Back to Journals » Patient Preference and Adherence » Volume 16
Utilization of Hydroxyurea Among Patients Diagnosed with Sickle Cell Disease in Jazan, Saudi Arabia
Authors Gohal GA ![]() , Gosadi IM
, Gosadi IM ![]() , Cittana Iqbal BA, Ghazwani YH, Daghriri AM, Shugairi AA, Daghriri KA, Zurayyir AJ, Nemri AA, Abdulhaq MA
, Cittana Iqbal BA, Ghazwani YH, Daghriri AM, Shugairi AA, Daghriri KA, Zurayyir AJ, Nemri AA, Abdulhaq MA
Received 20 September 2022
Accepted for publication 1 November 2022
Published 8 November 2022 Volume 2022:16 Pages 3059—3067
DOI https://doi.org/10.2147/PPA.S390568
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Gassem A Gohal,1 Ibrahim M Gosadi,2 Basheer Ahmed Cittana Iqbal,3 Yahya H Ghazwani,3 Amal M Daghriri,3 Ahmad A Shugairi,4 Khaled A Daghriri,5 Atyaf J Zurayyir,6 Abdulrhman A Nemri,7 Monera A Abdulhaq8
1Department of Pediatrics, Faculty of Medicine, Jazan University, Jazan, Saudi Arabia; 2Department of Family and Community Medicine, Faculty of Medicine, Jazan University, Jazan, Saudi Arabia; 3Department of Pediatric Hematology and Oncology, Prince Mohammed Bin Nasser Hospital, Jazan, Saudi Arabia; 4Department of Adult Hematology and Oncology, Prince Mohammed Bin Nasser Hospital, Jazan, Saudi Arabia; 5Department of Internal Medicine, Prince Sultan Military Medical City, Riyadh, Saudi Arabia; 6Department of Obstetrics and Gynecology, King Abdulaziz Medical City, Riyadh, Saudi Arabia; 7Department of General Surgery, Security Force Hospital, Riyadh, Saudi Arabia; 8Faculty of Medicine, Jazan University, Jazan, Saudi Arabia
Correspondence: Ibrahim M Gosadi, Department of Family and Community Medicine, Faculty of Medicine, Jazan University, P.O. Box: 2349, Jazan, 82621, Saudi Arabia, Tel +966 562137711, Email [email protected]
Purpose: The early diagnosis of sickle cell disease (SCD) patients and getting appropriate treatment are crucial for improving clinical outcomes. This study aims to assess the use of hydroxyurea among patients diagnosed with SCD and assess factors influencing the attitude toward the medication and the reasons for discontinuation.
Methods: This study was a cross-sectional investigation targeting parents or caregivers of children diagnosed with SCD in the Jazan region of Saudi Arabia. Data were collected from tertiary healthcare hospitals via a self-administered questionnaire. The questionnaire was composed of sections measuring the participants’ demographics, the number of children diagnosed with SCD, the use of hydroxyurea, and the parents’ beliefs about hydroxyurea.
Results: There were 301 parents or caregivers recruited. The majority of the recruited participants were mothers (54.5%), and nearly half of the sample were older than 35. More than 80% of the participants declare that one or more of their children are receiving hydroxyurea to manage SCD. The majority of participants declared that using hydroxyurea reduced the frequency of body pain episodes, emergency department visits, and hospital admissions. Participants’ major concern about the use of hydroxyurea was related to the fear of weakening their immunity (29.5%) and hydroxyurea’s perceived effect on fertility (16.8%). Furthermore, 52 (18%) of the participants declared that the use of hydroxyurea to manage the disease was stopped; the main reasons for stopping was their belief that hydroxyurea had side effects and its impact on weakening of their immune system.
Conclusion: The findings indicate the importance of increasing the role of clinicians in educating patients and caregivers about the use of hydroxyurea and its benefits.
Keywords: sickle cell disease, hydroxyurea, Jazan, Saudi Arabia
Introduction
Hemoglobin disorders have been estimated to affect five percent of the world’s population, with low- and middle-income countries reporting a higher incidence of the disease.1,2 Sickle cell disease (SCD) is a hemoglobin disorder that results from a genetic mutation, causing the development of the S hemoglobin and the impairment of hemoglobin. The mutant S hemoglobin impairs the function of red blood cells, leading to several clinical manifestations, including hemolytic anemia and the incidence of vaso-occlusion that can affect several body organs,3 impacting the overall quality of life and mental health of patients affected with the disease.4,5
SCD can have life-threatening and long-term ramifications and may reduce life expectancy. Early diagnosis of patients affected with SCD, prompt identification of sickle cell crises, and appropriate treatment can be crucial for improving clinical outcomes.6 Although treatments that can improve the outcome of the disease are available, several socioeconomic factors can influence access,7 and adherence to the medications, leading to an increased disease burden in some areas of the world.8
Management plans for SCD can be individualized and vary according to the clinical presentation and occurrence of acute or chronic complications. Management can include but is not limited to using analgesics, antibiotics, oxygenation, hydration, or blood transfusions. Furthermore, disease-modifying therapies can be used to manage SCD, such as hydroxyurea and stem cell transplantation. Furthermore, disease-modifying therapies can be used to manage SCD, such as hydroxyurea, L glutamine, voxelotor, crizanlizumab gene therapy and stem cell transplantation.
Hydroxyurea is an antineoplastic agents that inhibits ribonucleotide reductase; increases HbF in RBC red cell hydration and nitric oxide production; and decreases the expression of red cell adhesion molecules, white blood cell count, reticulocytes, and platelets.9 The current evidence indicates that hydroxyurea is a safe, well-tolerated, and effective medication for managing SCD. Hydroxyurea is a standard treatment option for SCD and is used in patients over the age of 9 months due to its impact on increasing fetal hemoglobin,10 irrespective of the disease’s severity.11 Nonetheless, despite the recent evidence-based recommendations describing hydroxyurea use as a standard management option for SCD, there is variability in its utilization due to availability, medication accessibility, and compliance.12
SCD is a relatively common health condition in Saudi Arabia, with a prevalence of 4.2% for sickle-cell trait and 0.26% for SCD.13 One of the measures established in Saudi Arabia for the prevention of SCD is a premarital screening program.14 Furthermore, Saudi citizens can benefit from the freely available healthcare services provided by multiple healthcare establishments, including access to healthcare, utilization of laboratory and imaging services, and free medications for SCD patients. Hydroxyurea is considered a standard treatment option of patients with SCD in Saudi Arabia and can be prescribed in capsules and syrup forms. In addition to its prescription, education on hydroxyurea is provided during standard health care via verbal communication between the treating physicians and the parents or caregivers. Studies that assessed the utilization of hydroxyurea for SCD in Saudi Arabia indicated a reduction in vaso-occlusive crises, hospital admissions and stays,15,16 and the need for blood transfusion.17
Although hydroxyurea is considered a safe and effective drug for treating SCD, patients’ discontinuation of hydroxyurea and resistance to utilization among SCD patients has been reported. In a study involving 298 SCD patients from Oman, it was reported that the prevalence of discontinuing hydroxyurea was 57%, where the most common reason for discontinuation was the suspected adverse side effects of the drug.18 In a similar study conducted in Saudi Arabia, which measured the awareness of hydroxyurea in the Eastern province of Saudi Arabia, involving a sample of 107 SCD patients, it was reported that less than 70% of the patients had heard of hydroxyurea and half of those who received the medication discontinued it.19
The southern region of Saudi Arabia has a high prevalence of SCD compared to other regions in the country. The evidence concerning the utilization and acceptance of hydroxyurea among SCD in the southern region is currently lacking. This study aims to assess the utilization of hydroxyurea among patients diagnosed with SCD. Furthermore, this study aims to assess the factors influencing the patients’ attitude toward the medication and the reasons for discontinuing it.
Methodology
Study Context
This study was a cross-sectional investigation targeting parents or caregivers of children diagnosed with SCD in the Jazan region of Saudi Arabia. Data were collected between November 2020 and March 2022 from pediatric department of tertiary healthcare hospitals in the Jazan region. Ethical approval to conduct the investigation was granted via the Research Ethics Committee of Jazan Health Directory, Saudi Ministry of Health (ethical approval number 165/2020, dated April 16, 2020). The participation of the parents or caregivers was performed after securing the informed consent that the study would be performed in accordance with the Declaration of Helsinki.
Data Collection Tool
Data were collected via a self-administered questionnaire. The questionnaire was composed of sections measuring the participants’ demographics, the number of children diagnosed with SCD, the use of hydroxyurea, and the parents’ beliefs about hydroxyurea with a total of 14 items. The questionnaire was based on similar studies conducted in the United States.20,21 Consultants in pediatric medicine reviewed the questionnaire items to ensure contents validity of the questionnaire. Furthermore, to test the suitability of the questionnaire for the community of interest, the questionnaire was piloted on a sample of 30 parents, clarifying the items and time needed to complete the questionnaire.
Data Collection and Analysis
The targeted population of the current investigation was identified in the inpatient pediatric departments of the targeted hospitals. Identified participants were included if they agreed to participate and had a minimum of one child with SCD. Parents or caregivers who were not associated with a child with SCD were excluded. Trained medical students identified the subjects, assessed meeting the identified subjects of the inclusion criteria, and distributed the questionnaires. To enhance the clarity of the questionnaires to the participants, the medical students were present at the time of completing the questionnaire and could respond to queries raised by the participants. The students collected the distributed questionnaires upon completion.
Due to the difficulty of identifying and accessing the study sample, a non-random and convenient sampling approach was used. The sample size estimation was based on the study by Alsalman et al, which investigated the use of hydroxyurea among SCD patients in the Eastern province of Saudi Arabia.19 The StatCal function of EpiInfo was used to estimate the sample size for the current investigation. Based on a prevalence of 50% of discontinuation of hydroxyurea, a 95% confidence level, and a five percent margin of error, a sample of 384 was estimated.
Data Analysis
Data analysis was performed via the Statistical Package for Social Sciences (version 25). Due to the questionnaire’s reliance on binary and categorical data, frequencies and proportions were used to report the study’s findings. However, the question concerning reasons for stopping hydroxyurea was open, enabling parents and caregivers to write down their own beliefs. The answers were screened by a single investigator to group similar responses and to identify the main reasons for stopping the medication.
Results
A total of 319 parents and caregivers met the inclusion criteria and were approached for the current investigation, of whom 301 agreed to participate. Table 1 summarizes the demographic characteristics of the participants. The majority of the recruited participants were mothers (54.5%), nearly half of the sample were older than 35 years of age, and 89.7% were married at the time of recruitment. Most were government employees or housewives, and less than half of the sample had a university education. Finally, more than half of the sample had more than one child diagnosed with SCD.
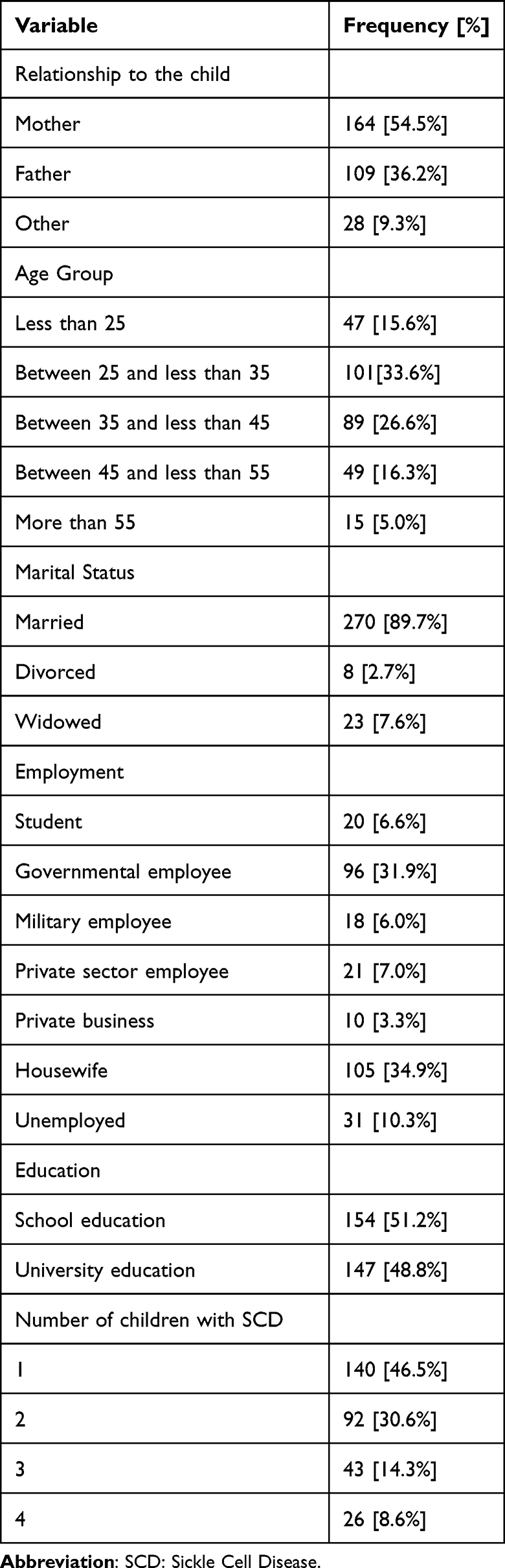 |
Table 1 Demographic Characteristics of 301 Parents and Caregivers of Children Diagnosed with SCD in Jazan, Saudi Arabia |
Table 2 illustrates the participants’ perceptions about the use of hydroxyurea for managing SCD. The majority of the participants believe that hydroxyurea has a beneficial impact on reducing episodes of pain, particularly chest pain, shortness of breath, and the risk of stroke among SCD patients. When the participants were asked about the possible mechanism of hydroxyurea for managing SCD, the majority indicated that hydroxyurea increases blood hemoglobin. The major concern of the participants about using hydroxyurea was related to the fear of weakened immunity (29.5%) and hydroxyurea’s perceived effect on fertility (16.8%). Finally, The most common source of information concerning use of hydroxyurea for SCD management was their treating physician (44.5%).
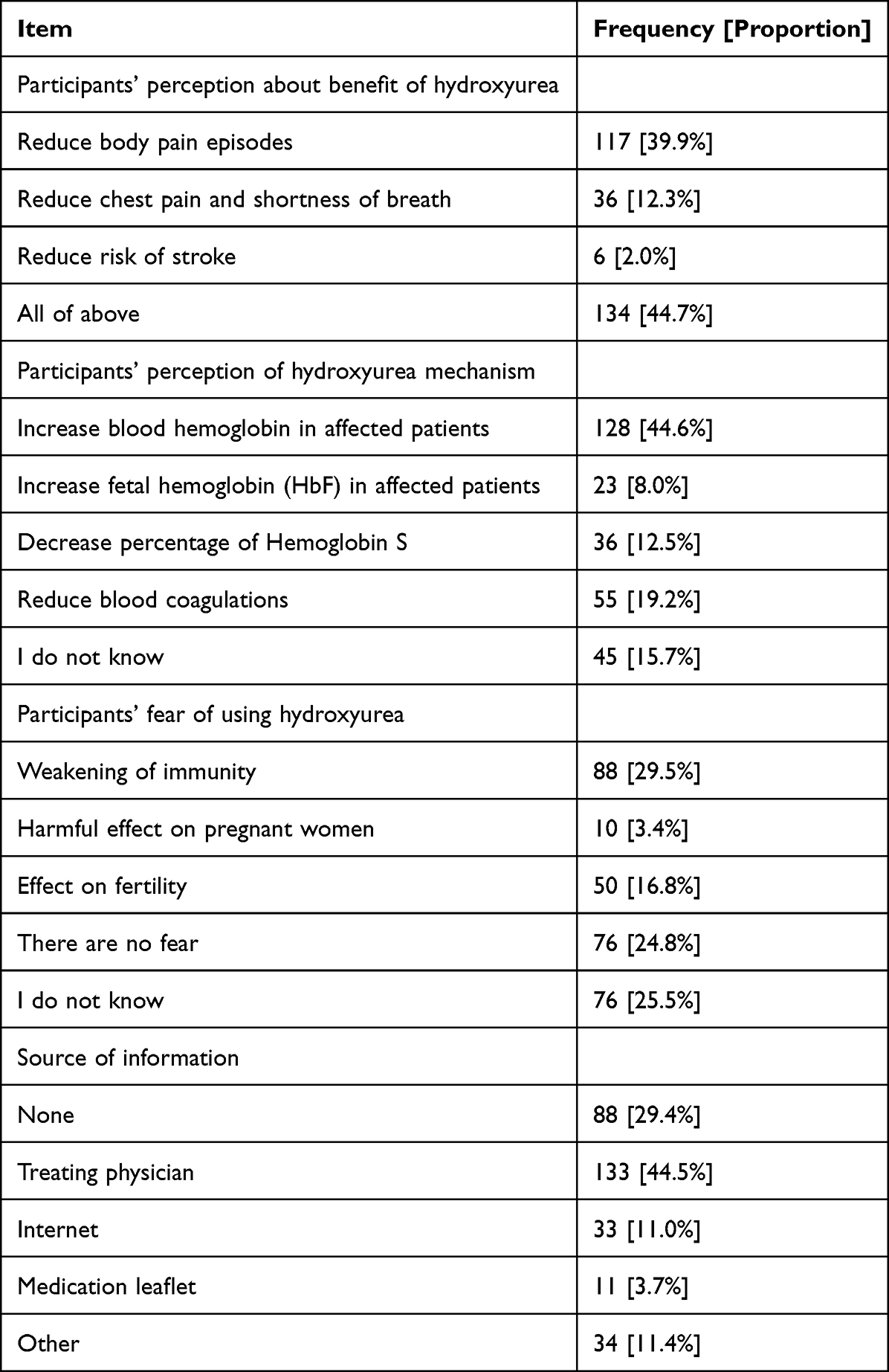 |
Table 2 Perception of 301 Parents or Caregivers of Children Diagnosed with SCD About the Use of Hydroxyurea |
Using hydroxyurea for children diagnosed with SCD in the Jazan region is illustrated in Table 3. More than 80% of the participants declared that one or more of their children are receiving hydroxyurea to manage SCD. The majority of the participants declared that the use of hydroxyurea was associated with a reduction in body pain episode frequency, emergency department visits, and hospital admission. Nonetheless, 52 (18%) participants declared that the use of hydroxyurea to manage the disease was stopped; the main reason was that they believed hydroxyurea had side effects and could weaken their immune systems.
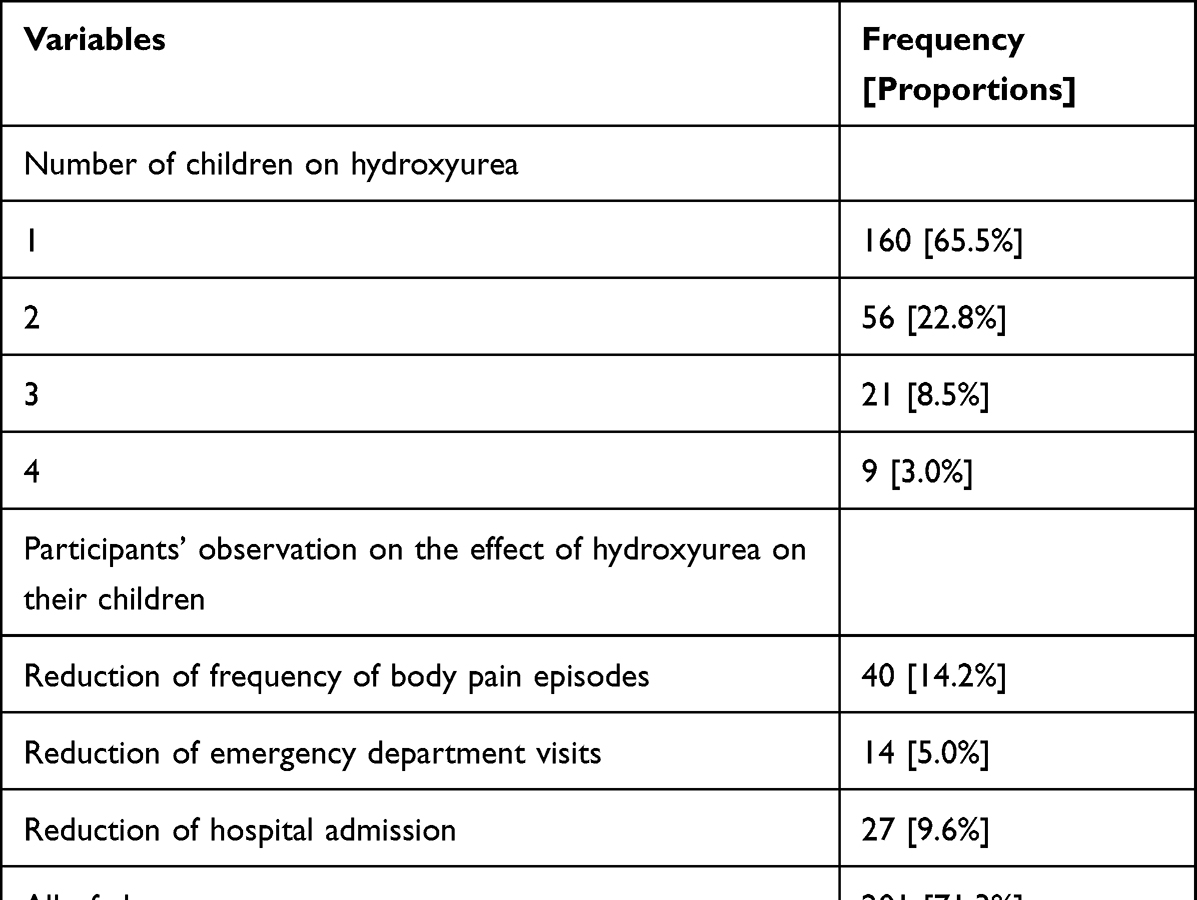 |
Table 3 Use of Hydroxyurea Among Children Diagnosed with SCD as Reported by 301 Parents or Caregivers in Jazan, Saudi Arabia |
Discussion
This study was a cross-sectional investigation that targeted the parents or caregivers of children affected with SCD. Among the identified sample, a good overall perception of the beneficial effects of hydroxyurea in managing SCD was observed. However, nearly one-fifth of the sample reported stopping hydroxyurea use in their affected children because they believed hydroxyurea use was associated with the developed side effects and thought it was weakening their children immune system.
The findings of our investigation can be compared to similar national and international investigations. A study conducted in the Eastern province of Saudi Arabia by Alsalman et al that included a sample of 107 adult patients with SCD indicated that only 63% initiated hydroxyurea treatment, of whom 50% discontinued the treatment. The main reason for discontinuation was preparation for pregnancy and the development of side effects.19 Although our sample was restricted to the use of hydroxyurea among children with SCD, the use of hydroxyurea was higher (80%). Furthermore, the study by Alsalman et al and the current investigation detected similar reasons for stopping hydroxyurea treatment because of fears of the side effects.
The findings of our investigation indicate a relatively good perception of the beneficial impacts of using hydroxyurea to manage SCD, and it can be argued that this perception may explain the higher acceptance of hydroxyurea for managing SCD among our sample in comparison to the findings of similar literature. In a study that included a sample of 298 Omani SCD patients, only 128 were on hydroxyurea. Furthermore, among the 128 using hydroxyurea, 57% discontinued the medication, the fear of side effects being the most common factor for discontinuation.18
Concerns about the safety of hydroxyurea and the fear of potential side effects are the main reasons for the discontinuation of hydroxyurea for managing SCD. Due to the use of hydroxyurea as a chemotherapeutic agent, parents may believe hydroxyurea could cause cancer despite a lack of clinical evidence.22 The side effects of hydroxyurea therapy in patients with SCD are usually mild, and most children tolerate hydroxyurea without complications. However, the most frequently reported side effect is reversible cytopenia. In our study, five parents reported discontinuing hydroxyurea due to thrombocytopenia, and eight reported discontinuation due to neutropenia. The current clinical evidence indicates that the associated toxicities are transient and can be reversed by withholding the hydroxyurea for two weeks and resuming administration at a lower dose, closely monitoring the complete blood counts.23,24 Furthermore, the Pediatric Hydroxyurea Phase 3 Clinical Trial (BABY HUG) reported that hydroxyurea was not associated with an increased risk of bacteremia or serious infection.9 This indicates the importance of raising awareness among parents and caregivers of these reversible side effects, thus reducing the discontinuation rates of hydroxyurea.
In addition to the fear of side effects, other reasons were reported in our study that indicated difficulty accessing hydroxyurea and not attending the follow-up visits. In a study conducted in the United States involving a sample of 173 parents of children affected with SCD, it was indicated that not being offered hydroxyurea as a management option was one of the main reasons for not receiving hydroxyurea.20 Furthermore, three participants of our sample indicated that plans for performing bone marrow transplantation were the reasons for hydroxyurea discontinuation. However, it is worth noting that hydroxyurea use has been reported to reduce the risk of stem cell rejection among SCD patients undergoing transplantation.25
In the current investigation, 50 participants (16.8%) declared their fears about the potential effect of hydroxyurea on their children’s fertility. Nonetheless, reproduction in SCD patients is believed to be affected by many factors, such as hypogonadism secondary to transfusional iron overload and disturbed menstruation in females secondary to hormonal and non-hormonal factors.26–28 However, the evidence concerning the potential impact of hydroxyurea on fertility is conflicting. A study that assessed the impact of hydroxyurea on sperm parameters before puberty among 46 SCD patients reported that despite the presence of semen abnormalities among all the patients, there was no difference in semen quantitative and qualitative semen characteristics between the group which received hydroxyurea and the group which did not.29 However, a study that recruited 44 patients and assessed semen parameters after initiating hydroxyurea indicated that the administration of hydroxyurea aggravated semen impairment. A review that included 17 studies assessing the overall impact of hydroxyurea in managing SCD indicated there was no sufficient evidence to support the potential impact of hydroxyurea on patients’ fertility.30
The reasons for discontinuing hydroxyurea detected in our sample indicate the presence of several clinical implications. Some participants in our investigation stopped using hydroxyurea after observing improvements in their children or after a certain age. This indicates a need to raise clinicians’ awareness about the importance of educating the patients and their caregivers about hydroxyurea, its benefits, its reversible side effects, and how discontinuation affects their children’s health.
This investigation has several strengths and limitations. The main strengths of the current investigation are related to using an open-ended approach to measure the reasons for continuing hydroxyurea. There are inherent limitations arising from the sampling methodology, and the reliance on parents or caregivers attending clinical settings may reduce the generalizability of the findings in comparison to when the recruitment is being made in outpatient clinics or community settings.
Conclusion
This study detected an overall perceived benefit and accepted use of hydroxyurea among parents and caregivers of children with SCD in Jazan. However, nearly one-fifth of the sample declared they had discontinued their hydroxyurea treatment. Upon enquiring about the reasons for discontinuation, various reasons were identified, which mainly centered around the perceived occurrence of side effects. The findings indicate the importance of increasing the role of clinicians in educating patients and caregivers about the use of hydroxyurea and its benefits. Furthermore, the treating clinicians should emphasize on educating the parents and caregivers about hydroxyurea’s reversible side effects, and how discontinuation affects their children’s health. Additionally, conducting campaigns to increase the awareness of the targeted population about the benefits of using hydroxyurea for SCD is warranted.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from any funding agency.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. World Health Organization. Sickle Cell Disease: factsheet; 2021. Available from: https://www.afro.who.int/health-topics/sickle-cell-disease.
2. El-Hazmi MA, Al-Hazmi AM, Warsy AS. Sickle cell disease in Middle East Arab countries. Indian J Med Res. 2011;134(5):597–610.
3. Sundd P, Gladwin MT, Novelli EM. Pathophysiology of sickle cell disease. Annu Rev Pathol. 2019;14:263–292.
4. Osunkwo I, Andemariam B, Minniti CP, et al. Impact of sickle cell disease on patients’ daily lives, symptoms reported, and disease management strategies: results from the international Sickle Cell World Assessment Survey (SWAY). Am J Hematol. 2021;96(4):404–417.
5. Alhomoud MA, Gosadi IM, Wahbi HA. Depression among sickle cell anemia patients in the Eastern Province of Saudi Arabia. Saudi J Med Med Sci. 2018;6(1):8–12.
6. Pinto VM, Balocco M, Quintino S, Forni GL. Sickle cell disease: a review for the internist. Intern Emerg Med. 2019;14(7):1051–1064.
7. Lee L, Smith-Whitley K, Banks S, Puckrein G. Reducing health care disparities in sickle cell disease: a review. Public Health Rep. 2019;134(6):599–607.
8. Wastnedge E, Waters D, Patel S, et al. The global burden of sickle cell disease in children under five years of age: a systematic review and meta-analysis. J Glob Health. 2018;8(2):021103.
9. Wang WC, Ware RE, Miller ST, et al. Hydroxycarbamide in very young children with sickle-cell anaemia: a multicentre, randomised, controlled trial (BABY HUG). Lancet. 2011;377(9778):1663–1672.
10. Luchtman-Jones L, Pressel S, Hilliard L, et al. Effects of hydroxyurea treatment for patients with hemoglobin SC disease. Am J Hematol. 2016;91(2):238–242. doi:10.1002/ajh.24255
11. Ware RE, Aygun B. Advances in the use of hydroxyurea. Hematology Am Soc Hematol Educ Program. 2009;2009:62–69.
12. Power-Hays A, Ware RE. Effective use of hydroxyurea for sickle cell anemia in low-resource countries. Curr Opin Hematol. 2020;27(3):172–180.
13. Jastaniah W. Epidemiology of sickle cell disease in Saudi Arabia. Ann Saudi Med. 2011;31(3):289–293.
14. Gosadi IM. National screening programs in Saudi Arabia: overview, outcomes, and effectiveness. J Infect Public Health. 2019;12(5):608–614.
15. Al-Jam’a AH, Al-Dabbous IA. Hydroxyurea in sickle cell disease patients from Eastern Saudi Arabia. Saudi Med J. 2002;23(3):277–281.
16. Azmet FR, Al-Kasim F, Alashram WM, Siddique K. The role of hydroxyurea in decreasing the occurrence of vasso-occulusive crisis in pediatric patients with sickle cell disease at King Saud Medical City in Riyadh, Saudi Arabia. Saudi Med J. 2020;41(1):46–52.
17. Alzahrani F, Albaz GF, AlSinan F, et al. Hydroxyurea use among children with sickle cell disease at King Abdulaziz University Hospital in Jeddah City. Cureus. 2021;13(2):e13453.
18. Jose J, Elsadek RA, Jimmy B, George P. Hydroxyurea: pattern of use, patient adherence, and safety profile in patients with sickle cell disease in Oman. Oman Med J. 2019;34(4):327–335.
19. Alsalman M, Alkhalifa H, Alkhalifa A, et al. Hydroxyurea usage awareness among patients with sickle-cell disease in Saudi Arabia. Health Sci Rep. 2021;4(4):e437.
20. Oyeku SO, Driscoll MC, Cohen HW, et al. Parental and other factors associated with hydroxyurea use for pediatric sickle cell disease. Pediatr Blood Cancer. 2013;60(4):653–658.
21. Haywood C
22. Björkholm M, Derolf AR, Hultcrantz M, et al. Treatment-related risk factors for transformation to acute myeloid leukemia and myelodysplastic syndromes in myeloproliferative neoplasms. J Clin Oncol. 2011;29(17):2410–2415.
23. Heeney MM, Ware RE. Hydroxyurea for children with sickle cell disease. Hematol Oncol Clin North Am. 2010;24(1):199–214.
24. Hankins JS, Ware RE, Rogers ZR, et al. Long-term hydroxyurea therapy for infants with sickle cell anemia: the HUSOFT extension study. Blood. 2005;106(7):2269–2275.
25. Brachet C, Azzi N, Demulder A, et al. Hydroxyurea treatment for sickle cell disease: impact on haematopoietic stem cell transplantation’s outcome. Bone Marrow Transplant. 2004;33(8):799–803.
26. Noetzli LJ, Panigrahy A, Mittelman SD, et al. Pituitary iron and volume predict hypogonadism in transfusional iron overload. Am J Hematol. 2012;87(2):167–171.
27. Fung EB, Harmatz PR, Lee PD, et al. Increased prevalence of iron-overload associated endocrinopathy in thalassaemia versus sickle-cell disease. Br J Haematol. 2006;135(4):574–582.
28. Hagag AA, El-Farargy MS, Elrefaey S, Abo El-enein AM. Study of gonadal hormones in Egyptian female children with sickle cell anemia in correlation with iron overload: single center study. Hematol Oncol Stem Cell Ther. 2016;9(1):1–7.
29. Joseph L, Jean C, Manceau S, et al. Effect of hydroxyurea exposure before puberty on sperm parameters in males with sickle cell disease. Blood. 2021;137(6):826–829.
30. Nevitt SJ, Jones AP, Howard J. Hydroxyurea (hydroxycarbamide) for sickle cell disease. Cochrane Database Syst Rev. 2017;4(4):Cd002202.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Quality of Life and the Presence of Depression Among Adults with Hair Loss in the South of Saudi Arabia
Alomaish AR, Gosadi IM, Dallak FH, Darraj AI, Jaafari SM, Alshamakhy AE, Mleeh NT
Psychology Research and Behavior Management 2022, 15:1989-1996
Published Date: 4 August 2022
Development and Validation of the Patient/Caregiver Reported Hydroxyurea Evaluation of Adherence for Life (HEAL) Scale
Janson IA, Bloom EM, Hampton KC, Meier ER, Rampersad AG, Kronenberger WG
Patient Preference and Adherence 2022, 16:3229-3239
Published Date: 10 December 2022
Outcomes of Hydroxyurea Accessed via Various Means and Barriers Affecting Its Usage Among Children with Sickle Cell Anaemia in North-Western Tanzania
Ambrose EE, Kidenya BR, Charles M, Ndunguru J, Jonathan A, Makani J, Minja IK, Ruggajo P, Balandya E
Journal of Blood Medicine 2023, 14:37-47
Published Date: 21 January 2023
Factors Affecting Awareness of Pregnancy Screening for Group B Streptococcus Infection Among Women of Reproductive Age in Jazan Province, Saudi Arabia
Zoli SI, Baiti MA, Alhazmi AA, Khormi RM, Sayegh MA, Altubayqi T, Darisi AM, Alhasani RA, Alhazmi SH, Gharawi SO, Muhajir AA, Alhazmi AH
Journal of Multidisciplinary Healthcare 2023, 16:2109-2116
Published Date: 26 July 2023
Predictors of Intensive Care Admission Among Adult Patients with Sickle Cell Disease in Eastern Province of Saudi Arabia
Alsalman M, Alsalman Z, Alkhalifa HA, Alfaraj AN, Alkhalifah A, Almulihi Q
Journal of Blood Medicine 2023, 14:671-680
Published Date: 27 December 2023