J, Lawrence J, Stewart M, Nakano N, Khanduja V. Does virtual reality simulation have a role in training trauma and orthopedic surgeons? Bone Joint J. 2018;100(5):559–565. doi:10.1302/0301-620X.100B5.BJJ-2017-1439
4. Rheinberg F, Vollmeyer R, Burns B. QCM: a questionnaire to assess current motivation in learning situations. Diagnostics. 2001;47:57–66.
5. Martin JA, Regehr G, Reznick R, et al. Objective structured assessment of technical skill (OSATS) for surgical residents. Br J Surg. 1997;84(2):273–278. doi:10.1046/j.1365-2168.1997.02502.x
6. Mandal P, Ambade R. Surgery training and simulation using virtual and augmented reality for knee arthroplasty. Cureus. 2022;14(9):e28823. PMID: 36225417; PMCID: PMC9535617. doi:10.7759/cureus.28823
7. Bjorgul K, Novicoff WM, Saleh K. Learning curves in hip fracture surgery. J Int Orthop. 2011;35(1):113–119. doi:10.1007/s00264-010-0950-7
8. Blumstein G, Zukotynski B, Cevallos N, et al. Randomized trial of a virtual reality tool to teach surgical technique for tibial shaft fracture intramedullary nailing. J Surg Educ. 2020;77(4):SS1931–SS1937. doi:10.1016/j.jsurg.2020.01.002
9. Camp CL, Krych AJ, Stuart MJ, Regnier TD, Mills KM, Turner NS. Improving resident performance in knee arthroscopy: a prospective value assessment of simulators and cadaveric skills laboratories. JBJS. 2016;98(3):220–225. doi:10.2106/JBJS.O.00440
10. Price AJ, Erturan G, Akhtar K, et al. Evidence-based surgical training in orthopedics: how many arthroscopies of the knee are needed to achieve consultant-level performance? Bone Joint J. 2015;97-B(10):1309–1315. doi:10.1302/0301-620X.97B10.35973
11. Ruikar DD, Hegadi RS, Santosh K. A systematic review on orthopedic simulators for psychomotor skill and surgical procedure training. J Med Syst. 2018;42(9):168. doi:10.1007/s10916-018-1019-1
12. Shi J, Hou Y, Lin Y, Chen H, Yuan W. Role of visuohaptic surgical training simulator in resident education of orthopedic surgery. World Neurosurg. 2018;111:e98–e104. doi:10.1016/j.wneu.2017.12.015
13. Doughty M, Ghugre NR, Wright GA. Augmenting performance: a systematic review of optical see-through head-mounted displays in surgery. J Imaging. 2022;8(7):203. PMID: 35877647; PMCID: PMC9318659. doi:10.3390/jimaging8070203
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Outcomes of Non-Penetrating Deep Sclerectomy for Primary Congenital Glaucoma Performed by Experienced versus Trainee Surgeons: A Cohort Study

Khan OA, Sesma G, Alawi A, AlWazae M
Clinical Ophthalmology 2023, 17:897-906
Published Date: 16 March 2023
Implementation and Analysis of a Fully Immersive Virtual Reality-Based Emergency Training in a Surgical Curriculum
El-Sourani N, Mühling T, Klarmann R, Quintes S, Bockhorn M
Advances in Medical Education and Practice 2025, 16:811-823
Published Date: 16 May 2025
Holographic Imaging Combined with VR Simulation in Obstetrics and Gynecology Resident Training: A Review on Skill Development and Patient Privacy Protection
Yi L, Dong Z, Zeng J, Ou J, Zhao E
International Journal of Women's Health 2026, 18:590972
Published Date: 21 April 2026