Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
Willingness to Undergo Corrective Surgery After Breast-Conserving Surgery in Chinese Patients with Breast Deformities: A Single-Center Study
Authors Zhang J, Wu Z, Gao J, Gao F, Guo F
Received 4 April 2026
Accepted for publication 9 June 2026
Published 12 June 2026 Volume 2026:18 614465
DOI https://doi.org/10.2147/BCTT.S614465
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Jingyan Zhang,1,* Zejun Wu,2,* Jingyan Gao,2 Fang Gao,3 Fan Guo2
1Department of Breast Surgery, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Third Hospital of Shanxi Medical University, Tongji Shanxi Hospital, Taiyuan, 030032, People’s Republic of China; 2Department of Breast Surgery, Third Hospital of Shanxi Medical University, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Taiyuan, 030032, People’s Republic of China; 3Department of Breast Surgery, Shanxi Provincial People′s Hospital, Taiyuan, Shanxi, 030000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fan Guo, Email [email protected]
Objective: To assess willingness to undergo corrective surgery among patients with breast deformities after breast-conserving surgery (BCS) and to identify factors associated with surgical decision-making.
Methods: This single-center cross-sectional study included female breast cancer patients who underwent BCS at Shanxi Bethune Hospital between July 2012 and December 2024, completed adjuvant radiotherapy, and had at least one year of follow-up after radiotherapy. Breast deformity was assessed using the Clough classification. A structured questionnaire evaluated perceived breast appearance, satisfaction, appearance-related distress, willingness toward corrective surgery, reasons for refusal, facilitating factors, and information needs. Willingness was defined as patients’ self-reported acceptance of considering corrective surgery at the time of the survey, rather than a confirmed operative plan. Associations were assessed using univariate analyses.
Results: Among 306 patients with post-BCS breast deformities, 123 (40.2%) expressed willingness to undergo corrective surgery and 183 (59.8%) declined. Surgical willingness showed unadjusted associations with several sociodemographic and clinical characteristics, including residence, income, travel time to medical care, deformity grade, postoperative complications, and recurrence/metastasis status. Among patients declining correction, the most important barriers were concern about complications or reconstruction failure (12.3%), financial burden (12.1%), acceptance of current appearance (11.2%), and reluctance to undergo another surgical procedure (10.0%). Among willing patients, the main facilitators were desire to improve body image/self-confidence (16.0%) and physician recommendation (16.0%).
Conclusion: Willingness to undergo corrective surgery after BCS was relatively low and appeared to be shaped by economic burden, risk perception, and appearance-related needs. These findings should be interpreted cautiously because of the single-center cross-sectional design and the absence of multivariable adjustment.
Keywords: breast cancer, breast-conserving surgery, breast deformities, corrective surgery, surgical decision-making, cross-sectional study
Introduction
Breast cancer is one of the most common malignancies among women worldwide, including in China.1,2 With improvements in screening and advances in comprehensive treatment, an increasing number of patients are being diagnosed and treated at early stages.3,4 Breast-conserving surgery (BCS), combined with radiotherapy, has been extensively validated in terms of oncological safety, demonstrating local control rates and overall survival comparable to those of mastectomy.5,6 Consequently, BCS has become a key treatment strategy for early-stage breast cancer. Compared with mastectomy, BCS offers clear advantages in preserving breast appearance and improving patients’ quality of life and psychological well-being.7–9 With ongoing advances in systemic therapy and precision oncology, survival outcomes for patients with breast cancer have continued to improve, shifting increasing attention toward survivorship, body image, and long-term quality-of-life outcomes.10,11
However, despite the significant benefits of BCS in terms of survival and body image, a growing number of reports indicate that some patients develop varying degrees of breast deformities after surgery, including breast asymmetry and displacement of the nipple–areola complex.12–14 Previous studies have reported that poor cosmetic outcomes or breast deformities may occur in up to one-quarter or more of patients after BCS,15,16 particularly among those with larger excision volumes or who receive radiotherapy.17 Abnormal breast appearance not only affects cosmetic results but may also negatively impact body image, self-esteem, confidence, and social interactions, thereby reducing overall quality of life.18
With the development of oncoplastic surgery, a variety of corrective procedures for post-BCS deformities have emerged, including local glandular rearrangement, various chest wall perforator flaps, autologous fat grafting, and contralateral breast symmetry procedures.19 Evidence indicates that, when indications are strictly observed, these reconstructive techniques do not increase the risk of local recurrence or distant metastasis.20,21 Nevertheless, the proportion of patients who actually undergo corrective surgery in clinical practice remains limited.22
From the perspective of shared decision-making, a patient’s choice regarding additional breast surgery may be shaped not only by clinical indications, but also by perceived risk, expected benefits, personal values, family support, financial capacity, and access to reliable information.23–25 However, most existing studies on reasons for declining breast reconstruction or corrective surgery have focused on immediate or delayed reconstruction after mastectomy and have primarily been conducted in Western countries.26 Evidence specifically addressing corrective surgery for post-BCS breast deformities remains limited, and Chinese data systematically exploring refusal reasons, facilitating factors, and information needs are particularly scarce. Therefore, the present study aimed to evaluate willingness to undergo corrective procedures among patients with breast deformities after BCS and to analyze factors associated with their decision-making, with the goal of informing postoperative education, risk communication, and shared decision-making.
Materials and Methods
Research Design and Participants
This single-center cross-sectional study included female patients with breast cancer who underwent BCS at the Breast Surgery Department of Shanxi Bethune Hospital between July 2012 and December 2024, completed adjuvant radiotherapy, and had at least one year of follow-up after radiotherapy.
The inclusion criteria were: (1) pathologically confirmed breast cancer; (2) receipt of BCS; (3) completion of adjuvant radiotherapy with at least one year since radiotherapy; (4) female sex; (5) confirmed presence of breast deformities upon evaluation; and (6) willingness to participate in follow-up and complete the study questionnaire.
Exclusion criteria were: (1) inability to assess the presence of breast deformities; (2) loss to follow-up or death; and (3) refusal to complete the questionnaire or missing key outcome variables.
Assessment of Breast Deformity
Postoperative breast appearance was independently evaluated by three investigators using the Clough classification of breast deformities. According to this classification, Grade I indicates a breast with a generally normal appearance but with some asymmetry compared to the contralateral side; Grade II indicates a noticeable deformity that can be corrected through local breast reconstruction; and Grade III indicates severe deformity or diffuse fibrosis, typically requiring mastectomy combined with reconstruction for correction.27 Before the formal assessment, the research team conducted a pilot evaluation on 20 non-study cases to standardize scoring criteria and minimize interobserver variability. Inter-rater consistency was ensured through consensus discussion and agreement checks.
Questionnaire Design and Data Collection
Data were collected using a structured questionnaire developed based on a literature review and clinical experience. The questionnaire covered the following domains: demographic characteristics, socioeconomic status, disease- and treatment-related information, self-perceived breast deformity/asymmetry, satisfaction with current breast appearance, appearance-related distress, willingness to undergo corrective surgery, concerns and reasons for declining correction, facilitating factors among patients willing to consider correction, and information needs for surgical decision-making.
The questionnaire was developed in three stages. First, the research team drafted the initial version after reviewing literature on breast reconstruction, cosmetic outcomes after BCS, and patient decision-making. Second, a pilot survey was conducted with five patients to assess clarity, acceptability, and logical order. Finally, wording and item order were revised according to patient feedback. The questionnaire included categorical single-choice items and multiple-response items; no total score or composite scale was calculated. For refusal reasons, patients could first select all applicable reasons and were then asked to identify the one to three most important reasons among those selected. The questionnaire was used for exploratory analysis and has not undergone formal psychometric validation.
After obtaining initial verbal agreement to participate, the research team sent electronic informed consent forms to patients via WeChat. Patients who provided electronic written informed consent then completed the questionnaire electronically. The survey was designed to record patients’ current views and did not require that patients had already scheduled corrective surgery. Disease- and treatment-related information was primarily obtained from the hospital database and electronic medical records, with additional verification from patients when necessary. Questionnaires that included a response to the key item on willingness to undergo corrective surgery were considered valid. Patients were instructed to complete the questionnaire independently. If participants had difficulty using the electronic form, research staff provided only technical assistance and did not suggest or modify any response. Before questionnaire completion, all participants received the same brief neutral explanation regarding the survey purpose and the general concept of corrective surgery. No individualized surgical recommendation, detailed risk estimate, or expected outcome prediction was provided at this stage; any questions raised by participants were answered using standardized neutral wording.
Variables Definition
The primary outcome variable was willingness to undergo corrective surgery for breast deformity. In this study, willingness referred to patients’ self-reported acceptance of considering corrective surgery at the time of questionnaire completion if clinically appropriate; it did not indicate that surgery had been scheduled or would necessarily be performed in the short term. Patients were categorized as willing or unwilling/refusing according to their response to this key item. The main independent variables included age, marital status, educational level, employment status, place of residence, annual household income, type of health insurance, one-way travel time to hospital, caregiving burden, Clough deformity grade, tumor-node-metastasis (TNM) stage, time since BCS, receipt of chemotherapy, receipt of endocrine therapy, postoperative complications, and current recurrence or metastasis treatment status.
Data Analysis
All statistical analyses were performed using SPSS version 26.0. Categorical variables were presented as counts and percentages, and age was summarized as median and interquartile range. Comparisons between the willing and unwilling groups were conducted using the chi-square test or Fisher’s exact test for categorical variables, as appropriate. Willingness to undergo corrective surgery was treated as the dependent variable in exploratory univariate analyses. No multivariable regression analysis was performed in the present study; therefore, the reported P-values should be interpreted as unadjusted associations rather than independent predictors. For questionnaire items allowing multiple selections, results were presented as the number of responses for each option and the percentage of total responses, unless otherwise specified. Two-sided tests were used, and a P-value of less than 0.05 was considered statistically significant.
Results
Participant Characteristics
A total of 346 patients were consecutively recruited. After excluding 25 invalid questionnaires and 15 patients who declined follow-up, 306 questionnaires were included in the final analysis (Figure 1). Among them, 123 patients (40.2%) expressed willingness to undergo corrective surgery, while 183 patients (59.8%) declined. The median age of participants was 52 years (IQR, 47–58), and the majority were married (96.7%). Deformity grades were predominantly Grade I and Grade II, accounting for 41.5% and 36.6%, respectively, while Grade III deformities accounted for 21.9%. Most patients had undergone surgery within the past two years (79.7%).
 |
Figure 1 Flow chart. |
Comparisons between groups revealed that, compared with patients who declined corrective surgery, those willing to undergo surgery were more likely to reside in urban areas (56.1% vs 37.2%, P = 0.001), be employed full-time (37.4% vs 21.3%, P < 0.001), and have a medium household income (50.4% vs 33.3%, P < 0.001). Additionally, the proportion of Grade III deformities was higher among patients willing to undergo correction (31.7% vs 15.3%, P < 0.001). Conversely, postoperative complications (58.5% vs 7.3%, P < 0.001) and recurrence or metastasis rates (17.5% vs 4.9%, P = 0.001) were higher in the group that declined surgery. No statistically significant between-group differences were observed in medical insurance status or receipt of chemotherapy (Table 1).
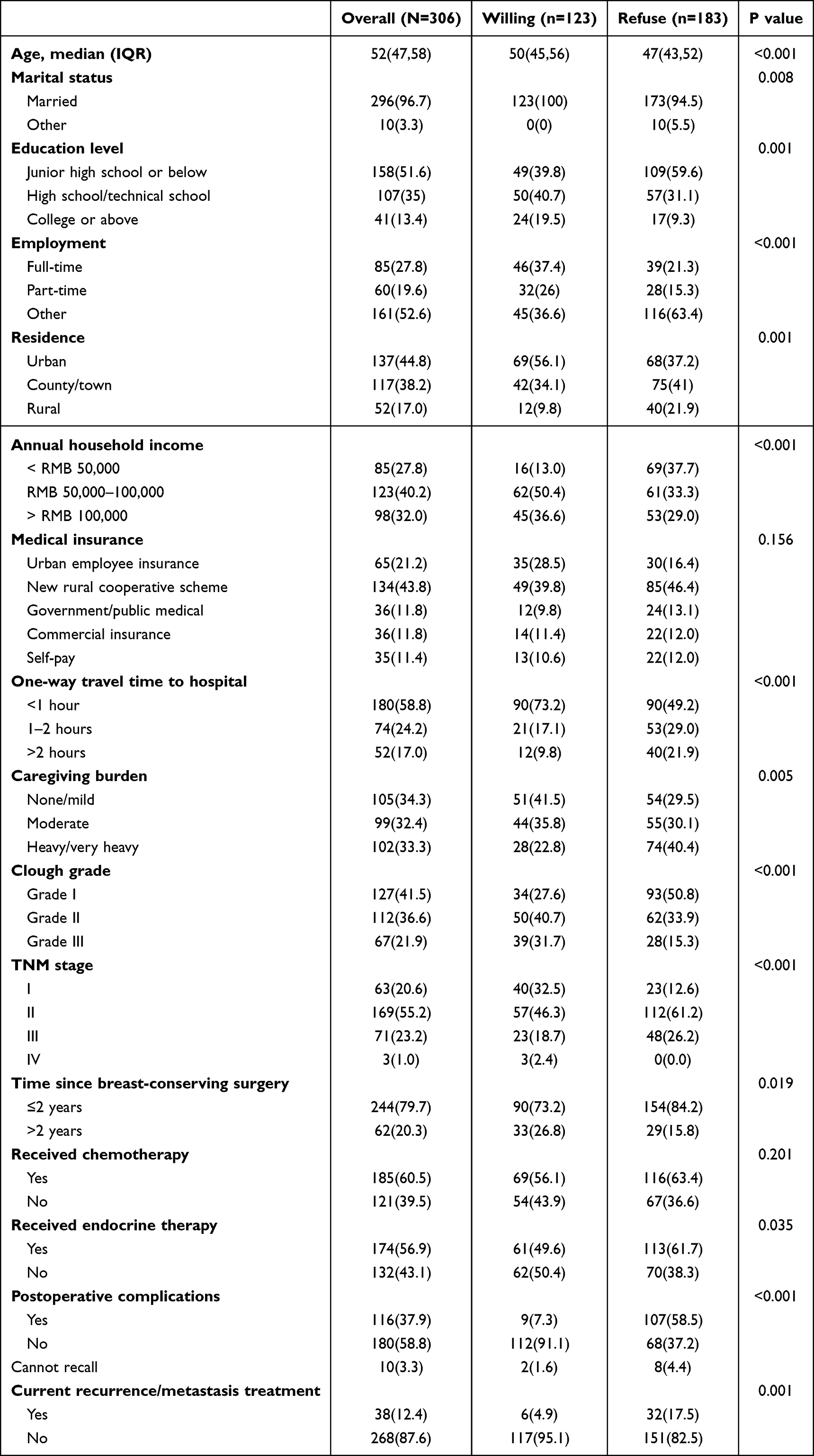 |
Table 1 Baseline Characteristics of Breast-Conserving Surgery Patients by Willingness to Undergo Corrective Surgery |
Perception of Postoperative Breast Appearance and Psychological Impact
Regarding self-assessed changes in the appearance of the affected breast, moderate asymmetry was the most commonly reported, accounting for 33.7% of patients, followed by mild asymmetry (28.1%) and severe asymmetry (26.1%), while 12.1% of patients were unable to judge. Overall, 59.8% of patients perceived at least moderate asymmetry. In terms of satisfaction with breast appearance, 55.9% of patients reported being “very dissatisfied,” 33.7% rated it as “neutral,” and only 10.5% reported being satisfied. Regarding appearance-related psychological impact, 48.4% of patients reported being “very distressed,” 24.2% reported “moderate distress,” and only 27.5% reported minimal or no distress. Overall, the majority of patients were dissatisfied with postoperative breast appearance, and a substantial proportion reported varying degrees of appearance-related psychological distress (Figure 2).
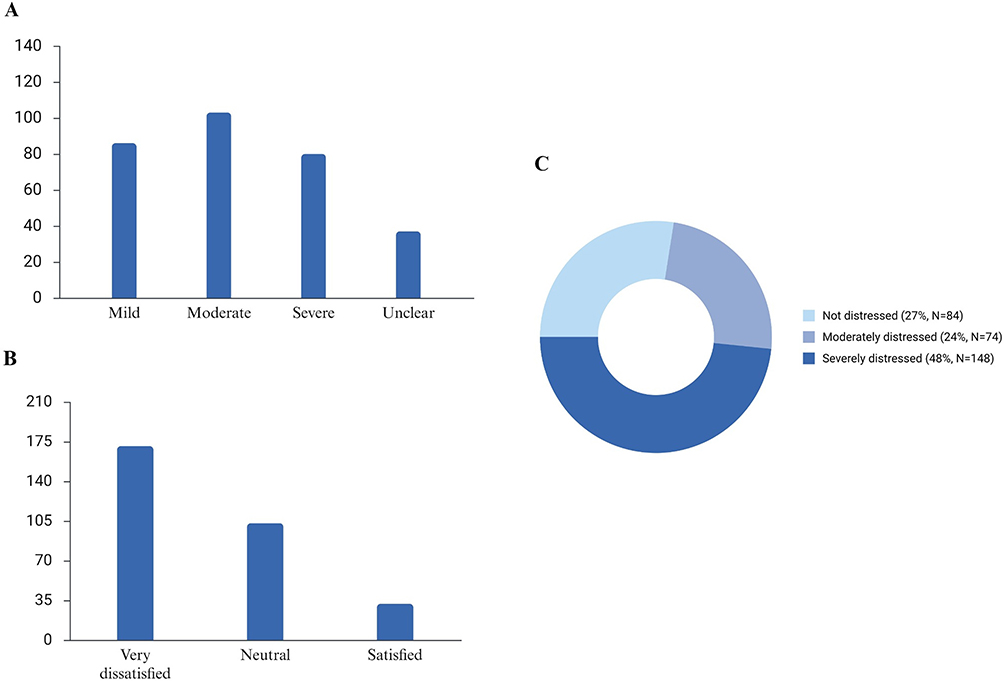 |
Figure 2 Self-perceived breast asymmetry and psychological distress after BCS (Perceived degree of deformity/asymmetry of the affected breast: (A) Your level of satisfaction with your current breast: (B) and Degree of distress caused by appearance issues: (C)). |
Main Reasons for Declining Corrective Surgery
Among patients who declined corrective surgery (Figure 3A), financial burden was the most frequently reported reason (11.1%), followed by reluctance to undergo another surgical procedure, anesthesia, or recovery process (10.0%), concern about oncological safety (9.9%), perception that the current appearance was acceptable (9.0%), and worry about postoperative complications or repair failure (8.9%). In addition, some patients cited uncertainty regarding surgical outcomes (8.4%), high caregiving burden (7.9%), lack of reliable information (6.3%), and concern about difficulty in recovery after reoperation following radiotherapy (5.9%). Family opposition (2.4%) and inconvenient transportation (3.0%) were reported less frequently.
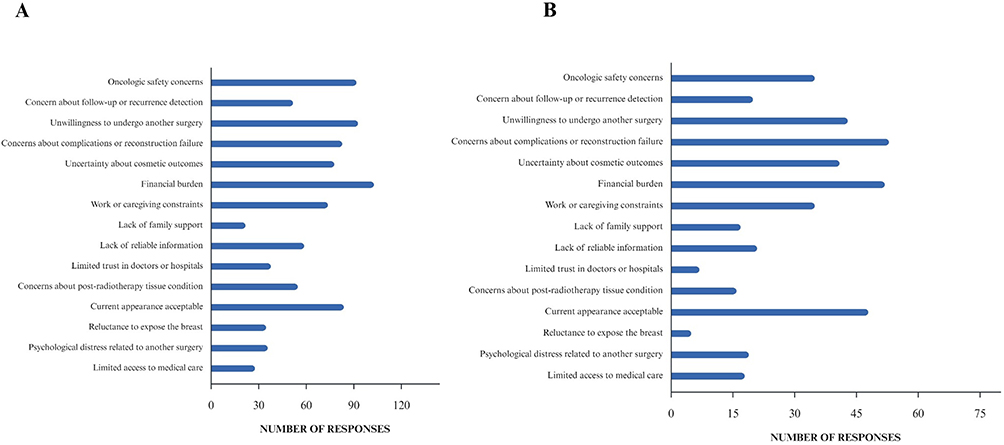 |
Figure 3 Reasons for declining corrective surgery for breast deformities (Distribution of all selected reasons: (A) Ranking of the most important reasons: (B)). |
When patients were further asked to select the one to three most important factors among those previously chosen (Figure 3B), the ranking changed slightly. Concern about complications or repair failure (12.3%) and financial burden (12.1%) were the top two factors, followed by perception that the current appearance was acceptable (11.2%) and reluctance to undergo another surgical procedure (10.0%). Uncertainty regarding surgical outcomes (9.5%) and concern about oncological safety (8.1%) also held moderate weight, whereas distrust of physicians or hospitals (1.6%) and privacy concerns (1.2%) were reported less frequently.
Facilitating Factors for Willingness to Undergo Corrective Surgery
Among patients willing to undergo corrective surgery (Figure 4), multiple factors jointly influenced their decision. The most commonly reported facilitating factors were the desire to improve body image or self-confidence (16.0%) and physician recommendation (16.0%). Other factors included inconvenience in dressing or daily activities (14.4%), noticeable appearance-related distress (14.0%), and having observed successful cases (14.0%). Support from partners or family members (13.6%) and affordability of the procedure (12.1%) were also reported as motivating factors by some patients.
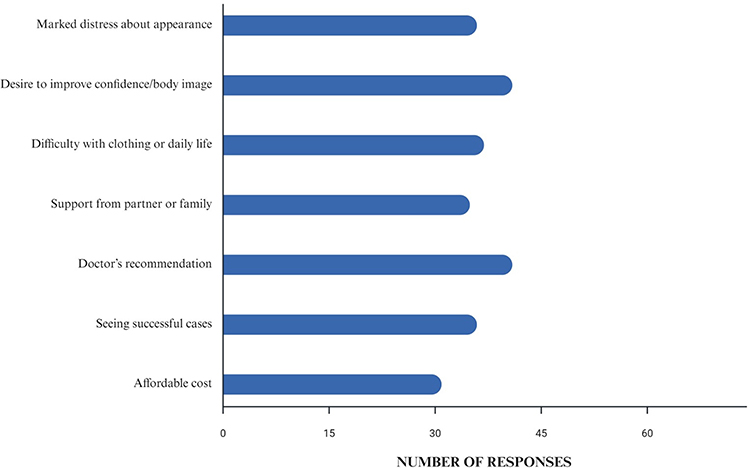 |
Figure 4 Facilitating Factors for Willingness to Undergo Corrective Surgery. |
Overall, the need for psychological and body image improvement, together with professional medical advice, played a prominent role in patients’ decisions to pursue corrective surgery.
Information Needs for Surgical Decision-Making
Among patients willing to undergo corrective surgery, information needs regarding the procedure were concentrated on several key aspects (Table 2). The most frequently reported concerns were surgical costs and reimbursement (23.6%) and the surgical approach with expected outcomes (23.1%). Other important concerns included potential complications and recovery-related issues (19.2%) as well as whether the surgery might affect follow-up or risk of recurrence (18.1%). In addition, 15.9% of patients expressed a desire to review real case photographs or previous examples to better understand surgical outcomes.
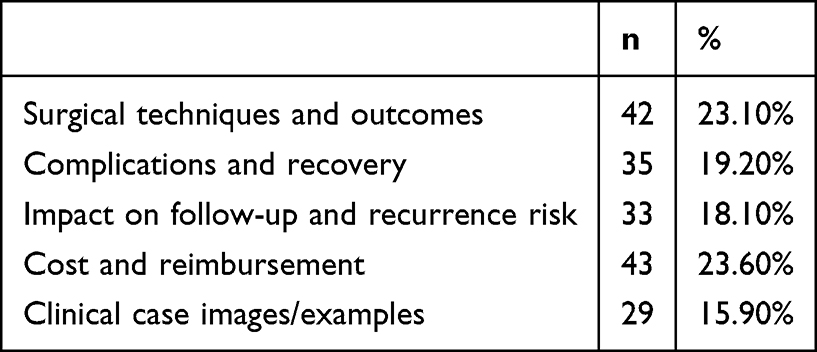 |
Table 2 Information Needs for Correction Decision-Making |
Overall, financial information and expected surgical outcomes were the most important factors influencing patients’ decision-making, while a substantial proportion of patients also sought detailed explanations regarding procedural safety and recovery.
Discussion
This study focused on patients who developed breast deformities after BCS and evaluated their willingness to undergo corrective surgery and factors associated with this decision. Only 40.2% of patients expressed willingness to undergo correction, whereas nearly 60% declined. This proportion is generally consistent with previous studies reporting that the uptake of breast reconstruction or corrective procedures is lower than the number of potentially eligible patients.28 In the present study, univariate comparisons and questionnaire responses suggested that willingness was related to both objective conditions and subjective perceptions. Concerns about complications or repair failure, financial burden, acceptance of current appearance, and reluctance to undergo another surgical procedure were the main barriers, whereas the desire to improve body image and physician recommendation were important facilitating factors.
The relatively low willingness observed in this study may be understood within a shared decision-making framework. Decisions about corrective surgery are not based solely on deformity severity or surgical feasibility, but also on how patients weigh expected cosmetic benefit against surgical risk, recovery burden, family responsibilities, economic pressure, and trust in medical advice. International studies have shown that, even in settings with relatively abundant healthcare resources, the actual rate of reconstruction or correction remains substantially lower than the population with potential indications.29 Similar patterns were observed in this Chinese cohort. Cultural and social factors may further influence this process; for example, family opinions may carry considerable weight, conservative attitudes toward additional surgery may reduce demand, and out-of-pocket expenses may make patients more cautious even when appearance-related distress is present.23,24 These findings suggest that postoperative counseling should address not only medical indications but also patient values, family context, and practical barriers. In the Chinese clinical context, decisions about additional surgery may also involve spouses or adult children, and household financial priorities and caregiving arrangements may therefore compete with the patient’s appearance-related needs.
It is noteworthy that most patients were dissatisfied with their postoperative breast appearance, and a substantial proportion reported significant appearance-related psychological distress. More than half perceived at least moderate asymmetry, while nearly 90% were not satisfied with breast appearance. Approximately three-quarters reported varying degrees of psychological distress related to appearance. Previous studies have shown that changes in breast appearance not only affect body image but may also negatively impact self-esteem, confidence, and social interactions, thereby reducing overall quality of life.30 However, even in the presence of significant distress, patients may decline further surgery due to practical or psychological factors, partially explaining the relatively low willingness observed in this study.
Regarding reasons for declining surgery, the main concerns were surgical risks and financial burden. Many patients worried that additional surgery could cause complications or repair failure, particularly in the context of prior radiotherapy, which may affect tissue healing and surgical outcomes.31 Financial burden was also a significant barrier. Although some corrective procedures are important for improving quality of life, limited reimbursement in the healthcare system may increase the economic pressure on patients and their families.32,33 Some patients were also concerned that corrective surgery could affect tumor recurrence or metastasis risk, although current evidence suggests that, when indications are strictly followed, these reconstructive techniques are oncologically safe.
Physician recommendation appeared to play an important role in surgical decision-making. Among patients willing to undergo correction, physician advice and the desire to improve body image were the most commonly cited facilitating factors. This may reflect the role of clinicians in reducing uncertainty, clarifying whether a patient is an appropriate candidate, explaining potential benefits and risks, and helping patients distinguish oncological safety concerns from cosmetic or reconstructive issues. In addition, patients’ information needs were concentrated on costs and reimbursement, surgical techniques and expected outcomes, potential complications and recovery, and possible effects on follow-up or recurrence detection. These findings indicate that communication should be structured and practical, rather than limited to a general recommendation. Visual examples, explanation of procedure-specific risks, discussion of radiotherapy-related tissue conditions, and transparent information on financial issues may help patients make more informed choices, although whether such strategies increase uptake requires prospective evaluation.25 In clinical practice, this may be implemented as a stepwise counselling process: assessment of deformity severity and appearance-related distress, discussion of feasible corrective options, explanation of costs and reimbursement, clarification of complications and recovery, confirmation that oncological follow-up will not be compromised, and presentation of representative case examples when appropriate.
Limitations
This study has several strengths. It specifically analyzed patients with breast deformities following BCS, a clinically relevant population that has received less attention than patients undergoing reconstruction after mastectomy. In addition, this study assessed multiple dimensions, including sociodemographic characteristics, disease- and treatment-related factors, subjective appearance perception, refusal reasons, facilitating factors, and information needs, thereby providing a patient-centered perspective on decision-making. However, several limitations should be noted. First, this was a single-center study, and the sample was relatively concentrated, which limits the generalizability of the findings. Second, the cross-sectional design captured willingness at only one time point; patient preferences may change with disease status, family circumstances, financial conditions, or further consultation. Third, part of the information was based on self-reported questionnaire data, which may be affected by recall bias, subjective interpretation, and differences in patients’ prior understanding of corrective surgery. Fourth, the questionnaire was developed for exploratory use and was not formally psychometrically validated. Finally, the statistical analysis was limited to univariate comparisons without multivariable adjustment; therefore, the observed associations should not be interpreted as independent predictors or causal relationships. In addition, although a standardized survey process was used, patients’ baseline knowledge of corrective surgery was not measured, and differences in pre-existing understanding may have influenced their responses. Future multicenter prospective studies using validated decision-making instruments, standardized information provision, objective cosmetic assessment, and multivariable modelling are needed to further clarify the determinants of corrective surgery willingness after BCS.
Conclusion
In this single-center exploratory study, willingness to undergo corrective surgery among patients with breast deformities after BCS was relatively low. Financial burden, perceived surgical risk, acceptance of current appearance, and reluctance to undergo another procedure were major barriers, whereas body-image needs and physician recommendation were key facilitators. These findings support the need for more structured postoperative counseling and decision support, while future prospective studies with multivariable analysis are required to confirm independent determinants of surgical willingness.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the corresponding author, without undue reservation.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the Shanxi Bethune Hospital Ethics Committee (No. YXLL-2026-028).
Consent to Participate
The patients/participants provided their written informed consent to participate in this study. The manuscript has been read and approved by all the authors.
Acknowledgments
The authors would like to thank all participants and staff involved in the project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Internal Research/Matching Funds of the Department of Scientific Research, Shanxi Bethune Hospital (Third Hospital of Shanxi Medical University) (Grant No. 041256).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca A Cancer J Clin. 2024;74(3):229–11.
2. Tao X, Li T, Gandomkar Z, Brennan P, Reed W. Incidence, mortality, survival, and disease burden of breast cancer in China compared to other developed countries. Asia-Pac J Clini Oncol. 2023;19(6):645–654. doi:10.1111/ajco.13958
3. Kim J, Harper A, Mccormack V, et al. Global patterns and trends in breast cancer incidence and mortality across 185 countries. Nature Med. 2025;31(4):1154–1162. doi:10.1038/s41591-025-03502-3
4. Benitez Fuentes JD, Morgan E, De Luna Aguilar A, et al. Global stage distribution of breast cancer at diagnosis: a systematic review and meta-analysis. JAMA Oncol. 2024;10(1):71. doi:10.1001/jamaoncol.2023.4837
5. Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. New Engl J Med. 2002;347(16):1233–1241.
6. Vasilyeva E, Nichol A, Bakos B, et al. Breast conserving surgery combined with radiation therapy offers improved survival over mastectomy in early-stage breast cancer. Am J Surg. 2024;231:70–73.
7. Li S, Li X, Li D, Zhao Q, Zhu L, Wu T. A meta-analysis of randomized controlled trials comparing breast-conserving surgery and mastectomy in terms of patient survival rate and quality of life in breast cancer. Int J Qual Health Care. 2024;36(2). doi:10.1093/intqhc/mzae043
8. Se Hanson XL, Roubaud M, Desnyder S, et al. Long-term quality of life in patients with breast cancer after breast conservation vs mastectomy and reconstruction. JAMA Surg. 2022;157(6):e220631. doi:10.1001/jamasurg.2022.0631
9. Kim M, Tadros A, Boe L, et al. Breast-Conserving therapy versus postmastectomy breast reconstruction: propensity score-matched analysis. Ann Surg Oncol. 2024;31(12).
10. Y L, Yuan Q, H Y, et al. Impact of post-neoadjuvant chemotherapy biomarker changes on long-term oncological outcomes in Non-pCR breast cancer. Clin Breast Cancer. 2026;26(4):144–9e2. doi:10.1016/j.clbc.2026.02.006
11. Yuan Q, Sha Y, R Y, et al. Machine learning-based identification of kbhb-affected tumor cell subsets as prognostic and therapeutic targets in breast cancer. J Transl Med. 2025;24(1):71. doi:10.1186/s12967-025-07555-3
12. Vincenzo V, Francesco M, Chiara Z, et al. Breast reconstruction: the oncoplastic approach. J Clin Med. 2024;13(16).
13. Fitzal F, Bolliger M, Dunkler D, et al. Retrospective, multicenter analysis comparing conventional with oncoplastic breast conserving surgery: oncological and surgical outcomes in women with high-risk breast cancer from the OPBC-01/iTOP2 Study. Ann Surg Oncol. 2022;29(2):1061–1070. doi:10.1245/s10434-021-10809-1
14. Sevgi K, Ahmet Serkan İ, Enver Ö, et al. Outcomes of reconstructive techniques in breast cancer using BCCT. core software. World J Surg Oncol. 2024;22(1). doi:10.1186/s12957-024-03343-3.
15. Berry M, Ad Fitoussi AC, Couturaud B, Salmon R, Salmon RJ. Oncoplastic breast surgery: a review and systematic approach. J Plast Reconstruct Aesthetic Surg. 2010;63(8):1233–1243. doi:10.1016/j.bjps.2009.05.006
16. Catsman Coriene JLM, Beek Martinus A, Voogd Adri C, Mulder Paul GH, Luiten Ernest JT. The COSMAM TRIAL a prospective cohort study of quality of life and cosmetic outcome in patients undergoing breast conserving surgery. BMC Cancer. 2018;18(1).
17. Chu C, Hu K, Wu R, Bau D. Radiation-irritated skin and hyperpigmentation may impact the quality of life of breast cancer patients after whole breast radiotherapy. BMC Cancer. 2021;21(1). doi:10.1186/s12885-021-08047-5
18. De Oliveira-Junior I, Da Silva F, Sarri A, Vieira R. Do non-mammary conditions influence patients’ cosmetic perception after breast conserving surgery? Front Oncol. 2025;14.
19. Primeera W, Malata Charles M, Benson John R. Frontiers | oncoplastic and reconstructive breast surgery. Front Oncol. 2023;13.
20. Kollias V, Kollias J. Safety and efficacy of anterior intercostal artery perforator flaps in oncoplastic breast reconstruction. ANZ J. Surg. 2022;92(5):1184–1189. doi:10.1111/ans.17496
21. Prasidha I, Boyages J, Lam T. Safety of reduction mammaplasty and mastopexy after breast conservation therapy and radiation therapy: a case series. Ann Plast Surg. 2023;90(1):27–32. doi:10.1097/SAP.0000000000003333
22. Wu Z, Zhong L, Gu J, Xie H, Guo F. Correction of breast deformities after breast-conserving surgery in Chinese women with breast cancer: a narrative review. Front Oncol. 2025;15:1648679. doi:10.3389/fonc.2025.1648679
23. Seki H, Komiya T, Sowa Y, et al. Factors influencing surgical decision-making in breast cancer: a multicenter study in Japan. Eur J Surg Oncol. 2026;52(5):111739. doi:10.1016/j.ejso.2026.111739
24. Kawasaki Y, Hirai K, Nii M, Kizawa Y, Uchinuno A. Factors involved in shared decision-making regarding treatment selection by patients with cancer. Cancer Diagnosis Prognosis. 2024;4(1):57–65. doi:10.21873/cdp.10286
25. Su Y, Sun C, Chiu W, Kang Y, Chen C. Patient decision aids for breast cancer reconstruction: a systematic review and network meta-analysis of randomized controlled trials. Plast Reconstr Surg. 2024;154(5):929–940. doi:10.1097/PRS.0000000000011292
26. Monica M, Yun L, Alderman Amy K, et al. Breast reconstruction access. JAMA Surg. 2014;149(10).
27. Clough K, Cuminet J, Fitoussi A, Nos C, Mosseri V. Cosmetic sequelae after conservative treatment for breast cancer: classification and results of surgical correction. Ann Plast Surg. 1998;41(5).
28. Ho D, Chan E, Izwan S, et al. Uptake of breast reconstruction following mastectomy: a Gold Coast experience. ANZ J Surg. 2022;92(11):3011–3016. doi:10.1111/ans.17703
29. Jagsi R, Jiang J, Momoh A, et al. Trends and variation in use of breast reconstruction in patients with breast cancer undergoing mastectomy in the United States. J Clin Oncol. 2014;32(9):919–926. doi:10.1200/JCO.2013.52.2284
30. Jang Y, Seong M, Sok S. Influence of body image on quality of life in breast cancer patients undergoing breast reconstruction: mediating of self-esteem. J Clin Nurs. 2023;32(17–18):6366–6373. doi:10.1111/jocn.16621
31. Piroth MD, Krug D, Baumann R, et al. Implant-based reconstruction and adjuvant radiotherapy in breast cancer patients—current status and DEGRO recommendations. Strahlenther Onkol. 2024;201(4).
32. Rochlin Danielle H, Rizk Nada M, Evan M, Wagner Todd H, Sheckter Clifford C. Commercial price variation for breast reconstruction. JAMA Surg. 2023;158(2).
33. Huynh Kristine A, Mayank J, Chang W, et al. State-Specific medicaid expansion and autologous breast reconstruction among patients undergoing mastectomy. JAMA Netw Open. 2021;4(8). doi:10.1001/jamanetworkopen.2021.19141.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Popularity of Traditional Chinese Medicine Use Among Breast Cancer Patients in North China: A Cross-Sectional Study
Zhao R, Zhang J, Gou Q, Gao J
Breast Cancer: Targets and Therapy 2023, 15:577-589
Published Date: 10 August 2023
Knowledge, Attitude, and Practice Towards Rehabilitation in Patients with Breast Cancer: A Cross-Sectional Study
Zhou Y, Lu Q, Yu X
Journal of Multidisciplinary Healthcare 2025, 18:1483-1492
Published Date: 12 March 2025