Back to Journals » Journal of Inflammation Research » Volume 19
The Predictive Value of Systemic Inflammatory Markers from Failed Single-Dose Methotrexate Therapy in Tubal Ectopic Pregnancy: A Retrospective Single-Center Study
Received 8 November 2025
Accepted for publication 4 March 2026
Published 23 March 2026 Volume 2026:19 578852
DOI https://doi.org/10.2147/JIR.S578852
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Xin Du
Ruoxi Liu, Shuangdi Li
Department of Gynecology, School of Medicine, Shanghai First Maternity and Infant Hospital, Tongji University, Shanghai, People’s Republic of China
Correspondence: Ruoxi Liu, Department of Gynecology, School of Medicine, Shanghai First Maternity and Infant Hospital, Tong Ji University, Shanghai, People’s Republic of China, Email [email protected]
Purpose: Assessing the systemic inflammatory markers as a prognostic factor for resistance to methotrexate in ectopic pregnancy.
Methods: This retrospective cohort study included 412 cases of patients with tubal ectopic pregnancy who received single-dose methotrexate (MTX) therapy at the Obstetrics and Gynecology Hospital affiliated with Tongji University from January 2019 to January 2024. Participants were categorized into successful and unsuccessful cohorts according to single-dose methotrexate treatment. Systemic inflammatory parameters, particularly lymphocyte counts, NLR, and β-hCG, were collected for each case from blood tests. Regression analyses were employed to pinpoint independent risk factors linked to treatment failure. A nomogram was developed to represent these relationships. The model’s ability to distinguish outcomes was assessed by the area under the curve (AUC).
Results: The research sample included 302 successful individuals and 110 unsuccessful ones. Compared with baseline, NLR decreased by less than 40.3% on Day 4 (95% [CI] 1.26– 3.12), while β-hCG levels rose on Day 4 (95% CI: 1.14– 2.80). HCG levels > 342.25 mIU/mL on day 0 (95% CI 1.74– 4.40) and lymphocyte counts > 2.165 × 109/L on day 4 (95% CI 1.39– 3.42) were also predictive factors for treatment failure. ROC curve area was 0.705 (95% CI: 0.650– 0.760), with a Hosmer–Lemeshow test P-value above 0.05 (P = 0.607).
Conclusion: Among systemic inflammatory markers, NLR and lymphocyte levels significantly correlate with treatment failure. Incorporating them with β-hCG into the model enhances risk predictive capability.
Keywords: systemic inflammatory markers, neutrophil-to-lymphocyte ratio, clinical predictive modeling, ectopic pregnancy, methotrexate
Introduction
Ectopic pregnancy involves a fertilized egg implanting outside the uterus, with tubal pregnancy being the most common type.1 It occurs in 2% to 3% of early pregnancies.2 The management is mainly divided into three categories: expectant management, drug therapy, and surgical treatment. Methotrexate (MTX) is a chemotherapeutic antimetabolite highly sensitive to trophoblastic cells. Reports indicate that MTX therapy achieves success in approximately 70–90% of cases.3 Stovall et al introduced the single-dose MTX protocol (calculated at 50 mg/m2 body surface area) in 1991. This procedure has been widely adopted and continued to this day due to its simplicity and safety. However, treatment failure can lead to rupture of ectopic masses, posing life-threatening risks such as hemorrhage and hemodynamic instability.4 Additionally, due to the prolonged duration of MTX therapy, initial results typically require one week to assess, which can cause patient anxiety, exacerbate the condition, and even lead to doctor-patient conflicts. Therefore, in clinical practice, determining whether single-dose methotrexate therapy is more likely to succeed or fail for a patient remains a challenge.
Existing predictive models primarily rely on other biomarkers such as β-hCG and progesterone, the size masses, and cardiac activity in ectopic pregnancies.5–7 Additionally, several machine learning algorithms and ultrasound radiomics models incorporating ectopic pregnancy-related medical history and complex imaging parameters have been successively developed.8–12 However, regrettably, systemic inflammatory markers, closely linked to trophoblast proliferation and pathological inflammation, have not been widely incorporated into these models. Recently, NLR, an immune-inflammatory marker derived from peripheral blood, has garnered significant attention. It is associated with various diseases and has demonstrated certain efficacy in predicting the progression and severity of benign and malignant gynecological diseases.13–16 MTX exerts its therapeutic effect by inhibiting trophoblast proliferation through blocking folic acid metabolism, thereby modulating the systemic inflammatory microenvironment. Neutrophils and lymphocytes respond differently to the efficacy of MTX. Specifically, effective MTX treatment induces trophoblast apoptosis, alleviates pathological inflammation, thereby leading to changes in NLR. Notably, Days 0 and 4 correspond to the early critical window of MTX treatment.
As ectopic pregnancy rates have risen sharply, early stratification and prediction of high-risk ectopic pregnancy patients are significant. However, current studies mostly focus on the baseline levels of NLR, and data regarding the dynamic changes of inflammatory markers are limited. Therefore, this investigation aims to explore the prognostic significance of early NLR changes for ectopic pregnancy patient outcomes following single-dose MTX therapy.
Materials and Methods
Ethical Approval
We analyzed Obstetrics and Gynecology Hospital ectopic pregnancy cases from January 2019 through January 2024. Ethical approval (KS24275) was secured from the Tongji University School of Medicine’s affiliated Obstetrics and Gynecology Hospital for this research. Then patient demographic and clinical data were obtained from the Medical Record System. Conducted under Helsinki Declaration, this retrospective study waived patient consent requirements.
Study Design
This study was designed and conducted in accordance with the RECORD guidelines. Exclusion criteria included embryonic cardiac activity on ultrasound and the selection of patients who received expectant treatment or initial surgical treatment. Furthermore, to prevent potential pharmacological interactions, patients with rheumatic or inflammatory conditions were also omitted from consideration. In contrast, the selection criteria involved the following: (1) confirmed ectopic pregnancy through clinical diagnosis; (2) administration of single-dose methotrexate treatment regimen; (3) access to comprehensive medical records. Diagnosis of ectopic pregnancy was determined by an initial physical examination, laboratory (especially serum β-hCG levels), and sonographic evaluation. The doctor confirmed an ectopic pregnancy when transvaginal imaging located a gestational sac outside the uterine cavity, coupled with suboptimal β-hCG growth that failed to hit the 66% mark within 48 hours, or the absence of embryonic tissue following uterine evacuation procedures.7 After all these criteria were applied, 412 patients were enrolled in the research (Figure 1). After assessment of vital signs and symptoms, a standard 50 mg/m2 dose of methotrexate was injected into hemodynamically stable patients with ectopic pregnancies who were potentially at risk and closely monitored, according to the methodology for EP cases.
 |
Figure 1 Flowchart illustrating patient selection protocol. Abbreviations: MTX, Methotrexate; NLR, Neutrophil-to-Lymphocyte Ratio. |
Data Collection
We defined the day of MTX administration as day 0. Blood samples were collected on days 0, 4, and 7, stored in ethylenediaminetetraacetic acid (EDTA) tubes, and subsequently subjected to β-hCG and blood count tests. The variation in β-hCG levels between days 0 and 4 (β-hCG, days 0–4) was calculated using the formula (hCG4–hCG0)/hCG0. NLR, days 0–4 and PLR, days 0–4 were calculated using the same algorithm. Negative values were interpreted to indicate a decrease in βhCG levels, whereas positive values indicated an increase. Therapeutic success involved resolving tubal pregnancy (βhCG < 10IU/L) after just one MTX administration without the need for additional treatment. Treatment failure was determined if additional MTX or surgical intervention was required.
Statistical Analysis
Data were presented for nominal variables such as rates and proportions (%), while the χ2-test and Fisher’s Exact test were employed for group comparisons. For normally distributed continuous data, means plus or minus standard deviations (SD) were reported, with the Mann–Whitney U-test used for comparing groups. In contrast, non-normally distributed variables were shown with medians and interquartile ranges (IQR), with the Wilcoxon rank-sum test serving as the method for group comparisons. Binary logistic regression analysis was used to screen the independent risk factors for failure of single-dose methotrexate treatment of ectopic pregnancy. Binary logistic regression identified independent risk markers for treatment failure, with significant variables incorporated into a nomogram. ROC was used to assess model differentiation, calibration curves, and the Hosmer–Lemeshow (HL) test reflected model calibration, and decision curves were used to analyze clinical utility. Analysis executed with R 4.3.3 and Zstats 1.0. P < 0.05 (two-tailed) was deemed statistically significant.
Results
All 412 (100%) eligible cases were included, of whom 302 (73.3%) were efficiently treated, and 110 (26.7%) patients did not respond to the treatment. Table 1 presents the baseline qualities. There were no statistically significant distinctions in terms of age, BMI, gravidity, gestational age, current ART pregnancy, previous live births, prior ectopic pregnancy, or previous pelvic surgery (P = 0.626, P = 0.115, P = 0.800, P = 0.187, P = 0.271, P = 0.529 and P = 0.676, respectively) between the cohorts. However, the anexal mass diameter was significantly larger in failure group. Furthermore, Day 0 hCG, Day 4 hCG and Day 4 Lymphocytes were considerably higher in the failure group (P < 0.001, P < 0.001, and P = 0.008, respectively). There was no difference in Day 0 NLR, Day 0 PLR, Day 4 NLR and Day 4 PLR (P = 0.443, P = 0.729, P = 0.100, and P = 0.126, respectively). Considerable variation in β-hCG (days 0–4), NLR (days 0–4), PLR (days 0–4) were observed (P = 0.020, P = 0.031 and P = 0.037, respectively) (Table 2). To assess the predictive performance of the indicators in predicting treatment outcomes, ROC analysis was performed (Table 3). The discriminatory power of Day 0 hCG, Day 4 hCG, Day 4 Lymphocytes, β-hCG, days 0–4, NLR, days 0–4, PLR, days 0–4, and Diameter of adnexal mass parameters to predict methotrexate success, according to the ROC curve analysis and AUC values, and the cut-points are demonstrated in Table 3. These parameters were categorized into two groups according to the cutoff values. One-way regression analysis showed that Day 0 hCG > 342.25mIU/mL (odds ratio [OR] 2.77, 95% CI [1.74–4.40]), Day 4 hCG > 304.8mIU/mL ([OR] 2.81, 95% CI [1.73–4.57]), Day 4 Lymphocytes > 2.165× 109/L ([OR] 2.18, 95% CI [1.39–3.42]), β-hCG, days 0–4 increased by more than 35.7% ([OR] 1.79, 95% CI [1.14–2.80]), NLR, days 0–4 declined by less than 40.3% ([OR] 1.99, 95% CI [1.26–3.12]), and PLR, days 0–4 decreased by less than 23% ([OR] 0.51, 95% CI [0.32–0.82]) were connected with treatment failure (Table 4). The results of multivariate regression indicated that a reduction in NLR was less than 40.3% by day 4 compared to baseline (odds ratio [OR] 1.99, 95% confidence interval [CI] 1.26–3.12), elevated hCG on day 4 relative to day 0 (OR 1.79, 95% CI 1.14–2.80), initial hCG concentrations above 342.25 mIU/mL at day 0 (OR 2.77, 95% CI 1.74–4.40), and lymphocyte counts greater than 2.165 × 109/L on day 4 (OR 2.18, 95% CI 1.39–3.42) significantly correlated with treatment failure (Table 5).
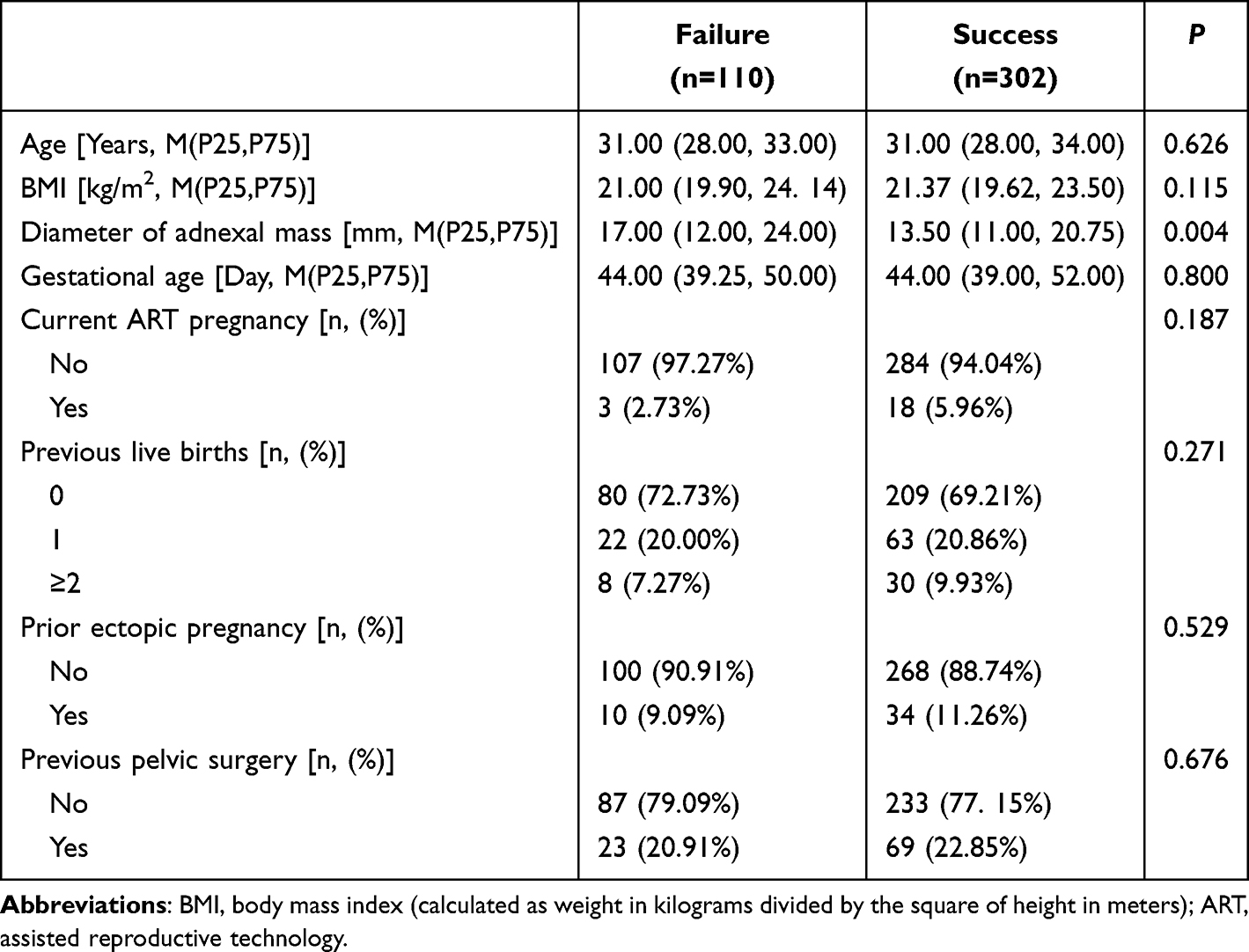 |
Table 1 Baseline Characteristics of Participants (N = 412) |
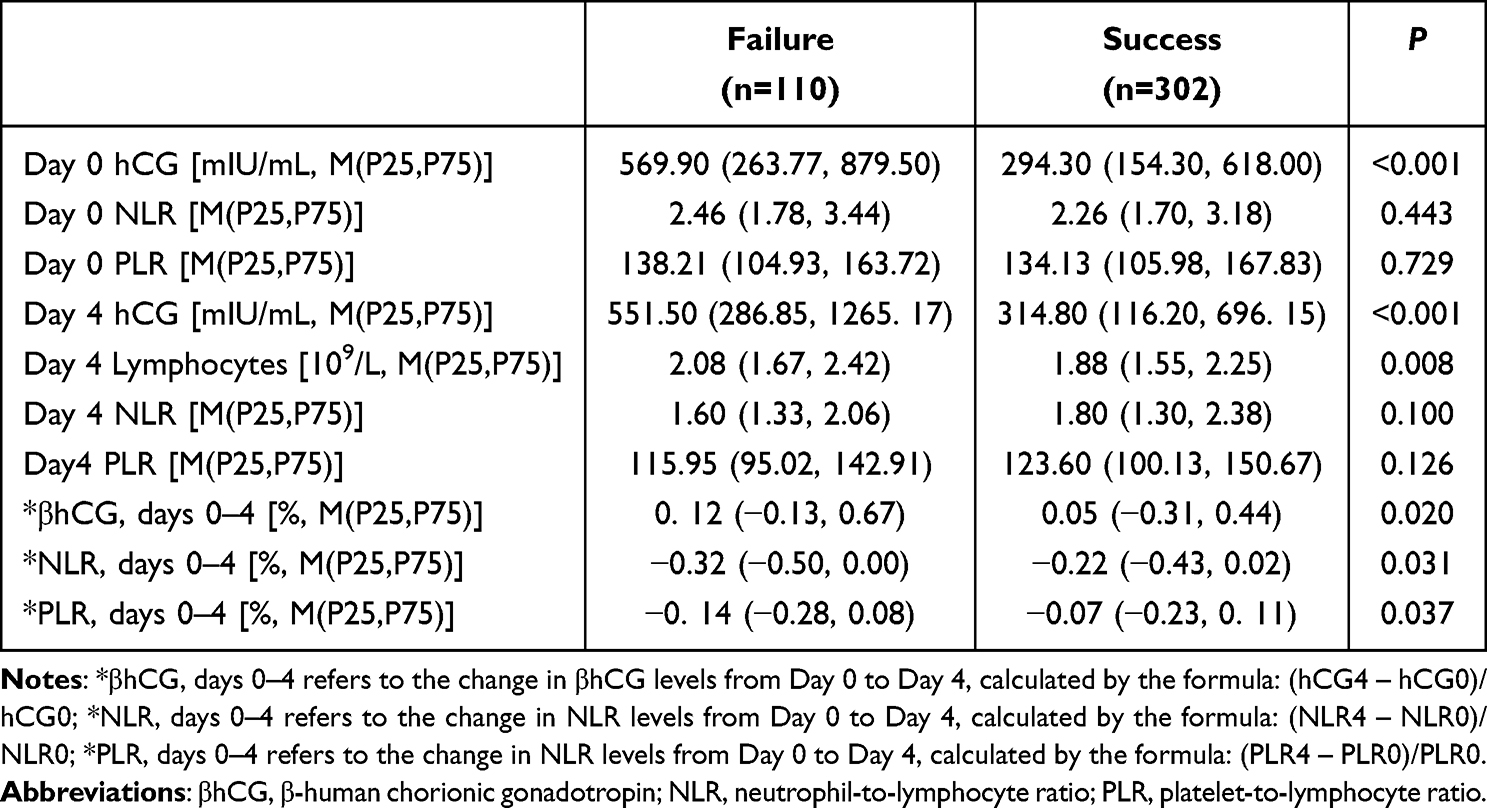 |
Table 2 Comparison of Hemogram Parameters, Hemogram-Derived Ratios, and β-hCG Level of Patients at Admission and Follow-Up Between Groups. (N = 412) |
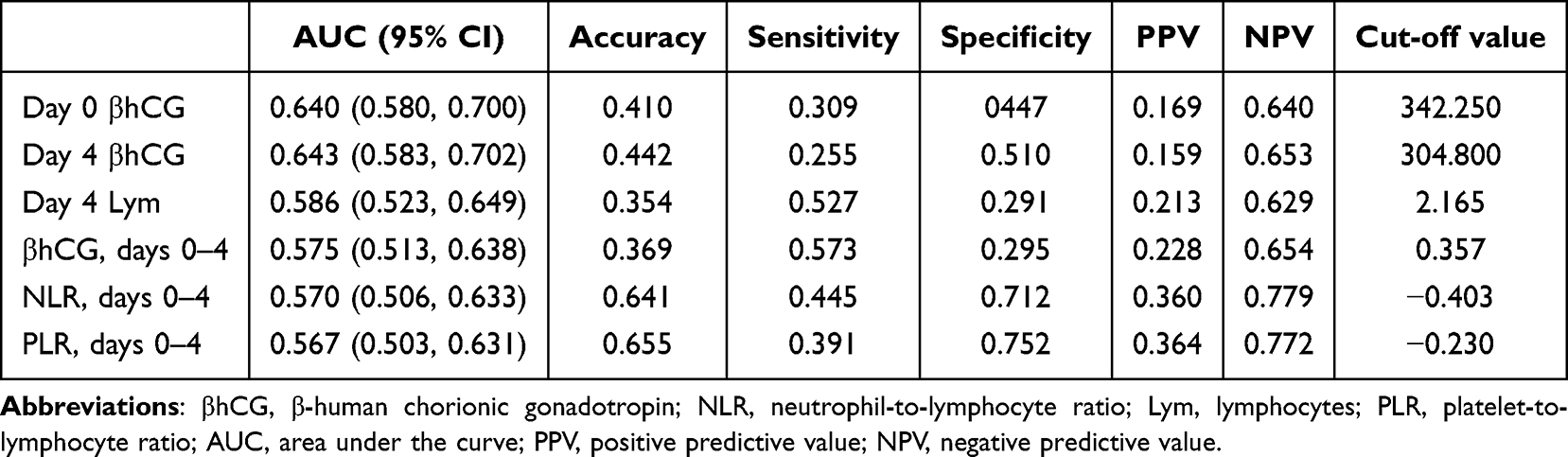 |
Table 3 Diagnostic Performance of Indicators in Predicting Single-Dose Methotrexate Treatment Failure |
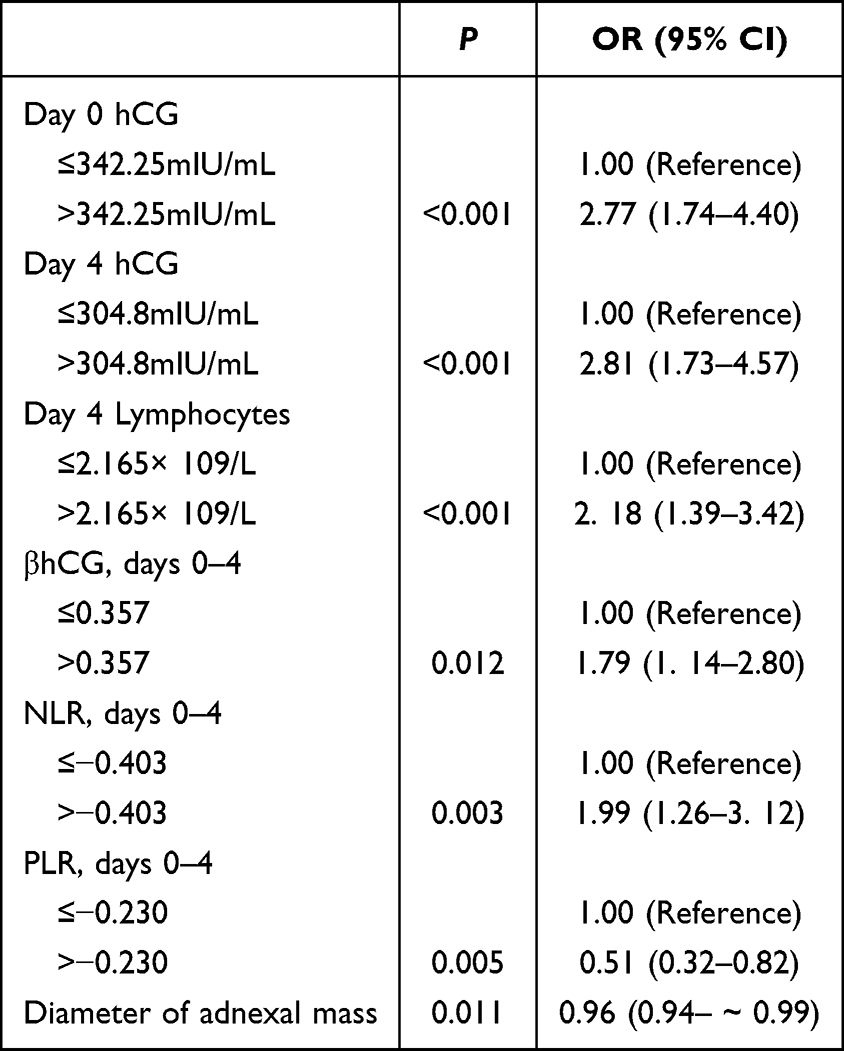 |
Table 4 Univariate Analysis to Explore the Role of Different Factors in Predicting the Efficacy of Single-Dose Methotrexate Administration |
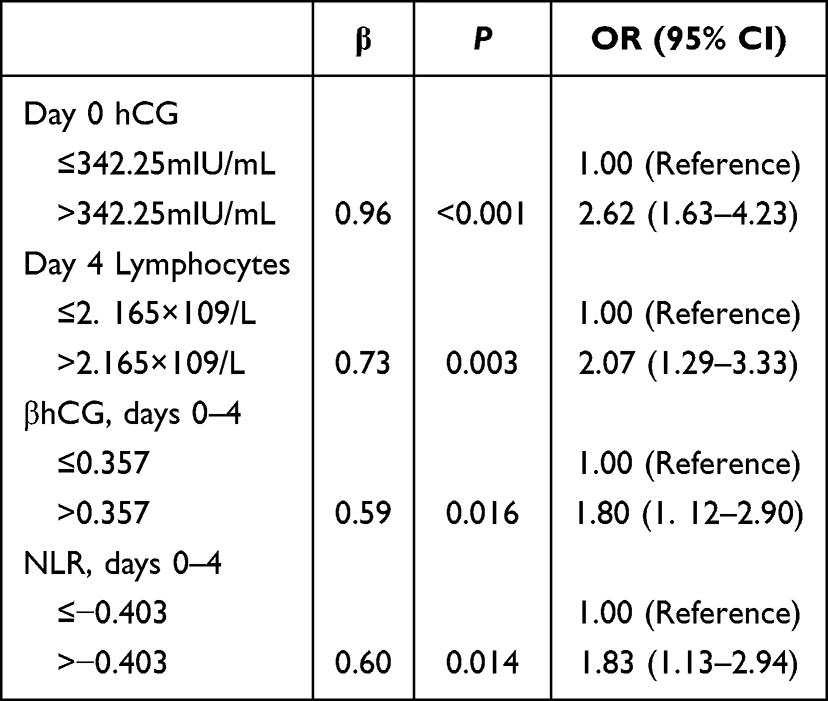 |
Table 5 Multivariate Analyses for Different Factors in Predicting Outcome of Single-Dose Methotrexate Administration |
Utilizing Day 0 hCG, Day 4 lymphocyte, β-hCG, days 0–4, NLR, days 0–4, to develop a predictive model. Scores were allocated to this model based on its variables, with their summation yielding the total (Figure 2). The ROC curve’s area is 0.705 (CI 95%: 0.650–0.760), with a sensitivity of 0.727 (CI 95%: 0.644–0.810) and a specificity of 0.619 (CI 95%: 0.564–0.674) (Figure 3). Figure S1 depicts the model’s calibration curve, with the HL-test indicating an appropriate fit (P = 0.607). The clinical decision curve, shown in Figure S2, shows some clinical benefit.
 |
Figure 2 Predictive nomogram of treatment outcomes for single-dose methotrexate for ectopic pregnancy. Abbreviations: β-hCG, days 0–4: the changes in β-hCG levels from day 0 to day 4; NLR, days 0–4: the changes in NLR levels from day 0 to day 4. |
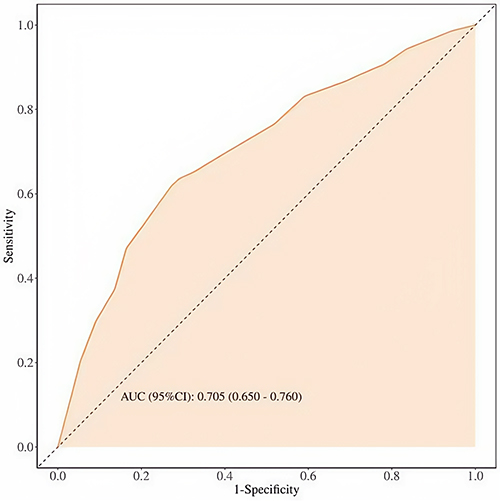 |
Figure 3 Receiver operating characteristic (ROC) curve for the ability of the nomogram to predict treatment outcome. Area under the curve (AUC): 0.705 (95% CI: 0.650–0.760). |
Discussion
Although the rate of single-dose MTX success in the treatment of asymptomatic EP is between 70% and 90%, considering that treatment failure may lead to life-threatening rupture of the ectopic mass and intra-abdominal hemorrhage, as well as provoking the patient’s anxiety and nervousness while waiting for the evaluation of the treatment effect. A recent meta-analysis has demonstrated the adverse long-term reproductive impacts of EP, including hypertensive disorders of pregnancy, placental abruption, subsequent ectopic pregnancy, and other related conditions.17 Therefore, we need to look for some other possible factors associated with treatment outcomes in the clinical setting. This study seeks to explore factors for treatment failure in cases with ectopic pregnancy receiving single-dose methotrexate and to build a model for predicting the failure risk. In an obstetrics and gynecology hospital in China, 412 single-dose methotrexate-treated ectopic pregnancies were retrospectively analyzed by collecting physical examination data and laboratory results. We found that a reduction in NLR of less than 40.3% by day 4 versus baseline, an increase in β-hCG by day 4 versus day 0, Day 0 β-hCG > 342.25mIU/mL, as well as Day 4 Lymphocytes > 2.165×109/L, were linked to failure outcome.
Research on methotrexate efficacy for ectopic pregnancy therapy is currently in progress.
Studies have shown that the reaction of multiple inflammatory cells has been detected in the systemic circulation of patients with ectopic pregnancy (EP).18 Neutrophils are the most abundant leukocyte within peripheral blood, accounting for approximately 40–70% of the total count, and are primarily associated with the body’s inflammatory response. Lymphocytes, which possess innate immune functions, play a crucial role in anti-infective immunity. The neutrophil-to-lymphocyte ratio (NLR) reflects systemic immune-inflammatory status and effectively assesses the balance of systemic inflammatory and immune regulation.19 Relevant studies indicate that compared to patients with unruptured ectopic pregnancies, those with ruptured tubal pregnancies exhibit significantly higher NLR levels. Furthermore, elevated NLR levels correlate with a higher risk of tubal rupture. Kanmaz et al reported NLR as a therapeutic success indicator, finding that 161 MTX-treated cases showed lower NLR at days 0, 4, and 7 versus those undergoing surgery20 However, changes in NLR were less successful in predicting success than a 15% reduction in hCG levels from days 4 to 7. Akkaya et al21 reported that in stable tubal ectopic pregnancies, patients treated with MTX exhibited significantly elevated RDW and MPV levels compared to those undergoing surgical intervention, while NLR levels were significantly reduced Sarıkaya et al compared to patients treated with MTX and those undergoing surgery, finding significantly elevated NLR and monocyte–lymphocyte ratio (MLR) in the surgical group Abuduxukuer et al22 found that a Day 4 NLR reduction under 23% from Day 0 levels correlated with a significantly declined of success rate. Our findings suggest that a reduction of NLR below 40.3% by Day 4 versus Day 0 correlates with MTX monotherapy failure. In previously developed predictive models, the cutoff values for NLR change and HCG change were −23% and 15%, respectively. This study generally aligns with these findings, though differences may stem from variations in the study populations.
In our study, β-hCG levels were also incorporated into the final predictive model. However, there remains no agreement regarding the specific β-hCG threshold at which methotrexate (MTX) treatment efficacy begins to decline. The current clinical success criterion is a β-hCG decrease exceeding 15% between days 4 and 7. This study suggests that a 35.7% increase in serum β-hCG levels on day 4 compared to baseline predicts treatment failure, necessitating consideration of repeat MTX therapy or surgical intervention. A prospective cohort study demonstrated that a serum β-hCG increase of <18% or any decrease from baseline to day 4 enhanced the success rate of single-dose MTX therapy.23 Soykan Sert et al found that the AUC for predicting the success of MTX treatment using serum β-hCG from baseline to day 4 was 0.832.24 Girija et al25 observed that a 10% HCG decline in HCG levels on day 4 predicted treatment success. Similarly, Wong et al26 observed that a 6% reduction on day 4 served as a treatment successful indicator. These findings collectively suggest that early changes in β-hCG levels may serve as an early predictor of treatment efficacy. This nomogram developed in this study demonstrates moderate predictive performance at day 4. Nevertheless, this study has certain limitations. Firstly, due to the nature of the retrospective study, our sample size was determined by the available clinical data; thus, the lack of formal sample size and power calculation constitutes one of the limitations of this study. Additionally, other limitations include the retrospective, single-center study design, potential residual confounding by unmeasured factors affecting inflammatory markers, and unavoidable selection bias. The nomogram developed in this study is hypothesis-generating with moderate discriminative performance and requires external validation as well as prospective, multicenter validation prior to routine clinical adoption. These metrics are derived from a complete blood count (CBC), offering an affordable and straightforward assessment without any extra costs. Currently, many hospitals only measure serum hCG levels. We recommend performing CBC tests simultaneously to assess NLR and lymphocyte levels. Inflammatory markers should be integrated as a complementary tool with classic predictive indicators such as adnexal mass size and β-hCG changes. Moreover, it is important to recognize that neutrophils and lymphocytes are non-specific markers, vulnerable to influence from various factors.
Data Sharing Statement
The data in this study are available on request from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The research protocol was approved by the Institutional Review Board of Shanghai First Maternity and Infant Hospital with a waiver of informed consent (Approval No. KS24275), as it involved retrospective data collection with patient identifiers anonymized and replaced by coded information to ensure strict confidentiality.
Author Contributions
Ruoxi Liu; Conceptualization, Data curation, Formal analysis, Writing-original draft, Writing – review and editing.
Shuangdi Li; Conceptualization, Writing – review and editing.
All authors contributed to this study. All authors read and approved the final paper All authors agreed on the journal to which the article has been submitted and agreed to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors have no conflicts of interest.
References
1. American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 191: tubal ectopic pregnancy. Obstet Gynecol. 2018;131(2):e65–9. doi:10.1097/AOG.0000000000002464
2. Al Naimi A, Moore P, Brüggmann D, Krysa L, Louwen F, Bahlmann F. Ectopic pregnancy: a single-center experience over ten years. Reprod Biol Endocrinol. 2021;19(1):79. doi:10.1186/s12958-021-00761-w
3. Saadati N, Najafian M, Masihi S, Safiary S, Abedi P. Comparison of two different protocols of methotrexate therapy in medical management of ectopic pregnancy. Iran Red Crescent Med J. 2015;17(12):e20147. doi:10.5812/ircmj.20147
4. Papageorgiou D, Sapantzoglou I, Prokopakis I, Zachariou E. Tubal ectopic pregnancy: from diagnosis to treatment. Biomedicines. 2025;13(6):1465. doi:10.3390/biomedicines13061465
5. Hu Y, Zhang W, Yao Z, Deng L, Guan Q, Wang X. Development and validation of a dynamic prediction model for single-dose methotrexate treatment success in tubal ectopic pregnancy: a multicentre cohort study in Chinese hospitals. BMJ Open. 2025;15(9):e092110. doi:10.1136/bmjopen-2024-092110
6. Scarpelli E, Capozzi VA, Roberto L, et al. Predictors of methotrexate success and fertility outcomes in tubal ectopic pregnancy: a retrospective cohort study. Med Kaunas Lith. 2025;61(6):1058. doi:10.3390/medicina61061058
7. Brunello J, Guerby P, Cartoux C, et al. Can early βhCG change and baseline progesterone level predict treatment outcome in patients receiving single dose methotrexate protocol for tubal ectopic pregnancy? Arch Gynecol Obstet. 2019;299(3):741–745. doi:10.1007/s00404-019-05068-1
8. Du X, Chen Q, Lu M, et al. An individualized risk prediction tool for ectopic pregnancy within the first 10 weeks of gestation based on machine learning algorithms. Front Med. 2025;12:1726606. doi:10.3389/fmed.2025.1726606
9. Zhao X, Wu T, Zeng S, et al. Development and validation of a machine learning–based clinical model for predicting rupture in ectopic pregnancy: a web-based nomogram approach. J Multidiscip Healthc. 2025;18:5781–5799. doi:10.2147/JMDH.S536476
10. Aghayari A, Sorayaie Azar A, Taheri-Anganeh M, et al. Prediction of ectopic pregnancy using interpretable machine learning algorithms. BMC Pregnancy Childbirth. 2025;25(1):1119. doi:10.1186/s12884-025-08179-7
11. Zhang M, Sheng J. The application of super-resolution ultrasound radiomics models in predicting the failure of conservative treatment for ectopic pregnancy. Reprod Biol Endocrinol RBE. 2025;23(1):102. doi:10.1186/s12958-025-01437-5
12. Jung YJ, Zhang H-S, Lee EJ, et al. The development of an ultrasound-based scoring system for the prediction of interstitial pregnancy. J Clin Med. 2025;14(12):4238. doi:10.3390/jcm14124238
13. Kunicki M, Rzewuska N, Gross-Kępińska K. Immunophenotypic profiles and inflammatory markers in premature ovarian insufficiency. J Reprod Immunol. 2024;164:104253. doi:10.1016/j.jri.2024.104253
14. Kirsch-Mangu AT, Țîpcu A, Gâta VA, et al. Neutrophil to lymphocyte ratio a prognostic tool in endometrial cancer among classical prognostic factors. Diagn Basel Switz. 2025;15(17):2172. doi:10.3390/diagnostics15172172
15. Zhang Z, Lang J. The prognostic and clinical value of neutrophil-to-lymphocyte ratio (NLR) in ovarian cancer: a systematic review and meta-analysis. J Med Biochem. 2024;43(4):323–333. doi:10.5937/jomb0-46035
16. Gorun OM, Ratiu A, Citu C, et al. The role of inflammatory markers NLR and PLR in predicting pelvic pain in endometriosis. J Clin Med. 2024;14(1):149. doi:10.3390/jcm14010149
17. Papageorgiou D, Sapantzoglou I, Zachariou E, Antsaklis P, Daskalakis G, Pergialiotis V. Impact of ectopic pregnancy on the outcomes of the subsequent pregnancy: a systematic review and meta-analysis. J Clin Med. 2025;14(12):4112. doi:10.3390/jcm14124112
18. Bilir C, Soysal C, Bıyık İ, et al. The relationship between hemogram based inflammatory indices and prognosis in ectopic pregnancy cases treated with methotrexate. Sci Rep. 2025;15(1):23114. doi:10.1038/s41598-025-09149-x
19. Mollinedo F. Neutrophil degranulation, plasticity, and cancer metastasis. Trends Immunol. 2019;40(3):228–242. doi:10.1016/j.it.2019.01.006
20. Kanmaz AG, Inan AH, Beyan E, Budak A. Role of various complete blood count parameters in predicting the success of single-dose methotrexate in treating ectopic pregnancy. Pak J Med Sci. 2018;34(5):1132–1136. doi:10.12669/pjms.345.15356
21. Akkaya H, Uysal G. Can hematologic parameters predict treatment of ectopic pregnancy? Pak J Med Sci. 2017;33(4):937–942. doi:10.12669/pjms.334.12418
22. Abuduxukuer R, Chen X, Ni J, Li S, Lu W. Day 4 and day 0 neutrophil-to-lymphocyte ratios as predictors of treatment failure with single-dose methotrexate for ectopic pregnancies. Int J Gynaecol Obstet off Organ Int Fed Gynaecol Obstet. 2024;165(1):131–137. doi:10.1002/ijgo.15248
23. Mackenzie SC, Moakes CA, Doust AM, et al. Early (days 1–4) post-treatment serum hCG level changes predict single-dose methotrexate treatment success in tubal ectopic pregnancy. Hum Reprod. 2023;38(7):1261–1267. doi:10.1093/humrep/dead089
24. Soykan Sert Z, Bertizlioğlu M. The role of inflammatory markers and βhCG levels in predicting the success of single-dose methotrexate treatment in tubal ectopic pregnancy. Int J Gynaecol Obstet off Organ Int Fed Gynaecol Obstet. 2025;169(2):639–644. doi:10.1002/ijgo.16084
25. Girija S, Manjunath AP, Salahudin A, et al. Role of day 4 HCG as an early predictor of success after methotrexate therapy for ectopic pregnancies. Eur J Obstet Gynecol Reprod Biol. 2017;215:230–233. doi:10.1016/j.ejogrb.2017.06.020
26. Wong L, Fung LWY, Cheung C-W, Lao TT. Trends in serum human chorionic gonadotropin levels 0–4 days after methotrexate administration for predicting tubal ectopic pregnancy treatment success. Int J Gynaecol Obstet off Organ Int Fed Gynaecol Obstet. 2018;141(2):245–249. doi:10.1002/ijgo.12419
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Comparative Analysis of Neutrophil-to-Lymphocyte Ratio, Systemic Immune-Inflammation Index, and Hemoglobin-Albumin-Lymphocyte-Platelet Score in Migraine
Öztürk P, Aktan Ç
Journal of Inflammation Research 2026, 19:625473
Published Date: 10 July 2026