Back to Journals » Journal of Pain Research » Volume 16
Vigilance to Painful Laser Stimuli is Associated with Increased State Anxiety and Tense Arousal
Authors Meeker TJ ![]() , Saffer MI, Frost J, Chien JH
, Saffer MI, Frost J, Chien JH ![]() , Mullins RJ, Cooper S, Bienvenu OJ, Lenz FA
, Mullins RJ, Cooper S, Bienvenu OJ, Lenz FA ![]()
Received 17 March 2023
Accepted for publication 4 November 2023
Published 4 December 2023 Volume 2023:16 Pages 4151—4164
DOI https://doi.org/10.2147/JPR.S412782
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jonathan Greenberg
Timothy J Meeker,1,2 Mark I Saffer,1 Jodie Frost,1 Jui-Hong Chien,1 Roger J Mullins,1,2 Sean Cooper,1 O Joseph Bienvenu,3 Fred A Lenz1
1Department of Neurosurgery, Johns Hopkins University, Baltimore, MD, USA; 2Department of Biology, Morgan State University, Baltimore, MD, USA; 3Department of Psychiatry and Behavioral Sciences, Johns Hopkins University, Baltimore, MD, USA
Correspondence: Timothy J Meeker, Department of Biology, Morgan State University, 1700 East Cold Spring Lane, Key Hall G51, Baltimore, MD, 21251, USA, Tel +1-443-885-3070, Email [email protected]
Introduction: Pain is frequently accompanied by enhanced arousal and hypervigilance to painful sensations. Here, we describe our findings in an experimental vigilance task requiring healthy participants to indicate when randomly timed moderately painful stimuli occur in a long train of mildly painful stimuli.
Methods: During a continuous performance task with painful laser stimuli (CPTpain), 18 participants rated pain intensity, unpleasantness, and salience. We tested for a vigilance decrement over time using classical metrics including correct targets (hits), incorrectly identified non-targets (false alarms), hit reaction time, and false alarm reaction time. We measured state anxiety and tense arousal before and after the task.
Results: We found a vigilance decrement across four 12.5-minute blocks of painful laser stimuli in hits [F3,51=2.91; p=0.043; time block 1>block 4 (t=2.77; p=0.035)]. Both self-report state anxiety (tpaired,17=3.34; p=0.0039) and tense arousal (tpaired,17=3.20; p=0.0053) increased after the task. We found a vigilance decrement during our laser pain vigilance task consistent with vigilance decrements found in other stimulus modalities. Furthermore, state anxiety positively correlated with tense arousal.
Discussion: CPTpain acutely increased tense arousal and state anxiety, consistent with previous results implicating the reciprocal interaction of state anxiety and acute painful sensations and the role of pain in augmenting tense arousal. These results may indicate a psychological process which predisposes the hypervigilant to developing greater acute pain, resulting in positive feedback, greater pain and anxiety.
Keywords: continuous performance task, false alarms, pain, vigilance, salience
Introduction
Pathological vigilance to painful and pain-related stimuli is linked to individual burden of chronic pain and predictive of post-op pain.1–3 This burden of pain is in turn related to increased anxiety and arousal.4,5 Despite the clinical importance of hypervigilance to painful stimuli, most studies reporting effects of pain on attentional mechanisms use visual attention-bias tasks to pain-related stimuli such as pain-related words or faces of those in pain, or self-report measures such as the Pain Vigilance and Avoidance Questionnaire.6–9 These tools are subjective and reflect attentional bias toward pain-related semantic or visual stimuli and do not incorporate painful stimuli.9,10 Furthermore, these tests do not measure changes in behavior over time, a core characteristic of vigilance.11 Meta-analyses of attention bias studies show evidence of mixed or small effects indicating that attention bias is increased in chronic pain patients compared to control populations.8,9,12
Previously, our group examined behavior, performance, and self-reported characteristics of painful thermal stimuli in an experimental model of vigilance. We reported a decrement in vigilance performance over time on task during a continuous performance task requiring discrimination of painful targets from non-targets (CPTpain).13 This decrement was also observed during sustained attention to target stimuli in other sensory modalities.11,13–15 We reported that tense arousal during the CPTpain positively correlated with pain unpleasantness, consistent with negatively valenced stimuli and affective states or moods driving tense arousal.5,16 Furthermore, tense arousal was related to state anxiety, but not trait anxiety, consistent with the dynamic nature of increased tense arousal in headache pain.5,17
Modifying our task to use a laser stimulus made it possible to selectively evoke activation of Aδ- and C-fiber nociceptors without activation of Aβ primary afferents evoked by the ongoing physical contact of a thermode.18–20 When evaluating evoked potentials measured with scalp electroencephalography, laser evoked potentials have the benefits of being comparable to larger body of evidence and allow more precise temporal resolution given the short duration stimulus.21–24
According to the biased competition model of attention, task-directed and stimulus-driven mechanisms impinge on task performance.25 Painful stimuli are both aversive and inherently salient, suggesting psychological elements associated with painful stimuli result in cognitions related to stress and threat.4,5,25,26 Consistent with this hypothesis, we predicted increases in both state anxiety and tense arousal, which we measured immediately before and after the CPT with painful laser stimuli.5,27 Furthermore, consistent with our prior reports, we predicted state anxiety and tense arousal would be correlated during the experience of painful stimuli.13
Materials and Methods
Participant Recruitment
We recruited 24 healthy volunteers from neighbors, staff, students, and trainees of the Johns Hopkins Hospital and University. Participants who were enrolled included 8 women (18 to 47 years old) and 16 men (18 to 75 years old). Exclusion criteria included active neurological conditions, including the presence of or self-report of history of chronic pain, psychiatric conditions, and medical conditions. All participants gave written informed consent before the study, all study procedures were approved and renewed yearly by the Johns Hopkins School of Medicine Institutional Review Board, and the study complied with the Declaration of Helsinki.
Stimuli Determination and Psychophysical Characterization
Laser stimuli were produced using a Nd:YAP 1340 nm wavelength laser (El.En. Group, Florence, Italy). Laser parameters included a 10mm-diameter beam with 20ms-pulse duration and energies ranging from 10J to 15J (fluence = 12.74 to 19.11 J/cm2). Laser parameters of a 10mm diameter beam with 20ms pulse duration with 14.5J intensity regularly failed to fire, therefore the staircase included intensities from 10 to 14J in 0.5J increments. When choosing a target laser intensity, we used 15J only when stimuli of 13J were painful but still rated below 1.5 out of 10 on a numerical rating scale (NRS). Laser stimuli were applied to the distal half of the dorsal forearm and dorsum of the hand. The time between each successive stimulus on the same area of skin during any trial series was at least 3 minutes.
Participants were fitted with laser protective glasses and experienced a staircase of laser intensities (10 to 14J in 0.5J increments) which they perceptually classified as “none”, “warm”, or “pain”. The staircase started at the median energy of 12J, ascended to 14J, and then descended and ascended two more times. For those stimuli classified as “pain”, participants rated the salience, pain intensity and pain unpleasantness all on a 0–10 computerized NRS. Participants who did not endorse any of the stimuli as consistently painful were excluded. Mild (2 to 3/10 NRS) and moderate (4 to 5/10 NRS) pain stimulus energies were selected.
Training, Habituation and Continuous Performance Task
We have previously shown that the presentation order of habituation and continuous performance task with painful stimuli (CPTpain) within a similar experimental protocol had no effect on pain intensity of the first block of habituation or CPTpain.13 Furthermore, there was no effect of order on the change in pain intensity, change in pain unpleasantness or change in salience. Therefore, we kept the order of habituation and CPTpain fixed to avoid long-term sensitization or habituation effects of the 480 stimuli over the hour of the CPTpain.
Next, participants were instructed:
For this next test, the skin will rapidly increase in temperature and a word on the monitor will indicate whether the stimulus is a ‘high’ stimulus or a ‘low’ stimulus. Please concentrate on learning the association of the stimulus with the classification. Please put on the headphones and stare at the crosshairs.
Participants experienced a random train of 20 stimuli (10 mild, 10 moderate). Three seconds before receiving the stimuli they were shown either the word “high” for the moderate stimulus or “low” for the mild stimulus (Figure 1). After this “training” session, participants rated pain intensity, pain unpleasantness, and salience of the stimuli as well as degree of mind-wandering, and tense arousal. Participants were instructed on the meaning of pain intensity, pain unpleasantness and salience using a standard script (adapted from):28
There are three aspects of your perception which we are interested in measuring: the intensity – how strong the stimulus feels, the unpleasantness – how disturbing the stimulus is for you, and the salience – how much the stimulus is able to attract or grab your attention. The distinction between these aspects of perception might be made clearer if you think of listening to a sound, such as a radio. As the volume of the sound increases, I can ask you how loud it sounds, how unpleasant it is to you, or how much you are distracted by the sound. The intensity of the stimulus is like loudness; the unpleasantness of the stimulus depends not only on intensity, but on other factors which may affect you; and the salience of the stimulus is the ability of the stimulus to attract your attention. Although some sensations may be equally intense and unpleasant and salient, we would like you to judge these aspects of your pain independently. Please put the headphones on and stare at the crosshairs.
 |
Figure 1 Participants completed four blocks of the continuous performance task with painful stimuli (CPTpain). Each block consisted of 120 stimuli, 36 of which were targets, (high intensity) stimuli distributed randomly within four sub-blocks. All stimuli were 20 ms laser pulses with a random interstimulus interval (ISI) between 4 and 9 s. The dotted line in the lower panel is the threshold temperature for pain, as established for participants individually. |
To verify discrimination of mild and moderate pain stimuli, participants experienced a series of 20 stimuli (10 mild, 10 moderate) where they were instructed:
For this next test, the skin will rapidly increase in temperature. Please press the button on the response pad as soon as you detect the more intense stimulus. Please be as accurate as you can but press the button as quickly as you are able to. Please press the button only once. Please put on the headphones and stare at the crosshairs.
Participants performed the training task during a series of 20 stimuli up to 4 times, until they achieved a performance of 16 out of 20 correct trials. If the participant performed below 0.8 (80%) correct trials after two series of stimuli, the increment between the mild and moderate pain stimuli was increased by 0.5J while keeping both stimuli above the pain threshold. Data from each participant were evaluated for performance. Criteria for inclusion in data analysis was a correct trial rate and the balanced accuracy (0.5*(Hit Rate+Correct Rejection Rate)) greater than 0.7 (70%) during the first block of the CPT.29 If participants performed above chance, but below inclusion criteria, they were contacted to repeat the session once and their data was included if their performance met inclusion criteria. Six participants (3 F) were excluded from the 24 first enrolled based on failure to distinguish between mildly and moderately painful stimuli as in our previously published protocol.13 Participants excluded at this point in the protocol did not participate in any subsequent part of the protocol. After the final successfully discriminated series of stimuli, participants rated pain intensity, pain unpleasantness, salience of the stimuli, degree of mind-wandering, and tense arousal.
Next, participants experienced two 2.5-minute series of stimuli to control for possible effects of habituation. Mild and moderate painful laser stimuli alternated with a 5 s interstimulus interval for a total of 30 total stimuli. Participants were instructed:
For this next test, the skin will rapidly increase in temperature several times. You will answer some questions about the sequence of stimuli and then we will repeat the sequence. Please put on the headphones now.
After each 2.5-minute series of stimuli, participants rated pain intensity, pain unpleasantness, salience of the stimuli, intrinsic attention to pain, degree of mind-wandering, and tense arousal.13,30,31 Tense arousal was measured using the tense arousal (TA) subscale of the Activation-Deactivation Checklist.31 Participants were instructed to “Please use the rating scale next to each word to describe your feelings at this moment”. Five adjectives (Jittery, Intense, Clutched-up, Tense, and Fearful) were rated using a 4-point Likert scale anchored at 1 (definitely do not feel) and 4 (definitely feel). During the habituation blocks, participants were not required to differentiate between the two stimulus types and did not have access to the mouse button.
Finally, participants performed the continuous performance task with painful stimuli (CPTpain), which was composed of 4 blocks of 120 laser stimuli made up of 36 target (moderate pain) and 84 nontarget (mild pain) laser stimuli with a randomized interstimulus interval of 4 to 9.13,32 Within each block, target and nontarget stimuli were fully randomized in four subblocks. After each of the 4 blocks, participants rated pain intensity, pain unpleasantness, salience of the stimuli, degree of mind-wandering, and tense arousal. For this section of the study, participants were instructed:
For this next test, the skin will rapidly increase in temperature several times. Please press the button on the response pad as soon as you detect the more intense stimulus. Please be as accurate as you can but press the button as quickly as you are able to. You will answer some questions about the sequence of stimuli, and we will repeat the sequence. Please press the button only once after each stimulus. Please put on the headphones and stare at the crosshairs.
Psychological Questionnaires
To identify psychological factors that may contribute to sensory perception and task performance during vigilance to pain, participants completed self-report questionnaires over a one-hour period before the sensory testing. These included: PCS: Pain Catastrophizing Scale,33 PASS: Pain Anxiety Symptom Scale,34 ASI: Anxiety Sensitivity Index,35 STAI: State and Trait Anxiety Inventory,36 Activation-Deactivation Checklist,31 and the NEO Five Factor Inventory.37,38 STAI State Anxiety and tense arousal from the Activation-Deactivation Checklist were also assessed immediately after the participant completed the CPTpain task.
Statistical Analysis
All statistical analyses were conducted using R version 3.6.3. Data from all variables were assessed for normality using the Shapiro–Wilk test. Data were analyzed after Z-transformation to scale and standardize each variable. All variables were evaluated for the presence of outliers, defined as values more than three median absolute deviations from the median.39 No outliers were detected.
We tested for a vigilance decrement over time using a linear mixed model (LMM), with the factor of time represented by the four blocks in the protocol.40 In the LMM, each outcome variable (eg, number of hits or false alarms per block, average hit or average false alarm response time per block), was modeled as a within-participant factor of time with participant as a random effect. The effect of time was explicitly modeled by comparing block 1 to blocks 2, 3 and 4, as in Dunnett’s method, with the covariance structure of the model assuming compound symmetry. This has the effect of reducing the number of possible pairwise comparisons and is warranted by extensive prior literature examining the vigilance decrement in other sensory modalities.41 We previously reported the superiority of this model compared to a simple repeated-measures analysis of variance (RM-ANOVA) model assuming compound symmetry, a model including an autoregressive correlation structure for time, and a model for each test.32 All post hoc comparisons across time were corrected for multiple comparisons with a normed multivariate t correction.42
We report F-stat values for the fixed effects derived from LMMs using the ANOVA function in Rbase and p-values derived using corrected degrees of freedom from the Kenward–Roger correction.43–45 All bivariate correlations were tested using the ppcor package in R.46 Because we evaluated many variables at each task block, over time on task, we corrected for the repeated-measures correlation with a t-test using the effective degrees of freedom. For figures, we used the R package ggscatter to create bivariate scatterplots with corresponding 95% confidence curves for relationships of interest. We used a paired t-test to assess changes in state anxiety and tense arousal between before and after the CPT with painful laser stimuli. We calculated correlation values for all simple and partial correlations while controlling separately for age and sex (See Supplemental Tables 1 and 2).
Results
Stimulus Characteristics and Perception
The mean laser energy that produced mild pain (nontarget) was 12.0 Joules (SD=0.72; range = 10.5J to 13J), while the mean laser energy to produce moderate pain (target) was 13.9J (SD=0.73; range = 12.5J to 15J). The mean pain intensity reported in response to mild pain (nontarget) was 2.6 out of 10 (SD=1.1; range = 0.9 to 4.6), while that reported in response to moderate pain (target) was 4.5 (SD=1.8; range = 1.8 to 8.1). Before the habituation protocol, there were 19 mostly painful laser stimuli during laser energy selection, then 20 painful stimuli during each training and verification period.
When using the LMM to compare the first block to CPTpain blocks 2, 3, and 4, there was no significant change in pain intensity ratings (F3,50=0.39; p=0.76), pain unpleasantness ratings (F3,50=0.27; p=0.85), or salience ratings (F3,50=2.03; p=0.12). Also, during habituation trials, there were no significant reductions in pain intensity ratings (tpaired,17=0.00; p=1.00), pain unpleasantness ratings (tpaired,17=0.27; p=0.79), or salience ratings (tpaired,17=−0.33; p=0.75). These results support the absence of sensitization or habituation in pain intensity, pain unpleasantness and salience during painful laser stimulation. In addition, the change in pain intensity ratings (R=−0.37; p=0.13), change in pain unpleasantness ratings (R=−0.085; p=0.74) and change in salience ratings (R=0.30; p=0.22) were not correlated within individuals between the habituation and CPT tasks. These results support that the order of habituation and CPT task during the protocol did not influence stimulus perception across the protocol.
Vigilance Decrement
The vigilance decrement related to painful stimuli is indicated by the decrease in hits over time in a CPT with a painful target (CPTpain). During the CPTpain, hits significantly decreased during time on task across task blocks [F3,51=2.91; p=0.043; comparison of block 1 with block 4 was significant (t=2.77; p=0.035); Figure 2A]. In contrast, mean hit RTs to target stimuli did not change by block (F3,51=0.31, p=0.82; Figure 2B). Therefore, the most basic element of vigilance, the vigilance performance decrement, was found during CPTpain providing a conceptual replication of our previous results.32
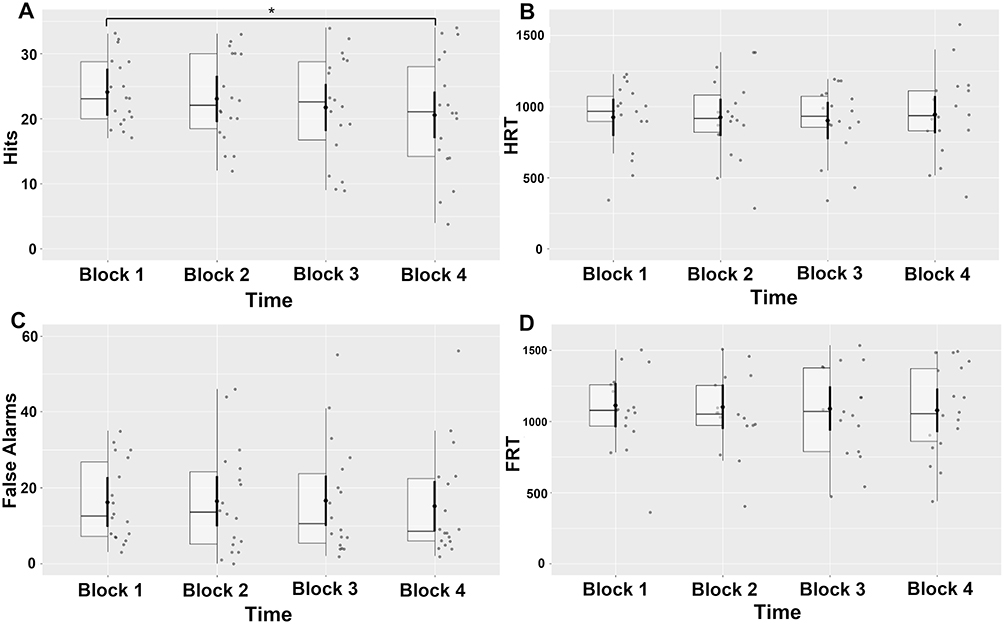 |
Figure 2 Vigilance metrics over the four blocks of continuous performance task (CPT) with a painful target. (A) Hits over time on task. (B) Hit reaction time over time on task. (C) False alarms over time on task. (D) False alarm reaction time over time on task. Bold error bars represent standard error of mean; boxes represent interquartile intervals. * = p < 0.05. |
False alarms did not significantly change with time on task (F3,51=0.33; p=0.80; Figure 2C). Similar to mean hit RTs, mean false alarm RTs to nontarget stimuli did not change by block (F3,51=0.16, p=0.93; Figure 2D).
Finally, both state anxiety (tpaired,17=3.34; p=0.0039) and tense arousal (tpaired,17=3.20; p=0.0053) significantly increased after the CPTpain when compared to the time immediately before the CPTpain. Importantly, there was no significant change in tense arousal during habituation (tpaired,17=1.75; p=0.098), though the difference between the change during CPTpain and the absence of the change during habituation was also not significant ((tpaired,17=1.45; p=0.17).
Tense Arousal, Pain Intensity and Unpleasantness
During CPT with painful laser stimuli, tense arousal positively correlated with salience (R=0.380; t-stat=2.96; p=0.0046), but not pain intensity (R=−0.0084; t-stat=−0.061; p=0.952) or pain unpleasantness (R=0.189; t-stat=1.40; p=0.172) (Figure 3A; Supplemental Table 1) – a distinctly different pattern than we observed with the thermode. As pain intensity, pain unpleasantness and salience are often highly correlated with each other, we tested a 4-variable partial correlation model relating tense arousal, pain intensity, pain unpleasantness and salience during CPT with painful laser stimuli. Within this partial correlation model, tense arousal was positively correlated with salience (R=0.433; t-stat=3.47; p=0.0011), negatively correlated with pain intensity (R=−0.385; t-stat=−3.01; p=0.0040) and not significantly correlated with pain unpleasantness (R=0.138; t-stat=1.00; p=0.321).
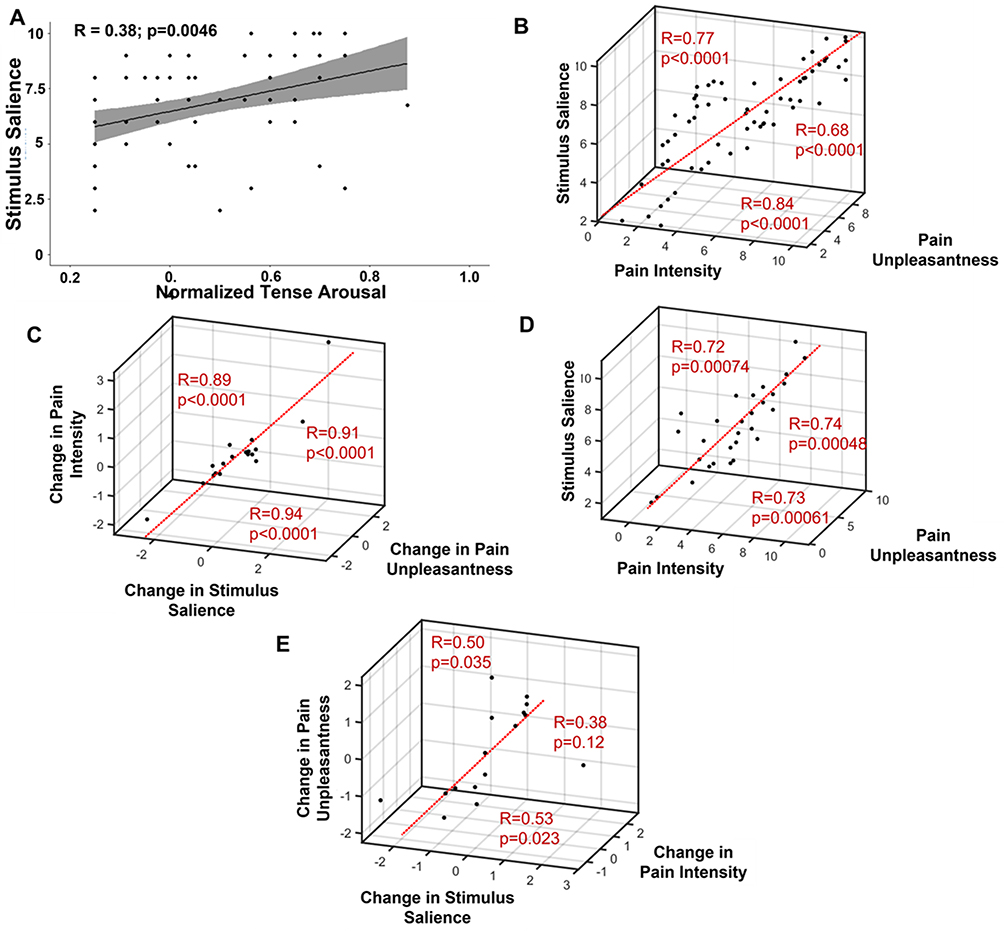 |
Figure 3 Pearson correlations between (A) salience and tense arousal during the continuous performance task with painful stimuli (CPTpain). Pearson correlations among (B) salience, pain intensity and pain unpleasantness and (C) change in salience, change in pain intensity, and change in pain unpleasantness during the continuous performance task with painful stimuli (CPTpain). Pearson correlations among (D) salience, pain intensity and pain unpleasantness and (E) change in salience, change in pain intensity, and change in pain unpleasantness during the habituation phase. In part A, the gray area indicates the 95% confidence interval. |
During the habituation task, in a partial correlation model including tense arousal, pain intensity, pain unpleasantness and salience, tense arousal trended toward being negatively correlated with pain intensity (R=−0.426; t-stat=−1.883; p=0.078), but not correlated with pain unpleasantness (R=0.298; t-stat=1.25; p=0.229) or salience (R=0.292; t-stat=1.22; p=0.240). In bivariate correlations tense arousal was not significantly correlated with pain intensity (R=−0.019; t-stat=0.077; p=0.940), pain unpleasantness (R=0.283; t-stat=1.18; p=0.259), or salience (R=0.284; t-stat=1.18; p=0.254).
To examine the interrelationships of pain intensity, pain unpleasantness and salience across the CPT, as well as the change within the CPT, and to compare this to interrelationships during the habituation period, we used bivariate. For ratings during the CPTpain, we tested bivariate correlations among pain intensity, pain unpleasantness and salience, pain intensity was positively correlated with pain unpleasantness (R=0.839; t-stat=11.12; p<0.0001) and salience (R=0.767; t-stat=8.63; p<0.0001), while pain unpleasantness was positively correlated with salience (R=0.684; t-stat=6.76; p<0.0001) (Figure 3B).
Next, for changes in ratings during CPTpain, we tested bivariate correlation among change in pain intensity, change in pain unpleasantness and change in salience. During the CPT with painful laser stimuli, change in pain unpleasantness and change in salience (R=0.938; t-stat=10.78; p<0.0001) and change in pain intensity (R=0.908; t-stat=8.69; p<0.0001) were positively correlated, while change in pain intensity and change in salience were also significantly positively correlated (R=0.886; t-stat=7.64; p<0.0001) (Figure 3C).
To compare the CPTpain results with ratings taken during the habituation phase of the paradigm, we tested a separate set of bivariate correlations among pain intensity, pain unpleasantness and salience during the painful laser habituation. Consistent with extensive prior literature, pain intensity was positively correlated with pain unpleasantness (R=0.729; t-stat=4.26; p=0.00061) and salience (R=0.721; t-stat=4.16; p=0.00074), while pain unpleasantness was positively correlated with salience (R=0.738; t-stat=4.37; p=0.00048) (Figure 3D).
Finally, during painful laser habituation, change in salience positively correlated with change in pain unpleasantness (R=0.498; t-stat=2.30; p=0.035) and with the change in pain intensity (R=0.534; t-stat=2.52; p=0.023), but the change in pain intensity and change in pain unpleasantness were not significantly correlated (R=0.378; t-stat=1.635; p=0.122) (Figure 3E).
Together these results suggest a tighter coupling of pain intensity, pain unpleasantness and salience during the CPTpain when compared to the habituation task. To test this prediction, we evaluated the differences in bivariate correlation coefficients between phases of our paradigm, comparing habituation to CPTpain. The differences between the habituation phase and CPTpain phase in the correlation coefficients among pain intensity, pain unpleasantness and salience were not significant (PI vs PU: ∆R=0.11; t-stat=0.44; p=0.66; PI vs salience: ∆R=0.046; t-stat=0.18; p=0.86; PU vs salience: ∆R=−0.054; t-stat=−0.22; p=0.83). In contrast, differences between the habituation phase and CPTpain phase in the correlation coefficients among change in pain intensity and change in pain unpleasantness were significant, while the difference between change in pain intensity and change in salience and between change in pain unpleasantness and change in salience were not significant (∆PI vs ∆PU: ∆R=0.53; t-stat=2.50; p=0.024; ∆PI vs ∆salience: ∆R=0.35; t-stat=1.50; p=0.15; ∆PU vs ∆salience: ∆R=0.44; t-stat=1.96; p=0.068). The results in this section were not significantly affected by controlling for age or sex (Supplemental Table 1).
Influence of Anxiety and Neuroticism on Tense Arousal
During CPT with painful laser stimuli, tense arousal positively correlated with state anxiety (R=0.268; t-stat=2.01; p=0.050) and neuroticism (R=0.353; t-stat=2.72; p=0.0088) but not trait anxiety (R=0.132; t-stat=0.96; p=0.341) (Figure 4A; Supplemental Table 2). As state anxiety, trait anxiety and neuroticism are highly correlated, we tested the 4-variable partial correlation model including tense arousal, state and trait anxiety as well as neuroticism. Within the partial correlation model, tense arousal was positively correlated with neuroticism (R=0.291; t-stat=2.20; p=0.033), but not with state anxiety (R=0.134; t-stat=0.997; p=0.333) or trait anxiety (R=−0.142; t-stat=1.04; p=0.305).
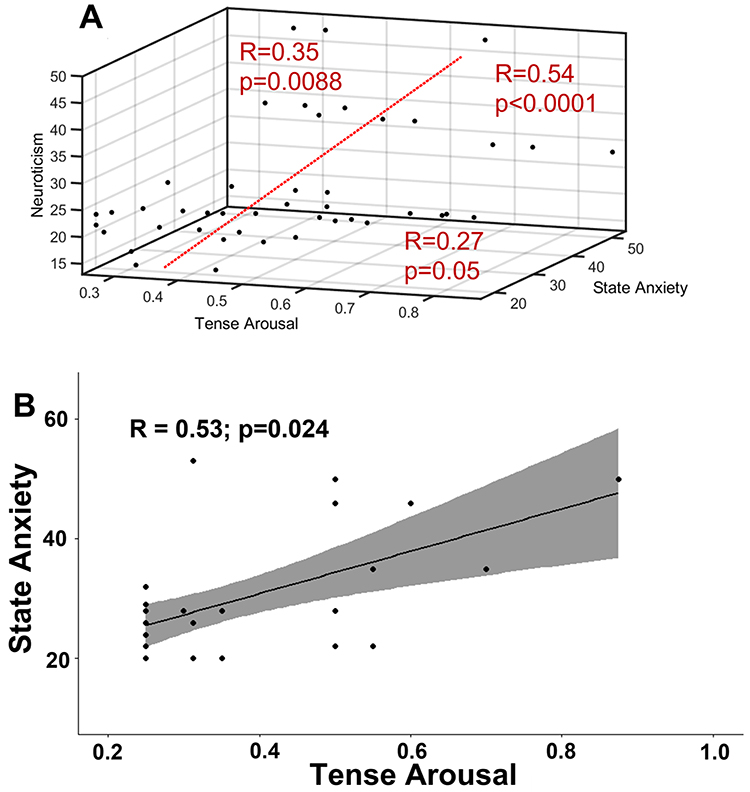 |
Figure 4 Pearson correlations among (A) neuroticism, state anxiety and tense arousal during the continuous performance task with painful stimuli (CPTpain). Pearson correlations between (B) tense arousal and state anxiety during the habituation phase. In part B, the gray area indicates the 95% confidence interval. |
During painful laser habituation, tense arousal positively correlated with state anxiety (R=0.529; t-stat=2.50; p=0.024), but not neuroticism (R=0.401; t-stat=1.751; p=0.099) or trait anxiety (R=0.154; t-stat=0.626; p=0.541) (Figure 4B). In the 4-variable partial correlation model, there was a trend for a positive correlation between tense arousal and state anxiety (R=0.459; t-stat=2.06; p=0.056), but no relationship with trait anxiety (R=−0.262; t-stat=−1.09; p=0.294) or neuroticism (R=0.266; t-stat=1.10; p=0.286). The results in this section were not significantly affected by controlling for age or sex (Supplemental Table 2).
Discussion
In the current report, we extend our results characterizing experimental vigilance to painful stimuli with comparatively slow thermal stimuli13,32 to a CPT with painful rapid laser stimuli (CPTpain). Specifically, we found a vigilance decrement in hits during time on task. There was no change in false alarms, HRT, or FRT. These findings contrasted with our previous results with 1.5s thermal stimuli where there was a vigilance decrement in both false alarms and hits during time on task.13,32 In the current report, using painful laser stimuli, we replicated our finding of a positive relationship of tense arousal with state anxiety during the CPTpain. Consistent with the negative valence and threat associated with painful stimuli that are associated with actual or potential tissue damage by the IASP criteria,47 we found both tense arousal and state anxiety were greater after the CPTpain than before.
During the CPT with painful thermal stimuli delivered by a thermode we previously showed tense arousal positively correlated with pain intensity and pain unpleasantness, but not salience consistent with the relationship between tense arousal and negative valence.13 During phasic painful stimulation, participants typically report pain intensity, pain unpleasantness and salience ratings that are closely correlated with each other.48 Significant psychological manipulations such as meditation or induction of negative moods uncouple these relationships.49,50
While pain intensity and pain unpleasantness were not positively correlated with tense arousal during the CPTpain, as they were previously with painful thermal stimuli delivered with the thermode,13 salience was positively related to tense arousal. Differential peripheral afferent nerve fiber recruitment by thermal stimuli from laser compared to thermode, touch inhibition of certain qualities of pain by the thermode and differences in spatial summation may explain these differences between the experimental results.51–57 The touch inhibition associated with the thermode may be tonic when the thermode remains in place during a multiple stimuli task, or phasic as in our prior study when the thermode is moved from place to place on the skin.13 Finally, we found that pain intensity, pain unpleasantness and salience were positively correlated with each other throughout the CPTpain and during the habituation task. Furthermore, while the change in pain intensity, change in pain unpleasantness, and change in salience were all positively correlated during the CPTpain, there was no positive correlation between change in pain intensity and change in pain unpleasantness during habituation. This suggests these variables are tightly associated when participants attend closely to stimuli during the CPTpain. This contrasts with the habituation task, where participants are free to think of external stimuli or internal thoughts. This may weaken the link between pain intensity and pain unpleasantness, as reported in recent meditation studies.50,58–60
We have now reported a vigilance decrement in hits with thermal stimuli delivered by both thermode and laser. While we found a decrement in hits and false alarms during time on task with the 1.5 s plateau painful thermal stimulus, we only found a decrement in hits with the painful laser stimulus.13 This difference in the form of vigilance decrement is similar to that found in visual vigilance tasks when varying the discriminability of visual stimuli.14 The more discriminable a stimulus, the more easily participants can tell successive stimuli apart from one another in terms of magnitude. In a task with more difficult to discriminate stimuli, time on task is associated with a decrease in hits without a change or with a decrease in false alarms. In contrast, an easier task with more discriminable stimuli causes a vigilance decrement in hits and increment in false alarms.61 The initial discriminability of successive thermal stimuli delivered by the thermode was 0.93±0.006 (mean±SEM), whereas the initial discriminability in the laser vigilance task was 0.83±0.016.32 The effect of change in type of vigilance decrement is generally ascribed to high event rate tasks (≥30 per minute). However, as the system transmitting painful thermal stimuli is dominated by slow conduction velocity primary afferents, we may expect a lower rate of stimuli to saturate the sensory channel for painful stimuli.62,63 Our experimental design reflects this fact; at 15 stimuli per minute there is minimal interaction between successive painful stimuli. More rapid rates of painful stimuli presentation have traditionally led to sensitization.64 Hence, the vigilance decrement we see with thermal stimuli delivered by the laser may be due to sensory channel saturation and not simply high event rate. Careful experiments are required to elucidate this possibility.
During the CPT with painful thermal stimuli delivered by a thermode we previously found tense arousal positively correlated with state anxiety, trait anxiety, and neuroticism.13 During CPT with painful laser stimuli, we found that tense arousal positively correlated with state anxiety and neuroticism but was not related trait anxiety. This largely replicates the results found with painful thermal stimuli delivered by thermode, and fully replicates our previously reported partial correlation results.13
Both tense arousal and state anxiety increased significantly during the CPT pain. During the pre-task period, tense arousal may reflect anxiety related to anticipation of the experimental task. However, tense arousal levels were relatively low at pre-task baseline. Furthermore, the tense arousal and state anxiety reported by the participants during the CPTpain, were positively associated with each other. The relevance of our CPTpain method to potential mechanisms underlying the psychological drivers of pain severity are made clear by the interaction between state anxiety and acute pain. An association of tense arousal with headache intensity in headache has been identified and longitudinal findings in patients suffering from chronic pain have demonstrated a temporally dependent role of anxiety and depression in the exacerbation of chronic pain.5,65 A recent longitudinal study found baseline anxiety in patients with musculoskeletal pain predicted pain severity twelve months later.66 More specific to state anxiety, a recent systematic meta-analysis found that while pre-surgery state anxiety predicts the development post-surgical pain, trait anxiety was only a weak predictor of chronic post-surgery pain spanning multiple procedures and patient groups.67,68 Furthermore, pre-procedural state anxiety predicts the expectation and experience of post-procedural pain following third molar extraction.69,70 In studies of prolonged acute pain such as capsaicin exposure or cold pressor task, state anxiety is associated with pain intensity, tolerance and intensity of capsaicin-induced mechanical hyperalgesia.71,72 Further studies with a control task, such as CPT with warm or vibratory stimuli, should examine whether these changes in state anxiety or tense arousal are potentially related specifically to painful stimuli or are common due to task difficulty.
In the current study, we found that changes in pain intensity, unpleasantness and salience were highly positively correlated during the CPTpain. Positive correlations among change in pain intensity and change in salience, as well as change in pain unpleasantness and change in salience over time on task during habituation were lower. In the case of change in pain intensity versus change in pain unpleasantness were not significant. These findings are consistent with participants maintaining their attention on the sensory characteristics of the painful stimuli, especially when performing the CPTpain. Given that participants seem to be maintaining attention on the sensory characteristics of the painful stimuli, this may be related to each participant’s intrinsic attention to pain.73 This contention requires further research.
Human factors research clearly indicates that performance in a CPT protocol is influenced by attention as well as arousal, reflecting a state of physiological readiness.74–76 Well-established biopsychological models divide arousal into components including tense and energetic arousal.31,77–79 Negative valence is the factor that may distinguish fearful, unpleasant tense arousal from energetic arousal.16,80 In fact, energetic and tense arousal often co-vary except in the presence of pain81 or with time on task in a CPT.41,82 Over time, energetic arousal undergoes a progressive and reproducible decrease,41,83 while there is an increase in tense arousal74,84 and scores in sustained performance tasks.85,86 Tense arousal is related to clinical pain, which suggests that high tense arousal and intrinsic attention to pain may identify patients at risk for chronic pain.81,87
Previous reports have implicated disinhibition of the dorsolateral prefrontal cortex from the amygdala during threat-related hypervigilance, which regulates attentional processes related to nonthreatening visual stimuli in a train of threatening stimuli.88 Prefrontal structures, such as the left dorsolateral prefrontal cortex, are activated during both experimental vigilance and in participants with high levels of trait anxiety during conflict processing. Accordingly, decreased volumes of these structures are found in phobias, panic disorders, and chronic pain.89–92 These overlapping anatomical and behavioral effects suggest that vigilance in chronic pain and anxiety disorders may share common features, consistent with an underlying mechanism mediating the relationships among tense arousal, pain unpleasantness, and trait and state anxiety during vigilance to pain. While our present findings provide further support to the body of evidence on experimental vigilance to pain, our study has some limitations. Primarily, our sample size is relatively small for behavioral findings. However, mitigating against this weakness is that many findings support previously reported results in a different cohort experiencing a similar experimental protocol.13 Furthermore, given the intensive data collection session, common in vigilance studies, rater fatigue may have exacerbated the effects of sustained attention.
Conclusion
We have found support for our previous findings that vigilance to painful stimuli during a CPT with a painful stimulus is characterized by a vigilance decrement in hits. Furthermore, we found additional support that state anxiety positively correlates with tense arousal. During our task pain intensity, unpleasantness and salience ratings were tightly intertwined, and their relationships and changes over time were more related to each other during vigilance to painful laser stimuli during time on task compared to the habituation phase. Performing the CPTpain task was associated with enhanced tense arousal and state anxiety.
Acknowledgments
FAL acknowledges funding from NIH-National Institute of Neurological Disorders and Stroke (R01-NS107602) and Johns Hopkins Neurosurgery Pain Research Institute (JHNPRI) (Grant recipient). TJM acknowledges funding from JHNPRI-Postdoctoral Scholar (Grant recipient). JHC, MIS, SC, JF, and OJB have nothing to acknowledge.
Disclosure
The authors report no conflicts of interest in this work.
References
1. McDermid AJ, Rollman GB, McCain GA. Generalized hypervigilance in fibromyalgia: evidence of perceptual amplification. Pain. 1996;66(2–3):133–144. doi:10.1016/0304-3959(96)03059-X
2. Lautenbacher S, Huber C, Schofer D, et al. Attentional and emotional mechanisms related to pain as predictors of chronic postoperative pain: a comparison with other psychological and physiological predictors. Pain. 2010;151(3):722–731. doi:10.1016/j.pain.2010.08.041
3. Herbert MS, Goodin BR, Pero ST, et al. Pain hypervigilance is associated with greater clinical pain severity and enhanced experimental pain sensitivity among adults with symptomatic knee osteoarthritis. Article. Ann Behav Med. 2014;48(1):50–60. doi:10.1007/s12160-013-9563-x
4. Cathcart S, Petkov J, Pritchard D. Effects of induced stress on experimental pain sensitivity in chronic tension-type headache sufferers. Article. Eur J Neurol. 2008;15(6):552–558. doi:10.1111/j.1468-1331.2008.02124.x
5. Cathcart S, Pritchard D. Time-series analyses of general arousal and headache activity in the natural environment. Headache. 1999;39(3):213–217. doi:10.1046/j.1526-4610.1999.3903213.x
6. Asmundson GJ, Kuperos JL, Norton GR. Do patients with chronic pain selectively attend to pain-related information?: preliminary evidence for the mediating role of fear. Pain. 1997;72(1–2):27–32. doi:10.1016/S0304-3959(97)00010-9
7. Roelofs J, Peters ML, McCracken L, Vlaeyen JWS. The pain vigilance and awareness questionnaire (PVAQ): further psychometric evaluation in fibromyalgia and other chronic pain syndromes. Pain. 2003;101(3):299–306. doi:10.1016/s0304-3959(02)00338-x
8. Roelofs J, Peters ML, Zeegers MP, Vlaeyen JW. The modified Stroop paradigm as a measure of selective attention towards pain-related stimuli among chronic pain patients: a meta-analysis. Eur J Pain. 2002;6(4):273–281. doi:10.1053/eujp.2002.0337
9. Crombez G, Van Ryckeghem DM, Eccleston C, Van Damme S. Attentional bias to pain-related information: a meta-analysis. Pain. 2013;154(4):497–510. doi:10.1016/j.pain.2012.11.013
10. Edwards RR, Fillingim RB. Self-reported pain sensitivity: lack of correlation with pain threshold and tolerance. Eur J Pain. 2007;11(5):594–598. doi:10.1016/j.ejpain.2006.09.008
11. Fortenbaugh FC, DeGutis J, Esterman M. Recent theoretical, neural, and clinical advances in sustained attention research. Ann N Y Acad Sci. 2017;1396(1):70–91. doi:10.1111/nyas.13318
12. Jones EB, Sharpe L, Andrews S, et al. The time course of attentional biases in pain: a meta-analysis of eye-tracking studies. Pain. 2021;162(3):687–701. doi:10.1097/j.pain.0000000000002083
13. Emerson NM, Meeker TJ, Greenspan JD, et al. Missed targets, reaction times, and arousal are related to trait anxiety and attention to pain during an experimental vigilance task with a painful target. J Neurophysiol. 2020;123(2):462–472. doi:10.1152/jn.00331.2019
14. Davies DR, Parasuraman R. The Psychology of Vigilance. Academic Press Inc; 1982:288.
15. Mackworth NH. The breakdown of vigilance during prolonged visual search. Quar J Exper Psychol. 1948;1(1):6–21. doi:10.1080/17470214808416738
16. Yik MSM, Russell JA, Barrett LF. Structure of self-reported current affect: integration and beyond. J Personal Soc Psychol. 1999;77(3):600–619. doi:10.1037/0022-3514.77.3.600
17. Matthews G, Campbell SE, Falconer S, et al. Fundamental dimensions of subjective state in performance settings: task engagement, distress, and worry. Emotion. 2002;2(4):315–340. doi:10.1037/1528-3542.2.4.315
18. Iannetti GD, Leandri M, Truini A, Zambreanu L, Cruccu G, Tracey I. A delta nociceptor response to laser stimuli: selective effect of stimulus duration on skin temperature, brain potentials and pain perception. Clin Neurophysiol. 2004;115(11):2629–2637. doi:10.1016/j.clinph.2004.05.023
19. Bromm B, Treede RD. Nerve fibre discharges, cerebral potentials and sensations induced by CO2 laser stimulation. Hum Neurobiol. 1984;3(1):33–40.
20. Bromm B, Lorenz J. Neurophysiological evaluation of pain. Electroencephalogr Clin Neurophysiol. 1998;107(4):227–253. doi:10.1016/s0013-4694(98)00075-3
21. Markman T, Liu CC, Chien JH, Crone NE, Zhang J, Lenz FA. EEG analysis reveals widespread directed functional interactions related to a painful cutaneous laser stimulus. J Neurophysiol. 2013;110(10):2440–2449. doi:10.1152/jn.00246.2013
22. Chien JH, Liu CC, Kim JH, Markman TM, Lenz FA. Painful cutaneous laser stimuli induce event-related oscillatory EEG activities that are different from those induced by nonpainful electrical stimuli. J Neurophysiol. 2014;112(4):824–833. doi:10.1152/jn.00209.2014
23. Beydoun A, Morrow TJ, Shen JF, Casey KL. Variability of laser-evoked potentials: attention, arousal and lateralized differences. Electroencephalogr Clin Neurophysiol. 1993;88(3):173–181. doi:10.1016/0168-5597(93)90002-7
24. Treede R-D, Magerl W, Baumgärtner U. Laser-evoked potentials for assessment of nociceptive pathways in humans. Pain Forum. 1998;7(4):191–195. doi:10.1016/s1082-3174(98)80005-6
25. Bishop SJ. Neural mechanisms underlying selective attention to threat. Ann N Y Acad Sci. 2008;1129:141–152. doi:10.1196/annals.1417.016
26. Eccleston C, Crombez G. Pain demands attention: a cognitive-affective model of the interruptive function of pain. Psychol Bull. 1999;125(3):356–366. doi:10.1037/0033-2909.125.3.356
27. Zimmer C, Basler HD, Vedder H, Lautenbacher S. Sex differences in cortisol response to noxious stress. Clin J Pain. 2003;19(4):233–239. doi:10.1097/00002508-200307000-00006
28. Price DD, McGrath PA, Rafii A, Buckingham B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain. 1983;17(1):45–56. doi:10.1016/0304-3959(83)90126-4
29. Straube S, Krell MM. How to evaluate an agent’s behavior to infrequent events?-Reliable performance estimation insensitive to class distribution. Front Comput Neurosci. 2014;8:43. doi:10.3389/fncom.2014.00043
30. Kucyi A, Salomons TV, Davis KD. Mind wandering away from pain dynamically engages antinociceptive and default mode brain networks. Proc Natl Acad Sci U S A. 2013;110(46):18692–18697. doi:10.1073/pnas.1312902110
31. Thayer RE. Factor analytic and reliability studies on the activation-deactivation adjective check list. Psychol Rep. 1978;42(3 pt 1):747–756. doi:10.2466/pr0.1978.42.3.747
32. Meeker TJ, Emerson NM, Chien JH, et al. During vigilance to painful stimuli: slower response rate is related to high trait anxiety, whereas faster response rate is related to high state anxiety. Article. J Neurophysiol. 2021;125(1):305–319. doi:10.1152/jn.00492.2020
33. Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psycholl Ass. 1995;7(4):524–532. doi:10.1037/1040-3590.7.4.524
34. McCracken LM, Zayfert C, Gross RT. The pain anxiety symptoms scale: development and validation of a scale to measure fear of pain. Pain. 1992;50(1):67–73. doi:10.1016/0304-3959(92)90113-P
35. Reiss S, Peterson RA, Gursky DM, McNally RJ. Anxiety sensitivity, anxiety frequency and the prediction of fearfulness. Behav Res Ther. 1986;24(1):1–8. doi:10.1016/0005-7967(86)90143-9
36. Spielberger CD. Manual for the State-Trait Anxiety Inventory for Adults (Forms Y1 and Y2). Mind Garden Inc; 1983.
37. Bienvenu OJ, Samuels JF, Costa PT, Reti IM, Eaton WW, Nestadt G. Anxiety and depressive disorders and the five-factor model of personality: a higher- and lower-order personality trait investigation in a community sample. Depress Anxi. 2004;20(2):92–97. doi:10.1002/da.20026
38. McCrae RR, Costa PT. Validation of the five-factor model of personality across instruments and observers. J Pers Soc Psychol. 1987;52(1):81–90. doi:10.1037//0022-3514.52.1.81
39. Leys C, Ley C, Klein O, Bernard P, Licata L. Detecting outliers: do not use standard deviation around the mean, use absolute deviation around the median. J Exper Soc Psychol. 2013;49(4):764–766. doi:10.1016/j.jesp.2013.03.013
40. Galecki A, Burzykowski T. Linear mixed-effects models using r: a step-by-step approach. In: Springer Texts in Statistics. Vol. 417. Springer; 2013:542.
41. Grier RA, Warm JS, Dember WN, Matthews G, Galinsky TL, Parasuraman R. The vigilance decrement reflects limitations in effortful attention, not mindlessness. Human Factors. 2003;45(3):349–359. doi:10.1518/hfes.45.3.349.27253
42. Hofert M. On sampling from the multivariate t distribution. R J. 2013;5(2):129–136. doi:10.32614/RJ-2013-033
43. Kenward MG, Roger JH. An improved approximation to the precision of fixed effects from restricted maximum likelihood. Comput Stat Data Anal. 2009;53(7):2583–2595. doi:10.1016/j.csda.2008.12.013
44. Kenward MG, Roger JH. Small sample inference for fixed effects from restricted maximum likelihood. Biometrics. 1997;53(3):983–997. doi:10.2307/2533558
45. Luke SG. Evaluating significance in linear mixed-effects models in R. Behav Res Methods. 2017;49(4):1494–1502. doi:10.3758/s13428-016-0809-y
46. Kim S. ppcor: an R package for a fast calculation to semi-partial correlation coefficients. Commun Statis Appl Method. 2015;22(6):665–674. doi:10.5351/csam.2015.22.6.665
47. Raja SN, Carr DB, Cohen M, et al. The revised international association for the study of pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982. doi:10.1097/j.pain.0000000000001939
48. Quiton RL, Greenspan JD. Across- and within-session variability of ratings of painful contact heat stimuli. Article. Pain. 2008;137(2):245–256. doi:10.1016/j.pain.2007.08.034
49. Loggia ML, Mogil JS, Bushnell MC. Experimentally induced mood changes preferentially affect pain unpleasantness. J Pain. 2008;9(9):784–791. doi:10.1016/j.jpain.2008.03.014
50. Zorn J, Abdoun O, Bouet R, Lutz A. Mindfulness meditation is related to sensory-affective uncoupling of pain in trained novice and expert practitioners. Eur J Pain. 2020;24(7):1301–1313. doi:10.1002/ejp.1576
51. Greenspan JD, Roy EA, Caldwell PA, Farooq NS. Thermosensory intensity and affect throughout the perceptible range. Somato Motor Res. 2003;20(1):19–26. doi:10.1080/0899022031000083807
52. Price DD, McHaffie JG, Larson MA. Spatial summation of heat-induced pain: influence of stimulus area and spatial separation of stimuli on perceived pain sensation intensity and unpleasantness. J Neurophysiol. 1989;62(6):1270–1279. doi:10.1152/jn.1989.62.6.1270
53. Mancini F, Nash T, Iannetti GD, Haggard P. Pain relief by touch: a quantitative approach. Pain. 2014;155(3):635–642. doi:10.1016/j.pain.2013.12.024
54. Nahra H, Plaghki L. Modulation of perception and neurophysiological correlates of brief CO2 laser stimuli in humans using concurrent large fiber stimulation. Somatosens Mot Res. 2003;20(2):139–147. doi:10.1080/0899022031000105172
55. Morin C, Bushnell CM. Temporal and qualitative properties of cold pain and heat pain: a psychophysical study. Pain. 1998;74(1):67–73. doi:10.1016/s0304-3959(97)00152-8
56. Svensson P, Rosenberg B, Beydoun A, Morrow TJ, Casey KL. Comparative psychophysical characteristics of cutaneous CO2 laser and contact heat stimulation. Somatosens Mot Res. 1997;14(2):113–118. doi:10.1080/08990229771114
57. Dusch M, van der Ham J, Weinkauf B, et al. Laser-evoked potentials mediated by mechano-insensitive nociceptors in human skin. Eur J Pain. 2016;20(5):845–854. doi:10.1002/ejp.810
58. Wells RE, Collier J, Posey G, et al. Attention to breath sensations does not engage endogenous opioids to reduce pain. Pain. 2020;161(8):1884–1893. doi:10.1097/j.pain.0000000000001865
59. Brown CA, Jones AKP. Meditation experience predicts less negative appraisal of pain: electrophysiological evidence for the involvement of anticipatory neural responses. Pain. 2010;150(3):428–438. doi:10.1016/j.pain.2010.04.017
60. Perlman DM, Salomons TV, Davidson RJ, Lutz A. Differential effects on pain intensity and unpleasantness of two meditation practices. Emotion. 2010;10(1):65–71. doi:10.1037/a0018440
61. Parasuraman R, Mouloua M. Interaction of signal discriminability and task type in vigilance decrement. Percept Psychophys. 1987;41(1):17–22. doi:10.3758/BF03208208
62. Price DD, Hu JW, Dubner R, Gracely RH. Peripheral suppression of first pain and central summation of second pain evoked by noxious heat pulses. Pain. 1977;3(1):57–68. doi:10.1016/0304-3959(77)90035-5
63. Zotterman Y. Touch, pain and tickling: an electro-physiological investigation on cutaneous sensory nerves. J Physiol. 1939;95(1):1–28. doi:10.1113/jphysiol.1939.sp003707
64. Price DD, Hayes RL, Ruda M, Dubner R. Spatial and temporal transformations of input to spinothalamic tract neurons and their relation to somatic sensations. J Neurophysiol. 1978;41(4):933–947. doi:10.1152/jn.1978.41.4.933
65. Lerman SF, Rudich Z, Brill S, Shalev H, Shahar G. Longitudinal associations between depression, anxiety, pain, and pain-related disability in chronic pain patients. Psychosom Med. 2015;77(3):333–341. doi:10.1097/PSY.0000000000000158
66. Bair MJ, Poleshuck EL, Wu J, et al. Anxiety but not social stressors predict 12-month depression and pain severity. Clin J Pain. 2013;29(2):95–101. doi:10.1097/AJP.0b013e3182652ee9
67. Giusti EM, Lacerenza M, Manzoni GM, Castelnuovo G. Psychological and psychosocial predictors of chronic postsurgical pain: a systematic review and meta-analysis. Pain. 2021;162(1):10–30. doi:10.1097/j.pain.0000000000001999
68. Masselin-Dubois A, Attal N, Fletcher D, et al. Are psychological predictors of chronic postsurgical pain dependent on the surgical model? A comparison of total knee arthroplasty and breast surgery for cancer. J Pain. 2013;14(8):854–864. doi:10.1016/j.jpain.2013.02.013
69. van Wijk AJ, de Jongh A, Lindeboom JA. Anxiety sensitivity as a predictor of anxiety and pain related to third molar removal. J Oral Maxillofac Surg. 2010;68(11):2723–2729. doi:10.1016/j.joms.2010.06.174
70. Wang TF, Wu YT, Tseng CF, Chou C. Associations between dental anxiety and postoperative pain following extraction of horizontally impacted wisdom teeth: a prospective observational study. Medicine. 2017;96(47):e8665. doi:10.1097/md.0000000000008665
71. Cimpean A, David D. The mechanisms of pain tolerance and pain-related anxiety in acute pain. Health Psychol Open. 2019;6(2):2055102919865161. doi:10.1177/2055102919865161
72. Meeker TJ, Schmid AC, Liu Y, et al. During capsaicin-induced central sensitization, brush allodynia is associated with baseline warmth sensitivity, whereas mechanical hyperalgesia is associated with painful mechanical sensibility, anxiety and somatization. Eur J Pain. 2021;25(9):1971–1993. doi:10.1002/ejp.1815
73. Adams G, Harrison R, Gandhi W, van Reekum CM, Salomons TV. Intrinsic attention to pain is associated with a pronociceptive phenotype. Pain Rep. 2021;6(2):e934. doi:10.1097/pr9.0000000000000934
74. Kamzanova AT, Kustubayeva AM, Matthews G. Use of EEG workload indices for diagnostic monitoring of vigilance decrement. Human Factors. 2014;56(6):1136–1149. doi:10.1177/0018720814526617
75. Krupski A, Raskin DC, Bakan P. Physiological and personality correlates of commission errors in an auditory vigilance task. Psychophysiology. 1971;8(3):304–311. doi:10.1111/j.1469-8986.1971.tb00460.x
76. Gevins A, Smith ME, McEvoy L, Yu D. High-resolution EEG mapping of cortical activation related to working memory: effects of task difficulty, type of processing, and practice. Cereb Cortex. 1997;7(4):374–385. doi:10.1093/cercor/7.4.374
77. Thayer RE. Measurement of activation through self-report. Psychol Rep. 1967;20(2):663–678. doi:10.2466/pr0.1967.20.2.663
78. Matthews G, Desmond PA. Task-induced fatigue states and simulated driving performance. Q J Exp Psychol A. 2002;55(2):659–686. doi:10.1080/02724980143000505
79. Warm JS, Parasuraman R, Matthews G. Vigilance requires hard mental work and is stressful. Human Factors. 2008;50(3):433–441. doi:10.1518/001872008X312152
80. Schimmack U, Rainer R. Experiencing activation: energetic arousal and tense arousal are not mixtures of valence and activation. Emotion. 2002;2(4):412–417. doi:10.1037/1528-3542.2.4.412
81. Cathcart S, Pritchard D. Relationships between arousal-related moods and episodic tension-type headache: a biopsychological study. Headache. 1998;38(3):214–221. doi:10.1046/j.1526-4610.1998.3803214.x
82. Thayer RE. The Biopsychology of Mood and Arousal. Oxford University Press; 1990.
83. Helton WS, Warm JS. Signal salience and the mindlessness theory of vigilance. Acta Psychol. 2008;129(1):18–25. doi:10.1016/j.actpsy.2008.04.002
84. Pattyn N, Neyt X, Henderickx D, Soetens E. Psychophysiological investigation of vigilance decrement: boredom or cognitive fatigue? Physiol Behav. 2008;93(1–2):369–378. doi:10.1016/j.physbeh.2007.09.016
85. Matthews G, Davies DR, Holley PJ. Cognitive predictors of vigilance. Hum Factors. 1993;35(1):3–24. doi:10.1177/001872089303500101
86. Matthews G, Warm JS, Smith AP. Task engagement and attentional resources. Human Factors. 2017;59(1):44–61. doi:10.1177/0018720816673782
87. Murphy AI, Lehrer PM. Headache versus nonheadache state: a study of electrophysiological and affective changes during muscle contraction headaches. Behavioral Medicine. 1990;16(1):23–30. doi:10.1080/08964289.1990.9934588
88. Bishop SJ. Neurocognitive mechanisms of anxiety: an integrative account. Trends Cogn Sci. 2007;11(7):307–316. doi:10.1016/j.tics.2007.05.008
89. Berkowitz RL, Coplan JD, Reddy DP, Gorman JM. The human dimension: how the prefrontal cortex modulates the subcortical fear response. Rev Neurosci. 2007;18(3–4):191–207. doi:10.1515/REVNEURO.2007.18.3-4.191
90. Bishop SJ. Trait anxiety and impoverished prefrontal control of attention. Nat Neurosci. 2009;12(1):92–98. doi:10.1038/nn.2242
91. Langner R, Eickhoff SB. Sustaining attention to simple tasks: a meta-analytic review of the neural mechanisms of vigilant attention. Psychol Bull. 2013;139(4):870–900. doi:10.1037/a0030694
92. Seminowicz DA, Moayedi M. The Dorsolateral Prefrontal Cortex in Acute and Chronic Pain. J Pain. 2017;18(9):1027–1035. doi:10.1016/j.jpain.2017.03.008
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.