Back to Journals » Clinical Ophthalmology » Volume 17
Visual Outcomes of a Second-Generation, Enhanced UV Protected Light Adjustable Lens in Cataract Patients with Previous LASIK and/or PRK
Authors Wong JR, Folden DV ![]() , Wandling GR, Schaefer S, Stephens J, Boots C, Nichols CJ, Everson MH, Johnson R
, Wandling GR, Schaefer S, Stephens J, Boots C, Nichols CJ, Everson MH, Johnson R
Received 1 September 2023
Accepted for publication 29 October 2023
Published 6 November 2023 Volume 2023:17 Pages 3379—3387
DOI https://doi.org/10.2147/OPTH.S432457
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jennifer R Wong,1,* David V Folden,2,3,* George R Wandling,2,3 Scott Schaefer,2,4 Jeff Stephens,2,4 Calvin Boots,1,2 Carter J Nichols,2,4 Marshall H Everson,2,4 Ryan Johnson2,4
1Praxis Vision, Edina, MN, USA; 2Twin Cities Eye Consultants, Edina, MN, USA; 3North Suburban Eye Specialists, Coon Rapids, MN, USA; 4Edina Eye Physicians & Surgeons, Edina, MN, USA
*These authors contributed equally to this work
Correspondence: David V Folden Department of Cataract & Refractive Surgery, Twin Cities Eye Consultants, 3777 Coon Rapids Blvd NW, Coon Rapids, MN, 55433, USA, Tel +1 763-421-7420, Fax +1 763-421-0730, Email [email protected]
Purpose: To report on the visual outcomes of the second-generation (ActivShieldTM) Light Adjustable Lens (LAL) used in cataract surgery for patients with a history of laser refractive surgery (LASIK and/or photorefractive keratectomy [PRK]) using a co-managed, open-access methodology.
Patients and Methods: This retrospective case series of consecutive patients with history of laser refractive surgery implanted with the second-generation LAL with an emmetropic target were included in the study. Following surgery, all patients received their ultraviolet (UV) light treatments at a separate open-access facility through a co-managed arrangement. Uncorrected distance visual acuity (UDVA), spherical equivalent (SE), and residual cylinder for eyes with an emmetropic refractive target were the primary outcome measures as documented at the patient’s final, stable, refractive postoperative exam.
Results: Thirty-three patients (34 eyes) with a history of laser refractive surgery were included in the study and implanted with the second-generation LAL with a postoperative emmetropic refractive target. Twenty-eight (82.4%) saw 20/20 or better and 9 (26.5%) saw 20/15 or better. The mean SE was 0.01 ± 0.31 D and 33 (97.1%) were within ± 0.50 D SE of plano. The mean residual cylinder was − 0.28 ± 0.32 D and 30 (88.2%) were within ± 0.50 D.
Conclusion: Use of the second-generation LAL was efficacious in cataract surgical patients with a history of LASIK and/or PRK using a co-managed, open-access methodology.
Keywords: ActivShieldTM, light adjustable lens, LAL, cataract surgery, refractive surgery, LASIK, PRK
Introduction
The Light Adjustable Lens (LAL; RxSight, Inc.) is an intraocular lens (IOL) that provides noninvasive postoperative adjustment to the lens power, correcting both residual spherical and cylindrical refractive errors after cataract surgery. The LAL power is adjusted with a spatially profiled ultraviolet (UV) light beam using a Light Delivery Device (LDD) in the weeks following IOL implantation and refractive stabilization.1,2 The LDD facilitates changes in the curvature and power of the LAL by exposing special photosensitive macromers in the IOL to UV radiation (365 nm). Macromers in the irradiation zone are polymerized, and a concentration gradient is formed. Unexposed macromers migrate down the gradient, physically changing the shape and power of the LAL to achieve the patient’s refractive target. Up to 3 D of spherocylindrical refractive change is possible.3 Once refractive stability is secured and the patient’s refractive goals are achieved, the LAL receives two refractively neutral lock-in treatments to the remaining macromers preventing any further refractive changes to the LAL. Refractive adjustments typically begin 3 weeks postoperatively and are completed 5–6 weeks postoperatively but can vary depending on the postoperative refractive stabilization of each individual patient. Final refractive adjustments and lock-in are delayed until refractive stability is confirmed. Patients wear RxSight UV protective glasses until 24 hours after the last lock-in to help prevent uncontrolled refractive changes to the LAL from ambient environmental UV light.
A second-generation LAL was approved in 2021 and incorporates an enhanced UV absorber (ActivShieldTM) providing added protection against ambient environmental UV light exposure.4 This feature may aid in extending final treatments and lock-in, ensuring refractive stability and outcomes, with less concern for the detrimental effects of environmental UV light exposure.
Patients with a history of laser refractive surgery (LASIK and/or photorefractive keratectomy [PRK]) have an altered anterior and posterior corneal surface relationship, which poses challenges to preoperative biometry, IOL calculations, and postoperative refractive error largely through altered predictability of effective lens position (ELP) following cataract surgery.5–7 Because the LAL can be adjusted to neutralize refractive error following cataract surgery, it provides a refractive advantage in this postrefractive patient population by mitigating the effects of refractive surprise. Two previous peer-reviewed studies have reported visual outcomes that included the first commercially available LAL on post-myopic laser refractive surgery eyes.8,9 Folden and Wong reported the first visual outcomes of the second-generation LAL, including a cohort of 20 postrefractive patients, many of which were highly complex with combinations of LASIK, PRK, RK, and/or limbal relaxing incisions (LRIs) but did not stratify specifically for the most commonly encountered laser refractive surgeries, including LASIK and PRK.10
Although previous studies have reported outcomes implanting LAL in patients with a history of corneal refractive surgery, a clinical study has yet to be published on post-laser refractive surgery patients receiving exclusively the second-generation LAL. The aim of this study is to report on the visual outcomes of the second-generation LAL in patients with a history of LASIK and/or PRK. To our knowledge, this is the first report of its kind in the peer-reviewed literature.
Patients and Methods
Study Design and Participants
This retrospective case series evaluated the visual outcomes of a consecutive series of post-LASIK and/or PRK patients from 5 surgeons within a single private practice setting after cataract extraction and IOL implantation with a second-generation Light Adjustable Lens (ActivShieldTM LAL; RxSight, Inc.) between July 2021 and April 2022. No patient-specific data was used in the analysis, and all patients were de-identified. The study was registered with the International Standard Randomized Controlled Trial Number Registry (ISRCTN 57719133) and approved by an institutional review board (SALUS IRB, Austin, TX). This study was performed in accordance with the tenets of the Declaration of Helsinki. Requirement for written consent was waived by the IRB due to the study’s retrospective design.
Inclusion criteria included patients with a history of myopic or hyperopic LASIK and/or PRK undergoing cataract surgery and choosing the second-generation (ActivShieldTM) LAL with an emmetropic goal (±0.25 D) and a minimum dilated pupil diameter of 6.5 mm. Exclusion criteria included eyes with a myopic refractive target for monovision, prior history of radial keratotomy (RK) or automated lamellar keratoplasty (ALK), 1 line of reduced Snellen corrected distance visual acuity (CDVA) related to amblyopia, macular/corneal pathology, or other diseases limiting visual acuity, and lacking visual outcome data of at least 3 months postoperatively. Intraoperative complications were not considered as an exclusion criterion unless it was felt to limit the visual outcome.
Surgeries were performed by 5 surgeons at 2 ambulatory surgery centers (ASCs) in Blaine and Edina, Minnesota. All UV light treatments were performed by 2 physicians (LDD Specialists) in Edina, Minnesota, using a co-managed arrangement at an open-access facility as previously described.10
All patients had a comprehensive preoperative ophthalmic examination prior to their cataract surgery. Biometry was achieved using an IOLMaster 500, Lenstar, or Pentacam AXL. Topographic imaging was obtained using Pentacam HR/AXL or Galilei G4 for all patients. The Post-Refractive IOL Calculator at American Society of Cataract and Refractive Surgery (ASCRS) was used to calculate IOL powers with emphasis on the Barrett True K and Barrett True K (No History) formulas.
The primary outcome measures for this study were monocular uncorrected distance visual acuity (UDVA), monocular mean spherical equivalent (SE), and monocular mean residual cylinder for eyes with an emmetropic target at the patients’ final, stable, refractive postoperative exam.
Surgical Technique and LDD Adjustments
All surgeries were performed with topical anesthesia using a 2.4 mm clear corneal, self-sealing temporal incision and widened to 2.8–3.0 mm for LAL implantation. All patients received the second-generation LAL.
Approximately three weeks following cataract surgery when refractive stabilization was confirmed, patients underwent their first LDD treatment to adjust the LAL power with a refractive target of plano. Up to three LDD refractive adjustments were performed followed by two final lock-in treatments, ending around the 5–6 week postoperative period averaging 41.1 days [range 24–90 days]. Light treatments were separated by at least 72 hours. Although this study was unable to track compliance, patients were instructed to wear RxSight UV protective glasses from the time of lens implantation until 24 hours after the last lock-in treatment was completed.
Final postsurgical exams included manifest refraction (MRx) with CDVA and UDVA. A standard phoropter was used to determine the subjective MRx rounding in steps of 0.25 D, using a computer calibrated Snellen chart for Visual Acuity (VA) testing under photopic conditions.
Results
Sixty-nine eyes from the medical records of 40 consecutive patients were evaluated. Thirty-five eyes were excluded from the study and data analysis for the following reasons: twenty-eight eyes had a myopic monovision refractive goal, 4 eyes had limited CDVA from macular pathology, and 3 eyes of 3 patients were lost to follow-up or unwilling to return for postoperative examination of at least 3 month duration. Thirty-four eyes from 33 patients with a mean age of 63.5 ± 6.4 years [range: 52.2, 75.3] were implanted with the second-generation LAL with a pseudophakic emmetropic target and were included in the analysis.
One intraoperative complication required sulcus placement and optic capture of the LAL but did not require vitrectomy or result in loss of CDVA and was included in the data set. One patient required a PRK refractive enhancement, but their pre-PRK visual outcome data was used in the analysis. Six (17.6%) eyes required a YAG posterior capsulotomy with post-YAG visual outcome data used in the analysis. One patient lost 1 line of BCVA that was likely related to the patient’s untreated posterior capsule opacification (PCO) at their final refractive postoperative exam. No adverse effects from the LAL or LDD treatments were noted.
Table 1 shows patient demographics as well as previous laser refractive surgery and LDD refractive adjustment profiles. Data was evaluated at a final, stable, postoperative refractive examination averaging 137.0 ± 71.1 [90, 371], which averages 95.9 ± 69.8 days from final lock-in treatment. The average number of refractive adjustments was 1.5 ± 0.6. Table 2 shows the postsurgical LDD treatments corrected a mean SE of 0.38 ± 0.39 D [−0.38, 1.25] and mean cylinder of −0.38 ± 0.39 D [−1.50, 0.00] with a refractive target of plano.
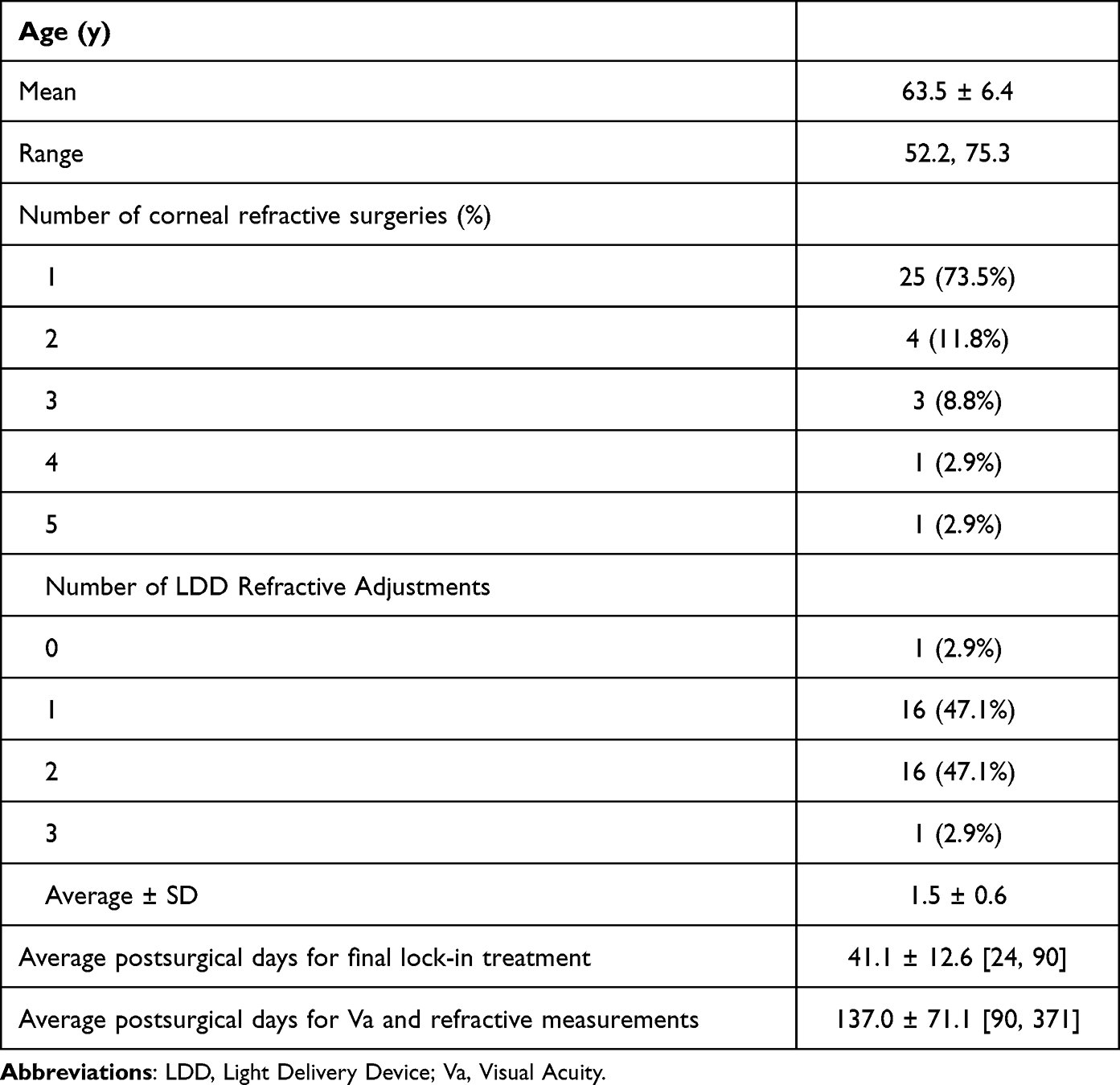 |
Table 1 Patient Demographics, Refractive History, and LDD Refractive Adjustment Profiles |
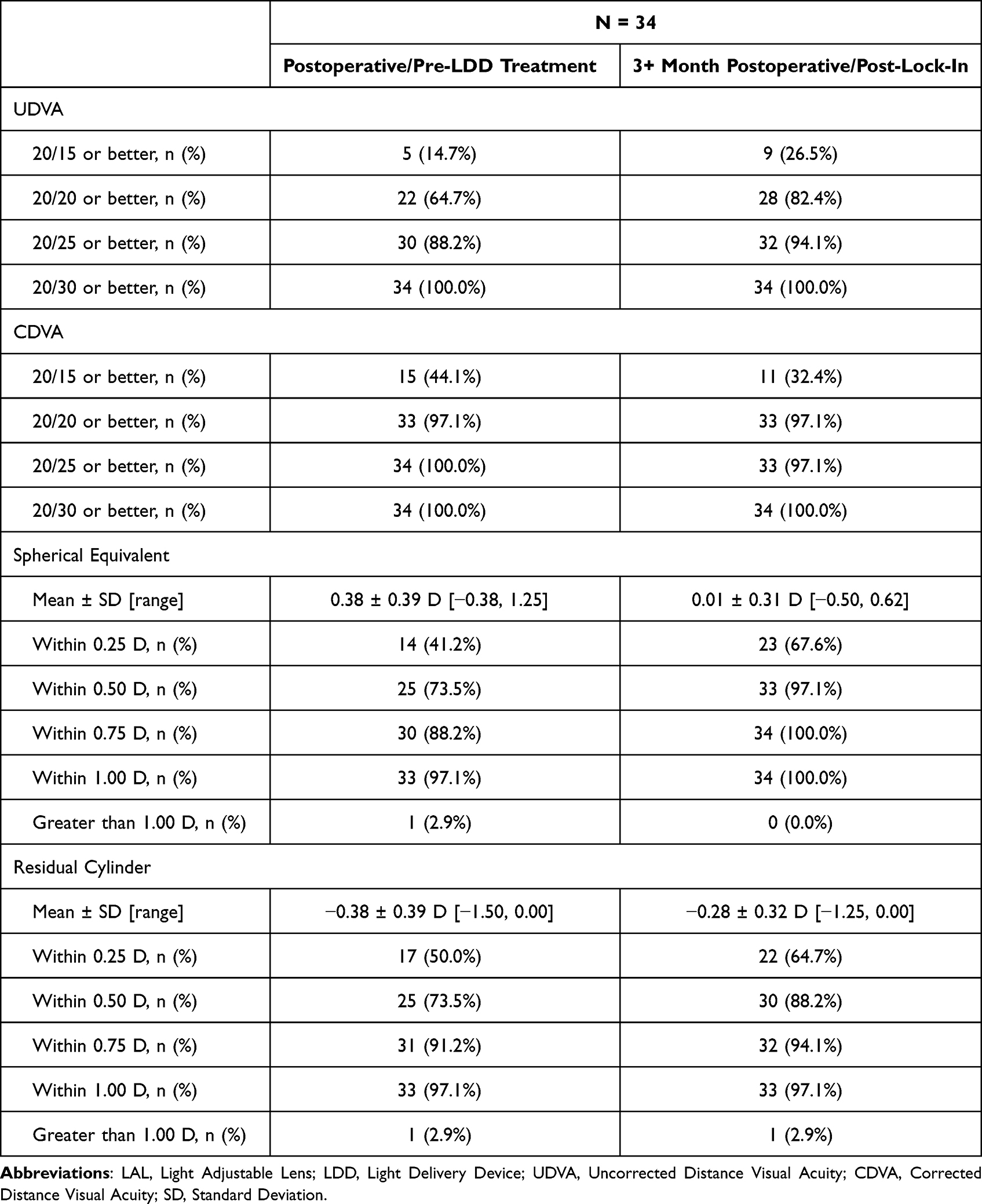 |
Table 2 Postrefractive LAL Visual Outcomes with a Pseudophakic Emmetropic Target |
At the final postoperative examination, UDVA was 20/20 or better in 82.4% (28/34), and 20/15 or better in 26.5% (9/34) with a mean SE of 0.01 ± 0.31 D [−0.50, 0.62] and mean cylinder of −0.28 ± 0.32 D [−1.25, 0.00 D]. Following all postoperative LDD refractive adjustments and final lock-in treatment, LAL patients experienced good CDVA and UDVA and a low level of residual refractive error, as shown in Table 2 and Figures 1–4. Table 2 shows a comparison of postoperative/pre-LDD treatment with final post-lock-in refractive and VA outcomes. Eyes achieving residual SE and cylinder measurements within 0.5 D improved from 19 (55.9%) pre-LDD refractive adjustments to 28 (82.4%) at the 3+ month postoperative/post-lock-in exam using a two-sample t-Test (p = 0.017). Figures 1 and 2 show a comparison of both UDVA and CDVA at the final postoperative/post-lock-in exam. Figures 3 and 4 show residual SE and residual cylinder, respectively, at the final postoperative/post-lock-in exam.
 |
Figure 1 Cumulative Snellen Visual Acuity (20/x or better) at 3+ Month Postoperative/Post-LDD Lock-In. Abbreviation: LDD, Light Delivery Device. |
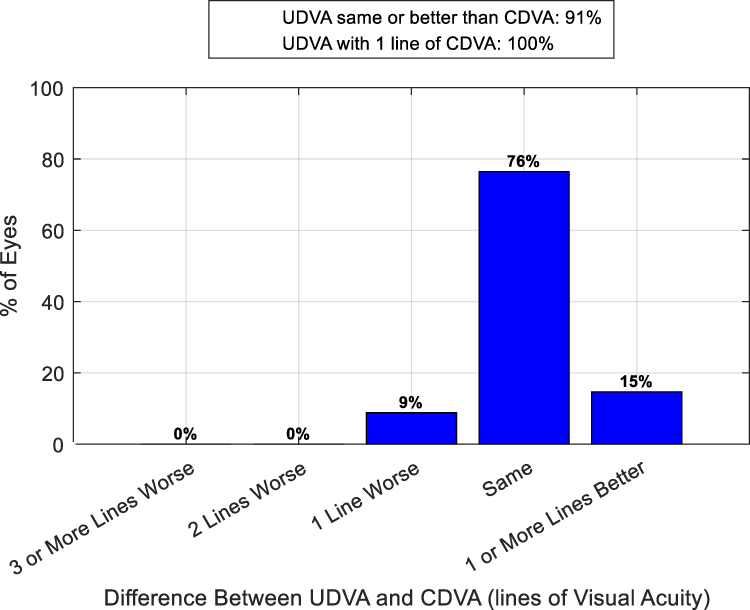 |
Figure 2 Difference between UDVA and CDVA (Snellen Lines) at 3+ Month Postoperative/Post-LDD Lock-In. Abbreviation: LDD, Light Delivery Device. |
 |
Figure 3 Postoperative Spherical Equivalent Refraction (D) at 3+ Month Postoperative/Post-LDD Lock-In. Abbreviation: LDD, Light Delivery Device. |
 |
Figure 4 Postoperative Refractive Cylinder (D) at 3+ Month Postoperative/Post-LDD Lock-In. Abbreviation: LDD, Light Delivery Device. |
Table 3 compares the refractive accuracy when correcting residual postsurgical hyperopic, myopic, and neutral/zero SE outcomes with LDD refractive treatments. There was no statistically significant difference among the treatments.
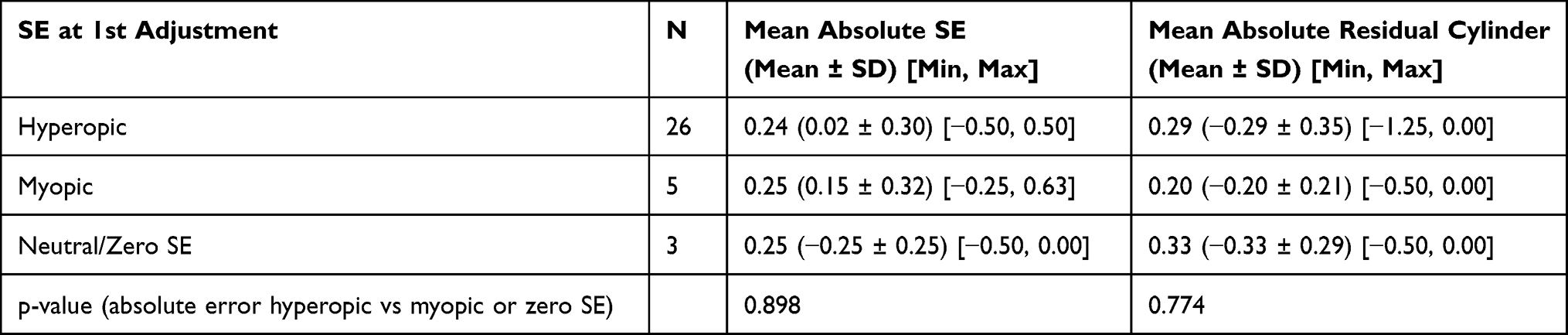 |
Table 3 3+ Month Postoperative/Post-Lock-in SE and Residual Cylinder for Hyperopic, Myopic, and Neutral/Zero SE LDD Treatments |
Discussion
Eyes with a history of corneal refractive surgery have altered corneal refractive power, decreasing the accuracy of biometric imaging, IOL power calculations, and the predictability of ELP following cataract surgery. The result is an increase in postoperative refractive error and reduced UCVA.7 Use of the LAL in patients with previous corneal refractive surgery minimizes postoperative refractive error and increases UCVA.8–12
Patients with a history of laser refractive surgery (LASIK and/or PRK) receiving a nonadjustable IOL in cataract surgery have been widely reported. When using all ASCRS calculator formulas, Wang and Koch found that the average value for accuracy was within ±0.5 D in 45% to 72% for myopic LASIK/PRK and 47.6% to 66.7% for hyperopic LASIK/PRK.7 More recently, Ferguson et al reported 71.9% of eyes within ±0.5 D for post-myopic LASIK/PRK and 70.2% within ±0.5 D for hyperopic LASIK/PRK. Their mean IOL prediction error range was −1.62, 1.90 (myopic correction) and −2.77, 1.76 (hyperopic correction) with 13% of cases resulting in an IOL prediction error exceeding 1 D.13 These studies highlight refractive outliers remain problematic when using nonadjustable IOLs in post-laser refractive surgical eyes.
Patients with a history of laser refractive surgery receiving LAL in cataract surgery have also been reported.8–10 These reports, however, included patients receiving the first-generation (non-ActivShieldTM) LAL or did not specifically stratify for post-laser refractive surgical outcomes using the second-generation (ActivShieldTM) LAL. Brierley first reported outcomes using the first-generation LAL in postrefractive patients. Ninety-seven percent of 34 eyes were within ±0.50 D of target. Only 20 of the 34 eyes had an emmetropic goal of which 65% (13/20) had an UDVA of 20/20.8 Moshirfar et al reported 55% of 36 eyes were within ±0.50 D of target and 31% had UDVA of 20/20.9 Both Brierley and Moshirfar et al reported only on patients that had previous myopic laser refractive surgery.8,9 Folden and Wong first reported on the visual outcomes of the second-generation LAL. Their study included a small cohort of 20 postrefractive patients, many of which had combinations of LASIK, PRK, RK, and/or limbal relaxing incisions (LRIs) but did not stratify specifically for post-laser refractive surgical patients. They reported that 100% of their postrefractive eyes were within ±0.50 D SE of plano and 95% saw 20/20 or better.10
The current study is the first report on the exclusive use of the second-generation LAL used in patients with a history of laser refractive surgery and included both myopic or hyperopic LASIK and/or PRK. Uncorrected distance visual acuity was 20/20 or better in 82.4% (28/34) and 97.1% (33/34) were within ±0.50 D of target. Stratifying visual outcome data based on previous myopic versus hyperopic laser refractive surgery could not be completed since details of patients’ corneal refractive surgeries could not be confirmed for most patients. Topographically, corneal refractive treatments can be estimated but not confirmed. Moreover, many patients had multiple procedures which may have included both myopic and hyperopic correction for residual under- or over-corrected refractive error of the original treatment. Previous LASIK/PRK treatments were only estimated when using the Post-Refractive IOL Calculator at ASCRS.
Interestingly, Figure 2 shows 15% of eyes had an improvement of 1 line or better UDVA compared with CDVA. A high percentage of eyes in this study had low residual SE and cylinder. Patients with low/negligible refractive error may have recognized reduced visual quality by looking through the optical media of net neutral/zero SE phoropter lenses versus their uncorrected state. Additionally, statistical noise related to normal variability in patient responses during visual acuity testing and less “push” on the Snellen chart once the MRx was achieved may have all contributed to this statistic.
Twenty-eight of 33 (84.8%) patients in this study chose a binocular monovision refractive goal with the LAL and had some degree of myopic defocus in their non-dominant eye (≥0.50 D). Targeting a myopic goal in the patients’ reading eye was a fluid process during LDD treatments and customized based on patient feedback throughout the postoperative period. Additionally, uncorrected near visual acuity (UCNVA) was not performed at a standardized distance but was held at the patient’s preferred reading distance and adjusted accordingly with LDD treatment. Because of the non-standardized and subjective nature of near vision testing, the authors contend that eyes with an emmetropic goal in this study provided the clearest analysis on the refractive accuracy of the LAL.
Six (17.6%) eyes required a YAG capsulotomy. This may have occurred early with subtle PCO during the LDD treatments if it was thought to impact refractive measurements and subsequent LDD correction. This was performed to encourage refractive stability and improve the accuracy of postsurgical measurements, LDD treatments, and long-term visual outcomes. Additionally, 84.8% of patients chose a binocular monovision refractive goal and may have required early YAG capsulotomy in their emmetropic eye to maximize the visual quality of their refractive state.
Although the final refractive postoperative/post-lock-in mean SE and residual cylinder values were low, refractive outliers can still occur with the LAL as demonstrated in Table 2 and Figures 3 and 4. Postrefractive patients have longer and shorter axial lengths that could impact the rate at which final effective lens positioning and complete refractive stabilization occurs. Consideration for further delaying final LDD treatments in postrefractive patients could be considered to help eliminate refractive outliers. Additionally, corneal effects related to prior laser refractive surgery, including alterations in corneal asphericity, higher order aberrations, and corneal clarity, could potentially impact LDD treatment profiles and final refractive outcomes. Limitations of the study include the lack of a well-defined end point for final postoperative refractive and VA measurements. Most patients had a scheduled 3-month postoperative examination. However, some patients were initially lost to follow-up, rescheduled for a later date, had additional refractive postoperative exams, and/or required management of posterior capsule opacification (PCO) beyond their scheduled 3-month postoperative exam. Data from their most complete refractive postoperative examination of longest postoperative duration were used for the analysis.
This study evaluated the outcomes of patients with history of laser refractive surgery receiving the second-generation LAL, which provides redundant UV absorption via ActivShieldTM, better protecting the IOL from the unpredictable refractive effects of environmental UV light.4 This study also highlights a co-managed, open-access methodology from multiple surgeons and LDD specialists. While LAL offers clear pseudophakic refractive advantages for patients with previous history of laser refractive surgery, the additional postoperative visits required for LDD treatment are time consuming and can pose a logistical challenge to the surgeon’s schedule. A co-managed arrangement allows the surgeon to maintain focus on their surgical role and an LDD Specialist to focus solely on the skills necessary for performing LDD treatments and achieving the patient’s refractive goals. An open-access arrangement allows an LDD Specialist to work with multiple surgeons, streamlining their workflow and increasing their experience and expertise. We propose that a co-managed, open-access methodology fosters proficiency and when combined with the second-generation LAL may contribute to improved refractive outcomes.
Conclusion
Patients with history of corneal refractive surgery have altered corneal refractive power resulting in an increase in postoperative refractive error and reduced UCVA following cataract surgery. Use of the second-generation (ActivShieldTM) LAL was efficacious in cataract surgical patients with a history of LASIK and/or PRK using a co-managed, open-access methodology.
Acknowledgments
We thank Hannah Schoenecker for her data collection, organization, and analysis and Terri Flom for providing research guidance.
Funding
No public or private support was provided for this study.
Disclosure
Jennifer R. Wong, OD is a paid consultant for RxSight.
No other authors report any financial or proprietary interests.
References
1. Schwartz DM. Light-adjustable lens. Trans Am Ophthalmol Soc. 2003;101:417–436.
2. Schwartz DM, Sandstedt CA, Chang SH, Kornfield JA, Grubbs RH. Light-adjustable lens: development of in vitro nomograms. Trans Am Ophthalmol Soc. 2004;102:
3. Dick HB, Gerste RD. Future intraocular lens technologies. Ophthalmology. 2021;128(11):e206–e213. doi:10.1016/j.ophtha.2020.12.025
4. RxSight® PMA P160055; S015: change Design/Components/Specifications/Material. 2021.
5. Diehl JW, Yu F, Olson MD, Moral JN, Miller KM. Intraocular lens power adjustment nomogram after laser in situ keratomileusis. J Cataract Refract Surg. 2009;35(9):1587–1590. doi:10.1016/j.jcrs.2009.04.038
6. Norrby S. Sources of error in intraocular lens power calculation. J Cataract Refract Surg. 2008;34(3):368–376. doi:10.1016/j.jcrs.2007.10.031
7. Wang L, Koch DD. Intraocular lens power calculations in eyes with previous corneal refractive surgery: review and expert opinion. Ophthalmology. 2021;128(11):e121–e131. doi:10.1016/j.ophtha.2020.06.054
8. Brierley L. Refractive results after implantation of a light-adjustable intraocular lens in postrefractive surgery cataract patients. Ophthalmology. 2013;120(10):1968–1972. doi:10.1016/j.ophtha.2013.03.010
9. Moshirfar M, Henrie MK, Payne CK, Hansen AM, Ronquillo YC, Hoopes PC. Comparing visual outcomes of light adjustable intraocular lenses in patients with and without prior history of corneal refractive surgery. J Refract Surg. 2023;39(5):311–318. doi:10.3928/1081597X-20230222-01
10. Folden DV, Wong JR. Visual outcomes of an enhanced UV protected light adjustable lens using a novel co-managed, open-access methodology. Clin Ophthalmol. 2022;16:2413–2420.
11. Moshirfar M, Duong AA, Shmunes KM, Castillo-Ronquillo YS, Hoopes PC. Light adjustable intraocular lens for cataract surgery after radial keratotomy. J Refract Surg. 2020;36(12):852–854. doi:10.3928/1081597X-20201002-01
12. Rocha G, Mednick ZD. Light-adjustable intraocular lens in post-LASIK and post-traumatic cataract patient. J Cataract Refract Surg. 2012;38(6):1101–1104. doi:10.1016/j.jcrs.2012.03.017
13. Ferguson TJ, Downes RA, Randleman JB. IOL power calculations after LASIK or PRK: Barrett True-K biometer-only calculation strategy yields equivalent outcomes as a multiple formula approach. J Cataract Refract Surg. 2022;48(7):784–789. doi:10.1097/j.jcrs.0000000000000883
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Three Tonometers in Measuring Intraocular Pressure in Eyes That Underwent Myopic Laser in situ Keratomileusis and Photorefractive Keratectomy
Ang RET, Bargas NVR, Martinez GHA, Sosuan GMN, Nabor-Umali MI
Clinical Ophthalmology 2022, 16:1623-1637
Published Date: 27 May 2022
Visual and Topographic Outcomes of Corneal Collagen Cross Linking for Post LASIK Ectasia
Nasef MH, El Emam SY, Haleem TI, Shalaby WS, Allam WA
Clinical Ophthalmology 2022, 16:2025-2032
Published Date: 20 June 2022
Photorefractive Keratectomy Enhancement (PRK) After Small-Incision Lenticule Extraction (SMILE)
Moshirfar M, Parsons MT, Chartrand NA, Lau CK, Stapley S, Bundogji N, Ronquillo YC, Hoopes PC
Clinical Ophthalmology 2022, 16:3033-3042
Published Date: 12 September 2022
Quality of Vision After LASIK, PRK and FemtoLASIK: An Analysis Using the Double Pass Imaging System HD AnalyzerTM®
Vieira R, Marta A, Abreu AC, Monteiro S, Brochado MDC
Clinical Ophthalmology 2022, 16:3351-3359
Published Date: 10 October 2022
The Combined Utilization of Epithelial Thickness Mapping and Tomography in Keratorefractive Surgery Screening: One Imaging Modality is Not Sufficient
Corbin WM, Payne CJ, Momeni-Moghaddam H, Ronquillo YC, Hoopes Snr PC, Moshirfar M
Clinical Ophthalmology 2023, 17:1457-1463
Published Date: 24 May 2023