")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Willingness to Receive mHealth Services Among Patients with Diabetes on Chronic Follow-up in Public Hospitals in Eastern Ethiopia: Multicenter Mixed-Method Study
Authors Firdisa D , Abera A , Dereje J , Asefa F
Received 2 October 2023
Accepted for publication 6 December 2023
Published 13 December 2023 Volume 2023:16 Pages 4081—4099
DOI https://doi.org/10.2147/DMSO.S428210
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Dawit Firdisa,1 Admas Abera,1 Jerman Dereje,2 Fekede Asefa1,3
1School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 2Department of Psychiatry, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 3Department of Pediatrics, College of Medicine, University of Tennessee Health Science Center (UTHSC) - Oak Ridge National Laboratory (ORNL) Center for Biomedical Informatics, Memphis, TN, 38103, USA
Correspondence: Dawit Firdisa, School of Public Health, College of Health and Medical Sciences, Haramaya University, P.O.box, 235, Harar, Ethiopia, Tel +251961794645, Email [email protected]
Background: Management of diabetes requires a long-term care strategy, including support for adherence to a healthy lifestyle and treatment. Exploring the willingness of patients with diabetes to receive mHealth services is essential for designing efficient and effective services. This study aimedto determine willingness to receive mHealth services and associated factors, as well as explore the barriers to receive mHealth services among patients with diabetes.
Methods: A multicenter mixed-method study was employed from September 1 to November 30, 2022. For the quantitative part, a total of 365 patients with diabetes receiving chronic follow-up at three public hospitals were enrolled. Data were gathered using structured questionnaires administered by interviewers, entered into Epi-data version 4.6, and analyzed using Stata version 17. A binary and multivariable logistic regression model was computed to identify the associated factors. For qualitative, eight key informants and seven in-depth interviews were conducted. After verbatim transcription and translation, the data were thematically analyzed using ATLAS.ti V. 7.5.
Results: Overall, 77.3% had access to a mobile phone, and 74.5% of them were willing to receive mHealth services. Higher odds of willingness to receive mHealth services were reported among patients with an age below 35 years [AOR = 4.11 (1.15– 14.71)], attended formal education [AOR = 2.63 (1.19– 5.77)], without comorbidity [AOR = 3.6 (1.54– 8.41)], < 1-hour travel to reach a health facility [AOR = 3.57 (1.03– 12.36)], answered unknown calls [AOR = 2.3 (1.04– 5.13)], and were satisfied with health-care provider service [AOR = 2.44 (1.04– 5.72)]. In the qualitative part, infrastructure, health facilities, socioeconomic factors, and patients’ behavioral factors were major identified barriers to receiving mHealth services.
Conclusion: In this study, the willingness to receive mHealth services for those who have access to mobile phones increased. Additionally, the study highlighted common barriers to receiving mHealth services.
Keywords: willingness, mHealth, mobile phone, diabetes, mixed method, eastern Ethiopia
A Letter to the Editor has been published for this article.
Introduction
Diabetes mellitus (DM) is one of the main causes of morbidity and mortality, with over five million deaths estimated globally in 2017 due to diabetes.2 According to the International Diabetes Federation, 79% of patients with diabetes reside in low- and middle-income countries (LMICs), and the burden is expected to rise in the future.3 In 2019, there were 463 million estimated patients with diabetes globally, with the number anticipated to reach 700 million by 2045. In Africa, 24 million adults had diabetes in 2021, and Ethiopia was ranked fourth with regard to the number of patients with diabetes.4,6 A systematic review and meta-analysis in Ethiopia revealed that the prevalence of diabetes in the country was 6.5%.3 Currently, diabetes is a major area of focus for mHealth interventions, despite being underexplored in sub-Saharan Africa (SSA).7,8
mHealth is a medical and public health intervention assisted by mobile phones, patient monitoring devices, personal digital assistants, or other wireless technologies.9 mHealth services, including smartphone-based diabetes applications, played a significant role in diabetes prevention and follow-up intervention programs in high-income countries (HICs), where they are being utilized for bringing initiatives designed to promote a healthy diet, regular physical activity, prevent obesity, improve patient engagement in diabetes care, as well as reduce the number of care dropouts and glycemic control due to poor communication between the patient and the service providers.10–14
Poor communication between the patient and the health-care provider, the patients’ lack of knowledge regarding the disease condition and treatment, the complexity of the regimen, fear and experience of side effects, the cost of medication, and a lack of conviction about the necessity of treatment are all barriers to adherence to diabetes medication.15–17 Furthermore, adherence to diabetes medication and care remains a problem in LMICs.18,19 For instance, a study carried out in Ethiopia revealed that 25% of patients with diabetes properly followed their prescribed medications and dietary recommendations.20
These traditional barriers to accessing diabetes care can be overcome through the use of mobile phone devices in medical and public health practices.21 This approach offers advantages such as reducing travel and hospital waiting times, enhancing chronic disease prevention, patient care, and self-management, monitoring and provision of client-centered health information, lowering the cost of diabetes care, and improving the lives of underserved populations.21–24 Therefore, this study aimed to determine the willingness and associated factors among patients with diabetes for chronic follow-up in public hospitals in eastern Ethiopia.
Methods and Materials
Study Setting and Design
This study employed a multicenter institution-based sequential explanatory mixed-method approach in which a quantitative cross-sectional study was sequentially integrated into a qualitative phenomenological study. The study was conducted at three major public hospitals in eastern Ethiopia (Hiwot Fana Comprehensive Specialized University Hospital in Harar City, Dilchora Referral Hospital in Dire Dawa City, and Sheik Hassan Yabare Referral Hospital in Jigjiga City) from September 1–November 30, 2022. More than 2200 patients with diabetes were on follow-up during the study period in these three hospitals.
Study Population and Sampling Approach
For quantitative part, the study populations were patients with diabetes (including both type I and type II) on chronic follow-up in selected public hospitals, whereas patients with diabetes and health-care providers (HCPs) in the selected hospitals were study participants for qualitative part. Patients with diabetes who have been diagnosed before 3 months of the data collection time, attending a diabetes follow-up clinic during the study period and willing to participate in the study were included in the study.
The sample size was determined using both a single and double population proportion formula. The maximum sample was achieved by using a double proportion formula by considering the assumptions: 95% confidence level, 80% power, and one-to-one ratio between case and control proportions: p1 = percentage of population who travel by car to come to a health facility (71.9%), p2 = percentage of population who travel by foot to come to a health facility (56.7%) based on a study conducted in northwest Ethiopia (23), and 10% of non-respondents. The final sample size was 365.
Systematic random sampling was employed to select study participants for the quantitative part. From each selected hospital, the number of participants included in the study was determined using proportional allocation based on their actual number of patients with diabetes. Respondents were selected while they were on their follow-up visits at the facility. On the first day of data collection, the first respondent was randomly selected from first six (k) respondents who came for the service followed by every other kth respondent who was selected and interviewed until the required sample size was reached.
For the qualitative part, a purposeful sampling method was employed to select participants based on their diabetes information or experiences that members of the population were likely to possess. Seven in-depth interviews were conducted with patients with diabetes, and eight key informant interviews were held with health-care providers (nurse and physicians who provide services for patients with diabetes). Data collection was stopped when information saturation was reached, meaning that no additional data emerged during data collection.
Data Collection and Quality Control Procedures
For the quantitative part, data were collected by 10 trained clinical nurses through face-to-face interviews using a structured questionnaire adapted from previous studies (23, 25) after being validated before use. Onsite supervision was performed by one data supervisor and the principal investigator. A pretest was done outside the study area on about 5% of the sample size. Moreover, data collectors were given two days of training with the aim of the study and the data collection tools. The completeness and quality of data collection were supervised daily, and feedback was provided to the data collectors.
For qualitative part, data were collected for 1 month in working hours each day. Participants were pre-identified and scheduled for interview. The data collector used an interview guide to facilitate interviews process. Guides were prepared in English, Amharic, Afan Oromo, and Af-Somali and were piloted in similar settings before being used for the study. Two trained data collectors experienced with qualitative data collection conducted in-depth interviews after 2-day training was given. Sony ICD PX470 sound recorder was used to record the participants’ responses. The interviews were conducted in a quiet and private room, which took about 20–40 min. The interviews were audio-recorded. Field notes were taken for all interviews to record any non-verbal observations. Upon completion of each in-depth interview, a trained language professional produced a complete transcript and translation of the data for data entry and analysis. Furthermore, transcriptions, translations, and coding of the data were reviewed with audio recordings to check for accuracy and authenticity. The rigor of the qualitative data was assured through thoughtful and deliberate planning, ongoing application of researcher reflexivity, and honest communication between the researcher and the audience regarding the study and its results.
Data Analysis
For quantitative part, data were coded and entered using Epi Data V.4.6 and then exported to Stata V.17 for analysis. Frequency and cross-tabulations were used to describe the data. The associations between the characteristics of respondents and their willingness to receive mHealth services were analyzed using bivariable and multivariable logistic regression analyses. The backward selection method was used to select variables with a p-value of <0.25 in the bivariable logistic regression analyses. These variables were entered into a multivariable logistic regression to adjust for the effect of confounding. The model was fitted with the Hosmer and Lemeshow goodness-of-fit test of 0.6345, and a p-value of 0.05 was considered to be significant.
For qualitative part, the recorded Amharic and Afaan Oromo versions that were transcribed and translated back to English version. Field notes were expanded while on the field. Before themes and codes were identified, the researcher fully read and reread interview transcripts, independently identified possible themes and codes, and then pooled observations. Coding and analysis were done using Atlas.ti V.7.5 software. In general, inductive thematic analysis was used, in which themes were developed that represented the whole idea of categories.
Results
Quantitative Findings
Socio Demographic Characteristics of Participants
A total of 365 patients with diabetes have participated in this study. The age of the respondents ranges from 15 to 88 years, with a mean age of 48.3 years (standard deviation (SD) = 17.5). Overall, 51.5% of the respondents were females, 64.4% were married, and 62.7% attended primary or above educational level (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Patients with Diabetes on Chronic Follow-Up at Selected Public Hospitals, Eastern Ethiopia 2022 |
Mobile Phone Access
More than three-quarters, 77.3% (95% CI: 72.6–81.3%), had access to a mobile phone, of which 37.9% were smart phones. Access to mobile phones was higher among urban residents (78.2%) as compared to rural residents (73.2%), among male (82.5%) compared female (72.3%) participants. Similarly, participants who earned $50 USD per month had higher access (87.2%) to mobile phone compared to who earned <$50 USD per month (65.9%) (Table 2).
 |
Table 2 Mobile Phone Access Among Patients with Diabetes at Selected Public Hospitals, Eastern Ethiopia 2022 |
Willingness to Receive mHealth Services
Among participants with access to mobile phone, willingness to receive mHealth services was 77.2% among females and 71.9% among males (Table 3). Additionally, 79.8% of participants who had access to television and 76.3% of those who had access to radio were willing to receive mHealth services (Table 4). From participants who reported being satisfied with their health-care providers, 78.2% expressed a willingness to receive mHealth services, compared to 59.6% among those who were not satisfied (Table 4). Furthermore, 75.9% participants who perceived benefit of mobile-based support for adherence were willing to receive mHealth service as compared to 69.3% among their counterparts (Table 4).
 |
Table 3 Willingness to Receive mHealth Services Among Patients with Diabetes at Selected Public Hospitals, Eastern Ethiopia 2022 |
 |
Table 4 Willingness to Receive mHealth Services Stratified by Socioeconomic, Environmental And Behavioral Factors Among Patients with Diabetes at Selected Public Hospitals, Eastern Ethiopia 2022 |
Table 5 shows willingness to receive mHealth services across patterns of mobile phone usage. Of participants who had access to mobile phones, 74.8% of smartphone owners had a willingness to receive mHealth services compared 74.3% participants without a smartphone. Similarly, participants who used their mobile phone for health communication were more willing (81.5%) to receive mHealth services than those who did not (71.6%). The willingness to receive mHealth services was higher among patients with diabetes who always held their mobile phone (75.8%) compared to those who held their mobile phone sometimes (70.4%). Patients who allowed others to use and access their mobile phones had a lower willingness to receive mHealth services than those who did not (71.7% vs 76.3%). Additionally, internet users via mobile phone showed a higher willingness to receive mHealth services compared to non-users (79% vs 70.5%).
 |
Table 5 Willingness to Receive mHealth Services Stratified by Pattern of Mobile Phone Use Among Patients with Diabetes on Chronic Follow-Up in Public Hospitals, Eastern Ethiopia, 2022 |
Among participants, 44.4% of who were unwilling to receive mHealth service reported difficulties in operating their phones and 33.3% perceived mHealth services were not important (Figure 1). Moreover, of individuals willing to receive mHealth services, 73.8% showed a willingness to receive dietary-related information; while 67.1% expressed interest in receiving guidance on things they should avoid (Figure 2).
 |
Figure 1 Reason for being unwilling to receive mHealth services among patients with diabetes on chronic follow up in public hospitals, eastern Ethiopia, 2022. |
 |
Figure 2 Diabetic information needed to be received by patients with diabetes on chronic follow up among those who are willing to receive mHealth services in public hospitals, eastern Ethiopia, 2022. |
Factors Associated with Willingness to Receive mHealth Services
Results of the bivariable analyses indicated that age, marital status, educational status, residence, occupation, average monthly income, types of diabetes, presence of comorbidity, route of medication, television ownership, time to reach the health facility, satisfaction with health-care providers’ service, having heard DM-related information, follow-up care services, open communication with health-care providers, availability of electricity, and availability of a telecommunication network were associated with willingness to receive mHealth service.
Moreover, previously using mobile phone for a health communication, changing mobile phone number in the last 12 months, not willing to answer calls from unknown number, using internet by their mobile phone, preferred mode of communications, locking mobile phone with passwords, access to mobile phone by others, current use of mobile phone for adherence, and availabilities of time or place for calls were significantly associated with willingness to receive mHealth services at a p value of <0.25. All of these associated factors were entered in the multivariable logistic regression analysis model to control for the effect of confounders.
Table 6 shows the result of the multivariable logistic regression model. The respondents with aged <35 years had 4.1 times more odds of willingness to use mHealth services than those 35 years of age and older [AOR=4.1 (95% CI: 1.2–14.7)]. Educated respondents had 2.6 times more odds of willingness to use mHealth services than uneducated respondents [AOR=2.6 (95% CI: 1.2–5.8)]. Patients with other comorbidities had 3.6 times more odds of willingness than those without comorbidities [AOR=3.6 (95% CI: 1.5–8.4)]. On the other hand, respondents who were satisfied with health-care providers had more odds to express their willingness to receive mHealth services than those who were not satisfied [AOR=2.4 (95% CI: 1.0–5.7)], while those who answer unknown calls were 2.3 times more willing as compared with those who do not answer unknown calls (2.3 (1.0–5.1)). Moreover, individuals who traveled for less than 1 hr had 3.6 times more odds to express willingness compared with those who traveled more than 1 hr (3.6 (95% CI:1.0–12.4)).
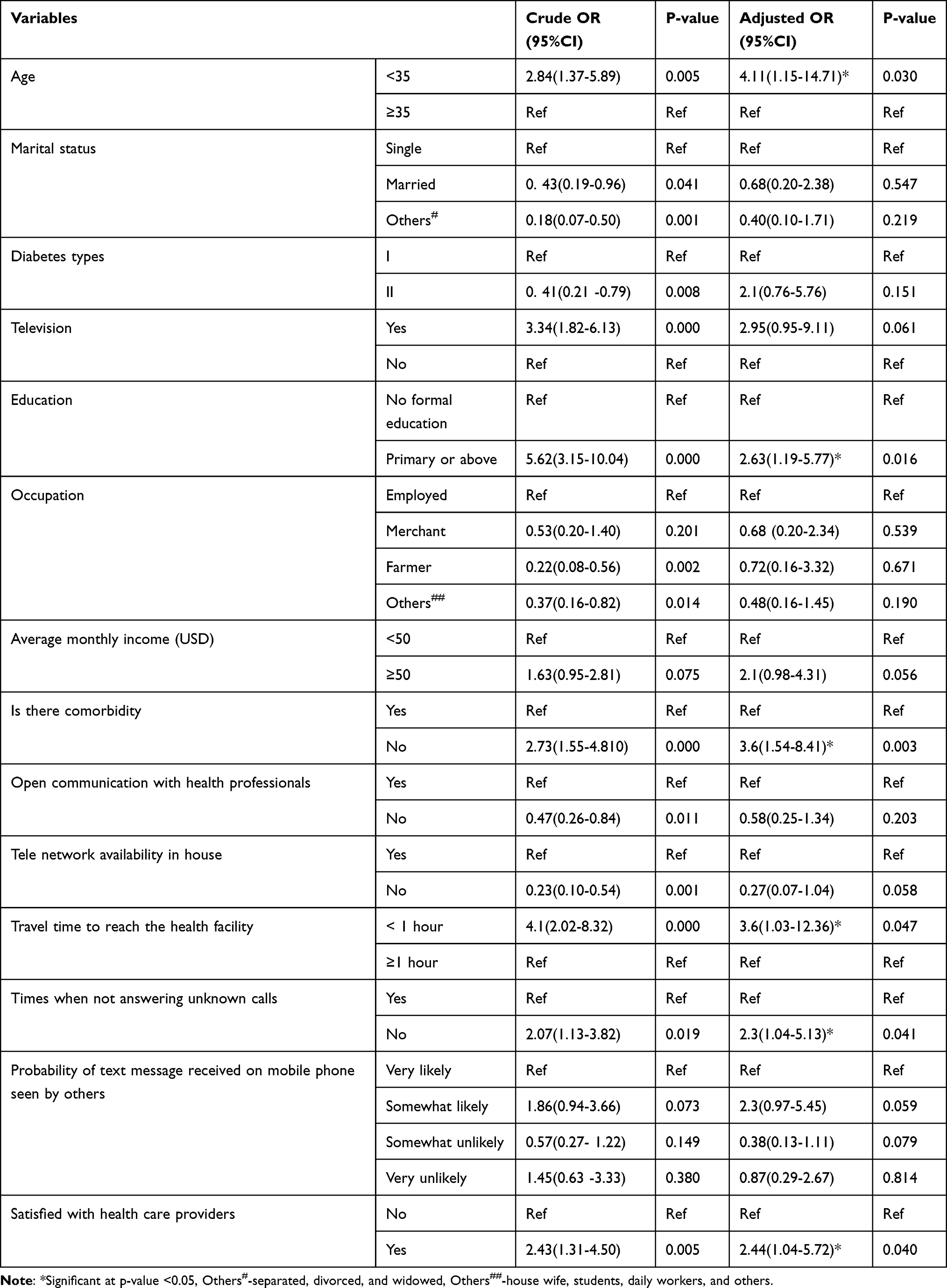 |
Table 6 Bivariable and Multivariable Analyses of Factors Associated with Willingness to Receive mHealth Services Among Patients with Diabetes on Chronic Follow-Up at Selected Public Hospitals, Eastern Ethiopia 2022 |
Qualitative Findings
Themes Identified During the Analysis
The analysis of 15 interviews (primary documents) resulted in 90 open codes being merged into 42 codes, then categorized under 11 subthemes (categories) from which four major themes (subcategories) were emerged. The key themes and sub-themes with identified barriers are shown in Table 7.
 |
Table 7 Themes and sub-themes emerged for qualitative study on barriers to receive mHealth services among patients with diabetes on chronic follow up in public hospitals, Eastern Ethiopia, 2022 |
Lack of access to network
This finding revealed that the network problem is one of the barriers towards willingness to receiving mHealth services among patients with diabetes on chronic follow-up.
A 42-year-old male patient stated his opinion as:
There might be a network problem especially for those who come from rural area where network can’t reach. One of the problems with a network is that it prevents you from meeting or communicating with many people, especially those who live in remote areas away from health facilities. (IDI-1)
Lack of access to electricity
The finding also depicted a lack of access to electricity as a barrier towards willingness to utilize mHealth services.
A 36-year-old female patient reported:
There are places in remote rural areas where electricity is not available. Because of this our mobile phone usually becomes off until we go to town to charge it, unless for those we charge by solar, if we own. This may be the reason why we don’t usually able to use such a new technology. (IDI-3)
Ownership of mobile phone
The results also demonstrated that willingness to receive mHealth services is hindered by not possessing a mobile phone.
A male medical doctor, age 26, stated:
First, it is questionable that all patients have access to a mobile phone. Not only mobile phone, but also a kind of mobile phone for using different applications like smartphone to utilize these services could also be another challenge. (KI-11).
Economic status
This study also indicated that low socioeconomic status is a barrier towards willingness to receive mHealth services.
A 29-year-old female nurse shared her experience as follows:
I think the inability to pay for this service could be one of the obstacles to receiving this service. The second is a lack of understanding about these mHealth services, so first giving information about mHealth services to patients is very important. (KI-15)
Lack of awareness about mHealth services
This study indicated that a lack of awareness about mHealth services is a barrier toward willingness to receive mHealth services among patients with diabetes on chronic follow-up.
A nurse who is 36 years old stated:
Patients with diabetes have no awareness about utilizing technology like mobile phone to receive health services. A lot of peoples even do not have any idea regarding mobile health services or they have no information or knowledge about mHealth services. (KI-14).
Lack of knowledge about mHealth services
This study also indicated that a lack of knowledge about mHealth services is a barrier toward willingness to receive mHealth services among patients with diabetes on chronic follow-up.
A 55-year-old male patient also expressed his idea as:
Lack of knowledge is one of the problems. Because, for example, if you ask me something about the disease, it is difficult for me to understand it because I don’t know the medical words that have no direct meaning to translate to our country’s language. Due to this reason, it could be difficult to apply this service to us. (IDI-9)
Resistance to accept new services
Again, the finding also indicated that a resistance to accept this new service is among the barriers toward willingness to receive mHealth services.
A 30-year-old male doctor shared his experience as follows:
What I think could be a problem is that when you introduce this new service, there could be a resistance to accept this service. For instance, I don’t use Telebir [an application used for digital money services] even though I have access and could possibly use it, but I am not interested in using this service. So, this could also be other challenges. (KI-12)
Low satisfaction toward mobile phone services
The study also showed that low satisfaction toward mobile phone services is a barrier toward willingness to receive mHealth services. A 65-year-old male patient described his experience as follows:
In terms of receiving health care services over mobile phone, it could be challenging for me to believe in being treated over the phone only without physical contact between patient and doctor. Because, as you know, I do not think it is worthwhile to be treated unless I have seen and reached out by health care professionals. (IDI-5).
Difficulty of applying uniformly to all patients
The study also identified the difficulty of applying uniformly to all patients as a barrier toward willingness to receive mHealth services. A 65-year-old male patient stated:
I think this will take a lot of time to implement it. Frist there could be a few numbers of patients who can read and use the application to use these services. Lack of knowledge to read and write the text messages and also there could be lack of understanding of the medical terms could be the major problems to implement these services. If we go down to those who come from rural area there is low proportion of people who can read and write. (KII-11).
Potential lack of appropriate counseling from health professionals
From the findings, we see that a lack of appropriate counseling from HCPs is one of the barriers toward willingness to receive mHealth services. A 42-year-old male patient stated his experience as follows:
There is no doctor who has paid attention to side effects. It is through our efforts that we know the follow-up situations. Most doctors, as far as I have seen, do not add or inform patients of the potential side effects of medications. They do not care about us. People hear about the side effects from outside as rumors. But it’s bad to do that. It is irrelevant to reduce medication amounts for fear of side effects because one is harming oneself. And these conditions exist. Of course, that is due to a lack of appropriate counseling from doctors. (IDI-1).
Lack of sufficient number of health professionals
The result also indicated that a lack of a sufficient number of HCPs is another barrier toward willingness to receiving mHealth services. A 30-year-old male medical doctor said that:
There is usually a lack of enough health care professionals to provide healthcare services. The proportion of healthcare professionals to patients in our country is very low; this could be the problem with the health system in our country. Even until this time, there are a lot of patients who are dying due to a lack of service because there are not enough healthcare professionals at the health facility. So, to implement this new service the number of health professionals should be increased. (KI-12)
Discussion
In this study, access to mobile phone and willingness to receive mHealth services among those who have access to mobile phones becomes 77.3% and (74.5%), respectively. Age, educational status, time to reach the health facility, presence of comorbidity, satisfaction with the health-care provider, and willingness to answer unknown calls were significantly associated with willingness to receive mHealth services.
Access to mobile phone in this study was 77.3%, which is consistent with a study conducted on patients with diabetes in northwestern Ethiopia, 77.8%,23 on chronically ill patients in North Central Honduras (78.2%)26 and on ART patients (76.2%) in northwestern Ethiopia.27 The exponential growth in the global distribution of cell phones may be the cause of this similarity.
However, access to mobile phones in this study is higher than studies conducted on hypertension in Bangladesh (61.6%),28 This discrepancy may be due to differences in study settings because this study has been conducted in major towns of the region, which make the respondents more accessible to mobile phones. Also, the difference in socioeconomic status between diabetes and HIV/AIDS patients may be another reason.
Additionally, access to mobile phones in this study is lower than in studies conducted on HIV/AIDS patients in northwest Ethiopia (85.5%), patients with diabetes in southern Ethiopia (91.4%), chronic disease patients in India (81.5%), and patients with diabetes in Nigeria (97.3%).21,29–31 This discrepancy may result from regional variations in socioeconomic level, health literacy, and the acceptance of technology’s positive effects on human health.
In this study, 74.5% of patients with diabetes who had access to a mobile phone were willing to receive mHealth services, which is comparable to a study done on patients with diabetes in northwestern Ethiopia (70.5%)23 and Nigeria (72.6%).21 However, it is higher than studies conducted on patients with diabetes in southern part of Ethiopia (59.1%),31 chronic disease patients in India (60%),30 and patients with diabetes in northern Ethiopia (47.1%).32 The discrepancy could be due to differences in socio-economic and digital technology awareness among study participants. Willingness to receive mHealth services was lower than in a study conducted on chronic illnesses conducted in North Central Honduras (80%).26 This difference might be due to the difference in the ICT development index and socioeconomic status across countries.
Having attended a formal education was positively associated with the willingness to receive mHealth services. This is a robust finding from numerous studies on various health programs, including ART patients, child immunization, and pregnant women receiving antenatal and prenatal care, which were carried out in the majority of LMICs.21,23,25–27,33 The observed association may be due to the likelihood that increased educational status will boost awareness of managing diabetes and provide greater access to a cell phone and mobile network.
Age is also another positively associated factor with willingness to receive mHealth services. This finding is in line with previous studies.25,27,33–35 The findings suggest that younger age groups are the most suitable for adopting mHealth services because they are more exposed to technology than older people.
Those who answer unknown calls are also positively associated with willingness to receive mHealth services. This finding is in line with study done in Ethiopia among ART patients.27 This similarity may be due to those who answer unknown calls and are mainly interested in using mHealth services.
Time taken to reach a health facility is also another significant associated factor for willingness to receive mHealth services. Those who traveled less than 1 hr were more likely to be willing compared with those who travel greater than 1 hr. This finding is in line with studies done in Ethiopia among ART patients.27 However, this contradicts a study conducted on patients with diabetes in northwestern Ethiopia.23 This disparity might be due to differences in study settings and characteristics of study participants.
Furthermore, those who are satisfied with health-care providers were more likely to be willing than those who did not satisfied. This result is consistent with studies conducted on patients with diabetes in northwestern Ethiopia.23 The similarity could be due to those who were satisfied with HCPs may have strong confidence on them that may increase their willingness.36 Also, those who have comorbidities were more likely to be willing than those who have no comorbidities. This is because comorbidity might have profound effects on patients’ ability to manage their self-care and pose significant barriers to lifestyle changes that make them less willing.
Qualitative study mainly focused on identification of barriers to receive mHealth services among patients with diabetes on chronic follow-up in public hospitals in eastern Ethiopia. The findings of this study identified infrastructure, health facilities, socioeconomic factors, and patients’ behavioral related barriers to receiving mHealth services.
This finding is consistent with a study conducted to explore facilitators of and barriers to mHealth adoption in older adults with heart failure, which shows barriers identified are lack of knowledge regarding how to use mHealth, cost of technology, and limited or fixed income.37 Our finding is also in line with the study conducted to assess barriers to and facilitators of the use of mobile health apps from a security perspective, indicating that the cost of apps and lack of security features in mHealth apps were barriers to adoption of mHealth apps.38
Limitations of the Study
This study is not without limitations. Since the study is institution-based, only respondents who came for follow-up services during data collection time were interviewed. Moreover, the study was done at hospitals in a major town administration, which would have overstated the accessibility of patients with diabetes to mobile phones and their willingness to receive mHealth services, which may affect the generalizability of the findings. The survey was also interviewer-administered, there may be a risk of social desirability bias that would have made more participants respond as willing. The willingness was also assessed only for those who already have a mobile phone, so the generalizability is restricted to only those who access mobile phones.
Conclusion
Our findings identify a high willingness to receive mHealth services among those who have access to mobile phones. Age, educational status, time to reach the health facility, presence of comorbidity, satisfaction with the health-care provider, and willingness to answer unknown calls are significantly associated with willingness to receive mHealth services.
Additionally, qualitative findings identified infrastructure, health facilities, socioeconomic factors, and patients’ behavioral factors as major barriers to receiving mHealth services. Therefore, implementing mHealth services for self-care, adherence support, and behavioral counseling and to improve patients’ knowledge might change the livelihood of patients with diabetes.
Abbreviations
BP, High Blood Pressure; DM, Diabetes mellitus; HCPs, Health-care providers; HICs, High-income countries; HTN, Hypertension; ICT, Information and Communication Technology; IDF, International diabetes federation; IDIs, In-depth Interviews; IT, Information Technology; KI, Key informants; LMICs, Low- and middle-income countries; mHealth, Mobile Health; MMR, Mixed-method research; NCDs, Non-Communicable Diseases; SMS, Short/text Message Service; SSA, sub-Saharan Africa; WHO, World Health Organization.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Ethical clearance and approval of the research protocol was obtained from Haramaya University, College of Health and Medical Sciences, Institutional Health Research Ethics Review Committee (IHRERC), and a formal support letter was written from College of Health and Medical Sciences to all concerned Regional State Health Bureau. The regional health bureau has written a letter of support to all concerned public hospitals. Furthermore, written informed consents were obtained from the participant health institutions and all health professionals. Also, informed written consent from all participants and a parent or legal guardian of participants under 18 years of age was obtained. Moreover, the participants’ informed consent included publication of anonymized responses. All the personal data concerning study participants kept were strictly confidential, and all the details of participants were anonymous during database preparation, ie, all the study subjects were coded with pseudo names. Furthermore, even during the data management and report drafting periods, ethical considerations were maintained. In general, the authors are pleased to inform that this study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We would like to express our sincere gratitude to the administrators of the hospitals where this study was conducted for their invaluable assistance and provision of necessary information and support. We would also like to extend our heartfelt thanks to the study participants for their willingness to take part in the research and for generously dedicating their time.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Haramaya University as part of master’s thesis project.
Disclosure
The authors declare that there is no conflict of interest.
References
1. Wei L, Bu X, Wang X, Liu J, Ma A, Wang T., Global burden of aortic aneurysm and attributable risk factors from 1990 to 2017. Global Heart 2021;16(1):
2. Cho N, Shaw J, Karuranga S, et al. IDF diabetes atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
3. Zeru MA, Tesfa E, Mitiku AA, Seyoum A, Bokoro T. Prevalence and risk factors of type-2 diabetes mellitus in Ethiopia: systematic review and meta-analysis. Sci Rep. 2021;11(1):21733. doi:10.1038/s41598-021-01256-9
4. Atlas D. International diabetes federation.
5. Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
6. Alwan AJ; Gsrond. Global status report on noncommunicable diseases 2010.
7. Abaza H, Marschollek M. mHealth application areas and technology combinations. Methods Inf Med. 2017;56(S 01):e105–e22. doi:10.3414/ME17-05-0003
8. Muralidharan S, Ranjani H, Anjana RM, Allender S, Mohan V. Mobile health technology in the prevention and management of type 2 diabetes. Indian J Endocrinol Metab. 2017;21(2):334. doi:10.4103/ijem.IJEM_407_16
9. WHO. PMTCT Strategic Vision 2010-2015: Preventing Mother-to-Child Transmission of HIV to Reach the UNGASS and Millennium Development Goals: Moving Towards the Elimination of Paediatric HIV; 2009.
10. Berkshire U; Consulting VWJWD. mHealth for development: the opportunity of mobile technology for healthcare in the developing world. Innov Technol Gov Glob. 2009;4:103-–118
11. Kamis K, Janevic MR, Marinec N, et al. A study of mobile phone use among patients with noncommunicable diseases in La Paz. Bolivia. 2015;11(1):1–10.
12. Driscoll KA, Corbin KD, Maahs DM, et al. Biopsychosocial aspects of weight management in type 1 diabetes: a review and next steps. Curr Diab Rep 2017;17(8):1–9.
13. Agboola S, Palacholla RS, Centi A, Kvedar J, Jethwani K, A multimodal mHealth intervention (featforward) to improve physical activity behavior in patients with high cardiometabolic risk factors: rationale and protocol for a randomized controlled trial. JMIR Res Protoc 2016;5(2):
14. Kebede MM, Zeeb H, Peters M, Heise TL, Pischke CR. Pischke CRJDt, therapeutics. Effectiveness of digital interventions for improving glycemic control in persons with poorly controlled type 2 diabetes: a systematic review, meta-analysis, and meta-regression analysis. Diabetes Technol Ther. 2018;20(11):767–782. doi:10.1089/dia.2018.0216
15. de Vries ST, Keers JC, Visser R, et al. Medication beliefs, treatment complexity, and non-adherence to different drug classes in patients with type 2 diabetes. J Psychosom Res. 2014;76(2):134–138. doi:10.1016/j.jpsychores.2013.11.003
16. Gadkari AS, McHorney CA. Medication nonfulfillment rates and reasons: narrative systematic review. Curr Med Res Opin. 2010;26(3):683–705. doi:10.1185/03007990903550586
17. Walz L, Pettersson B, Rosenqvist U, et al. Impact of symptomatic hypoglycemia on medication adherence, patient satisfaction with treatment, and glycemic control in patients with type 2 diabetes. Patient Preference Adherence. 2014;8:593. doi:10.2147/PPA.S58781
18. Karachaliou F, Simatos G, Simatou AJFi E. The challenges in the development of diabetes prevention and care models in low-income settings. Front Endocrinol. 2020;11:518. doi:10.3389/fendo.2020.00518
19. Tan X, Patel I, JJIip C. Review of the four item morisky medication adherence scale (MMAS-4) and eight item morisky medication adherence scale (MMAS-8). Innov Pharm. 2014;5(3):5.
20. Abebe SM, Berhane Y, Worku AJS. Barriers to diabetes medication adherence in North West Ethiopia. Springerplus. 2014;3:1–6.
21. Olamoyegun MA, Raimi TH, Ala OA, Fadare JO. Mobile phone ownership and willingness to receive mHealth services among patients with diabetes mellitus in South-West, Nigeria. Pan Afr Med J. 2020;37.
22. Habte BM, Kebede T, Fenta TG, HJBrn B. Explanatory models of adult patients with type 2 diabetes mellitus from urban centers of central Ethiopia. BMC Res Notes 2016;9(1):1–11.
23. Jemere AT, Yeneneh YE, Tilahun B, Fritz F, Alemu S, MJBo K. Access to mobile phone and willingness to receive mHealth services among patients with diabetes in Northwest Ethiopia: a cross-sectional study. BMJ Open. 2019;9(1):e021766. doi:10.1136/bmjopen-2018-021766
24. Mendoza G, Okoko L, Konopka S, Jonas EJA. African Strategies for Health Project. mHealth Compendium. 3. . World Health Organization; 2013.
25. Fikadie B, Willingness to receive short message service mHealth interventions to improve prenatal care among pregnant women attending antenatal care at health centers in Gondar town administration, northwest Ethiopia. 2017.
26. Piette JD, Mendoza-Avelares MO, Milton EC, Lange I, Fajardo R. Access to mobile communication technology and willingness to participate in automated telemedicine calls among chronically ill patients in Honduras. Telemed E-Health. 2010;16(10):1030–1041. doi:10.1089/tmj.2010.0074
27. Kebede M, Zeleke A, Asemahagn M, Fritz F. Willingness to receive text message medication reminders among patients on antiretroviral treatment in North West Ethiopia: a cross-sectional study. BMC Med Inf Decis Making. 2015;15(1). doi:10.1186/s12911-015-0193-z
28. Islam FMA, Lambert EA, Islam SMS, Hosen MA, Thompson BR, Lambert GW. Understanding the sociodemographic factors associated with intention to receive SMS messages for health information in a rural area of Bangladesh. BMC Public Health. 2021;21(1). doi:10.1186/s12889-021-12418-9
29. Abdi Y. The Use of Mobile Phone for HIV/AIDS Patients Clinical Attendance and Follow-Up in Art Providing Hospitals in Addis Ababa. Ethiopia: Addis Ababa University; 2011.
30. Ramachandran N, Srinivasan M, Thekkur P, Johnson P, Chinnakali P, Naik BN. Mobile phone usage and willingness to receive health-related information among patients attending a chronic disease clinic in rural Puducherry, India. J Diabetes Sci Technol. 2015;9(6):1350–1351. doi:10.1177/1932296815599005
31. Bogale B, Habte A, Haile D, Guteta M, Mohammed N, Gebremichael MA. Willingness to receive mHealth messages among diabetes patients at mizan tepi university teaching hospital: implications for digital health. Patient Prefer Adherence. 2022;16:1499–1509. doi:10.2147/PPA.S364604
32. Walle AD, Jemere AT, Tilahun B, et al. Intention to use wearable health devices and its predictors among diabetes mellitus patients in Amhara region referral hospitals, Ethiopia: using modified UTAUT-2 model. Inform Med Unlocked 2023;36:101157.
33. Endehabtu B, Weldeab A, Were M, Lester R, Worku A, Tilahun B. Mobile phone access and willingness among mothers to receive a text-based mHealth intervention to improve prenatal care in northwest Ethiopia: cross-sectional study. JMIR Pediatr Paren. 2018;1(2):e9. doi:10.2196/pediatrics.9618
34. Mekonnen ZA, Gelaye KA, Were MC, Tilahun B. Mothers intention to use mobile phone text message reminders for routine child vaccination in Northwest. 2020.
35. Zurovac D, Otieno G, Kigen S, et al. Ownership and use of mobile phones among health workers, caregivers of sick children and adult patients in Kenya: cross-sectional national survey. Glob Health. 2013;9(1):20. doi:10.1186/1744-8603-9-20
36. Alimena S, Air MEJMPo PA. Trust, satisfaction, and confidence in health care providers among student and professional dancers in France. Med Probl Perform Artists. 2016;31(3):166–173. doi:10.21091/mppa.2016.3030
37. Cajita MI, Hodgson NA, Lam KW, Yoo S, Han HR. Facilitators of and barriers to mHealth adoption in older adults with heart failure. CIN. 2018;36(8):376–382. doi:10.1097/CIN.0000000000000442
38. Byambasuren O, Beller E, Hoffmann T, Glasziou P; uHealth. Barriers to and facilitators of the prescription of mHealth apps in Australian general practice: qualitative study. JMIR mHealth uHealth. 2020;8(7):e17447. doi:10.2196/17447
 © 2023 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
© 2023 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.