Back to Journals » Nature and Science of Sleep » Volume 8
Which oropharyngeal factors are significant risk factors for obstructive sleep apnea? An age-matched study and dentist perspectives
Authors Ruangsri S, Jorns TP, Puasiri S, Luecha T, Chaithap C, Sawanyawisuth K ![]()
Received 15 September 2015
Accepted for publication 17 March 2016
Published 8 July 2016 Volume 2016:8 Pages 215—219
DOI https://doi.org/10.2147/NSS.S96450
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Steven Shea
Supanigar Ruangsri,1,2 Teekayu Plangkoon Jorns,1,2 Subin Puasiri,3 Thitisan Luecha,4 Chariya Chaithap,4 Kittisak Sawanyawisuth5,6
1Department of Oral Biology, Faculty of Dentistry, 2Neuroscience Research and Development Group (NRDG), 3Department of Community Dentistry, Faculty of Dentistry, 4Faculty of Dentistry, 5Department of Medicine, Faculty of Medicine, 6Research Center in Back, Neck, Other Joint Pain and Human Performance (BNOJPH), Khon Kaen University, Khon Kaen, Thailand
Objective: Obstructive sleep apnea (OSA) is a common sleep breathing disorder. Untreated OSA may lead to a number of cardiovascular complications. Dentists may play an important role in OSA detection by conducting careful oral examinations. This study focused on the correlation of oral anatomical features in Thai patients who presented with OSA.
Methods: We conducted a prospective comparative study at a sleep/hypertension clinic and a dental clinic at Khon Kaen University in Thailand. Patients with OSA were enrolled in the study, along with age-matched patients with non-OSA (controls). Baseline characteristics, clinical data, and oropharyngeal data of all patients were compared between the two groups. Oropharyngeal measurements included tongue size, torus mandibularis, Mallampati classification, palatal space, and lateral pharyngeal wall area. Multivariate logistic regression analysis was used to identify the factors associated with OSA.
Results: During the study period, there were 156 patients who met the study criteria; 78 were patients with OSA and the other 78 were healthy control subjects. In the OSA group, there were 43 males with a mean age of 53 (standard deviation 12.29) years and a mean BMI of 30.86 kg/mm2. There were 37 males in the control group with a mean age of 50 (standard deviation 12.04) years and a mean BMI of 24.03 kg/mm2. According to multivariate logistic analysis, three factors were perfectly associated with OSA, including torus mandibularis class 6, narrow lateral pharyngeal wall, and Mallampati class 4. There were two other significant factors associated with having OSA, namely, BMI and Mallampati classification. The adjusted odds ratios (95% confidence interval) of these two factors were 1.445 (1.017, 2.052) and 5.040 (1.655, 15.358), respectively.
Conclusion: Dentists may play an important role in the detection of OSA in patients with high BMI through careful oropharyngeal examination in routine dental treatment. A large torus mandibularis, Mallampati class 4, and a narrow lateral pharyngeal wall are important anatomical risk factors for OSA.
Keywords: obstructive sleep apnea, neck circumference, torus mandibularis, tongue size, Mallampati classification, palatal vault, lateral pharyngeal wall, hypertension
Introduction
The prevalence of obstructive sleep apnea (OSA) has been reported to be 2%–4% in the general population.1 It is a contributing factor for cardiovascular diseases such as hypertension, coronary artery disease, and stroke, as well as for traffic accidents and poor quality of life.2–4 Diagnosis of OSA can be made using polysomnography in patients who have an apnea–hypopnea index of more than five events per hour. Obesity is a major risk factor for OSA. Other risk factors are oral abnormalities such as macroglossia and a narrow pharynx.5 Early detection and treatment of OSA have been shown to reduce the risk of cardiovascular diseases and, thus, death from heart diseases, and to reduce the frequency of strokes.3
Dentists actually play an important role in OSA diagnosis and treatment. They see patients’ oral cavity in daily practice and can identify those who are at risk of OSA. In addition, oral appliances can be custom-made for OSA treatment. Several craniofacial factors have been reported to be important risk factors for OSA. Neck circumference of >17 inches (43.2 cm) in men and 16 inches (40.6 cm) in women increases the risk of OSA. Similarly, large tongue and Mallampati classification are also significant predictors of OSA. A small study from People’s Republic of China conducted with 15 patients with OSA showed that neck circumference and craniofacial measurements such as anterior superior hyoid to mandibular plane or the velum tip to the pharyngeal wall parallel to the Frankfurt horizontal were associated with OSA.6 These factors may require several landmarks and are not practical for clinical use. This study aimed to evaluate if any oropharyngeal parameters associated with OSA can be detected using methods that are more practical for a dentist.
Methods
This prospective study was a sleep/hypertension clinic, out patient unit, Department of Medicine, Faculty of Medicine and a dental clinic, out patient unit, Faculty of Dentistry, Khon Kaen University from August to October 2013. We compared the craniofacial factors of patients with OSA and patients with non-OSA. Patients diagnosed with OSA were consecutively enrolled at the sleep/hypertension clinic, while non-OSA controls were enrolled at the dental clinic.
The diagnosis of OSA was made based on the presence of apnea–hypopnea index greater than or equal to five events per hour. Age-matched controls were enrolled at the dental clinic after they were found to have a negative risk of OSA using the Berlin questionnaire.7 The age of each control subject matched to each patient was between ±3 years. Patients were also excluded if they were younger than 30 years of age, had no functional teeth, or had previously undergone surgical procedures to treat OSA. The study protocol was approved by the Khon Kaen University Institutional Ethics Committee of human research (HE561022).
Baseline characteristics, clinical data, and oropharyngeal data of all patients were collected. Neck circumference was measured over cricoid cartilage in a neutral position. Oropharyngeal evaluation included torus mandibularis, tongue size, Mallampati classification, palatal space, and lateral pharyngeal wall area. Details of each measurement were as follows.
Torus mandibularis is the hard tissue located at the lower mandible. According to the classification of Agbaje et al8 and Reichart et al,9 there are six levels of torus mandibularis identified by the diameter and location of the tori as follows:
- Level 1: diameter <6 mm on one side of lower mandible
- Level 2: diameter <6 mm on both sides of lower mandible
- Level 3: diameter of 6 mm to 2 cm on one side of lower mandible
- Level 4: diameter of 6 mm to 2 cm on both sides of lower mandible
- Level 5: diameter >2 cm on one side of lower mandible
- Level 6: diameter >2 cm on both sides of lower mandible
Tongue size as identified by Huynh et al’s classification by using tongue position and tongue scalloping was as follows10:
- Small tongue: tongue edge does not cover lower teeth in resting position.
- Normal tongue: tongue edge partially covers lingual cusps of lower teeth.
- Macroglossia: tongue edge covers more than half of lower teeth or scalloped tongue is seen.
Participants were asked to protrude their tongues as much as possible in a neutral sitting position and classified according to Mallampati classification11 as follows:
- Class 1: soft palate and uvula completely visible
- Class 2: soft palate and uvula partially visible
- Class 3: soft palate and base of uvula visible
- Class 4: only hard palate visible
Mallampati classification in each patient was assessed by one author (TL). TL and KS (a sleep medicine physician) were piloted 10 patients in Mallampati evaluation prior to the study. The kappa correlation score of both evaluators (TL and KS) was 0.9.
Palatal space was determined by palatal width and depth. The palatal width was measured by placing and folding a sterile hard paper between the inner gums of both upper first molars. This sterile hard paper was then measured with a ruler. The palatal width was classified according to Patel as narrow (<30 mm), normal (30–42 mm), and large palatal width (>42 mm).12 The palatal depth was measured by placing a sterile toothpick in the center of the previous position of the sterile hard paper, and the palatal width was measured to the top of the hard palate. The palatal depth was classified into one of three levels: short or shallow palatal depth (<15 mm), normal (15–20 mm), and deep palatal depth (>20 mm).
The lateral pharyngeal wall area was defined as either normal or narrow by using a tongue blade to compress the patient’s tongue. If no lateral soft tissue was found in the pharyngeal cavity, the lateral pharyngeal wall area was recorded as normal. If lateral soft tissue invaded the pharyngeal cavity, this was classified as narrow.13
Sample size calculation
A previous study showed that macroglossia had a prevalence of 41.2% and the odds ratio (OR) for OSA was 2.13 According to this data, the estimated prevalence of macroglossia in non-OSA population was 26%. With confidence of 95% and a power of 80%, the estimated sample size was 78 in each group (OSA and non-OSA groups).
Statistical analyses
Baseline and clinical characteristics of both patients with OSA and controls were analyzed using descriptive statistics. Wilcoxon rank sum/Student’s t-test and Fisher’s exact tests/chi-square test were applied to compare the differences in numbers and proportions between the two groups, respectively, when appropriate. P-values <0.05 were considered significant.
Univariate logistic regression analysis was applied to calculate the crude OR of individual variables for OSA. All clinically significant variables were included in subsequent multivariate logistic regression analyses. Analytical results were presented as crude OR, adjusted OR, and 95% confidence intervals. The goodness of fit of the multivariate logistic regression model was tested using the Hosmer–Lemeshow method. All data analysis was performed using STATA software (StataCorp LP, College Station, TX, USA).
Results
One hundred and fifty-six patients met the study criteria; of these, 78 were in the OSA group and the other 78 were control subjects. The OSA group patients had a mean age of 53.33 years and a mean BMI of 30.86 kg/m2; 43 of the patients were male. The control group subjects had a mean age of 50.40 years and a mean BMI of 24.03 kg/m2; 37 subjects were male in this group.
The OSA group displayed five different anatomical factors that differed from the control group, including neck circumference, palatal width, macroglossia, Mallampati classification, and narrowness of the lateral pharyngeal wall (Table 1). The OSA group had significantly larger neck circumference (41.02 vs 36.38 cm) and a higher proportion of subjects with wide palatal width (80.27% vs 42.31%), macroglossia (66.67% vs 19.23%), Mallampati class 4 (50.00% vs 14.10%), and narrow lateral pharyngeal wall (31.75% vs 0%) than the control group.
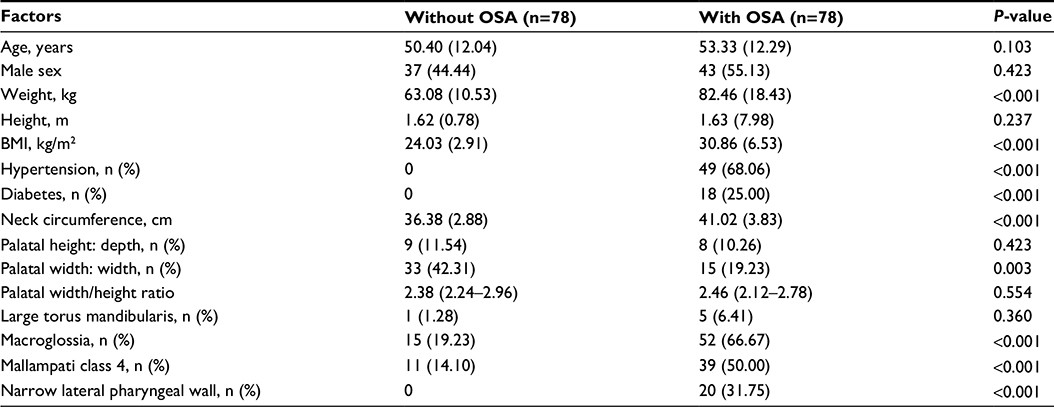 | Table 1 Comparison of clinical factors between patients without and with OSA Abbreviation: OSA, obstructive sleep apnea. |
According to multivariate logistic analysis, three factors were perfectly associated with OSA, including torus mandibularis class 6, narrow lateral pharyngeal wall, and Mallampati class 4. Two other factors that were also independently associated with OSA were BMI and Mallampati classification (Table 2).
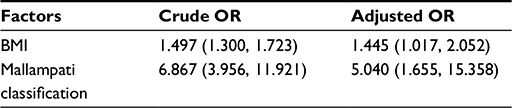 | Table 2 Significant factors associated with having OSA according to multivariate logistic regression analysis Notes: Data presented as OR (95% CI). The final model is adjusted for age, sex, neck circumference, palatal width/height ratio, torus mandibularis, and tongue size. Torus mandibularis class 6, narrow lateral pharyngeal wall, and Mallampati class 4 perfectly predicted OSA. The Hosmer-Lemeshow Chi-square test was 4.33 (P value 0.826). Abbreviations: OSA, obstructive sleep apnea; OR, odds ratio; CI, confidence interval. |
Discussion
Dentists can detect patients with OSA through oral examination in daily practice. First, redness of the soft palate and uvula area may be an evidence of snoring.14 If any of the following are present, OSA should be considered: torus mandibularis larger than 2 cm, narrow lateral pharyngeal wall, Mallampati class 4, or obesity. The first three factors perfectly predicted OSA by multivariate logistic regression analysis, indicating a very high risk of OSA.
Obesity is the main risk factor for OSA.14 In this study, we found that for each 1 kg/m2 BMI increase, risk factors for OSA increased by 1.5 times. Neck circumference of >40 cm in Asian populations is associated with OSA and obesity,15 but it was not an independent factor for OSA in this study. This may be explained by the greater effect of BMI compared to neck circumference.
Mallampati class 4 and narrow lateral pharyngeal wall,13 indicating a narrow oropharyngeal airway, suggest high risk of OSA. Previous studies have also shown that a narrow oropharyngeal space increases the risk of OSA.16–18 Tongue volume/oral cavity volume ratio was higher in patients with OSA compared with controls.17 The risk of OSA in subjects with Mallampati class 3 is five times higher than that in those with Mallampati class 2 (Table 2). Even though macroglossia is another factor indicating a narrow oropharyngeal cavity, it is not an independent factor for OSA after adjustments are made for other factors such as age, sex, and BMI (Table 2). These data suggest that only some oropharyngeal factors, and not all of them, are important risk factors for OSA.
Torus mandibularis is an anatomical variation that may be a risk factor for OSA. The prevalence of these tori may be different among different countries or ethnicities. The prevalence rates of tori in Thai and German populations were 9% and 2.4%, respectively.9 In this study, the overall prevalence of tori was 30.13% (47 subjects). Large tori mandibulares (level 6) were more common in patients with OSA than in control subjects (6.4% vs 1.3%). The proportion of subjects with large torus mandibularis was not statistically significant according to Fisher’s exact test. However, it perfectly predicted OSA according to multivariate logistic regression analysis. The latter statistical method is more robust, more reliable, and controls other confounders. In other words, large torus mandibularis (>2 cm) indicated high risk of OSA.
OSA group had lesser proportion of patients with wide palatal width compared with control group, as shown in Table 1 (19.23% vs 42.31%). This indicates that narrow palatal width may be more common in patients with OSA, as previously reported.12 However, after adjusting for other factors (Table 2), the palatal width/height ratio was not found to be an independent factor for OSA. Only Mallampati classification remained significant in the final model. We used the palatal ratio instead of either palatal width or palatal height in the model. The reason is that the palatal factor should be an area, not just only height or width. Also, using numeric values (palatal ratio) is more robust than categorical data (narrow or wide) when put in the statistical model.
The strength of this study was that both groups of patients were age matched, reducing confounding from age which is an important risk factor for OSA. There are several limitations in this study. Subjects were enrolled in the control group if they obtained a negative result on using the Berlin questionnaire. As a result, hypertension was one of the exclusion criteria and could not be included in the multivariate logistic analysis. Some oropharyngeal and physical factors were not included in this study, such as malocclusion or waist circumference.19–22 This study may not apply to other specific populations (ie, children who may not have fully developed anatomical structure).23–27 Further studies using a larger study population and looking at other risk factors such as malocclusion and torus palatinus are necessary to confirm our results.
Conclusion
Dentists may play an important role in the detection of OSA in hypertensive or high BMI patients through routine oropharyngeal examination. Large torus mandibularis, Mallampati class 4, and narrow lateral pharyngeal wall are important anatomical risk factors for OSA.
Acknowledgments
The authors would like to thank Mr Dylan Southard for his English editing of the manuscript through Publication Clinic KKU, Thailand, the Thailand Research Fund (IRG5780016), and TRF Senior Research Scholar Grant from the Thailand Research Fund (TRF grant number RTA5880001), and by the Higher Education Research Promotion and National Research University Project of Thailand, Office of the Higher Education Commission, Thailand, through the Health Cluster (SHeP-GMS), Khon Kaen University.
Disclosure
The authors report no conflicts of interest in this work.
References
Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328(17):1230–1235. | ||
Botros N, Concato J, Mohsenin V, Selim B, Doctor K, Yaggi HK. Obstructive sleep apnea as a risk factor for type 2 diabetes. Am J Med. 2009;122(12):1122–1127. | ||
Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046–1053. | ||
Dyken ME, Im KB. Obstructive sleep apnea and stroke. Chest. 2009;136(6):1668–1677. | ||
Maniglia AJ. Sleep apnea and snoring, an overview. Ear Nose Throat J. 1993;72(1):16, 19. | ||
Chang ET, Shiao GM. Craniofacial abnormalities in Chinese patients with obstructive and positional sleep apnea. Sleep Med. 2008;9(4):403–410. | ||
Pereira EJ, Driver HS, Stewart SC, Fitzpatrick MF. Comparing a combination of validated Questionnaires and level III portable monitor with polysomnography to diagnose and exclude sleep apnea. J Clin Sleep Med. 2013;9(12):1259–1266. | ||
Agbaje JO, Arowojolu M, Kolude B, Lawoyin JO. Torus palatinus and torus mandibularis in a Nigerian population. Afr J Oral Health. 2005;2:30–36. | ||
Reichart PA, Neuhaus F, Sookasem M. Prevalence of torus palatinus and torus mandibularis in Germans and Thai. Community Dent Oral Epidemiol. 1988;16(1):61–64. | ||
Huynh NT, Morton PD, Rompré PH, Papadakis A, Remise C. Associations between sleep-disordered breathing symptoms and facial and dental morphometry, assessed with screening examinations. Am J Orthod Dentofacial Orthop. 2011;140(6):762–770. | ||
Mallampati SR, Gatt SP, Gugino LD, Desai SP, Waraksa B, Freiberger D, Liu PL. A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J. 1985;32(4):429–34. | ||
Patel M. A study of the hard palate in the skulls of central Indian population. Int J Pharm Bio Sci. 2012;3(2):527–533. | ||
Schellenberg JB, Maislin G, Schwab RJ. Physical findings and the risk for obstructive sleep apnea. The importance of oropharyngeal structures. Am J Respir Crit Care Med. 2000;162(2 Pt 1):740–748. | ||
Victor LD. Obstructive sleep apnea. Am Fam Physician. 1999;60(8):2279–2286. | ||
Khoo SM, Tan WC, Ng TP, Ho CH. Risk factors associated with habitual snoring and sleep-disordered breathing in a multi-ethnic Asian population: a population-based study. Respir Med. 2004;98(6):557–566. | ||
Weiss TM, Atanasov S, Calhoun KH. The association of tongue scalloping with obstructive sleep apnea and related sleep pathology. Otolaryngol Head Neck Surg. 2005;133(6):966–971. | ||
Iida-Kondo C, Yoshino N, Kurabayashi T, Mataki S, Hasegawa M, Kurosaki N. Comparison of tongue volume/oral cavity volume ratio between obstructive sleep apnea syndrome patients and normal adults using magnetic resonance imaging. J Med Dent Sci. 2006;53(2):119–126. | ||
Rodrigues MM, Dibbern RS, Goulart CW. Nasal obstruction and high Mallampati score as risk factors for obstructive sleep apnea. Braz J Otorhinolaryngol. 2010;76(5):596–599. | ||
Perillo L, Esposito M, Caprioglio A, Attanasio S, Santini AC, Carotenuto M. Orthodontic treatment need for adolescents in the Campania region: the malocclusion impact on self-concept. Patient Prefer Adherence. 2014;8:353–359. | ||
Santamaria F, Esposito M, Montella S, et al. Sleep disordered breathing and airway disease in primary ciliary dyskinesia. Respirology. 2014;19(4):570–575. | ||
Perillo L, Esposito M, Contiello M, Lucchese A, Santini AC, Carotenuto M. Occlusal traits in developmental dyslexia: a preliminary study. Neuropsychiatr Dis Treat. 2013;9:1231–1237. | ||
Carotenuto M, Bruni O, Santoro N, Del Giudice EM, Perrone L, Pascotto A. Waist circumference predicts the occurrence of sleep-disordered breathing in obese children and adolescents: a questionnaire-based study. Sleep Med. 2006;7(4):357–361. | ||
Esposito M, Antinolfi L, Gallai B, et al. Executive dysfunction in children affected by obstructive sleep apnea syndrome: an observational study. Neuropsychiatr Dis Treat. 2013;9:1087–1094. | ||
Carotenuto M, Gimigliano F, Fiordelisi G, Ruberto M, Esposito M. Positional abnormalities during sleep in children affected by obstructive sleep apnea syndrome: the putative role of kinetic muscular chains. Med Hypotheses. 2013;81(2):306–308. | ||
Carotenuto M, Esposito M, Parisi L, et al. Depressive symptoms and childhood sleep apnea syndrome. Neuropsychiatr Dis Treat. 2012;8:369–373. | ||
Carotenuto M, Esposito M, Pascotto A. Facial patterns and primary nocturnal enuresis in children. Sleep Breath. 2011;15(2):221–227. | ||
Carotenuto M, Santoro N, Grandone A, et al. The insulin gene variable number of tandem repeats (INS VNTR) genotype and sleep disordered breathing in childhood obesity. J Endocrinol Invest. 2009;32(9):752–755. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.