Back to Journals » Clinical Ophthalmology » Volume 20
Visual and Patient-Reported Outcomes of a Non-Diffractive Extended Depth-of-Focus Intraocular Lens with Micro-Monovision in Eyes with Early Macular Pathology
Authors Demircan E ![]() , Rabinovitch D, Ahmed IIK
, Rabinovitch D, Ahmed IIK ![]() , Varma DK
, Varma DK
Received 18 April 2026
Accepted for publication 18 June 2026
Published 14 July 2026 Volume 2026:20 618031
DOI https://doi.org/10.2147/OPTH.S618031
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Elif Demircan,1 David Rabinovitch,1 Iqbal Ike K Ahmed,1– 4 Devesh K Varma1,3,4
1Prism Eye Institute, Oakville, ON, Canada; 2John A. Moran Eye Center, University of Utah, Salt Lake, UT, USA; 3Institute for Better Health, Trillium Health Partners, Mississauga, ON, Canada; 4Department of Ophthalmology & Vision Sciences, University of Toronto, Toronto, ON, Canada
Correspondence: Elif Demircan, Prism Eye Institute, 2201 Bristol Circle, Suite 100, Oakville, ON, L6H 0J8, Canada, Email [email protected]
Purpose: To evaluate visual and patient-reported outcomes after bilateral implantation of a non-diffractive extended depth of focus (EDOF) IOL (AcrySof IQ Vivity, Alcon) in patients with early macular pathology.
Design: Single-site, prospective, non-comparative pilot cohort study.
Patients and Methods: The study included 20 patients (40 eyes) undergoing bilateral cataract surgery with at least one eye with early-stage macular pathology, specifically age-related macular degeneration (AREDS category 2) or epiretinal membrane (stage 0). All patients received bilateral implantation of the non-diffractive EDOF IOL targeted for micro-monovision. Primary outcomes were monocular corrected distance visual acuity (CDVA) and distance-corrected intermediate visual acuity (DCIVA) at 3 months. Secondary outcomes included binocular CDVA, DCIVA, and distance-corrected near visual acuity (DCNVA); uncorrected distance, intermediate and near visual acuity (UDVA, UIVA, UNVA); refractive outcomes; contrast sensitivity and patient-reported outcomes, including satisfaction and visual disturbances.
Results: At 3 months, median (IQR) monocular CDVA, DCIVA, and DCNVA were 0.00 (0.00– 0.10), 0.18 (0.08– 0.28), and 0.40 (0.30– 0.50) logMAR, respectively. Binocular CDVA, DCIVA, and DCNVA were 0.00 (0.00– 0.00), 0.13 (0.08– 0.18), and 0.35 (0.22– 0.40). Binocular UDVA, UIVA, and UNVA were 0.00 (0.00– 0.00), 0.08 (− 0.01– 0.11), and 0.30 (0.20– 0.33) logMAR, respectively. 90% of dominant and 95% of non-dominant eyes were within ± 0.50 D of the intended outcome. Photopic contrast sensitivity was within normal range, while mesopic values were near the lower end of normal. Most patients (90%) were satisfied with their vision. Visual disturbances were low in frequency, severity, and bothersomeness, with median Rasch-calibrated scores of 32, 27, and 29, respectively.
Conclusion: In patients with early macular pathology, bilateral implantation of a non-diffractive EDOF IOL demonstrated promising distance and intermediate vision, favorable near visual outcomes, and high patient satisfaction with minimal visual disturbances. Larger, prospective, comparative studies are warranted to define candidacy for patients with macular pathology.
Keywords: cataract, intraocular lens, extended depth-of-focus, epiretinal membrane, age-related macular degeneration, micro-monovision
Introduction
With advancements in intraocular lens (IOL) technology, patient expectations for post-surgical visual quality have increased, and ophthalmologists are increasingly able to meet these demands.1 However, cataract surgery in patients with concurrent retinal pathology requires careful consideration and preoperative planning.
Diffractive multifocal (MF) IOLs improve range of vision by dividing light into different foci, reducing spectacle dependence, but they can cause visual disturbances and reduced contrast sensitivity.2 Patients with macula-affecting conditions such as age-related macular degeneration (AMD) and epiretinal membrane (ERM) often have reduced visual capabilities and contrast sensitivity at baseline and may also experience metamorphopsia and other visual disturbances that negatively affect visual quality. Diffractive MF IOLs can further exacerbate these issues, and their use is considered relatively contraindicated in patients with retinal diseases.3–8
Extended Depth of Focus (EDOF) IOLs are designed to enhance depth of focus while reducing unwanted visual aberrations compared to MF IOLs.9–11 The AcrySof IQ Vivity IOL (Alcon) is a non-diffractive EDOF lens that aims to provide distance, intermediate, and functional near vision with minimal visual disturbances.10,12 By avoiding diffractive light splitting, its design may be less compromising in eyes with compromised macular function, where contrast preservation is critical. A reduction in monocular mesopic contrast sensitivity compared to a monofocal lens has been reported.13,14 However, Bala et al found that differences in binocular contrast sensitivity relative to a monofocal IOL are minimal under both photopic and mesopic conditions.14
Adequate near vision is a recognized concern with EDOF IOLs. Therefore, micro-monovision, in which the dominant eye is targeted for emmetropia and the non-dominant eye for slight myopia (typically ≤−0.50 D), has been reported to improve near visual function while preserving good binocular distance and intermediate visual acuity.15 Currently, there is limited evidence on the outcomes of the non-diffractive EDOF IOL in patients with macular disease.3,16 To our knowledge, the use of a micro-monovision strategy with non-diffractive EDOF IOLs in patients with macular disease has not been specifically evaluated. This study evaluates objective and subjective visual outcomes after bilateral implantation of AcrySof IQ Vivity IOL with micro-monovision in patients with early ERM and/or AMD.
Material and Methods
Design
This prospective, single-center, non-comparative pilot cohort study enrolled 40 eyes from 20 patients with early-stage macular pathology who underwent bilateral cataract removal via routine small-incision phacoemulsification surgery with the implantation of a non-diffractive EDOF IOL. All patients were targeted for micro-monovision, with the non-dominant eye targeted for −0.50 D. The study adhered to the principles of the Declaration of Helsinki and was approved by the Advarra Institutional Review Board (Aurora, ON, Canada; protocol number: Pro00048754). All participants provided informed consent for both treatment and study participation.
Patients
Patients were eligible for inclusion in this study if they were: (1) age ≥ 45 years with cataracts eligible for bilateral cataract surgery, (2) corrected distance visual acuity (CDVA) of 0.3 logMAR (20/40 Snellen) or worse, considered as part of the overall clinical assessment for bilateral cataract surgery eligibility, (3) visual potential of at least 20/32 in both eyes, (4) planned cataract removal by routine small-incision surgery, and (5) calculated lens power within commercially available ranges. In addition, participants were required to have at least one of the following conditions in at least one eye: (6) early AMD characterized by the presence of multiple small drusen, a few intermediate drusen (63–124 µm in diameter), and/or retinal pigment epithelium abnormalities (AREDS category 2), or (7) early ERM stage 0, indicated by a semi-transparent membrane that does not cause retinal distortion or obscure underlying blood vessels, also known as cellophane maculopathy. AREDS category 2 was selected to include eyes with early macular changes and relatively preserved visual potential while minimizing confounding from more advanced AMD-related visual impairment.
Patients were excluded if they had: (1) intermediate AMD or worse (AREDS category ≥ 3), (2) prior corneal refractive surgery, (3) planned astigmatic keratotomy and limbal relaxing incisions, (4) macular edema, (5) advanced macular pathology (6) active anterior or posterior segment inflammation, (7) history of any disease causing intraocular inflammation, (8) other ocular comorbidities, such as glaucoma, diabetic retinopathy, retinitis pigmentosa, and Stargardt’s disease, (9) severe corneal endothelial dysfunction (eg, corneal edema, fluctuating vision, thickened cornea), (10) zonular weakness that could affect IOL centration or stability, (11) amblyopia or mono-fixation syndrome, and (12) participation in another investigational drug or device study that could confound the results.
Intermediate AMD or worse was defined by the presence of extensive small or intermediate drusen, any large drusen, geographic atrophy, or neovascular AMD in either eye. Advanced macular pathology included geographic atrophy or choroidal neovascular membrane associated with reduced potential (< 20/40). Early ERM identification, AMD classification, and overall macular pathology assessment were performed by a single clinician using spectral-domain optical coherence tomography (SD-OCT) and clinical fundus findings, according to the predefined study definitions. Intergrader reliability assessment was not performed.
Preoperative Evaluation
Eligible patients underwent a comprehensive preoperative ophthalmologic evaluation, including medical history, visual acuity (VA) assessment, ocular dominance testing, manifest refraction, and intraocular pressure measurement. A detailed slit-lamp examination and dilated fundus examination were also performed. Biometric measurements were obtained using the IOLMaster 700 (Carl Zeiss Meditec AG, Jena, Germany), and IOL power was calculated using the Barrett Universal II formula. Toric IOLs were selected in cases with predicted residual astigmatism of ≥ 0.5 D, assuming a surgically induced astigmatism of 0.12 D and temporal incisions at 180 and 0 degrees for right and left eyes, respectively. All patients were targeted for micro-monovision, aiming for −0.50 D in the nondominant eye and emmetropia in the dominant eye.
Surgical Technique
All surgeries were performed by two experienced surgeons using a standardized small-incision phacoemulsification technique and consistent surgical protocols. A 2.2 mm temporal corneal incision was created. The anterior chamber was filled with a viscoelastic device. Capsulorhexis was performed manually, and the crystalline lens was removed with phacoemulsification (Centurion Vision System, Alcon). Using an injector, IOL was inserted into the capsular bag through the main incision. Viscoelastic was subsequently removed with the irrigation and aspiration handpiece. The interval between the contralateral eye surgeries was at most two months.
Intraocular Lens
The AcrySof IQ Vivity (Alcon) is an aspheric, non-diffractive EDOF IOL designed to provide an extended range of vision.17 Introduced in 2020, it incorporates proprietary non-diffractive X-WAVE technology, which extends the range of vision by stretching and shifting the wavefront of light, thereby improving visual performance for both distance and intermediate vision while preserving functional near vision.18
Postoperative Outcome Measures
All patients underwent comprehensive ophthalmic examinations at post-operative visits. Outcome assessments were performed three months after the second eye surgery. Safety was evaluated by recording all adverse events reported by investigators or participants at each visit.
Visual Acuity and Refractive Outcomes
Primary outcomes included monocular corrected distance visual acuity (CDVA) and distance-corrected intermediate visual acuity (DCIVA) at 66 cm under photopic conditions (85 cd/m2). Additional outcomes included monocular distance-corrected near visual acuity (DCNVA), as well as binocular CDVA, DCIVA, and DCNVA; uncorrected distance (UDVA), intermediate (UIVA), and near visual acuity (UNVA), along with manifest refraction. Postoperative refractive accuracy was assessed by calculating the mean absolute error (MAE), median absolute error (MedAE), and mean arithmetic error (MArE) between the achieved and target refractions for all eyes. The proportion of eyes within ±0.50 D of the intended refraction was also determined.
Contrast Sensitivity
Postoperative binocular contrast sensitivity was measured using the CSV-2000 (VectorVision, Fairfield, CT, USA) across different spatial frequencies under photopic and mesopic conditions. Mean log contrast sensitivity values were recorded at spatial frequencies of 3, 6, 12, and 18 cycles per degree (cpd) under photopic conditions and at 3, 6, and 12 cpd under mesopic conditions. Preoperative contrast sensitivity was not assessed due to the potential impacts of cataracts on baseline measurements.
Patient Satisfaction and Quality of Vision
Subjective visual outcomes were assessed using the Catquest-9SF and Quality of Vision (QoV) questionnaires. The Catquest-9SF is a validated, Rasch-scaled instrument evaluating vision-related functional limitations in daily activities.19,20 The QoV questionnaire is a validated tool that assesses the frequency, severity, and bothersomeness of visual disturbances.21,22 Responses were converted to a Rasch-scaled linear interval score (0–100) with higher scores indicating worse symptoms. Reported percentages were calculated based on the number of patients who provided responses for each specific symptom, not the total cohort (n=20).
Statistical Analysis
No formal sample size was calculated as this was an exploratory pilot study. All data analyses were conducted using SPSS Inc. (Chicago, IL), SAS Studio (Cary, NC), and Python 3.9. Descriptive statistics were calculated for all primary and secondary outcomes. Continuous variables were summarized as median (interquartile range, IQR), and categorical variables as frequencies and percentages. Given the small sample size and non-normal distribution of the data, non-parametric tests were used. For comparisons between independent groups, the Mann–Whitney U-test was applied. For paired comparisons, the Wilcoxon signed-rank test was used. As a sensitivity analysis, monocular eye-level outcomes were additionally evaluated using linear mixed-effects models with patient included as a clustering variable to account for inter-eye correlation. All visual acuity measurements were converted to the logarithm of the minimum angle of resolution (logMAR) scale for statistical analysis and reported as logMAR VA equivalents. A two-sided p-value of <0.05 was considered statistically significant.
The results were presented using standard graphs for reporting outcomes of intraocular lens-based refractive surgery.23 Additionally, cumulative histograms for binocular CDVA and UDVA were included.
Results
Study Population
The study included 20 patients (40 eyes) who underwent bilateral cataract surgery. Each participant had at least one eye with early AMD or early ERM.
Seven patients had bilateral AMD, and six patients had bilateral ERM, while seven patients had unilateral ERM with a normal contralateral eye.
Among the 40 eyes, 19 eyes (47.5%) had early ERM, and 14 eyes (35.0%) had early AMD. The remaining seven eyes (17.5%) were normal contralateral eyes without macular pathology (Figure 1). The cohort had an equal gender distribution (50% male, 50% female), with a mean age of 70.5 ± 9.7 years. No intraoperative or postoperative adverse events were observed. Baseline preoperative characteristics were comparable between eyes with ERM and AMD (Table 1).
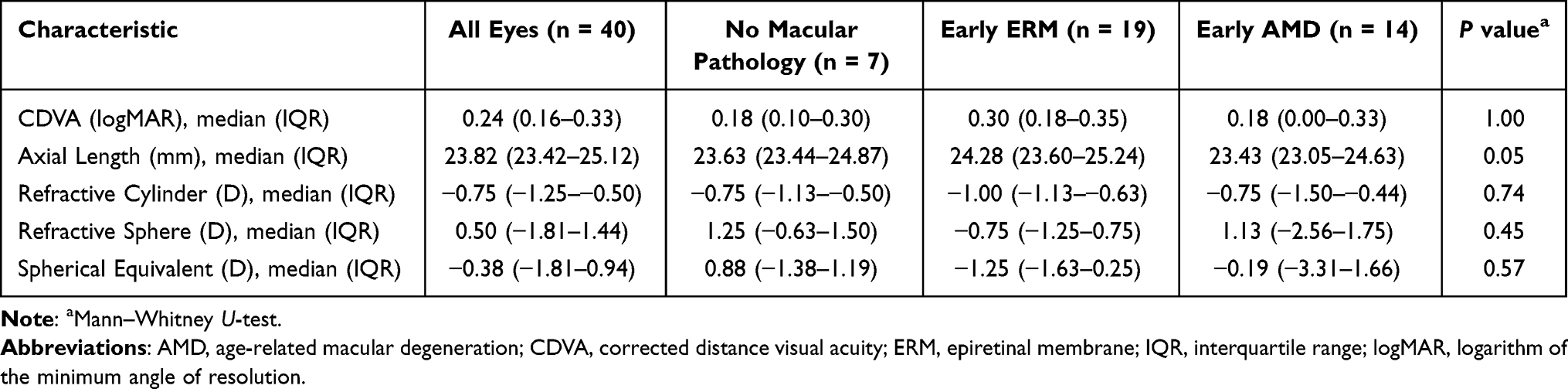 |
Table 1 Preoperative Ocular Characteristics Between Patients with Early ERM and Early AMD |
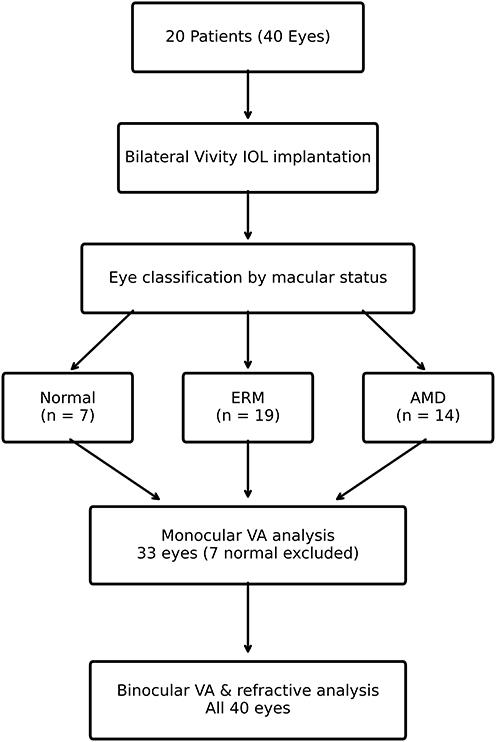 |
Figure 1 Flow diagram illustrating patient and eye inclusion. Twenty patients (40 eyes) were included, of whom 7 had bilateral AMD, 6 had bilateral ERM, and 7 had unilateral ERM. A total of 40 eyes were included in refractive analyses, and 33 eyes were included in monocular visual acuity analyses after exclusion of normal contralateral eyes. Abbreviations: AMD, age-related macular degeneration; ERM, epiretinal membrane. |
Visual Acuity and Refractive Outcomes
For monocular visual acuity analyses, the seven normal contralateral eyes were excluded, yielding a total of 33 eyes. All 40 eyes were included in the refractive analysis. A flow diagram is shown in Figure 1.
Table 2 summarizes monocular visual and refractive outcomes, categorized by dominant and non-dominant eyes and further stratified by ERM and AMD status. At the 3-month follow-up, the median (IQR) monocular CDVA, DCIVA, and DCNVA were 0.00 (0.00–0.10), 0.18 (0.08–0.28), and 0.40 (0.30–0.50) logMAR, respectively, with a statistically significant improvement in monocular CDVA observed across all eyes (P < 0.001), including both ERM (P < 0.001) and AMD (P = 0.02) subgroups. These findings were unchanged in a sensitivity analysis using a linear mixed-effects model accounting for inter-eye correlation.
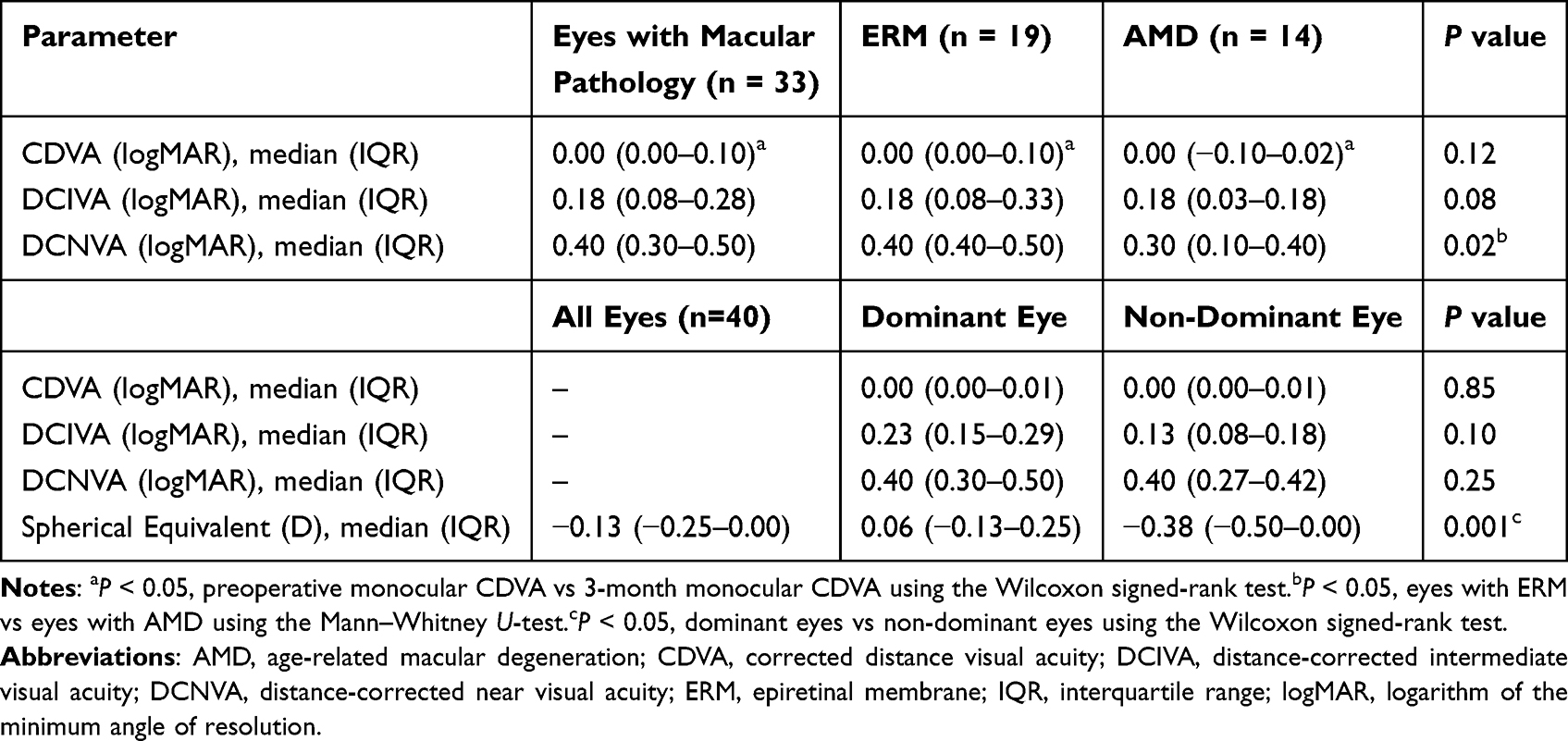 |
Table 2 Postoperative Monocular Visual and Refractive Outcomes by Macular Pathology and Ocular Dominance at 3 Months |
Table 3 summarizes binocular distance-corrected and uncorrected visual acuities. The median (IQR) binocular CDVA, DCIVA, and DCNVA were 0.00 (0.00–0.00), 0.13 (0.08–0.18), and 0.35 (0.22–0.40) logMAR, respectively. The median (IQR) UDVA, UIVA, and UNVA were 0.00 (0.00–0.00), 0.08 (−0.01–0.11), and 0.30 (0.20–0.33) logMAR, respectively. Notably, 19 of 20 patients (95%) achieved binocular UDVA and CDVA of 20/25 (≈ 0.10 logMAR) or better (Figure 2).
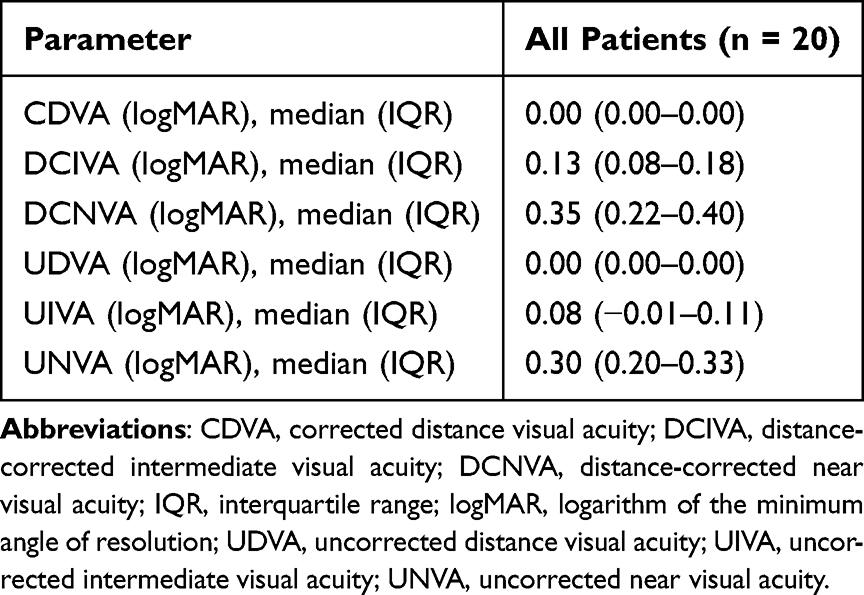 |
Table 3 Postoperative Binocular Corrected and Uncorrected Visual Outcomes at 3 Months |
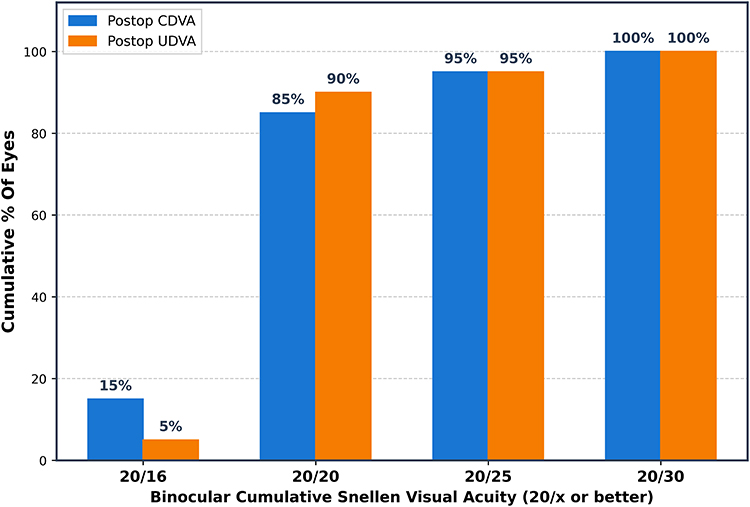 |
Figure 2 Postoperative binocular CDVA and UDVA at 3 months. Cumulative percentage of eyes achieving 20/x or better binocular distance visual acuity. Blue bars represent CDVA, and Orange bars represent UDVA. Abbreviations: CDVA, corrected distance visual acuity; UDVA, uncorrected distance visual acuity. |
The median (IQR) target refraction of chosen IOL was −0.05 D (−0.14–0.02) for the dominant eye, and −0.42 D (−0.51–−0.19) for the non-dominant eye. As anticipated, a significant difference in postoperative manifest spherical equivalent (SE) was observed between dominant and non-dominant eyes (P = 0.001). The median (IQR) SE for all eyes (n=40) was −0.13 (−0.25–0.00). The median (IQR) SE for dominant eyes was 0.06 (−0.13–0.25), and for non-dominant eyes, it was −0.38 (−0.50–0.00). MAE was 0.27 ± 0.29 D, MedAE was 0.16 D (IQR, 0.08–0.39 D), and MArE was 0.16 ± 0.37 D for dominant eyes; MAE was 0.26 ± 0.15 D, MedAE was 0.26 D (IQR, 0.15–0.37 D), and MArE was 0.05 ± 0.18 D for non-dominant eyes. Figure 3 shows the distribution of postoperative SE across all eyes (Figure 3A) and refractive accuracy relative to target (D) for dominant (Figure 3B) and non-dominant eyes (Figure 3C). A high proportion of eyes met the target refraction, with 90% of dominant and 95% of non-dominant eyes within ±0.50 D of the intended outcome.
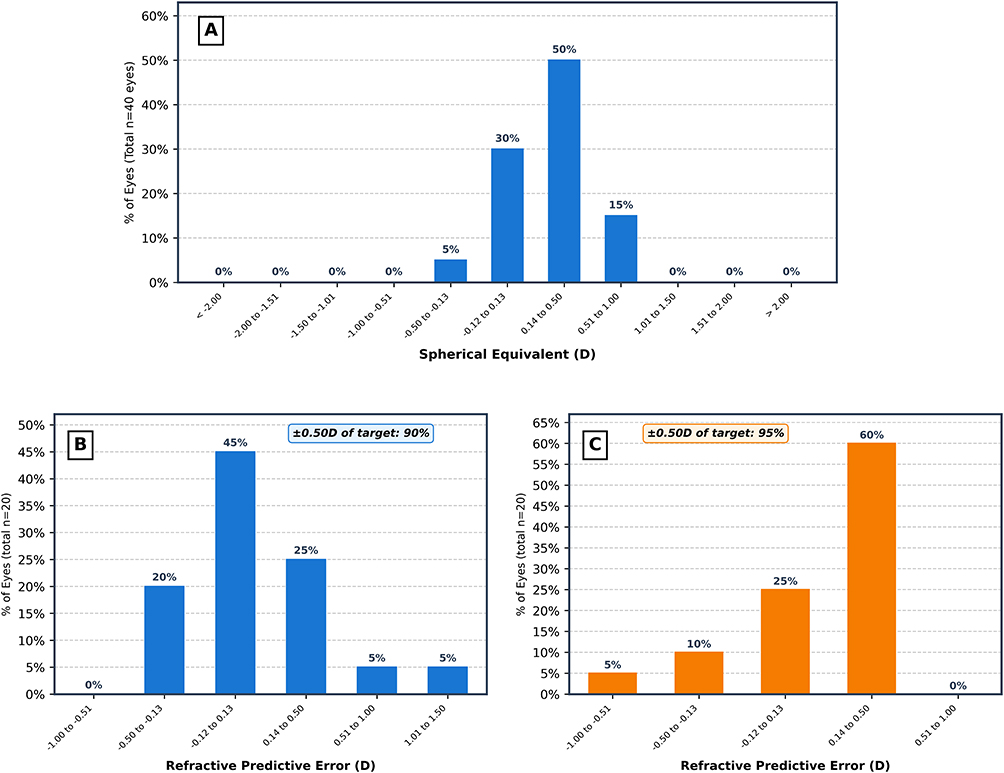 |
Figure 3 Postoperative spherical equivalent distribution and refractive accuracy at 3 months. (A) Distribution of postoperative spherical equivalents for all eyes. (B) Refractive accuracy relative to the intended target in dominant eyes. (C) Refractive accuracy relative to the intended target in non-dominant eyes. |
Contrast Sensitivity
Figure 4 illustrates the mean (SD) binocular contrast sensitivity (log units) under photopic and mesopic conditions at 3 months postoperatively. Photopic contrast sensitivity was within 1 SD of the manufacturer-reported normal range for individuals aged 50 to 75 years (Supplemental Table 1).24,25 Mesopic contrast sensitivity was compared with manufacturer-reported normative data derived from younger individuals (20–55 years) (Supplemental Table 2),24,25 as no age-matched normative data were available for our older study population. Mesopic values were near the lower limit of the reference range and, at some spatial frequencies, slightly below it.
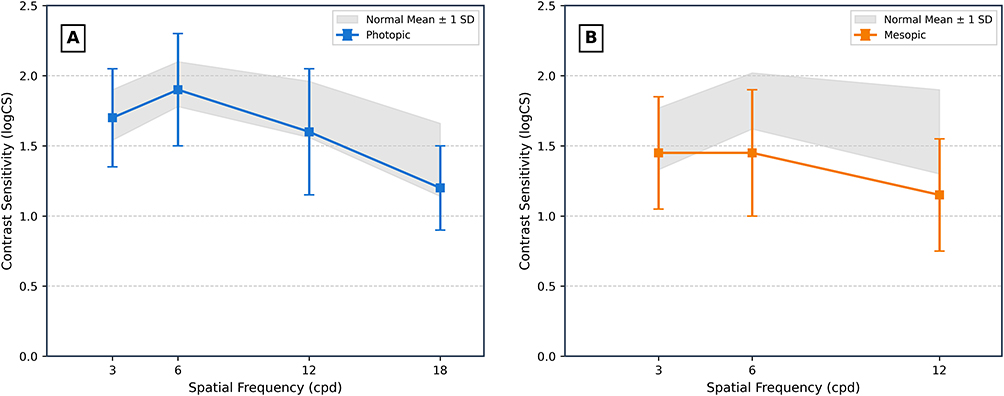 |
Figure 4 Mean (SD) binocular contrast sensitivity (log units) at 3 months postoperatively under photopic (A) and mesopic (B) conditions across spatial frequencies. Error bars represent standard deviation. Gray shaded areas represent normative reference ranges derived from manufacturer data (VectorVision, Greenville, OH, USA). Normative data were derived from individuals aged 50–75 years (photopic) and 20–55 years (mesopic). Abbreviations: cpd, cycles per degree. |
Patient Satisfaction and Quality of Vision
Figure 5 illustrates 3-month postoperative visual function outcomes across seven daily visual tasks assessed using the Catquest-9SF questionnaire. The most challenging task was reading newspaper print, with 55% of patients reporting “some difficulty,” and 10% reporting “no difficulty”. Despite this, most patients reported little to no difficulty with intermediate tasks such as handicrafts and hobbies, aligning with strong binocular UIVA results. The remaining two Catquest-9SF items assessed overall satisfaction with vision and difficulty in daily life. Overall, 90% of patients reported being “fairly” or “very satisfied” with their vision. Similarly, 90% of patients reported either no difficulty (60%) or only some difficulty (30%) in their daily life.
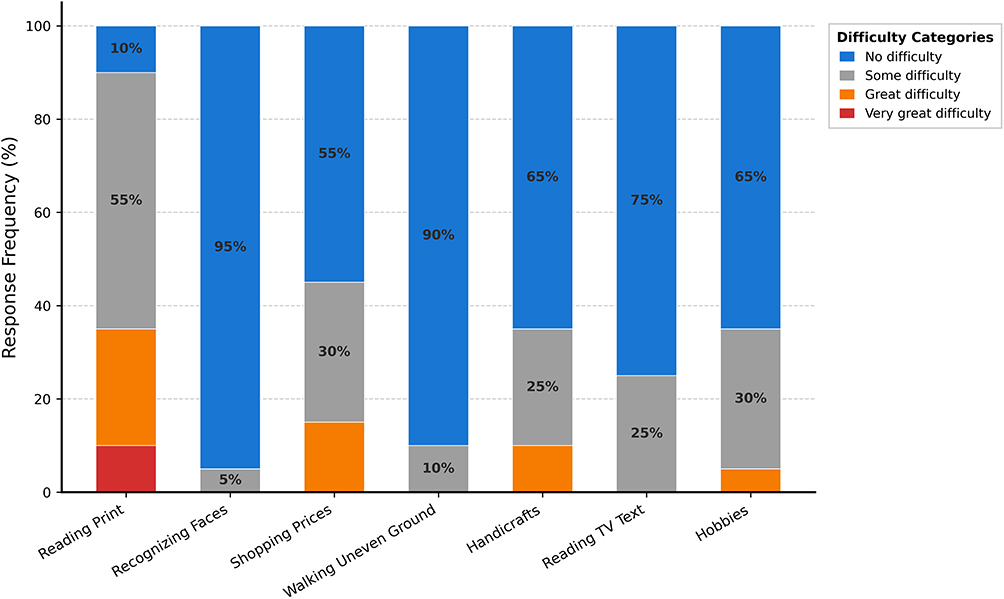 |
Figure 5 Catquest-9SF questionnaire responses at 3 months. Percentage of patients reporting levels of difficulty across seven daily visual tasks. The two overall assessment items (overall satisfaction with vision and overall difficulty in daily life) are reported separately in the text. |
Figure 6 shows the percentage of patients reporting the frequency, severity, and bothersomeness of various visual disturbances, as assessed by the QoV questionnaire. Aggregated Rasch-converted scores are presented in Figure 7. Most respondents reported visual symptoms as occurring “never” or “occasionally” across all categories. Overall, these findings indicate a low burden of visual disturbances in this cohort with early macular pathology.
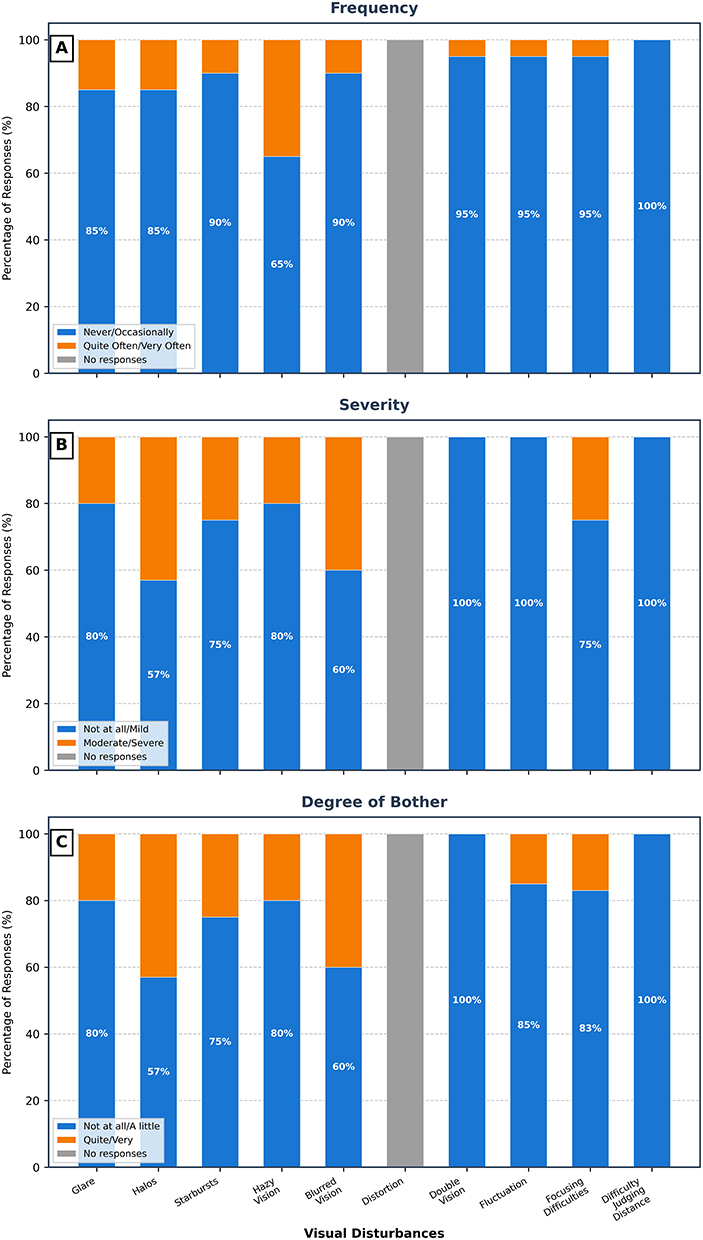 |
Figure 6 Quality of Vision (QoV) questionnaire responses at 3 months. (A) Frequency, (B) severity, and (C) bothersomeness of 10 visual disturbances. Percentages represent the proportion of responders for each symptom, not the total cohort (n=20). Response categories were grouped for analysis. |
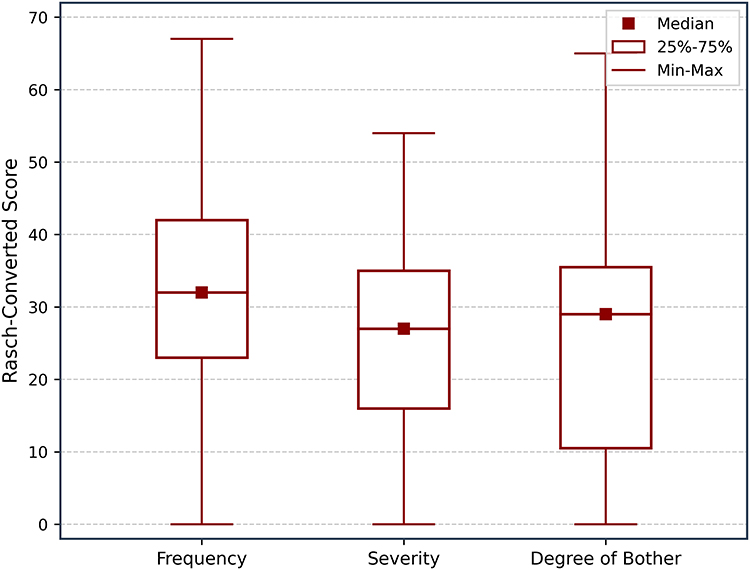 |
Figure 7 Box-and-whisker plot of Rasch-converted Quality of Vision (QoV) scores. |
Discussion
To the best of our knowledge, this is the first study to report clinical outcomes in patients with early macular pathology undergoing bilateral implantation of a non-diffractive EDOF IOL using a micro-monovision strategy. Nineteen of 20 patients (95%) achieved binocular UDVA and CDVA of 20/25 or better, with favourable UIVA, near visual outcomes, and contrast sensitivity within age-matched norms. Our findings suggest that eyes with ERM and AMD can achieve good distance and intermediate vision, along with favorable near visual outcomes, and minimal visual disturbances.
Median postoperative CDVA, DCIVA, DCNVA, UDVA, UIVA and UNVA were comparable to previously reported outcomes in patients without macular pathology who received the same IOL.14,26–28 This suggests that non-diffractive IOLs may be compatible with the visual needs of these patients. The median (IQR) binocular UIVA in this study was 0.08 (−0.01–0.11) logMAR, which was better than that reported in a previous study of the same IOL in eyes with stage 1–2 ERM targeted for emmetropia (0.14 ± 0.10 logMAR).3 Our better results may be explained by including only very early ERM without retinal distortion and by using a micro-monovision strategy. Notably, because macular pathology was required in at least one eye, seven patients with unilateral ERM had a normal contralateral eye included in the study. Although these eyes were excluded from monocular visual acuity analysis, we considered that they may have positively influenced binocular visual outcomes. To further evaluate this potential effect, we performed an exploratory sensitivity analysis excluding the seven patients with a normal contralateral eye. Binocular visual outcomes remained largely unchanged after exclusion, suggesting that inclusion of normal fellow eyes did not substantially influence the overall findings. Our results were also comparable to studies of non-diffractive EDOF implantation with micro-monovision in patients without macular pathology,14,26,28 suggesting that micro-monovision may support intermediate vision in patients with early macular pathology at levels similar to those without retinal disease.
The binocular UNVA of 0.30 (0.20–0.33) logMAR observed in our study is comparable to, or better than, outcomes reported for other EDOF IOLs.11,29 Compared with studies of non-diffractive EDOF IOL implantation targeting micro-monovision, near visual acuity was slightly worse.15,26 For example, Amelsfort et al reported a mean UNVA of 0.23± 0.12 logMAR, and Won et al reported 0.22± 0.12 logMAR, despite differences in the degree of myopic offset in the non-dominant eye across studies. Overall, this variation likely reflects a combination of refractive and methodological factors. Refractive accuracy appeared slightly lower in dominant eyes than non-dominant eyes; however, the clinical significance of this finding remains unclear.
In subgroup analyses, AMD eyes demonstrated better DCNVA than ERM eyes. Although this observation may suggest potential disease-related differences in near visual performance, it should be interpreted cautiously given the limited sample size and exploratory nature of these subgroup comparisons.
Contrast sensitivity results were encouraging, with photopic measurements falling within normal ranges at all spatial frequencies. Mesopic contrast sensitivity demonstrated a trend toward the lower end of the reference range. These findings should be interpreted with caution, given that the normative data available for mesopic contrast sensitivity comparison were derived from a younger population (20–55 years old) who would be expected to have superior contrast sensitivity; age-matched mesopic norms are not available.
Patient satisfaction at 3 months was high, with most patients reporting overall satisfaction with their vision. Although reading newspaper print remained the most challenging task, patients generally reported no difficulty with intermediate tasks such as handicrafts and hobbies, consistent with the observed intermediate visual outcomes.
Neural adaptation may also have contributed to subjective outcomes following micro-monovision, particularly in this older cohort with early macular pathology. Adaptation to mild induced anisometropia may vary between individuals and could influence perceived visual performance and satisfaction over time. Longer-term follow-up may help clarify the role of neural adaptation in this population.
Halos were the most frequently reported bothersome symptom, but they were reported as occurring “quite often” or “very often” by only a minority of respondents. The frequency, severity, and bothersomeness related to dysphotopsias, including glare, halos, and starbursts, were comparable to those reported in patients without macular pathology in studies by Gundersen et al30 and Bala et al,14 using the same questionnaire. When compared to a different EDOF IOL in patients without macular pathology, the median Rasch-converted scores in our study were lower (indicating better outcomes) for frequency, severity, and bothersomeness.29 Dysphotopsias were also lower than those associated with bifocal and trifocal lenses.29,31
These findings support consideration of Vivity IOL with micro-monovision in carefully selected patients with ERM or AMD with good visual potential, but do not justify extrapolation to more advanced macular disease. Furthermore, the progression of ERM or AMD and the long-term performance of this EDOF IOL in this population remain unknown. Given the progressive nature of macular disease, ongoing postoperative monitoring remains important, with attention to worsening visual symptoms and structural changes on SD-OCT. Longer-term studies are needed to better define optimal surveillance strategies in this population.
This study has several limitations. The relatively small sample size, particularly for each macular pathology subgroup, limits the statistical power. As a pilot study, these findings should be considered hypothesis-generating and viewed in the context of the study limitations. Because most results are presented for the total cohort rather than being stratified by pathology (due to the limited sample size), and because ERM and AMD represent distinct disease processes, the findings may not be fully generalizable and may have limited condition-specific interpretation. The absence of a control group is another limitation; however, we provided some normative data and historical references for comparison. The relatively short follow-up period further limits assessment of long-term visual outcomes and disease progression. Finally, the lack of age-matched normative data for mesopic contrast sensitivity represents an additional limitation. Despite these limitations, we feel this exploratory hypothesis-generating study is informative and adds to the current literature. Future studies with larger, stratified cohorts and appropriate control groups are needed to better define the role of non-diffractive IOL in patients with macular disease.
Conclusion
This study suggests that bilateral implantation of the non-diffractive EDOF IOL using a micro-monovision approach may provide promising visual outcomes in patients with early macular pathology. Patients achieved good distance and intermediate vision, favorable near visual outcomes and a low burden of visual disturbances. These findings support the potential use of this approach in carefully selected patients with early macular disease.
Abbreviations
AMD, age-related macular degeneration; AREDS, Age-Related Eye Disease Study; CDVA, corrected distance visual acuity; cpd, cycles per degree; DCIVA, distance-corrected intermediate visual acuity; DCNVA, distance-corrected near visual acuity; EDOF, extended depth of focus; ERM, epiretinal membrane; IOL, intraocular lens; logMAR, logarithm of the minimum angle of resolution; MAE, mean absolute error; MArE, mean arithmetic error; MedAE, median absolute error; QoV, Quality of Vision; SE, spherical equivalent; UDVA, uncorrected distance visual acuity; UIVA, uncorrected intermediate visual acuity; UNVA, uncorrected near visual acuity; VA, visual acuity.
Ethics Approval and Informed Consent
This study adhered to the tenets of the Declaration of Helsinki and was approved by the Advarra Institutional Review Board (Aurora, ON, Canada; protocol number: Pro00048754). The study was conducted at Prism Eye Institute, which does not have its own Research Ethics Board; therefore, approval was obtained through an independent external IRB. Written informed consent was obtained from all participants.
Funding
This was an investigator-initiated study supported by research funding from Alcon Vision, LLC, Fort Worth, TX, USA. The funding source has no role in the study design, collection, analysis, interpretation of data, or manuscript writing.
Disclosure
DKV: AbbVie: consulting (C), S; Alcon: C, honoraria (H), research funding/grant (R); Bausch & Lomb: C, R; Glaukos: C, R; Johnson & Johnson Vision: C, R; Labtician: C; Thea: C; Vizzario: C, stock ownership (O). IIKA: Aequus Pharmaceuticals Inc: C; Abbvie: C; Ace Vision Group, Inc: C; Aerie Pharmaceuticals Inc: C, R; Akorn: C; Alcon: C, H, R; Allergan: C, H, R; Aquea Health, Inc: C; ArcScan Inc: C; Avellino Lab USA, Inc: C; Avisi: C; Bausch Health: C; Beaver- Visitec International Inc: C; Bionode LLC: C; Camras Vision Inc: C, R; Beyeonics: C; Carl Zeiss Meditec AG: C, H; Centricity Vision, Inc: C; CorNeat Vision: C; Custom Surgical: C; ELIOS Vision, Inc: C; ElutiMed: C; Equinox: C; eyeFlow, Inc: C; Exhaura Limited: C; Genentech Inc: C; Glaukos Corp: C, R; Gore: C; Heine: C, H; Heru: C; Hexiris Pharma: C; Implandata: C; Iantrek: C; InjectSense Inc: C; Iridex Corp: C; iCare: R iSTAR Medical: C; Ivantis Inc: C, R; Johnson and Johnson Vision: C, H, R; Labtician Thea: C; LayerBio Inc: C; Leica Microsystems: C; Liqid Medical: C; Life Long Vision: C; Long Bridge Medical, Inc: C; MicroOptx: C; MST Surgical: C, H; Myra Vision: C; Noxelis: C; New World Medical: C, R; NovaEye: C; Orbitau: C; Ocular Instruments: C; Ocular Therapeutix: C; Oculo: C; Oculus Surgical: C; Omega Ophthalmic: C; Ocusciences: C; PolyActiva: C; PulseMedica: C; Peripherex: C; Perfuse Therapeutics: C; Qlaris Bio: C; Regeneration Pharmaceuticals Inc: C; Radius XR: C; Radiance Therapeutics, Inc: C; Ripple Therapeutics: C; Rheon Medical SA: C; Sanoculis Ltd: C; Santen: C, R; Shockwave Medical: C; Shifamed, LLC: C; Sight Sciences Inc: C; Singapore Biodesign: C; Sierra Clinical Services: C; SeonixBio: C;
Smartlens, Inc: C; Spyglass Pharma: C; Stroma Medical: C; Thea Pharma: C; TFS Health Science: C; Tavo Bio Therapeutics: C; ViaLase: C; Visci Ltd: C; Visus Therapeutics: C; Vizzario: C; VSY Biotechnology: C; WL Gore: C; Zilia, Inc: C. The authors report no other conflicts of interest in this work.
References
1. Zvorničanin J, Zvorničanin E. Premium intraocular lenses: the past, present and future. J Curr Ophthalmol. 2018;30(4):287–14. doi:10.1016/j.joco.2018.04.003
2. Salerno LC, Tiveron MC, Alió JL. Multifocal intraocular lenses: types, outcomes, complications and how to solve them. Taiwan J Ophthalmol. 2017;7(4):179–184. doi:10.4103/tjo.tjo_19_17
3. Jeon S, Choi A, Kwon H. Clinical outcomes after implantation of extended depth-of-focus AcrySof® Vivity® intraocular lens in eyes with low-grade epiretinal membrane. Graefes Arch Clin Exp Ophthalmol. 2022;260(12):3883–3888. doi:10.1007/s00417-022-05751-1
4. Kim B, Kwon S, Choi A, Jeon S. Influence of mild non-foveal involving epiretinal membrane on visual quality in eyes with multifocal intraocular lens implantation. Graefes Arch Clin Exp Ophthalmol. 2021;259(9):2723–2730. doi:10.1007/s00417-021-05225-w
5. Sinha R, Sahay P, Saxena R, Kalra N, Gupta V, Titiyal JS. Visual outcomes of binocular implantation of a new extended depth of focus intraocular lens. Indian J Ophthalmol. 2020;68(10):2111–2116. doi:10.4103/ijo.IJO_2139_19
6. Berdahl J, Bala C, Dhariwal M, Rathi H, Gupta R. Cost-benefit analysis of a trifocal intraocular lens versus a monofocal intraocular lens from the patient’s perspective in the United States. PLoS One. 2022;17(11):e0277093. doi:10.1371/journal.pone.0277093
7. Teichman JC, Ahmed IIK. Intraocular lens choices for patients with glaucoma. Curr Opin Ophthalmol. 2010;21(2):135–143. doi:10.1097/ICU.0b013e3283365154
8. Kamath GG, Prasad S, Danson A, Phillips RP. Visual outcome with the array multifocal intraocular lens in patients with concurrent eye disease. J Cataract Refract Surg. 2000;26(4):576–581. doi:10.1016/s0886-3350(99)00457-5
9. Kanclerz P, Toto F, Grzybowski A, Alio JL. Extended depth-of-field intraocular lenses: an update. Asia Pac J Ophthalmol. 2020;9(3):194–202. doi:10.1097/APO.0000000000000296
10. Kandavel R, Colvard M, Dredge J, et al. Comparative study between non-diffractive extended depth of focus and monofocal intraocular lenses. Clin Ophthalmol. 2023;17:1161–1168. doi:10.2147/OPTH.S402069
11. Tomagova N, Elahi S, Vandekerckhove K. Clinical outcomes of a new non-diffractive extended depth-of-focus intraocular lens targeted for mini-monovision. Clin Ophthalmol. 2023;17:981–990. doi:10.2147/OPTH.S405267
12. McCabe C, Berdahl J, Reiser H, et al. Clinical outcomes in a US registration study of a new EDOF intraocular lens with a nondiffractive design. J Cataract Refract Surg. 2022;48(11):1297–1304. doi:10.1097/j.jcrs.0000000000000978
13. US Food and Drug Administration. AcrySof™ IQ Vivity™ intraocular lens (IOL) – directions for use. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf/P930014S126C.pdf.
14. Bala C, Poyales F, Guarro M, et al. Multicountry clinical outcomes of a new nondiffractive presbyopia-correcting IOL. J Cataract Refract Surg. 2022;48(2):136–143. doi:10.1097/j.jcrs.0000000000000712
15. Won YK, Choi SH, Chung TY, Lim DH. Clinical Outcomes after Bilateral Implantation of a Wavefront-Shaping Extended Depth of Focus (EDOF) IOL with Mini-Monovision. J Clin Med. 2024;13(11):3225. doi:10.3390/jcm13113225
16. Thananjeyan AL, Siu A, Jennings A, Bala C. Extended depth-of-focus intraocular lens implantation in patients with age-related macular degeneration: a pilot study. Clin Ophthalmol Auckl NZ. 2024;18:451–458. doi:10.2147/OPTH.S442931
17. Alcon announces european launch of vivity, the only presbyopia-correcting intraocular lens with X-WAVE Technology | alcon.com. Available from: https://www.alcon.com/media-release/alcon-announces-european-launch-vivity-only-presbyopia-correcting-intraocular-lens-x.
18. Shafer BM, McCabe C, Reiser H, Newsom TH, Berdahl J. The REVIVE Study: long Term Outcomes of a Novel Non-Diffractive Extended Vision IOL versus Monofocal Control IOL. Clin Ophthalmol Auckl NZ. 2022;16:3945–3950. doi:10.2147/OPTH.S390380
19. Lundström M, Pesudovs K. Catquest-9SF patient outcomes questionnaire: nine-item short-form Rasch-scaled revision of the Catquest questionnaire. J Cataract Refract Surg. 2009;35(3):504–513. doi:10.1016/j.jcrs.2008.11.038
20. Schlenker MB, Minotti SC, Kabanovski A, et al. Catquest-9SF questionnaire and eCAPS: validation in a Canadian population. PLoS One. 2020;15(9):e0237788. doi:10.1371/journal.pone.0237788
21. Schmid R, Luedtke H, Borkenstein AF. Enhanced depth-of-focus intraocular lenses: latest wavefront-shaped optics versus diffractive optics. Optom Vis Sci off Publ Am Acad Optom. 2022;99(4):335–341. doi:10.1097/OPX.0000000000001894
22. McAlinden C, Pesudovs K, Moore JE. The Development of an Instrument to Measure Quality of Vision: the Quality of Vision (QoV) Questionnaire. Invest Ophthalmol Vis Sci. 2010;51(11):5537–5545. doi:10.1167/iovs.10-5341
23. Reinstein DZ, Archer TJ, Srinivasan S, et al. Standard for reporting refractive outcomes of intraocular lens-based refractive surgery. J Cataract Refract Surg. 2017;43(4):435–439. doi:10.1016/j.jcrs.2017.04.005
24. Pomerance GN, Evans DW. Test-retest reliability of the CSV-1000 contrast test and its relationship to glaucoma therapy. Invest Ophthalmol Vis Sci. 1994;35(9):3357–3361.
25. VectorVision. Normal values for photopic and mesopic contrast sensitivity. Available from: https://www.vectorvision.com/csv1000-norms/.
26. van Amelsfort T, Webers VSC, Bauer NJC, Clement LHH, van den Biggelaar FJHM, Nuijts RMMA. Visual outcomes of a new nondiffractive extended depth-of-focus intraocular lens targeted for minimonovision: 3-month results of a prospective cohort study. J Cataract Refract Surg. 2022;48(2):151–156. doi:10.1097/j.jcrs.0000000000000825
27. Jeon S, Choi A, Kwon H. Analysis of uncorrected near visual acuity after extended depth-of-focus AcrySof® VivityTM intraocular lens implantation. PLoS One. 2022;17:e0277687. doi:10.1371/journal.pone.0277687
28. Coassin M, Mori T, Di Zazzo A, et al. Effect of minimonovision in bilateral implantation of a novel non-diffractive extended depth-of-focus intraocular lens: defocus curves, visual outcomes, and quality of life. Eur J Ophthalmol. 2022;32(5):2942–2948. doi:10.1177/11206721211064018
29. Hammond MD, Potvin RVO. Visual Quality and Patient Satisfaction: comparing a Blended Bifocal Approach to Bilateral Extended Depth of Focus Intraocular Lens Implantation. Clin Ophthalmol Auckl NZ. 2019;13:2325–2332. doi:10.2147/OPTH.S232800
30. Gundersen KG, Potvin R. Clinical outcomes and quality of vision associated with bilateral implantation of a wavefront shaping presbyopia correcting intraocular lens. Clin Ophthalmol Auckl NZ. 2021;15:4723–4730. doi:10.2147/OPTH.S342947
31. Tran DB, Owyang A, Hwang J, Potvin R. Visual acuity, quality of vision, and patient-reported outcomes after bilateral implantation with a trifocal or extended depth of focus intraocular lens. Clin Ophthalmol Auckl NZ. 2021;15:403–412. doi:10.2147/OPTH.S295503
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Refractive and Visual Outcomes of a Monofocal Non-Constant Aberration Aspheric Intraocular Lens
Hernández-Martínez A, Díaz-del-Rio MA, Ruiz-Santos M, Ruiz-Mesa R, Tañá-Rivero P
Clinical Ophthalmology 2022, 16:2521-2530
Published Date: 10 August 2022
The REVIVE Study: Long Term Outcomes of a Novel Non-Diffractive Extended Vision IOL versus Monofocal Control IOL
Shafer BM, McCabe C, Reiser H, Newsom TH, Berdahl J
Clinical Ophthalmology 2022, 16:3945-3950
Published Date: 28 November 2022
Clinical Outcomes of a Monofocal, Optimized, Aspheric, Hydrophobic Acrylic Intraocular Lens Implant
García-Tomás B, Marín-Sánchez JM, García-Elskamp C, Alcon-Ruiz E, Montesinos-López L, García Martínez-Lozano B
Clinical Ophthalmology 2023, 17:3215-3224
Published Date: 27 October 2023
Extended Depth-of-Focus Intraocular Lens Implantation in Patients with Age-Related Macular Degeneration: A Pilot Study
Thananjeyan AL, Siu A, Jennings A, Bala C
Clinical Ophthalmology 2024, 18:451-458
Published Date: 13 February 2024
Two-Year Follow-Up of the MINI WELL Non-Diffractive Extended Depth-of-Focus Intraocular Lens: A Retrospective Observational Study
Sborgia A, Curatolo MC, Barattini DF, Niro A, Barattini L, Sborgia G
Clinical Ophthalmology 2026, 20:602800
Published Date: 24 June 2026