Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
ZJU Index as a Predictive Tool for Diabetes Incidence: Insights from a Population-Based Cohort Study
Authors Wu C, Loh YH ![]() , Huang H, Xu C
, Huang H, Xu C
Received 17 November 2023
Accepted for publication 30 January 2024
Published 12 February 2024 Volume 2024:17 Pages 715—724
DOI https://doi.org/10.2147/DMSO.S446042
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Chenjiao Wu,1,* Yi Hao Loh,2,* Hangkai Huang,3 Chengfu Xu3
1Department of Nursing, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, People’s Republic of China; 2Medical Bachelor and Bachelor of Surgery (MBBS), Zhejiang University School of Medicine, Hangzhou, 310003, People’s Republic of China; 3Department of Gastroenterology, Zhejiang Provincial Clinical Research Centre for Digestive Diseases, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chengfu Xu, Department of Gastroenterology, the First Affiliated Hospital, Zhejiang University School of Medicine, No. 79 Qingchun Road, Hangzhou, 310003, People’s Republic of China, Tel +86-571-87236863, Email [email protected]
Background: In previous studies, the ZJU index was reported to be a superior predictor of nonalcoholic fatty liver disease in the Chinese population compared to the Fatty Liver Index. However, whether the ZJU Index is significantly associated with diabetes among Asian populations has not been determined.
Methods: The NAGALA study was carried out at Murakami Memorial Hospital (Gifu, Japan) beginning in 1994. This study included the data of the subjects who underwent health check-ups from 2004 to 2015. The ZJU Index comprises body mass index (BMI), fasting plasma glucose, triglyceride, and alanine aminotransferase-to-aspartate aminotransferase (ALT) levels and an adjustment point for females. We conducted Cox proportional hazard regression to evaluate the association between quartiles of the ZJU Index and the risk of incident diabetes.
Participants: A total of 15,464 individuals who underwent health check-ups were included in this study.
Results: A total of 373 cases of incident diabetes were documented during 93,350 person-years of follow-up. As the ZJU index increased, the incidence of diabetes gradually increased (P < 0.001). According to the multivariable model adjusted for metabolic covariates, the fourth quartile of the ZJU Index was positively associated with the risk of diabetes compared to the first quartile (HR=2.519, 95% CI=1.297− 4.891). Subgroup analysis revealed that the association between the ZJU index and diabetes risk was significant in subjects aged younger than 40 years (HR=3.327, 95% CI=1.544− 7.171), in females (HR=4.480, 95% CI=1.302− 15.419), in individuals with a BMI< 25 kg/m2 (HR=3.812, 95% CI=1.992− 7.293) and in individuals with a nonregular exercise (HR=2.479, 95% CI=1.193− 5.152).
Conclusion: We observed a positive association between the ZJU Index and incident diabetes in the general population.
Keywords: ZJU index, diabetes, epidemiology
Introduction
Diabetes mellitus (DM) is commonly defined as a group of metabolic disorders characterized by chronic hyperglycemia.1 The burden of diabetes is currently expanding at an alarming rate, with projected increases in incidence, prevalence, mortality, and disability-adjusted life years from 2018 to 2025.2 According to estimates from the International Diabetes Federation Diabetes Atlas, it is estimated that the number of individuals with diabetes will reach 693 million by 2045, with more than 90% of diabetes cases comprising type 2 diabetes mellitus (T2DM).3 Notably, Asia accommodates more than 60% of diabetic individuals, and this prevalence is closely associated with aging, urbanization, and lifestyle changes.4 Renowned for its detrimental impact on individuals’ well-being, national economies, and healthcare systems, diabetes remains one of the most significant global health challenges of the 21st century.
In contrast to type 1 diabetes mellitus (T1DM), which is associated with autoimmune conditions,5 the etiology of T2DM involves multiple factors, including both nonmodifiable and modifiable risk factors.6 A positive family history, sex, ethnicity (such as Asian, Hispanic, or Black American), obesity status, and lifestyle factors (such as physical activity, alcohol consumption, sleep duration, and dietary habits) are recognized etiological factors for diabetes. In particular, various studies have demonstrated a higher incidence of fatty liver in individuals with T2DM.7 Patients with nonalcoholic fatty liver disease (NAFLD) were also found to have an increased risk of developing T2DM;8–10 hence, some researchers suggest a bidirectional relationship between these two metabolic disorders.11 Several scholars also argue that the term “metabolic-associated fatty liver disease (MAFLD)” should be used instead of NAFLD.12 NAFLD is defined by the presence of steatosis in more than 5% of hepatocytes, with little or no alcohol consumption.13 Pathogenically, the association between these two diseases involves insulin resistance, impaired triglyceride metabolism, immune responses, and subsequent hyperinsulinemia caused by β-cell dysfunction in T2DM patients.14
Among the commonly used NAFLD predictors, the fatty liver index (FLI) and ZJU index are models that do not directly include the presence of diabetes mellitus.15,16 A myriad of studies provide evidence that the severity of NAFLD, assessed by the FLI, predicts the development of diabetes.17–19 However, the FLI was initially developed and validated in Western populations, raising concerns about its accuracy in assessing NAFLD among the Asian population.20 A previous study conducted by our team revealed that the ZJU Index, which comprises four independent risk factors for NAFLD, namely, body mass index (BMI), fasting plasma glucose, triglyceride, and the alanine aminotransferase-to-aspartate aminotransferase ratio, and an adjustment point for females, is a superior predictor of NAFLD in the Chinese population compared to the FLI.21 This raises the following question: can the ZJU Index be considered a novel model for investigating the association between NAFLD and the onset of diabetes? To date, no research has explored the link between the ZJU Index and the occurrence of diabetes, suggesting that this topic is worthy of in-depth investigation.
In summary, there is a need for comprehensive research on the relationship between the ZJU Index and incident diabetes, including the specific predictive accuracy of the ZJU Index for diabetes and any variations observed in different populations. Therefore, this study aimed to thoroughly assess the relationship between the ZJU Index and incident diabetes in a large cohort of Asian adults.
Methods
Study Cohort
The present study retrieved data from the NAGALA study, which was carried out at Murakami Memorial Hospital (Gifu, Japan) beginning in 1994. This study included the data of the subjects who underwent health check-ups from 2004 to 2015. This study enrolled 15,464 individuals who underwent health checkups based on the following exclusion criteria: (i) were taking medications at baseline, (ii) had diabetes or impaired fasting glucose at baseline, and (iii) had incomplete covariate data. The NAGALA study was approved by the Murakami Memorial Hospital Institutional Ethics Review Board (IRB2018-09-01), and all participants provided informed consent.
Data Collection
Participants responded to questionnaires about their medical history and lifestyles. Alcohol intake per week was calculated based on the quantity and type of alcohol consumed in the last month. The definition of alcohol consumption was alcohol intake greater than 40 g per week.22 A regular physical exerciser was defined as an individual who participated in any type of activity more than once a week. For smoking status, the participants were categorized into three groups: never, ex or current. Individuals who had never smoked were defined as nonsmokers; ex-smokers, participants who had smoked cigarettes in the past but quit smoking until baseline; and current smokers, participants who smoked at the baseline visit. Experienced nurses were responsible for the measurement of standing height, body weight and blood pressure. After an overnight fast, venous samples were collected for laboratory tests. The diagnostic criteria for diabetes mellitus were fasting plasma glucose ≥7 mmol/L, HbA1c ≥6.5% or a self-reported history of diabetes. NAFLD was defined as the presence of fatty liver without other causes of chronic liver disease, including hepatitis B or hepatitis C infection or genetic, autoimmune or drug-induced liver disease. The ultrasonographic presentation of fatty liver included liver and kidney echo contrast, deep liver attenuation, liver brightness and vessel blurring. The ZJU index was calculated using the following formula:15
ZJU Index = BMI (kg/m2) + fasting plasma glucose (mmol/L) + triglyceride (mmol/L) + 3 × alanine aminotransferase (IU/L)/aspartate aminotransferase (IU/L) ratio (+2, if female).
Statistical Analyses
The data are presented as medians (interquartile ranges) due to skewed distributions or as proportions. Participants were stratified into four groups based on the quartile of the ZJU Index. To compare the clinical features among groups, one-way ANOVA and the chi-square test were used. After stratification, we conducted Cox proportional hazard regression to evaluate the association between quartiles of the ZJU Index and the risk of incident diabetes. We subsequently conducted Cox proportional hazard regression to evaluate the association between quartiles of the ZJU Index and the risk of incident diabetes. The proportional hazard hypothesis was tested. The covariates adjusted in Model 1 were age and sex. In Model 2, additional covariates were included: BMI, systolic blood pressure, diastolic blood pressure, smoking status, alcohol intake, physical activity, high-density lipoprotein-cholesterol, triglycerides and glycated hemoglobin A1c. Additionally, we performed subgroup analyses based on age, sex, BMI, physical activity and NAFLD status to further test the interactive effects of these conditions on the association between the ZJU Index and diabetes risk. K‒M curves displaying the cumulative incidence of diabetes stratified by the ZJU index were generated, and the Log rank test was used to compare the differences among groups. All the statistical analyses were performed using SPSS 26.0 software (SPSS, Inc., Chicago, IL). P <0.05 (2-tailed test) was considered to indicate statistical significance.
Results
Baseline Characteristics
Table 1 shows the clinical characteristics of the participants stratified by quartiles of the ZJU index. With increasing ZJU index, participants exhibited elevated proportions of drinkers and smokers, along with higher BMIs; blood pressure; total cholesterol; triglycerides; plasma glucose; and glycated hemoglobin A1c. Conversely, HDL-C levels decreased as the ZJU index increased.
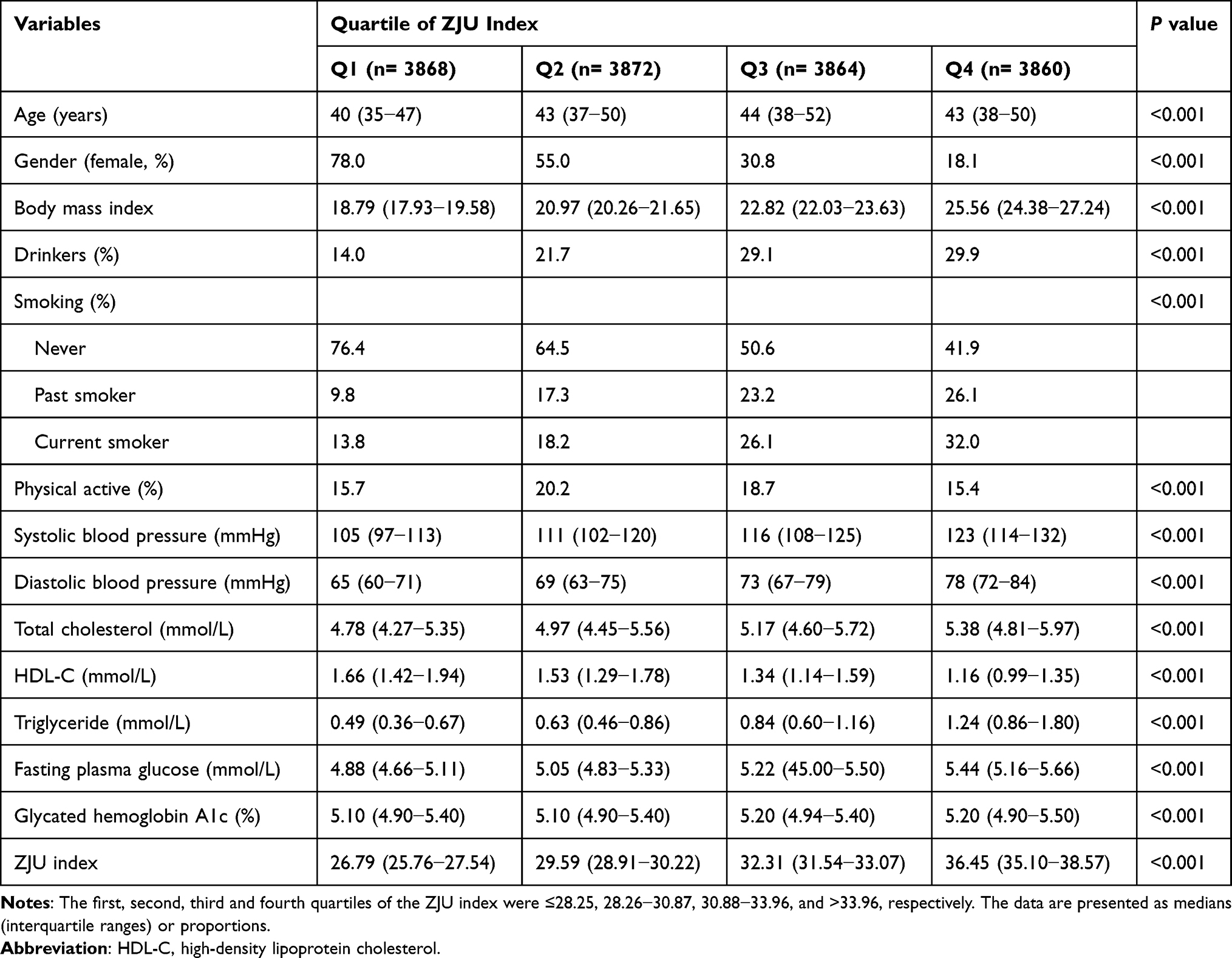 |
Table 1 Baseline Characteristics of the Study Population |
Association Between the ZJU Index and Incident Diabetes
A total of 373 cases of incident diabetes were documented during 93,350 person-years of follow-up (Table 2). The median follow-up duration to onset of diabetes was 5.9 years in this study. There was a clear positive correlation between the ZJU Index and the incidence of diabetes. According to the univariate model, the risk of diabetes development increased gradually with increasing age from the first quartile to the second, third and fourth quartiles. According to the multivariable-adjusted model, accounting for only age and sex, the ZJU index was positively correlated with diabetes risk. Although the association attenuated after adjusting for multiple potential confounders in the same multivariate analysis, compared with the first quartile, the fourth quartile of the ZJU Index continued to show a positive association with the risk of diabetes (HR: 2.519, 95% CI: 1.297−4.891). K‒M curves showed that the cumulative hazard ratio (HR) of diabetes was significantly greater in individuals with a higher ZJU index (Log rank test P <0.001) (Figure 1).
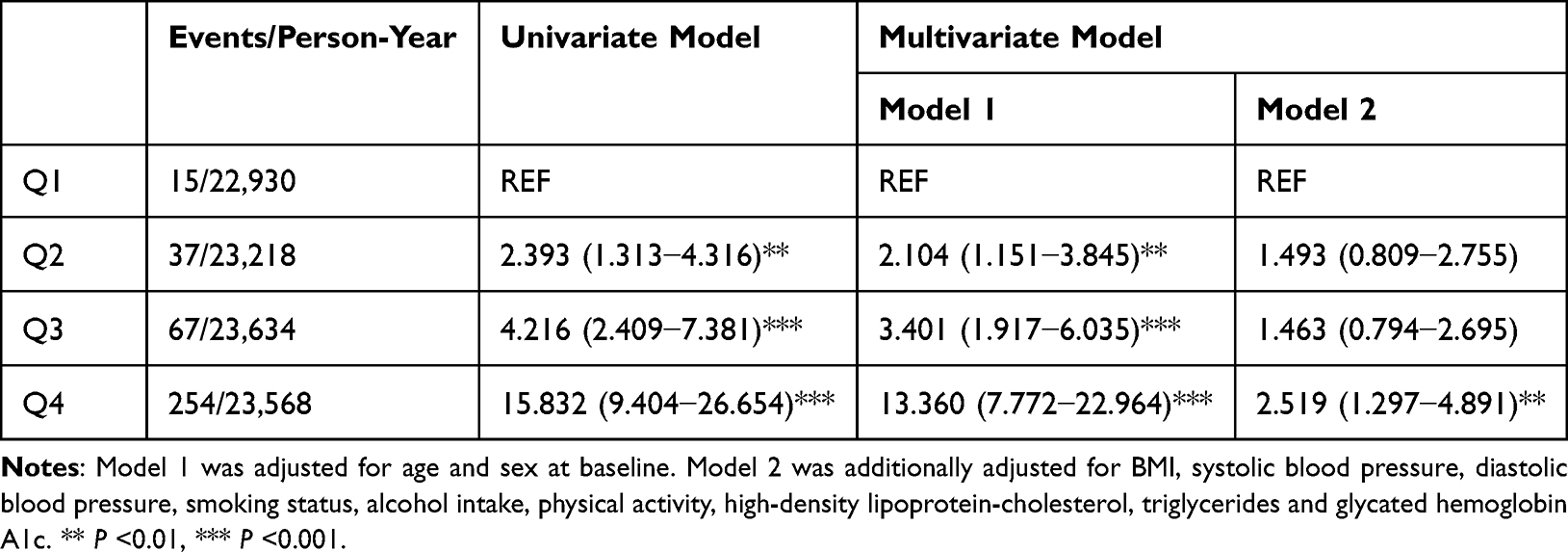 |
Table 2 Hazard Ratios for Diabetes Based on Quartiles of the ZJU Index at Baseline |
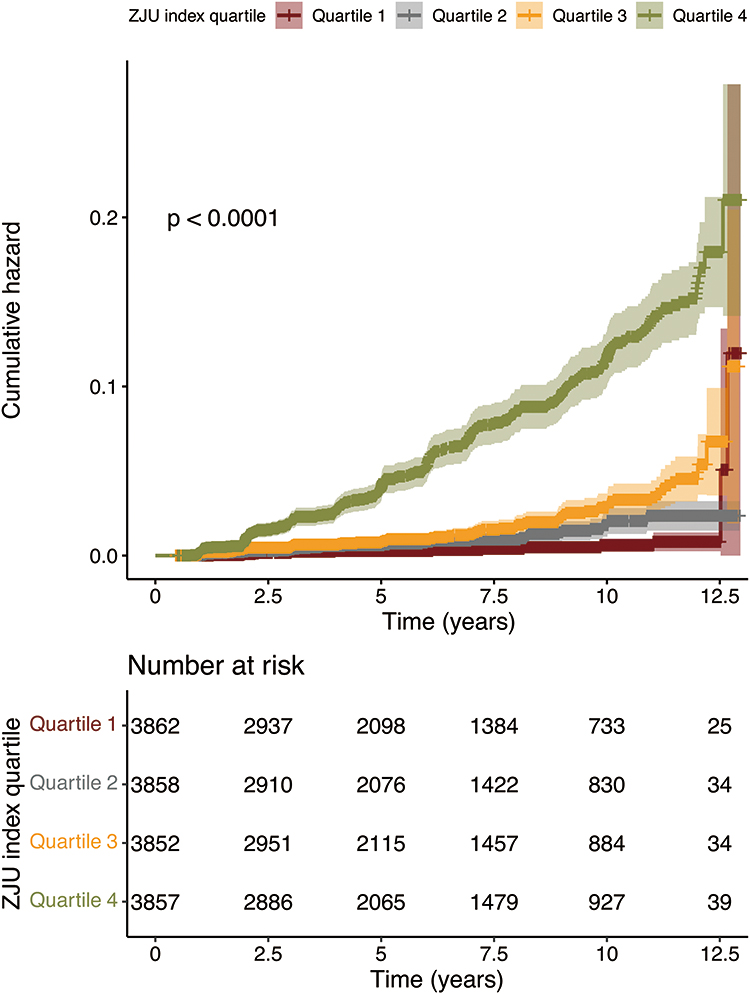 |
Figure 1 K‒M curves of participants according to the quartile of the ZJU index. |
Subgroup Analyses
According to our subgroup analyses (Table 3), the ZJU index-associated risk of diabetes remained significant for individuals aged younger than 40 years (HR=3.327, 95% CI=1.544−7.171), females (HR=4.480, 95% CI=1.302−15.419), individuals with a BMI<25 kg/m2 (HR=3.812, 95% CI=1.992−7.293) and nonregular exercisers (HR=2.479, 95% CI=1.193−5.152). These associations also did not differ due to the presence of NAFLD. None of these conditions significantly disrupted the association between the ZJU Index and diabetes incidence.
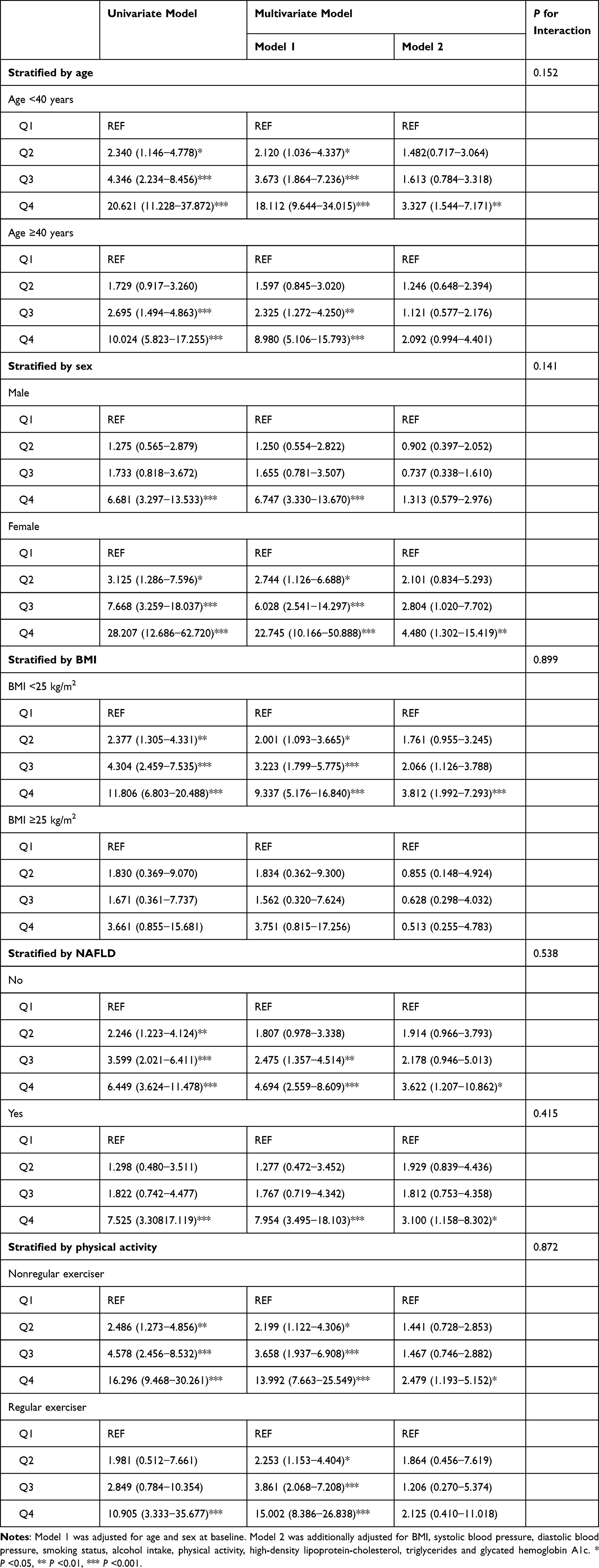 |
Table 3 Subgroup Analyses of the Association Between the ZJU Index and Risk of Incident Diabetes |
Discussion
The use of a noninvasive scoring system to predict the incidence of diabetes has been attempted by various authorities.23,24 Nevertheless, recent studies have unequivocally established a strong association between diabetes and NAFLD.25 NAFLD patients have been shown to exhibit a twofold greater risk of acquiring diabetes, regardless of obesity or other prevalent metabolic risk factors.8 In terms of outcomes, individuals with cooccurring DM and NAFLD are susceptible to cardiovascular and liver-related consequences, as are those with the most advanced stages of liver disease.26,27 Hence, predicting the incidence of diabetes, especially in a population possibly accompanied by NAFLD, is of paramount clinical significance.
In this study, we proposed the use of the ZJU index as a predictive marker of diabetes occurrence in patients with varying risks of NAFLD. Intriguingly, our findings revealed a positive association between the ZJU Index and T2DM incidence, even after we controlled for other variables. To further understand the correlation and trend of the ZJU index and incidence of diabetes, we conducted a subgroup analysis stratified by age, sex, BMI, NAFLD incidence and physical activity. The consistent results among the different groups with distinct stratification variables underscored the equally robust association between the ZJU index and diabetes incidence. Lifestyle factors affect the risk of developing diabetes.28 Previous studies have shown that smoking not only increases the risk of diabetes but also increases the risk of mortality and diabetic complications in patients with diabetes.29 More frequent alcohol intake lowers the risk of diabetes30, while heavy drinking is reported to increase diabetes risk.31
To determine the presence of NAFLD in the Chinese population, our team developed the “ZJU Index” in 2015, with the aim of providing an alternative to ultrasonography and screening patients indicated for CT and MRI.18 Compared with the Fatty Liver Index (FLI), the ZJU Index offers a comparable level of simplicity, as all its components are easily accessible, and it outperforms the FLI in predicting NAFLD incidence. The exclusion of waist circumference from the ZJU Index has been demonstrated to contribute to its independence across different races and ethnicities,32,33 whereas the addition of fasting plasma glucose values to the model fosters a closer relationship between NAFLD and T2DM.34 In this study, we demonstrated the effectiveness of the ZJU index in predicting the occurrence of diabetes in patients susceptible to NAFLD.
Both the univariate and multivariate Cox proportional hazard models demonstrated that the ZJU index is reliably associated with an increased incidence of diabetes. According to our stratified model, our study further revealed that the ZJU index was indisputably correlated with NAFLD and diabetes incidence, regardless of age, sex, BMI, NAFLD status and physical activity. K‒M analysis further revealed that patients in higher quartiles of the ZJU Index had a greater cumulative risk of developing diabetes over time. The significant difference in diabetes incidence among all four quartiles of the ZJU Index was demonstrated by a p value of <0.01 according to the Log rank test.
The ZJU index allows early identification of people at risk for T2DM, which is important for patients prone to NAFLD to make lifestyle changes or start treatment earlier. This could help to prevent or delay the onset of T2DM, which would have a significant impact on their health and well-being. In addition, the NRS-2002 can serve as a screening tool for both NAFLD and T2DM, thereby reducing unnecessary tests and procedures.
Our study has several strengths. First, the “DATADRYAD” database utilized in this retrospective study can provide a relatively large sample size that yields more robust estimates and enhances the generalizability of the findings. The database contains data from a Japanese population, which provides valuable insights for investigating the hypothesis that the ZJU Index is more well adapted for the Asian population. Second, we rigorously adjusted for statistical baselines to ensure the reliability of the results. Third, to ensure the validity of the findings, we performed subgroup analyses between the ZJU Index and incident diabetes incidence to enhance the understanding of potential effect modifications by different factors. Furthermore, the use of Kaplan‒Meier curves and cumulative hazard functions facilitates a clear and comprehensive visualization of survival probabilities and the cumulative risk of diabetes incidence over time.
Nonetheless, there are several limitations in our study. As a retrospective observational analysis, this study can demonstrate only an association inference rather than establish a causal relationship between the ZJU Index and the risk of diabetes. Moreover, although the utilization of Japanese data solidifies our finding that the ZJU index can predict the incidence of NAFLD and DM in the Asian population, further research is needed to validate its generalizability. Finally, in our model, the ZJU index can predict the risk of diabetes incidence but cannot be used to evaluate the outcome or prognosis of diabetes patients. Consequently, the efficiency and accuracy of the ZJU Index in this respect should be interpreted and investigated.
Through this study, we found a compelling positive association between the ZJU Index and incident diabetes in the Asian population. These findings can prompt early attention to the occurrence of diabetes in NAFLD patients and vice versa, facilitating timely implementation of therapeutic approaches. However, additional evidence must be gathered to validate the versatility of the ZJU index across diverse populations.
Strengths and Limitations of This Study
The strengths of this study include its longitudinal population-based design.
According to our model, the ZJU index can predict the risk of diabetes incidence but cannot be used to evaluate the outcome or prognosis of diabetes patients.
Data Sharing Statement
The data presented in this study are available upon request from the corresponding author.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Murakami Memorial Hospital Institutional Ethics Review Board (IRB2018-09-01). This study was a secondary analysis of NAGALA study and was exempt from approval.
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study involving anonymised data analysis only.
Acknowledgments
Special thanks to Fukui et al for sharing the available data from the NAGALA study.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2013;36 Suppl 1(Suppl 1):S67–S74. doi:10.2337/dc13-S067
2. Lin X, Xu Y, Pan X, et al. Global, regional, and national burden and trend of diabetes in 195 countries and territories: an analysis from 1990 to 2025. Sci Rep. 2020;10(1):14790. doi:10.1038/s41598-020-71908-9
3. Cho NH, Shaw JE, Karuranga S, et al. IDF Diabetes Atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabet Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
4. Nanditha A, Ma RCW, Ramachandran A, et al. Diabetes in Asia and the Pacific: implications for the Global Epidemic. Diabetes Care. 2016;39(3):472–485. doi:10.2337/dc15-1536
5. Atkinson MA, Eisenbarth GS, Michels AW. Type 1 diabetes. Lancet. 2014;383(9911):69–82. doi:10.1016/S0140-6736(13)60591-7
6. Galicia-Garcia U, Benito-Vicente A, Jebari S, et al. Pathophysiology of Type 2 Diabetes Mellitus. Int J Mol Sci. 2020;21(17). doi:10.3390/ijms21176275
7. Bhatt HB, Smith RJ. Fatty liver disease in diabetes mellitus. Hepatobiliary Surg Nutr. 2015;4(2):101–108. doi:10.3978/j.issn.2304-3881.2015.01.03
8. Targher G, Corey KE, Byrne CD, Roden M. The complex link between NAFLD and type 2 diabetes mellitus - mechanisms and treatments. Nat Rev Gastroenterol Hepatol. 2021;18(9):599–612. doi:10.1038/s41575-021-00448-y
9. Kasturiratne A, Weerasinghe S, Dassanayake AS, et al. Influence of nonalcoholic fatty liver disease on the development of diabetes mellitus. J Gastroenterol Hepatol. 2013;28(1):142–147. doi:10.1111/j.1440-1746.2012.07264.x
10. Mantovani A, Petracca G, Beatrice G, Tilg H, Byrne CD, Targher G. Nonalcoholic fatty liver disease and risk of incident diabetes mellitus: an updated meta-analysis of 501 022 adult individuals. Gut. 2021;70(5):962–969. doi:10.1136/gutjnl-2020-322572
11. Li Y, Wang J, Tang Y, et al. Bidirectional association between nonalcoholic fatty liver disease and type 2 diabetes in Chinese population: evidence from the Dongfeng-Tongji cohort study. PLoS One. 2017;12(3):e0174291. doi:10.1371/journal.pone.0174291
12. Eslam M, Newsome PN, Sarin SK, et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73(1):202–209. doi:10.1016/j.jhep.2020.03.039
13. American Diabetes Association. EASL-EASD-EASO Clinical Practice Guidelines for the management of nonalcoholic fatty liver disease. J Hepatol. 2016;64(6):1388–1402. doi:10.1016/j.jhep.2015.11.004
14. Buzzetti E, Pinzani M, Tsochatzis EA. The multiple-hit pathogenesis of nonalcoholic fatty liver disease (NAFLD). Metabolism. 2016;65(8):1038–1048. doi:10.1016/j.metabol.2015.12.012
15. Wang J, Ma L, Chen S, et al. Risk for the development of nonalcoholic fatty liver disease: a prospective study. J Gastroenterol Hepatol. 2018;33(8):1518–1523. doi:10.1111/jgh.14105
16. Bedogni G, Bellentani S, Miglioli L, et al. The Fatty Liver Index: a simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006;6(33):567.
17. Higashiura Y, Furuhashi M, Tanaka M, et al. High level of fatty liver index predicts new onset of diabetes mellitus during a 10-year period in healthy subjects. Sci Rep. 2021;11(1):12830. doi:10.1038/s41598-021-92292-y
18. Zhu Y, Hu H, Wu Y, et al. The association between fatty liver index and onset of diabetes: secondary analysis of a population-based cohort study. BMC Public Health. 2023;23(1):679. doi:10.1186/s12889-023-15442-z
19. Seo I-H, Lee HS, Lee Y-J. Fatty liver index as a predictor for incident type 2 diabetes in community-dwelling adults: longitudinal findings over 12 years. Cardiovasc Diabetol. 2022;21(1):209. doi:10.1186/s12933-022-01642-1
20. Cho E-J, Jung G-C, Kwak M-S, et al. Fatty Liver Index for Predicting Nonalcoholic Fatty Liver Disease in an Asymptomatic Korean Population. Diagnostics. 2021;11(12):46.
21. Wang J, Xu C, Xun Y, et al. ZJU index: a novel model for predicting nonalcoholic fatty liver disease in a Chinese population. Sci Rep. 2015;5(16494). doi:10.1038/srep16494
22. Hashimoto Y, Hamaguchi M, Kojima T, et al. Modest alcohol consumption reduces the incidence of fatty liver in men: a population-based large-scale cohort study. J Gastroenterol Hepatol. 2015;30(3):546–552. doi:10.1111/jgh.12786
23. Wedekind LE, Mahajan A, Hsueh W-C, et al. The utility of a type 2 diabetes polygenic score in addition to clinical variables for prediction of type 2 diabetes incidence in birth, youth and adult cohorts in an Indigenous study population. Diabetologia. 2023;66(5):847–860. doi:10.1007/s00125-023-05870-2
24. Lindström J, Tuomilehto J. The diabetes risk score: a practical tool to predict type 2 diabetes risk. Diabetes Care. 2003;26(3):725–731.
25. Lee YH, Cho Y, Lee BW, et al. Nonalcoholic Fatty Liver Disease in Diabetes. Part I: epidemiology and Diagnosis. Diabetes Metab J. 2019;43(1):31–45. doi:10.4093/dmj.2019.0011
26. Dharmalingam M, Yamasandhi PG. Nonalcoholic Fatty Liver Disease and Type 2 Diabetes Mellitus. Indian J Endocrinol Metab. 2018;22(3):421–428. doi:10.4103/ijem.IJEM_585_17
27. Gutiérrez-Cuevas J, Santos A, Armendariz-Borunda J. Pathophysiological Molecular Mechanisms of Obesity: a Link between MAFLD and NASH with Cardiovascular Diseases. Int J Mol Sci. 2021;22(21). doi:10.3390/ijms222111629
28. Lambrinou E, Hansen TB, Beulens JW. Lifestyle factors, self-management and patient empowerment in diabetes care. Eur J Prev Cardiol. 2019;26(2_suppl):55–63. doi:10.1177/2047487319885455
29. Durlach V, Vergès B, Al-Salameh A, et al. Smoking and diabetes interplay: a comprehensive review and joint statement. Diabetes Metab. 2022;48(6):101370. doi:10.1016/j.diabet.2022.101370
30. Sato KK, Hayashi T, Harita N, et al. Relationship between drinking patterns and the risk of type 2 diabetes: the Kansai Healthcare Study. J Epidemiol Community Health. 2012;66(6):507–511. doi:10.1136/jech.2010.109777
31. Li MJ, Ren J, Zhang WS, et al. Association of alcohol drinking with incident type 2 diabetes and prediabetes: the Guangzhou Biobank Cohort Study. Diabetes Metab Res Rev. 2022;38(6):e3548. doi:10.1002/dmrr.3548
32. C-P F, Ali H, Rachakonda VP, Oczypok EA, DeLany JP, Kershaw EE. The ZJU index is a powerful surrogate marker for NAFLD in severely obese North American women. PLoS One. 2019;14(11):e0224942. doi:10.1371/journal.pone.0224942
33. Li L, You W, Ren W. The ZJU index is a powerful index for identifying NAFLD in the general Chinese population. Acta Diabetol. 2017;54(10):905–911. doi:10.1007/s00592-017-1024-8
34. Brambilla P, La Valle E, Falbo R, et al. Normal fasting plasma glucose and risk of type 2 diabetes. Diabetes Care. 2011;34(6):1372–1374. doi:10.2337/dc10-2263
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risks of Developing Diabetes and Hyperglycemic Crisis Following Carbon Monoxide Poisoning: A Study Incorporating Epidemiologic Analysis and Animal Experiment
Huang CC, Chen TH, Ho CH, Chen YC, Chen RJ, Wang YJ, Hsu CC, Lin HJ, Wang JJ, Chang CP, Guo HR
Clinical Epidemiology 2022, 14:1265-1279
Published Date: 1 November 2022
The DIAbetes MANagement and Treatment (DIAMANT) Cohort
Overbeek JA, Swart KMA, van der Pal EYM, Blom MT, Beulens JWJ, Nijpels G, Elders PJM, Herings RMC
Clinical Epidemiology 2022, 14:1453-1462
Published Date: 5 December 2022
Pregnancy Outcomes in Women with Type 1 Diabetes by Socioeconomic and Mental Health Disadvantages
Gundersen TW, Clausen TD, Ringholm L, Jensen DM, Damm P, Kragelund Nielsen K, Backman HE, Lauenborg J, Mathiesen ER, Skipper N, Kofoed-Enevoldsen A, Knorr S
Clinical Epidemiology 2026, 18:601414
Published Date: 27 May 2026