")
Back to Journals » International Journal of General Medicine » Volume 16
Prevalence and Associated Factors of Vitamin D Deficiency in High Altitude Region in Saudi Arabia: Three-Year Retrospective Study
Authors Abdelsalam M , Nagy E , Abdalbary M, Alsayed MA, Ali AAS, Ahmed RM, Alsuliamany ASM, Alyami AH , Althaqafi RMM, Alsaqqa RM, Ali SI, Aljohani B, Alghamdi AA, Alghamdi FA, Alsulaimani AA
Received 17 May 2023
Accepted for publication 3 July 2023
Published 12 July 2023 Volume 2023:16 Pages 2961—2970
DOI https://doi.org/10.2147/IJGM.S418811
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mostafa Abdelsalam,1,2 Eman Nagy,2 Mohamed Abdalbary,2 Mona Abdellatif Alsayed,1,3 Amr Abouzed Salama Ali,4 Reham Metwally Ahmed,1 Abdulbadie Saleh M Alsuliamany,1 Ali H Alyami,5– 7 Raad MM Althaqafi,8 Raghad M Alsaqqa,9 Safaa Ibrahim Ali,10 Bakar Aljohani,11 Ahmed Abdullah Alghamdi,12 Faisal A Alghamdi,9 Adnan A Alsulaimani1
1Internal Medicine Department, Alameen General Hospital, Taif, Saudi Arabia; 2Mansoura Nephrology and Dialysis Unit, Internal Medicine Department, Faculty of Medicine, Mansoura University, Mansoura, Egypt; 3Department of Pediatrics, Faculty of Medicine, Mansoura University, Mansoura, Egypt; 4Mansoura Medical District, Family Medicine Hospitals, Ministry of Health, Mansoura, Egypt; 5Department of Surgery, Ministry of the National Guard – Health Affairs, Jeddah, Saudi Arabia; 6Department of Surgery, Abdullah International Medical Research Center, Jeddah, Saudi Arabia; 7Department of Orthopedics, King Saud Bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia; 8Orthopedic Surgery Department, King Abdulaziz Specialist Hospital, Taif, Saudi Arabia; 9College of Medicine, Taif University, Taif, Saudi Arabia; 10General Medicine Faculty, Sechenov University, Moscow City, Russian Federation; 11Neuroradiology, AlHada Military Hospital, Taif, Saudi Arabia; 12College of Medicine, Al-Baha University, Al Baha, Saudi Arabia
Correspondence: Eman Nagy, Mansoura Nephrology and Dialysis Unit, Internal Medicine Department, Faculty of Medicine, Mansoura University, Mansoura, Egypt, Email [email protected]
Background: Vitamin D has many functions in the human body, and its deficiency is associated with skeletal and non-skeletal diseases. Vitamin D deficiency (blood level of 25 (OH) vitamin D < 20 ng/mL) has been reported worldwide, including Kingdom of Saudi Arabia (KSA). Its prevalence and associated factors vary according to KSA region. Therefore, this study aimed to explore the prevalence and risk factors of vitamin D deficiency in the Taif region of KSA.
Methods: This retrospective study included patients who attended outpatient clinics at the Alameen General Hospital from 2019 to 2021. Demographic, clinical, and laboratory data were collected using a hospital software system.
Results: The study included 2153 patients and vitamin D deficiency was diagnosed in 900 (41.8%) of whom were diagnosed with vitamin D deficiency. It was more common in males (P=0.021), younger age (< 0.001), and in patients without comorbidities. There was a positive correlation between 25 (OH) vitamin D levels and blood cholesterol, high-density lipoprotein, calcium, and vitamin B12 levels. In the binary logistic regression analysis, age was the most significant predictor (P< 0.001), followed by the absence of thyroid disease (P=0.012) and asthma (P=0.030).
Conclusion: Vitamin D deficiency is common in the Saudi population despite sunny weather in KSA. It is more prevalent among males, younger individuals, and those without comorbidities such as thyroid diseases and asthma.
Keywords: vitamin D, prevalence, risk factors, KSA, calcium
Introduction
Vitamin D deficiency is currently recognized as a major health problem worldwide, affecting both sexes and all age groups.1 A severe vitamin D deficiency may result in rickets in infants and children, osteomalacia in adults, and subclinical vitamin D deficiency, which is more prevalent and is linked to osteoporosis. In addition, vitamin D deficiency is associated with non-skeletal diseases.2
Sun exposure is the main source of vitamin D in addition to dietary intake.3 Different factors regulate vitamin D in the body, such as serum calcium levels, parathyroid hormone (PTH) levels, intestinal absorption, and renal function.4
Vitamin D deficiency is diagnosed by measuring the serum concentration of 25-hydroxyvitamin D or 25(OH)D, which is deemed deficient when it drops below 20 ng/mL and insufficient when the 25(OH)D level is 21–29 ng/mL.5 Multiple factors contribute to vitamin D deficiency, some of which are related to the residential region and its impact on weather, availability of food products rich in vitamin D, local culture, and life style.6
In the Kingdom of Saudi Arabia (KSA), despite the plentiful sunshine available throughout the year in all regions and the availability of food products rich in vitamin D, there is a high prevalence of vitamin D deficiency in different age and sex groups. Vitamin D deficiency is more common in female with KSA.7 Between 2013 and 2014, a school-based cross-sectional study was conducted in three regions of Saudi Arabia. Vitamin D deficiency and insufficiency are prevalent in the Central, Western, and Eastern regions of KSA. Additionally, women, residents of the eastern region, and people from lower socioeconomic classes are at higher risk.8
Regarding Taif City, a retrospective study among orthopedic patients conducted between 2016 and 2017 revealed that 15.4% of patients had a normal level of 25 (OH) vitamin D, whereas 53.1% of patients had vitamin D deficiency. Male patients had a higher prevalence of deficiency (60.3%) than did female patients (51%). All age categories demonstrated a significant prevalence of insufficiency, with the 19-year-old age group showing the highest frequency.9 A study conducted among female students at Taif University to estimate 25 (OH) vitamin D and calcium levels revealed that young females had a significant frequency of vitamin D deficiency with normal calcium levels.10
All previous studies agree on the presence of a high prevalence of vitamin D deficiency among the residents of Taif city, but there is also a significant variance in the highest prevalence among different age groups and sexes. This study aimed to evaluate the levels of 25 (OH) vitamin D and assess the prevalence of vitamin D deficiency among both sexes and different age groups in Taif city and its relationship with other clinical and laboratory findings.
Methods
This retrospective study included all patients who visited the outpatient clinics at Alameen General Hospital in Taif City from 1st January 2019 to 31st December 2021, and underwent 25 (OH) vitamin D evaluation for any cause. The study was conducted according to the declaration of Helsinki and approved by IRB committee of Research and Studies Department, Directorate of Health Affairs, Taif (Registration number HP-02-T-067 and approval number 791). Patients whose laboratory results were unavailable, who were taking vitamin D supplements, or who had comorbidities affecting calcium and vitamin D metabolism were excluded from the study.
Patients who visited the outpatient clinics of Alameen General Hospital in Taif City throughout the three years of the study were 3560 and 1407 patients were excluded due to unavailability of 25 (OH) vitamin D assays or prescribed vitamin D supplements. Thus, 2153 patients were enrolled in the study.
A hospital software system was used to retrieve patient data. This software was used to collect demographic, clinical, and biochemical data. The demographic data included age, gender, and nationality of the patients. The presence of comorbidities (such as hypertension, diabetes mellitus, osteoporosis, gout, and heart and thyroid diseases) were collected from the system. In addition, estimated glomerular filtration rate (eGFR), complete blood count (CBC), thyroid function tests, fasting lipid profile, liver function tests, hemoglobin A1c, erythrocyte sedimentation rate (ESR), C-reactive protein, levels of 25 (OH) vitamin D and vitamin B12, and serum creatinine and calcium were obtained from the software system.
Efforts were made to minimize possible biases in the data and data analysis. Selection bias was minimized by enrolling all qualified patients in the sample. Misclassification or information bias was controlled using validated data collection instruments.
Statistical Analysis
Data was coded, computed and analyzed using Statistical Package for the Social Sciences (SPSS) version 25. Frequency tables were used to present qualitative data (numbers and percentages). The Shapiro–Wilk test was used to determine the normality of the quantitative data, and the median and interquartile range (25th – 75th percentile) were used to present the results. To examine the relationship between categorical variables, the chi-square test was performed. If the expected cell count in a table with four cells was less than five, Fisher’s exact test was used instead, and the Monte Carlo test was used in tables with more than four cells.
Continuous normally distributed data were correlated using Pearson’s correlation, whereas non-normally distributed data were correlated using Spearman’s rho. Between qualitative groups, non-normally distributed variables were compared using the Mann–Whitney U-test, whereas regularly distributed variables were compared using the independent sample t-test. To predict independent factors for 25 (OH) vitamin D, a binary logistic regression analysis was performed. The forward Wald approach was used to enter significant predictors from the univariate analysis into the regression model. The adjusted odds ratios (AOR) with 95% confidence intervals (CIs) were calculated.
Results
The study included 2153 participants with a mean age of 43.5 ± 15.9 years. The majority of the patients were female (64%), Saudi (92.8%), and had 25 (OH) vitamin D levels for screening purposes (96.8%). Most of the patients (61%) were referred from internal medicine clinics. Hypertension and diabetes were found in 17.2% and 16.3% of the patients, respectively. None of the studied individuals was maintained on vitamin D supplements for at least one year.
Vitamin D deficiency, defined as a 25 (OH) vitamin D level<20 ng/mL, was present in 41.8% of the patients. Vitamin D deficiency is more common among younger patients, males, non-diabetics, non-hypertensive patients, and those without thyroid disorders. There was no difference in 25 (OH) vitamin D levels according to nationality, referral clinic, or the reason for testing. Moreover, 25 (OH) vitamin D levels did not differ according to the stage of kidney dysfunction and did not correlate with eGFR as a continuous variable. Table 1 shows the baseline characteristics and patient demographics in the study group according to the 25 (OH) vitamin D status. Figure 1 shows the distribution of vitamin D deficiency according to age and sex.
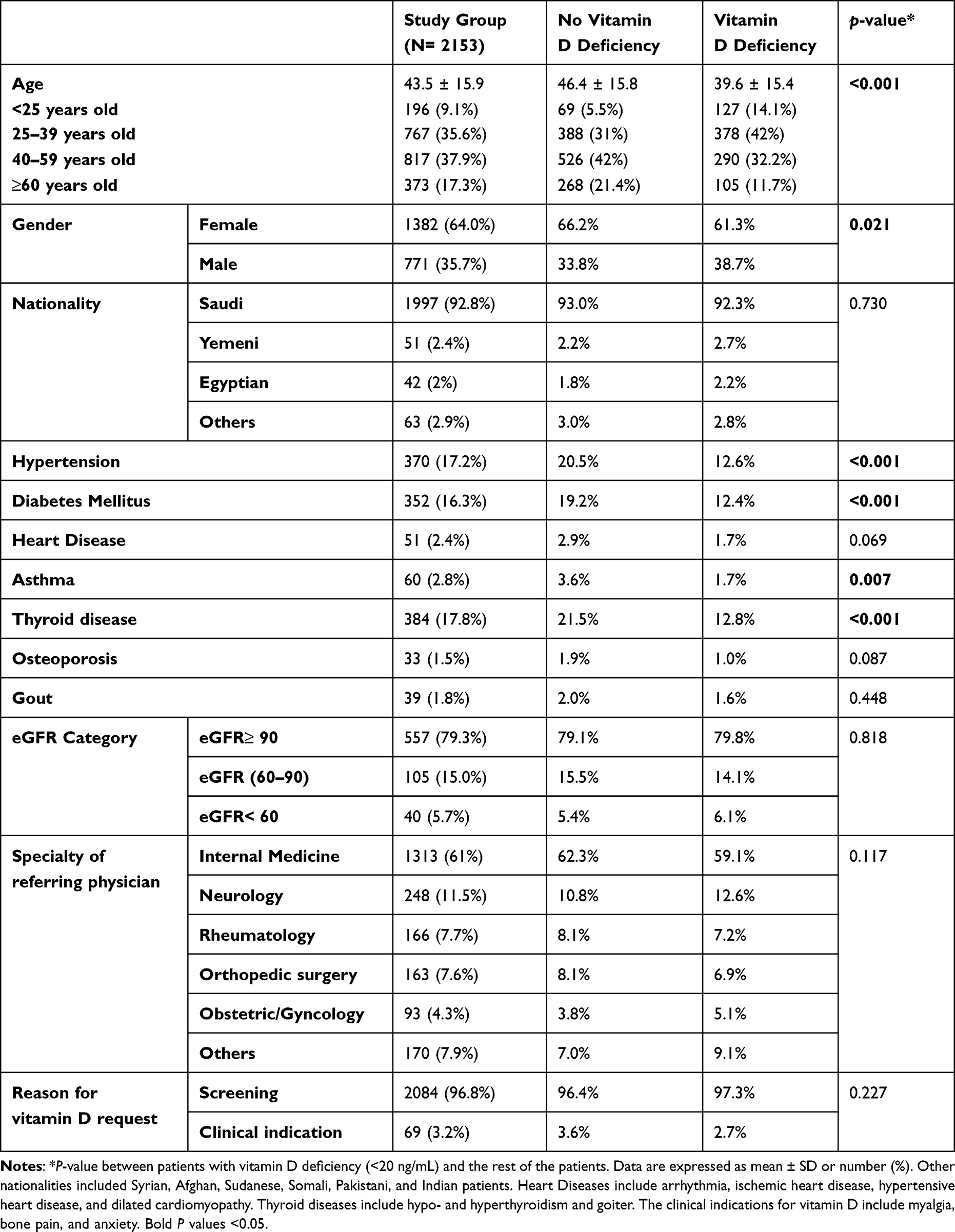 |
Table 1 Baseline Characteristics and Patients Demographics |
 |
Figure 1 Vitamin D deficiency categorized according to age groups and gender. |
Thyroid function, liver function, lipid profile, complete blood count (CBC), and vitamin B levels were within the normal ranges in most patients. Thyroid stimulating hormone (TSH) and free T4 levels did not differ according to 25 (OH) vitamin D level, while free triiodothyronine (T3) levels were higher among patients with vitamin D deficiency (P=0.026) but did not show a significant correlation with 25 (OH) vitamin D as a continuous variable (rho=−0.123, P=0.062). Patients with vitamin D deficiency had lower mean corpuscular volume (MCV), mean corpuscular hemoglobin concentration (MCHC), and Eosinophils (P<0.001, 0.001, and 0.002, respectively). Moreover, they had lower high-density lipoprotein (HDL) and vitamin B levels (P= 0.017 and 0.015, respectively), and liver enzymes showed an inverse relationship with 25 (OH) vitamin D. Direct bilirubin levels, even in the majority of patients within the normal range, were higher among patients with vitamin D deficiency (P=0.045). As a continuous variable, 25 (OH) vitamin D levels correlated positively with serum calcium levels (rho=0.085, P= 0.043). Table 2 shows the laboratory characteristics of the study group according to 25 (OH) vitamin D level. Table 3 shows the significant but week correlation between 25 (OH) vitamin D levels and other variables.
 |
Table 2 Laboratory Results Among Study Group and According to 25 (OH) Vitamin D Status |
 |
Table 3 Significant Correlations Between Vitamin-D Level and Other Parameters |
In the regression analysis, variables with significant differences according to 25 (OH) vitamin D status among patients’ characteristics, younger age, absence of asthma, and thyroid diseases were the predictors of vitamin D deficiency (Table 4). Lower serum calcium levels were a significant predictor of vitamin D deficiency in laboratory data (Table 5). Among the significant predictors of vitamin D deficiency, younger age was the most significant (p<0.001) (Table 6).
 |
Table 4 Binary Logistic Regression for Predictors of Vitamin D Deficiency Among Patients’ Characteristic |
 |
Table 5 Binary Logistic Regression for Predictors of Vitamin D Deficiency Among Patients’ Laboratory Data |
 |
Table 6 Binary Logistic Regression for Significant Predictors of Vitamin D Deficiency |
Discussion
Vitamin D plays a significant role in malignancies and in the cardiovascular, immunological, and endocrine systems, in addition to regulating calcium and phosphorus metabolism, and preserving bone and mineral homeostasis.11,12 Vitamin D deficiency is associated with various immunological,13 cardiovascular,14 and hematological diseases.15 The prevalence of vitamin D deficiency in KSA varies in different studies from 17% to 87% and differs according to age and sex.16 Thus, the aim of the current study was to evaluate the prevalence of vitamin D deficiency among both sexes and different age groups in Taif City, KSA, and its relationship with other clinical and laboratory findings.
In the current study, the mean 25 (OH) vitamin D was 43.5 ng/mL, and 41.8% of the study population had a vitamin D deficiency. Vitamin D deficiency was significantly higher in males than females and in younger individuals than in older individuals. Vitamin D deficiency was significantly higher in people who did not have comorbidities such as hypertension, diabetes mellitus, asthma, and thyroid diseases. Calcium levels were positively correlated with 25 (OH) vitamin D levels.
The high prevalence of vitamin D deficiency can be attributed to several factors. These causes include changes in lifestyle with daytime sleep and nighttime activities, sedentary work environment, shared culture of Islamic type of dressing where most Muslims are covered, high temperatures preventing people from sun exposure, and low consumption of vitamin D-rich foods. In addition, the patients do not take any vitamin D supplements. The prevalence of vitamin D deficiency in the current study is comparable to the results reported by Alghamdi et al, who studied 360 Saudi patients admitted to the cardiology department17 and Kaddam et al conducted a school-based study in three different regions in KSA (4035 students and 2104 employees) and found that 44% of employees had vitamin D deficiency.8 However, this prevalence is much higher than that reported by Naeem et al, who reported a prevalence of 28.3% among 180 healthy individuals in KSA.18 However, some studies have reported higher prevalence. Among the 1475 patients attending orthopedic clinics in the KSA, 53.1% had a vitamin D deficiency.9 In addition, the prevalence of vitamin D deficiency among Saudi Arabian citizens is 74.57%.19 A meta-analysis conducted in 2018 on the prevalence of vitamin D deficiency in the KSA revealed that it was 81.0%, with a confidence interval of 95% 68–90 among different populations.16 These differences between Saudi studies might be due to various patient characteristics, including age groups and the presence of comorbidities, in addition to different areas studied in KSA with different lifestyles and weather conditions. People living in the Taif region, which is located at high altitudes, are more vulnerable to vitamin D deficiency. The intensity of the ultraviolet B radiation required to convert 7-dehydrocholesterol in the skin to cholecalciferol depends on latitude, season, and altitude.20 When determining the need for national public health policies and practices for vitamin D supplementation or food fortification, the effect of altitude must be considered along with latitudinal global position, typical cloud cover or pollution, concealing traditional and protective clothing, race or ethnicity, dietary practices, and other confounding factors of urban and rural dwelling.21
The concealed clothing nature of females and their use of sunblock cream in addition to the higher chance of sun exposure in males due to working outdoors result in decreased exposure of females to sunlight. This could lead to the expectation that vitamin D deficiency would be more common in females than males. Several studies confirm this hypothesis.17,22–27 However, other studies have revealed that males have a higher prevalence of vitamin D deficiency than females.28–31 In the present study, vitamin D deficiency was more common in males than in women, across all age groups. This can be explained by the presence of other associated risk factors that might be common in a particular sex, such as smoking. Smoking is associated with vitamin D deficiency.30,32,33 The clothing style, working status, and smoking habits of the studied individuals were not collected; therefore, this issue cannot be clarified.
In the current study, individuals with vitamin D deficiency were younger than those without. This result is consistent with those reported by Alsuwaida et al,27 Alfawaz et al,25 Hendi et al,9 and Al-Faris et al7 However, this result contradicts those of other studies.30,34 Young individuals in KSA usually have a relatively low dietary intake of vitamin D.35 This is because of the infrequent consumption of healthy foods that contain adequate amounts of vitamin D (eg, dairy products) and frequent consumption of low-vitamin D foods, such as energy-dense foods (eg, fast food and soft drinks). In addition, older people adhere to customs and traditions that keep them exposed to sunlight, such as walking outside and not completely dependent on transportation.
As vitamin D plays a role in the modulation of the immune system, in addition to the presence of vitamin D receptors in immune systems such as B-cells, T-cells, and antigen-presenting cells, vitamin D deficiency might be implicated in the presence of autoimmune thyroid diseases, as shown in studies.36–39 However, in the current study, vitamin D deficiency was higher in the patients without thyroid disease. The type of thyroid disease in the studied individuals was not available, which could explain the absence of a relationship between the presence of thyroid disease and vitamin D deficiency in addition to the possible history of vitamin D supplementation in patients with thyroid diseases.
Vitamin D may play a role in the pathogenesis of asthma by influencing lung development, controlling immunological responses, and remodeling airway smooth muscle.40 Many studies have found an association between vitamin D deficiency and the occurrence of asthma,41–44 however in the current study, patients without asthma experienced more vitamin D deficiency than those with asthma. This can also be explained by the probability that patients with asthma will be taking vitamin D supplements. The higher prevalence of vitamin D deficiency in patients without comorbidities might be due to the continuous check-ups and routine investigations of patients with comorbidities who visit clinics regularly in contrast to patients without comorbidities.
In agreement with the present study, Alfawaz et al,25 and Hendi et al,9 blood levels of 25 (OH) vitamin D were positively correlated with serum calcium levels. This result is consistent with normal physiological processes in which vitamin D is directly involved in calcium homeostasis.5
The current study was performed in a large number of patients, and the associations between vitamin D deficiency and multiple clinical and laboratory parameters were studied. However, this study has some limitations. These limitations include the lack of a questionnaire asking about dietary calcium and phosphorus, socioeconomic status, sun exposure, and clothing styles. In addition, the study included only patients from hospitals; therefore, large population-based studies are required. Moreover, the retrospective design of the study with a single measurement of 25 (OH) vitamin D levels and lack of body mass index data of the patients are among the limitations of this study.
Conclusion
Vitamin D deficiency is common among the Saudi population despite sunny weather in KSA. It is more prevalent among males, younger individuals, and those without comorbidities such as thyroid diseases and asthma. There was a positive association between the blood levels of 25 (OH) vitamin D and serum calcium. This prompts an intensification of efforts towards changing dietary habits and lifestyles to reduce vitamin D deficiency to prevent the occurrence of vitamin D-related diseases.
Ethical Consideration
The study was approved by IRB committee of Research and Studies Department, Directorate of Health Affairs, Taif (Registration number HP-02-T-067 and approval number 791).
Informed Consent
The current study was retrospective and depended on collection of data of patients from the electronic system by using their hospital ID numbers without identifying their personal data. Thus, the consent of patients was waived.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Palacios C, Gonzalez L. Is vitamin D deficiency a major global public health problem? J Steroid Biochem Mol Biol. 2014;144:138–145. doi:10.1016/j.jsbmb.2013.11.003
2. Autier P, Boniol M, Pizot C, Mullie P. Vitamin D status and ill health: a systematic review. Lancet Diabetes Endocrinol. 2014;2:76–89. doi:10.1016/S2213-8587(13)70165-7
3. Chang S-W, Lee H-C. Vitamin D and health-The missing vitamin in humans. Pediatr Neonatol. 2019;60:237–244. doi:10.1016/j.pedneo.2019.04.007
4. Elsammak M, Al-Wossaibi A, Al-Howeish A, Alsaeed J. High prevalence of vitamin D deficiency in the sunny Eastern region of Saudi Arabia: a hospital-based study. EMHJ. 1995;1995:17.
5. Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357:266–281. doi:10.1056/NEJMra070553
6. Tsiaras W, Weinstock MA. Factors influencing vitamin D status. Acta Derm Venereol. 2011;91:115–124. doi:10.2340/00015555-0980
7. AlFaris NA, AlKehayez NM, AlMushawah FI, AlNaeem AN, AlAmri ND, AlMudawah ES. Vitamin D deficiency and associated risk factors in women from Riyadh, Saudi Arabia. Sci Rep. 2019;9:1–8. doi:10.1038/s41598-019-56830-z
8. Kaddam IM, Al-Shaikh AM, Abaalkhail BA, et al. Prevalence of vitamin D deficiency and its associated factors in three regions of Saudi Arabia: a cross-sectional study. Saudi Med J. 2017;38:381. doi:10.15537/smj.2017.4.18753
9. Hendi OM, Abdulaziz AA, Alzahrani AA, Mohammed AA, Algethami AM, Alzahrani KM. Prevalence of vitamin D deficiency among patients attending orthopedic clinic in Taif, Saudi Arabia: a single center study. Kuwait Med J. 2021;53:312–316.
10. Hawsawi R, Al Sarhan B, Samargandi S, Hashim AA. Prevalence of Vitamin-D and calcium deficiencies in female university students: an exploratory study in Taif, Kingdom of Saudi Arabia; 2017.
11. Kechichian E, Ezzedine K. Vitamin D and the skin: an update for dermatologists. Am J Clin Dermatol. 2018;19:223–235. doi:10.1007/s40257-017-0323-8
12. Zittermann A, Pilz S. Vitamin D and cardiovascular disease: an update. Anticancer Res. 2019;39:4627–4635. doi:10.21873/anticanres.13643
13. Charoenngam N, Holick MF. Immunologic effects of vitamin D on human health and disease. Nutrients. 2020;12:2097. doi:10.3390/nu12072097
14. Bouillon R. Vitamin D and cardiovascular disorders. Osteoporos Int. 2019;30:2167–2181. doi:10.1007/s00198-019-05098-0
15. Kulling PM, Olson KC, Olson TL, Feith DJ, Loughran TP Jr. Vitamin D in hematological disorders and malignancies. Eur J Haematol. 2017;98:187–197. doi:10.1111/ejh.12818
16. Al-Daghri NM. Vitamin D in Saudi Arabia: prevalence, distribution and disease associations. J Steroid Biochem Mol Biol. 2018;175:102–107. doi:10.1016/j.jsbmb.2016.12.017
17. Alghamdi SJH, Omer EO, Zafar M, Herzallah HKI. Association of Vitamin D deficiency with cardiovascular disease among Saudi patients in Saudi Arabia. Int J Prev Med. 2020;11:11. doi:10.4103/ijpvm.IJPVM_320_18
18. Naeem Z, AlMohaimeed A, Sharaf FK, Ismail H, Shaukat F, Inam SB. Vitamin D status among population of Qassim region, Saudi Arabia. Int J Health Sci. 2011;5:116.
19. Altowijri A, Alloubani A, Abdulhafiz I, Saleh A. Impact of nutritional and environmental factors on vitamin D deficiency. Asian Pac J Cancer Prev. 2018;19:2569. doi:10.22034/APJCP.2018.19.9.2569
20. Wacker M, Holick MF. Sunlight and vitamin D: a global perspective for health. Dermato-Endocrinology. 2013;5:51–108. doi:10.4161/derm.24494
21. Calvo MS. High-altitude living and vitamin D: factors associated with viral risk? Am J Clin Nutr. 2020;112:915–916. doi:10.1093/ajcn/nqaa250
22. Al-Daghri NM, Hussain SD, Ansari MG, et al. Decreasing prevalence of vitamin D deficiency in the central region of Saudi Arabia (2008–2017). J Steroid Biochem Mol Biol. 2021;212:105920. doi:10.1016/j.jsbmb.2021.105920
23. Takiishi T, Gysemans C, Bouillon R, Mathieu C. Vitamin D and diabetes. Rheum Dis Clin. 2012;38:179–206. doi:10.1016/j.rdc.2012.03.015
24. Al-Zoughool M, AlShehri A, Alqarni A, Alarfaj A, Tamimi W. Vitamin D status of patients visiting health care centers in the coastal and Inland Cities of Saudi Arabia. J Public Health Res Dev Count. 2015;1:14–21.
25. Alfawaz H, Tamim H, Alharbi S, Aljaser S, Tamimi W. Vitamin D status among patients visiting a tertiary care center in Riyadh, Saudi Arabia: a retrospective review of 3475 cases. BMC Public Health. 2014;14:1–6. doi:10.1186/1471-2458-14-159
26. Tuffaha M, El Bcheraoui C, Daoud F, et al. Deficiencies under plenty of sun: vitamin D status among adults in the Kingdom of Saudi Arabia, 2013. N Am J Med Sci. 2015;7:467. doi:10.4103/1947-2714.168675
27. Alsuwadia AO, Farag YM, Al Sayyari AA, et al. Prevalence of vitamin D deficiency in Saudi adults. Saudi Med J. 2013;34:814–818.
28. Guardia G, Parikh N, Eskridge T, Phillips E, Divine G, Rao DS. Prevalence of vitamin D depletion among subjects seeking advice on osteoporosis: a five-year cross-sectional study with public health implications. Osteoporos Int. 2008;19:13–19. doi:10.1007/s00198-007-0456-3
29. Bogunovic L, Kim AD, Beamer BS, Nguyen J, Lane JM. Hypovitaminosis D in patients scheduled to undergo orthopaedic surgery: a single-center analysis. J Bone Joint Surg Am. 2010;92:2300. doi:10.2106/JBJS.I.01231
30. Gorter E, Krijnen P, Schipper I. Vitamin D deficiency in adult fracture patients: prevalence and risk factors. Eur J Trauma Emerg Surg. 2016;42:369–378. doi:10.1007/s00068-015-0550-8
31. Minter M, Augustin H, van Odijk J, Vanfleteren LE. Gender differences in vitamin D status and determinants of vitamin D insufficiency in patients with chronic obstructive pulmonary disease. Nutrients. 2023;15:426. doi:10.3390/nu15020426
32. Larose TL, Chen Y, Camargo CA, Langhammer A, Romundstad P, Mai X-M. Factors associated with vitamin D deficiency in a Norwegian population: the HUNT study. J Epidemiol Community Health. 2014;68:165–170. doi:10.1136/jech-2013-202587
33. Smith JT, Halim K, Palms DA, Okike K, Bluman EM, Chiodo CP. Prevalence of vitamin D deficiency in patients with foot and ankle injuries. Foot Ankle Int. 2014;35:8–13. doi:10.1177/1071100713509240
34. Hood MA, Murtha YM, Della Rocca GJ, Stannard JP, Volgas DA, Crist BD. Prevalence of low vitamin D levels in patients with orthopedic trauma. Am J Orthop. 2016;45:E522–E526.
35. Zareef TA, Jackson RT, Alkahtani AA. Vitamin D intake among premenopausal women living in Jeddah: food sources and relationship to demographic factors and bone health. J Nutr Metab. 2018;2018. doi:10.1155/2018/8570986
36. Chao G, Zhu Y, Fang L. Correlation between Hashimoto’s thyroiditis–related thyroid hormone levels and 25-hydroxyvitamin D. Front Endocrinol. 2020;11:4. doi:10.3389/fendo.2020.00004
37. Sulejmanovic M, Begić A, Mujaric-Bousbia F, Salkic S, Ramas A, Ramas A. The relationship between thyroid antibodies and vitamin D level in primary hypothyroidism. Arch Med. 2020;74:359. doi:10.5455/medarh.2020.74.359-362
38. Planck T, Shahida B, Malm J, Manjer J. Vitamin D in Graves disease: levels, correlation with laboratory and clinical parameters, and genetics. Eur Thyroid J. 2018;7:27–33. doi:10.1159/000484521
39. Ma J, Wu D, Li C, et al. Lower serum 25-hydroxyvitamin D level is associated with 3 types of autoimmune thyroid diseases. Medicine. 2015;13:94. doi:10.1186/s12916-015-0329-0
40. Mailhot G, White JH. Vitamin D and immunity in infants and children. Nutrients. 2020;12:1233. doi:10.3390/nu12051233
41. Ogeyingbo OD, Ahmed R, Gyawali M, et al. The relationship between vitamin D and asthma exacerbation. Cureus. 2021;2021:13.
42. Wang Q, Ying Q, Zhu W, Chen J. Vitamin D and asthma occurrence in children: a systematic review and meta-analysis. J Pediatr Nurs. 2022;62:e60–e68. doi:10.1016/j.pedn.2021.07.005
43. Hall SC, Fischer KD, Agrawal DK. The impact of vitamin D on asthmatic human airway smooth muscle. Expert Rev Respir Med. 2016;10:127–135. doi:10.1586/17476348.2016.1128326
44. Bener A, Ehlayel MS, Tulic MK, Hamid Q. Vitamin D deficiency as a strong predictor of asthma in children. Int Arch Allergy Immunol. 2012;157:168–175. doi:10.1159/000323941
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.