Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Vitamin B6, B9, and B12 Intakes and Cognitive Performance in Elders: National Health and Nutrition Examination Survey, 2011–2014
Authors Xu H ![]() , Wang S
, Wang S ![]() , Gao F, Li C
, Gao F, Li C
Received 3 September 2021
Accepted for publication 15 February 2022
Published 9 March 2022 Volume 2022:18 Pages 537—553
DOI https://doi.org/10.2147/NDT.S337617
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Hui Xu,1 Shanshan Wang,1 Feng Gao,2 Caihong Li3
1Department of Fundamental Nursing, The Nursing and Health College of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China; 2Department of Obstetrics and Gynecology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China; 3Department of Development Planning, Aviation General Hospital, Beijing, People’s Republic of China
Correspondence: Caihong Li, Department of Development Planning, Aviation General Hospital, No. 4, Beiyuan Road, Chaoyang District, Beijing, 100012, People’s Republic of China, Tel +86 10-59520205 ; +86 13811048937, Email [email protected]
Purpose: This research intended to investigate vitamin B6, B9, and B12 consumption in relation to the risk of low cognitive performance (LCP) among elderly adults.
Patients and Methods: We analyzed data of 2421 participants retrieved from the National Health and Nutrition Examination Survey (NHANES) 2011– 2014 database in this cross-sectional study. Cognitive performance was evaluated by the Consortium to Establish a Registry for Alzheimer’s disease (CERAD) word learning and recall modules, the animal fluency test (AF), and the digit symbol substitution test (DSST). Participants who scored the lowest 25th percentile were categorized in the LCP group. The Dietary Interview-Total Nutrient Intakes dataset was used to determine the dietary intake of B vitamins in the participants. The low intake group and adequate intake group were differentiated based on the recommended dietary allowance. Subgroup analyses were conducted to assess the relations between 3 B vitamins and cognitive performance among different sex, race, and age groups.
Results: Compared with low vitamin B6 intake (< 1.7 mg/day), adequate vitamin B6 intake (≥ 1.7 mg/day) corresponded to a 31.7% decrease in LCP odds in the DSST tests. Participants who consumed adequate B9 (≥ 400 mcg/day) were associated with 31.2%, 33.8%, and 46.5% declines in the risk of LCP in the CERAD, AF, and DSST tests in contrast to those having low B9 intake (< 400 mcg/day). Adequate vitamin B12 intake (≥ 2.4 mcg/day) correlated with a lower LCP occurrence in the CERAD, AF, and DSST tests, with 30.5%, 21.5%, and 33.3% reductions, respectively. Further, the relations between 3 B vitamins and cognitive performance varied across different sex, race, and age groups of people.
Conclusion: Adequate dietary vitamin B9 and B12 intakes are significantly associated with a better cognitive performance in immediate and delayed memory recall, categorical verbal fluency, processing speed, sustained attention, and working memory among elders assessed in the CERAD, AF, and DSST tests.
Keywords: vitamin B6, pyridoxine, B9, folate, B12, cobalamin, cognition, National Health and Nutrition Examination, NHANES, dietary intake
Introduction
The global population of elderly people aged 60 or above is expected to double from 12% to 22%, reaching 2 billion by 2050.1 As the size of the elder population increases substantially, age-related health conditions have raised considerable concerns. Aging is commonly accompanied by cognitive function declines, such as processing speed, attention, certain memories, language, visuospatial abilities, and executive functioning.2 Cognitive changes or deficits that affect one’s ability to perform daily activities are considered major neurocognitive disorders. The definition and diagnostic criteria of several cognitive disorders are provided by the Diagnostic and Statistical Manual of Mental Disorders (DSM-5).3 According to the World Health Organization, the economic burden of dementia, a cognitive disorder that impacts daily functioning, costs approximately US$ 818 billion in 2015.4
Although current pharmaceutical treatment is limited, studies have shown promising effects of lifestyle change and dietary intervention on slowing the progression of cognitive impairments.5–7 Vitamin B complex plays an essential role in maintaining proper physiological functions of cellular energy metabolism, methylation, DNA synthesis and repair, immune system, and steroid hormone activity.8 Because of the crucial function vitamin B complex performs in homocysteine metabolism, suboptimal vitamin B levels have been linked to cognitive decline.9 Homocysteine, a sulfur-containing amino acid, has established a putative relationship with cognitive decline.10 The association between elevated plasma homocysteine levels and cognitive impairments may be attributed to mechanisms involving the methylation pathways. It has been proposed that homocysteine is associated with brain atrophy, oxidative stress, DNA damage, increased apoptosis, excitotoxicity, and neurodegeneration.9
Vitamin B6 (Pyridoxine), vitamin B9 (Folate), and vitamin B12 (Cobalamin) are the three core B vitamins that facilitate homocysteine metabolism. In the process of resynthesizing methionine from homocysteine, vitamin B9, in the form of tetrahydrofolate, and B12 mainly participate in the remethylation of homocysteine to methionine.11 To be further metabolized in the human body, homocysteine enters the trans-sulfuration pathway to form cysteine, the process of which requires the presence of pyridoxal phosphate, the coenzyme form of vitamin B6.11,12
The aging-related decrease in satiety predisposes the elderly to vitamin B deficiencies or suboptimal vitamin B levels.11 Thus, the neuro-protective properties of vitamin B may assist the prevention and management of poor cognitive performance among elders to a considerable extent.
Since vitamin B complex is proposed to be a protective factor of cognitive decline,9,10,13–15 previous studies focused on three critical B vitamins, vitamin B6, B12, and B9,16,17 when examining the association between vitamin B and cognitive functions in the elderly. However, there are limited publications on specific cognitive domains affected by vitamin B deficiencies, so this study intended to investigate whether dietary vitamin B6, B9, and B12 intakes were in relation to cognitive performance among the elderly, through the Consortium to Establish a Registry for Alzheimer’s disease (CERAD) word learning and recall modules, the Animal Fluency test (AF), and the Digit Symbol Substitution Test (DSST) which assessed different cognitive domains. We further performed subgroup analyses to demonstrate if and how the relations between 3 B vitamins and cognitive performance varied across different sex, race, and age groups of elderly people.
Methods
Study Participants
The National Health and Examination Survey (NHANES) collected nation-wide representative data, aiming to assess the health and nutritional status of adults and children in the United States. There were two main parts of the NHANES program, an in-home interview and a physical examination in a mobile examination center (MEC).18 All protocols were approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board. Only the NHANES 2011–2012 and 2013–2014 cycles evaluated cognitive functions in both the questionnaire and MEC examination. Thus, we downloaded 2011–2012 and 2013–2014 NHANES public data for analysis in this research. A total of 2937 participants were aged >60 years and completed cognitive assessment. Individuals who had missing data in vitamin B6, B9, and B12 intakes, body mass index (BMI), poverty income ratio (PIR), alcohol use, education level, hypertension, and cardiovascular diseases were excluded (n=516). In total, 2421 people were included in this study (Figure 1).
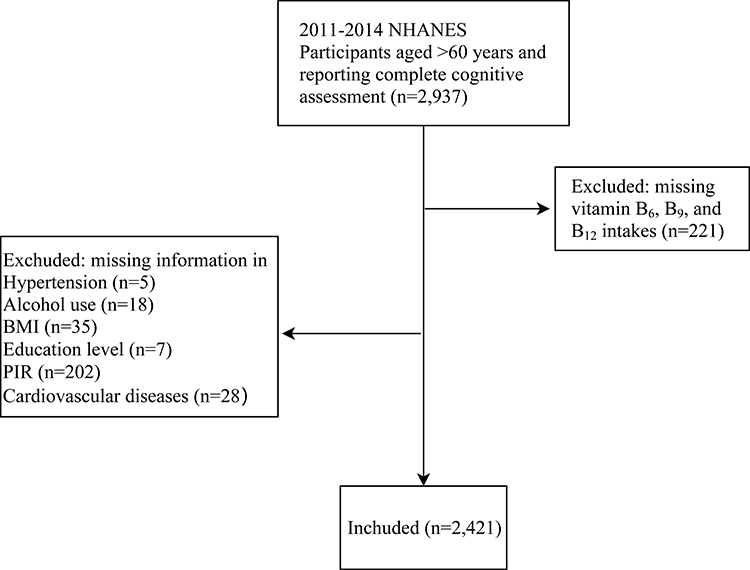 |
Figure 1 Flow chart of selecting eligible participants. |
Cognitive Performance Assessment
During the MEC examination, a series of cognitive function assessments were administered to participants aged 60 years or older, including the CERAD word learning and recall modules, AF, and DSST. All the collected data were available in the cognitive functioning questionnaire (CFQ).
The CERAD consisted of learning trials and delayed recall, which examined immediate and delayed memory recall.19 Participants were visually or auditorily presented with 10 words and instructed to read aloud. Participants recalled as many as possible words immediately after the presentation and after the completion of the AF and DSST. The AF evaluated the categorical verbal fluency by asking the participants to name as many animals as possible in 1 minute.20 The participant gained one point for each animal correctly named. The processing speed, sustained attention, and working memory were evaluated by the DSST.21 The DSST was a paper-delivered test composed of a reference at the top and 133 boxes containing the numbers 1–9, in random order, adjoined in rows on a page with an empty box underneath each number. The reference was 9 numerical numbers paired with unique symbols. Participants were asked to match the corresponding symbols in the 133 boxes using the reference in 2 minutes.
Since there is no standard cut-offs for CERAD, AF and DSST to define low cognitive performance (LCP), we categorized participants who scored the lowest 25th percentile in each of the tests into the LCP group and the remaining participants into the normal cognitive performance (NCP) group. This method was consistent with those applied in multiple previous NHANES cognitive studies.22–26 Respective cut-off values for CERAD, AF and DSST were 5, 13 and 35.
Dietary Intake Assessment
Dietary intake data from the 24-hour dietary recall interview were collected using a validated USDA Automated Multiple-Pass Method during the MEC examination.27 We obtained vitamin B6, B9 and B12 consumption from the Dietary Interview-Total Nutrient Intakes dataset. Vitamin intakes were further categorized into two groups, a group with vitamin intakes equal to or higher than the Recommended Dietary Allowance (RDA) and a group with vitamin intakes lower than the RDA. Vitamin B6 intake was categorized into a group of <1.7 mg/day and a group of ≥1.7 mcg/day. Vitamin B9 intake was classified into a group consuming ≥400 mcg/day and a group consuming <400 mcg/day. Vitamin B12 consumption was divided into ≥2.4 mcg/day and <2.4 mcg/day. In all the analyses, the group with intakes lower than the RDA was the reference group.
Potential Covariates
Alcohol use and social-economic status were associated with cognitive functions, and were therefore considered potential covariates in this study.10 Alcohol consumers were defined using the Alcohol Use Questionnaire (ALQ) question ALQ101: “Had at least 12 alcohol drinks/1 yr?” Participants who answered “Yes” were categorized as alcohol consumers. Social-economic status was evaluated using the PIR available in the Demographic Variables & Sample Weight (DEMO) as INDFMPIR. PIR is the ratio of family income to poverty, which was calculated by dividing family income by the poverty guidelines. Therefore, we classified PIR <1 as the low-income group.
Medical Conditions
Hypertension patients were determined based on the examination data. The participants were defined as having hypertension if their systolic pressure is ≥140 mmHg, and diastolic pressure is ≥90 mmHg. Additionally, people who answered “Yes” to the Blood Pressure & Cholesterol Questionnaire (BPQ) question 020, “{Have you/Has SP} ever been told by a doctor or other health professional that {you/s/he} had hypertension, also called high blood pressure?” were classified as having hypertension. Diabetic patients were identified if their plasma fasting glucose level ≥126 mg/dL or Hemoglobin A1c ≥6.5%. In addition, participants who answered “yes” to Diabetes Questionnaire (DIQ) question 010,
The next questions are about specific medical conditions. {Other than during pregnancy, {have you/has SP}/{Have you/Has SP}} ever been told by a doctor or health professional that {you have/{he/she/SP} has} diabetes or sugar diabetes? Were defined as diabetic.
Cardiovascular diseases, including congestive heart failure, coronary heart disease, angina, heart attack, and stroke, were determined based on the Medical Conditions Questionnaire (MCQ) 160b-f:
Has a doctor or other health professional ever told {you/SP} that {you/s/he} had congestive heart failure/coronary (kor-o-nare-ee) heart disease/angina (an-gi-na) (also called angina pectoris)/a heart attack (also called myocardial infarction (my-o-car-dee-al in-fark-shun))/a stroke?
Statistical Analysis
Continuous variables were presented as means and standard deviations (Mean ± SD), while categorical variables were described as cases and percentages. Baseline characteristics were compared using the independent-t-test and Pearson chi-square test. Univariate and multivariate logistic regression models were applied to analyze the association between vitamin B intakes and cognitive performance. Crude model was a univariate model. Model 1 was a multivariate model adjusted for age and gender. Model 2 was a multivariate model adjusted for age, gender, race, education level, PIR, hypertension, heart failure, heart attack, and stroke for the CERAD test, adjusted for age, gender, race, education level, marital status, PIR, alcohol use, hypertension, and stroke for the AF test, and adjusted for age, gender, race, education level, marital status, PIR, alcohol use, diabetes, hypertension, heart failure, heart attack, and stroke for the DSST test. Odds Ratios (ORs), 95% Confidence Intervals (CIs), and P value were also acquired using the logistic regression models. Further, we have performed subgroup analyses to demonstrate if and how the relations between 3 B vitamins and cognitive performance varied across different sex, race, and age groups of people. Moreover, we included NHANES sample weights in statistical analysis of this study. All statistical tests were two-sided with a significance level set at 0.05. We used SAS 9.4 (SAS Institute, inc. Cary, NC, USA) for all the statistical analyses and R 4.02 for forest plots in this research.
Results
Baseline Characteristics
Of the 2421 participants, 337 were classified into the LCP group based on the CERAD test, 398 into the LCP group according to the AF test, and 563 into the LCP group when assessed by the DSST. Baseline characteristics were compared between the two groups, as shown in Table 1. Means, SDs, and ranges for these cognitive tests are shown in Supplementary Table 1. Across all the three cognitive measures, age, race, education level, PIR, hypertension, stroke, vitamin B9 intake were significantly different between the NCP and LCP groups.
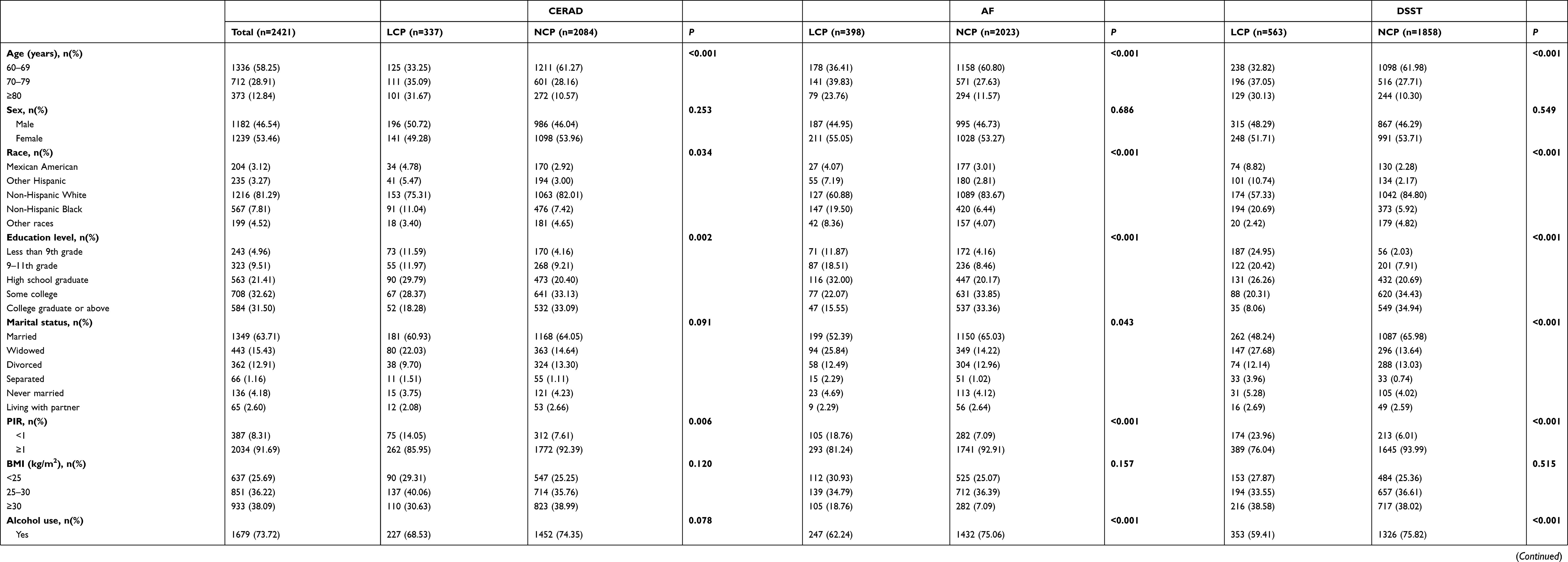 |
Table 1 Characteristics of n=2421 Study Participants, NHANES 2011–2014 |
The LCP group had a higher proportion of participants aged 70–79 years and ≥80 years than the NCP group in all the three cognitive tests. Across all the cognitive measures, the LCP group had a higher percentage of the participants with hypertension than the NCP group. The CERAD test revealed a significantly higher proportion of heart failure in the LCP group (13.39%) than the NCP group (5.82%). Similarly, the percentage of individuals with heart failure was significantly higher in the LCP group (13.37%) than that in the NCP group (4.84%) in the DSST test. The prevalence of stroke was higher in the LCP group than that in the NCP group across all three tests.
In terms of vitamin B intakes, the LCP group showed a higher percentage of people consuming <1.7 mg/day vitamin B6 than the NCP group (59.52% vs 47.56%, P=0.001) when assessed by the DSST test. In all three cognitive assessments, the proportion of participants consuming vitamin B9 <400 mg/day in the LCP group was greater than that in the NCP group. As evaluated by the AF and DSST test, the proportion of low vitamin B12 intake, <2.4 mg/day, was significantly higher in the LCP group than that in the NCP group.
Vitamin B Intake and Cognitive Performance
To further investigate whether vitamin B6, B9, and B12 intakes were associated with cognitive performance, logistic regression models were implemented. In terms of vitamin B intakes, vitamin B6 intake <1.7 mg/day, vitamin B9 intake <400 mcg/day, and vitamin B12 intake <2.4 mcg/day were set as the reference groups in all analyses.
When assessing immediate and delayed memory recall by the CERAD test, after controlling for age, gender, race, education level, PIR, hypertension, heart failure, heart attack, and stroke, vitamin B6 intake was not associated with the risk of LCP (P=0.659). Compared with the reference group, higher vitamin B9 intake (≥400 mcg/day) was associated with a 0.312 decrease in the odds of LCP (OR: 0.688, 95% CI: 0.507–0.934, P=0.018). Similarly, higher vitamin B12 consumption was also associated with a lower risk of LCP (OR: 0.695, 95% CI: 0.522–0.924, P=0.014) (Table 2, Figure 2).
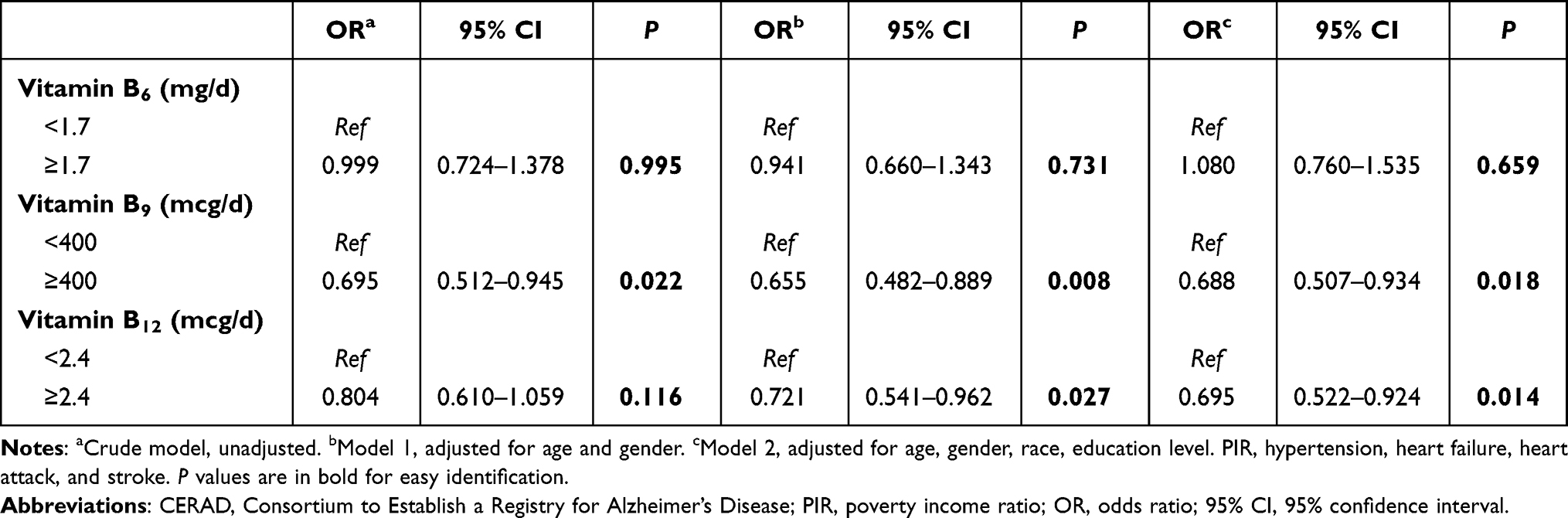 |
Table 2 Logistic Regression Models-CERAD Test |
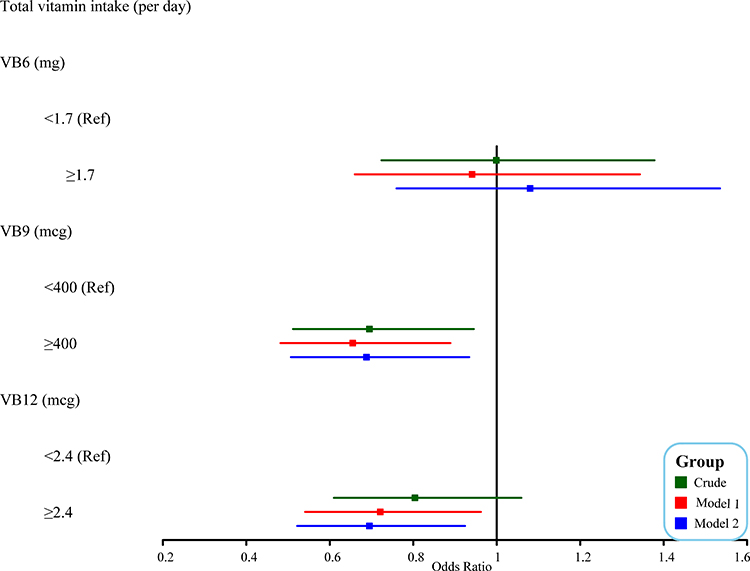 |
Figure 2 Forest plot of the CERAD test. Abbreviations: CERAD, consortium to establish a registry for Alzheimer’s disease; PIR, poverty income ratio; VB6, vitamin B6; VB9, vitamin B9; VB12, vitamin B12. |
The results were similar in the AF tests, with vitamin B6 consumption not being associated with the risk of LCP while vitamin B9 and vitamin B12 intake relating to the odds of LCP. No significant relationship was observed between vitamin B6 consumption and the risk of low categorical verbal fluency (P=0.214). Adequate vitamin B9 intake was linked to a 33.8% lower risk of LCP (OR: 0.662, 95% CI: 0.445–0.986, P=0.043), in contrast to the reference group. Compared with the reference group, the odds of LCP decreased by 21.5% when people consumed ≥2.4 mg vitamin B12 per day (OR: 0.785, 95% CI: 0.626–0.984, P=0.036) (Table 3, Figure 3).
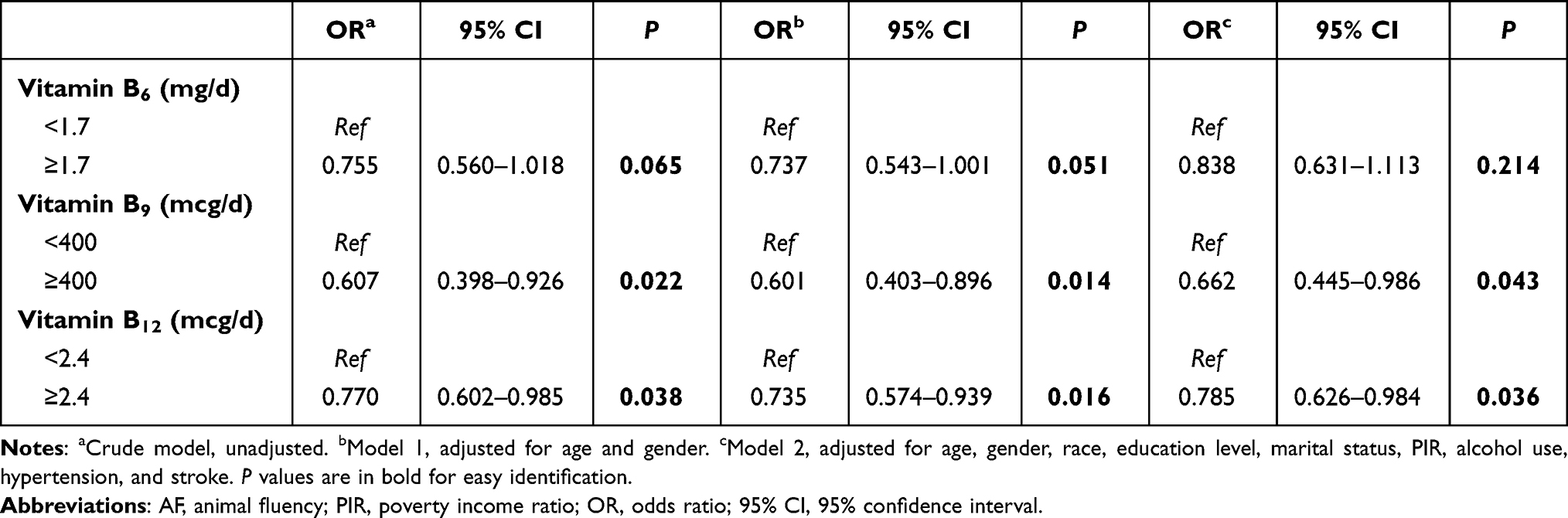 |
Table 3 Logistic Regression Models-AF Test |
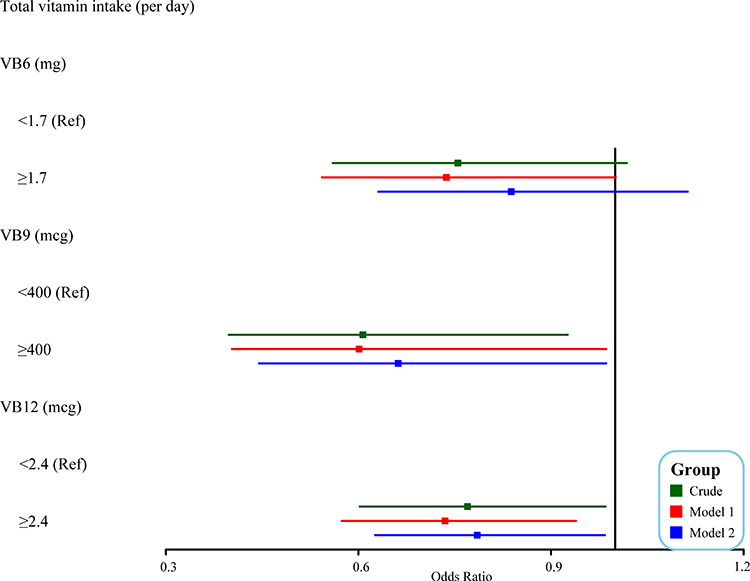 |
Figure 3 Forest plot of the AF test. Abbreviations: AF, animal fluency; PIR, poverty income ratio; VB6, vitamin B6; VB9, vitamin B9; VB12, vitamin B12. |
The relationship between vitamin consumptions and the performance of processing speed, sustained attention, and working memory was evaluated using the DSST test. In model 2, controlling for age, gender, race, education level, marital status, PIR, alcohol use, diabetes, hypertension, heart failure, heart attack, and stroke, adequate vitamin B6 intake (≥1.7 mg/day) was associated with a 31.7% lower risk of LCP (OR: 0.683, 95% CI: 0.505–0.925, P<0.001) compared with low vitamin B6 intake (<1.7 mg/day). Similarly, higher B9 consumption (≥400 mcg/day) was linked to a 0.465 decrease in the odds of LCP (OR: 0.535, 95% CI: 0.363–0.789, P=0.003). Compared with vitamin B12 intake <2.4 mcg/day, vitamin B12 intake ≥2.4 mcg/day indicated a 0.333 decrease in the odds of LCP (OR: 0.667, 95% CI: 0.521–0.855, P=0.002) (Table 4, Figure 4).
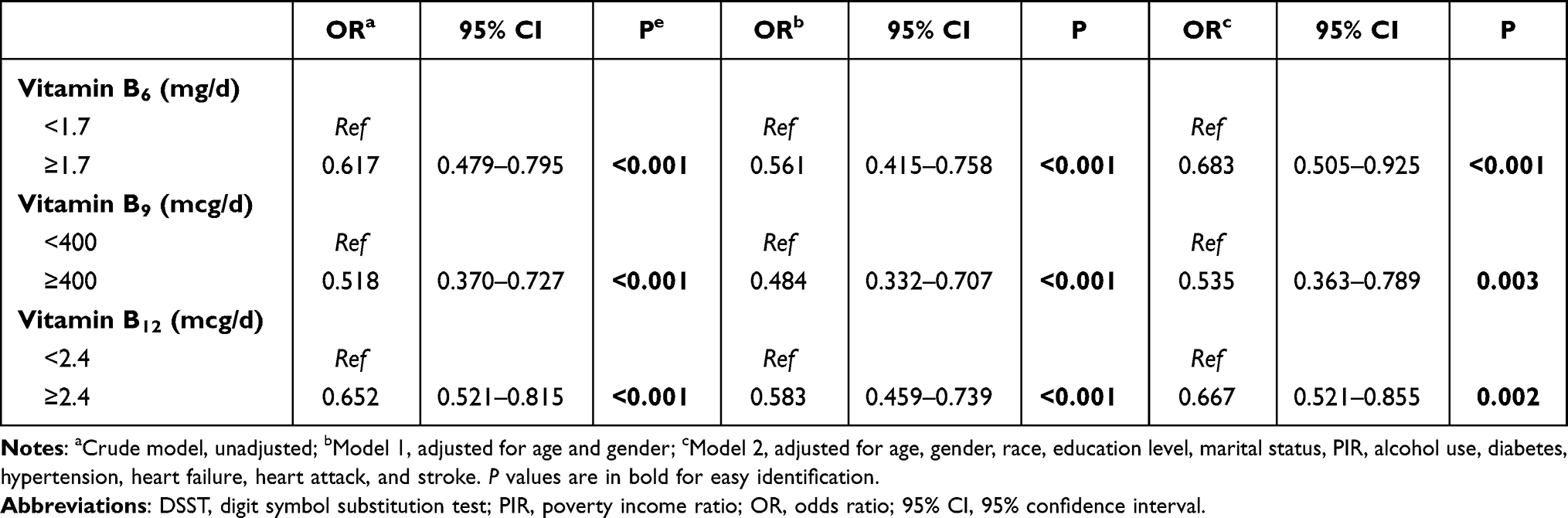 |
Table 4 Logistic Regression Models-DSST Test |
 |
Figure 4 Forest plot of the DSST test. Abbreviations: DSST, digit symbol substitution test; PIR, poverty income ratio; VB6, vitamin B6; VB9, vitamin B9; VB12, vitamin B12. |
Vitamin B Intake and Cognitive Performance Across Different Sex, Race, and Age Groups
Subgroup analyses were performed to demonstrate if and how the relations between 3 B vitamins and cognitive performance varied across different sex, race, and age groups of the elderly. After covariate adjustment, under the CERAD test, adequate intake of vitamin B6 was associated with lower odds of LCP than low vitamin B6 intake among older adults aged 60–69 years (OR: 0.545, 95% CI: 0.364–0.816, P=0.004) and of non-Hispanic black race (OR: 0.652, 95% CI: 0.431–0.988, P=0.044), while it was not significantly related to the risk of LCP for people of other ages, both sexes, and other races (all P> 0.05). The inverse association between vitamin B9 intake and odds of LCP was significant for people aged 60–69 years (OR: 0.362, 95% CI: 0.219–0.599, P<0.001), older men (OR: 0.568, 95% CI: 0.349–0.924, P=0.024) and women (OR: 0.532, 95% CI: 0.352–0.804, P=0.004), and the elderly of non-Hispanic white (OR: 0.502, 95% CI: 0.345–0.730, P<0.001). Older people of 60–69 (OR: 0.347, 95% CI: 0.214–0.536, P<0.001), 70–79 (OR: 0.603, 95% CI: 0.370–0.981, P=0.042) and ≥ 80 (OR: 0.658, 95% CI: 0.449–0.965, P=0.033) years, of both male (OR: 0.501, 95% CI: 0.369–0.681, P<0.001) and female (OR: 0.547, 95% CI: 0.387–0.773, P=0.001) genders, of non-Hispanic white (OR: 0.501, 95% CI: 0.368–0.681, P<0.001) and non-Hispanic black (OR: 0.578, 95% CI: 0.378–0.883, P=0.013) races with adequate vitamin B12 intake had lower risks of LCP, as compared with those with low vitamin B12 intake (Table 5, Figure 5).
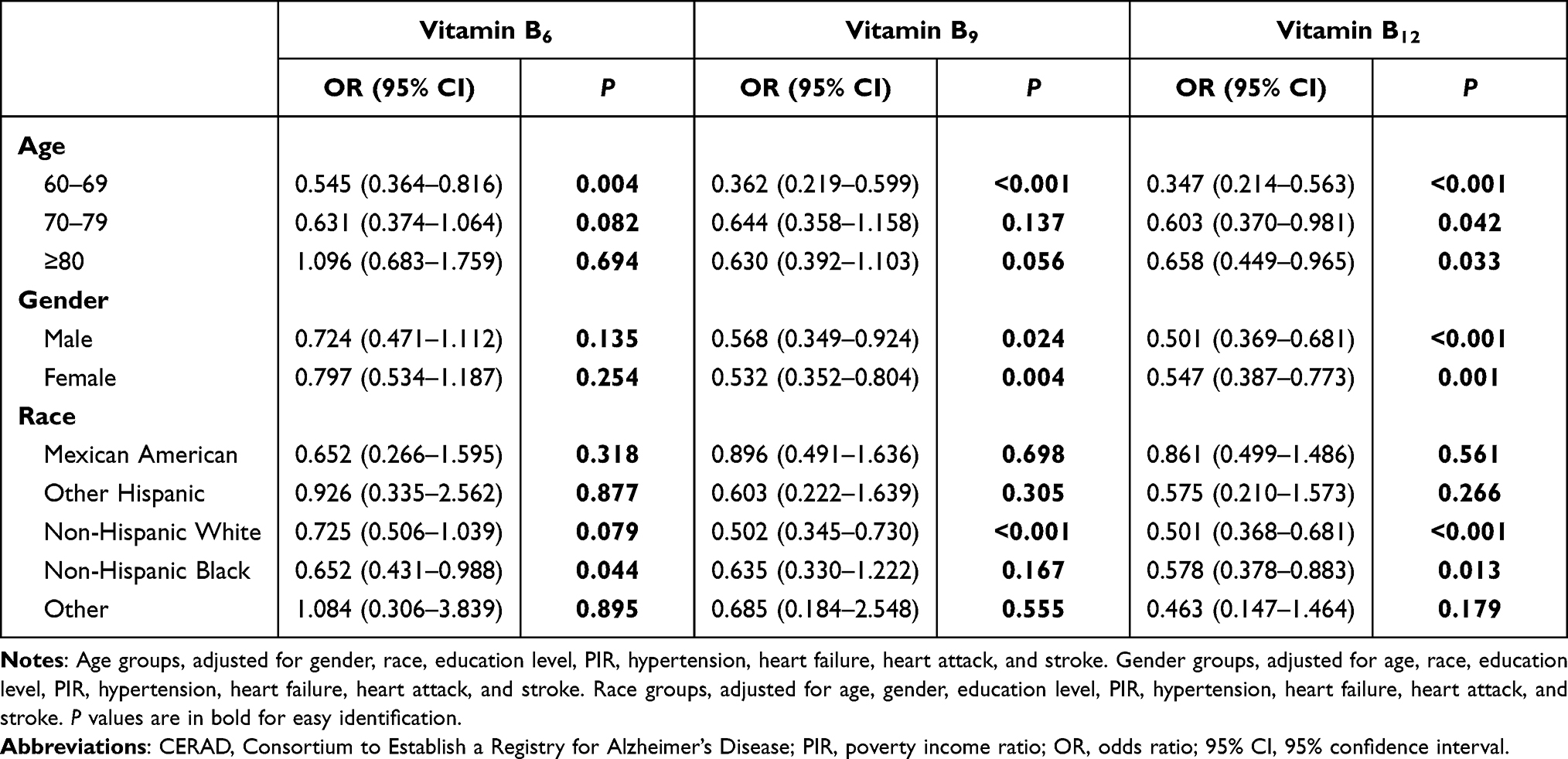 |
Table 5 Subgroup Analysis-CERAD Test |
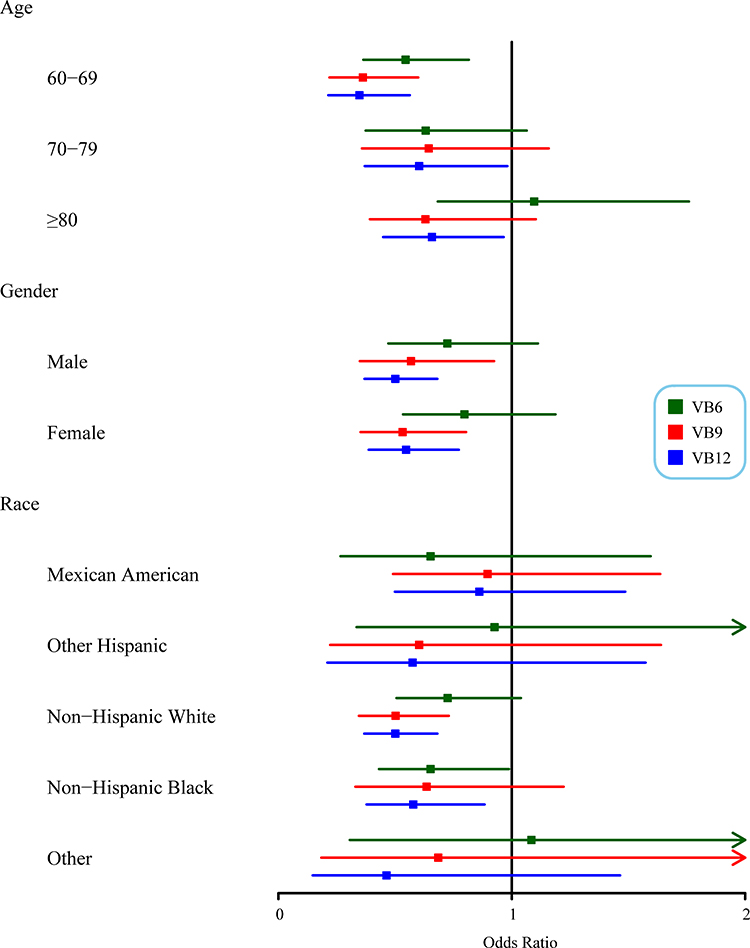 |
Figure 5 Forest plot of the CERAD test for subgroup analysis. Abbreviations: CERAD, consortium to establish a registry for Alzheimer’s disease; PIR, poverty income ratio; VB6, vitamin B6; VB9, vitamin B9; VB12, vitamin B12. |
In the AF test, adequate intake of vitamin B6 was associated with lower odds of LCP than low vitamin B6 intake among older males (OR: 0.686, 95% CI: 0.488–0.964, P=0.031), and older adults of non-Hispanic white race (OR: 0.515, 95% CI: 0.347–0.765, P=0.002). People of 60–69 (OR: 0.364, 95% CI: 0.218–0.607, P<0.001) and ≥ 80 (OR: 0.303, 95% CI: 0.124–0.737, P=0.010) years, older men (OR: 0.579, 95% CI: 0.376–0.891, P=0.015), and the elderly of non-Hispanic white race (OR: 0.409, 95% CI: 0.242–0.691, P=0.002) having adequate vitamin B9 consumption had decreased odds of LCP, in contrast to those consuming low vitamin B9. Vitamin B12 intake was negatively correlated with the risk of LCP for individuals of 60–69 years (OR: 0.449, 95% CI: 0.308–0.654, P<0.001), elderly males (OR: 0.543, 95% CI: 0.410–0.720, P<0.001), the elderly of non-Hispanic white race (OR: 0.533, 95% CI: 0.371–0.766, P=0.001) (Table 6, Figure 6).
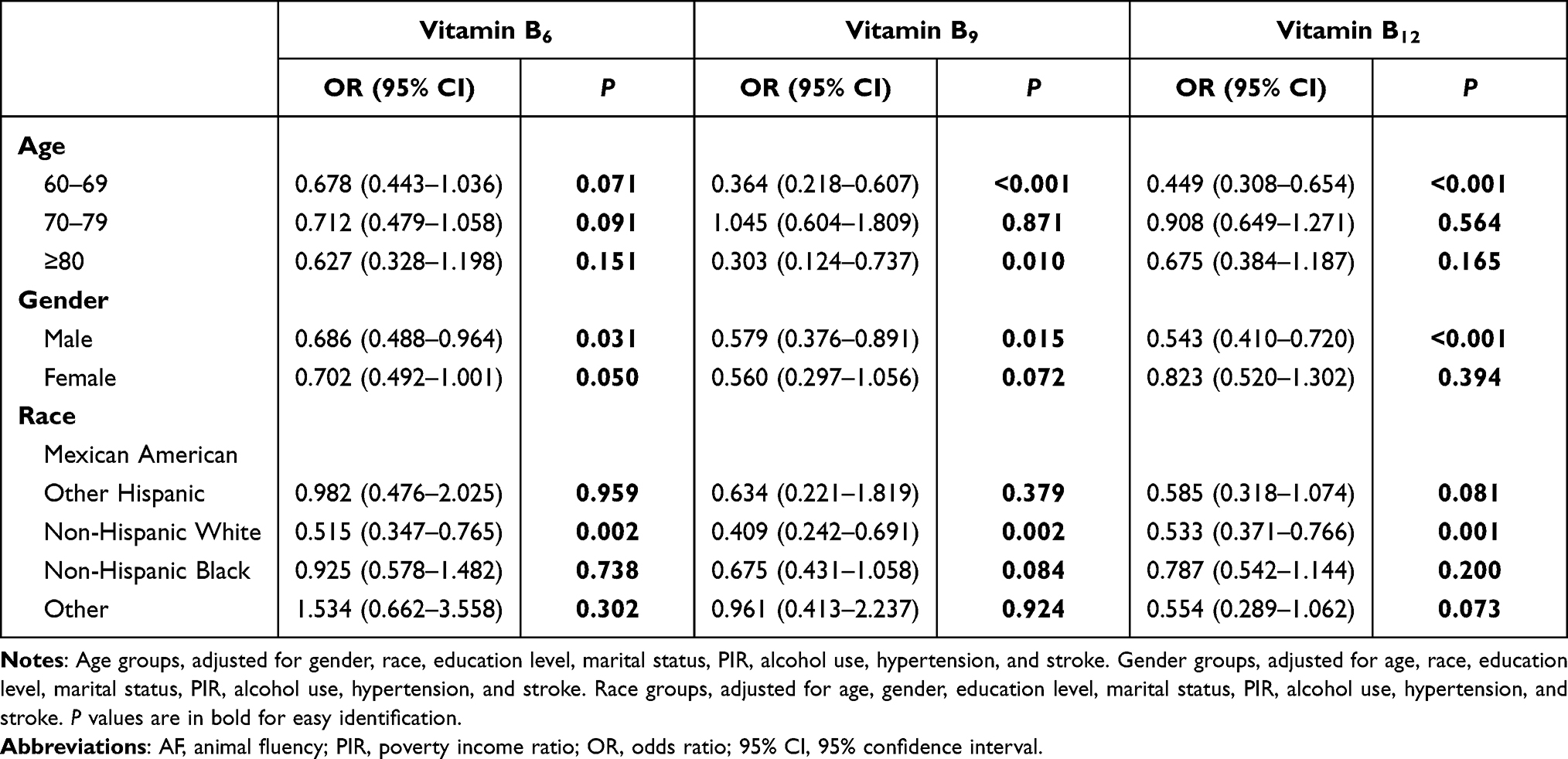 |
Table 6 Subgroup Analysis-AF Test |
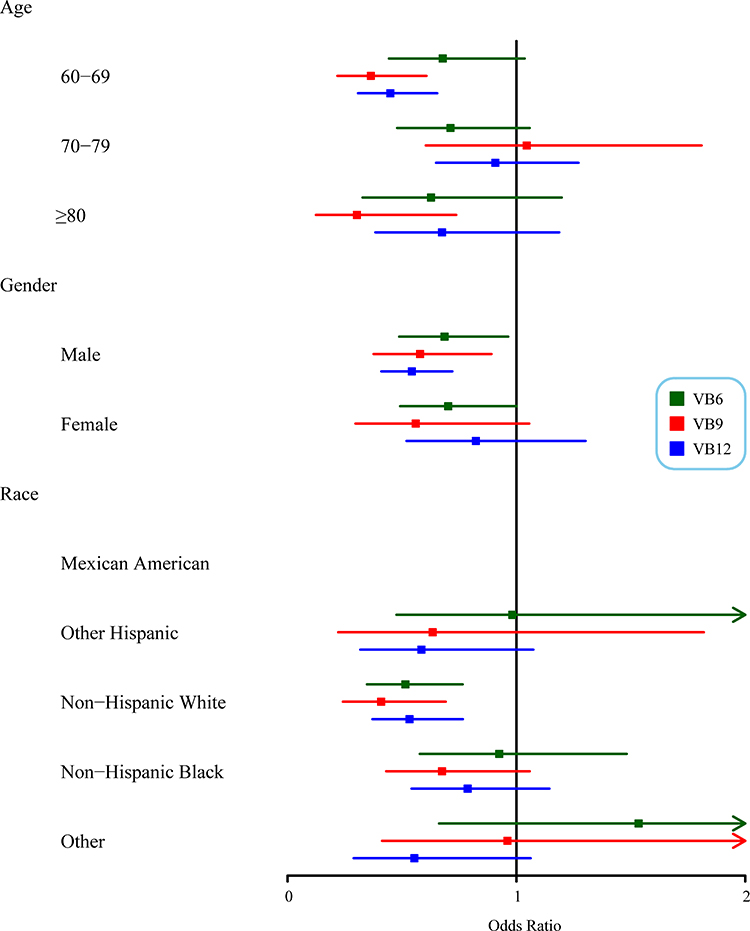 |
Figure 6 Forest plot of the AF test for subgroup analysis. Abbreviations: AF, animal fluency; PIR, poverty income ratio; VB6, vitamin B6; VB9, vitamin B9; VB12, vitamin B12. |
As regards assessment by the DSST test, adequate vitamin B6 intake was linked to a reduced risk of LCP in older adults of 70–79 years (OR: 0.459, 95% CI: 0.289–0.727, P=0.002), male gender (OR: 0.630, 95% CI: 0.412–0.963, P=0.034), and non-Hispanic white race (OR: 0.597, 95% CI: 0.389–0.917, P=0.020), in comparison with low vitamin B6 intake. People of 60–69 (OR: 0.543, 95% CI: 0.340–0.868, P=0.012), 70–79 (OR: 0.525, 95% CI: 0.287–0.961, P=0.038) and ≥ 80 (OR: 0.518, 95% CI: 0.270–0.994, P=0.048) years, older men (OR: 0.437, 95% CI: 0.271–0.706, P=0.001), and the elderly of non-Hispanic white race (OR: 0.463, 95% CI: 0.257–0.834, P=0.012) having adequate vitamin B9 consumption had lower odds of LCP than those consuming low vitamin B9. Vitamin B12 consumption was inversely associated with the risk of LCP for elderly people of male sex (OR: 0.573, 95% CI: 0.396–0.830, P=0.004) and non-Hispanic white race (OR: 0.650, 95% CI: 0.455–0.926, P=0.019) (Table 7, Figure 7).
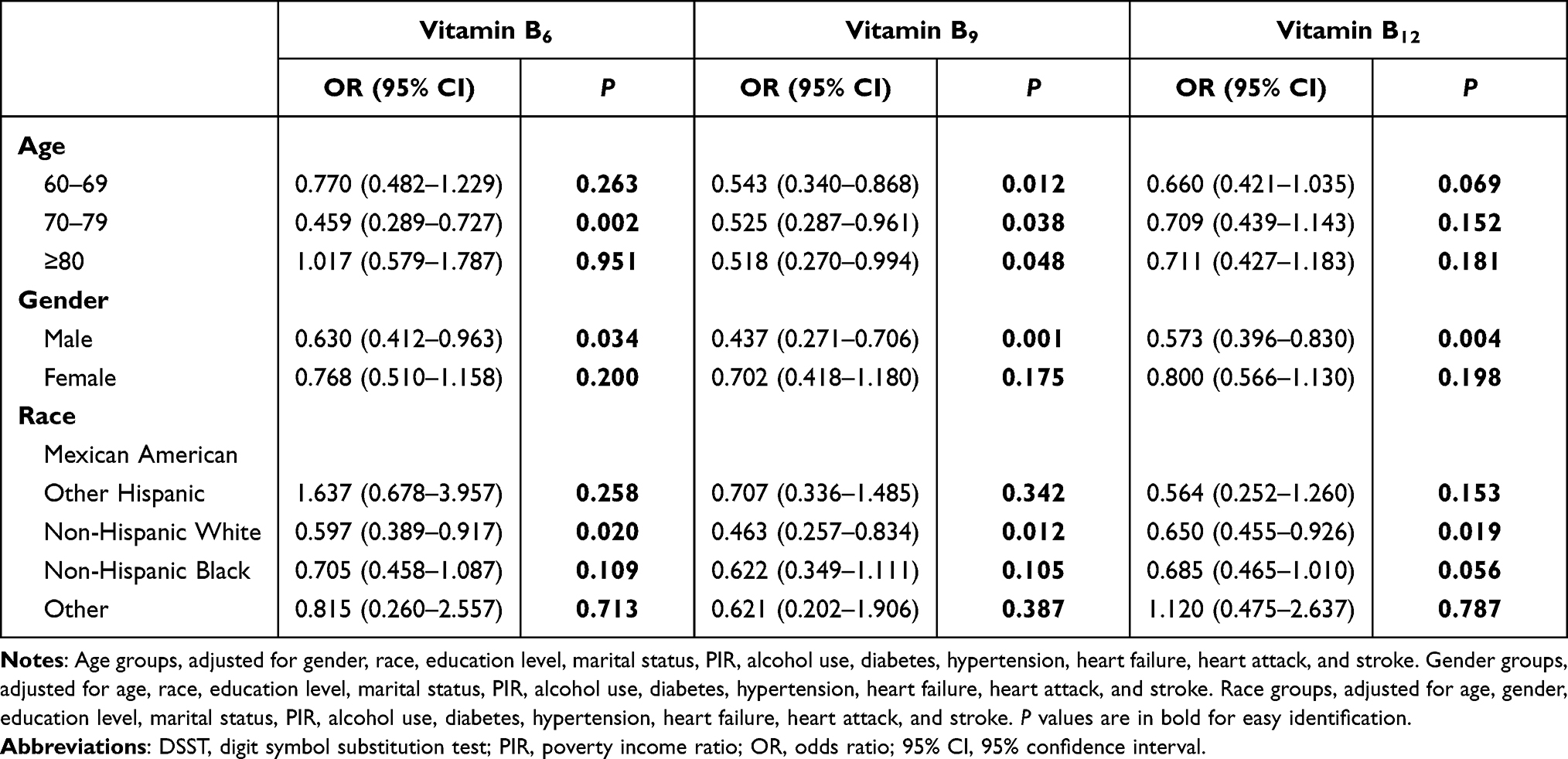 |
Table 7 Subgroup Analysis-DSST Test |
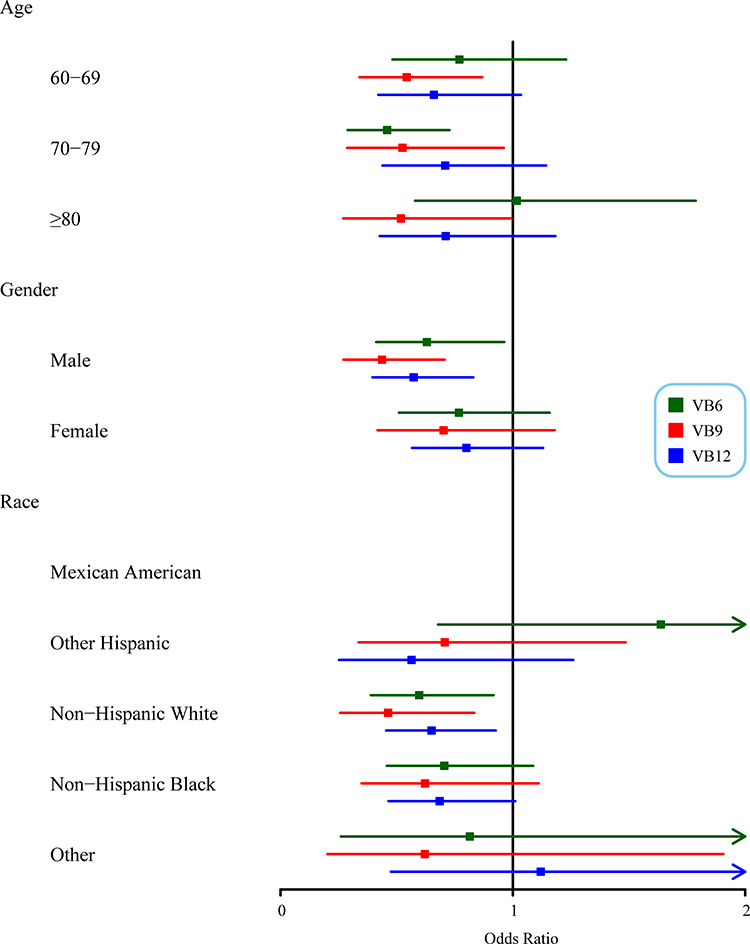 |
Figure 7 Forest plot of the DSST test for subgroup analysis. Abbreviations: DSST, digit symbol substitution test; PIR, poverty income ratio; VB6, vitamin B6; VB9, vitamin B9; VB12, vitamin B12. |
Discussion
Our findings suggest that vitamin B9 and vitamin B12 intakes strongly correlate with cognitive performances among elderly participants. Individuals who consumed adequate vitamin B9 and vitamin B12 are associated with significantly better cognitive performances across all three cognitive tests, including immediate and delayed memory recall, categorical verbal fluency, processing speed, sustained attention, and working memory. Of the three cognitive tests, adequate vitamin B9 and vitamin B12 consumption display the greatest protective effects using the DSST test. Furthermore, adequate vitamin B6 intake is only associated with better cognitive performance when evaluated by the DSST test, implying the prominent role of B vitamins in maintaining normal processing speed, sustained attention, and working memory among elderly people. Further, the relations between 3 B vitamins and cognitive performance vary across different sex, race, and age groups of people.
For vitamin B6, results from the DSST test demonstrate that sufficient intake (≥1.7 mg/day) decreases the risk of low processing speed, sustained attention, and working memory by 31.7% when comparing to inadequate intake (<1.7 mg/day). When compared with low B9 intake (<400 mcg/day), adequate B9 consumption (≥400 mcg/day) is associated with 31.2%, 33.8%, and 46.5% decreases in the risk of low performances in immediate and delayed memory recall, categorical verbal fluency, and impaired processing speed, sustained attention, and working memory, respectively. Adequate vitamin B12 intake also decreases the risk of low immediate and delayed memory recall, low categorical verbal fluency, and low processing speed, sustained attention, and working memory, corresponding to 30.5%, 21.5%, and 33.3% reductions.
The RDA of vitamin B6, B9, and B12 intakes is the same among adults, while the RDA of vitamin B6 is different among elderly males and females.28 To maintain the consistency and simplicity of our analysis, we used ≥1.7 mg/day, the RDA for the elderly male population, as the reference for the adequate vitamin B6 intake group. Since the RDA for the elderly female population was 1.5 mg/day, the low vitamin B6 group contained a portion of female participants that consumed adequate vitamin B6. Nevertheless, a significant reduction in the risk of LCP was still observed when partially including the females with adequate vitamin B6 consumption in the DSST test, implying the significant protective effect of vitamin B6 on the processing speed, sustained attention, and working memory among the elderly.
The Tolerable Upper Intake Level (UL) is the highest level of daily nutrient intake that is unlikely to lead to any risk of adverse health effects to almost all individuals in the general population.28 The ULs of vitamin B6 and vitamin B9 are 100 mg/day and 1000 mcg/day, respectively, and no UL has been established for vitamin B12. Excessive intake of B9 may lead to high serum unmetabolized folic acid and result in an unknown effect.29 Therefore, future clinical study is required to determine the ideal range of vitamin B6, B9, and B12 intakes for elders.
The strong association observed in our study was allied with previous cross-sectional research among aging men from the Veterans Affairs Normative Aging Study (VANAS).17 The VANAS study collected baseline plasma level and dietary intake of vitamin B6, B9, and B12, and found a significant positive linear association between dietary intake and cognitive performance. A more recent animal study using the wild-type male mice discovered that low B9 and low vitamin B6/B12 diets increased neuronal degeneration as compared with the control group,30 implying the crucial impact of dietary B vitamin consumption on cognitive performances.
However, inconclusive results was also detected in studies that examined the effect of dietary or supplement vitamin B6, B9, and B12 intakes on cognitive functions. Kado et al examined the plasma vitamin B6, B9, and B12 concentrations in relation to cognitive function among community-dwelling elders aged 70–79 years by conducting a cross-sectional and longitudinal analysis, the result of which only revealed an association between plasma B9 level and cognitive functions but not between vitamin B6 and B12 levels and cognitive functions.16 A randomized control trial research studied the efficacy of multivitamin supplementation containing vitamin B6, folic acid, and vitamin B12 among elderly Asian patients with Alzheimer’s disease. The cognitive function did not change appreciably with B vitamin supplementation.31 Because of the inconsistent findings, a previous review study suggested that the short-term benefit of vitamin B6 in improving cognitive functions was not supported by strong evidence.32
Several factors may contribute to the discrepancies in research results, including distinct target populations, dissimilar variable measurements, different cognitive evaluation standards, and varied study designs. It is possible that vitamin B6, B9, and B12 intakes establish a more robust relationship with cognitive performances among elderly people. Thus, Thus, lager-scale and multi-center studies of high quality are warranted to confirm our findings or further clarify the effects of B vitamins on the cognitive performance of the elderly.
Some potential mechanisms could be considered when interpreting the association between vitamin B6, B9 and B12 intakes and particular cognitive domains evaluated by the CERAD, AF and DSST tests among the elderly. Vitamin B6 consumption can improve memory status by affecting the function of N-methyl-D-aspartate receptors in addition to enhancing the expression of brain-derived neurotrophic factor (BDNF) in the hippocampus.33,34 Vitamin B6 deficiency relates to cognitive deficits and changes in brain structure.35 Greater intake of vitamin B6 is associated with an increased gray matter volume in the upper frontal gyrus in healthy older adults.36 A positive correlation between vitamin B6 intake and greater local cortical folds was also found in the inferior frontal gyrus and other parts of the brain region.37 Supplementation with vitamin B6 may result in better preservation of gray matter in patients with poor cognitive performance. Vitamin B6 might also relate to the structural integrity of white matter tracts associated with the left middle frontal gyrus, which is linked to processing speed.38 Vitamin B9 was also shown to be positively associated with processing speed, memory recall and verbal fluency,39 while limited evidence focuses on the underlying mechanisms. In the nervous system, B12 is a coenzyme necessary for myelin synthesis, and its deficiency is linked to attention deficits, memory impairment, and dementia.40 Vitamin B12 is involved in acetylcholine synthesis in the brain. Acetylcholine is an essential neurotransmitter for the formation of memory traces and the physiological basis of long-term memory.41 Vitamin B12 is also involved in the synthesis of monoamine neurotransmitters, which play a role in executive function.42 These 3 B vitamins may correlate with the influences of anti-N-Hcy-protein autoantibodies on attention and processing speed.43 More research is underscored to explore more about the association mechanism of vitamin B and different dimensions of cognitive performance. Of note, the DSST was more sensitive to Vitamin B levels than the other two tests. We hypothesized that this may be attributed to more cognitive domains assessed by the DSST test, and vitamin B6, B9 and B12 levels were more significantly associated with cognitive domains in the DSST test than those in the other two tests.
Currently, limited publications focused on specific cognitive domains affected by vitamin B deficiencies, so this study would add to the body of evidence, with a relatively large nationally representative data. Our study uncovered generalizable findings of the therapeutic potential of dietary vitamin B6, B9, and B12 intakes in managing LCP among the elderly population. Besides, subgroup analyses exhibited that the relations between 3 B vitamins and cognitive performance vary across different sex, race, and age groups of people. The limitations of our study mainly lied in the cross-sectional design: i) our study could not establish causality between vitamin B intake and cognitive performance; ii) within-person variations of dietary vitamin B intake may exist.
Conclusion
Vitamin B9 and B12 intakes are strongly associated with LCP odds among elderly participants. Vitamin B6 consumption is linked with the DSST test that captures processing speed, sustained attention, and working memory. Adequate dietary vitamin B9 and B12 intakes correlate with lower risk of LCP among elders, corresponding to an approximately 30% reduction in LCP odds when assessed by the CERAD, AF, and DSST tests. Longitudinal studies are needed to show causation between vitamin B6, B9 and B12 intakes and cognitive performance.
Funding
This study was supported by Joint Project of the Medical Science and Technology of Henan Province (2018020264).
Disclosure
The authors reported no conflicts of interest in this work.
References
1. World Health Organization. Ageing and health; 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.
2. Harada CN, Natelson Love MC, Triebel K. Normal cognitive aging. Clin Geriatr Med. 2013;29(4):737–752. doi:10.1016/j.cger.2013.07.002
3. Association AP. Diagnostic and Statistical Manual of Mental Disorders.
4. World Health Organization. Dementia; 2020. Accessed from: https://www.who.int/news-room/fact-sheets/detail/dementia.
5. Morris MC, Tangney CC, Wang Y, et al. MIND diet slows cognitive decline with aging. Alzheimers Dement. 2015;11(9):1015–1022. doi:10.1016/j.jalz.2015.04.011
6. Chang M, Jonsson PV, Snaedal J, et al. The effect of midlife physical activity on cognitive function among older adults: AGES—Reykjavik study. J Gerontol A Biol Sci Med Sci. 2010;65A(12):1369–1374. doi:10.1093/gerona/glq152
7. Phillips C. Lifestyle modulators of neuroplasticity: how physical activity, mental engagement, and diet promote cognitive health during aging. Neural Plast. 2017;2017:1–22. doi:10.1155/2017/3589271
8. Mikkelsen K, Apostolopoulos V. B vitamins and ageing. In: Harris JR, Korolchuk VI, editors. Biochemistry and Cell Biology of Ageing: Part I Biomedical Science. Vol 90. Subcellular Biochemistry. Springer Singapore; 2018:451–470.
9. Mikkelsen K, Stojanovska L, Tangalakis K, Bosevski M, Apostolopoulos V. Cognitive decline: a vitamin B perspective. Maturitas. 2016;93:108–113. doi:10.1016/j.maturitas.2016.08.001
10. Beydoun MA, Beydoun HA, Gamaldo AA, Teel A, Zonderman AB, Wang Y. Epidemiologic studies of modifiable factors associated with cognition and dementia: systematic review and meta-analysis. BMC Public Health. 2014;14:643. doi:10.1186/1471-2458-14-643
11. Gropper SS, Smith JL, Carr TP. Advanced nutrition and human metabolism. In: Cengage Learning.
12. Yudkoff M. Disorders of amino acid metabolism. In: Brady ST, Siegel GJ, Albers RW, Price DL, editors.Basic Neurochemistry. 8th ed. Elsevier; 2012: 737-754.
13. Smith AD, Refsum H. Homocysteine, B vitamins, and cognitive impairment. Annu Rev Nutr. 2016;36:211–239. doi:10.1146/annurev-nutr-071715-050947
14. Smith AD. The worldwide challenge of the dementias: a role for B vitamins and homocysteine? Food Nutr Bull. 2008;29(2_suppl1):S143–S172. doi:10.1177/15648265080292S119
15. Selhub J, Bagley LC, Miller J, Rosenberg IH. B vitamins, homocysteine, and neurocognitive function in the elderly. Am J Clin Nutr. 2000;71(2):614S–620S. doi:10.1093/ajcn/71.2.614s
16. Kado DM, Karlamangla AS, Huang M-H, et al. Homocysteine versus the vitamins folate, B6, and B12 as predictors of cognitive function and decline in older high-functioning adults: macArthur studies of successful aging. Am J Med. 2005;118(2):161–167. doi:10.1016/j.amjmed.2004.08.019
17. Tucker KL, Qiao N, Scott T, Rosenberg I, Spiro A. High homocysteine and low B vitamins predict cognitive decline in aging men: the veterans affairs normative aging study. Am J Clin Nutr. 2005;82(3):627–635. doi:10.1093/ajcn/82.3.627
18. National Center for Health Statistics. NHANES - about the National Health and Nutrition Examination Survey; 2020. Available from: https://www.cdc.gov/nchs/nhanes/about_nhanes.htm.
19. Morris JC, Heyman A, Mohs RC, et al. The Consortium to Establish a Registry for Alzheimer’s Disease (CERAD). Part I. Clinical and neuropsychological assessment of Alzheimer’s disease. Neurology. 1989;39(9):1159–1165. doi:10.1212/WNL.39.9.1159
20. Strauss E, Sherman EMS, Spreen O. A Compendium of Neuropsychological Tests: Administration, Norms, and Commentary.
21. Ryan JJ, Lopez SJ. Wechsler adult intelligence scale-III. In: Dorfman WI, Hersen M, editors. Understanding Psychological Assessment. Perspectives on Individual Differences. Springer US; 2001:19–42.
22. Brody DJ, Kramarow EA, Taylor CA, McGuire LC. Cognitive performance in adults aged 60 and over: National Health and Nutrition Examination Survey, 2011–2014. Natl Health Stat Rep. 2019;126:1–23.
23. Dong X, Li S, Chen J, Li Y, Wu Y, Zhang D. Association of dietary ω-3 and ω-6 fatty acids intake with cognitive performance in older adults: National Health and Nutrition Examination Survey (NHANES) 2011–2014. Nutr J. 2020;19(1):25. doi:10.1186/s12937-020-00547-7
24. Dong X, Li S, Sun J, Li Y, Zhang D. Association of coffee, decaffeinated coffee and caffeine intake from coffee with cognitive performance in older adults: National Health and Nutrition Examination Survey (NHANES) 2011–2014. Nutrients. 2020;12(3):840. doi:10.3390/nu12030840
25. Chen SP, Bhattacharya J, Pershing S. Association of vision loss with cognition in older adults. JAMA Ophthalmol. 2017;135(9):963–970. doi:10.1001/jamaophthalmol.2017.2838
26. Bailey RL, Jun S, Murphy L, et al. High folic acid or folate combined with low vitamin B-12 status: potential but inconsistent association with cognitive function in a nationally representative cross-sectional sample of US older adults participating in the NHANES. Am J Clin Nutr. 2020;112(6):1547–1557. doi:10.1093/ajcn/nqaa239
27. Blanton CA, Moshfegh AJ, Baer DJ, Kretsch MJ. The USDA automated multiple-pass method accurately estimates group total energy and nutrient intake. J Nutr. 2006;136(10):2594–2599. doi:10.1093/jn/136.10.2594
28. Institute of Medicine. Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; 2006.
29. Bailey LB, Stover PJ, McNulty H, et al. Biomarkers of nutrition for development—folate review12345. J Nutr. 2015;145(7):1636S–1680S. doi:10.3945/jn.114.206599
30. Nuru M, Muradashvili N, Kalani A, Lominadze D, Tyagi N. High methionine, low folate and low vitamin B6/B12 (HM-LF-LV) diet causes neurodegeneration and subsequent short-term memory loss. Metab Brain Dis. 2018;33(6):1923–1934. doi:10.1007/s11011-018-0298-z
31. Sun Y, Lu C-J, Chien K-L, Chen S-T, Chen R-C. Efficacy of multivitamin supplementation containing vitamins B6 and B12 and folic acid as adjunctive treatment with a cholinesterase inhibitor in Alzheimer’s disease: a 26-week, randomized, double-blind, placebo-controlled study in Taiwanese patients. Clin Ther. 2007;29(10):2204–2214. doi:10.1016/j.clinthera.2007.10.012
32. Malouf R, Evans JG. Vitamin B6 for cognition. Cochrane Database Syst Rev. 2003;4. doi:10.1002/14651858.CD004393
33. Barichello T, Generoso JS, Simões LR, et al. Vitamin B6 prevents cognitive impairment in experimental pneumococcal meningitis. Exp Biol Med (Maywood). 2014;239(10):1360–1365. doi:10.1177/1535370214535896
34. Guilarte TR. Vitamin B6 and cognitive development: recent research findings from human and animal studies. Nutr Rev. 1993;51(7):193–198. doi:10.1111/j.1753-4887.1993.tb03102.x
35. Selhub J, Troen A, Rosenberg IH. B vitamins and the aging brain. Nutr Rev. 2010;68(Suppl 2):S112–S118. doi:10.1111/j.1753-4887.2010.00346.x
36. Erickson KI, Suever BL, Prakash RS, Colcombe SJ, McAuley E, Kramer AF. Greater intake of vitamins B6 and B12 spares gray matter in healthy elderly: a voxel-based morphometry study. Brain Res. 2008;1199:20–26. doi:10.1016/j.brainres.2008.01.030
37. Jannusch K, Jockwitz C, Bidmon HJ, Moebus S, Amunts K, Caspers S. A complex interplay of vitamin B1 and B6 metabolism with cognition, brain structure, and functional connectivity in older adults. Front Neurosci. 2017;11:596. doi:10.3389/fnins.2017.00596
38. Turken A, Whitfield-Gabrieli S, Bammer R, Baldo JV, Dronkers NF, Gabrieli JD. Cognitive processing speed and the structure of white matter pathways: convergent evidence from normal variation and lesion studies. Neuroimage. 2008;42(2):1032–1044. doi:10.1016/j.neuroimage.2008.03.057
39. Bryan J, Calvaresi E, Hughes D. Short-term folate, vitamin B-12 or vitamin B-6 supplementation slightly affects memory performance but not mood in women of various ages. J Nutr. 2002;132(6):1345–1356. doi:10.1093/jn/132.6.1345
40. Briani C, Dalla Torre C, Citton V, et al. Cobalamin deficiency: clinical picture and radiological findings. Nutrients. 2013;5(11):4521–4539. doi:10.3390/nu5114521
41. Haam J, Yakel JL. Cholinergic modulation of the hippocampal region and memory function. J Neurochem. 2017;142(Suppl2):111–121. doi:10.1111/jnc.14052
42. Leung BM, Kaplan BJ. Perinatal depression: prevalence, risks, and the nutrition link–a review of the literature. J Am Diet Assoc. 2009;109(9):1566–1575. doi:10.1016/j.jada.2009.06.368
43. Włoczkowska O, Perła-Kaján J, Smith AD, de Jager C, Refsum H, Jakubowski H. Anti-N-homocysteine-protein autoantibodies are associated with impaired cognition. Alzheimers Dement. 2021;7(1):e12159. doi:10.1002/trc2.12159
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.