Back to Journals » International Journal of Women's Health » Volume 17
Vitamin D, Homocysteine, and Thyroid Dysfunction as Risk Factors for Missed Abortion: A Retrospective Risk Factor Analysis
Authors Fang Q, Sang L, Du S, Wang R, Wu H, Yang L, Yu J
Received 19 November 2024
Accepted for publication 15 May 2025
Published 31 May 2025 Volume 2025:17 Pages 1587—1596
DOI https://doi.org/10.2147/IJWH.S507470
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Qianjin Fang, Lin Sang, Shihua Du, Runqiu Wang, Haihong Wu, Lu Yang, Jie Yu
Department of Obstetrics and Gynecology, The Second People’s Hospital of Hefei, Hefei Hospital Affiliated to Anhui Medical University, Hefei, Anhui Province, 230011, People’s Republic of China
Correspondence: Qianjin Fang, Department of Obstetrics and Gynecology, The Second People’s Hospital of Hefei, Hefei Hospital Affiliated to Anhui Medical University, Hefei, Anhui Province, 230011, People’s Republic of China, Email [email protected]
Objective: This study aimed to identify potential associations between missed abortion (MA) and risk factors, including low levels of vitamin D, high homocysteine, and abnormal thyroid function, among women undergoing early pregnancy assessments, thereby bridging the clinical knowledge gap regarding modifiable risk factors for MA.
Methods: This retrospective study analyzed serum levels of vitamin D, (25-(OH)-D3), homocysteine (Hcy), and thyroid hormones (thyroid-stimulating hormone [TSH], thyroid peroxidase antibodies [TPOAb]) in 158 women who experienced missed abortion compared to 237 women with normal early pregnancy outcomes.
Results: MA patients had significantly lower vitamin D levels (P = 0.04), higher Hcy (P < 0.05), and evidence of abnormal thyroid function, including TSH levels ≥ 4 mIU/L (P = 0.01) and positive TPOAb (P = 0.02). Low vitamin D was significantly associated with an increased risk of MA (odds ratio = 1.8; P = 0.03).
Conclusion: These findings suggest that low vitamin D levels may be a potential risk factor for MA, highlighting the importance of monitoring and supplementation in early pregnancy to reduce the risk of missed abortion. As this study is retrospective, it cannot establish causality between the identified factors and MA.
Keywords: missed abortion, vitamin D, homocysteine, thyroid function, risk factors
Introduction
Missed abortion (MA) is defined as the retention of a nonviable embryo or fetus within the uterine cavity, with a closed cervical os, prior to 20 weeks of gestation. It is characterized by the absence of embryonic or fetal development and lack of natural expulsion. MA accounts for approximately 15% of clinically recognized pregnancies. Common etiological factors for MA include chromosomal abnormalities, anatomical defects of the reproductive system, dietary and environmental factors, and infections of the reproductive system.1 As a result, understanding the etiology of MA and implementing preventive strategies have become critical clinical concerns.
Vitamin D plays a vital role in supporting conception and fetal development. Pregnant women must meet not only their own metabolic needs but also the nutritional requirements of the developing fetus throughout the pregnancy, leading to an increased demand for essential nutrients. Despite the well-documented prevalence of vitamin D deficiency in 65% of Chinese pregnant women, few studies have quantified its synergistic effects with thyroid autoimmunity on MA risk. This heightened demand can often result in deficiencies of various nutrients, particularly of Vitamin D. Insufficient or deficient Vitamin D levels during pregnancy may contribute to adverse pregnancy outcomes.2 Previous studies have shown that Vitamin D deficiency is linked to elevated levels of inflammatory markers in the body, which in turn may increase homocysteine (Hcy) levels.3
Hcy is an intermediate metabolite produced during the metabolic conversion of methionine via the folate cycle and is not derived from dietary sources. Previous studies have shown that elevated serum levels of Hcy may be linked to genetic defects in enzyme function.4,5 The most commonly mutated gene is methylenetetrahydrofolate reductase (MTHFR). Such mutations impair the remethylation of Hcy, reduce MTHFR activity, and lead to elevated serum Hcy levels. Mutations in other genes, such as those encoding cystathionine beta synthase, methionine synthase, and methionine synthase reductase, can also result in Hcy accumulation. This accumulation may cause DNA hypomethylation. Elevated Hcy levels during pregnancy are associated with an increased risk of prethrombotic states and embryonic damage, both of which may contribute to MA. Additionally, serum Hcy levels have been shown to be influenced by thyroid function, with studies identifying a positive correlation between Hcy and thyroid-stimulating hormone (TSH) levels.6,7
Thyroid hormone (TH) levels fluctuate during pregnancy to meet the physiological demands of the mother and fetus. The placenta plays a key role in regulating thyroid function by secreting hormones that influence the hypothalamic-pituitary-thyroid axis. Thyroid-stimulating hormone (TSH), secreted by the pituitary gland, regulates TH levels in the body, serving as a key marker of thyroid function. In pregnant women with hypothyroidism, TSH levels are elevated. Chorionic gonadotropin, secreted by the placenta in early pregnancy, shares a similar chemical structure to TSH and can competitively bind to TSH receptors, leading to increased TH production. This, in turn, triggers negative feedback response that reduces TSH secretion.8 Additionally, placental estrogen significantly stimulates the hepatic synthesis of thyroxine-binding globulin (TBG) from the liver, which binds TH and increases TH levels.9 Disruptions in the thyroid hormone secretion axis during pregnancy can result in thyroid dysfunction and hormonal imbalances. Such imbalances may impair embryonic and fetal growth and development, potentially contributing to MA.
Current research indicates that the factors influencing MA are multifaceted and involve complex interactions. This study aimed to investigate the underlying relationship between Vitamin D levels, Hcy concentrations, and thyroid function, as well as their association with MA, thereby bridging the clinical knowledge gap regarding modifiable risk factors for MA.
Study Participants and Methods
Study Participants and Inclusion Criteria
The study group included 158 women who experienced missed abortions (≤ 12 weeks) and met the inclusion and exclusion criteria. These individuals were treated at the Department of Obstetrics and Gynecology at the Second People’s Hospital of Hefei between December 2022 and June 2024 and were retrospectively analyzed as the study group. The control group consisted of 237 healthy women who underwent normal early pregnancy terminations during the same period. Participants in both the study and control groups were consecutively enrolled during the study period. To minimize selection bias, all eligible cases meeting the inclusion criteria were included, and controls were matched by age (± 2 years) and gestational week (± 1 week).
Inclusion criteria: (1) Women with a singleton pregnancy who met the diagnostic criteria for MA or in the early stage of pregnancy; (2) No history of exposure to radiation, toxic substances, or hazardous materials; (3) No history of reproductive system infections within the past three months; (4) No use of tobacco, alcohol, or other harmful substances; (5) No intake of vitamin D-containing medications in the past six months; (6) No history of thyroid disease or use of medications containing TH within the past six months.
Exclusion criteria: (1) Developmental malformations of the reproductive system; (2) Presence of autoimmune diseases; (3) Endocrine system disorders; (4) Abnormal liver or renal function; (5) History of malignant neoplastic diseases.
The study flowchart is shown in Figure 1.
 |
Figure 1 Study flowchart. |
Clinical Data Collection
General clinical information was collected from all participants, including age, body mass index (BMI, weight [kg]/height [m²]), number of pregnancies and deliveries, number of days of gestation, and history of uterine scars. Blood samples were collected from the study participants to test for 25-hydroxy Vitamin D3 (25-(OH)-D3), Hcy, thyroid function, and thyroid peroxidase antibodies (TPOAbs). Data on dietary habits (eg, vitamin D supplementation, fish consumption), physical activity frequency, and season of blood collection (winter/spring vs summer/autumn) were retrospectively extracted from medical records. Blood samples were collected from fasting participants between 8:00 and 10:00 AM to minimize diurnal variation. Serum 25-(OH)-D3 levels were measured using chemiluminescence immunoassay (CLIA, Roche Diagnostics, Cobas e601 analyzer). Hcy was quantified via enzymatic cycling assay (Abbott ARCHITECT c8000), and thyroid function tests (TSH, FT3, FT4) were performed using electrochemiluminescence immunoassay (Roche Cobas e411). All assays followed manufacturer protocols, and internal quality controls were run daily with inter-assay coefficients of variation < 5%. This study was approved by the Ethics Committee of the Second People’s Hospital of Hefei (Approval Number: No.2022-KY-131).
Judgment Criteria for Clinical Data
(1) Vitamin D level: 25-(OH)-D3 ≥ 75 nmol/L indicated Vitamin D sufficiency; 50 nmol/L ≤ 25-(OH)-D3 < 75 nmol/L indicated Vitamin D insufficiency; 25-(OH)-D3 < 50 nmol/L indicated Vitamin D deficiency.10 (2) Hcy ≥ 15 μmol/L was considered hyperhomocysteinemia (H-Hcy).11 (3) TSH ≤ 4.0 mIU/L was considered normal thyroid function.12 The judgment criteria for thyroid function-related indexes were based on the reference values provided by the Laboratory Department of the Second People’s Hospital of Hefei. Specifically, free triiodothyronine (FT3): 1.58 to 3.91 pg/mL; free thyroxine (FT4): 0.70 to 1.48 ng/dL; triiodothyronine (T3): 0.58 to 1.62 ng/dL; thyroxine (T4): 5.00 to 14.50 μg/mL; TPOAb: < 9.00 IU/mL. Single-time-point measurements were adopted due to resource constraints. Although this approach limits the assessment of temporal variability, all assays were performed in duplicate, and results with intra-assay CV > 10% were excluded. Instrument calibration was performed weekly using certified reference materials.
Statistical Methods
The data were analyzed using SPSS software, version 26.0. One-way ANOVA was used to compare quantitative data between the two groups. For qualitative data comparisons, either the chi-square test or Fisher’s exact test was applied. Multivariate logistic regression analysis was conducted to identify risk factors associated with MA. Multivariate logistic regression models were adjusted for age, BMI, parity, dietary habits, and season of blood collection. A P < 0.05 was considered statistically significant.
Results
Comparison of General Clinical Data
Quantitative data was expressed as mean ± standard deviation  . No statistically significant differences were observed between the two groups in terms of age, BMI, number of pregnancies and deliveries, history of uterine scars, or number of days of gestation (P > 0.05). However, the incidence of abortion history was significantly higher in the study group compared to the control group (χ² = 7.272, P = 0.007) indicating a statistically significant difference (Table 1).
. No statistically significant differences were observed between the two groups in terms of age, BMI, number of pregnancies and deliveries, history of uterine scars, or number of days of gestation (P > 0.05). However, the incidence of abortion history was significantly higher in the study group compared to the control group (χ² = 7.272, P = 0.007) indicating a statistically significant difference (Table 1).
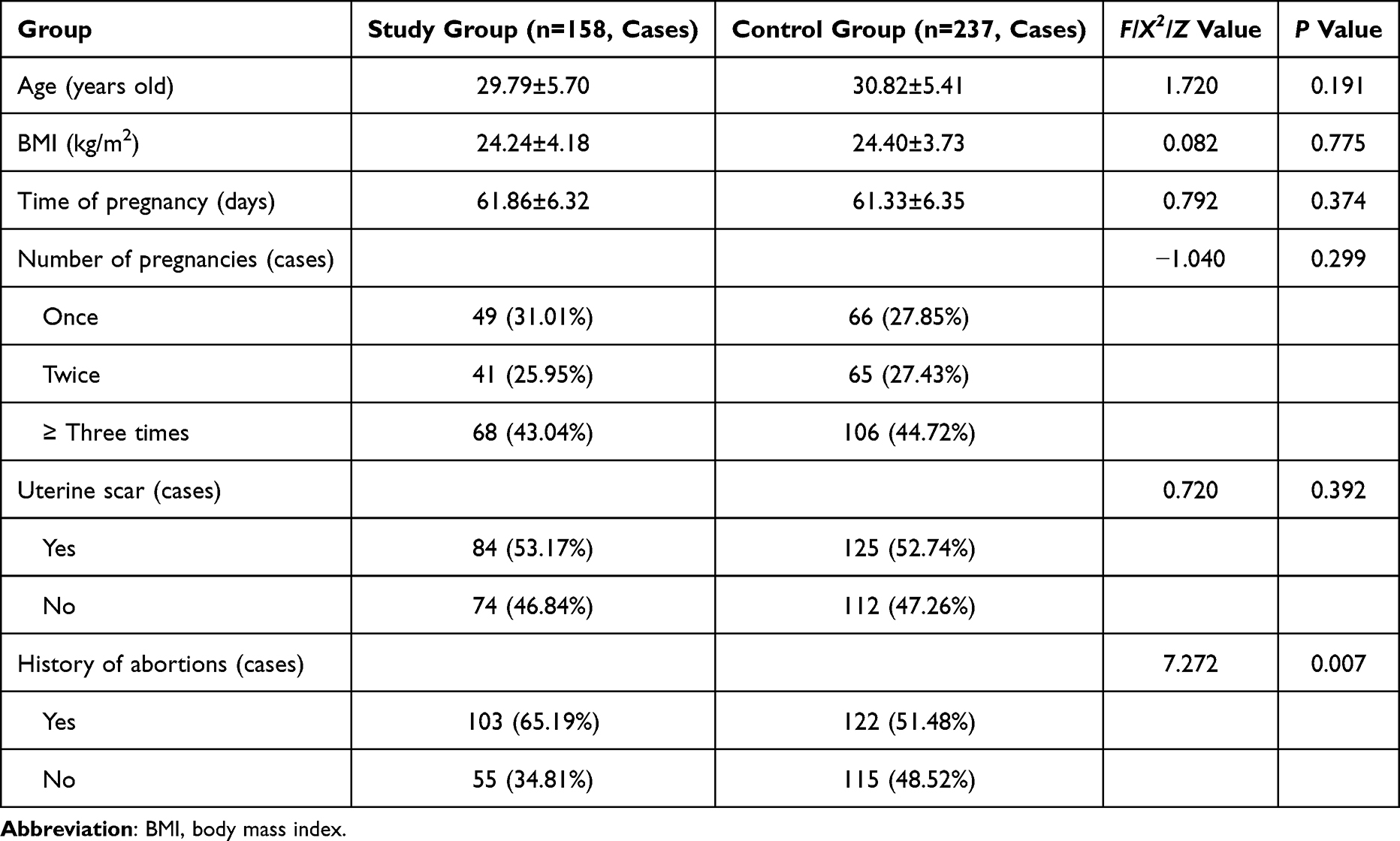 |
Table 1 Baseline Characteristics of the Study and Control Groups |
Comparison of Vitamin D Levels
The mean serum 25-(OH)-D3 level in the MA group (38.2 ± 12.5 nmol/L) was significantly lower than in the control group (52.7 ± 15.3 nmol/L), with a mean difference of −14.5 nmol/L (95% CI: −18.2 to −10.8; P = 0.027). In the study group, 121 women (76.58%) demonstrated 25-(OH)-D3 deficiency, 25 women (15.82%) exhibited insufficiency, and only 12 women (7.59%) had sufficient levels. In comparison, in the control group, 159 women (67.09%) exhibited 25-(OH)-D3 deficiency, 36 women (15.19%) exhibited insufficiency, and 42 women (17.72%) had sufficient levels. The study group exhibited a significantly higher prevalence of 25-(OH)-D3 deficiency (76.58% vs 67.09%, P = 0.013), with an adjusted OR of 1.82 (95% CI: 1.12–2.95) for MA risk (Table 2).
 |
Table 2 Comparison of Vit D Levels Between the Two Groups |
Comparison of Serum Hcy Levels
Serum Hcy levels in the study group were significantly higher than those in the control group (F = 6.914, P = 0.009). In the study group, 39 women (24.68%) had H-Hcy, while in the control group, 32 women (13.50%) had H-Hcy. H-Hcy ≥ 15 μmol/L was observed in 24.68% of MA cases versus 13.50% of controls, representing an 82.8% increased risk (Relative Risk = 1.83, 95% CI: 1.21–2.76; P = 0.005) (Table 3).
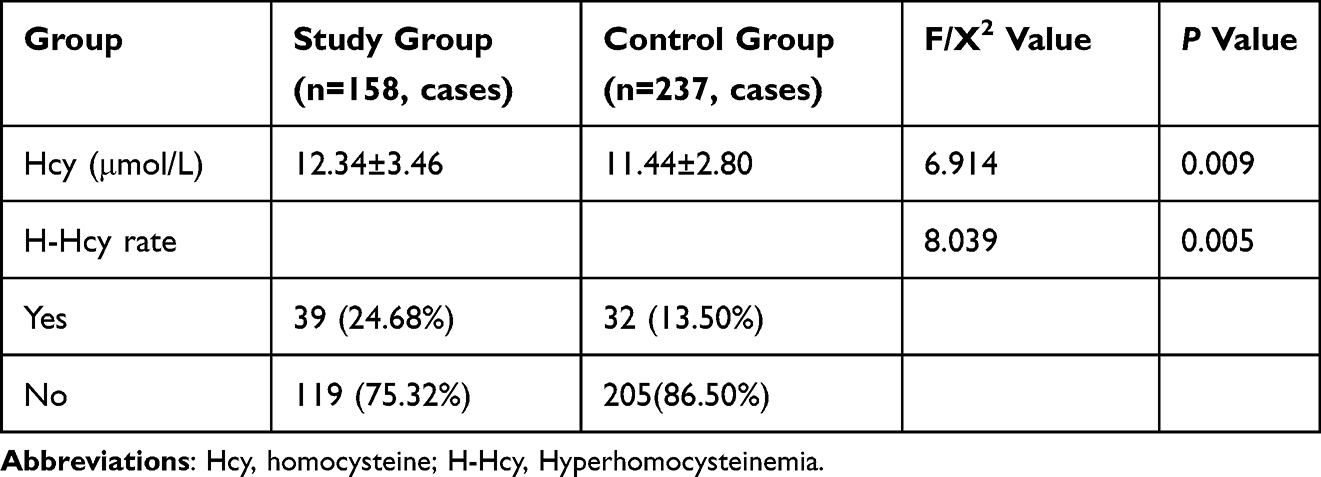 |
Table 3 Comparison of Hcy Levels Between the Two Groups |
Comparison of Thyroid Function-Related Indices Between the Two Groups
No statistically significant differences were observed in FT4 and T4 levels between the two groups (P > 0.05). However, the levels of T3, FT3, TSH, and TPOAb were significantly higher in the study group compared to the control group (P < 0.05). The rate of elevated TSH was significantly higher in the study group than in the control group (P = 0.018). Furthermore, the incidence of positive TPOAb was also higher in the study group compared to the control group (P = 0.015) (Table 4).
 |
Table 4 Comparison of Thyroid Function Between the Two Groups |
Risk Factors of MA and Correlation Analysis
While individual associations between MA and factors such as vitamin D deficiency, H-Hcy, or thyroid dysfunction have been reported in prior studies, this study uniquely integrates these variables into a multivariate model. Our analysis highlights the combined impact of these factors, demonstrating that their synergistic effects may amplify the risk of MA, a perspective less explored in existing literature.
Logistic regression analysis was performed using clinical indicators that showed statistically significant differences between the two groups as independent variables, with the occurrence of MA as the dependent variable. The results identified several risk factors for MA, including a history of abortions, elevated Hcy levels, increased TSH, and positive TPOAb. Conversely, adequate levels of Vitamin D were found to be a protective factor against MA. Specifically, Each prior abortion was associated with a 41.5% increase in MA risk (odds ratio [OR] = 1.415 per abortion, 95% CI: 1.251–1.687). Women with ≥ 2 previous abortions had an OR of 2.63 (95% CI: 1.89–3.67) compared to nulligravid women. Adequate 25-(OH)-D3 levels were associated with a decreased risk of MA (OR = 0.732, 95% CI: 0.610–3.171), suggesting a protective role for Vitamin D. Elevated H-Hcy levels were associated with an increased risk of MA (OR = 1.336, 95% CI: 1.183–1.618), indicating Hcy as a potential risk factor. Women with TSH ≥4 mIU/L had a 3.8-fold higher risk of MA compared to those with normal TSH (OR = 3.80, 95% CI: 2.06–7.04; P < 0.001). This represents the strongest modifiable risk factor identified in our analysis, highlighting elevated TSH as a risk factor. Additionally, TPOAb positivity (≥ 9 IU/mL) was associated with an 81.9% elevated MA risk (OR = 1.82, 95% CI: 1.09–3.05; P = 0.022). The risk further increased to OR = 2.95 (95% CI: 1.45–5.98) when combined with TSH ≥ 4 mIU/L, suggesting TPOAb positivity as another potential risk factor. Subgroup analysis revealed that women with both vitamin D deficiency (25-(OH)-D3 <50 nmol/L) and H-Hcy ≥ 15 μmol/L had a 4.2-fold higher risk of MA (OR = 4.2, 95% CI: 2.1–8.5) compared to those with normal levels, underscoring the clinical significance of addressing multiple risk factors simultaneously.
The observed associations may reflect underlying pathophysiological interactions. For instance, vitamin D deficiency could impair immune tolerance and placental angiogenesis, while elevated Hcy levels may induce oxidative stress and endothelial dysfunction, collectively disrupting early pregnancy maintenance. Additionally, thyroid autoimmunity (as indicated by TPOAb positivity) and elevated TSH might further exacerbate these effects by altering hormonal balance and inflammatory responses. Although our study design precludes causal inferences, these hypotheses align with emerging evidence on multifactorial pregnancy loss mechanisms and warrant further experimental validation.
Key Quantitative Findings: Vitamin D deficiency conferred the highest population-attributable risk (PAR = 34.2%), followed by elevated TSH (PAR = 28.7%) and H-Hcy (PAR = 19.5%).The combined effect of all three factors (Vitamin D deficiency + TSH ≥ 4 + H-Hcy) resulted in an OR of 8.92 (95% CI: 4.15–19.14).
Discussion
MA is a common pathological condition during pregnancy, and as China adjusts its contraception policies and experiences ongoing societal changes, the associated challenges—both familial and societal—are becoming increasingly pronounced. As a result, preventing and managing MA has become urgent concerns for obstetricians and gynecologists. The pathogenesis and etiology of MA are complex, with recent research suggesting that embryonic chromosomal abnormalities may play a key role in its occurrence. Additionally, environmental factors, hormonal imbalances, and other variables are closely linked to its development.13,14 Studies on endocrine and immune factors have revealed correlations between thyroid function, Vitamin D, Hcy, and MA. Furthermore, Vitamin D may act as a significant trigger for the development of MA.15
Vitamin D is an essential nutrient for normal pregnancy outcomes, and its deficiency has been associated with several adverse pregnancy outcomes, including increased risk of MA. Over half of pregnant women experience Vitamin D deficiency or insufficiency, with high rates observed globally.16 Seasonal variations also affect Vitamin D levels, with more pronounced deficiencies occurring in winter. This is likely due to reduced outdoor activity during the colder months, which hampers the synthesis and absorption of Vitamin D.
Immune tolerance at the maternal-fetal interface is crucial for a successful pregnancy. A balanced interaction between the inflammatory axes, Th1/Th2 and Treg/Th17, regulated by Vitamin D, is key to sustaining immune tolerance. An increase in Th1/Th2 levels during pregnancy heightens the immune-inflammatory response, while Treg/Th17 cells produce anti-inflammatory cytokines to help maintain immune homeostasis. In cases of Vitamin D deficiency, Th1/Th2 levels rise, while Treg/Th17 levels decrease. This imbalance compromises immune tolerance at the maternal-fetal interface, leading to a higher risk of adverse pregnancy outcomes.17–19 Vitamin D also plays an important role in maintaining immune balance between uterine natural killer (NK) cells and peripheral blood NK cells. It regulates receptor expression, cytokine secretion, and NK cell binding to target cells, reducing the cytotoxic effects of peripheral blood NK cells on embryos.20 Thus, Vitamin D is critical for immune tolerance at the maternal-fetal interface and serves as an independent risk factor for adverse pregnancy outcomes. In this study, serum 25-(OH)-D3 levels, a marker of Vitamin D status, were lower in the study group than in the control group. Furthermore, the prevalence of Vitamin D deficiency was higher among women in the study group. These findings suggest that Vitamin D insufficiency or deficiency may increase the risk of MA. Therefore, improving Vitamin D levels in pregnant women could contribute to better pregnancy outcomes. Hcy, widely recognized as an independent risk factor for cardiovascular disease, has also been shown to impact the female reproductive system. This dual role of vitamin D in regulating both Hcy metabolism and thyroid autoimmunity may explain its protective effect against MA, as demonstrated in our multivariate analysis (OR = 0.732).
Hcy is primarily eliminated from the body through metabolic pathways, with only a small fraction remaining in the bloodstream at low levels.21 During pregnancy, Hcy levels tend to be lower than in non-pregnant women due to blood dilution from increased blood volume and enhanced utilization. However, if pregnant women have genetic variations in enzymes or deficiencies in metabolic cofactors, Hcy can accumulate. H-Hcy can damage vascular endothelial cells, disrupt their mRNA expression, and result in abnormal production of angiogenesis factors. This imbalance can impair the body’s antioxidant defenses, alter coagulation processes, and lead to poor vascularization in the placental villi and decidua. These effects may increase the risk of MA and other adverse pregnancy outcomes.22 Notably, abnormal Hcy metabolism is closely linked to genetic factors. For instance, the MTHFR C677T gene polymorphism can impair folate metabolism, leading to elevated Hcy levels. Pregnant women with the MTHFR TT genotype exhibit significantly higher Hcy levels compared to those with CC/CT genotypes, which correlates with an increased risk of recurrent miscarriage 3333. Additionally, mutations in the cystathionine beta-synthase gene may disrupt Hcy metabolic pathways. Although genetic data were not collected in this study, genetic variants likely contribute to H-Hcy in some patients. Future studies should integrate genotyping analyses to clarify gene-environment interactions in MA pathogenesis.
Previous studies have highlighted a link between H-Hcy in the embryo culture medium and transfer failure. H-Hcy may trigger the production of reactive oxygen species (ROS), which disrupt the embryonic environment and lower the success rate of embryo transfer.23,24 Additionally, H-Hcy can interfere with DNA methylation in embryonic cells, disrupting essential processes like cell proliferation and apoptosis. This disruption can cause abnormal growth and development of embryos and fetuses, ultimately increasing the risk of malformations and adverse pregnancy outcomes.25
In this study, the incidence of H-Hcy was significantly higher in the study group (24.68%) compared to the control group (13.50%) as shown in Table 3. This suggests that Hcy accumulation may be associated with MA, consistent with previous research. The study also found that women experiencing MA had higher H-Hcy levels compared to those with normal early pregnancies that required termination. Furthermore, individuals with H-Hcy had a significantly higher risk of MA (OR = 1.336, 95% CI: 1.183–1.618), indicating that H-Hcy could serve as a potential risk factor for MA. Therefore, Hcy levels may be useful as a predictor for pregnancy outcomes.
The endocrine profile of pregnant women differs from that of non-pregnant women. An imbalance between the supply and demand for TH during pregnancy can affect fetal development. In severe cases, this imbalance may lead to MA during early pregnancy.26 In this study, while there were no statistically significant differences in serum T3, T4, FT3, and FT4 levels between the two groups, the study group exhibited higher levels of TSH and TPOAb compared to the control group. Additionally, the incidence of TSH levels ≥ 4.0 mIU/L was higher in the study group than in the control group.
Typically, TSH levels are lower during normal pregnancy. However, elevated TSH levels disrupt the balance of the Th1/Th2 axis in decidual cells, which can impair immune tolerance at the maternal-fetal interface and increase the risk of adverse pregnancy outcomes.27,28 This mechanism is similar to what occurs in Vitamin D deficiency. High TSH levels not only inhibit the thyroid axis through negative feedback, leading to decreased thyroid function that can impact embryonic development and result in MA, but they also suppress progesterone production by granulosa cells and hinder placental function. These effects can interfere with embryonic development, increasing the likelihood of threatened abortion and, in severe cases, MA.
Thyroid autoantibodies not only recognize and bind to their specific antigens but also target receptors for human chorionic gonadotropin (HCG), which share similarities with antigens found in the zona pellucida and placenta. Specifically, these autoantibodies target the HCG receptor on the corpus luteum, impairing its ability to support a normal pregnancy, which can lead to MA.29 In this study, the rate of positive TPOAb was significantly higher in the study group compared to the control group, indicating that positive TPOAb may serve as a risk factor for MA. Previous research has demonstrated that women with abnormal thyroid function and positive TPOAb are at an increased risk of MA, developmental abnormalities, and other pregnancy complications. Therefore, monitoring thyroid function in pregnant women is crucial for early detection and intervention, which can improve pregnancy outcomes.30
Numerous studies have shown a positive correlation between Vitamin D deficiency, H-Hcy and TSH levels, and the presence of positive TPOAb with the development of MA. Vitamin D has the ability to influence the balance of Th1/Th2 cells, thereby modulating the expression of TPOAb. Research indicates that Vitamin D supplementation in pregnant women with normal thyroid function and positive TPOAb can significantly reduce the expression levels of TPOAb.31 In a prospective study, Vitamin D intervention was provided to pregnant women, and the results demonstrated that serum Hcy levels were lower in the study group compared to the control group, along with a reduction in pregnancy complications.32 This suggests that Vitamin D’s role in promoting positive immune regulation may contribute to these outcomes, consistent with the findings of our study. Additionally, the risk of MA was higher in women with a history of previous abortion (OR = 1.415, 95% CI: 1.251–1.687). This suggests that a history of abortion may increase the risk of MA, potentially due to endometrial damage or infections related to the procedure, which can trigger an immune-inflammatory response. This response may disrupt immune tolerance at the maternal-fetal interface in subsequent pregnancies.
This study identified correlations between Vitamin D, Hcy, TSH, TPOAb, and MA. These findings provide valuable insights for clinical decision-making. However, the study had several limitations. Notably, the absence of relevant immune indicators prevented a deeper exploration of the mechanisms through which Vitamin D may exert its effects. Additionally, factors such as dietary habits, work, and living environments could have influenced data collection, potentially introducing biases. While serum Hcy levels can be affected by multiple factors, this study did not comprehensively account for the potential influence of diet or the living environment. Furthermore, while miscarriage was considered as a pregnancy outcome, cases of threatened abortion were not included, limiting the broader applicability of the findings.
Clinically, our findings suggest that a composite assessment of vitamin D, Hcy, and thyroid function could refine risk stratification for MA. For example, women with concurrent deficiencies in vitamin D and elevated Hcy may benefit from targeted interventions (eg, vitamin D supplementation and folate therapy) to mitigate MA risk. This integrated approach represents a pragmatic advancement over single-biomarker strategies currently in use.
This study has several limitations. First, the retrospective design may introduce information bias. For example, data on confounders such as folate intake or genetic polymorphisms rely on the completeness of medical records, which were not systematically collected. Furthermore, selection bias may arise because the control group comprised only women opting for elective termination, potentially underrepresenting the general pregnant population. Second, although we adjusted for key confounders, unmeasured factors (eg, genetic predisposition, detailed sunlight exposure) could influence outcomes. Third, vitamin D levels may vary seasonally; however, our analysis accounted for blood collection season. Future prospective studies with repeated measurements are warranted to validate these findings. Additionally, interventional trials could test whether correcting vitamin D deficiency or reducing Hcy levels lowers MA incidence, thereby translating our findings into clinical practice.
Conclusion
In conclusion, this study confirms that vitamin D deficiency, H-Hcy, elevated TSH levels, and the presence of positive TPOAb are closely associated with MA. A history of abortion, along with H-Hcy, TSH, and positive TPOAb, have been identified as significant risk factors for MA. Additionally, Vitamin D plays a crucial role in maintaining a healthy pregnancy. Our findings highlight four modifiable risk factors for missed abortion: vitamin D deficiency (25-(OH)-D3 <50 nmol/L), H-Hcy ≥ 15 μmol/L, subclinical hypothyroidism (TSH ≥ 4 mIU/L), and TPOAb positivity (≥ 9 IU/mL). Among these, vitamin D insufficiency emerges as the most actionable target for prevention. Therefore, clinical practice should prioritize testing for Vitamin D levels, Hcy, and thyroid function in women preparing for pregnancy or in the early stages of pregnancy. Early intervention is essential to reduce the incidence of MA.
Abbreviations
25-(OH)-D3, 25-hydroxy Vitamin D3; MA, missed abortion; TH, thyroid hormones; TPOAb, thyroid peroxidase antibodies; Hcy, homocysteine; H-Hcy, Hyperhomocysteinemia; TBG, thyroxine binding globulin; FT3, free triiodothyronine; FT4, free thyronine; T3, triiodothyronine; T4, thyroxine; TSH, thyroid stimulating hormone; HCG, human chorionic gonadotropin.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki (as was revised in 2013). The study was approved by Ethics Committee of the Second People’s Hospital of Hefei (Approval Number: No.2022-KY-131). Written informed consent was obtained from all participants.
Acknowledgments
We are particularly grateful to all the people who have given us help on our article.
Funding
No external funding received to conduct this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Gong G, Yin C, Huang Y, et al. A survey of influencing factors of missed abortion during the two-child peak period. J Obstet Gynaecol. 2021;41(6):977–980. doi:10.1080/01443615.2020.1821616
2. Radzinsky VE, Ramazanova FU, Khamoshina MB, Azova MM, Orazov MR, Orazmuradov AA. Vitamin D insufficiency as a risk factor for reproductive losses in miscarriage. Gynecol Endocrinol. 2021;37(sup1):8–12. doi:10.1080/09513590.2021.2006451
3. Verdoia M, Nardin M, Gioscia R, et al. Association between vitamin D deficiency and serum Homocysteine levels and its relationship with coronary artery disease. J Thromb Thrombolysis. 2021;52(2):523–531. doi:10.1007/s11239-021-02391-w
4. Kaplan P, Tatarkova Z, Sivonova MK, et al. Homocysteine and Mitochondria in Cardiovascular and Cerebrovascular Systems. Int J Mol Sci. 2020;21(20):7698. doi:10.3390/ijms21207698
5. Portillo F, Vázquez J, Pajares MA. Protein-protein interactions involving enzymes of the mammalian methionine and homocysteine metabolism. Biochimie. 2020;173:33–47. doi:10.1016/j.biochi.2020.02.015
6. Ding X, Wang Y, Liu J, Wang G. Impaired Sensitivity to Thyroid Hormones Is Associated With Elevated Homocysteine Levels in the Euthyroid Population. J Clin Endocrinol Metab. 2022;107(9):e3731–e3737. doi:10.1210/clinem/dgac371
7. Barjaktarovic M, Steegers EAP, Jaddoe VWV, et al. The Association of Thyroid Function With Maternal and Neonatal Homocysteine Concentrations. J Clin Endocrinol Metab. 2017;102(12):4548–4556. doi:10.1210/jc.2017-01362
8. Haddow JE, McClain MR, Lambert-Messerlian G, et al. Variability in thyroid-stimulating hormone suppression by human chorionic gonadotropin during early pregnancy. J Clin Endocrinol Metab. 2008;93(11):4552. doi:10.1210/jc.2008-0568
9. McKinnon B, Li H, Richard K, et al. Synthesis of thyroid hormone binding proteins transthyretin and albumin by human trophoblast. J Clin Endocrinol Metab. 2005;90(12):6714–6720. doi:10.1210/jc.2005-0696
10. Holick MF. Vitamin D: evolutionary, physiological and health perspectives. Curr Drug Targets. 2011;12(1):4–18. doi:10.2174/138945011793591635
11. Guieu R, Ruf J, Mottola G. Hyperhomocysteinemia and cardiovascular diseases. Ann Biol Clin. 2022;80(1):7–14. doi:10.1684/abc.2021.1694
12. Du H, Wu D, Zhou X, et al. Preconception TSH and Adverse Pregnancy Outcomes in China: a Nationwide Prospective Cohort Study. J Clin Endocrinol Metab. 2022;107(7):e2770–e2776. doi:10.1210/clinem/dgac208
13. Lidegaard, Mikkelsen AP, Egerup P, et al. Pregnancy loss: a 40-year nationwide assessment. Acta Obstet Gynecol Scand. 2020;99(11):1492–1496. doi:10.1111/aogs.13860
14. Zhang X, Li J, Gu Y, et al. A pilot study on environmental and behavioral factors related to missed abortion. Environ Health Prev Med. 2011;16(4):273–278. doi:10.1007/s12199-010-0196-4
15. Bespalova O, Bakleicheva M, Kovaleva I, et al. Expression of vitamin D and vitamin D receptor in chorionic villous in missed abortion. Gynecol Endocrinol. 2019;35(sup1):49–55. doi:10.1080/09513590.2019.1653563
16. Holick MF, Chen TC. Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr. 2008;87(4):1080S–6S. doi:10.1093/ajcn/87.4.1080S
17. Jiao X, Wang L, Wei Z, et al. Vitamin D deficiency during pregnancy affects the function of Th1/Th2 cells and methylation of IFN-γ gene in offspring rats. Immunol Lett. 2019;212:98–105. doi:10.1016/j.imlet.2019.06.012
18. Ji J, Zhai H, Zhou H, et al. The role and mechanism of vitamin D-mediated regulation of Treg/Th17 balance in recurrent pregnancy loss. Am J Reprod Immunol. 2019;81(6):e13112. doi:10.1111/aji.13112
19. Muyayalo KP, Huang XB, Qian Z, et al. Low circulating levels of vitamin D may contribute to the occurrence of preeclampsia through deregulation of Treg /Th17 cell ratio. Am J Reprod Immunol. 2019;82(4):e13168. doi:10.1111/aji.13168
20. Chen X, Diao L, Lian R, et al. Potential impact of maternal vitamin D status on peripheral blood and endometrium cellular immunity in women with recurrent implantation failure. Am J Reprod Immunol. 2020;84(1):e13243. doi:10.1111/aji.13243
21. Finkelstein JD. The metabolism of homocysteine: pathways and regulation. Eur J Pediatr. 1998;157(2):S40–S44. doi:10.1007/PL00014300
22. Dogan GO, Sahin O. Exploring the association of hyperhomocysteinemia with early pregnancy losses: a retrospective case-control study in a tertiary clinic in Türkiye. Medicine. 2024;103(32):e39101. doi:10.1097/MD.0000000000039101
23. Boyama BA, Cepni I, Imamoglu M, et al. Homocysteine in embryo culture media as a predictor of pregnancy outcome in assisted reproductive technology. Gynecol Endocrinol. 2016;32(3):193–195. doi:10.3109/09513590.2015.1102877
24. Ogawa S, Ota K, Takahashi T, et al. Impact of Homocysteine as a Preconceptional Screening Factor for In Vitro Fertilization and Prevention of Miscarriage with Folic Acid Supplementation Following Frozen-Thawed Embryo Transfer: a Hospital-Based Retrospective Cohort Study. Nutrients. 2023;15(17):3730. doi:10.3390/nu15173730
25. Zhang H, Wang Y, Sang Y, et al. Combination of S-adenosylhomocysteine and scriptaid, a non-toxic epigenetic modifying reagent, modulates the reprogramming of bovine somatic-cell nuclear transfer embryos. Mol Reprod Dev. 2014;81(1):87–97. doi:10.1002/mrd.22287
26. Dhillon-Smith RK, Melo P, Kaur R, et al. Interventions to prevent miscarriage. Fertil Steril. 2023;120(5):951–954. doi:10.1016/j.fertnstert.2023.08.955
27. Kuroda K, Matsumura Y, Ikemoto Y, et al. Analysis of the risk factors and treatment for repeated implantation failure: oPtimization of Thyroid function, IMmunity, and Uterine Milieu (OPTIMUM) treatment strategy. Am J Reprod Immunol. 2021;85(5):e13376. doi:10.1111/aji.13376
28. Liu S, Xu F, Wei H, et al. The correlation of thyroid autoimmunity and peripheral and uterine immune status in women with recurrent miscarriage. J Reprod Immunol. 2020;139:103118. doi:10.1016/j.jri.2020.103118
29. Gungor K, Dokuzeylul Gungor N. Antithyroid antibodies may predict serum beta HCG levels and biochemical pregnancy losses in euthyroid women with IVF single embryo transfer. Gynecol Endocrinol. 2021;37(8):702–705. doi:10.1080/09513590.2020.1830968
30. Thangaratinam S, Tan A, Knox E, et al. Association between thyroid autoantibodies and miscarriage and preterm birth: meta-analysis of evidence. BMJ. 2011;342:d2616. doi:10.1136/bmj.d2616
31. Aktaş HŞ. Vitamin B12 and Vitamin D Levels in Patients with Autoimmune Hypothyroidism and Their Correlation with Anti-Thyroid Peroxidase Antibodies. Med Princ Pract. 2020;29(4):364–370. doi:10.1159/000505094
32. Godfrey KM, Titcombe P, El-Heis S, et al. Maternal B-vitamin and vitamin D status before, during, and after pregnancy and the influence of supplementation preconception and during pregnancy: prespecified secondary analysis of the NiPPeR double-blind randomized controlled trial. PLoS Med. 2023;20(12):e1004260. doi:10.1371/journal.pmed.1004260
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence and Associated Factors of Vitamin D Deficiency in High Altitude Region in Saudi Arabia: Three-Year Retrospective Study
Abdelsalam M, Nagy E, Abdalbary M, Alsayed MA, Ali AAS, Ahmed RM, Alsuliamany ASM, Alyami AH, Althaqafi RMM, Alsaqqa RM, Ali SI, Aljohani B, Alghamdi AA, Alghamdi FA, Alsulaimani AA
International Journal of General Medicine 2023, 16:2961-2970
Published Date: 12 July 2023