Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Using a Mixed-Method Approach to Explore the Factors Influencing the Family Resilience of Stroke Survivors in China
Authors Han K, Chen Y, Li M, Cui L
Received 11 September 2023
Accepted for publication 9 January 2024
Published 19 January 2024 Volume 2024:17 Pages 275—287
DOI https://doi.org/10.2147/JMDH.S439737
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kunjing Han,1,* Yiping Chen,2,* Min Li,2 Liping Cui1
1Department of Nursing, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, 030032, People’s Republic of China; 2School of Nursing, Shanxi Medical University, Jinzhong, Shanxi Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liping Cui, Department of Nursing, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, No. 99, Longcheng Street, Taiyuan, 030032, People’s Republic of China, Tel +86 0351-8368114, Email [email protected]
Background: Stroke is a critical public health issue in China that necessitates a closer examination of family resilience (defined here as the collective capacity of individuals, families and communities to effectively navigate challenges, recover from adverse events and foster positive adaptation). Amid rising stroke incidence, this study addresses the dearth of research on family resilience among stroke survivors in China, aiming to assess its level, identify influencing factors and establish coping strategies for family caregivers.
Methods: This mixed-methods research employed a sequential explanatory design. Questionnaires were distributed to 258 stroke survivors and their family members at outpatient follow-up visits. In the first stage (ie the quantitative research stage), the research tools for data collection included a general demographic sociological data questionnaire, the Family Resilience Assessment Scale (FRAS), the Self-Efficacy for Managing Chronic Disease 6-Item Scale, the Caregiver Burden Scale, the Family Functioning Scale and the Social Support Rating Scale. Quantitative data were analysed using IBM SPSS 26.0 software, utilising descriptive statistics for summarising sociodemographic characteristics and conducting analyses, such as independent-sample t-tests, one-way analysis of variance and Spearman correlation analysis. The second stage (ie the qualitative research stage) involved complementing and validating the data, developing a quantitative–qualitative interview framework and selecting participants for interviews. Colaizzi’s seven-step analysis was applied to analyse interview data. In the third stage, the quantitative and qualitative research results were integrated, and a comprehensive analysis was performed to obtain an accurate conclusion.
Results: A total of 242 families responded to the questionnaire (response rate: 93.8%). In total, the mean age of stroke survivors was 61.86 ± 8.76 years old, and 69.8% were male. The quantitative results showed that the FRAS mean score was (185.33 ± 24.78), which was above the medium level. The multiple linear regression analysis confirmed that family function was the strongest influencing factor on family resilience (β = 0.948, p < 0.01). The qualitative analysis revealed four themes of family adaptation experience: loss of independence and certainty, facing threats and challenges, seeking family advantage resources and adopting coping strategies.
Conclusion: This hybrid study sheds light on the adaptation process of the families of stroke survivors, revealing family function as the primary influencer of resilience. Recognising that eliminating risk factors is challenging, our suggestion is for clinical practitioners to emphasise family strengths and implement resilience-oriented interventions. Focusing on enhancing coping abilities and fostering adaptation within families can aid in the rehabilitation process, promoting the well-being and growth of both the family unit and individual members, while alleviating caregiver burden.
Keywords: stroke, resilience, mixed-method, quantitative research, qualitative research
Introduction
Stroke, an acute-onset cerebrovascular disease, is one of the most critical public health problems worldwide. The World Health Organization reported that 15 million people worldwide are diagnosed with stroke yearly, of whom 500 die and another 5 million are permanently disabled.1 In China, stroke incidence has been reported to increase by an average of 8.3% per year2 and the Global Burden of Disease 2019 study results showed that China has the highest incidence of stroke at >30%.3 One study estimated that the number of stroke survivors could increase to 31.7 million by 2030.4 A total of 75% of stroke survivors are incapacitated, while 40% are severely disabled,5 adversely impacting their quality of life. However, some survivors and their families can recover from adversities, gain new advantages and utilise social resources in times of such challenges.6
Walsh et al7 argued that a high level of household resilience helps families withstand the challenges that the disease brings. Family resilience refers to using resources, such as individuals, families and communities, to support recovery from adverse events, achieve positive outcomes and facilitate good family adaptation.8 In China, the stroke pathway involves a complex interplay of factors influenced by the healthcare system, cultural norms and socioeconomic conditions. China faces unique challenges in managing strokes due to the sheer magnitude of stroke cases and the evolving healthcare infrastructure. Unlike other developed countries, the level of medical services in China’s grassroots communities is still in its infancy. As a result, approximately 80% of patients prefer home care.9 Owing to the acute onset of stroke, some patients become permanently disabled, which allows caregivers to adapt to their unexpected roles as carers with little preparation.10 In addition, many family caregivers face significant problems, such as financial constraints, inadequate rehabilitation knowledge and overburdening.11 The transition from hospital to home is considered the most challenging period for stroke survivors and their families since they must adapt to the distress that the disease brings.12
At present, family resilience has been studied in several chronic disease groups, such as the families of patients with cancer and those with acquired immunodeficiency syndrome, although it is rarely applied in the families of stroke survivors in China.13 Family resilience is the starting point and may be an intervention target to promote the adaptation of patients in China after a stroke. However, research on family resilience is limited.14–16 Unfortunately, they did not identify a specific period that impacted family resilience. Therefore, the purpose of this study was threefold: (1) to gain a preliminary understanding of the level of family resilience of stroke survivors in China, (2) to explore the factors influencing the family resilience of stroke survivors in China and identify the favorable factors and risk factors and (3) to establish effective coping strategies for patients’ family members and provide a theoretical basis for strengthening their coping abilities.
Methods
Study Design
The study was conducted at a tertiary hospital in central China. The researchers used a sequential explanatory mixed-method approach17 to expand and strengthen the understanding of the family resilience of stroke survivors in China. This approach comprised two main components: (1) a questionnaire and (2) interviews. The first stage of this study involved a quantitative research methodology; this was used to understand the status of the family resilience of stroke survivors, explore the correlation between family resilience and self-efficacy in disease management, caregiver burden, family function and social support and analyse the factors influencing the family resilience of stroke survivors in China.
To select representative patient families for interviews purposefully, the second stage of this study adopted a qualitative research methodology (based on the results of a quantitative research questionnaire analysis). A semi-structured interview framework analysed and mined critical themes, clarified the factors that act as obstacles in building family resilience of stroke survivors and explored possible favorable factors.
Participants
The participants included primary caregivers from a tertiary hospital in central China via a convenient sampling method. The inclusion criteria were as follows: (1) A patient in the family was diagnosed with a stroke, and the patient was cared for at home; (2) the primary caregiver was a family member; (3) the patient and their primary caregiver were ≥18 years old and had good verbal communication. Participation in this study was voluntary. The exclusion criteria included patients and/or carers diagnosed with cognitive impairment or severe mental illness. Data were collected between April 2021 and July 2021.
The study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Shanxi Bethune Hospital (Ethics batch number: YXLL-2023-091). For the qualitative studies, the checklist for qualitative studies was applied. The purpose and process of the research were introduced to the potential participants during hospitalisation, and informed consent was obtained before the study. The baseline survey was conducted after stabilising vital signs, and contact information was collected for follow-ups. The follow-ups were conducted face-to-face when the patients could attend the clinics or by telephone when it was inconvenient for them to come to the clinics. The researchers collected data in the first stage by asking the participants to complete six questionnaires (Supplementary Information).
Data Analysis
Quantitative Research
In the quantitative research stage, social support was measured using a general demographic sociological data questionnaire, the Family Resilience Assessment Scale (FRAS), the Self-Efficacy for Managing Chronic Disease 6-Item Scale to measure self-efficacy in disease management, the Caregiver Burden Scale to assess caregiver burden, the Family Functioning Scale to evaluate the family function and the Social Support Rating Scale.
The quantitative data collection process was as follows: The questionnaire was distributed by the researcher to the families of patients who had suffered a stroke who met the inclusion criteria in the outpatient ward of the Department of Neurology of a tertiary-level hospital in a province in China. Before the survey, the researcher established a good relationship of trust with the patients and their family caregivers, informing them of the purpose, methodology and content of this study and voluntarily filling out an informed consent form, informing them that this questionnaire was limited to this study and would not disclose their privacy. The self-efficacy questionnaire was completed by the patients themselves, or the researcher read the questions and the patients answered them and then the researcher completed them on their behalf. The other questionnaires were completed by the primary family caregiver on behalf of the family. After the questionnaires were completed, the researcher checked the questionnaires for completeness, and if there were any incorrectly filled or omitted options, they were corrected and verified on the spot with the study participants and the patients were thanked.
The survey data were analysed using IBM SPSS 26.0 software. Sociodemographic data and participants’ characteristics were summarised using descriptive statistics (ie the mean and standard deviation of continuous variables and the frequency and percentage of categorical variables). An independent-sample t-test or a one-way analysis of variance was used to analyse the differences in family resilience between different sociodemographic data, and p < 0.05 was considered statistically significant. In addition, Spearman correlation analysis was used to analyse the correlation between the self-efficacy of disease management, caregiver burden, family function, social support and family resilience. Finally, the variables with p < 0.05 in the univariate analysis were taken as independent variables, and the total family resilience score was taken as a dependent variable. A multiple linear regression analysis was performed using a stepwise method, with the family resilience level as the dependent variable and statistically significant variables from the univariate analysis as independent variables, to clarify further the effect of each influencing factor on the family resilience of stroke survivors.
Qualitative Research
A phenomenological approach was adopted to delve into the lived experiences of stroke survivors and their families. This approach was chosen for its suitability in uncovering the essence of these experiences, allowing for an in-depth understanding of the phenomenon under investigation.
The recruitment process involved selecting patient families that were representative of the current status of different family resilience levels. A representative sample was selected with due consideration of family resilience score, age, family situation, place of residence, different stages of the disease, degree of illness, caregiver’s literacy level and caregiver’s work status. The interviews were conducted by two researchers, one of whom was responsible for conducting the interviews, while the other, with the consent of the interviewees, synchronised the audio recording of the interviews, while recording the interviewees’ reactions and expressions objectively. During the interviews, the researchers tried to avoid inducing the interviewees with their subjective opinions. If there were any doubts about the content of the interviews, they would promptly repeat the interviews to the interviewees to confirm the accuracy of the information. Within 24 hours after each interview, the researcher listened to the interview recordings, read the on-site transcripts several times and organised the transcripts word by word and sentence by sentence into a word version of the information, with non-verbal information such as pauses, emotional reactions and body movements in parentheses in the corresponding positions, to ensure that the organised information maintained accuracy, authenticity and completeness.
Colaizzi’s seven-step analysis was used to analyse the interview data. Specifically, it included the following: (1) recording in detail and carefully studying all interview materials, (2) extracting meaningful statements that echoed the phenomenon of family resilience, (3) extracting and summarising the meaning of valuable expressions, (4) organising the extracted meanings into themes, theme groups and categories, (5) linking the theme to a complete narrative of the research phenomenon, (6) stating the essential structure, (7) feeding the results of the resulting data analysis back to the interviewees to verify the accuracy of the content and, finally, gradually refining and sublimating the research themes through feedback from the research subjects, group discussions and expert confirmation. Thematic analysis was employed to identify patterns, themes and categories within the qualitative data. The process involved data familiarisation, generation of initial codes, searching for themes, reviewing themes, defining and naming themes and producing the final report. Reflexivity, though not explicitly mentioned, was integral to the process, with researchers acknowledging and critically reflecting on their assumptions, biases and preconceptions throughout the analysis.
Ethics
Participants provided written consent and were explicitly informed that anonymised responses may be published as part of the study findings. Participants retained the right to withdraw from the study at any time. Personal information and relevant data were anonymised and coded to ensure confidentiality and privacy.
Results
General Information About the Patients
A total of 258 questionnaires were distributed, 242 of which were recovered, yielding a 93.8% successful recovery rate. Fourteen primary caregivers took part in Phase II of this study, with sample sizes determined by data saturation.
Patients who responded to the questionnaire were predominantly male (69.8%), married (85.1%) and the breadwinner of the family (62.0%); the predominant disease type was ischemic stroke (94.9%), mean age 61.86 ± 8.76 years. Most family caregivers were women (64.5%) and were aged <59 years (85.9%), mean age 53.62±7.49 years. Participants in the qualitative study were aged 30–68 years, and eight were the spouses of stroke survivors (Table 1). The participant information for qualitative research is shown in Table 2.
 |
Table 1 Demographic and Clinical Characteristics of Stroke Patients and Caregivers in Phase 1 |
 |
Table 2 Demographic Information of Phase 2 |
Quantitative results
Disease Management Self-Efficacy Score
The chronic disease management self-efficacy scale was used to evaluate the self-efficacy of patients who had suffered a stroke in this study. The total score ranges from 0 to 10 points; the total average was (5.61 ± 1.26) points, showing a medium-low level. The average score of disease symptom management efficacy was (4.65 ± 1.36), and the average score of disease commonality management efficacy was (6.57 ± 1.58). Among them, 24.7% (82 cases) were at a low level, 67.3% (163 cases) were at a medium level and 7.8% (19 cases) were at a high level.
Family Caregiver Burden Score
The family caregiver burden score was (35.83 ± 20.92), in which the personal burden score was (23.36 ± 13.43) and the responsibility burden score was (12.47 ± 5.23). The burden of family care for patients who had suffered a stroke accounted for 32.0% at the severe level, 47.5% at the moderate level and 26.5% at the no- or mild-burden level, indicating that most of the caregiver burden in the families of patients in this study was at the moderate level.
Family Function Score
The total score of family function in this study ranged from 13 to 41 points, with an mean score of (27.721 ± 5.16). The mean score of the entries was (2.31±0.43), and the scores for family function items were 12, 7, 2, 6, 11, 1, 9, 10, 5, 4, 3, 8, in descending order.
Social Support Score
In this study, the scores of family social support of patients who had suffered a stroke ranged from 23 to 59 points, with an average score of (40.46 ± 7.52) points, among which the scores of objective support, subjective support and social support utilisation were (14.36 ± 4.43) points, (18.47 ± 5.23) points and (7.65 ± 2.36) points, respectively. The average scores of the three dimensions were ranked from low to high as utilisation of support, objective support and subjective support, among which 34.1% (82 cases) of families with patients were at the high level and 65.9% (159 cases) were at the medium level. The results showed that the level of family social support of patients who had suffered a stroke was generally at the medium level.
Family Resilience Score
The mean FRAS score was (185.33 ± 24.78), which was above the medium level (the range of scores on this scale is 49–245). The score of the family belief subscale was (66.15 ± 8.45), and the score of the family strength subscale was (119.17 ± 16.47). The mean score of each item of the family resilience of stroke survivors was >3.4. Among them, the degrees of family resilience of stroke survivors with different marital statuses, medical payment methods, stroke courses, caregiver’s education levels and work situations differed. The difference was statistically significant (p < 0.05), as shown in Table 3. For example, the families of divorced and widowed patients had lower levels of resilience than the families of married patients.
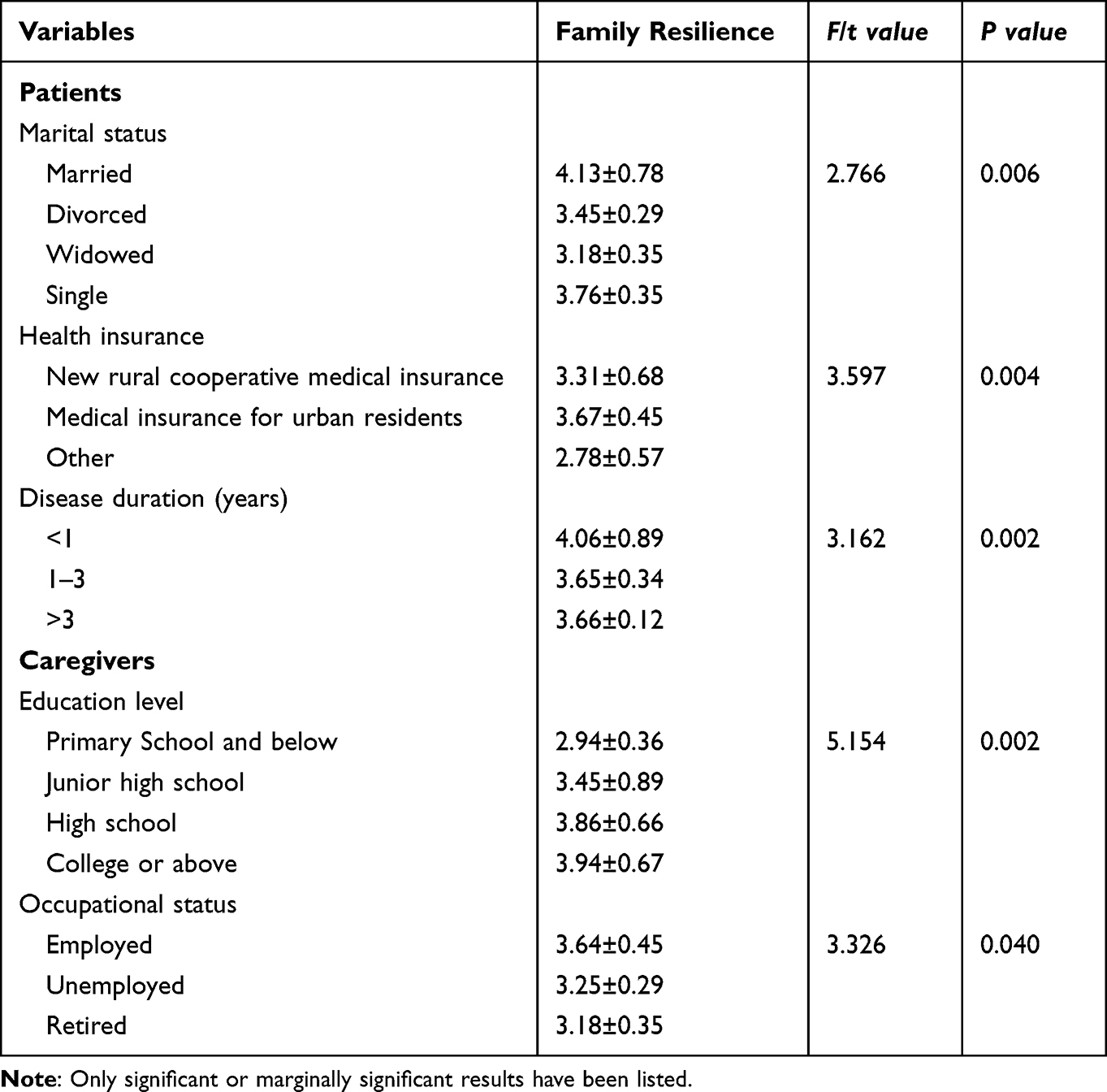 |
Table 3 Comparison of Family Resilience in Different Sociodemographic Characteristics |
The Spearman correlation analysis results showed that cerebral apoplexy and the faith and strength of patients’ families were positively correlated with self-efficacy scores, disease symptom management efficiency, common disease management efficiency, social support, objective support, subjective support and the degree of support utilisation, but they were negatively correlated with family function and care burden (Table 4).
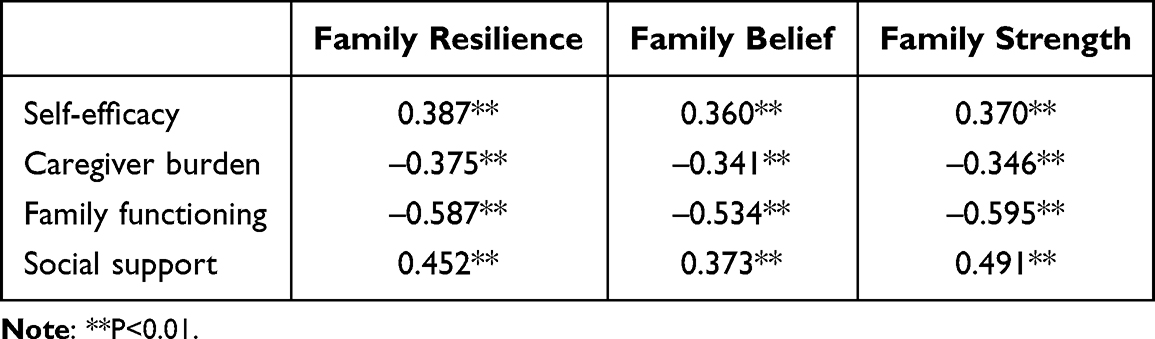 |
Table 4 Correlations (r) Among Family Resilience, Self-Efficacy, Caregiver Burden, Family Functioning, and Social Support |
The multiple stepwise regression analysis results showed that eight variables entered the regression equation, and the researcher concluded that family function was the strongest influencing factor on family resilience (β = 0.948, p < 0.01). Other variables are shown in Table 5.
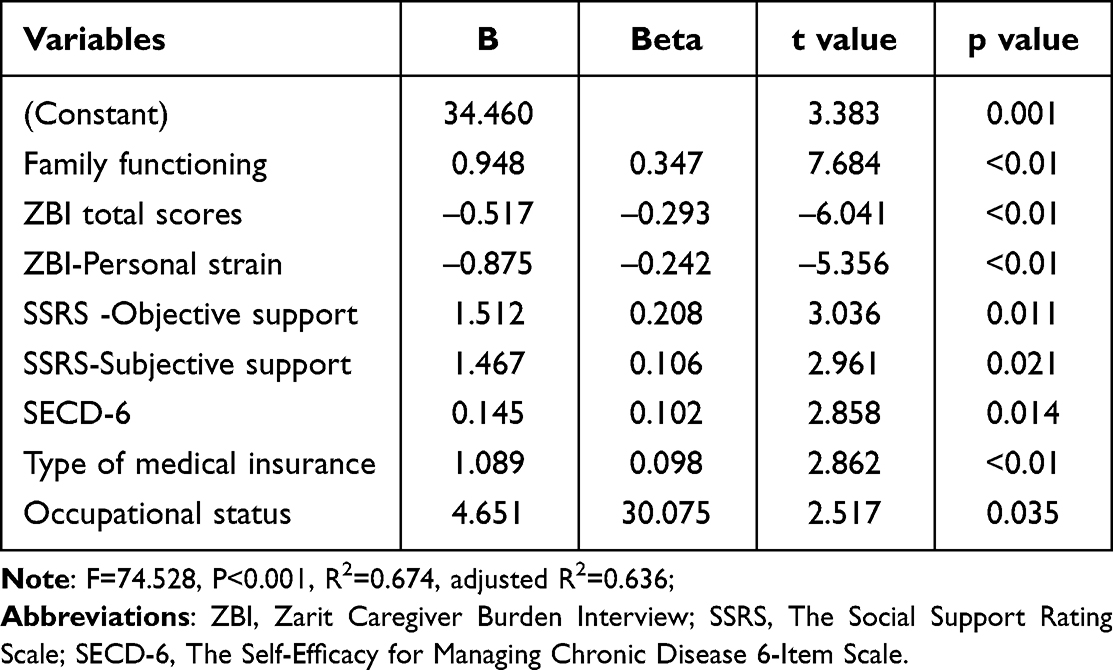 |
Table 5 Multivariate Linear Regression Analysis |
Qualitative Results
Theme 1: Loss of Independence and Certainty
Subtheme 1: Loss of Independence
Stroke impairment causes the loss of independence and normal activities of daily living; it directly impacts the daily lives of family members, particularly the loss of independence and autonomy and the ability of the primary caregiver to plan their daily work and life appropriately. Some of the participants’ statements are reproduced below:
S1: He suddenly became incapable of doing anything; his right arm couldn’t be lifted, and eating and going to the bathroom were difficult. In order to take care of him, you do not have to do anything else yourself; you can only do that at home.
S7: My son rarely travels on business, and sometimes, he won’t go out for drinks or food with friends since his mother is ill. No way! I am older: I cannot handle her alone; my son can only come back early from work and give me a hand.
S12: As soon as I graduated, I went straight to Shanghai to work. Now I have resigned from my job and returned to my hometown because my mother needs my help to take care of her father.
Subtheme 2: Full of Uncertainty
Patients who suffer strokes have no way of knowing whether the disease will recur or what life will be like once they leave hospital and return home. Some of the participants noted the following:
S6: It is hard for me to go out in an emergency when my mother is home alone because I am scared that she may fall.
S9: In the beginning, he recovered very well, and I could return to work normally. However, he suddenly developed epilepsy when he was doing rehabilitation exercises, and now he is walking worse than before.
S14: Now whatever you plan is futile; just count the days, and don’t ask for too much.
Theme 2: Facing threats and challenges
Subtheme 1: Heavy Economic Burden
A long rehabilitation process and high medical expenses are associated with stroke, which places enormous financial pressure on families. Moreover, some family caregivers have to reduce their working hours or even leave their jobs to care for patients. The financial impact on the family was mentioned by some family caregivers.
S9: My salary wasn’t great, and now I have to change shifts or take time off to take care of him. When he was healthy, our family relied heavily on him to work so that the kids could attend school and support the family. But now that he is sick, if I absolutely need money, I borrow from friends and family.
Subtheme 2: Post-Stroke Negative Emotions
Most stroke survivors are left with sequelae, coupled with the uncertainty of stroke recurrence owing to the high disability rate of the disease. Patients experience negative emotions, such as anxiety, depression, stigma, anger and mood disorders. At the same time, heavy caring tasks also bring negative psychological experiences to family caregivers, such as anxiety, fear, depression, role strain and fatigue.
Participants Expressed the Following
S1: He has a strong personality. Although he has told us all his psychological words, I can feel his heart is still sad. Why should it happen to him?
S10: Sometimes, while lying in bed at night, a person will often shed tears; I am often anxious and nervous, afraid that he will relapse.
Subtheme 3: Heavy Care Burden
The fatigue of long-term care work and the lack of professional care knowledge impose a heavy burden on family caregivers. Mental strain, reduced social interaction, physical fatigue, sleep disturbances and memory loss are common symptoms of family caregivers. Participants expressed the following:
S3: I often get a little dizzy, a little overwhelmed, and I often have to take medication.
S5: I often have dreams or insomnia at night. I can’t sleep well. I have no energy during the day, and my memory is not as good as before.
Theme 3: Utilising Family Resources
Subtheme 1: Internal Family Support
After the onset of the disease, families face unprecedented pressure; for instance, family members need to utilise their own resource advantages, including family members’ personality traits, health status, education level, care ability and beliefs about illness, to help families adapt to the new changes. One participant said the following:
S4: This happened to my mother all of a sudden. It’s no use being sad for us as children. We should still be positive and optimistic.
Subtheme 2: Relationships Within the Family
This mainly refers to the quality of the relationships between family members or family caregivers and patients before onset. A family with a good relationship will naturally support each other in all aspects to help the family adapt to difficulties better and faster. One participant said the following:
S1: We have always had a good relationship, and our son is very dutiful. He works very well, and he can’t accept that this happened, but I am glad that he was able to speak up and not keep it to himself.
Subtheme 3: Support from External Resources
After a stroke, various forms of support from relatives, friends and community health services coupled with adequate social interaction can effectively improve the resilience level of families to a large extent. Participants expressed the following:
S7: The community hospital near our house is very good. It has rehabilitation equipment, and the doctor is extremely professional. Every afternoon I push my wheelchair to take him to do rehabilitation.
S8: I will not let him stay at home every day; every day I push him to the community below to see others play chess and cards; ah, to let him have more contact with the outside, people are happy.
Theme 4: Adopting Coping Strategies
Family coping is a gradual process in which families use existing family resources to continuously generate and develop new behaviours to strengthen their ability to adapt to stressful events. Family members must redefine their roles, adjust the division of labour and adapt to the new environment. Family caregivers turn to others for help, learning about nursing and rehabilitation, rebuilding their daily habits and changing their mindsets. Some of the participants expressed the following:
S6: My husband used to only go to work and do nothing at home. Now I have to take care of my mother, so I can only change him to cook for the child every day. The child said that he did not like to eat what he did, and he did not want to do it, but there is no way, I do not know what good way.
S9: Every day I go online to learn some simple movements and to help him do rehabilitation activities. Professional movements cannot be learned, as there is no one to teach; ah, I can only learn to do a little bit: better than no activity.
Figure 1 shows the themes and subthemes extracted from qualitative content analysis.
 |
Figure 1 Themes and subthemes extracted from qualitative content analysis. |
Discussion
In this research, we found that the family resilience of stroke survivors was above the medium level and was correlated with positive family functioning. Other factors that influenced family resilience included adaption experience (the process through which families adjust their daily routines to care for a family member’s rehabilitation after a stroke), uncertainty about the future, financial burdens and negative emotions.
Family functioning was the most important component of family resilience. The requirement for adjusting to daily routines to care for the rehabilitation of a family member after a stroke demonstrates the presence of one of the qualities of family resilience in overcoming problems.18 The quantitative results did not allow for the understanding of how families adapt to changed living conditions when dealing with an adverse situation, but our qualitative results generated information pertinent to some phenomena of interest in the Chinese context, and the quantitative findings support the discovered themes. The loss of independence felt by stroke survivors affects caregivers’ independence, but filial piety and some family values may support family members in overcoming their negative experiences.
A strong interpersonal relationship after a stroke is important for the well-being of both patients and family caregivers. The findings of other studies highlight areas to consider in promoting strong relationships between patients and family caregivers. Cohesion and a strong emotional connection between family members support them in facing and overcoming such challenges. In this study, most caregivers were spouses. A good marital status was a protective factor for family resilience, and the marital relationship was an important link to maintaining the harmony and stability of the family relationship. Spouses provide unconditional care, strong psychological comfort and motivation for patients. The subtheme of “relationships within family systems” in the qualitative research section seems to explain this phenomenon. However, studies have shown that around 54% of families of stroke survivors experience relationship problems, and nearly 38% of couples experience open conflict.19 Without supportive intervention, relationship problems tend to increase after a stroke, deteriorating relationship quality over time.20 To reduce or eliminate the negative emotions of patients and family caregivers, medical staff and community healthcare providers should promptly discover and inform them of self-regulation methods, such as mindfulness therapy, music therapy and diary writing.21
Informal caregivers describe their post-stroke lives as having been “turned upside down”.22 Caring for stroke survivors frequently burdens unpaid informal family caregivers because of the rapidly progressive nature of the disability and the ongoing, frequent and unpredictable nature of stroke recovery.23 Participants in qualitative studies described financial, psychological and care burden threats and challenges they faced in adjusting to illness stress, which was also confirmed in quantitative studies. Not only did the caregiver burden affect family resilience but family resilience was worse when medical care had to be paid for. Family caregivers regularly bear the substantial costs of stroke survivors for a long time, and in some cases, they even forego treatment because they cannot afford such expenditure,24 which significantly increases the risk of delayed recovery and even stroke recurrence.
This study found that multi-channel economic support can adjust the impact of diseases on families, which is similar to the research findings of Lopez-Espuela25 and Kariyawasam,26 among others. Therefore, it is necessary to advocate for government departments to continue to implement medical insurance policies for serious diseases, formulate corresponding healthcare policies and promote re-employment-related measures to address the financial burden and employment status of family caregivers.
Studies have shown that while coping with disease, the effectiveness of the coping strategy is directly related to whether a patient’s family can achieve a good level of resilience. Mobilising resources and adopting positive coping strategies can reduce the vulnerability of families to cope with stress and enhance their resilience.27 At the individual level, patients should be encouraged to promptly perform self-psychological counselling, and family members should repeatedly encourage patients to enhance their sense of self-efficacy and self-worth. At the same time, family members, particularly caregivers, should be encouraged to perform timely self-regulation to maintain good physical and mental states.
In addition, this study found that, similar to the research results of Lietz28 and Weitzel et al,29 strong and powerful social support was a protective factor for the family resilience of stroke survivors, involving community and other resources to help families cope with challenges, obtain information and access emotional/instrumental support.
This study lays the groundwork for future research in understanding and enhancing family resilience among stroke survivors in China. Subsequent investigations could delve into developing targeted interventions addressing the identified challenges, such as financial burdens and negative emotions. Exploring the effectiveness of support systems, both internal and external, on family resilience would be valuable. Additionally, longitudinal studies tracking the evolution of coping strategies and their impact on family well-being over time could provide insights for intervention development. Further examination of the cultural nuances influencing family dynamics and resilience in the Chinese context would contribute to a comprehensive understanding. Overall, future research should aim to inform practical strategies and policies that enhance the adaptive capacity of families facing the complex repercussions of stroke.
Limitations
This study recognises certain limitations that warrant consideration. First, the Chinese version of the family resilience assessment tool may have contributed to participant fatigue and potentially impacted response accuracy, given the extended questionnaire and investigation events. While efforts were made to minimise these effects, future research should focus on refining the assessment tool and developing a specific scale tailored to the context of stroke survivors to enhance the efficiency and ethical robustness of data collection. Additionally, the cross-sectional survey in the initial phase introduces a potential bias, and long-term follow-up may have influenced participants’ work experiences, particularly among nursing staff. Longitudinal studies are recommended to establish causal relationships between study variables. Moreover, future research should explore additional factors and identify family strengths, contributing to a more comprehensive understanding of family resilience in the context of stroke survivors.
Conclusions
This study used mixed methods to help healthcare workers better understand the adaptation process of the families of stroke survivors and the factors influencing family resilience, including dominant resources and risk factors. Among these, family function was found to be the strongest influencing factor. Eliminating risk factors from a patient’s life is practically impossible, but increasing their ability to cope with and adapt to difficult conditions despite increased risk factors is very important. Therefore, we suggest that clinical personnel focus on family strengths and conduct family resilience-oriented interventions to facilitate the adaptation, recovery and growth of the family as a unit as well as its individual members in the process of stroke rehabilitation and to reduce the burden on caregivers.
Disclosure
The authors declare no potential competing interests.
References
1. Stroke. Cerebrovascular accident. Available from: http://www.emro.who.int/health-topics/stroke-cerebrovascular-accident/index.html.
2. Griauzde J, Ravindra VM, Chaudhary N, Gemmete JJ, Pandey AS. Neuroprotection for ischemic stroke in the endovascular era: a brief report on the future of intra-arterial therapy. J Clin Neurosci. 2019;69:289–291. doi:10.1016/j.jocn.2019.08.001
3. Ma Q, Li R, Wang L, et al. Temporal trend and attributable risk factors of stroke burden in China, 1990–2019: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health. 2021;6(12):e897–e906. doi:10.1016/S2468-2667(21)00228-0
4. Gerotziafas GT, Catalano M, Colgan MP, et al.; Scientific Reviewer C. Guidance for the management of patients with vascular disease or cardiovascular risk factors and COVID-19: position paper from VAS-European independent foundation in angiology/vascular medicine. Thromb Haemost. 2020;120(12):1597–1628. doi:10.1055/s-0040-1715798
5. of the Report TW. Report on cardiovascular health and diseases in China 2021: an updated summary. Biomed Environ Sci. 2022;35(7):573–603. doi:10.3967/bes2022.079
6. Camak DJ. Addressing the burden of stroke caregivers: a literature review. J Clin Nurs. 2015;24(17–18):2376–2382. doi:10.1111/jocn.12884
7. Walsh F. Family resilience: a framework for clinical practice. Family Process. 2003;42(1):1–18. doi:10.1111/j.1545-5300.2003.00001.x
8. Xie JH, Mei HB, Ouyang YQ, et al. Analysis of influencing factors of family resilience in children with congenital tibial pseudoarthrosis. Risk Manag Healthc Policy. 2022;15:331–337. doi:10.2147/RMHP.S339503
9. Chen JJ, Wang QL, Li HP, Zhang T, Zhang SS, Zhou MK. Family resilience, perceived social support, and individual resilience in cancer couples: analysis using the actor-partner interdependence mediation model. Eur J Oncol Nurs. 2021;52:101932. doi:10.1016/j.ejon.2021.101932
10. Han Y, Liu Y, Zhang X, Tam W, Mao J, Lopez V. Chinese family caregivers of stroke survivors: determinants of caregiving burden within the first six months. J Clin Nurs. 2017;26(23–24):4558–4566. doi:10.1111/jocn.13793
11. Schulz R, Eden J. National Academies of Sciences E, Medicine: recommendations to Support Family Caregivers of Older Adults. In: Families Caring for an Aging America. National Academies Press (US); 2016.
12. Cai F, Li L, Du J, et al. Status and influencing factors of family stress resistance in young and middle-aged stroke patients. Nursing Research. 2021;35(03):538–541.
13. Zhang X, Wang A, Guan T, Kuang Y, Zhang Y, Wu F. Reliability and validity of the Chinese version of the Walsh family resilience questionnaire among community-dwelling disabled elderly individuals (WFRQ-CE). Front Psychol. 2023;13:1095958. doi:10.3389/fpsyg.2022.1095958
14. Zhang W, Zhou W, Ye M, Gao Y, Zhou L. Family resilience of stroke survivors within 6 months after a first-episode stroke: a longitudinal study. Front Psychiatry. 2022;13:968933. doi:10.3389/fpsyt.2022.968933
15. Zhang W, Gao Y, Ye M, Zhou W, Zhou L. Family resilience and its predictors among patients with a first-ever stroke one month after stroke: a cross-sectional study. Top Stroke Rehabil. 2023;30(7):691–699. doi:10.1080/10749357.2023.2165270
16. Zhang W, Ye MM, Gao YJ, Zhou LS. Dyadic profiles of family resilience among patients with first-episode stroke: a longitudinal study of the first 6 months after stroke. J Clin Nurs. 2023;32(13–14):3672–3681. doi:10.1111/jocn.16458
17. Creswell JW. Research design - qualitative, quantitative, and mixed methods approaches - A framework for design; 2003.
18. Walsh F. Applying a family resilience framework in training, practice, and research: mastering the art of the possible. Fam Process. 2016;55(4):616–632. doi:10.1111/famp.12260
19. Daniel K, Wolfe CD, Busch MA, McKevitt C. What are the social consequences of stroke for working-aged adults? A systematic review. Stroke. 2009;40(6):e431–440. doi:10.1161/STROKEAHA.108.534487
20. Green TL, King KM. Experiences of male patients and wife-caregivers in the first year post-discharge following minor stroke: a descriptive qualitative study. Int J Nurs Stud. 2009;46(9):1194–1200. doi:10.1016/j.ijnurstu.2009.02.008
21. Araújo O, Lage I, Cabrita J, Teixeira L. Intervention in informal caregivers who take care of older people after a stroke (InCARE): study protocol for a randomised trial. J Adv Nurs. 2015;71(10):2435–2443. doi:10.1111/jan.12697
22. Bulley C, Shiels J, Wilkie K, Salisbury L. Carer experiences of life after stroke - A qualitative analysis. Disabil Rehabil. 2010;32(17):1406–1413. doi:10.3109/09638280903531238
23. Caro CC, Costa JD, Da Cruz DMC. Burden and quality of life of family caregivers of stroke patients. Occup Ther Health Care. 2018;32(2):154–171. doi:10.1080/07380577.2018.1449046
24. Wagachchige Muthucumarana M, Samarasinghe K, Elgán C. Caring for stroke survivors: experiences of family caregivers in Sri Lanka - A qualitative study. Top Stroke Rehabil. 2018;25(6):397–402. doi:10.1080/10749357.2018.1481353
25. Lopez-Espuela F, Zamorano JD, Ramírez-Moreno JM, Jiménez-Caballero PE, Portilla-Cuenca JC, Lavado-García JM. Casado-Naranjo I: determinants of quality of life in stroke survivors after 6 months, from a comprehensive stroke unit: a longitudinal study. Biol Res Nurs. 2015;17(5):461–468. doi:10.1177/1099800414553658
26. Kariyawasam PN, Pathirana KD, Hewage DC. Factors associated with health related quality of life of patients with stroke in Sri Lankan context. Health Qual Life Outcomes. 2020;18(1):129. doi:10.1186/s12955-020-01388-y
27. Trute B, Benzies KM, Worthington C, Reddon JR, Moore M. Accentuate the positive to mitigate the negative: mother psychological coping resources and family adjustment in childhood disability. J Intellect Dev Disabil. 2010;35(1):36–43. doi:10.3109/13668250903496328
28. Lietz CA, Julien-Chinn FJ, Geiger JM, Hayes Piel M. Cultivating resilience in families who foster: understanding how families cope and adapt over time. Fam Process. 2016;55(4):660–672. doi:10.1111/famp.12239
29. Weitzel EC, Glaesmer H, Hinz A, et al. What builds resilience? Sociodemographic and social correlates in the population-based LIFE-adult-study. Int J Environ Res Public Health. 2022;19(15). doi:10.3390/ijerph19159601
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Quantitative and Qualitative Research on Management Strategies for Dyspnoea in Elderly Patients with Coronary Heart Disease Complicated with Chronic Heart Failure
Niu YN, Li R, Zhao P, He P, Li YL, Wang Y
Journal of Multidisciplinary Healthcare 2022, 15:2007-2013
Published Date: 10 September 2022
A Qualitative Study on the Humanistic Care Needs of Patients with Stroke and Their Families
Li M, Xie H, Luo Q, Huang G, Xu G, Cheng Y, Li J
Journal of Multidisciplinary Healthcare 2023, 16:717-730
Published Date: 16 March 2023
The Correlation Between Caregivers Burden and Quality of Life Among Family Caregivers of Stroke Survivors: The Mediating Role of Resilience
Handayani F, Kusumaningrum NSD, Dwidiyanti M
Nursing: Research and Reviews 2024, 14:91-102
Published Date: 19 June 2024
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Coping and Resilience in Chinese Couples with Connective Tissue Diseases: A Culturally Informed Qualitative Explanation
Cai X, Xu S, Dong C, Gu Z
Patient Preference and Adherence 2026, 20:578038
Published Date: 17 February 2026