Back to Journals » Risk Management and Healthcare Policy » Volume 16
What Makes a Hospital Excellent? A Qualitative Study on the Organization and Management of Five Leading Public Hospitals in China
Authors Zhao J ![]() , Wu X
, Wu X ![]() , Chen Y, Li T, Han Y, Liu T, Liu Y
, Chen Y, Li T, Han Y, Liu T, Liu Y
Received 7 June 2023
Accepted for publication 8 September 2023
Published 18 September 2023 Volume 2023:16 Pages 1915—1927
DOI https://doi.org/10.2147/RMHP.S424711
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Haiyan Qu
Jinhong Zhao, Xue Wu, Yuan Chen, Tao Li, Yunrui Han, Tingfang Liu, Yuanli Liu
School of Health Policy and Management, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, 100730, People’s Republic of China
Correspondence: Tingfang Liu; Yuanli Liu, School of health policy and management, Chinese Academy of Medical Sciences & Peking Union Medical College, No. 9, Dongdansantiao Street, Dongcheng District, Beijing, 100730, People’s Republic of China, Tel +86 13501008967 ; +86 13522592907, Fax +86 010-65105750, Email [email protected]; [email protected]
Purpose: To summarize the organizational and management experiences and explore the organizational theoretical model of five leading public hospitals in China.
Patients and Methods: Purposive sampling was used to select five leading hospitals in different regions of China under the National Health Commission and Provincial Health Commission as study hospitals for the study. From August 2021 to March 2022, 8 leaders and 39 managers from these hospitals were surveyed using semi-structured interviews. The data and information were analyzed in four dimensions using thematic analysis and grounded theory, focused on summarizing the experiences and practices of China’s leading hospitals in organizational system, culture, operations and performance management, and employee development. This study complied with the COREQ guidelines for reporting qualitative research.
Results: An organizational system model of the characteristics of hospital excellence was developed using four core attributes: organizational system, organizational culture, operations and performance management, and employee development; the model was named the System–Culture–Operation–Performance–Employee (SCOPE) model. Organization and management among leaders and managers in China’s leading hospitals are based on the SCOPE process, resulting in employees’ well-being, patients’ positive outcomes, and organizational excellence. In terms of hospital culture, while adhering to the Hippocratic Oath, the hospital is deeply influenced by traditional Chinese culture, which emphasizes “benevolence” and “love”, leading all staff to adhere to “patient-centered care and service.” In terms of operations management, a separate operations management department is responsible for hospital operations and performance assessment. As for employee development, the staff’s sense of reverence for their profession is emphasized and a reasonable salary system and good practice environment are established to promote staff motivation.
Conclusion: The SCOPE model reveals the perspectives of leaders and managers in China’s leading hospitals regarding organization and management under a Chinese cultural background. These findings can complement the existing literature on hospital management systems.
Keywords: hospital management, excellence, lessons, qualitative study, model
Introduction
Efficient organizational systems and management capabilities improve organizational cohesion and play an important role in building organizational culture, operational management, and staff development.1–3 As one of the most complex organizations, hospitals have received increasing attention in terms of their organizational structure and management level.4 In addition, the COVID-19 pandemic has created an entirely new set of challenges for the world’s health system. Therefore, it is important to continuously improve hospital management systems to meet such challenges.5
Hospital organization and management systems differ among different countries and regions owing to the differences in social systems, economic conditions, cultural backgrounds, and health care systems.6,7 Evidence from high-income countries suggests that summarizing and promoting hospital management excellence can stimulate better hospital development.2 The Malcolm Baldrige Performance Excellence framework in the United States provides a reference model for organizational excellence; previous studies have shown that hospital leadership, strategy, culture, operations management, and staff management have a positive effect on hospital excellence.8–10 However, experiences regarding hospital organization and management in low- and middle-income countries have rarely been summarized,11 and there is a lack of evidence from hospitals in these countries.
China’s ongoing health care reform is part of a broader effort to ensure a healthy population, and public hospitals play a central role in the provision of medical services.12 Since the implementation of the medical and health reform in 2009, strengthening the organization and management of public hospitals has become an important element.13,14 During 2019–2022, Chinese government departments issued a series of policies to promote the management of public hospitals, guiding hospitals at different levels to further implement their functional positioning and improve the quality and efficiency of medical services.15,16 Since 2018, “the system of the hospital president under the leadership of the Communist Party Committee (CPC)” has become the main organizational system in Chinese public hospitals. In this system, the hospital president is the legal representative of the hospital, and the CPC led by the secretary has the main role in determining the direction of hospital development, promoting reforms, and making decisions on major events and their implementation. It is important to note that the aim of the CPC involvement in the governance of public hospitals is to promote the party’s principles of social welfare and public service and to ensure the provision of high-quality health care services to the public. The system can be summarized as a model that combines professional management with party guidance for effective health care governance. Overall, the system of having a hospital president under the leadership of the CPC reflects the unique governance structure of public hospitals in China, which aims to ensure the delivery of quality health care services while adhering to the party principles and national health care policies.
Most studies on hospital organization and management by Chinese scholars have focused on health care staff satisfaction, patient experience, and quality and safety of care,17–20 and some scholars have drawn on hospital management tools to assess the level of hospital management in China.21–23 However, few scholars have summarized and described the organizational structure and management of Chinese public hospitals,24 especially with respect to the strengths, characteristics, and experiences of well-known Chinese hospitals in terms of organization and management. Therefore, in this study, we aimed to summarize the organizational and management experiences of five top-ranked hospitals in China, explore the organizational framework and management of leading public hospitals in China, and summarize the experiences of different hospitals in terms of their organizational system, cultural values, operations and performance, and staff development. Our findings can serve as a reference for hospital reforms, improving staff and patient satisfaction, and enhancing core competitiveness in China and other countries.
Materials and Methods
Study Design and Participants
The idea in selecting the study hospitals was to cover leading hospitals in the eastern, central, and western regions of China. Therefore, we employed a purposive sampling method, first selecting four general hospitals (located in the eastern, central, and western regions) from the “A++” ranked hospitals within the jurisdiction of the central government, as they represent the top providers of national healthcare services. Additionally, we chose one hospital (located in the eastern region) from the “A+” ranked hospitals under the jurisdiction of the provincial government to encompass broader medical practices. Table 1 presents basic information about the sample hospitals (the names of the hospitals are anonymized).
 |
Table 1 Basic Information of the Sample Hospitals |
We planned to invite 2 leaders and 8 managers from each sample hospital to participate in semi-structured interviews. Inclusion criteria for the interviewees were as follows: (1) the president (vice president), party secretary (vice secretary), and functional department managers of the sample hospitals; (2) informed consent was provided by all participants to voluntarily participate in this survey; and (3) Employees of the sample hospital, not the independent contractors. Exclusion criteria were as follows: (1) employees with less than 1 year of work experience in the hospital; (2) employees who were unable to communicate effectively or to participate in the interview independently.
Data Collection
We drew on the Malcolm Baldrige Performance Excellence framework25 to design an organizational and management assessment framework for public hospitals comprising hospital organizational structure, leadership, values, operations, performance management, and staff development. The assessment framework was informed by previous surveys and the available literature. Interview framework was reviewed in two expert consultation meetings and through discussions (Supplementary Table 1).
From August 2021 to March 2022, we conducted on-site investigations at these five hospitals. Fifteen days prior to the survey, we collaborated with the hospital coordinators to identify the list of leaders and managers who would participate in the on-site investigation, ensuring their compliance with the inclusion and exclusion criteria. Seven days before the survey, we provided the interview framework to the hospital coordinators, emphasizing that the research participants had to familiarize themselves with the interview content in advance. During the actual survey, two leaders from two sample hospitals did not participate, and one manager from another hospital also did not participate. In the end, a total of 8 leaders (L1-L8) and 39 managers (M1-M39) participated in the interviews, and all of them met the inclusion criteria.
Interviews were conducted in private conference rooms in each sample hospital, which met the interview requirements. Each interview was conducted for 30–90 min after informed consent was provided by the interviewees. Two senior faculty members served as interviewers, and one or two graduate students who recorded and transcribed the interviews. The interviewees in the first sample hospital participated in the initial interview to test the interview framework. Interviewees were given the opportunity to review their own interview results.26 The study design and data analysis processes are shown in Figure 1.
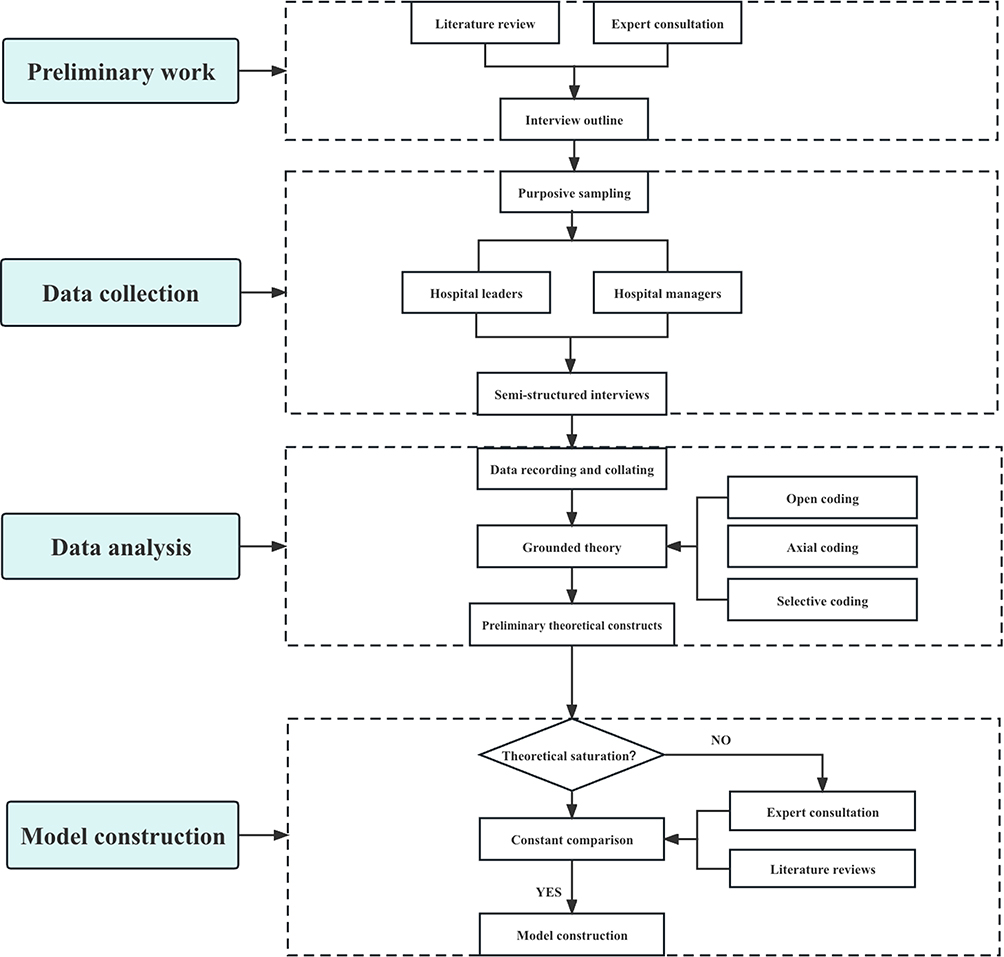 |
Figure 1 Study design and data analysis processes. |
Research Methodology
Thematic analysis is a commonly used qualitative data analysis method aimed at identifying and understanding the important concepts, perspectives, and experiences expressed by research participants in specific themes or research domains.27 Based on the participants’ beliefs and experiences, we applied thematic analysis to identify the connotations and extent of the study topics regarding hospital organization and management. Moreover, the interaction processes and implications of the study dimensions were discussed and explained.28,29 Corbin and Strauss’ (1990) grounded theory, based on a pragmatic philosophical perspective, was employed to better understand and develop the organization and management model of Chinese public hospitals.30
Statistical Analysis
The interview recordings were first transcribed verbatim and then coded based on the interview outline and research dimensions. The textual material was conceptualized; to avoid bias in the coding process and to obtain greater precision, the data were compared with homogeneously classified interview data in data analysis. In addition, prior to coding the survey results, screening was performed based on the following criteria: (1) clear descriptions; (2) described experiences or specific practices in hospital organization and management; and (3) descriptions were relevant to the research topic. The first and second authors completed this process and integrated similar descriptions for further analysis. Microsoft Excel 2016 software (Microsoft, Seattle, WA, USA) was used to filter and integrate the original descriptions of the survey respondents.
The researchers read the transcripts and descriptions repeatedly to ensure their familiarity with and sensitivity to the data if important information was missed. The first and second authors coded the original transcripts and descriptions separately during the coding phase and then compared the results until their codes agreed. If there was any disagreement in coding, help was sought from the corresponding author to make a final decision. NVivo 12.0 software (QSR International Pty Ltd, Massachusetts, USA) was used to analyze the transcript text and comprehensive descriptions.
Results
Basic Information About Hospitals and Participants
Four of the five study hospitals (H1–H4) included in this survey are under the direction of the Chinese national health administration, whereas one study hospital (H5) is under the direction of the provincial health administration. In terms of geographic location, H1, H3, and H5 are located in the eastern region of China, H4 is located in the central region, and H2 is located in the western region of China. In terms of hospital grade, all five hospitals are tertiary class A hospitals. Regarding hospital level in 2018–2020, all were A+ and above (Table 1). Eight presidents and secretaries and 39 functional managers were recruited for the interview. Table 2 shows the detailed characteristics of the survey participants.
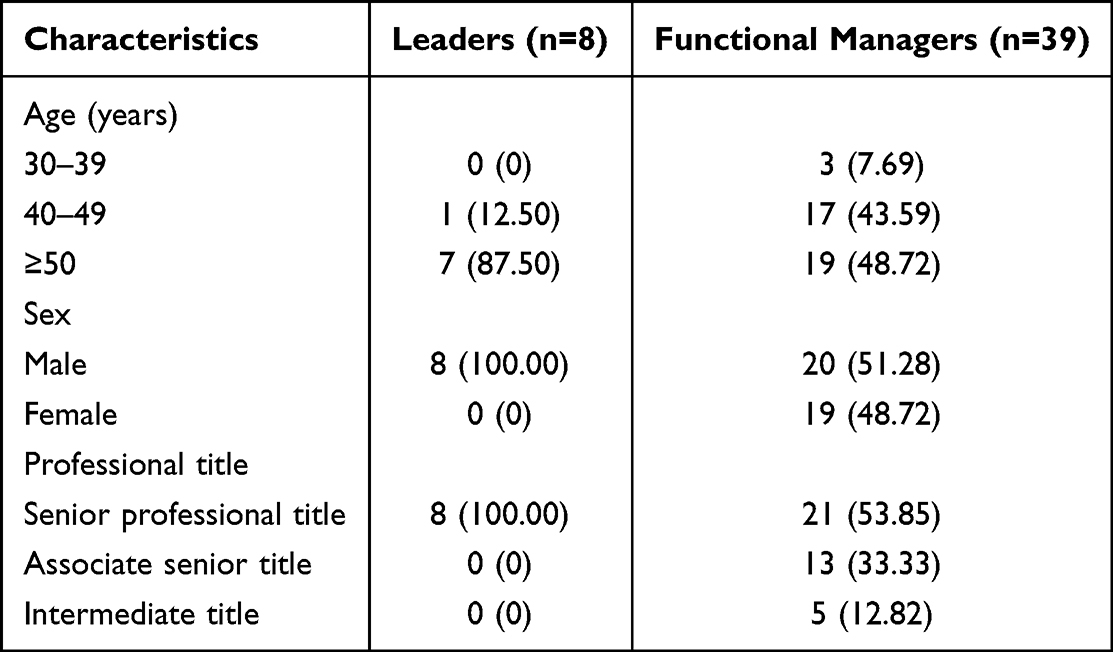 |
Table 2 Demographic Characteristics, n (%) |
Organizational and Management Model from China’s Leading Hospitals
An organizational system model of the characteristics of hospital excellence was developed using thematic analysis and grounded theory (Table 3), which revealed the perspectives of leaders and managers of China’s leading hospitals regarding organization and management under a Chinese cultural background. The organizational system model of the characteristics of hospital excellence was named “System–Culture–Operation–Performance–Employee (SCOPE)” model, focusing on a well-developed organizational structure, the positive role of cultural values, efficient operations and performance, and a systematic staff development system (Figure 2). According to the thematic analysis method, we carefully read and repeatedly analyzed the interview data, organizing similar content into themes and assigning descriptive names to each theme. Key findings focused on the core drivers and motivations that the interviewees reported for their hospital work and the ways in which they described their approaches and methods for promoting hospital excellence in practice. We next present the results of the four-dimensional assessment of the leading Chinese hospitals, for each dimension, we first outline the summarized experiences and then proceed to the results of the participants’ interviews.
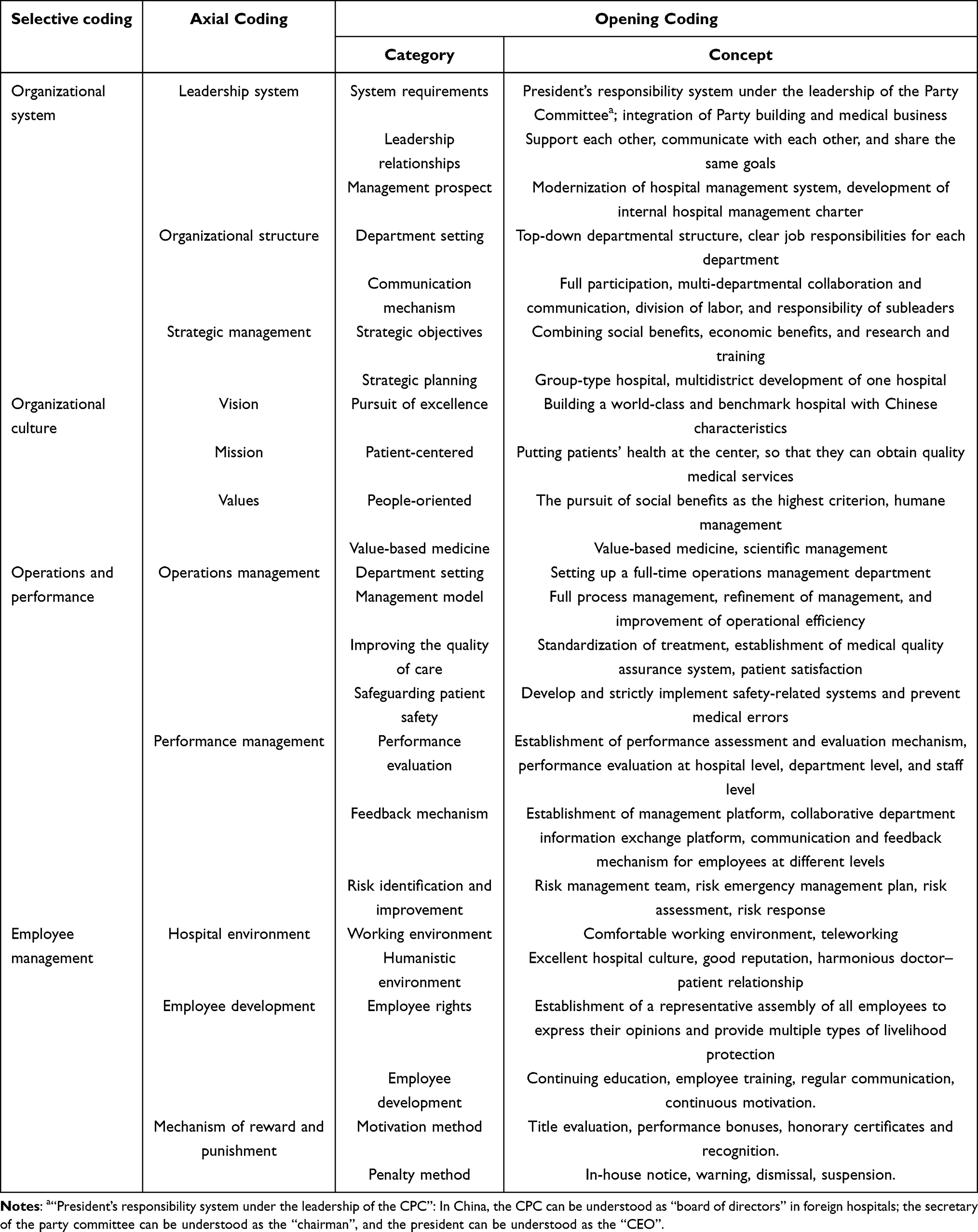 |
Table 3 Coding Process of Organization and Management in China’s Public Hospitals |
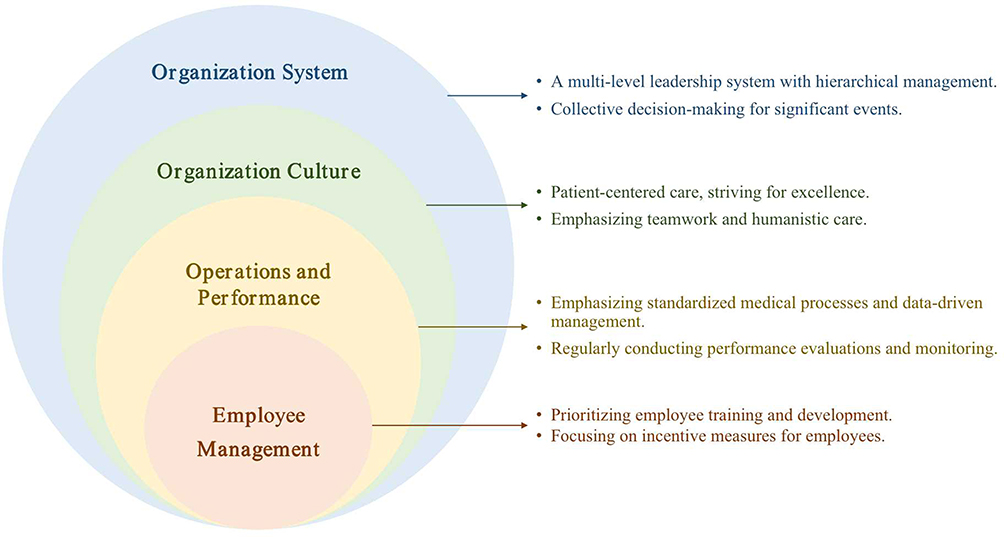 |
Figure 2 System–Culture–Operation–Performance–Employee (SCOPE) model. |
Organizational System
The organizational structure of a hospital determines its functioning, in which leadership plays a crucial role.31 The leadership system of Chinese hospitals is a collective decision-making leadership system comprising members of the Party Committee (Secretary) and the President (Director). In the decision-making process, scientific, democratic, and normative aspects are adhered to. Major issues are ultimately discussed collectively in the Party Committee meeting and the Dean’s Office and jointly voted on, thereby effectively avoiding blind, unscientific decisions brought about by individual leaders’ centralized power. Moreover, the party secretary and the president cooperate and communicate effectively, forming an efficient and harmonious leadership relationship that motivates hospital staff to work earnestly and greatly improves the operational efficiency of the hospital.
One secretary stated,
There should be organizational effects at the hospital system level, and the leadership team (secretary and president) should be inclusive and work together. (L3)
A president said,
We (secretary and president) are not able to maintain a high level of agreement on everything; there are always different opinions and constant communication. (L4)
Another secretary said,
All party committee members make decisions collectively to avoid blind and unscientific decisions. (L7)
Organizational Culture
Good cultural values may also contribute to the overall success of a hospital.32,33 Our study found that the tenets of the well-known hospitals in China include “care and service”, the core value of “patient-centeredness”, and the ultimate vision of building “world-class hospitals with Chinese characteristics.” This is due to the fact that Chinese public hospitals, while adhering to the Hippocratic Oath, are deeply influenced by traditional Chinese culture, which emphasizes benevolence, love, merit, and virtue;28 thus, cultural values are integrated into the daily work of the hospitals, continuously improving the overall sense of honor and cohesion among staff. In terms of social services, all hospital staff participate in international medical aid and domestic social services to varying degrees. Through social services and international medical assistance, the brand-building and international visibility of Chinese hospitals are continuously promoted.
One president said,
Our hospital management system puts the hospital’s culture at a very high level; a hospital has no soul without culture, and we are committed to the idea that the hospital’s cultural values can penetrate into the marrow of each employee. (L6)
Another president stated,
Our vision is to build a hospital that promotes people’s satisfaction, with Chinese characteristics and world-class disciplines, as well as first-class quality and branding, which are our three major goals, respectively. (L8)
One medical department manager explained the hospital’s cultural values from the perspective of the hospital’s executive leadership:
We have always adhered to the core value of ‘patient-centeredness.’ The core of the hospital’s existence is to serve patients, and the daily work content is focused on patient-centeredness. (M24)
Operations and Performance Management
Hospital operations and performance management play an important role in improving hospital management and contributing to the stable development of hospitals in a modern social environment and with industry competition.34 Based on our findings, the sample hospitals have dedicated operations management departments to analyze the overall hospital operations, optimize the allocation of hospital resources and processes, and fully motivate staff using performance appraisals. The purpose of an operations management department is “service, communication, and innovation”, that is, serving operations management in each department, liaising between departments, and continuously innovating the performance appraisal system to successfully accomplish the hospital’s goals and improve the hospital’s overall service capacity.
One secretary said,
Our operations concept is not simply operations management but the whole hospital management concept, a mature modern enterprise management system using methods, means, and tools in our hospital internal management to remove the profit-seeking; this is what we want to do. (L5)
Another secretary said,
Performance is not independent; performance and operations are related. Operations are not independent; operations and business are related. Business is not independent; business and management are related. Thus, business, operations, and performance, these are managed as one, for integration. (L8)
A middle manager in charge of operations said,
The clinical staff serves the patients, the hospital is for the clinical services; the hospital operations overall are the responsibility of the manager. Hospital operations are transferred to a special operations management department, which plays a greater role. (M18)
Employee Management
Medical staff is the core of meeting medical needs and medical development, and high-level medical staff comprises the leaders in medical development and scientific progress. Job satisfaction among medical personnel is closely related to the current job status, performance appraisal system, leadership, hospital management, and compensation.35 In China, both government and hospital leaders attach importance to access, happiness, and satisfaction among medical staff. The interviewees from five hospitals mentioned practices related to staff development, particularly emphasizing the importance of a scientifically based and effective staff development mechanism and incentive mechanism. The introduction of talent at different levels and rewards for innovation, talent, and recognition, as well as further training and expert cooperation, has been used to cultivate a sense of honor among staff. This guarantees the hierarchical echelon and quality of hospital talent and provides a good employment mechanism for the high-quality development of the hospital.
One president expressed,
How to stimulate the vitality of each person is the top priority of management, and we have a talent office with a plan for each stage of staff development. (L4)
A medical department administrator stated,
Our hospital leadership provided us with a better space in terms of innovation by setting up a dedicated staff innovation center which is both a challenge and a good opportunity to practice. (M9)
A manager in the personnel department said,
When it comes to staff development, a sense of honor of the staff is important. We participate in hospital competitions or awards for different projects that we do, so that people can feel a sense of honor in this platform. (M17)
Discussion
In this study, we employed a semi-structured interview approach to interview leaders and managers of prominent hospitals in China. We conducted a thematic analysis of the interview data, which resulted in the identification of four key themes. Subsequently, a hospital organization and management model was developed using grounded theory, ensuring the reliability of the research findings. The data integration results in the four domains of the organization and management model as follows: (1) organizational system, (2) organizational culture, (3) operations and performance, and (4) employee management. This is the first qualitative study on organization and management in the five leading hospitals from different regions under the jurisdiction of the central and provincial governments in China. In many cases, we were able to link the lessons regarding hospital organizational and management practices to hospital success and excellence. The findings provide a reference for promoting hospital excellence in developing countries, and the summarized hospital organization and management experiences may help health care leaders, researchers, and hospital managers to conduct in-depth investigation and research. Despite we focus on hospital management experiences in the institutional, economic, and cultural contexts of China, our findings are also internationally informative, given the increasing academic focus on the impact of research and the processes by which researchers generate findings.36
The present organization and management model focuses on hospital systems, cultural values, and operations and performance management. The most distinctive of these is the organizational system and culture of Chinese hospitals, and the most effective is operations and performance management. Toussaint, Griffith, and Shortell (2020) jointly explored the role of the Lean, Shingo, and Baldrige Framework for continuous improvement in hospital management; their study showed that hospitals of excellence had high-performance outcomes on key indicators such as leadership, operating costs, quality of care, and staff management.10 Indeed, a well-developed organizational system is the key to hospital excellence,37 and there is a strong association among hospital leadership, organizational culture, and hospital performance.38 In China, public hospitals operate within a unique governance structure that combines professional management with party leadership. The CPC provides guidance and oversight to ensure that the hospital adheres to national health care policies and principles. In addition, a collective decision-making system is adopted in Chinese public hospital in which multiple departments participate in hospital management and operations to avoid blind and unscientific decision-making. Based on studies in the United States, Canada, and Iran, collective leadership interventions have the potential to positively influence the quality of care and staff welfare and improve team performance.39 McAuliffe also showed the positive effects of collective leadership on hospital performance based on evidence from the United Kingdom.40
For improving the quality and safety of care, it is critical how hospital leaders pass on the hospital’s cultural values, actively engage staff, and positively exert cultural appeal.41 Furthermore, traditional Chinese culture is centered on Confucianism, which includes benevolence, righteousness, propriety, wisdom, and trustworthiness, embodying moral principles and the values and behaviors of individuals within the Chinese cultural context.42 We found that Chinese public hospitals adhere to the Hippocratic Oath but are also deeply influenced by traditional Chinese culture, such as benevolence, love, merit, and virtue. The essence of hospital organizational culture is to create a working environment and atmosphere for employees that reflect a sense of intimacy in a close organization through multidimensional management initiatives. Specifically, organizational culture should stimulate the sense of value, responsibility, and mission among medical staff at work, which is conducive to prompting employees to cordially identify with the value of their work from the heart, to regard work difficulties as an opportunity to showcase their abilities, as a process of emotional support and communication, and to promote identification with the organization and improve motivation to complete work and work.
Since 2005, there has been growing attention to operations management in Chinese public hospitals. In 2020, Chinese government departments issued policies to strengthen the operations management of public hospitals, further improving the level of scientific, standardized, refined, and informed hospital operations management. Compared with China, developed countries such as those in North America and Europe focused earlier on the application of enterprise operations management tools and instruments in hospital management, promoting the establishment of hospital operations management departments, and informatization and digitization of operations management.43,44 Performance management has shifted from focusing on individual hospital staff effectiveness and departmental effectiveness to hospital organizational performance and from focusing on economic benefits to a comprehensive reflection of operational efficiency, social equity, and responsibility.45
Medical employees are crucial for meeting medical needs and medical development, and high-level medical staff leads medical development and scientific progress.46 Both the central government and local governments in China promote the training of medical talent at different levels to improve access, happiness, and satisfaction among medical staff. Considering growing demands for medical services in hospitals, hospital employees are facing an increasing workload.47 China’s leading hospitals mainly address these issues by cultivating the employees’ sense of respect for their profession and establishing a reasonable compensation system.
The organizational system, culture, operations and performance, and employee management in China’s public hospitals are interlinked and can influence each other. Effective employee management is essential for ensuring high-quality patient care and achieving positive hospital performance outcomes. Public hospital management should focus on creating a positive and supportive organizational culture that encourages transparency, accountability, and open communication among staff. This can help to identify problems quickly and may facilitate effective problem-solving. It would also be useful to establish performance indicators and metrics to monitor and evaluate hospital operations and employee performance, ensuring that they align with the hospital’s goals and objectives. Overall, a well-designed and effectively managed organization system, culture, operations, and employee management can lead to better patient outcomes, improved hospital performance, and increased employee job satisfaction.
Limitations
Despite the novelty of our findings, there are certain limitations to this study. First, the small number of study hospitals limits the generalizability of the findings; however, we tried to enhance the generalizability of the findings by describing in detail the interview data from five highly representative hospitals. Second, we used a qualitative study design to analyze the data but could not obtain stronger evidence-based results in quantitative analysis. However, as in our study, qualitative research methods are the most appropriate when the study population is complex or when real-world studies do not meet the criteria for quantitative data collection.48,49
Conclusion
The present study provides a theoretical model of organization and management in Chinese leading public hospitals. The Chinese public hospital leadership system comprises a collective decision-making system consisting of the CPC and the president, a focus on “patient-centeredness” in cultural values, a separate operations management department, staff management that fosters a sense of professional reverence, and a reasonable compensation system to increase staff motivation. These findings complement the available literature on hospital management in China and may contribute to the promotion of high-quality and sustainable development of hospitals in low- and middle-income countries.
Ethics Approval and Considerations
This study was conducted in accordance with the guidelines of the Declaration of Helsinki and was approved by the Chinese Academy of Medical Sciences & Peking Union Medical College Institutional Review Board (CAMS & PUMC-IRC-2020-026). The ethics committee approved verbal informed consent for interview participants. Participation in the study was voluntary. Verbal informed consent was obtained from all of the participants before data collection, and the participants were explicitly informed that their responses would be anonymized and potentially published as part of the research findings.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Fundamental Research Funds for the Central Universities, China (2020-RC630-001 and 3332022166), and the Chinese Academy of Medical Sciences (CAMS) Innovation Fund for Medical Sciences (2021-I2M-1-046).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Allameh SF, Khajavirad N, Labaf A, et al. Twelve lessons on hospital leadership during COVID-19 pandemic. Arch Bone Jt Surg. 2020;8(Suppl1):277–280. doi:10.22038/abjs.2020.47829.2363
2. Tsai TC, Jha AK, Gawande AA, Huckman RS, Bloom N, Sadun R. Hospital board and management practices are strongly related to hospital performance on clinical quality metrics. Health Aff. 2015;34(8):1304–1311. doi:10.1377/hlthaff.2014.1282
3. Gentry L, Fleshman JW. Leadership and ethics: virtue ethics as a model for leadership development. Clin Colon Rectal Surg. 2020;33(4):217–220. doi:10.1055/s-0040-1709437
4. Drucker PF. Managing in the Next Society. Routledge; 2002.
5. Foglia E, Ferrario L, Schettini F, Pagani MB, Dalla Bona M, Porazzi E. COVID-19 and hospital management costs: the Italian experience. BMC Health Serv Res. 2022;22(1):991. doi:10.1186/s12913-022-08365-9
6. Nakagawa Y, Irisa K, Nakagawa Y, Kanatani Y. Hospital management and public health role of national hospitals after transformation into independent administrative agencies. Healthcare. 2022;10(10):2084. doi:10.3390/healthcare10102084
7. Liu HC. A theoretical framework for holistic hospital management in the Japanese healthcare context. Health Policy (New York). 2013;113(1–2):160–169. doi:10.1016/j.healthpol.2013.08.009
8. Maciel-Monteon M, Limon-Romero J, Gastelum-Acosta C, Baez-Lopez Y, Tlapa D, Rodríguez Borbón MI. Improvement project in higher education institutions: a BPEP-based model. PLoS One. 2020;15(1):e0227353. doi:10.1371/journal.pone.0227353
9. Rodríguez-González CG, Sarobe-González C, Durán-García ME, et al. Use of the EFQM excellence model to improve hospital pharmacy performance. Res Social Adm Pharm. 2020;16(5):710–716. doi:10.1016/j.sapharm.2019.08.030
10. Toussaint JS, Griffith JR, Shortell SM. Lean, Shingo, and the Baldrige framework: a comprehensive method to achieve a continuous-improvement management system. NEJM Catalyst. 2020;1(3). doi:10.1056/CAT.20.0114
11. Hu M, Chen W, Yip W. Hospital management practices in county-level hospitals in rural China and international comparison. BMC Health Serv Res. 2022;22(1):64. doi:10.1186/s12913-021-07396-y
12. Yip W, Fu H, Chen AT, et al. 10 years of health-care reform in China: progress and gaps in Universal Health Coverage. Lancet. 2019;394(10204):1192–1204. doi:10.1016/S0140-6736(19)32136-1
13. Central People’s Government of the People’s Republic of China. Opinions of the CPC Central Committee and State Council on deepening the reform of the medical and health system. Availablr from: http://www.gov.cn/test/2009-04/08/content_1280069.htm.
14. Li L, Fu H. China’s health care system reform: progress and prospects. Int J Health Plann Manage. 2017;32(3):240–253. doi:10.1002/hpm.2424
15. Central People’s Government of the People’s Republic of China. Opinions of the General Office of the State Council on strengthening the performance assessment of tertiary public hospitals. Available from: http://www.gov.cn/zhengce/content/2019-01/30/content_5362266.htm.
16. Central People’s Government of the People’s Republic of China. Opinions of the General Office of the State Council on promoting the high-quality development of public hospitals; 2021. Available from: http://www.gov.cn/zhengce/content/2021-06/04/content_5615473.htm.
17. Wang M, Liu GG, Bloom N, et al. Medical disputes and patient satisfaction in China: how does hospital management matter? Int J Health Plann Manage. 2022;37(3):1327–1339. doi:10.1002/hpm.3399
18. Zhang Y, Li Q, Liu H. From patient satisfaction to patient experience: a call to action for nursing in China. J Nurs Manag. 2020;28(2):450–456. doi:10.1111/jonm.12922
19. Cai S, Cai W, Deng L, Cai B, Yu M. Hospital organizational environment and staff satisfaction in China: a large-scale survey. Int J Nurs Pract. 2016;22(6):565–573. doi:10.1111/ijn.12471
20. Liang GM, Xie WC, Gan M, Gao JW, Liang Q, Zeng ZY. Healthcare quality and safety assessment based on annual scorekeeping. Front Public Health. 2022;10:937338. doi:10.3389/fpubh.2022.937338
21. Zhao H, Wang M, Cui Y, Liu GG. A validated survey to measure Chinese hospital management practices. MethodsX. 2023;10:102066. doi:10.1016/j.mex.2023.102066
22. Zhang D, Yan Y, Liu TF. Key factors influencing the effectiveness of hospital quality management tools: using the quality control circle as an example-A cross-sectional study. BMJ Open. 2022;12(2):e049577. doi:10.1136/bmjopen-2021-049577
23. Qiu H, Du W. Evaluation of the effect of PDCA in hospital health management. J Healthc Eng. 2021;2021:6778045. doi:10.1155/2021/6778045
24. Beaulieu ND, Chernew ME, McWilliams JM, et al. Organization and performance of US health systems. JAMA. 2023;329(4):325–335. doi:10.1001/jama.2022.24032
25. Griffith JR. An organizational model for excellence in healthcare delivery: evidence from winners of the Baldrige quality award. J Healthc Manag. 2017;62(5):328–341. doi:10.1097/JHM-D-16-00011
26. Aspinall C, Jacobs S, Frey R. The impact of intersectionality on nursing leadership, empowerment and culture: a case study exploring nurses and managers’ perceptions in an acute care hospital in Aotearoa, New Zealand. J Clin Nurs. 2021;30(13–14):1927–1941. doi:10.1111/jocn.15745
27. Braun V, Clarke V. What can “thematic analysis” offer health and wellbeing researchers? Int J Qual Stud Health Well-Being. 2014;9(1):26152. doi:10.3402/qhw.v9.26152
28. Zhang F, Peng X, Huang L, et al. A caring leadership model in nursing: a grounded theory approach. J Nurs Manag. 2022;30(4):981–992. doi:10.1111/jonm.13600
29. Chen X, Zhang Y, Zhang R, Shen G. ‘I Accelerate’ model: a grounded theory on conceptual framework of patient experience with nursing care in China. J Nurs Manag. 2021;29(5):1311–1319. doi:10.1111/jonm.13271
30. Corbin JM, Strauss A. Grounded theory research: procedures, canons, and evaluative criteria. Qual Sociol. 1990;13(1):3–21. doi:10.1007/BF00988593
31. Goniewicz K, Burkle FM, Hall TF, Goniewicz M, Khorram-Manesh A. Global public health leadership: the vital element in managing global health crises. J Glob Health. 2022;12:03003. doi:10.7189/jogh.12.03003
32. Sinkowitz-Cochran RL, Burkitt KH, Cuerdon T, et al. The associations between organizational culture and knowledge, attitudes, and practices in a multicenter Veterans Affairs quality improvement initiative to prevent methicillin-resistant Staphylococcus aureus. Am J Infect Control. 2012;40(2):138–143. doi:10.1016/j.ajic.2011.04.332
33. Curry LA, Linnander EL, Brewster AL, Ting H, Krumholz HM, Bradley EH. Organizational culture change in U.S. hospitals: a mixed methods longitudinal intervention study. Implement Sci. 2015;10:29. doi:10.1186/s13012-015-0218-0
34. Cui LJ. Consideration of hospital operation and management model innovation under modern hospital management system. China Gen Acct. 2021;2021(4):136–137.
35. Fang P, Luo Z, Fang Z. What is the job satisfaction and active participation of medical staff in public hospital reform: a study in Hubei province of China. Hum Resour Health. 2015;13:34. doi:10.1186/s12960-015-0026-2
36. Oliver K, Cairney P. The dos and don’ts of influencing policy: a systematic review of advice to academics. Palgrave Commun. 2019;5(1):1–11. doi:10.1057/s41599-019-0232-y
37. Chmielewska M, Stokwiszewski J, Markowska J, Hermanowski T. Evaluating organizational performance of public hospitals using the McKinsey 7-S framework. BMC Health Serv Res. 2022;22(1):1–12. doi:10.1186/s12913-021-07402-3
38. Rigamonti K. Injecting humanity into health care enhances the culture and quality of an organization. J Radiol Nurs. 2023;42:214–216. doi:10.1016/j.jradnu.2023.01.002
39. Silva JAM, Mininel VA, Fernandes Agreli H, Peduzzi M, Harrison R, Xyrichis A. Collective leadership to improve professional practice, healthcare outcomes and staff well-being. Cochrane Database Syst Rev. 2022;10(10):CD013850. doi:10.1002/14651858.CD013850.pub2
40. McAuliffe E, De Brún A, Ward M, et al. Collective leadership and safety cultures (Co-Lead): protocol for a mixed-methods pilot evaluation of the impact of a co-designed collective leadership intervention on team performance and safety culture in a hospital group in Ireland. BMJ Open. 2017;7(11):e017569. doi:10.1136/bmjopen-2017-017569
41. Butler GA, Hupp DS. Pediatric quality and safety: a nursing perspective. Pediatr Clin North Am. 2016;63(2):329–339. doi:10.1016/j.pcl.2015.11.005
42. Chen T, Li F, Leung K. Whipping into shape: construct definition, measurement, and validation of directive-achieving leadership in Chinese culture. Asia Pac J Manag. 2017;34:537–563. doi:10.1007/s10490-017-9511-6
43. Rijo R, Martinho R, Ermida D. Developing an enterprise architecture proof of concept in a Portuguese hospital. Procedia Comput Sci. 2015;64:1217–1225. doi:10.1016/j.procs.2015.08.511
44. Raimo N, De Turi I, Albergo F, Vitolla F. The drivers of the digital transformation in the healthcare industry: an empirical analysis in Italian hospitals. Technovation. 2023;121:102558. doi:10.1016/j.technovation.2022.102558
45. Ridgely MS, Buttorff C, Wolf LJ, et al. The importance of understanding and measuring health system structural, functional, and clinical integration. Health Serv Res. 2020;55(Suppl 3):1049–1061. doi:10.1111/1475-6773.13582
46. Cummings BM, Carballo V, Kalibatas O, et al. Impact of clinical process improvement training in an integrated delivery system. Am J Med Qual. 2021;36(3):156–162. doi:10.1177/1062860620943960
47. Shen Y, Jian W, Zhu Q, Li W, Shang W, Yao L. Nurse staffing in large general hospitals in China: an observational study. Hum Resour Health. 2020;18(1):1–7. doi:10.1186/s12960-020-0446-5
48. Khalaf IA, Al-Dweik G, Abu-Snieneh H, et al. Nurses’ experiences of grief following patient death: a qualitative approach. J Holist Nurs. 2018;36(3):228–240. doi:10.1177/0898010117720341
49. Broom A. Conceptualizing qualitative data. Qual Health Res. 2021;31(10):1767–1770. doi:10.1177/10497323211024951
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.