Back to Journals » Advances in Medical Education and Practice » Volume 12
Viewpoints on Healthcare Delivery Science Education Among Practicing Physicians in a Rural State
Authors Weeks K ![]() , Swanson M
, Swanson M ![]() , Manorot A, Conley G, Nellis J, Charlton M, Reed A
, Manorot A, Conley G, Nellis J, Charlton M, Reed A ![]()
Received 6 October 2020
Accepted for publication 11 December 2020
Published 11 January 2021 Volume 2021:12 Pages 29—39
DOI https://doi.org/10.2147/AMEP.S285463
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Kristin Weeks, 1, 2 Morgan Swanson, 1, 2 Amanda Manorot, 3 Gabriel Conley, 4, 5 Joseph Nellis, 6 Mary Charlton, 2 Alan Reed 7
1Medical Scientist Training Program, Carver College of Medicine, University of Iowa, Iowa City, IA, USA; 2Department of Epidemiology, College of Public Health, University of Iowa, Iowa City, IA, USA; 3Department of Obstetrics and Gynecology, University of Michigan, Ann Arbor, MI, USA; 4Medical Training Program, Carver College of Medicine, University of Iowa, Iowa City, IA, USA; 5Department of Business, Tippie College of Business, University of Iowa, Iowa City, IA, USA; 6Department of Surgery, Duke University, Durham, NC, USA; 7Department of Surgery, University of Iowa Hospitals and Clinics, Iowa City, IA, USA
Correspondence: Alan Reed
Department of Surgery, University of Iowa Hospitals and Clinics, SE 427 GH, 200 Hawkins Drive, Iowa City, IA 52242, USA
Tel +1 319-356-0537
Email [email protected]
Introduction: Healthcare Delivery Science Education (HDSE) covers important aspects of the business of medicine, including, operations management, managerial accounting, entrepreneurship, finance, marketing, negotiations, e-health and policy/advocacy. We need to investigate and understand practicing physicians’ viewpoints on HDSE in order to inform interventions capable of preventing the double loss phenomena and improving medical and continuing medical education opportunities in HDSE. This qualitative study aims to provide a rich, contextualized understanding of the HDSE experiences and interests of physicians practicing in a rural state through the intensive study of particular cases.
Materials and Methods: We interviewed 18 practicing physicians from a rural, Midwestern state over the telephone about their viewpoints on past experiences obtaining HDSE, interest in HDSE, barriers to pursuing HDSE, and interest in an example HDSE certificate program.
Results: Salient themes in our study were that physicians were interested in HDSE and believed HDSE could lead to improved patient care and practice efficiency. However, many of the respondents had not received longitudinal, diversified, didactic or practical HDSE. Time limited many physicians from pursuing HDSE opportunities. Many physicians in the study were interested in the example HDSE certificate program.
Discussion and Conclusions: Physicians in our qualitative study were interested in obtaining HDSE and had not received diversified, didactic HDSE in the past. Our research suggests innovative HDSE programs will likely be utilized and pursued if they are developed.
Keywords: healthcare delivery science, rural, management, continuing medical education, healthcare leadership
A Letter to the Editor has been published for this article.
A Response to Letter has been published for this article.
Introduction
The United States’ healthcare industry has grown exceedingly complex over the last 20 years. Some reimbursement is transitioning from fee-for-service to value-based models with associated risk.1–3 Moreover, technologies and governmental policies continue to rapidly evolve.1–3 Even as these changes are being implemented, the cost of healthcare in the United States continues to rise reaching $3.5 trillion in 2017 and amounting to 17.9% of the Gross Domestic Product.4–6
Due to their unique clinical viewpoints, physicians across all specialties are being called upon to assume wide-ranging formal and informal leadership and management roles in healthcare. In this variety of roles, they are faced with addressing a diverse set of priorities, from adapting to fee-for-service models, implementing technologies and policies, to improving medical outcomes and maintaining patient satisfaction.3,7 These leadership roles can range from managing a practice or committee, conducting a quality improvement project, restructuring their data management, to running an entire hospital system. The successful integration of physicians into leadership positions of all kinds has been demonstrated previously. For example, many hospitals with the highest quality scores have physician leaders.8 Likewise, hospital systems with physicians in management roles have been shown to have high management performance, operational effectiveness, and clinical quality.9–12
However, as physicians seek to assume leadership positions in healthcare, many are limited by financial resources, a lack of training, and time.3,7 A lack of training for leadership and management positions can result in a “double loss” phenomenon, or the loss of the physician’s clinical skilled-time when they devote more time to leadership, as well as the loss of expert healthcare leadership, if the physician lacks training and consummate skillsets.3 The lack of leadership training among practicing physicians might be due to limited exposure to formal healthcare delivery science education (HDSE) in medical school and continuing medical education (CME).8,9,11,13,14 HDSE covers important aspects of the business of medicine, including, operations management, managerial accounting, entrepreneurship, finance, marketing, negotiations, e-health and policy/advocacy. HDSE practicably helps physicians who are called upon to take on either formal or informal leadership roles.15–18
There is a lack of data in the literature evaluating practicing physicians’ experiences with and interest in HDSE. We need to investigate and understand practicing physicians’ viewpoints on HDSE in order to inform interventions capable of preventing the double loss phenomena when physicians take on formal or informal leadership roles, improve medical and continuing medical education opportunities in HDSE, and enhance physician success in leadership roles and the quality of healthcare delivery. It is particularly pressing to understand the viewpoints of practicing physicians working in a rural state where a growing health professional shortage complicates efforts to provide effective healthcare and illuminates disparities in practicing physicians’ HDSE. An improved understanding of these physicians’ viewpoints on HDSE will allow for the development of important tools, educational interventions, and systemic changes to help these physicians successfully address important issues in their state, including access and management obstacles.19,20
Through our qualitative research, we aimed to explore a rich, contextualized understanding of the HDSE experiences and interests of physicians practicing in a rural state through the intensive study of cases.21 In this qualitative study, practicing physicians in a rural state were interviewed about their past experiences with HDSE, current attitudes toward HDSE, interest in a limited model HDSE certificate program, and barriers to pursuing HDSE.
Methods
Instrument Creation
We created a structured interview guide to be used in telephone interviews that included both open- and closed-ended questions. The interview guide was goal-driven toward investigating our research question and was informed by a review of the literature as well as Roger’s Diffusion of Innovation Theory framework. The interview guide was pilot-tested and re-evaluated after initial interviews; no changes were made to the guide over the course of the study. The interview guide was structured to ask physicians about their specialty, years in practice, practice environment and the four areas of investigation, which included physicians’ past HDSE experiences, interest in future HDSE, barriers to HDSE, and viewpoints on a limited model certificate program (detailed verbatim in Box 1).
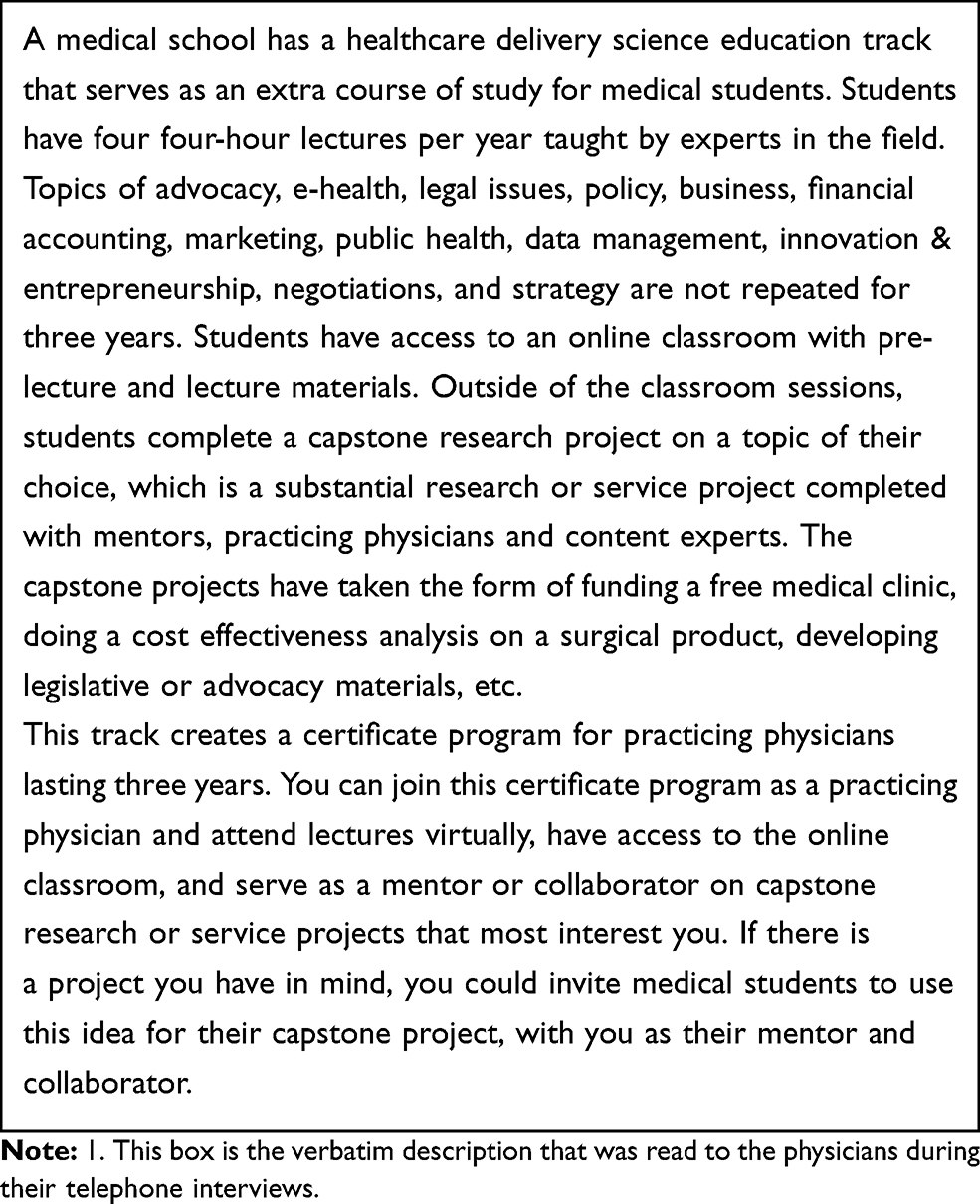 |
Box 1 Description of Our Healthcare Delivery Science Education Certificate Program for Practicing Physicians |
Theoretical Framework
We applied Rogers’ Diffusion of Innovation Theory framework toward designing the description of the limited model certificate program and soliciting respondents’ reactions to it.22,23 The Diffusion of Innovation Theory posits that people are more likely to adopt an innovation when the innovation is seen to have a relative advantage, compatibility, overcomes complexity, trialability, and observability.23 The example certificate program that was described to physician interviewees had a didactic and project component and was structured similarly to the program used for a medical student elective at our college. Our goal in including a project component was to provide participants with a real-life example of how to use learned information in a clinical setting to achieve tangible results. To reduce complexity in our certificate description, we did not discuss specific logistics of the hypothetical online platform nor additional requirements or grading schemes. Rather, we presented a straightforward certificate program requiring a relatively minimal time commitment (4 sessions per year, 4 hours per session) with the goal of providing physicians the basic fundamentals of HDSE (as opposed to a mastery level one might encounter in a degree bearing program) delivered in a virtual format for their convenience. We also asked physician participants to define their ideal time frame and level of commitment to reduce any subconscious barriers to trialability. After the analysis was completed, we applied the Diffusion of Innovation Theory five-component framework to summarize participants’ reactions to this particular example certificate learning option.
Participant Recruitment and Enrollment
We aimed to enroll an equal number of family medicine physicians and non-family medicine physicians to ensure we were able to observe differences, if they existed, between primary care providers and specialists. We were particularly interested in these two groups because it is likely they differ in practice structure (private practice versus hospital based), and their perceived needs and motivations for pursuing HDSE might differ as well. Participants were eligible if they were practicing, licensed physicians in Iowa in 2018 and 2019. Licensing was confirmed through the Iowa Board of Medical Examiners.
Two sampling and recruiting strategies were used. Family medicine physicians were sampled from the only family medicine research network in our state, which is composed of 310 family medicine physicians in 75 of our state’s 99 counties. The staff of the research network faxed recruitment letters to a random sample of 40 family medicine physicians after excluding the members in their network already participating as subjects in other research studies. Fax (versus email or telephone) is the only method used for communication by the research network. Non-family medicine physicians were recruited by maximum variation sampling across diverse hospital systems in our state and medical specialties. Two research teams at our institution emailed recruitment letters to the work email addresses of 12 non-family medicine physicians. Faxes were sent in batches of 20 and emails were sent in batches of six starting in January 2019.
Non-responders were re-contacted two additional times through fax (family medicine) and email (non-family medicine) within 2 weeks of each prior correspondence. In each correspondence, physicians were provided an informational invitation letter for the study, elements needed for informed consent, and a form to fill out that indicated their willingness to participate and three times/days that worked best for interviews.
We aimed to recruit physicians until we determined that saturation was achieved in each stratum, or when no additional themes were found.24 We achieved saturation after 40 family medicine and 12 non-family medicine physicians had been recruited (Figure 1).
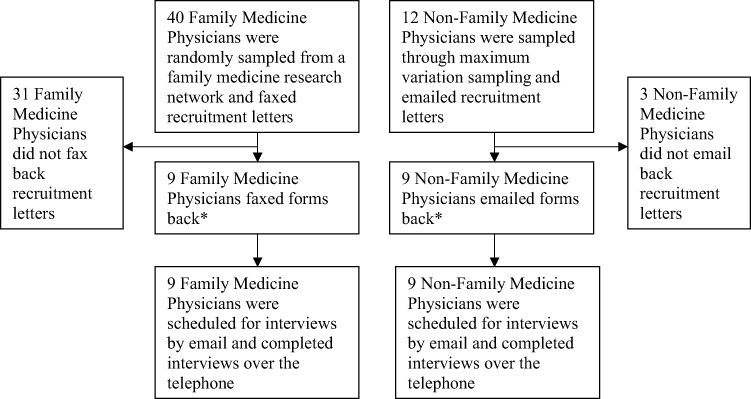 |
Figure 1 Recruitment strategy Notes: This figure provides a description of the recruitment strategy and study population that was enrolled. *Forms indicated a willingness to participate and three times/days that the physicians were available for interviews. |
Data Collection
One trained graduate research assistant (KW, Bachelor of Science, female, doctoral student with qualitative graduate experience) scheduled and conducted all interviews. Interviews were all formally scheduled by email and conducted over the telephone at the primary time/date preference that was provided by each physician. Participants were not familiar with the interviewer before the research encounter and learned that she was a student during interviews; they did not know her degree program, educational goals or other characteristics. Prior to each interview, participants provided informed consent, including the publication of anonymized responses. The consent process was approved by the IRB (#201901815) of the University of Iowa.
All interviews were conducted by telephone using a structured interview guide and were audio-recorded. Probing questions were used to clarify response options and illicit additional explanation. Further, participants were asked to reflect, add additional comments, and clarify any of their responses at the end of each interview. Participants were not re-contacted after the initial interview. The interviews lasted an average of 15 minutes. For all interviews, HDSE was defined as
The business of medicine, including, operations management, managerial accounting, entrepreneurship, finance, marketing, negotiations, e-health and policy/advocacy.
Participants were mailed twenty dollars as compensation following their interview. The last interview was conducted in April 2019.
Data Analysis
Telephone interviews were transcribed verbatim and reviewed for accuracy. Participants were not asked to review transcripts, nor to provide feedback about findings. Member checking was not conducted due to appropriate probing during interviews, invited reflection following interviews, active monitoring for consistency between responses during interviews, and concern about physicians’ time limitations.
Two independent reviewers (KW and MBS) evaluated all interview transcripts and assigned themes to the four areas being investigated.25 Disagreements between independent reviewers were noted, and discrepancies were addressed through collaborative discourse until a mutual agreement was reached.5 Deviant cases were analyzed and discussed following the subset of a grounded theory known as constant comparison.26 The themes generated for each area of investigation and the relative salience of themes were compared between the family medicine versus non-family medicine physician stratum. Due to the lack of difference between these groups, results were presented for the physician cohort overall.
Description of Study Participants
Eighteen physicians, nine family medicine physicians (23% participation rate) and nine non-family medicine physicians (75% participation rate) participated in our qualitative interview study (Image 2). Non-family medicine physicians were trained in pediatrics (2), internal medicine (2), surgical subspecialties (3), and psychiatry (1). Respondents practiced at both hospital and group practices worked for both publicly and privately owned systems, and were spread across a diverse set of healthcare systems in our state. Some held leadership positions, including one physician who was the head of a committee. Some were involved in the management of their own practices/departments and some had no formal or informal leadership roles at all. Most respondents were male. Two-thirds reported practicing in urban or suburban locations, and one-third reported practicing in a rural area (Table 1). Half had been practicing for less than 20 years.
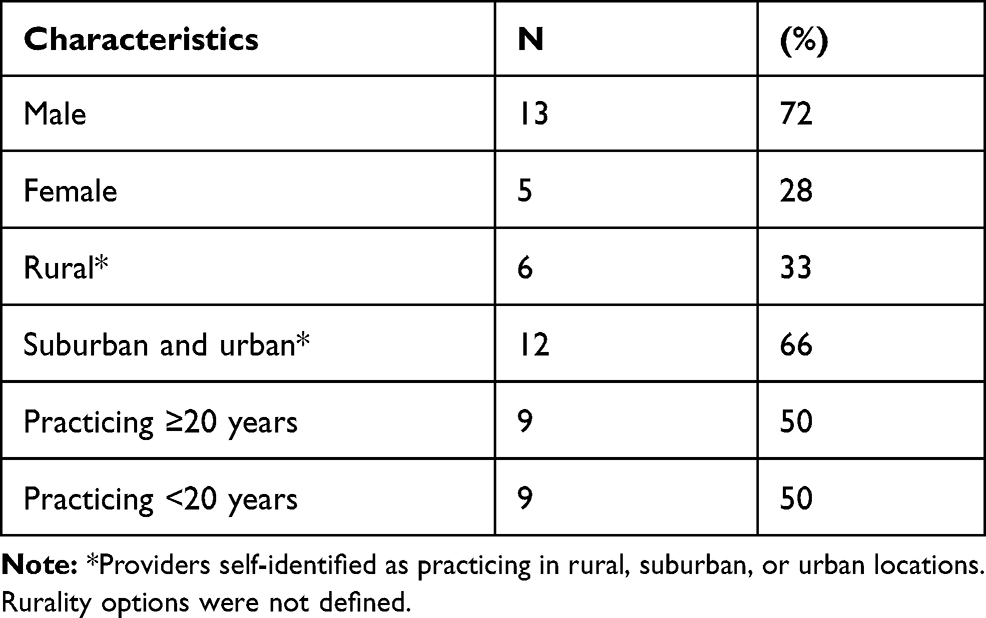 |
Table 1 Participant Demographics |
Results
Within our four areas of investigation (past experiences, current interest, barriers, and interest in a certificate program), we identified 14 subthemes, or 2–5 subthemes for each area of investigation (Table 2).
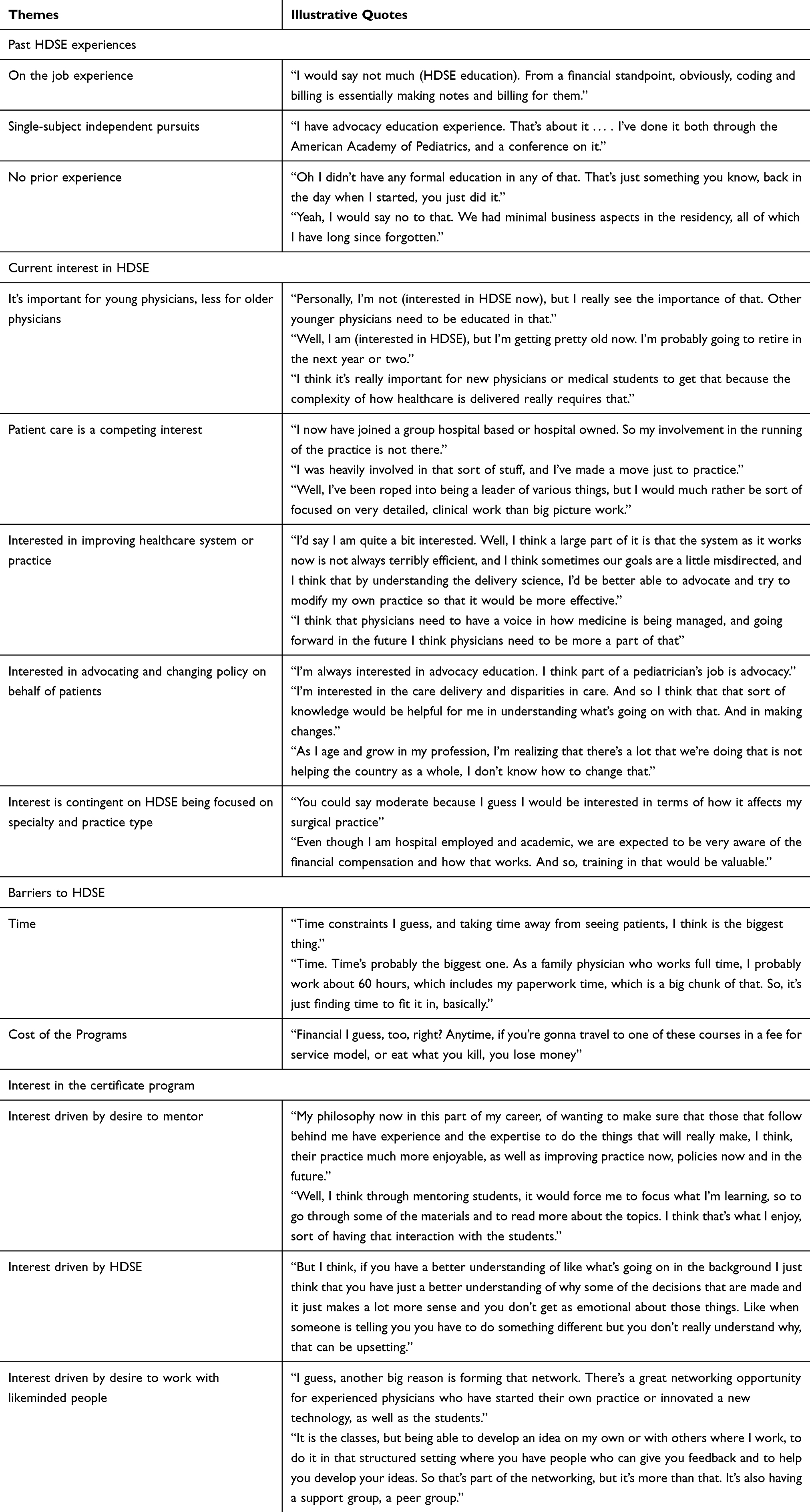 |
Table 2 Themes of Practicing Physicians’ Viewpoints on Healthcare Delivery Science Education |
Past HDSE Experiences
Most practicing physicians stated that HDSE was not a significant part of their medical education or their continuing education. A salient theme among practicing physicians was that they had not received structured didactic HDSE after residency through their place of employment. The physicians that had received unstructured HDSE at their place of employment had done so through on-the-job-training. On-the-job-training was described as topic-specific education, such as medical billing, leadership, or financial responsibility. On-the-job-training occurred alongside new non-clinical obligations. For example, physicians received on-the-job-training as a new member of a special committee or when newly assuming an administrative role. Another salient theme among practicing physicians was that they had single-subject opportunities in HDSE, such as conference lectures and lectures through their respective national organizations. These single-subject opportunities were only completed when specifically sought out by practicing physicians based on their own interests and initiatives. Finally, a salient theme among practicing physicians was that they lacked formal education on HDSE topics both during training and after completing residency. Some physicians mentioned they were optimistic that the amount of HDSE discussed in medical training and on-the-job training was slowly improving with time.
Current Interest in HDSE
Many practicing physicians were interested in obtaining HDSE, especially when delivered in a platform specific to their profession, practice type, and specialty. Interested participants thought HDSE would be valuable to them and, by extension, their patients. A growing dissatisfaction with the state of healthcare and a current inability to change the parts of their practice operations or their healthcare system they disliked seemed paramount to practicing physicians’ interest. Correcting inefficiencies, improving care delivery, and having a voice in how physicians are managed motivated providers’ interest in HDSE. Another salient theme among physicians was the desire to be able to improve their advocacy and policy literacy in order to optimize outcomes for their patient population, such as by actively supporting mental health funding reform. Commonly reported HDSE topics of interest were data management, policy and advocacy, public health, business management (operations), and financial management.
Disinterest in HDSE at the time of the interview was typically attributed to later career stage and competing goals and priorities, rather than a lack of interest in the topics. For example, some expressed they anticipated a decreased future interest because they were too advanced in their careers. Others were completely committed to seeing patients and did not want to detract any time away from patient care. Some physicians noted certain topics in HDSE did not interest them, but no one stated they were well informed on multiple HDSE topics or uninterested in every topic.
Barriers to HDSE
The overwhelming barrier to obtaining HDSE was time. Practicing physicians indicated many sources of time constraints, including family obligations, clinical duties, research efforts, email burdens and note writing. Physicians felt they were working at their limit most of the time. However, they still believed they could make time for HDSE if it were delivered in a flexible manner that required a modest time commitment. Other barriers were the cost of existing programs, cost of traveling to conferences, and a lack of programs targeted to physicians. Physicians also discussed life events that may make certain timeframes more optimal for HDSE than others, such as when their children left for college or when they did not have visiting trainees.
Interest in a Certificate Program
Most physicians were interested in the example certificate program that was presented to them. Physicians perceived the certificate program to have a relative advantage, compatibility, reduced complexity, trialability, and observability (Table 3). The main drivers for interest in the certificate were the subject matter, mentoring, and networking opportunities. Most saw professional advancement and leadership value in the didactic, expert-led lectures; however, some stated they were just curious to learn about HDSE from an intellectual standpoint. Practicing physicians also saw personal value in sharing their experiences with students. Some stated they felt a responsibility to their profession to help medical students. Finally, practicing physicians were interested in pursuing an HDSE certificate program for the purposes of forming relationships, such as connecting with new like-minded people. Some thought they could use their gained knowledge to build momentum in the workplace, solve an existing problem, and/or strengthen culture.
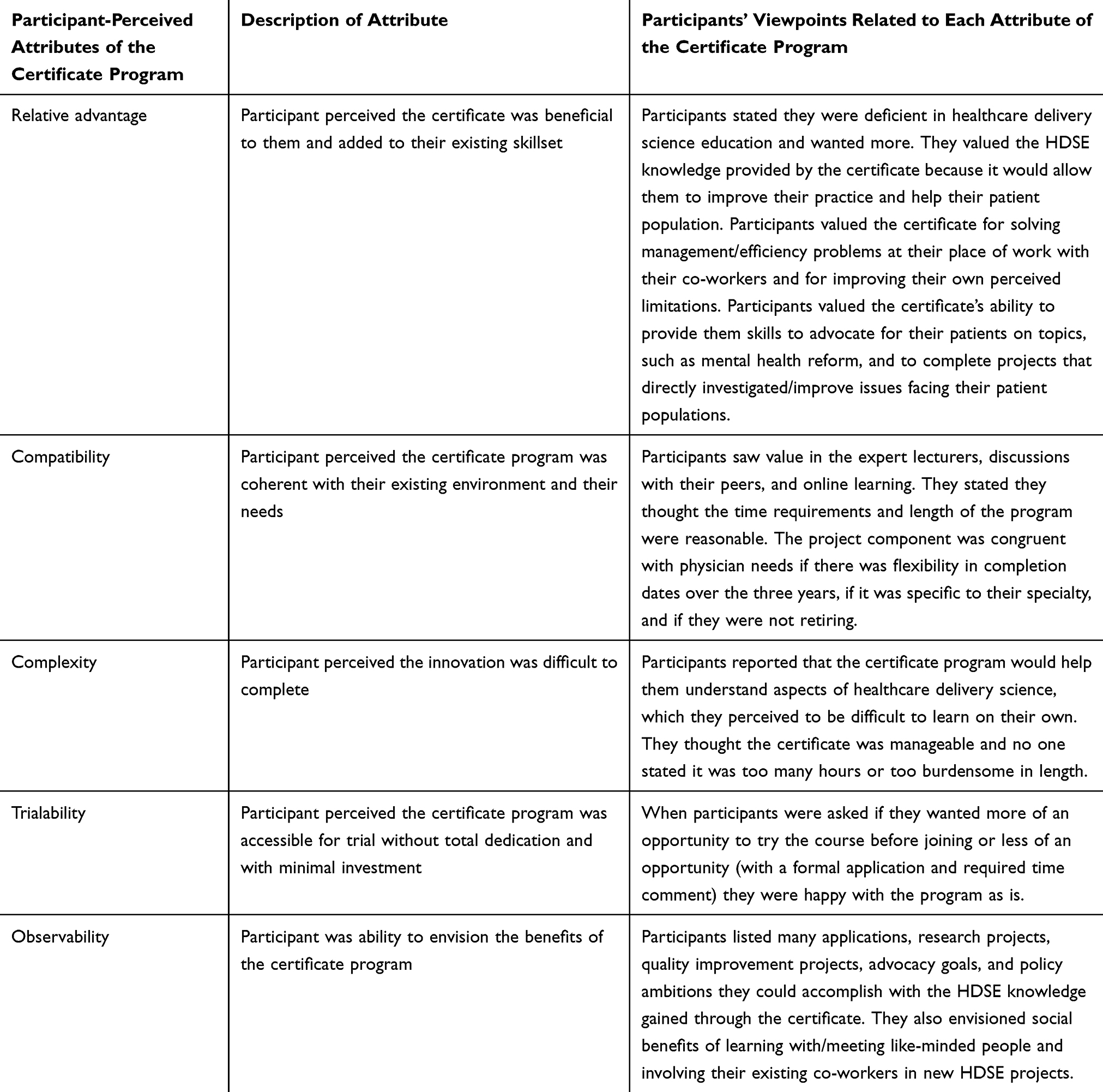 |
Table 3 Perceptions of the Certificate Program: An Outline Utilizing the Diffusion of Innovation Theory |
Discussion
Many of the physicians in our study were interested in HDSE and expressed the belief that HDSE could lead to improved patient care and practice efficiency. However, many of the respondents had not received longitudinal, diversified, didactic or practical HDSE. This appeared to be caused by systemic- and participant-level barriers including a lack of opportunities for HDSE. It is possible that hospitals/practice systems lack the specialization and expertise needed to build lasting training structures, the resources to outsource training, the capacity to prioritize training for all physicians, or the knowledge that there is an unmet need.3,27,28 For those physicians who had received HDSE, education was limited to periodic single-day conference-style opportunities and on-the-job-training in specific topics related to administrative needs. While this approach (termed “scatter-shot”) is popular and possibly effective in the short term, it is unlikely to create the scale and sustainability in physician leadership needed to champion the systemic change participants desired.3
Time and cost were the limitations that kept most physicians from pursuing HDSE. Low-cost or free online learning platforms (webinars, longitudinal distance-learning certificate programs done in short segments) are potential solutions.29 The steady rise of certificates, CME electives, and non-masters level opportunities for physicians over the last decade shows a promising trend in reducing participant barriers.30,31 However, it is likely that the time constraints of practicing physicians will continue to force many physicians to rely on the HDSE they received in medical school and residency training.32,33 Consequently, the medical education system should prioritize important HDSE topics and integrate them into the existing accreditation and education requirements.28,32,33
The main motivations physicians reported for pursuing HDSE were their desire to improve an aspect of their healthcare system or practice, and their desire to help their patient populations. This finding suggests many physicians saw a direct application for HDSE. Physicians interviewed were largely dissatisfied with policies and operations and lacked the skillsets to institute or advocate for a change. Concern for this was the prime motivation for our study. We are not surprised physicians were motivated by their desire to improve work conditions, environments, and policies. Three of the four factors that Linzer and others identified as causing burnout in healthcare professions include an inability to change work conditions, an inefficient work environment, and a misalignment of values and missions between physicians and the hierarchical executives or system.34–37 As physicians continue to perceive that changes need to be made and they are increasingly managed with standardized algorithms, workflows, and reimbursement policies, it is likely the motivations for the skillsets to change these will have more importance.
Physicians in our study were interested in the proposed limited model of the longitudinal HDSE certificate program because it allowed for didactic expert-led education, mentoring of future physicians, and networking with their peers. During interviews, physicians expressed an interest in applying the example certificate program’s project requirement to develop independent and collaborative efforts to solve the various access and management issues facing their practices and hospital systems. This could indicate physicians perceived their colleagues needed HDSE applied skillsets as well, or that they believe there are needed projects that require the work and commitment of a team. Either way, it is important future HDSE programs teach applied skills as well as didactic knowledge.27,38
Strengths and Limitations
Recall bias is a possible limitation among physicians remembering their educational experiences. However, we utilized signposting between each section and probing after each question to help physicians formulate their best answers. Member checking was not conducted. Interviewer bias was mitigated through recorded interviews and multiple coders. Interviewee reporting bias was mitigated by the ability to opt out of questions, and reassurance of data safety measures and de-identification.
We used a sample size similar to other articles with similar study designs, as well as an established saturation approach in our analysis.39–41 The physicians in this study originated from a single rural state and were chosen from two different sources using purposeful convenience sampling. Thus, the themes generated in this study may not be representative of the viewpoint of all physician populations nor generalizable to other populations. However, the goal of this study and qualitative research is not to generalize results, but to gain a deeper, non-numerical understanding of a culture.42 Qualitative studies analyze subjects’ experiences and thoughts in order to attain an insider’s view of the group under study.42 The information and insights related to the culture experienced by this group of practicing physicians can inform other researchers of potential cultures in their own study populations, and encourage further qualitative studies of other physician populations, generalizable quantitative studies of larger physician populations, and intervention studies to meet the HDSE needs of specific physician groups.
Qualitative studies that assess differences in viewpoints between other strata, such as gender, rurality of practice, fellowship training, rurality of patient population, and prior training experience are needed. This study was of physicians in a rural state. These physicians may have had low access to academic medical centers for continual training and education, high probability of working at a small practice and/or hospital, more difficulty recruiting and retaining peers with leadership expertise, more patients with government insurance or uninsured status, and higher likelihoods of working in settings owned by a healthcare system due to the limited viability of the rural independent practice. Further studies are needed with comparisons across rurality and within urban states.
Conclusion
The physicians in our qualitative study were interested in obtaining HDSE and had not received diversified, didactic HDSE in the past. Thus, there is a need for HDSE and the best time for the training is likely to be in the early stages of medical careers or during medical training. Development of further HDSE opportunities could provide physicians with the skills needed to make changes to their work environments and policies, enable them to help their patient populations, and increase their successes when participating in informal and formal leadership and management roles. Our research suggests innovative HDSE programs will likely be utilized and pursued if they are developed. Further research is needed in other physician populations’ HDSE culture and experiences.
Acknowledgments
We would like to thank Telligen Community Initiative, the Iowa Research Network (IRENE), the University of Iowa Surgery Department, Hugh Hansen, Clay Walker, Hayley Hansen, Katherine Merritt, Usha Balakrishnan, Diane Berwald, Jaclyn Searls, Kelli Parsons, Savannah Borman, and Heather Healy.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
A grant from Telligen Community Initiative obtained by the student leadership board of the Healthcare Delivery Science, Management, and Policy Distinction track at the University of Iowa funded this study. No one on the research team received a direct payment or increase in salary from Telligen Community Initiative for conducting this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chaudry J, Jain A, McKenzie S, Schwartz RW. Physician leadership: the competencies of change. J Surg Educ. 2008;65(3):213–220. doi:10.1016/j.jsurg.2007.11.014
2. Sonnino RE. Health care leadership development and training: progress and pitfalls. J Healthc Leadersh. 2016;8:19–29. doi:10.2147/JHL.S68068
3. Myers CG, Pronovost PJ. Making management skills a core component of medical education. Acad Med. 2017;92(5):582–584. doi:10.1097/ACM.0000000000001627
4. Centers for Medicare & Medicaid Services. National Health Expenditures 2017 Highlights. Centers for Medicare & Medicaid Services; 2019.
5. Silbaugh BR, Leider HL. Physician leadership is key to creating a safer, more reliable health care system. Physician Exec. 2009;35(5):12–16.
6. Faerber A, Andrews A, Lobb A, et al. A new model of online health care delivery science education for mid-career health care professionals. Healthc. 2019;7(4). doi:10.1016/j.hjdsi.2018.12.002.
7. Pearl RM, Fogel AL. New physicians will need business school skills. NEJM Catalyst. 2017;3(4).
8. Goodall AH. Physician-leaders and hospital performance: is there an association? Soc Sci Med. 2011;73(4):535–539. doi:10.1016/j.socscimed.2011.06.025
9. Castro PJ, Dorgan SJ, Richardson B. A healthier health care system for the United Kingdom. McKinsey Q. 2008;1–5.
10. Mountford J, Webb C. When clinicians lead: the McKinsey Quarterly. Healthc Leadersh Rep. 2009;28(5):1–3.
11. Falcone RE, Satiani B. Physician as hospital chief executive officer. Vasc Endovascular Surg. 2008;42(1):88–94. doi:10.1177/1538574407309320
12. Tasi MC, Keswani A, Bozic KJ. Does physician leadership affect hospital quality, operational efficiency, and financial performance? Health Care Manage Rev. 2019;44(3):3. doi:10.1097/HMR.0000000000000173
13. Hartley K. Untangling approaches to management and leadership across systems of medical education. BMC Health Serv Res. 2016;16(2):33–43. doi:10.1186/s12913-016-1391-9
14. Patel MS, Davis MM, Lypson ML. Advancing medical education by teaching health policy. N Engl J Med. 2011;364(8):695–697. doi:10.1056/NEJMp1009202
15. Gonzalo JD, Dekhtyar M, Starr SR, et al. Health systems science curricula in undergraduate medical education: identifying and defining a potential curricular framework. Acad Med. 2017;92(1):123–131. doi:10.1097/ACM.0000000000001177
16. DeFlitch C, Geeting G, Paz HL. Reinventing emergency department flow via healthcare delivery science. HERD. 2015;8(3):105–115. doi:10.1177/1937586715580949
17. Starr SR, Reed DA, Essary A, et al. Science of health care delivery as a first step to advance undergraduate medical education: a multi-institutional collaboration. Healthcare. 2017;5(3):98–104. doi:10.1016/j.hjdsi.2017.01.003
18. Gupta A, Sharda R. Improving the science of healthcare delivery and informatics using modeling approaches. Decis Support Syst. 2013;55(2):423–427. doi:10.1016/j.dss.2012.10.001
19. Shipman SA, Wendling A, Jones KC, Kovar-Gough I, Orlowski JM, Phillips J. The decline in rural medical students: a growing gap in geographic diversity threatens the rural physician workforce. Health Aff. 2019;38(12):2011–2018. doi:10.1377/hlthaff.2019.00924
20. Probst J, Eberth JM, Crouch E. Structural urbanism contributes to poorer health outcomes for rural America. Health Aff. 2019;38(12):1976–1984. doi:10.1377/hlthaff.2019.00914
21. Polit DF, Beck CT. Generalization in quantitative and qualitative research: myths and strategies. Int J Nurs Stud. 2010;47(11):1451–1458. doi:10.1016/j.ijnurstu.2010.06.004
22. Moseley SF. Everett Rogers’ diffusion of innovations theory: its utility and value in public health. J Health Commun. 2004;9(S1):149–151. doi:10.1080/10810730490271601
23. Rogers EM. Diffusion of Innovations. Simon and Schuster; 2010.
24. Guest G, Bunce A, Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. 2006;18(1):59–82. doi:10.1177/1525822X05279903
25. Luborsky MR. The Identification and Analysis of Themes and Patterns. 1994.
26. Rodriguez JG. Commentary: grounded theory and the constant comparative method. Br Med J. 1998;316(7137):1064–1066.
27. Butterworth K, Hayes B, Zimmerman M. Remote and rural: do mentors enhance the value of distance learning continuing medical education? Educ Health. 2011;24(3):539.
28. Goodall A, Stoller JK. The future of clinical leadership: evidence for physician leadership and the educational pathway for new leaders. BMJ Leader. 2017;1(2):8. doi:10.1136/leader-2017-000010
29. Atreja A, Mehta NB, Jain AK, et al. Satisfaction with web-based training in an integrated healthcare delivery network: do age, education, computer skills and attitudes matter? BMC Med Educ. 2008;8(1):48. doi:10.1186/1472-6920-8-48
30. Herzlinger RE, Kumar V, Schulman K, Staman K. Innovation in Health Care Education: A Call to Action. 2015.
31. Rotenstein L, Perez K, Wohler D, et al. Preparing health professions students to lead change. Leadersh Health Serv. 2019;32(2):182–194. doi:10.1108/LHS-02-2018-0011
32. Bohmer RM. Managing the new primary care: the new skills that will be needed. Health Aff. 2010;29(5):1010–1014. doi:10.1377/hlthaff.2010.0197
33. Emanuel EJ. Changing premed requirements and the medical curriculum. JAMA. 2006;296(9):1128–1131. doi:10.1001/jama.296.9.1128
34. Rothenberger DA. Physician burnout and well-being: a systematic review and framework for action. Dis Colon Rectum. 2017;60(6):567–576. doi:10.1097/DCR.0000000000000844
35. Linzer M, Manwell LB, Williams ES, et al. Working conditions in primary care: physician reactions and care quality. Ann Intern Med. 2009;151(1):
36. Linzer M, Konrad TR, Douglas J, et al. Managed care, time pressure, and physician job satisfaction: results from the physician worklife study. J Gen Intern Med. 2000;15(7):441–450. doi:10.1046/j.1525-1497.2000.05239.x
37. Linzer M, Visser MR, Oort FJ, Smets EM, McMurray JE, de Haes HC. Predicting and preventing physician burnout: results from the United States and the Netherlands. Am J Med. 2001;111(2):170–175. doi:10.1016/S0002-9343(01)00814-2
38. Nelson EA, McGuire AL. The need for medical education reform: genomics and the changing nature of health information. Genome Med. 2010;2(3):18. doi:10.1186/gm139
39. Saunders B, Sim J, Kingstone T, et al. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quant. 2018;52(4):1893–1907. doi:10.1007/s11135-017-0574-8
40. Boddy CR. Sample size for qualitative research. Qual Market Res Int J. 2016;19(4):426–432. doi:10.1108/QMR-06-2016-0053
41. Charmaz K, Belgrave L. Qualitative interviewing and grounded theory analysis. SAGE Handb Interview Res. 2012;2:347–365.
42. Tuli F. The basis of distinction between qualitative and quantitative research in social science: reflection on ontological, epistemological and methodological perspectives. Ethiop J Educ Sci. 2010;6(1).
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.