Back to Journals » Clinical Ophthalmology » Volume 16
Visual and Topographic Outcomes of Corneal Collagen Cross Linking for Post LASIK Ectasia
Authors Nasef MH, El Emam SY, Haleem TI, Shalaby WS, Allam WA
Received 12 April 2022
Accepted for publication 8 June 2022
Published 20 June 2022 Volume 2022:16 Pages 2025—2032
DOI https://doi.org/10.2147/OPTH.S370033
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Mohamed H Nasef, Sharif Y El Emam, Tamer I Haleem, Wesam S Shalaby, Waleed A Allam
Ophthalmology Department, Faculty of Medicine, Tanta University, Tanta, Gharbia, Egypt
Correspondence: Mohamed H Nasef, Tanta University Ophthalmology Hospital, Tanta University Medical Campus, Al-Geish St, Tanta, Gharbia, 31527, Egypt, Tel +20 10 02826555, Email [email protected]
Purpose: To assess the topographic and visual outcomes of corneal cross-linking (CXL) for post-LASIK ectasia.
Methods: A retrospective case series of patients who had progressive post-LASIK ectasia, with at least 2 years of follow-up. They had epithelium-off CXL. Topographical and visual changes were recorded.
Results: The study included 21 eyes of 11 patients. At month 24, the final logMAR corrected distance visual acuity (CDVA) and spherical equivalent (SE) were stable compared to baseline (0.16, and − 2.0 diopter (D), respectively). The final Kmean and Kmax were 42.5 and 47.4 D, respectively. Stability or improvement in CDVA, SE, and Kmax was seen in 17 eyes (81%). Significant corneal thinning was seen (438 vs 457 microns, p = 0.003). Thinning by 2% or more was seen in 12 eyes (57.1%). Failure of CXL was seen in 4 eyes (19%). No other ocular complications were seen.
Conclusion: CXL for post LASIK ectasia is a safe and effective modality. Despite corneal thinning, there was stability or improvement in topographic parameters and CDVA over the 2-year follow-up period.
Keywords: corneal collagen cross linking, corneal ectasia, LASIK, refractive surgery
Introduction
Laser-assisted in situ keratomileusis (LASIK) is one of the most commonly performed kerato-refractive procedures worldwide. The efficacy and safety of LASIK are well documented. Although rare, the complications associated with this procedure are not unknown. Intraoperative complications, such as suction loss, free cap, buttonhole flap and decentered ablation, and postoperative complications, such as flap striae and dislocation, diffuse lamellar keratitis, epithelial ingrowth, and refractive regression, have all been well reviewed.1
Iatrogenic keratectasia is a serious complication following corneal refractive surgery, specifically LASIK, with a reported prevalence of 1/2500.2 It manifests as a progressive increase in myopia and irregular astigmatism, a decrease in the uncorrected and corrected distant visual acuity, as well as an increased corneal steepening, reduced corneal biomechanical strength, and decreased corneal thickness.3 The clinical picture of ectasia resembles that of progressive keratoconus.4
Early cases of post-LASIK ectasia were described by Seiler and Quurke in 1998.5 Risk factors that increase the probability of post-LASIK ectasia include thin corneas, deep ablations, thin residual stromal bed, and corneal topographic abnormalities such as forme fruste keratoconus and pellucid marginal degeneration.6,7 However, ectasia continues to occur despite taking all safety measures, in cases with low myopia,8 cases with no obvious preoperative signs of keratoconus,9 and even following photorefractive keratectomy.10
Available treatment options are limited. The management ranges from spectacle use, rigid contact lenses, intrastromal corneal rings,11 lamellar keratoplasty,12 or penetrating keratoplasty.13 A more recent option is corneal collagen cross linking (CXL), that has been used for the treatment of iatrogenic ectasia.
CXL is a minimally invasive procedure used to slow down or stop the progression of keratoconus. It strengthens the biomechanical stability of the cornea via adding polymer bands between corneal collagen fibers. It uses topically applied riboflavin (vitamin B2) solution, to saturate the cornea, and ultraviolet A (UV-A), to set off a chemical reaction to induce trans-collagen cross-links shortening.14
Today, CXL is widely used for management of both keratoconus and ectasia. It significantly reduces the number of keratoplasties performed for keratoconus.15 It not only has a halting effect on keratoconus progression but can also lead to some regression of the ectatic changes, improvement of corneal regularity, and visual acuity.16
In the current study, we evaluated the corrected distant visual acuity (CDVA) and corneal topographic changes as following corneal collagen cross linking for cases with post-LASIK ectasia.
Patients and Methods
This retrospective case series was carried out at a tertiary eye care center. The study was approved by the Institutional Review Board (IRB) and Human Research Ethics Committee at the Faculty of Medicine, Tanta University, Egypt (approval code 35297/2/22), and was carried out in adherence to the tenets of the Declaration of Helsinki. The patients’ data confidentiality was maintained. A signed informed consent had been obtained after a full explanation of the condition and the treatment options. Similarly, the nature of the procedure and its potential complications were explained to all participants. The medical records of patients who underwent corneal collagen cross linking for progressive post-LASIK ectasia between January 2017 and January 2020, and had 2 or more years of follow-up were reviewed.
Patients over 18 years old, with a diagnosis of progressive post-LASIK ectasia and minimal central corneal thickness (CCT) of 400 microns, were included. Progressive ectasia was defined as a change in at least three of the following parameters verified by clinical examination and repeated Scheimpflug imaging over at least 6 months: Deterioration of CDVA or uncorrected distant visual acuity (UDVA) by ≥2 Snellen lines, significant changes in refractive error especially astigmatic component by ≥1.00 diopter (D), progressive steepening of corneal surface ≥1.00 D of either the mean K (Kmean) or maximum simulated keratometry (Kmax), which equals 3 standard deviations (SD), 2% reduction of corneal thickness, or increasing of the posterior corneal elevation. Pentacam HR (Oculus Optikgeräte GmbH, Wetzlar, Germany) was used to collect topographic data. Eyes with ocular surface pathology, those with less than 2-year postoperative follow-up, actual or intended pregnancy, and connective tissue diseases were excluded. Patients who underwent CXL combined with other procedures, such as intracorneal ring segments or photorefractive keratectomy, were also excluded.
Treatment procedures were performed by 3 surgeons (M.H, T.I, W.A). All surgeons were fellowship-trained cornea specialists. An epithelium-off CXL technique was used for all participants. The procedure was conducted under sterile settings in the operating theatre. Topical anesthesia was used in the form of benoxinate hydrochloride 0.4% eyedrops (Benox®, Eipico, Cairo, Egypt). After lid speculum placement, the central 8 mm corneal epithelium was removed by an Amoils brush. Riboflavin 5-phosphate 0.1% in 20% dextran solution (Ricrolin®, SOOFT Italia S.p.A., Montegiorgio, Italy) was instilled every 2 minutes for 20 minutes. According to the Dresden protocol of Theo Seiler,17 the ultraviolet A (UV-A) lamp (VEGA CBM-X-Linker (CSO, Florence, Italy)) was focused perpendicularly on the cornea with the radiant energy of 3.0 ± 0.3 mW/cm2 for 30 minutes of continuous exposure. During UV-A radiation, riboflavin drops were applied to the cornea every 2 minutes. After treatment, a bandage soft contact lens was inserted (ACUVUE®, Johnson & Johnson Vision Care, Inc.). Gatifloxacin 0.5% (GATISTAR®, Orchidia pharmaceuticals, Egypt) eyedrops were instilled, four times daily for seven days. Tobramycin-dexamethasone 0.1% eye drops (TOBRADEX®, Alcon Laboratories, Inc.) was also used 4 times daily, and was tapered over 4 weeks. Pain was controlled by orally administered non-steroidal anti-inflammatory drugs.
The patient was examined after 4–5 days following CXL, to evaluate epithelial healing, and detect any signs of infection. Contact lens was removed after complete epithelial healing.
Visits at baseline, postoperative months 6, 12, 18 and 24 were reviewed. Demographic data including age and sex were collected. Baseline and postoperative clinical data, at every visit, included CDVA and UDVA using Snellen chart, manifest refractions, and topographic parameters using Scheimpflug imaging including keratometry (K1, K2, Kmax) and CCT. The Kmean was calculated as average of the K1 and K2.
The main outcome measures were the changes in CDVA, refractive, and topographic parameters, pachymetry at month 24 following CXL as compared to baseline. The complication rate was identified as the percentage of eyes that had lost ≥2 Snellen lines of CDVA at month 24 follow-up as compared with baseline. CXL failure was defined as the percentage of eyes with a Kmax increase of ≥1.00 at month 24 follow-up as compared with baseline.18
No other ocular complications were noted, such as epithelial ingrowth, infectious keratitis, cataract formation, or retinal damage.
Statistical analyses were performed using SPSS statistics for Windows, version 27.0 (IBM Corp., Armonk, NY). Snellen visual acuity measurements were converted to logarithm of the minimum angle of resolution (logMAR) equivalents for the purpose of data analysis. Continuous variables were summarized as mean ± standard deviation. Proportions (%) were used to describe categorical variables. Paired sample t-tests were used to compare continuous variables within the same group. P-values less than 0.05 were considered significant.
Results
A total of 21 eyes of 11 patients were included in the study with a mean age of 31.3 ± 8.6 years. Eight patients (72.7%) were females. The baseline logMAR CDVA was 0.22 ± 0.2, baseline spherical equivalent (SE) was −2.0 ± 1.8 D, Kmean was 42.2 ± 3.3 D, Kmax was 48.6 ± 4.6 D, and CCT was 457.6 ± 48.4 microns.
Changes in the refractive measurements over time are displayed in Table 1. At month 24, all refractive parameter changes were statistically insignificant compared to baseline. Compared to baseline, the final logMAR CDVA was 0.16 ± 0.22 (p = 0.254), and the SE was −2.0 ± 2.7 D (p = 0.876). Figure 1 shows that CDVA remained stable in 5 eyes (23.8%), gained 1 line in 8 eyes (38.1%), and gained 2 lines or more in 4 eyes (19.1%). On the other hand, 4 eyes (19.1%) had deterioration of their CDVA. Figure 2 shows that the SE in 9 eyes remained stable (less than 1 D change) (43%), improved by 1.0 D in 6 eyes (28.5%), and improved by 2.0 D or more in 2 eyes (9.5%). Similarly, 4 eyes (19.1%) had deterioration of their SE.
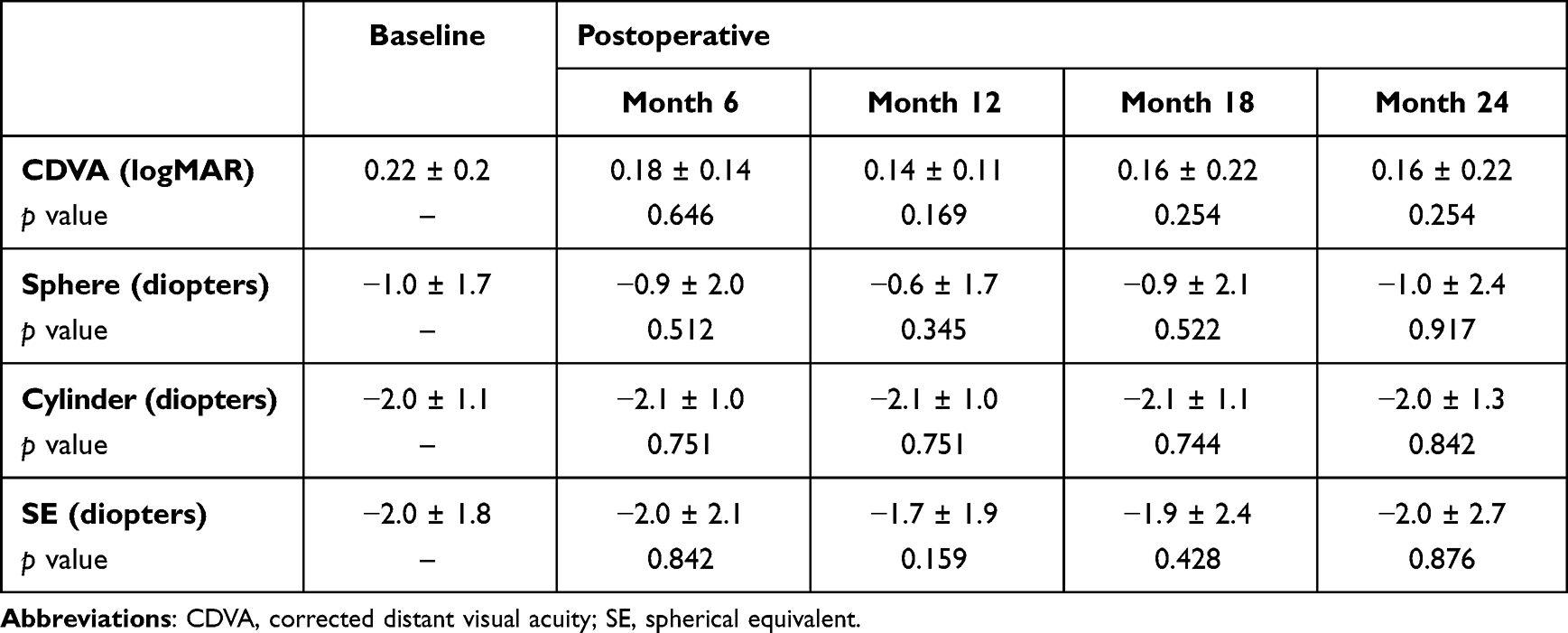 |
Table 1 Changes in Refractive Measurements Within the Follow-Up Period following Corneal Collagen Cross Linking |
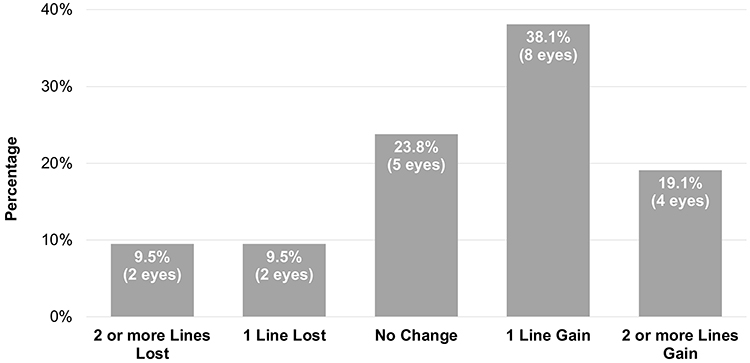 |
Figure 1 Corrected distant visual acuity at month 24 after corneal collagen cross linking. |
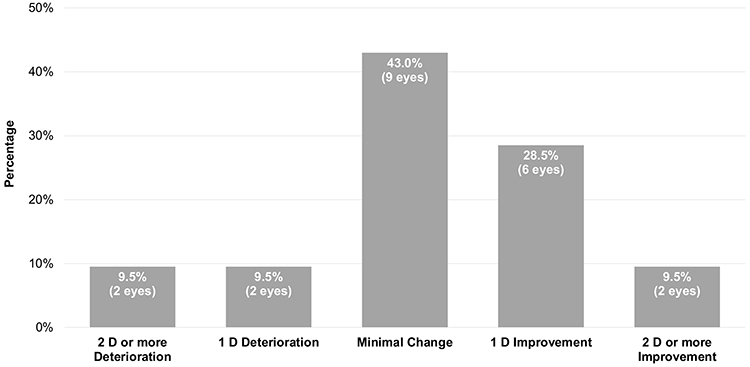 |
Figure 2 Change in spherical equivalent at month 24 compared to baseline after corneal collagen cross linking. |
Changes in the topographic measurements over time are displayed in Table 2. At month 24, most topographic parameter changes were statistically insignificant compared to baseline. The Kmax was 47.4 ± 4.1 D (p = 0.347), but CCT showed significant thinning as compared to baseline (438.2 ± 59.3 microns; p = 0.003). Figure 3 shows that Kmax in 3 eyes remained stable (14.3%), improved by 1.0 D in 4 eyes (19.1%), or improved by 2.0 D or more in 10 eyes (47.6%). On the contrary, an increase in the Kmax was seen in 4 eyes (19.1%). The Kmean was mostly stable throughout the follow-up period (42.2 ± 3.3 D at baseline, and 42.25 ± 3.75 D at month 24). Figure 4 shows that pachymetry in 8 eyes remained stable (38.1%) or decreased by 2% or more in 12 eyes (57.1%).
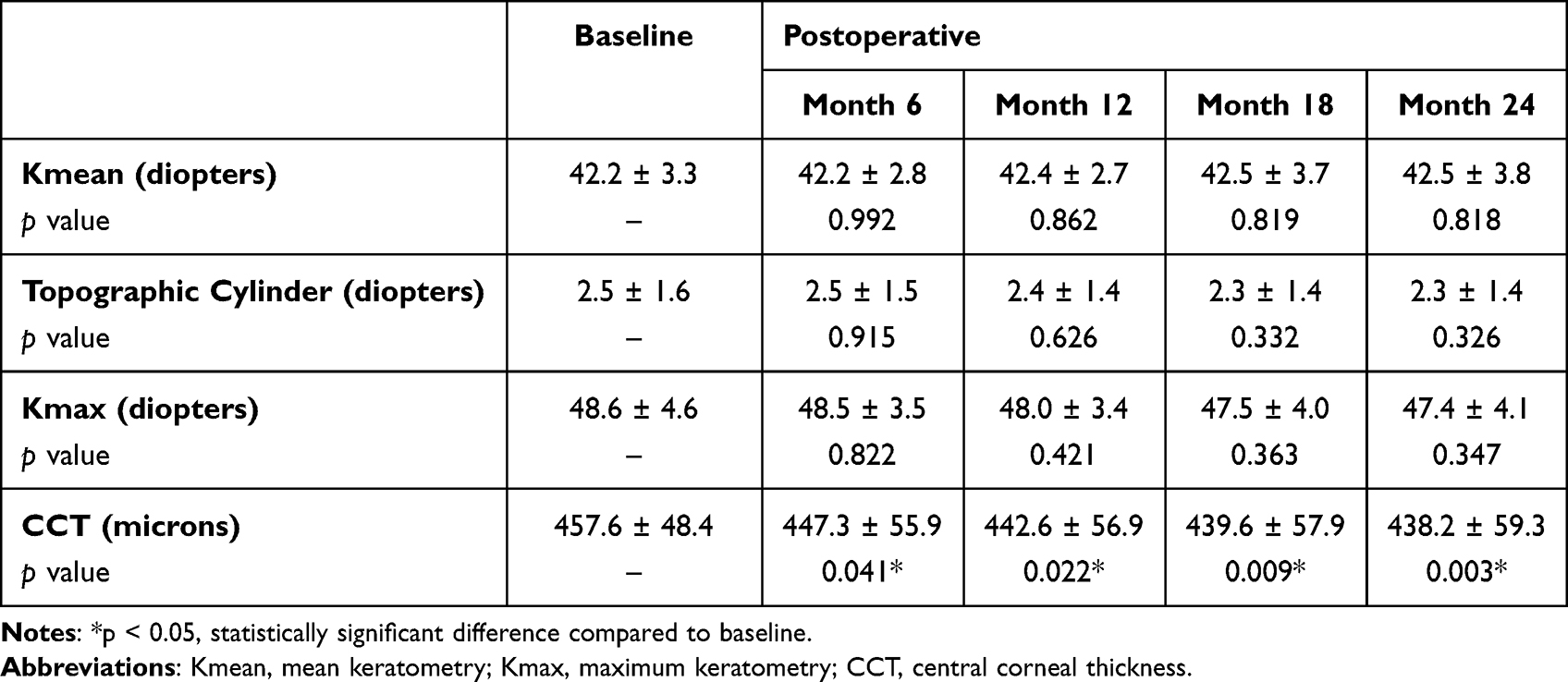 |
Table 2 Changes in Topographic Measurements Within the Follow-Up Period Following Corneal Collagen Cross Linking |
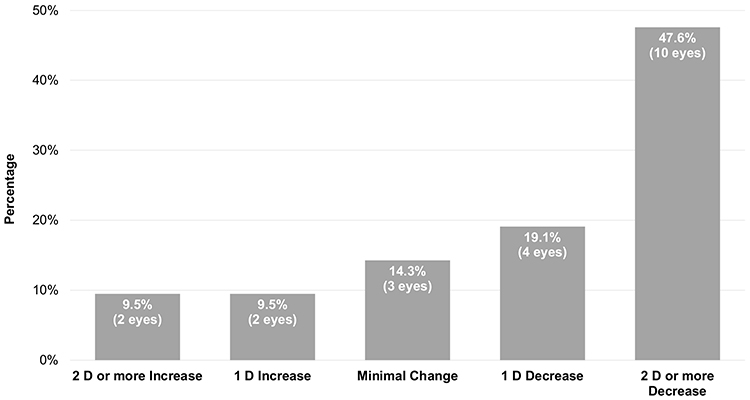 |
Figure 3 Change in maximum keratometry (Kmax) at month 24 compared to baseline after corneal collagen cross linking. |
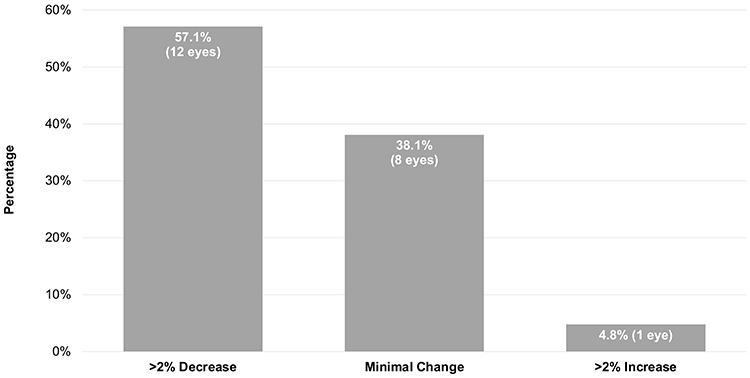 |
Figure 4 Change in pachymetry at month 24 compared to baseline after corneal collagen cross linking. |
At month 24, the complication rate (percentage of eyes with a loss of ≥2 Snellen lines of CDVA) was 9.5% (2 eyes), and the failure rate (percentage of eyes with an increase in Kmax of ≥1.00) was 19.0% (4 eyes). Those eyes with progressive keratectasia were managed by deep anterior lamellar keratoplasty.
All eyes developed a transient faint subepithelial haze after CXL, which disappeared within 3–6 months following treatment. No other ocular complications were reported.
Discussion
Corneal ectasia is a serious; however, uncommon complication that happens following corneal refractive surgery, due to the reduction in the biomechanical stability of the cornea, and leads to progressive visual deterioration.19 Corneal collagen cross linking, a minimally invasive procedure, has been proven to be the most effective method used to stop the ectasia progression via induction of corneal cross linking to increase corneal stability and stiffness.17 CXL use is not limited to post-LASIK ectasia, but also to other corneal ectatic conditions as keratoconus20 and pellucid marginal degeneration,21 as well as a therapeutic tool in corneal infections,22 and possibly in chemical burns23 and pseudophakic bullous keratopathy.24 Various techniques have been describes, alone,25 or in conjunction with ablation.26
We used a traditional epithelium-off technique, applying riboflavin and UV-A onto the corneal flap. Due to epithelial removal, the recovery is uncomfortable and takes a long duration. Various epithelium-on techniques have been developed.27 Although safer and more comfortable, it has shown inferior efficacy compared to the epithelium-off technique.28,29 Recent studies have investigated under-flap stromal bed CXL, via applying riboflavin directly to the stromal bed, after lifting the LASIK flap, and then application of UV-A after flap repositioning, whether as an adjunct with LASIK,30 or for post LASIK ectasia.31,32 The rationale is preserving the epithelium, which means less pain and faster recovery while strengthening the residual corneal bed, noting the flap has little contribution to the biomechanical strength of the cornea.33 Nevertheless, a recent study showed the traditional CXL to generate greater stiffening effect in the anterior cornea, compared to the under-flap protocol.34 Additionally, a possible complication is epithelial ingrowth into the flap interface.32
In this study, we assessed the stability of visual acuity and corneal topography following CXL in eyes with post LASIK ectasia, to add to the plethora of studies reporting the positive results of CXL in treating keratoconus, as well as post LASIK ectasia.35 In their 12-month US-based multicenter trial including 91 patients, Hersh et al showed that a significant improvement in the Kmax values and CDVA was seen in the crosslinking treatment group, compared to the sham group.36 Similarly, Sharif et al showed stability or improvement in CDVA in the majority of the study eyes, together with decrease of the Kmax, in 13 of the 17 treated eyes, over the 80 months follow-up period.37 A significant improvement in CDVA was also seen in studies by Yildirim et al and Tong et al.16,38
The aforementioned findings of previous studies are in agreement with the results of our work. In 17 of the 21 eyes included in this study, stabilization or improvement of the CDVA was seen. The topographic measurements were mostly stable or improved. The Kmax was stable in 3 eyes (14.3%), while improved in two thirds of the eyes (14 eyes, 66.6%).
However, some eyes did not respond as well to CXL, with variable failure rates. In our study, 2 eyes (9.5%) had a deterioration of CDVA by 1 line, and another 2 eyes (9.5%) had 2 or more-line deterioration. Kmax deterioration was also seen in 4 eyes (19.1%). Despite these 4 eyes being considered treatment failures, it is not clear if CXL was completely ineffective or merely did not slow progression completely.18
These negative results come in agreement with some of the previously published studies. In Hersh et al’s study, an increase in the mean Kmax value was seen in 3 eyes (4%), with a clinically uncorrelated decrease in the CDVA in a different set of 3 eyes (4%).36 In another study, 2 out of 14 eyes (14%) showed 2 or more diopter deterioration between 12 and 36 months of follow-up.38 Moreover, Marino et al’s case series had a 22.5% loss of 2 lines of more of CDVA at 2 years following accelerated CXL for cases with post-LASIK ectasia.39 Similarly, in a different study, 3 of the 22 post-LASIK ectatic eyes (14%) showed a 2 line or more decrease in visual acuity over the one-year follow-up period.40
Regarding corneal thickness, our study corroborates the data by Vinciguerra et al, which over a 12-month period, demonstrated a significant decrease in corneal thickness, following CXL for post-LASIK ectasia.41 Progressive corneal thickness reduction has been reported up to 6 years after CXL.42 This may be explained by new collagen compaction and disappearance of stromal edema.43
On the contrary, the study by Li et al showed an initial decrease in pachymetry within the first 3 months post CXL, with a rebound overall increase in corneal thickness at the end of their 12-month follow-up period.44 They explained this by the recovery of activated keratocytes, after their initial apoptosis following CXL, and laying down of thicker collagen fibers.45 Similarly, the normalization of the corneal thickness, towards baseline thickness, following initially thinning, was seen by Greenstein et al.46
These conflicting results may be related to our use of optical pachymetry, which leads to a pseudo-reduction in early postoperative keratometric measurements, due to the negative effect caused by epithelial thinning, keratocyte loss in the anterior-mid stroma, and changes in stromal reflectivity.47
Our study shows that CXL is a safe and effective interventional modality for post-LASIK ectasia. It halts the ectatic pathology, reduces corneal topographic indices, and improves visual acuity.
One limitation of this study is the retrospective nature. The lack of the comparative control, as 10 patients were treated bilaterally, is another limitation. Additionally, the interim analysis of a subpopulation, relatively small number of eyes, and incomplete follow-up for some subjects could also be considered. Nevertheless, the study has a long follow-up, with all the included patients having completed at least 24 months of follow-up.
Conclusion
Corneal collagen cross linking is a safe and effective procedure in cases with post-LASIK ectasia. It has a positive effect on the corneal topography, improving the topographic indices, with halting its progression. The majority of cases had stability of their visual acuity for a prolonged period of time.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sahay P, Bafna RK, Reddy JC, Vajpayee RB, Sharma N. Complications of laser-assisted in situ keratomileusis. Indian J Ophthalmol. 2021;69(7):1658–1669. doi:10.4103/ijo.IJO_1872_20
2. Spadea L, Cantera E, Cortes M, Conocchia NE, Stewart CW. Corneal ectasia after myopic laser in situ keratomileusis: a long-term study. Clin Ophthalmol. 2012;6:1801–1813. doi:10.2147/OPTH.S37249
3. Comaish IF, Lawless MA. Progressive post-LASIK keratectasia: biomechanical instability or chronic disease process? J Cataract Refract Surg. 2002;28(12):2206–2213. doi:10.1016/s0886-3350(02)01698-x
4. Probst LE, Machat JJ. Mathematics of laser in situ keratomileusis for high myopia. J Cataract Refract Surg. 1998;24(2):190–195. doi:10.1016/S0886-3350(98)80199-5
5. Seiler T, Quurke AW. Iatrogenic keratectasia after LASIK in a case of forme fruste keratoconus. J Cataract Refract Surg. 1998;24(7):1007–1009. doi:10.1016/s0886-3350(98)80057-6
6. Binder PS. Ectasia after laser in situ keratomileusis. J Cataract Refract Surg. 2003;29(12):2419–2429. doi:10.1016/j.jcrs.2003.10.012
7. Randleman JB, Russell B, Ward MA, Thompson KP, Stulting RD. Risk factors and prognosis for corneal ectasia after LASIK. Ophthalmology. 2003;110(2):267–275. doi:10.1016/S0161-6420(02)01727-X
8. Amoils PS, Deist MB, Gous P, Amoils PM. Iatrogenic keratectasia after laser in situ keratomileusis for less than −4.0 to −7.0 diopters of myopia. J Cataract Refract Surg. 2000;26(7):967–977. doi:10.1016/s0886-3350(00)00434-x
9. Klein SR, Epstein RJ, Randleman JB, Stulting RD. Corneal ectasia after laser in situ keratomileusis in patients without apparent preoperative risk factors. Cornea. 2006;25(4):388–403. doi:10.1097/01.ico.0000222479.68242.77
10. Randleman JB, Caster AI, Banning CS, Stulting RD. Corneal ectasia after photorefractive keratectomy. J Cataract Refract Surg. 2006;32(8):1395–1398. doi:10.1016/j.jcrs.2006.02.078
11. Rodriguez LA, Guillen PB, Benavides MA, Garcia L, Porras D, Daqui-Garay RM. Penetrating keratoplasty versus intrastromal corneal ring segments to correct bilateral corneal ectasia: preliminary study. J Cataract Refract Surg. 2007;33(3):488–496. doi:10.1016/j.jcrs.2006.09.048
12. Bilgihan K, Ozdek SC, Sari A, Hasanreisoglu B. Excimer laser-assisted anterior lamellar keratoplasty for keratoconus, corneal problems after laser in situ keratomileusis, and corneal stromal opacities. J Cataract Refract Surg. 2006;32(8):1264–1269. doi:10.1016/j.jcrs.2006.02.056
13. Tan DT, Por YM. Current treatment options for corneal ectasia. Curr Opin Ophthalmol. 2007;18(4):284–289. doi:10.1097/ICU.0b013e3281a7ecaa
14. Chunyu T, Xiujun P, Zhengjun F, Xia Z, Feihu Z. Corneal collagen cross-linking in keratoconus: a systematic review and meta-analysis. Sci Rep. 2014;4:5652. doi:10.1038/srep05652
15. Sandvik GF, Thorsrud A, Raen M, Ostern AE, Saethre M, Drolsum L. Does corneal collagen cross-linking reduce the need for keratoplasties in patients with keratoconus? Cornea. 2015;34(9):991–995. doi:10.1097/ICO.0000000000000460
16. Yildirim A, Cakir H, Kara N, et al. Corneal collagen crosslinking for ectasia after laser in situ keratomileusis: long-term results. J Cataract Refract Surg. 2014;40(10):1591–1596. doi:10.1016/j.jcrs.2014.01.042
17. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135(5):620–627. doi:10.1016/s0002-9394(02)02220-1
18. Koller T, Mrochen M, Seiler T. Complication and failure rates after corneal crosslinking. J Cataract Refract Surg. 2009;35(8):1358–1362. doi:10.1016/j.jcrs.2009.03.035
19. Randleman JB. Ectasia after LASIK: new treatments, new hope. J Refract Surg. 2011;27(5):319. doi:10.3928/1081597X-20110412-01
20. Vinciguerra P, Albe E, Frueh BE, Trazza S, Epstein D. Two-year corneal cross-linking results in patients younger than 18 years with documented progressive keratoconus. Am J Ophthalmol. 2012;154(3):520–526. doi:10.1016/j.ajo.2012.03.020
21. Spadea L. Corneal collagen cross-linking with riboflavin and UVA irradiation in pellucid marginal degeneration. J Refract Surg. 2010;26(5):375–377. doi:10.3928/1081597X-20100114-03
22. Li Z, Jhanji V, Tao X, Yu H, Chen W, Mu G. Riboflavin/ultraviolet light-mediated crosslinking for fungal keratitis. Br J Ophthalmol. 2013;97(5):669–671. doi:10.1136/bjophthalmol-2012-302518
23. Gao XW, Zhao XD, Li WJ, Zhou X, Liu Y. Experimental study on the treatment of rabbit corneal melting after alkali burn with Collagen cross-linking. Int J Ophthalmol. 2012;5(2):147–150. doi:10.3980/j.issn.2222-3959.2012.02.06
24. Arora R, Manudhane A, Saran RK, Goyal J, Goyal G, Gupta D. Role of corneal collagen cross-linking in pseudophakic bullous keratopathy: a clinicopathological study. Ophthalmology. 2013;120(12):2413–2418. doi:10.1016/j.ophtha.2013.07.038
25. Rechichi M, Mazzotta C, Daya S, Mencucci R, Lanza M, Meduri A. Intraoperative OCT pachymetry in patients undergoing dextran-free riboflavin UVA accelerated corneal collagen crosslinking. Curr Eye Res. 2016;41(10):1310–1315. doi:10.3109/02713683.2015.1118130
26. Rechichi M, Mazzotta C, Oliverio GW, et al. Selective transepithelial ablation with simultaneous accelerated corneal crosslinking for corneal regularization of keratoconus: STARE-X protocol. J Cataract Refract Surg. 2021;47(11):1403–1410. doi:10.1097/j.jcrs.0000000000000640
27. Ng SM, Ren M, Lindsley KB, Hawkins BS, Kuo IC. Transepithelial versus epithelium-off corneal crosslinking for progressive keratoconus. Cochrane Database Syst Rev. 2021;3:CD013512. doi:10.1002/14651858.CD013512.pub2
28. Nath S, Shen C, Koziarz A, et al. Transepithelial versus epithelium-off corneal collagen cross-linking for corneal ectasia: a systematic review and meta-analysis. Ophthalmology. 2021;128(8):1150–1160. doi:10.1016/j.ophtha.2020.12.023
29. Arance-Gil A, Villa-Collar C, Perez-Sanchez B, Carracedo G, Gutierrez-Ortega R. Epithelium-Off vs. transepithelial corneal collagen crosslinking in progressive keratoconus: 3 years of follow-up. J Optom. 2021;14(2):189–198. doi:10.1016/j.optom.2020.07.005
30. Lim EWL, Lim L. Review of laser vision correction (LASIK, PRK and SMILE) with simultaneous accelerated corneal crosslinking - long-term results. Curr Eye Res. 2019;44(11):1171–1180. doi:10.1080/02713683.2019.1656749
31. Wallerstein A, Adiguzel E, Gauvin M, Mohammad-Shahi N, Cohen M. Under-flap stromal bed CXL for early post-LASIK ectasia: a novel treatment technique. Clin Ophthalmol. 2017;11:1–8. doi:10.2147/OPTH.S118831
32. El-Khoury S, Abdelmassih Y, Amro M, Chelala E, Jarade E. Under-the-flap crosslinking and LASIK in early ectasia with hyperopic refractive error. J Ophthalmol. 2018;2018:4342984. doi:10.1155/2018/4342984
33. Eleftheriadis H, Prandi B, Diaz-Rato A, Morcillo M, Sabater JB. The effect of flap thickness on the visual and refractive outcome of myopic laser in situ keratomileusis. Eye. 2005;19(12):1290–1296. doi:10.1038/sj.eye.6701775
34. Zhang H, Roozbahani M, Piccinini AL, Hafezi F, Scarcelli G, Randleman JB. Brillouin microscopic depth-dependent analysis of corneal crosslinking performed over or under the LASIK flap. J Cataract Refract Surg. 2020;46(11):1543–1547. doi:10.1097/j.jcrs.0000000000000294
35. Sorkin N, Varssano D. Corneal collagen crosslinking: a systematic review. Ophthalmologica. 2014;232(1):10–27. doi:10.1159/000357979
36. Hersh PS, Stulting RD, Muller D, Durrie DS, Rajpal RK. U.S. multicenter clinical trial of corneal collagen crosslinking for treatment of corneal ectasia after refractive surgery. Ophthalmology. 2017;124(10):1475–1484. doi:10.1016/j.ophtha.2017.05.036
37. Sharif W, Ali ZR, Sharif K. Long term efficacy and stability of corneal collagen cross linking for post-LASIK ectasia: an average of 80mo follow-up. Int J Ophthalmol. 2019;12(2):333–337. doi:10.18240/ijo.2019.02.22
38. Tong JY, Viswanathan D, Hodge C, Sutton G, Chan C, Males JJ. Corneal collagen crosslinking for post-LASIK ectasia: an Australian study. Asia Pac J Ophthalmol. 2017;6(3):228–232. doi:10.22608/APO.2016197
39. Marino GK, Torricelli AA, Giacomin N, Santhiago MR, Espindola R, Netto MV. Accelerated corneal collagen cross-linking for postoperative LASIK ectasia: two-year outcomes. J Refract Surg. 2015;31(6):380–384. doi:10.3928/1081597X-20150521-04
40. Hersh PS, Greenstein SA, Fry KL. Corneal collagen crosslinking for keratoconus and corneal ectasia: one-year results. J Cataract Refract Surg. 2011;37(1):149–160. doi:10.1016/j.jcrs.2010.07.030
41. Vinciguerra P, Camesasca FI, Albe E, Trazza S. Corneal collagen cross-linking for ectasia after excimer laser refractive surgery: 1-year results. J Refract Surg. 2010;26(7):486–497. doi:10.3928/1081597X-20090910-02
42. Poli M, Lefevre A, Auxenfans C, Burillon C. Corneal collagen cross-linking for the treatment of progressive corneal ectasia: 6-year prospective outcome in a French population. Am J Ophthalmol. 2015;160(4):654–662 e1. doi:10.1016/j.ajo.2015.06.027
43. Mazzotta C, Caporossi T, Denaro R, et al. Morphological and functional correlations in riboflavin UV A corneal collagen cross-linking for keratoconus. Acta Ophthalmol. 2012;90(3):259–265. doi:10.1111/j.1755-3768.2010.01890.x
44. Li G, Fan ZJ, Peng XJ. Corneal collagen crosslinking for corneal ectasia of post-LASIK: one-year results. Int J Ophthalmol. 2012;5(2):190–195. doi:10.3980/j.issn.2222-3959.2012.02.15
45. Wollensak G, Wilsch M, Spoerl E, Seiler T. Collagen fiber diameter in the rabbit cornea after collagen crosslinking by riboflavin/UVA. Cornea. 2004;23(5):503–507. doi:10.1097/01.ico.0000105827.85025.7f
46. Greenstein SA, Shah VP, Fry KL, Hersh PS. Corneal thickness changes after corneal collagen crosslinking for keratoconus and corneal ectasia: one-year results. J Cataract Refract Surg. 2011;37(4):691–700. doi:10.1016/j.jcrs.2010.10.052
47. Caporossi A, Mazzotta C, Baiocchi S, Caporossi T. Long-term results of riboflavin ultraviolet a corneal collagen cross-linking for keratoconus in Italy: the Siena eye cross study. Am J Ophthalmol. 2010;149(4):585–593. doi:10.1016/j.ajo.2009.10.021
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Photorefractive Keratectomy Enhancement (PRK) After Small-Incision Lenticule Extraction (SMILE)
Moshirfar M, Parsons MT, Chartrand NA, Lau CK, Stapley S, Bundogji N, Ronquillo YC, Hoopes PC
Clinical Ophthalmology 2022, 16:3033-3042
Published Date: 12 September 2022
The Combined Utilization of Epithelial Thickness Mapping and Tomography in Keratorefractive Surgery Screening: One Imaging Modality is Not Sufficient
Corbin WM, Payne CJ, Momeni-Moghaddam H, Ronquillo YC, Hoopes Snr PC, Moshirfar M
Clinical Ophthalmology 2023, 17:1457-1463
Published Date: 24 May 2023
Visual Outcomes of a Second-Generation, Enhanced UV Protected Light Adjustable Lens in Cataract Patients with Previous LASIK and/or PRK
Wong JR, Folden DV, Wandling GR, Schaefer S, Stephens J, Boots C, Nichols CJ, Everson MH, Johnson R
Clinical Ophthalmology 2023, 17:3379-3387
Published Date: 6 November 2023