Back to Journals » Journal of Inflammation Research » Volume 19
A Comparative Analysis of Neutrophil-to-Lymphocyte Ratio, Systemic Immune-Inflammation Index, and Hemoglobin-Albumin-Lymphocyte-Platelet Score in Migraine
Received 24 May 2026
Accepted for publication 18 June 2026
Published 10 July 2026 Volume 2026:19 625473
DOI https://doi.org/10.2147/JIR.S625473
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Pınar Öztürk,1 Çile Aktan2
1Department of Neurology, Ankara Yıldırım Beyazıt University, Yenimahalle Training and Research Hospital, Ankara, Türkiye; 2Department of Pain Medicine, Antalya Training and Research Hospital, Antalya, Türkiye
Correspondence: Pınar Öztürk, Department of Neurology, Ankara Yıldırım Beyazıt University, Yenimahalle Training and Research Hospital, Ankara, Türkiye, Tel +905554799814, Email [email protected]
Background: Migraine is increasingly recognized as a neuroinflammatory disorder characterized by trigeminovascular activation and cytokine-mediated nociceptive sensitization. While leukocyte-derived indices such as the neutrophil-to-lymphocyte ratio (NLR) and systemic immune–inflammation index (SII) reflect dynamic inflammatory responses, the hemoglobin–albumin–lymphocyte–platelet (HALP) score represents a composite immunonutritional marker associated with chronic systemic inflammation. However, its potential relevance in migraine remains unclear.
Methods: In this retrospective cross-sectional study, 115 patients with migraine were included. HALP, NLR, platelet-to-lymphocyte ratio (PLR), and SII were calculated from laboratory parameters obtained within ± 14 days of clinical evaluation. Associations with clinical variables were analyzed using correlation and regression analyses. Discriminative performance for chronic versus episodic migraine was assessed using receiver operating characteristic (ROC) curve analysis with Youden index estimation.
Results: Among the 115 included patients, 99 (86.1%) had episodic migraine and 16 (13.9%) had chronic migraine. HALP was not associated with monthly headache frequency, disease duration, or analgesic use and showed limited discriminative performance. In contrast, NLR and SII were significantly elevated in chronic migraine and demonstrated moderate discriminatory ability for differentiating chronic from episodic migraine (AUC = 0.734 and 0.723, respectively). However, these estimates should be interpreted cautiously given the relatively small chronic migraine subgroup.
Conclusion: These findings suggest that migraine-related inflammatory processes may be more sensitively reflected by rapidly responsive leukocyte-derived indices than by composite immunonutritional markers such as HALP. The lack of association between HALP and clinical features may indicate that systemic inflammatory involvement in migraine is limited or variable, rather than persistently elevated.
Keywords: migraine, chronic migraine, HALP score, neutrophil-to-lymphocyte ratio, systemic immune–inflammation index, inflammatory biomarkers
Introduction
Migraine is a highly prevalent and disabling neurological disorder that causes a substantial burden worldwide and markedly reduces quality of life.1,2 The diagnostic classification of migraine has been clearly established in the third edition of the International Classification of Headache Disorders (ICHD-3), which defines its major clinical subtypes.3 According to the ICHD-3, chronic migraine is defined as headache occurring on ≥15 days per month for more than 3 months, with migraine features present on at least 8 days per month.3 Among these, chronic migraine is associated with greater attack frequency, higher functional impairment, and increased healthcare utilization compared with episodic migraine.4
Beyond this clinical distinction, migraine is increasingly recognized as a disorder of altered pain processing involving neurovascular and neuroimmune mechanisms.5 This evolving pathophysiological perspective has increased interest in identifying biomarkers that may reflect disease activity and migraine chronification.
Current literature indicates that the pathophysiology of migraine cannot be explained solely by vascular mechanisms; instead, it involves a combination of central sensitization, activation of the trigeminovascular system, and inflammatory processes. Accumulating evidence suggests that sterile inflammation within the meningeal tissues activates trigeminal nerve endings and enhances pain sensitivity, supporting the role of neuroinflammatory mechanisms in migraine.5
Elevated levels of pro-inflammatory cytokines have been reported in both episodic and chronic migraine patients.6 An important component of these inflammatory processes is the release of neuropeptides from the trigeminovascular system, particularly calcitonin gene-related peptide (CGRP), which has a central role in the initiation and maintenance of migraine.7 These findings further support the association of migraine with immune activation and neuroinflammatory signaling.8,9
Various hematological parameters have been explored as markers of inflammatory activity in migraine. Among these, the neutrophil-to-lymphocyte ratio (NLR) has been associated with attack severity and overall inflammatory burden in several studies.10,11
Another increasingly studied inflammatory biomarker is the systemic immune–inflammation index (SII), which incorporates neutrophil, lymphocyte, and platelet counts into a single measure. By integrating information from both innate immune activation and platelet-related inflammatory responses, SII may provide a broader assessment of inflammatory burden than NLR alone. Elevated SII levels have been reported in patients with chronic migraine and other neuroinflammatory conditions. However, NLR and SII primarily reflect dynamic leukocyte-mediated inflammatory responses and do not capture the broader immunonutritional and hematologic context.6,12,13
This limitation has increased interest in composite biomarkers. The hemoglobin–albumin–lymphocyte–platelet (HALP) score integrates these parameters into a single index that may better reflect the interaction between inflammation, immune status, and nutritional condition. The prognostic value of HALP has been demonstrated in several malignancies, and emerging evidence suggests potential relevance in cardiovascular disease, ischemic stroke, and epilepsy.14–16
No studies have specifically evaluated the HALP score in migraine. This represents a relevant gap, as the biological components of HALP are each linked to processes implicated in migraine pathophysiology. Albumin is closely related to systemic inflammation,17 iron deficiency has been associated with migraine in prior studies18, and hematological variability has also been reported in patients with migraine.19 Taken together, these observations provide a rationale for investigating whether HALP may reflect migraine-related inflammatory and immunonutritional alterations.
Therefore, comparing HALP with established inflammatory indices, such as the NLR, may clarify whether a multidimensional immunonutritional marker provides additional value in migraine. Although HALP theoretically reflects broader biological domains than leukocyte-derived indices, its relevance in migraine has not been investigated. Accordingly, this study aimed to evaluate whether HALP is associated with migraine severity and chronicity, and to compare its performance with NLR and SII in characterizing migraine-related inflammatory activity. We hypothesized that patients with chronic migraine would exhibit higher inflammatory biomarker levels than those with episodic migraine and that the multidimensional HALP score would demonstrate clinically relevant associations with migraine burden and chronicity.
Materials and Methods
This retrospective cross-sectional study was conducted in the Neurology Outpatient Clinic of Ankara Yıldırım Beyazıt University Yenimahalle Training and Research Hospital. Adult patients aged 18–65 years who were admitted between January 1, 2021, and November 30, 2025, and diagnosed with migraine based on the International Classification of Headache Disorders, 3rd edition (ICHD-3), were evaluated. Hospital Information Management System (HIMS) records were reviewed, and demographic characteristics, clinical visit notes, and laboratory results were systematically extracted using a standardized data collection form. A neurologist confirmed migraine diagnosis through integrated assessment of medical history, attack characteristics, and physical examination findings.
The patient screening process, exclusion criteria, and final study cohort are summarized in Figure 1.
 |
Figure 1 Flow diagram of patient screening, exclusion criteria, and final study cohort selection. The diagram illustrates the number of patients assessed for eligibility, reasons for exclusion, and the final number of episodic and chronic migraine patients included in the analysis. |
To ensure temporal relevance between laboratory parameters and clinical status, hemogram and biochemistry measurements were required to be performed within ±14 days of the clinical visit date. Records exceeding this window were excluded to minimize biological variability. HALP (Hemoglobin–Albumin–Lymphocyte–Platelet) was calculated using hemoglobin (g/L), albumin (g/L), lymphocyte (/L), and platelet (/L) values obtained from the same blood sample. Neutrophil-to-lymphocyte ratio (NLR) was calculated by dividing the absolute neutrophil count by the absolute lymphocyte count.
The Hemoglobin–Albumin–Lymphocyte–Platelet (HALP) score was calculated according to the following formula:
HALP = (Hemoglobin [g/L] × Albumin [g/L] × Lymphocyte count [/L]) / Platelet count [/L]. Strict exclusion criteria were applied to avoid confounding inflammatory conditions. Patients were excluded if they had acute infection, leukocytosis, markedly elevated C-reactive protein (CRP), chronic inflammatory disease (rheumatoid arthritis, systemic lupus erythematosus, vasculitis, Behçet’s disease, inflammatory bowel disease, psoriasis), active malignancy or cancer treatment within five years, hematological disorder, severe liver failure, nephrotic syndrome, or marked malnutrition. Individuals with major surgery, trauma, or blood transfusion within the previous three months and those receiving immunosuppressive or systemic corticosteroid therapy were also excluded. Patients with incomplete or inconsistent laboratory–clinical records were excluded from the final analysis.
Statistical Analyses
All statistical analyses were performed using IBM SPSS Statistics version 26.0. The distribution of continuous variables was assessed using the Kolmogorov–Smirnov test. Parametric comparisons were conducted with the Student’s t-test for normally distributed data, while non-parametric comparisons were made using the Mann–Whitney U-test for non-normally distributed variables. Categorical variables were compared using the chi-square test. Correlations between inflammatory biomarkers (HALP, NLR, PLR, and SII) and clinical parameters were examined using Pearson or Spearman correlation coefficients, depending on distributional characteristics. To evaluate the independent contribution of HALP and NLR to headache burden, multivariable linear regression models were constructed.
To determine the discriminatory capacity of inflammatory biomarkers for differentiating chronic from episodic migraine, receiver operating characteristic (ROC) curve analyses were conducted. Optimal threshold values for NLR and SII were calculated using the Youden index, and corresponding sensitivity, specificity, odds ratio (OR), and confusion matrix values were generated. Effect sizes were calculated using Cohen’s d to quantify the magnitude of differences between groups and to aid interpretation of the findings. A two-tailed p-value of <0.05 was considered statistically significant.
Results
A total of 149 migraine patients were screened, of whom 34 were excluded due to missing albumin results, active infection markers, malignancy, or rheumatologic disease (Figure 1). The remaining 115 patients were included in the final analysis, comprising 99 (86.1%) with episodic migraine and 16 (13.9%) with chronic migraine. The cohort’s mean HALP score was 55.22 ± 22.38, and the mean monthly headache frequency was 6.62 ± 5.11 days. When comparing migraine subtypes, patients with chronic migraine exhibited a markedly greater monthly headache burden than those with episodic disease (16.25 ± 2.89 vs 5.09 ± 3.34 headache days per month; p < 0.001), confirming the expected substantial clinical distinction between the two phenotypes. Baseline demographic and clinical characteristics of the study population are summarized in Table 1.
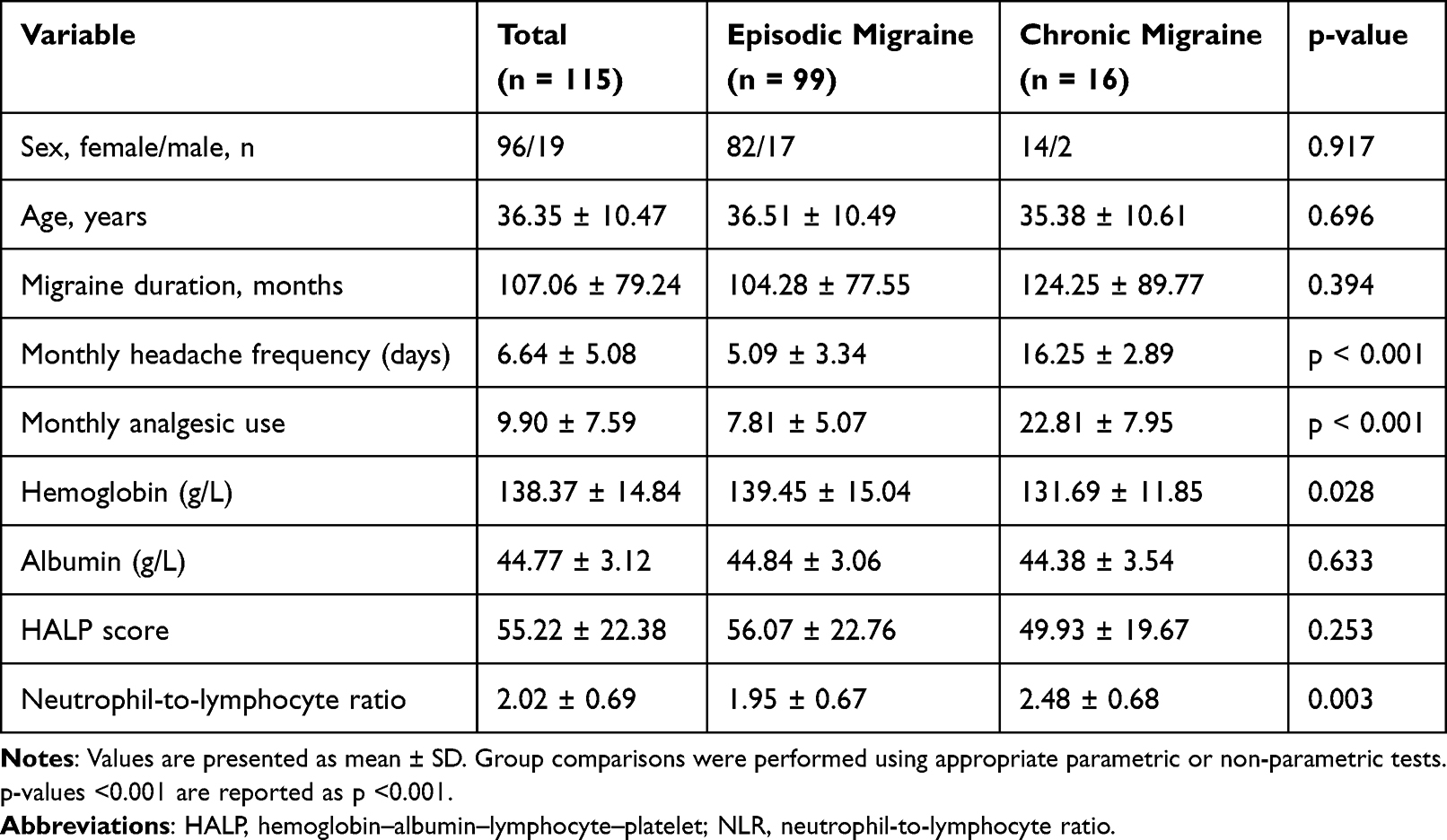 |
Table 1 Baseline Demographic and Clinical Characteristics of the Study Population |
Spearman correlation analysis revealed no significant association between HALP and migraine duration (ρ = –0.037, p = 0.720), monthly headache frequency (ρ = −0.077, p = 0.414), or monthly analgesic consumption (ρ = –0.032, p = 0.762) (Table 2).
 |
Table 2 Correlation Analysis Between Biomarkers and Clinical Variables |
Similarly, no correlation was observed between attack frequency and inflammatory indices PLR (ρ = 0.046, p = 0.624) or SII (ρ = 0.137, p = 0.144). ROC analysis demonstrated limited performance for HALP (AUC = 0.410–0.511) and PLR (AUC = 0.557) in migraine characterization (Figure 2). Multiple linear regression performed with monthly attack frequency as the dependent variable and HALP, NLR, and migraine duration as predictors revealed no significant effects for HALP (β = –0.0034, p = 0.880), NLR (β = +1.2145, p = 0.103), or migraine duration (β = +0.0068, p = 0.266), with an overall low model explanatory power (R2 = 0.035).
 |
Figure 2 Comparison of receiver operating characteristic (ROC) curve area under the curve (AUC) values for inflammatory biomarkers. The figure presents comparative AUC values of HALP, PLR, NLR, and SII for differentiating chronic from episodic migraine. |
A sex-stratified comparison showed that HALP scores were significantly higher in males than in females (79.70 ± 29.06 vs 50.37 ± 17.24; p < 0.001). Males also had higher hemoglobin levels (160.0 ± 11.7 vs 134.1 ± 11.1; p < 0.001) and albumin levels (46.42 ± 3.17 vs 44.45 ± 2.99; p = 0.037), whereas NLR did not differ by sex (2.03 ± 0.69 vs 2.02 ± 0.69; p = 0.871). A weak inverse correlation was observed between age and HALP (ρ = −0.178, p = 0.056), although this association did not reach statistical significance.
When categorized by age (<35, 35–50, >50 years), mean HALP values were 60.60 ± 23.18, 51.69 ± 22.50, and 52.23 ± 10.74, respectively. Although HALP values tended to be lower in older age groups, the overall difference did not reach statistical significance (Kruskal–Wallis p = 0.093). No statistically significant pairwise differences were observed after Bonferroni correction.
In the chronic–episodic comparison for inflammatory metrics, NLR and SII were significantly elevated among chronic migraine patients (NLR: 2.48 ± 0.68 vs 1.95 ± 0.67; p = 0.003, SII: 664.1 ± 165.9 vs 525.4 ± 236.5; p = 0.0043). HALP and PLR did not differ significantly between groups (both p > 0.25) (Table 3). The observed differences in NLR and SII between chronic and episodic migraine were associated with moderate-to-large effect sizes (Cohen’s d = 0.80 for NLR and 0.61 for SII), despite the relatively small chronic migraine subgroup.
 |
Table 3 Comparison Between Episodic and Chronic Migraine |
HALP tertile-based comparison of monthly headache frequency showed mean values of 6.89 ± 5.32, 7.03 ± 5.26, and 6.03 ± 4.71 days/month for the low, medium, and high tertiles, respectively. No significant difference in headache frequency was observed across HALP tertiles (Kruskal–Wallis p = 0.719), indicating the absence of a dose–response relationship between HALP levels and migraine burden (Figure 3).
 |
Figure 3 Monthly headache frequency according to tertiles of the Hemoglobin–Albumin–Lymphocyte–Platelet (HALP) score. Mean monthly headache frequency was comparable across low, medium, and high HALP tertiles, with no significant overall difference, supporting the absence of a clinically meaningful association between HALP level and migraine burden. |
In migraine type differentiation, ROC analysis identified NLR (AUC = 0.734) and SII (AUC = 0.723) as the most effective markers for distinguishing chronic from episodic migraine (Figure 4). The optimal NLR cut-off identified by the Youden index was 1.9087, yielding a sensitivity of 0.875 and a specificity of 0.626 (Table 4). At this threshold, 14 of 16 chronic migraine patients and 62 of 99 episodic migraine patients were correctly classified, whereas 2 chronic and 37 episodic migraine patients were misclassified.
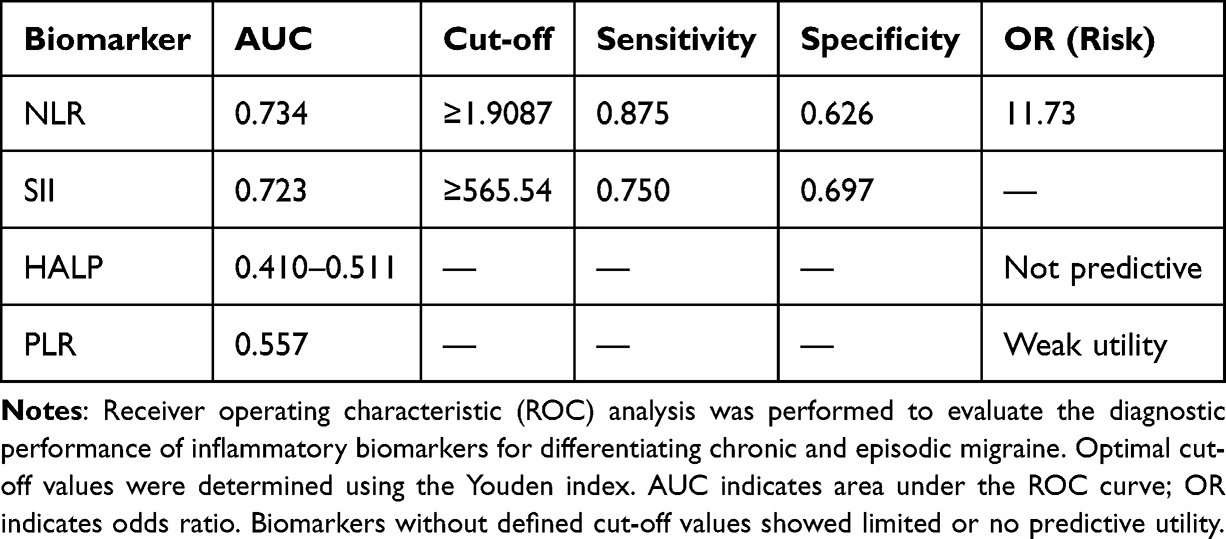 |
Table 4 ROC Analysis for Biomarkers in Chronic vs Episodic Migraine |
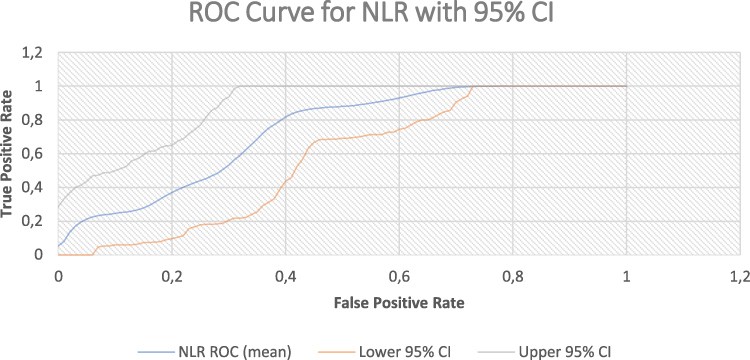 |
Figure 4 Receiver operating characteristic (ROC) curve of the neutrophil-to-lymphocyte ratio (NLR) for differentiating chronic and episodic migraine. The ROC curve demonstrates the diagnostic performance of NLR, including the area under the curve and 95% confidence intervals. |
Likewise, using the SII threshold of ≥565.5 resulted in correct identification of 69 episodic and 12 chronic patients, with 30 episodic and 4 chronic cases incorrectly assigned. At this threshold, patients with elevated NLR demonstrated approximately 11.7-fold increased odds of chronic migraine.
Discussion
This retrospective cross-sectional study investigated the relationship between the HALP score and clinical features of migraine, and compared its performance with established inflammatory indices, particularly the NLR and the SII. To our knowledge, this is the first study to evaluate HALP in a migraine population. The main findings can be summarized as follows. First, HALP was not associated with headache frequency, disease duration, or analgesic use and demonstrated limited ability to discriminate between episodic and chronic migraine. In contrast, NLR and SII were significantly elevated in chronic migraine and showed acceptable discriminative performance. Finally, HALP values were strongly influenced by sex and, to a lesser extent, by age, suggesting that HALP primarily reflects physiological variability rather than disease-related inflammatory activity.
Despite its theoretical appeal as a multidimensional biomarker integrating hematologic, inflammatory, and nutritional domains, HALP was not associated with headache frequency, disease duration, or analgesic use in this cohort and did not meaningfully distinguish episodic from chronic migraine. Its limited performance across correlation, subgroup, and ROC analyses suggests that HALP may be insufficiently sensitive to detect the relatively modest and fluctuating inflammatory changes associated with migraine severity or chronification. In a relatively young outpatient population without major systemic comorbidity, these findings support the view that migraine-related inflammation may not generate the sustained immunonutritional disturbance required to alter slowly changing composite markers such as HALP.
Previous studies have shown increased platelet activation and enhanced platelet–leukocyte interactions in migraine, supporting the presence of an inflammatory vascular response in this disorder.20 This is relevant to HALP-based interpretation because platelet-related changes may indeed accompany migraine; however, our findings suggest that such alterations are not sufficiently sustained or integrated at the immunonutritional level to generate a clinically informative HALP signal.
Neutrophils and lymphocytes play central roles in inflammatory signaling, and shifts in their circulating levels are commonly used to reflect systemic inflammatory status.21,22 During physiological stress, neutrophil counts tend to rise while lymphocyte levels decline, which helps explain why leukocyte-derived indices such as NLR and SII may be more sensitive than HALP to the dynamic inflammatory changes observed in migraine. Serum albumin levels typically decline during systemic inflammatory states because albumin functions as a negative acute-phase reactant, making it more informative in conditions characterized by sustained inflammatory burden rather than transient inflammatory fluctuations.23
Our results showed that NLR and SII had stronger discriminative performance than HALP for distinguishing chronic from episodic migraine, with AUCs of 0.734 and 0.723, respectively. By contrast, HALP was not meaningfully associated with any of the clinical parameters examined. This pattern is consistent with the view of migraine as a dynamic neuroimmune disorder characterized by transient trigeminovascular activation, cytokine release, and CGRP-mediated neurogenic inflammation rather than sustained systemic inflammatory burden.6,24
An apparent paradox arises from the observation that NLR and SII differed between chronic and episodic migraine whereas HALP did not. One possible explanation is that migraine chronification may generate a degree of persistent low-grade inflammatory activation sufficient to influence leukocyte-derived indices, yet insufficient to alter the more stable hematologic and nutritional components incorporated into the HALP score. Thus, the inflammatory signal associated with chronic migraine may be detectable at the cellular immune level without producing the broader systemic immunonutritional changes required to substantially affect HALP.
NLR and SII predominantly reflect acute innate immune activation and may therefore be more sensitive to the dynamic inflammatory changes associated with migraine.10,11,13 In contrast, HALP incorporates hematologic and nutritional components that are also influenced by factors such as nutritional status, hepatic protein synthesis, and chronic disease burden.25
Because these components generally change more slowly than leukocyte-derived indices, HALP may be less responsive to the episodic inflammatory fluctuations characteristic of migraine.25–27 The absence of meaningful associations between HALP and migraine characteristics further supports the notion that migraine-related inflammation is predominantly episodic rather than sustained. Accordingly, composite immunonutritional markers such as HALP may be less informative than rapidly responsive leukocyte-derived indices in this clinical setting.14,28,29 The relative stability of HALP across migraine subgroups further supports the view that migraine-related neuroimmune activation is episodic rather than sustained, consistent with transient CGRP-mediated inflammatory cascades rather than progressive immunometabolic disruption.24,30 In disorders characterized by persistent inflammatory pressure, reductions in albumin or lymphocyte counts are expected; however, this pattern was not observed in our cohort.
Notably, higher HALP, hemoglobin, and albumin levels observed in males suggest that baseline sex-related hematologic differences may outweigh disease-related variation. This finding is consistent with known sex differences in hemoglobin levels and the female predominance of migraine.1,19 Such effects may obscure subtle associations between HALP and migraine characteristics and highlight the importance of sex-stratified analyses.
These findings suggest that HALP should not be considered a negative biomarker but rather a context-dependent indicator that may be more informative in settings such as refractory migraine, metabolic comorbidity, or treatment response, rather than in single-time-point assessments. Its potential value may be better realized in longitudinal or intervention-based studies, where immunonutritional status is more likely to change over time.
The present findings have several implications for both clinical practice and future research. Although HALP did not show meaningful predictive or discriminative value in migraine, this result is informative because it suggests that routine hematologic–nutritional indices may remain relatively preserved despite migraine chronicity. In turn, this supports the view that migraine imposes a dynamic neuroimmune burden rather than a sustained systemic inflammatory disturbance.10
Clinically, these findings suggest that HALP alone is unlikely to be useful as a diagnostic or monitoring tool in routine migraine evaluation. In contrast, the superior discrimination of NLR and SII between chronic and episodic migraine points to a more acute inflammatory activation pattern reflected by leukocyte-derived inflammatory indices rather than by slower metabolic or nutritional pathways.31 Accordingly, simple and widely available blood-based markers may still have clinical value, particularly those reflecting rapid immune dynamics rather than slower immunonutritional changes.
Although ROC–Youden analysis identified NLR ≥1.91 and SII ≥565.5 as optimal thresholds for differentiating chronic from episodic migraine in this cohort, these values should be considered hypothesis-generating rather than clinically actionable. The small size of the chronic migraine subgroup (n = 16), together with the fact that the ROC-derived cut-offs were both identified and evaluated within the same dataset, limits the robustness and external validity of these estimates. Consequently, the reported discriminatory performance and odds ratios may be subject to optimism bias. Moreover, despite AUC values of 0.734 for NLR and 0.723 for SII, the corresponding confidence intervals were relatively wide (NLR: 95% CI, 0.622–0.838; SII: 95% CI, 0.596–0.836), reflecting the uncertainty associated with the limited number of patients with chronic migraine. Therefore, these findings should be interpreted cautiously and require validation in larger independent cohorts before any clinical application can be considered. Rather, they primarily underscore the relative superiority of rapidly responsive leukocyte-derived indices over composite immunonutritional markers in capturing migraine-related inflammatory dynamics.
This observation may partly explain the limited discriminative performance of HALP, as baseline sex-related physiology may attenuate disease-associated variation.32 Future studies should therefore evaluate HALP not only in cross-sectional settings but also in longitudinal and interventional designs, particularly in patients with high-frequency migraine, refractory migraine, or during treatment-response monitoring, where metabolic and immunologic changes may be more likely to emerge.
This study has several limitations. Its retrospective cross-sectional design precludes causal inference and does not permit assessment of temporal fluctuations in inflammatory markers across migraine phases. No a priori sample size calculation was performed because of the retrospective nature of the study. Furthermore, the relatively small chronic migraine subgroup (n = 16) may have limited statistical power for chronic-versus-episodic comparisons and reduced the ability to detect modest biomarker-related differences, particularly for HALP. Therefore, negative findings should be interpreted with caution and should be confirmed in larger prospective cohorts with a more balanced distribution of migraine subtypes. In addition, although strict exclusion criteria were applied, potentially relevant factors, including diet, body mass index, metabolic status, iron deficiency, sleep patterns, and menstrual phase, were not recorded and may have influenced HALP independently of migraine severity. Headache frequency and analgesic use were obtained from clinical records rather than prospective diary-based follow-up, which may have introduced recall and documentation bias. Furthermore, because HALP reflects relatively slowly changing hematologic and nutritional components, a single time-point measurement may be insufficient in a disorder marked by episodic neuroinflammatory activity. Finally, the single-center nature of the dataset and the absence of a healthy control group limit the generalizability and interpretation of these findings, and larger multicenter studies including non-migraine controls are needed to confirm the present results.
Conclusion
In this study, HALP did not correlate with headache frequency, migraine duration, or analgesic use and did not distinguish between episodic and chronic migraine. In contrast, NLR and SII showed acceptable discriminative performance, suggesting that migraine-related inflammatory activity is better reflected by rapidly responsive leukocyte-derived indices than by slower immunonutritional markers. These findings support the view that migraine is characterized by episodic neuroinflammatory activation rather than sustained systemic inflammatory burden. Although HALP was not informative in this cross-sectional setting, this should not be interpreted as biological irrelevance. Instead, it suggests that HALP may be more appropriately evaluated in longitudinal designs, larger chronic migraine cohorts, and clinical contexts marked by greater metabolic or inflammatory fluctuation, such as treatment-response monitoring or metabolically vulnerable subgroups.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Ankara Yıldırım Beyazıt University Yenimahalle Training and Research Hospital with decision number E-2025-38. Due to the retrospective design of the study, informed consent was waived by the ethics committee. Patient data were anonymized prior to analysis and handled in accordance with institutional and ethical standards to ensure confidentiality.
Author Contributions
Pınar Öztürk: Conceptualization, Methodology, Validation, Formal analysis, Investigation, Data curation, Writing—original draft preparation, Writing—review and editing.
Çile Aktan: Conceptualization, Methodology, Validation, Formal analysis, Investigation, Resources, Software, Visualization, Supervision, Project administration, Writing—original draft preparation, Writing—review and editing.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funding was received for this study.
Disclosure
The authors declare no conflicts of interest.
References
1. Natoli JL, Manack A, Dean B, Butler Q, Turkel CC, Stovner L. Global prevalence of chronic migraine: a systematic review. Cephalalgia. 2010;30(5):599–11. doi:10.1111/j.1468-2982.2009.01941.x
2. Dadali S, Babaoglu G, Sabuncu U, Akcaboy EY. Comparison of the efficacy of ultrasound-guided repeated greater occipital nerve blocks and greater occipital nerve pulsed radiofrequency in migraine treatment. Pain Physician. 2025;28(4):337–346.
3. Headache Classification Committee of the International Headache Society. The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
4. Blumenfeld AM, Bloudek LM, Becker WJ, Buse DC, Varon SF, Maglinte GA. Patterns of use and reasons for discontinuation of prophylactic medications for episodic and chronic migraine: results from the second International Burden of Migraine Study (IBMS-II). Headache. 2013;53:644–655. doi:10.1111/head.12055
5. Ramachandran R. Neurogenic inflammation and its role in migraine. Semin Immunopathol. 2018;40(3):301–314.
6. Martami F, Razeghi Jahromi S, Togha M, Ghorbani Z, Seifishahpar M, Saidpour A. The serum level of inflammatory markers in chronic and episodic migraine: a case-control study. Neurol Sci. 2018;39(10):1741–1749. doi:10.1007/s10072-018-3493-0
7. Leira Y, Ameijeira P, Domínguez C, et al. Periodontal inflammation and CGRP in chronic migraine. J Periodontol. 2019;90(9):1088–1095. doi:10.1002/jper.19-0051
8. Uzar E, Evliyaoglu O, Yucel Y, Ugur Cevik M, Acar A, Erdal ME. Serum cytokine and pro-brain natriuretic peptide levels in patients with migraine. Eur Rev Med Pharmacol Sci. 2011;15(10):1111–1116.
9. Morgan CT, Nkadimeng SM. The role of inflammation in migraine headaches: a review. FASEB BioAdv. 2025;7e70033. doi:10.1096/fba.2024-00188
10. Yazar HO, Yazar T, Aygün A, Kaygisiz Ş, Kirbaş D. Simple inflammatory blood parameters in migraine. Ir J Med Sci. 2020;189(2):677–683. doi:10.1007/s11845-019-02136-y
11. Karabulut KU, Egercioglu TU, Uyar M, Ucar Y. Neutrophil/lymphocyte ratio in migraine attacks. Ann Med Surg. 2016;10:52–56. doi:10.1016/j.amsu.2016.07.023
12. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
13. Wijeratne T, Murphy MJ, Wijeratne C, et al. Serial systemic immune inflammation indices: markers of acute migraine events or indicators of persistent inflammatory status? J Headache Pain. 2025;26:7. doi:10.1186/s10194-024-01929-6
14. Xu H, Zheng X, Ai J, Yang L. HALP score and cancer prognosis. Int Immunopharmacol. 2023;114:109496. doi:10.1016/j.intimp.2022.109496
15. Dong J, Jiang W, Zhang W, et al. HALP score and mortality. Front Oncol. 2024;14:1388610. doi:10.3389/fonc.2024.1388610
16. Fu J, Chen X, Li J, Rong B, Peng L. The hemoglobin, albumin, lymphocyte, and platelet (HALP) score predicts the prognosis of adults with status epilepticus: a retrospective study. J Inflamm Res. 2024;17:9625–9635. doi:10.2147/JIR.S491666
17. Soeters PB, Wolfe RR, Shenkin A. Hypoalbuminemia. JPEN J Parenter Enteral Nutr. 2019;43(2):181–193. doi:10.1002/jpen.1451
18. Singh RK, Kaushik RM, Goel D, Kaushik R. Association between iron deficiency anemia and chronic daily headache: a case-control study. Cephalalgia. 2023;43:3331024221143540. doi:10.1177/03331024221143540
19. Sarıcam G. Relationship between migraine headache and hematological parameters. Acta Neurol Belg. 2021;121(4):899–905. doi:10.1007/s13760-020-01362-x
20. Zeller JA, Lindner V, Frahm K, Baron R, Deuschl G. Platelet activation and platelet–leucocyte interaction in patients with migraine: subtype differences and influence of triptans. Cephalalgia. 2005;25(7):536–541. doi:10.1111/j.1468-2982.2005.00916.x
21. de Jager CP, Van Wijk PT, Mathoera RB. Lymphocytopenia and neutrophil–lymphocyte count ratio predict bacteremia better than conventional infection markers in an emergency care unit. Crit Care. 2010;14:R192.
22. Zahorec R. Ratio of neutrophil-to-lymphocyte counts—rapid and simple parameter of systemic inflammation and stress in critically ill patients. Bratisl Lek Listy. 2001;102(1):5–14.
23. Don BR, Kaysen G. Serum albumin: relationship to inflammation and nutrition. Semin Dial. 2004;17(6):432–437. doi:10.1111/j.0894-0959.2004.17603.x
24. Edvinsson L, Haanes KA, Warfvinge K, Krause DN. CGRP as the target of new migraine therapies: successful translation from bench to clinic. Nat Rev Neurol. 2018;14(6):338–350. doi:10.1038/s41582-018-0003-1
25. Farag CM, Antar R, Akosman S, Ng M, Whalen MJ. What is hemoglobin, albumin, lymphocyte, platelet (HALP) score? A comprehensive literature review of HALP’s prognostic ability in different cancer types. Oncotarget. 2023;14:153–172. doi:10.18632/oncotarget.28367
26. Lee SH, Kim JH, Kwon YS, Sohn JH. Role of peripheral inflammatory markers in patients with acute headache attack to differentiate between migraine and non-migraine headache. J Clin Med. 2022;11:6538. doi:10.3390/jcm11216538
27. Salahi M, Parsa S, Nourmohammadi D, et al. Immunologic aspects of migraine: a review of literature. Front Neurol. 2022;13:944791. doi:10.3389/fneur.2022.944791
28. Zhu X, Zhang Y, Wang A, et al. Association between hemoglobin, albumin, lymphocyte, and platelet (HALP) score and poor outcomes in acute ischemic stroke patients with type 2 diabetes mellitus: a study from the Third China National Stroke Registry. Front Neurol. 2025;15:1461188. doi:10.3389/fneur.2024.1461188
29. Xin Y, Wang Y, Shu Y, Liang H, Yang Y. HALP score predicts prognosis in patients with atrial fibrillation and acute coronary syndrome. BMC Cardiovasc Disord. 2025;25:507. doi:10.1186/s12872-025-04968-2
30. Charles A. The pathophysiology of migraine: implications for clinical management. Lancet Neurol. 2018;17(2):174–182. doi:10.1016/S1474-4422(17)30435-0
31. Vurallı D. Systemic inflammatory markers in chronic and episodic migraine. In:
32. Antar R, Farag C, Xu V, Drouaud A, Gordon O, Whalen MJ. Evaluating the baseline hemoglobin, albumin, lymphocyte, and platelet (HALP) score in the United States adult population and comorbidities: an analysis of the NHANES. Front Nutr. 2023;10:1206958. doi:10.3389/fnut.2023.1206958
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Role of Inflammatory Hematologic Indices in Predicting Acute Coronary Syndrome in Elderly Patients with Chronic Coronary Syndrome
Bao Q, Liu T, Song H, Bao W, Fan W
Journal of Inflammation Research 2025, 18:9637-9653
Published Date: 22 July 2025
Clinical Relevance of HALP Score in Predicting Hospital Stay Duration and Outcomes in Acute Heart Failure
Aydın MZ, Abdi IA
International Journal of General Medicine 2025, 18:7095-7100
Published Date: 26 November 2025
The Predictive Value of Systemic Inflammatory Markers from Failed Single-Dose Methotrexate Therapy in Tubal Ectopic Pregnancy: A Retrospective Single-Center Study
Liu R, Li S
Journal of Inflammation Research 2026, 19:578852
Published Date: 23 March 2026