Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
When Resectability Emerges After Systemic Therapy in Hepatocellular Carcinoma: A Proposed Response-Guided Consolidation Framework
Received 3 April 2026
Accepted for publication 14 May 2026
Published 4 June 2026 Volume 2026:13 613934
DOI https://doi.org/10.2147/JHC.S613934
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David Gerber
Yuan Cheng,1 Kunlin Xie2– 4
1Department of Medical Oncology, Jinling Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, Jiangsu, People’s Republic of China; 2Department of General Surgery, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 3Liver Transplant Center, Transplant Center, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 4Laboratory of Hepatic AI Translation, Frontiers Science Center for Disease-Related Molecular Network, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China
Correspondence: Kunlin Xie, Email [email protected]
Abstract: Immune checkpoint inhibitor–based combination therapies have increased the likelihood that a subset of patients with initially unresectable hepatocellular carcinoma (HCC) may achieve sufficient tumor regression to become technically resectable However, when resectability emerges systemic therapy, the optimal next step remains uncertain. Surgical resection may eradicate residual macroscopic disease, whereas continued systemic therapy may help maintain control of occult micrometastatic disease. In this review, we summarize the available evidence on surgical consolidation after conversion and propose a conceptual response-guided consolidation framework to support post-conversion decision-making. The current evidence base remains dominated by retrospective comparative studies, although early randomized data have recently emerged in selected populations. Overall, surgical consolidation appears feasible and may improve progression-related outcomes in carefully selected responders, but definitive survival benefit across all response categories remains unproven. Within the proposed framework, partial response appears to represent the most consistent clinical scenario supporting surgery, stable disease should be interpreted as a heterogeneous category requiring further biological and radiographic discrimination, and complete response remains the most uncertain setting in which surgery may not always be necessary. Beyond radiographic response alone, pathological response and biomarker-based predictive enrichment may help refine future selection strategies. We therefore suggest that post-conversion resectability should be viewed not simply as a technical surgical endpoint, but as a therapeutic decision point requiring multidisciplinary assessment of anatomical feasibility, response depth and durability, hepatic reserve, and biological risk. This proposed framework is intended as a practical interim model rather than an established clinical standard and requires prospective validation.
Keywords: hepatocellular carcinoma, conversion therapy, surgical consolidation, resectability, systemic therapy, response-guided framework, partial response, complete response
Introduction
The therapeutic landscape of hepatocellular carcinoma (HCC) has changed substantially in the era of immune checkpoint inhibitor–based combination therapies. Phase III trials have demonstrated improved objective response rates and survival compared with prior standards, thereby increasing the proportion of patients who achieve meaningful tumor regression.1–3 As a result, a subset of patients with initially unresectable disease may become technically resectable after treatment, a process commonly referred to as conversion to resectability.4–7
While this development represents an important therapeutic advance, it has also created a new clinical dilemma. When systemic therapy renders disease technically resectable, should surgery be undertaken as consolidation to eradicate residual macroscopic disease, or should systemic therapy be continued to maintain tumor control? Current international guidelines acknowledge the possibility of downstaging and conversion, but provide limited direction regarding this specific post-conversion decision point.8,9 Consequently, management remains heterogeneous across institutions and multidisciplinary teams.
This uncertainty reflects the gap between technical feasibility and clinical decision-making. Although tumor shrinkage may permit R0 resection (complete macroscopic and microscopic removal with negative margins), it does not necessarily imply eradication of viable tumor cells or occult micrometastatic disease. At the same time, prolonged systemic therapy carries cumulative toxicity, financial burden, and uncertainty regarding optimal duration.10–13 Against this background, a structured approach to post-conversion management is needed. In this review, we summarize the available clinical evidence on surgical consolidation after conversion and propose a response-guided, conceptual framework to support multidisciplinary decision-making when resectability emerges after systemic therapy in HCC.
Redefining Resectability in the Systemic Therapy Era
The advent of effective systemic therapies has fundamentally altered this landscape. Tumor burden and vascular invasion, and occasionally limited extrahepatic disease, may regress under treatment, converting disease previously deemed unresectable into technically resectable status. Downstaging and conversion are increasingly reported in contemporary cohorts, particularly with immune checkpoint inhibitor–based combinations.4–7 Resectability has therefore evolved from a baseline classification to a dynamic state that may emerge during the course of therapy.
However, the emergence of technical resectability after systemic therapy does not necessarily indicate durable oncologic control. Technical resectability reflects the anatomical possibility of complete macroscopic removal, whereas biological eradication implies elimination of viable tumor cells and suppression of microscopic disease. These two concepts may not fully coincide. Post-conversion surgical series have shown that radiographic response does not uniformly predict pathological clearance, underscoring the distinction between technical feasibility and biological response.14,15
In the systemic therapy era, resectability should therefore be viewed not simply as a surgical endpoint, but as a therapeutic decision point. It marks a stage at which anatomical feasibility, depth and durability of response, hepatic reserve, and overall disease biology must be reconsidered together. This distinction forms the conceptual basis for a response-guided consolidation strategy.
Current Clinical Evidence for Surgical Consolidation After Conversion
Surgical Consolidation After Systemic Therapy–Induced Conversion
Evidence directly addressing whether surgical resection should be performed after systemic therapy renders hepatocellular carcinoma (HCC) technically resectable remains limited but is gradually accumulating.
Several multicenter retrospective cohorts have evaluated patients with initially unresectable HCC who achieved objective response or disease control following immune checkpoint inhibitor–based systemic therapy and subsequently met criteria for curative-intent resection.10,14,16 In these studies, outcomes of patients undergoing surgical consolidation were compared with those of responders who continued systemic therapy without surgery.
Across analyses employing multivariable adjustment or propensity score matching, surgical resection after systemic therapy has been associated with improved progression-related endpoints. Hazard ratios for recurrence or progression in resected patients have generally ranged between approximately 0.5 and 0.7 in adjusted models.10,13 Median recurrence-free survival frequently exceeded 18–24 months in surgical cohorts, compared with approximately 8–14 months among non-surgically managed responders.5,10,17
Overall survival findings have been more heterogeneous but directionally similar. In cohorts enriched for patients achieving partial response (PR), median overall survival in resected patients often exceeded 30 months, whereas patients continuing systemic therapy alone demonstrated shorter survival durations.10,11,17 However, these comparisons are inherently subject to selection bias, as surgical candidates typically retained preserved liver function and favorable performance status.
Prospective evidence remains sparse. A recent phase III study enrolled patients with macrovascular invasion who achieved disease control after first-line immunotherapy-based therapy and were subsequently deemed resectable.13 Participants were randomized to surgical resection followed by maintenance therapy versus continued systemic therapy alone. The primary endpoint of time to treatment failure favored the surgical arm (hazard ratio approximately 0.6), whereas overall survival data were immature at the time of reporting. Although limited to a defined subgroup, this trial represents the first randomized comparison in the post-conversion setting.
Collectively, available systemic therapy–based studies suggest that surgical consolidation after conversion is feasible and may improve progression-related outcomes in selected responders. Definitive survival benefit across all response categories, however, remains unproven.
Evidence From Multimodal Downstaging Strategies
Data from locoregional downstaging strategies provide additional, although indirect, insight into post-conversion management. In a retrospective TACE cohort of 831 initially unresectable patients, 82 were successfully downstaged to resectable disease; among these, patients who underwent salvage resection had longer median overall survival than those who continued TACE alone (49 vs 31 months; HR 0.337, 95% CI 0.184–0.616), suggesting that local curative treatment may confer additional benefit after successful downstaging.18
Similarly, retrospective studies of Y-90 radioembolization have shown that a subset of initially unresectable patients can be converted to resection or transplantation, with encouraging long-term survival observed in those who ultimately undergo curative-intent treatment.19–21
However, these studies involve heterogeneous treatment paradigms and highly selected populations, and they do not isolate the independent effect of systemic therapy–induced response. Accordingly, they should be viewed as supportive and hypothesis-generating rather than definitive evidence for the specific decision node of surgery versus continued systemic therapy after systemic conversion.10,22
Evidence Landscape
Overall, current data indicate that technical resectability can be achieved after systemic or multimodal therapy in a subset of patients. Surgical consolidation in selected responders is associated with favorable progression-related outcomes, but most evidence derives from retrospective analyses and remains vulnerable to selection bias. Randomized validation across broader response strata is limited, underscoring the need for structured, biologically informed decision-making after conversion. The principal direct comparative studies informing this decision point are summarized in Table 1.
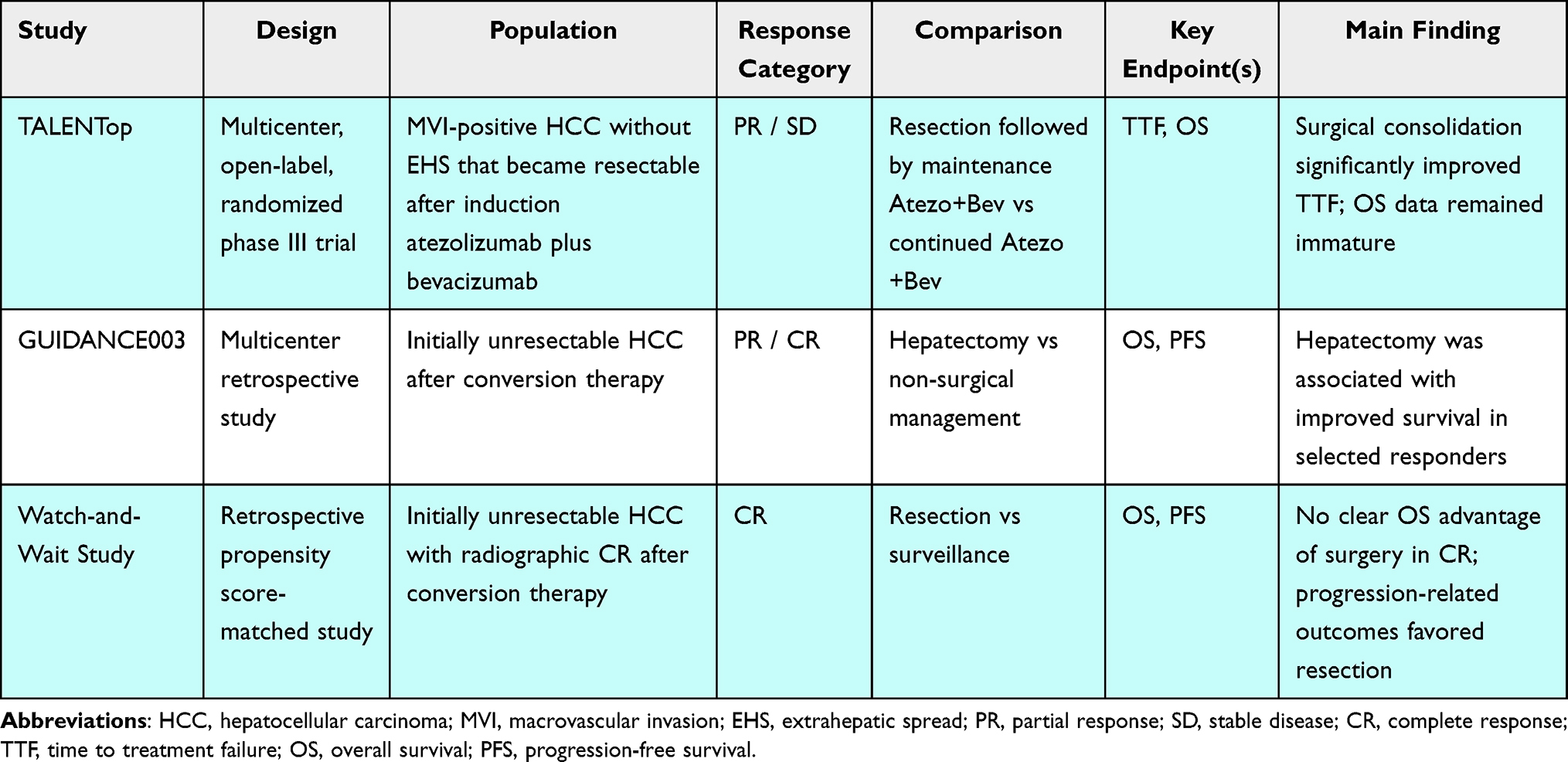 |
Table 1 Direct Comparative Studies of Surgical Versus Non-Surgical Management After Conversion in HCC |
A Response-Guided Consolidation Framework
When resectability emerges after systemic therapy in hepatocellular carcinoma, the central question is not merely whether surgery is technically feasible, but whether surgical consolidation is biologically and clinically justified. Given the heterogeneity of treatment response, residual tumor burden, and underlying disease biology, a uniform strategy is unlikely to be appropriate. Instead, consolidation decisions should be informed by both the depth and durability of response. On this basis, we propose a response-guided, conceptual framework structured around three principal response categories: stable disease (SD), partial response (PR), and complete response (CR). This framework is intended to support multidisciplinary discussion and hypothesis generation, rather than to function as a validated clinical algorithm.
Stable Disease: A Heterogeneous Category
Stable disease (SD) after systemic therapy should not be regarded as a biologically uniform state. Although SD does not meet formal criteria for objective response, it encompasses a broad spectrum of tumor behavior and does not necessarily indicate treatment resistance. In particular, SD with measurable tumor shrinkage may differ meaningfully from SD with slight interval growth or no meaningful change. Conceptually, SD accompanied by shrinkage may reflect biological sensitivity closer to partial response, whereas SD with interval enlargement may suggest emerging resistance.23
This distinction is increasingly supported by HCC-specific evidence. A recent study showed that patients with SD and tumor shrinkage could still derive benefit from surgery after immune-based therapy, whereas those with SD without shrinkage did not appear to benefit to the same extent.24
Accordingly, surgical consolidation in SD should remain individualized. SD alone should neither mandate nor automatically preclude resection; rather, decisions should integrate the direction and durability of tumor change, adequacy of hepatic reserve, technical feasibility, and the broader clinical context.
Partial Response: The Most Consistent Clinical Scenario
Partial response (PR) appears to represent the most clinically persuasive setting for surgical consolidation. Unlike SD, PR reflects unequivocal tumor regression and therefore provides stronger evidence of biological sensitivity to systemic therapy. Unlike complete response, however, PR still implies the presence of radiographically visible residual disease, leaving a clear target for local eradication.10,24,25
This combination of demonstrated systemic sensitivity and persistent macroscopic tumor burden is what makes PR particularly relevant to consolidation surgery. In this setting, resection is not intended to replace systemic therapy, but to complement it: systemic treatment has already shown activity against occult disease, while surgery may remove residual viable tumor that remains anatomically resectable As discussed in Section 3.1, the currently available post-conversion evidence most consistently suggests a progression-related benefit of surgery in responder populations, and this signal appears most persuasive in cohorts enriched for PR.10,16,25
Thus, in patients with preserved liver function, technically resectable disease, and acceptable operative risk, PR after systemic therapy may represent the most defensible context in which surgical consolidation can be considered. Nevertheless, PR alone should not be viewed as an automatic indication for resection; durability of response, vascular involvement, anticipated margin status, future liver remnant, and patient preference should all remain integral to multidisciplinary decision-making.
Complete Response: The Unresolved Scenario
Radiographic complete response (CR) introduces a different and less settled question. Although CR reflects maximal imaging response, radiographic disappearance does not uniformly equate to pathological eradication, and residual viable tumor may still be present despite imaging-defined CR.11,14,15
At the same time, the incremental value of surgery in CR populations remains uncertain. In the watch-and-wait versus resection study, patients who achieved radiographic CR had broadly comparable overall survival between strategies, although progression-related outcomes favored surgery; among those who achieved clinical complete response, survival outcomes were similar between surgical and non-surgical management.11 An earlier multicenter study reached a similar conclusion, suggesting that salvage hepatectomy may not be essential for at least some patients with clinical complete response, particularly when surgical risk is substantial.26
Taken together, these findings suggest that CR is prognostically favorable but does not automatically imply that surgery is required. In selected patients with durable CR, preserved liver function, and favorable baseline characteristics, continued systemic therapy or close surveillance may be reasonable alternatives. Conversely, surgery may still be considered when uncertainty regarding residual viable disease persists or when baseline high-risk features raise concern for relapse. At present, the available evidence does not support a uniform recommendation either for or against surgical consolidation in CR populations.
Integrating Response with Clinical Context
Across response strata, consolidation decisions should integrate at least three domains: (1) depth and durability of response, (2) technical feasibility together with sufficient hepatic reserve, and (3) baseline tumor biology and patient-specific operative risk. Resectability should therefore be viewed as a therapeutic inflection point rather than an automatic trigger for surgery. Importantly, the available evidence suggests that the benefit of surgery is most convincing in biologically sensitive but residually measurable disease, whereas its value is less certain in imaging-defined complete response and absent in some biologically unfavorable SD subsets.10–13,24,26
This framework is intended to support multidisciplinary decision-making rather than define a rigid algorithm. Given that much of the current evidence remains retrospective and vulnerable to selection bias, individualized interpretation remains essential until more mature randomized data become available.13,25 The proposed response-guided framework is illustrated in Figure 1.
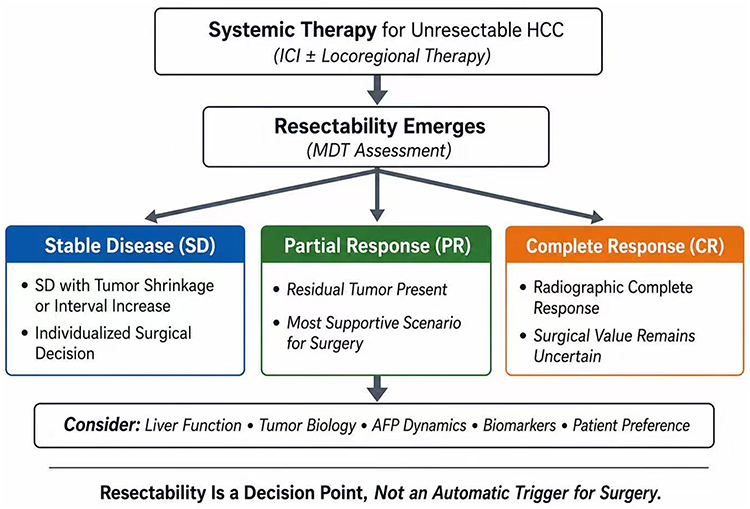 |
Figure 1 Response-Guided Consolidation Framework After Systemic Therapy–Induced Resectability in HCC. |
Beyond Radiographic Response: Pathologic Depth and Predictive Enrichment
The preceding sections suggest that surgical consolidation may confer meaningful benefit in selected patients after conversion. However, reliance on categorical radiographic response alone is insufficient to determine which patients are most likely to benefit from surgery. If surgical advantage is concentrated in biologically favorable subsets, more precise indicators of residual disease and relapse risk are required.
Pathologic Response and the Limits of Imaging
Across post-conversion surgical cohorts in HCC, pathologic response—particularly pathologic complete response (pCR)—has been consistently associated with favorable recurrence-free and overall survival. Patients achieving pCR demonstrate substantially lower recurrence risk than those with residual viable tumor.27–29
Importantly, radiographic complete response does not reliably predict pathological complete response. Residual viable tumor has been documented in a proportion of patients classified as imaging-defined CR, whereas extensive pathological necrosis may also be observed in some patients categorized as PR.30,31 This discordance highlights a central limitation of imaging-based assessment: radiographic clearance does not necessarily indicate biological eradication. Similar observations have also been reported across HCC27–29 and other solid tumors treated with modern systemic therapy, where pathological response may correlate more closely with long-term outcome than radiographic response alone.32 At present, pCR remains a postoperative endpoint rather than a preoperative decision tool. Its principal value lies in underscoring the importance of biological response depth, rather than serving as a sufficiently accurate marker for surgical selection before resection.
Predictive Enrichment Beyond RECIST
If surgical benefit depends on residual viable disease and relapse risk, post-conversion decision-making should extend beyond RECIST-based (Response Evaluation Criteria in Solid Tumors) categorization alone. Several complementary strategies are under investigation, although none is currently validated for routine surgical selection in this setting.
Advanced imaging approaches, including diffusion-weighted MRI parameters and CT-based radiomic models, have been explored as surrogates of tumor viability, but standardized thresholds and prospective validation remain limited.33
Serum biomarker kinetics, particularly dynamic changes in alpha-fetoprotein (AFP), have also been associated with treatment response and pathologic regression; however, specificity remains insufficient for independent surgical decision-making.15,31
Molecular indicators, such as circulating tumor DNA and minimal residual disease assays, are increasingly being studied as markers of residual tumor burden. Early data in HCC and other malignancies suggest prognostic relevance, but integration into routine post-conversion algorithms remains investigational.34,35
Integrated predictive models incorporating baseline tumor characteristics, response depth, and biomarker data are also emerging, yet most have been developed in upfront resection or exploratory cohorts rather than specifically in post-conversion populations.30,33,36
At present, no single modality reliably predicts pathological clearance or definitively identifies patients most likely to derive incremental benefit from surgery after conversion.
Clinical Perspective
Given the limitations of imaging-based assessment and the prognostic significance of pathological response, post-conversion decision-making should move toward biologically informed risk stratification rather than reliance on categorical response alone. Prospective studies embedding translational biomarkers and standardized pathological endpoints are essential to validate predictive enrichment strategies in this setting.
Future Directions and Conclusions
The increasing frequency with which resectability emerges after systemic therapy marks a meaningful transition in the management of hepatocellular carcinoma. What was once a binary classification of resectable versus unresectable disease has evolved into a dynamic continuum shaped by treatment response. This evolution has created a new clinical decision point for which evidence-based guidance remains incomplete.
Current data suggest that surgical consolidation may provide meaningful benefit in selected responders, particularly those with biologically sensitive but residually measurable disease. However, the evidence base remains dominated by retrospective studies, despite the recent emergence of randomized data in selected populations.10,11,13 Response definitions remain heterogeneous, and robust validation across predefined response strata is still limited. Accordingly, current observations should not be interpreted as establishing a universal standard of care, and individualized multidisciplinary decision-making remains essential.
Future research should address three priorities. First, prospective trials specifically comparing surgical consolidation with continued systemic therapy across predefined response categories are needed. Second, standardized pathological reporting, including harmonized definitions of pCR and major pathological response, should be incorporated into post-conversion studies to improve correlation between radiographic and biological response. Third, translational integration is critical. Biomarkers capable of estimating residual viable disease, such as molecular minimal residual disease assessment or validated imaging surrogates, may enable more rational predictive enrichment.
Equally important is recognition of the multidisciplinary nature of these decisions. Hepatic reserve, operative risk, baseline tumor burden, and patient preference must remain integral components of management. Resectability should therefore be viewed not as an automatic trigger for surgery, but as a decision node requiring synthesis of anatomical feasibility and biological risk.
In summary, the post-conversion setting in HCC represents an emerging and clinically relevant domain in which treatment paradigms are still being defined. The response-guided framework proposed here should be regarded as a conceptual and pragmatic interim model to support clinical reasoning, rather than an established clinical standard. Prospective validation, randomized evidence, and biomarker-guided patient selection will determine whether surgical consolidation ultimately becomes a selective standard or remains an individualized strategy in the systemic therapy era.
Funding
This work was funded by the Sichuan Provincial Science and Technology Plan (Key Research Projects, No. 2024YFFK0211), the Sichuan Province Health Care Research Project (No. 2025-114) and the Sichuan University “From 0 to 1” Innovative Research Project (No. 2023SCUH0059).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–8. doi:10.1056/NEJMoa1915745
2. Abou-Alfa GK, Lau G, Kudo M, et al. Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. NEJM Evid. 2022;1(8):EVIDoa2100070. doi:10.1056/EVIDoa2100070
3. Qin S, Chan SL, Gu S, et al. Camrelizumab plus rivoceranib versus sorafenib as first-line therapy for unresectable hepatocellular carcinoma (CARES-310): a randomised, open-label, international Phase 3 study. Lancet. 2023;402(10408):1133–1146. doi:10.1016/S0140-6736(23)00961-3
4. Yi Y, Sun BY, Weng JL, et al. Lenvatinib plus anti-PD-1 therapy represents a feasible conversion resection strategy for patients with initially unresectable hepatocellular carcinoma: a retrospective study. Front Oncol. 2022;12:1046584. doi:10.3389/fonc.2022.1046584
5. Xu B, Zhu XD, Shen YH, et al. Criteria for identifying potentially resectable patients with initially oncologically unresectable hepatocellular carcinoma before treatment with lenvatinib plus an anti-PD-1 antibody. Front Immunol. 2022;13:1016736. doi:10.3389/fimmu.2022.1016736
6. Zhu XD, Huang C, Shen YH, et al. Hepatectomy after conversion therapy using tyrosine kinase inhibitors plus anti-PD-1 antibody therapy for patients with unresectable hepatocellular carcinoma. Ann Surg Oncol. 2023;30(5):2782–2790. doi:10.1245/s10434-022-12530-z
7. Shimose S, Iwamoto H, Shirono T, et al. The impact of curative conversion therapy aimed at a cancer-free state in patients with hepatocellular carcinoma treated with atezolizumab plus bevacizumab. Cancer Med. 2023;12(11):12325–12335. doi:10.1002/cam4.5931
8. Vogel A, Meyer T, Sapisochin G, Salem R, Saborowski A. Hepatocellular carcinoma. Lancet. 2022;400(10360):1345–1362. doi:10.1016/S0140-6736(22)01200-4
9. Reig M, Sanduzzi-Zamparelli M, Forner A, et al. BCLC strategy for prognosis prediction and treatment recommendations: the 2026 update. J Hepatol. 2026;84(3):631–654. doi:10.1016/j.jhep.2025.10.020
10. Yang DL, Peng N, Nong JL, et al. Survival benefit of hepatectomy after complete or partial response to conversion therapy in unresectable hepatocellular carcinoma (GUIDANCE003): a multicenter study. Liver Cancer. 2025;14(6):687–703. doi:10.1159/000546052
11. Li B, Wang C, He W, et al. Watch-and-wait strategy vs resection in patients with radiologic complete response after conversion therapy for initially unresectable hepatocellular carcinoma: a propensity score-matching comparative study. Int J Surg. 2024;110(5):2545–2555. doi:10.1097/JS9.0000000000001155
12. Zhou Y, Wang H, Wu J, et al. Conversion resection or direct resection for patients with intermediate-stage hepatocellular carcinoma: a multicentre study. Liver Cancer. 2025:1–15. Epub ahead of print. PMID: 41415919; PMCID: PMC12711257. doi:10.1159/000549684
13. Sun H, Fan J, Shen F, et al. Liver resection versus continued atezolizumab plus bevacizumab in locally advanced hepatocellular carcinoma after atezolizumab/bevacizumab treatment (TALENTop): a multicenter, open-label, randomized phase III trial. Ann Oncol. 2025;36(suppl 5):1469MO. doi:10.1016/j.annonc.2025.08.2099
14. Yang DL, Yan YH, Lai YC, et al. Prognostic value of radiological and pathological complete response following immune-based conversion therapy in patients with unresectable hepatocellular carcinoma (GUIDANCE004). JHEP Rep. 2025;7(11):101587. doi:10.1016/j.jhepr.2025.101587
15. Scheiner B, Kang B, Balcar L, et al. Outcome and management of patients with hepatocellular carcinoma who achieved a complete response to immunotherapy-based systemic therapy. Hepatology. 2025;81(6):1714–1727. doi:10.1097/HEP.0000000000001163
16. Ma L, Yang DL, Zhong TM, et al. Prognostic usefulness of clinical complete response after PD-1 inhibitor-based combination therapy for unresectable hepatocellular carcinoma (GUIDANCE006). Liver Cancer. 2025:1–19. doi:10.1159/000549844
17. Li W, Zheng Z, Wang J, et al. Efficacy and safety of conversion surgery for advanced hepatocellular carcinoma after hepatic arterial infusion chemotherapy. J Hepatocell Carcinoma. 2024;11:463–475. doi:10.2147/JHC.S447387
18. Zhang Y, Huang G, Wang Y, et al. Is salvage liver resection necessary for initially unresectable hepatocellular carcinoma patients downstaged by transarterial chemoembolization? Ten years of experience. Oncologist. 2016;21(12):1442–1449. doi:10.1634/theoncologist.2016-0094
19. Salem R, Lewandowski RJ, Kulik L, et al. Radioembolization results in longer time-to-progression and reduced toxicity compared with chemoembolization in patients with hepatocellular carcinoma. Gastroenterology. 2011;140(2):497–507.e2. doi:10.1053/j.gastro.2010.10.049
20. Cucchetti A, Cappelli A, Ercolani G, et al. Selective Internal Radiation Therapy (SIRT) as conversion therapy for unresectable primary liver malignancies. Liver Cancer. 2016;5(4):303–311. doi:10.1159/000449341
21. Labgaa I, Tabrizian P, Titano J, et al. Feasibility and safety of liver transplantation or resection after transarterial radioembolization with Yttrium-90 for unresectable hepatocellular carcinoma. HPB. 2019;21(11):1497–1504. doi:10.1016/j.hpb.2019.03.360
22. Haber PK, Puigvehí M, Castet F, et al. Evidence-based management of hepatocellular carcinoma: systematic review and meta-analysis of randomized controlled trials (2002-2020). Gastroenterology. 2021;161(3):879–898. doi:10.1053/j.gastro.2021.06.008
23. Arita J, Ichida A, Nagata R, et al. Conversion surgery after preoperative therapy for advanced hepatocellular carcinoma in the era of molecular targeted therapy and immune checkpoint inhibitors. J Hepatobiliary Pancreat Sci. 2022;29(7):732–740. doi:10.1002/jhbp.1135
24. He T, Xu B, Yang ZY, et al. Stable disease without tumor shrink cannot benefit from surgery following immune-based therapy in potentially resectable hepatocellular carcinoma. Liver Cancer. 2026:1–13. doi:10.1159/000550497
25. Piao M, Li C, Huang Z, et al. Conversion surgery after immune checkpoint inhibitor-based combination therapy for initially unresectable hepatocellular carcinoma: a retrospective cohort study. Liver Cancer. 2025;14(4):456–473. doi:10.1159/000543994
26. Wu JY, Wu JY, Liu DY, et al. Clinical complete response after conversion therapy for unresectable hepatocellular carcinoma: is salvage hepatectomy necessary. J Hepatocell Carcinoma. 2023;10:2161–2171. doi:10.2147/JHC.S442341
27. Lin Q, Peng W, Yu X, et al. Pathological complete response after systemic therapy and curative resection in initially unresectable hepatocellular carcinoma: feasibility of a tumor-free with drug-free strategy. Liver Cancer. 2025:1–15. Epub ahead of print. PMID: 41551718; PMCID: PMC12807518. doi:10.1159/000549793
28. Jia J, Ding C, Mao M, et al. Pathological complete response after conversion therapy in unresectable hepatocellular carcinoma: a retrospective study. BMC Gastroenterol. 2024;24(1):242. doi:10.1186/s12876-024-03298-5
29. Zeng ZX, Wu JY, Wu JY, et al. Prognostic value of pathological response for patients with unresectable hepatocellular carcinoma undergoing conversion surgery. Liver Cancer. 2024;13(5):498–508. doi:10.1159/000536376
30. Yang C, Chen Y, Sheng L, et al. Prediction of pathologic response in unresectable hepatocellular carcinoma after downstaging with locoregional and systemic combination therapy. J Hepatocell Carcinoma. 2025;12:43–58. doi:10.2147/JHC.S499597
31. Huang C, Zhu XD, Shen YH, et al. Radiographic and α-fetoprotein response predict pathologic complete response to immunotherapy plus a TKI in hepatocellular carcinoma: a multicenter study. BMC Cancer. 2023;23(1):416. doi:10.1186/s12885-023-10898-z
32. Yang N, Yue HL, Zhang BH, et al. Predicting pathological response to neoadjuvant or conversion chemoimmunotherapy in stage IB-III non-small cell lung cancer patients using radiomic features. Thorac Cancer. 2023;14(28):2869–2876. doi:10.1111/1759-7714.15052
33. Wen H, Liang R, Liu X, et al. Predicting Pathological Response of Neoadjuvant Conversion Therapy for Hepatocellular Carcinoma Patients Using CT-Based Radiomics Model. J Hepatocell Carcinoma. 2024;11:2145–2157. doi:10.2147/JHC.S487370
34. Chaudhuri AA, Chabon JJ, Lovejoy AF, et al. Early Detection of Molecular Residual Disease in Localized Lung Cancer by Circulating Tumor DNA Profiling. Cancer Discov. 2017;7(12):1394–1403. doi:10.1158/2159-8290.CD-17-0716
35. Galli E, Patelli G, Villa F, et al. Circulating blood biomarkers for minimal residual disease in hepatocellular carcinoma: a systematic review. Cancer Treat Rev. 2025;135:102908. doi:10.1016/j.ctrv.2025.102908
36. Xu Y, Cai J, Zhong K, et al. Plasma-only circulating tumor DNA analysis detects minimal residual disease and predicts early relapse in hepatocellular carcinoma patients undergoing curative resection. Front Oncol. 2023;13:1119744. doi:10.3389/fonc.2023.1119744
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Hepatic Arterial Infusion Chemotherapy as a Timing Strategy for Conversion Surgery to Treat Hepatocellular Carcinoma: A Single-Center Real-World Study
Wang J, Zheng Z, Wu T, Li W, Wang J, Pan Y, Peng W, Hu D, Hou J, Xu L, Zhang Y, Chen M, Zhang R, Zhou Z
Journal of Hepatocellular Carcinoma 2022, 9:999-1010
Published Date: 14 September 2022
Hepatectomy After Conversion Therapy for Initially Unresectable HCC: What is the Difference?
Luo L, He Y, Zhu G, Xiao Y, Song S, Ge X, Wang T, Xie J, Deng W, Hu Z, Shan R
Journal of Hepatocellular Carcinoma 2022, 9:1353-1368
Published Date: 22 December 2022
Simultaneous and Sequential Use of Molecular Targeted Agents Plus Immune Checkpoint Inhibitors for Advanced Hepatocellular Carcinoma: A Real-World Practice in China
Li J, Huang L, Ge C, Zhu X, Qiu M, Chen C, Wei S, Yan Y
Journal of Hepatocellular Carcinoma 2023, 10:949-958
Published Date: 20 June 2023
Immunotherapy Efficacy in Advanced Hepatocellular Carcinoma in a Diverse and Underserved Population in the United States
Bteich F, Desai K, Zhang C, Kaur A, Levy RA, Bioh L, Wang A, Sultana S, Kaubisch A, Kinkhabwala M, Bellemare S, Fidvi S, Kanmaniraja D, Berkenblit R, Moon JY, Adedimeji A, Tow CY, Saenger Y
Journal of Hepatocellular Carcinoma 2024, 11:257-269
Published Date: 3 February 2024
Systemic Drugs for Hepatocellular Carcinoma: What Do Recent Clinical Trials Reveal About Sequencing and the Emerging Complexities of Clinical Decisions?
Himmelsbach V, Koch C, Trojan J, Finkelmeier F
Journal of Hepatocellular Carcinoma 2024, 11:363-372
Published Date: 19 February 2024