Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Unpacking Multi-Layered Challenges in Palliative Care Transitions: A Descriptive Qualitative Study of Multidisciplinary Teams in China
Authors Tang J, Li J, Wang X, Xiao M, Zhang Y, Tao H, Jiang Y, Yan Y, Zhao Q
Received 26 February 2026
Accepted for publication 20 May 2026
Published 26 May 2026 Volume 2026:19 605455
DOI https://doi.org/10.2147/JMDH.S605455
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Jiao Tang,1,2 Jie Li,3 Xingyu Wang,1 Mingzhao Xiao,2 Yunfeng Zhang,1 Hangcheng Tao,1 Yan Jiang,4 Yanfei Yan,1 Qinghua Zhao2
1School of Nursing, Chongqing Medical University, Chongqing, People’s Republic of China; 2Department of Nursing, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 3Mental Health Center, West China Hospital/West China School of Nursing, Sichuan University, Chengdu, People’s Republic of China; 4Department of Nursing, West China Hospital, Sichuan University, Chengdu, People’s Republic of China
Correspondence: Qinghua Zhao, Department of Nursing, The First Affiliated Hospital of Chongqing Medical University, Chongqing, 400016, People’s Republic of China, Tel +86186-0230-8866, Email [email protected]
Purpose: This study aimed to explore the challenges faced by Chinese multidisciplinary teams in transitioning patients with life-limiting illnesses to palliative care, utilizing the social-ecological model as a framework.
Participants and Methods: A descriptive qualitative study was conducted involving 39 multidisciplinary team members, including physicians, nurses, psychologists, social workers, rehabilitation therapists, nutritionists, traditional Chinese medicine therapists, nursing attendants, and volunteers from six health institutions. Data were collected through semi-structured focus group interviews and analyzed using both inductive and deductive thematic analysis.
Results: Four themes were identified: 1) dilemmas in individual end-of-life decision-making rights, with three subthemes: irrational perceptions hindering rational decision-making, the agony of life-and-death decision-making, protective medical practices inducing decision-making rights squeeze; 2) multiple constraints in the family fields, with three subthemes: external stigma of “unfilial” oppression, intrafamilial disparities in palliative care perceptions, distorted emotional connection among family members; 3) Intrinsic barriers in healthcare provision, with three subthemes: institutional deficits in palliative care literacy, professional competence gaps in palliative care delivery, and deficiency in quality control system for palliative care; and 4) constraints shaped by social environment, with four subthemes: insufficient funding support for palliative care, ambiguous palliative care pricing mechanisms, absence of practitioner safeguards in palliative care, and entrenched perceptions of life and death.
Conclusion: Palliative care transition were shaped by multi-layered challenges across micro-macro systems, rooted in cultural norms, healthcare provision, and structural inequities. Challenges such as protective medical care, stigma around “unfilial” behavior, and emotional connection within families offer novel perspectives on promoting palliative care transition. Addressing these challenges necessitates targeted strategies across patients (eg., implementing advance care planning consultations), families (eg., the reconceptualization of filial piety and its recalibration), healthcare institutions (eg., establishing evidence-based standards, guidelines, and screening tools), and social environment (eg., implementing universal death education to dismantle stigma). These strategies could promote culturally sensitive and sustainable palliative care transitions within similar healthcare and sociocultural contexts.
Keywords: palliative care, transition, multidisciplinary team, challenges, qualitative study
Introduction
Globally, health- and disease-related severe suffering poses a significant threat to individuals with life-limiting illnesses.1 Palliative Care, which actively provides comprehensive physical, psychological, and spiritual care for individuals with life-limiting illnesses, is an effective measure to alleviate severe health and disease-related suffering and to enhance the quality of life for both the individuals and their families.2 It has been incorporated by the World Health Organization2 as an essential component of people-centered integrated health services. Furthermore, a study indicated that patients with life-limiting illnesses require continuous palliative care for at least 12 weeks to derive significant benefits.3 This underscores the importance of early identification of patients who can benefit from palliative care and facilitating their transition to such service. Studies have reported that early palliative care not only improves patients’ quality of life, enhances prognostic awareness, facilitates communication about end-of-life preferences, and minimizes crises at the end of life, but also helps establish harmonious physician-patient relationships, increases patient and family satisfaction, and alleviates caregivers’ negative emotional experiences as well as caregiving burdens.4–6 Against this backdrop, the quality of transitional care—particularly the seamless transition from curative treatment to palliative care—has emerged as a critical determinant of whether these documented benefits can be fully realized in clinical practice.
Currently, transitional care is internationally recognized as a series of comprehensive, time-limited services aimed at providing patients with coordinated, continuous, and safe care during transitions between various medical services, healthcare providers, and medical settings.7 This approach seeks to prevent or mitigate the deterioration of health status among high-risk patients. However, the development of palliative care transitions remains inconsistent worldwide. Countries, such as the United States and the United Kingdom, have integrated tools like the Leeds eligibility criteria,8 the Gold Standards Framework,9 and the Surprise Question10 into routine clinical pathways for early palliative care screening and referral. In contrast, many countries and regions have yet to incorporate early palliative care into standardized practices for patients with life-limiting illnesses. For instance, in mainland China, there are currently no unified transitional standards for palliative care or standardized referral processes,11 leading to significant disparities in the availability and utilization of palliative care services across different regions. Until 2023, the “Guidelines for Integrated Diagnosis and Treatment of Cancer in China: Palliative Care”12 indicated that potential candidates for palliative care include “patients with clearly diagnosed, high-mortality advanced malignancies”, “cancer patients with poor functional status and ongoing failure of vital organs”, or those who present with “uncontrollable severe physiological symptoms, with or without serious mental and psychological symptoms”. However, the transition criteria for palliative care in Chinese non-cancer patients remain ambiguous and lack consistency.
These circumstances have resulted in a widespread phenomenon of delayed transitions to palliative care, wherein patients frequently make this transition only in the last 1–2 weeks of their lives or even during critical moments when they are facing imminent danger.11,13,14 Statistics indicated that the average length of stay in palliative care wards is only 5 days (with shorter stays correlating to reduced actual survival periods, reflecting a late transition to palliative care).13 Alarmingly, 14.4% of patients die within 24 hours of admission to the palliative care department.13 The study by Gu et al11 also found that among 759 patients transitioning to palliative care, 21 (2.77%) died within 24 hours of admission, and 121 (15.94%) died within one week of admission. Quaidoo et al14 reported a delayed transition rate to palliative care as high as 85.6%. Late palliative care transition not only hinders patients with life-limiting illnesses from receiving optimal hospice support and assistance but also prevents families from benefiting from hospice services, ultimately becoming an indicator of poor quality in palliative care.15–17 It is evident that promoting transitions to palliative care faces multiple challenges, and identifying these challenges during the transition process is an essential preliminary step.
Studies have confirmed that multidisciplinary team (MDT) collaboration could more effectively address the multidimensional and complex needs of patients with life-limiting illnesses, alleviate their physical and psychological suffering, and enhance their quality of life.18–20 In the palliative care transition process, MDT members assume complementary and irreplaceable functions. Specifically, physicians are responsible for assessing conditions and prognoses, screening for palliative care eligibility, and initiating discussions regarding transition decisions; nurses undertake symptom management, provide comfort care, facilitate patient-family communication, and coordinate transitions; nutritionists, psychologists, rehabilitation therapists and social workers offer nutritional support, psychological interventions, rehabilitation guidance, and social resources coordination, respectively; volunteers provide daily companionship and assist in creating comfortable care environments.18,21 However, significant shortcomings exist within the multidisciplinary service system for palliative care in mainland China. On one hand, there is a general shortage of multidisciplinary professionals, such as psychologists, social workers, and volunteers. On the other hand, most medical institutions have yet to establish a unified and systematic continuing education training system for MDTs, resulting in a lack of standardized training in palliative care for relevant practitioners.22,23 Consequently, the professional capabilities of MDT members during the palliative care transition are inconsistent, hindering the achievement of standardization and homogenization in palliative care transition practices.
MDTs play a critical role throughout the entire process of palliative care transition, encompassing early screening and eligibility assessment, patient-family communication and decision-making, as well as interdepartmental referral and care handover. Serving as both frontline practitioners in direct interact with patients and families and key implementers of institutional and governmental palliative care standards, policies, and regulations, these teams provide a unique perspective. Unlike the viewpoints of patients or families, which primarily illuminate their experiences and needs, the MDT perspective can identify systemic, modifiable challenges operating at the individual, interpersonal, organizational, and societal levels, many of which remain opaque to patients and families. Consequently, the holistic and process-oriented perspective of MDTs provides a more integrated evidence base for developing systemic interventions, moving beyond fragmented, single-layered solutions. However, existing research has rarely explored the challenges faced during palliative care transition from the MDT perspective. This oversight has resulted in a incomplete understanding of the various stakeholders involved and the multidimensional challenges they encounter. This gap is particularly pronounced in mainland China, where palliative care is still evolving and qualitative evidence regarding transition-related challenges remains limited. Moreover, such challenges are often context-specific, shaped by distinct characteristics of the healthcare system and sociocultural norms.
Palliative care transition is characterized by systemic complexity, necessitating an analysis of the challenges it encounters across multiple layers to construct a comprehensive explanatory framework. Drawing on Bronfenbrenner’s ecosystems theory, the social-ecological model underscores the importance of situating human development within a broader ecological context.24 This model can be employed to systematically organize the factors related to health and disease across various layers: the individual level (eg., attitudes), the relational level (eg., family environment), the community level (eg., healthcare institutions), and the societal level (eg., culture, regulations and policies). Therefore, guided by the social-ecological model, this study aimed to explore the challenges encountered during palliative care transition in mainland China from the MDT perspective. This exploration provides a theoretical foundation for formulating targeted and actionable intervention strategies that assist patients with life-limiting conditions in accessing palliative care earlier and avoiding the adverse effects associated with delayed transitions.
Materials and Methods
Study Design
This study employed a descriptive qualitative design using thematic analysis conducted through a series of focus group interviews. The descriptive qualitative approach is effective in exploring the diverse experiences and perceptions of individuals regarding the research question, offering direct and context-rich descriptions of real-world clinical practice.25,26 The focus group methodology was specifically selected for this study because it is particularly effective in capturing shared experiences, interactive dialogue, multidisciplinary consensus, and divergent perspectives, which cannot be fully elicited through one-on-one interviews.27 This method aligns directly with our core objective of thoroughly exploring team-based challenges in palliative care transitions.28 Furthermore, this study adhered to the Consolidated Criteria for Reporting Qualitative Studies (COREQ) checklists.29
Study Setting
This study was conducted across six healthcare institutions in Chongqing, the only municipality directly under the central government in southwestern China and a major transportation hub, with a population of approximately 32 million. According to the Seventh National Population Census bulletin, the city’s elderly population aged 65 and above constitutes 17.08%, ranking second nationwide, indicating a severe aging population situation.30 Since 2019, four administrative districts (Beibei District, Jiulongpo District, Shizhu County, and Fengdu County) in Chongqing have been successively included in the national pilot program for palliative care. These pilot regions are actively exploring palliative care practices, which contributes to expanding the public coverage of palliative care and improving responses to the challenges posed by population aging.
Participants and Recruitment
To comprehensively explore the challenges associated with the transition to palliative care, this study employed a two-stage participant selection strategy. Firstly, health institutions were selected through stratified sampling based on their years of palliative care provision. Subsequently, palliative care MDTs were recruited from these institutions using maximum variation purposive sampling. This method is widely regarded as the most effective in qualitative research, as it enables the selection of participants who demonstrate sufficient interest in the research question and are capable of providing rich, in-depth information.31 MDT members were recruited through a two-stage process. First, an official invitation letter was sent by the researchers’ institution to each participating healthcare institution to obtain formal institutional support and informed consent for participation. Second, designated liaisons at each site coordinated with the research team to facilitate recruitment of eligible team members—namely, healthcare professionals from various disciplines who had been involved in palliative care practice for at least six months. No prior relationship existed between the study authors and participants.
Data Collection
This study conducted semi-structured focus group interviews in July and August 2024. Based on the social-ecological model and previous studies, the interview outline development followed a rigorous three-stage process. First, the researchers (JT, JL, and QZ) drafted the preliminary interview outline based on the study objectives and a comprehensive literature review. Subsequently, experts in gerontology, oncology, and palliative care, along with a methodology expert skilled in qualitative study, were invited to provide guidance to refine the content organization, question sequencing, and phrasing, resulting in a revised interview outline. Finally, two doctors, one nurse, and one nurse manager assistant involved in palliative care practice participated in a focus group pre-interview to further optimize question formulation and interview procedures, ultimately finalizing the validated interview outline (Table 1). Additionally, a sociodemographic questionnaire was developed to capture essential participant characteristics, including gender, age, educational attainment, occupation, professional position, and years of palliative care experience (Table 1). This questionnaire facilitated contextual understanding of participants’ professional backgrounds and practice trajectories.
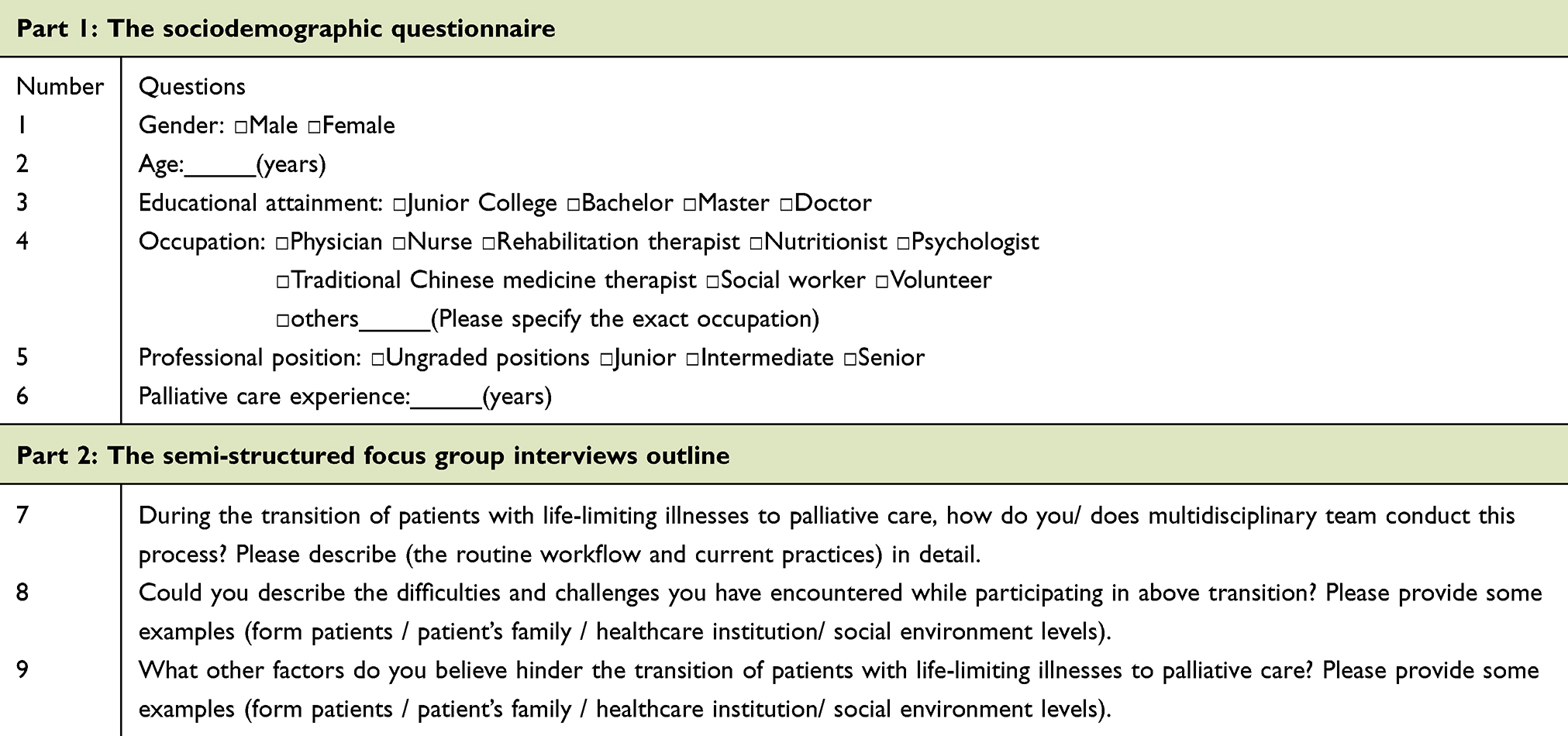 |
Table 1 The Instruments of Focus Group Interviews |
Formal interviews were conducted in independent, round-table conference rooms that could accommodate approximately 10 people at various health institutions, creating a safe, open, and comfortable environment for participants to authentic dialogue.32 The interview facilitator (JT) and on-site recorders (XW), all experienced palliative care researchers, had completed systematic coursework in qualitative research methodology and participated in theoretical-practical training programs, ensuring methodological rigor through their combined professional expertise. Prior to interview commencement, the facilitator comprehensively informed participants about the study background, purposes, procedures, potential benefits and risks, and privacy protection protocols to obtain their informed consent forms and complete the sociodemographic questionnaire. To ensure the quality of the focus group, the facilitator emphasized several key points to participants before the interviews:28 (1) each participant should speak in turn to prevent simultaneous conversations, which facilitates accurate recording of the discussion; (2) there are no “correct or incorrect” answers to any questions, and participants are encouraged to share their authentic experiences and viewpoints, even if they are critical.
During the interview, the facilitator maintained a strictly neutral stance, avoided leading questions, and allowed sufficient speaking time for quieter participants as well as those with dissenting views. Meanwhile, the facilitator employed active engagement techniques including probing, repetition, summarization, and responsive feedback to encourage participant expression. Focus groups were conducted without time constraints to enable comprehensive sharing of diverse experiences and perspectives. Data collection continued until information saturation was achieved, which was indicated by the absence of new themes or meaningful statements in the interviews, resulting in repetitive content. Hudson28 suggested that two focus groups might suffice to reach data saturation. It was determined that data saturation was reached after the fourth focus group interview, as no new categories or subthemes emerged across the social-ecological layers. To confirm saturation and enhance the richness and variability of perspectives, two additional focus group interviews were conducted.
Seven candidate institutions were invited for formal interviews, with one declining participation due to preparation for a government-mandated institutional inspection. A total of six focus groups were conducted, each consisting of 5 to 8 participants, with durations ranging from 77 to 156 minutes. All collected data were anonymized, encrypted, and securely stored with restricted access to authorized research personnel, ensuring data confidentiality. The interview recordings were transcribed verbatim within 72 hours following each interview, and the transcripts were subsequently returned to the corresponding participants for verification. Participants were allotted three working days to provide feedback regarding the accuracy of the transcripts and to supplement or revise their expressed views. A total of one supplementary comment was received from participants, all of which were incorporated into the final dataset for analysis. This validation procedure enhanced data credibility by confirming informational authenticity and minimizing interpretive bias.
Data Analysis
Data analysis was conducted employing both inductive and deductive thematic analysis methods.33,34 This combined approach to data analysis in qualitative studies has been previously employed to assess the influences on behavior within the healthcare sector.35–37 Inductive thematic analysis is data-driven and guided the initial phases of data analysis, effectively capturing participants’ perspectives and experiences. In contrast, deductive thematic analysis is theory-driven and guided the latter phases of data analysis, integrating the identified themes into established theoretical frameworks.
Initially, two researchers (JT and JL) conducted the inductive thematic analysis33 independently. The implementation procedures encompass the following steps. Step 1: Familiarizing with the data involved repeatedly engagement with interview transcripts and field notes to ensure a comprehensive understanding of the structural framework and content of data. Step 2: Generating initial codes entailed identifying information related to the challenges encountered during the transition to palliative care, thereby forming initial codes. Step 3: Searching for themes involved organizing the raw data corresponding to the initial codes and combining these codes meaningfully to provide valuable insights for the research question, ultimately identifying themes of broader significance. Step 4: Reviewing themes entailed examining the coded data under each theme to ensure that the coded content aligns with the original material. Data within the same theme should exhibit sufficient commonality and coherence, while data among different themes should demonstrate sufficiently distinct differences. Step 5: Theme conceptualization involved further analyzing the distinctions and connections among various themes, conducting iterative refinement of theme boundaries through team deliberation, and generating clear definitions and names for each theme. Step 6: Producing the report required integrating existing literature, raw data, initial codes, thematic concepts, and memos to ensure the results of the thematic analysis comprehensively address the research questions.
Based on the inductive thematic analysis, the identified themes were deductively mapped onto the social-ecological model. This process was led by researcher JT and JL, with support from XW, and finalized following discussions with QZ. Due to the limited understanding of the interest phenomenon, the deductive mapping was performed using the finalized themes rather than the original transcripts. This approach ensured that no relevant data potentially outside the scope of the social-ecological model was overlooked. Additionally, the deductive analysis offered an opportunity to validate the applicability of the social-ecological model in the context of Palliative Care Transitions.
Rigor and Trustworthiness
The rigor and trustworthiness of this study were established through the criteria of credibility, transferability, dependability, and confirmability.38 The combined professional expertise in palliative care and qualitative research of the researchers and a scientifically designed interview outline ensured the credibility of the study. A purposeful sampling approach using stratified sampling and maximum variation sampling enhanced the representativeness and transferability of the participants. Focus groups were conducted in a safe, open, and comfortable environment, with real-time audio recording and on-site field notes ensuring the confirmability of data collection. The interview recordings are transcribed promptly following each interview, and the resulting transcripts are returned to the participants for confirmation, correction, or supplementation, thereby ensuring the dependability of the data sources. Moreover, to enhance confirmability and reduce interpretive bias in the findings, this study employed analyst triangulation. Specifically, two researchers independently conducted the coding and analysis of the data, maintained a tracking record of the data collection and analysis process, and all team members participated in the discussion and interpretation of the results.
Results
The Sociodemographic Characteristics of Participants
A total of 39 participants (Table 2) came from a range of specialties, including nursing, psychology, nutrition, social work, and medicine. The majority of participants were female (N=32, 82%). Participants’ palliative care experience ranged from 0.5 to 10 years, ensuring a wide range of expertise (Table 2).
 |
Table 2 The Sociodemographic Characteristics of Participants |
Theme 1: Dilemmas in Individual End-of-Life Decision-Making Rights
Subtheme 1: Irrational Perceptions Hinder Rational Decision-Making
Information from non-official channels often leads to cognitive biases and misunderstandings regarding palliative care among patients with life-limiting illnesses. The stigmatized perceptions such as “waiting to die” and “euthanasia” position palliative care in opposition to rational decision-making for these patients. This misconception perpetuated by stigma delays patients’ transition to palliative care.
Patients often do not learn about palliative care through official channels, such as education provided by healthcare professionals, but rather through hearsay. Thus, some patients believe that choosing palliative care is “waiting to die”, while others equate it with “entering a nursing home” due to the absence of active treatment. These misconceptions may lead patients to resist or feel unwilling to choose palliative care, perceiving that opting for it signifies they have reached the “end of the road”. (Focus Group 1)
The understanding of palliative care remains inadequate. Many patients conflate palliative care with “euthanasia”, believing that opting for palliative care equates to “waiting to die”. This misconception contributes to their reluctance to transition to palliative care. (Focus Group 2)
Subtheme 2: The Agony of Life-and-Death Decision-Making
Patients with life-limiting illnesses frequently experience oscillating illness trajectories that precipitate existential dilemmas between the desire to live and the pursuit of relief. This dilemma encapsulates the agonizing decision-making process that patients face regarding the balance between life-prolonging interventions and quality-of-life optimization during the terminal phase of illnesses, which complicates their transition to palliative care.
Some patients experience fluctuations and changes in their condition during the course of treatment, which in turn affects their psychological state. For instance, when patients are in unbearable pain, they may wish for death as a means to escape their suffering. However, when the pain is managed, they may regain a desire to live, reigniting their hope and leading them to decide to undergo another round of chemotherapy in the hope of controlling the cancer. Yet, after chemotherapy, when their body cannot withstand the strain, they may once again wish for death, and this cycle continues. (Focus Group 1)
Subtheme 3: Protective Medical Practices Inducing Decision-Making Rights Squeeze
In cases of life-limiting diagnoses (eg., metastatic malignancies), some family members may communicate with healthcare professionals to implement protective medical practices for the patient, aiming to avoid severe psychological distress In this context, only family members are fully aware of the patient’s condition, while the patient themselves may be unaware or only partially informed Based on the principle of “benevolent concealment”, the absence of informed consent for patients can result in the erosion or even deprivation of the patient’s medical decision-making rights. The resultant therapeutic alienation transfers medical determination authority exclusively to surrogate decision-makers, who select “appropriate” interventions based on perceived patient interests rather than authentic patient values. Consequently, this situation presents a challenge for patients seeking to autonomously transition to palliative care.
Patients receiving protective medical care often lack complete aware about their own conditions, which hinders their ability to objectively assess their illnesses. Consequently, they frequently maintain high expectations for a cure and typically do not proactively request a transition to palliative care. (Focus Group 1)
Some family members are very insistent on implementing protective medical care, even after the patient has been admitted to the palliative care unit. They continue to insist on keeping the illnesses confidential. Consequently, only the family members are aware that the patient has entered the palliative care stage, while the patient remains unaware and is unable to make autonomous decisions. (Focus Group 1)
Theme 2: Multiple Constraints in the Family Fields
Subtheme 1: External Stigma of “Unfilial” Oppression
When families face the decision of transitioning a patient to palliative care, they must contend not only with public scrutiny and accountability from their social network for “not doing enough”, but also with concerns about being stigmatized as “unfilial”. Consequently, many families often equate “filial piety” with “overtreatment”, which lead to a blind insistence on life-sustaining technologies by family members, ultimately hindering a timely transition to palliative care.
Many family members, when deciding whether to admit a patient into hospice care, express concern about the opinions of others. For instance, if the patient passes away, other relatives are likely to ask, “How did the patient die?” and “Why wasn’t aggressive treatment pursued at the time?” As a result, family members take into account public opinion and pressure from relatives and friends, which may compel them to opt for aggressive treatment. (Focus Group 6)
Some family members fear that the public may perceive their choice of palliative care as an attempt to avoid spending money on the patient’s treatment or as a decision to forgo treatment altogether. Consequently, they worry about being labeled as “unfilial” and are therefore reluctant to allow the patient to enter palliative care. (Focus Group 2)
Under the influence of filial piety culture, family members often perceive that signing a palliative care consent form, at first glance, signifies a complete abandonment of efforts to rescue the patient. If this decision becomes known to other relatives and friends, it may generate a negative impression, prompting comments such as, “Why have you given up on treatment?” or “Why don’t you try treating them again?” Family members fear facing such pressure and criticism. (Focus Group 3)
Subtheme 2: Intrafamilial Disparities in Palliative Care Perceptions
Families of patients with life-limiting illnesses often exhibit cognitive disparities in palliative care due to socioeconomic inequities and intergenerational value conflicts. These disparities lead to divergent decision-making stances regarding the transition to palliative care. The polarized perspectives between prioritizing unconditional life extension and considering quality-of-life often result in decision-making deadlocks. Such deadlocks create ambiguous treatment goals and delay the decision-making process, ultimately compromising patients’ right to timely palliative care.
At the familial level, disparate perceptions of palliative care between patients and family members (eg., spouse and adult children) frequently result in discordant perspectives regarding palliative care transition decisions. (Focus Group 5)
Previously, we encountered a male patient in his 80s who had raised both a son and a daughter. The patient’s daughter, a corporate executive with a strong financial standing, believed that since the patient had devoted his entire life to the family, she should spare no effort in actively treating him. Conversely, the son felt that, given the patient’s advanced age and unclear consciousness, there was no need to pursue treatments that might increase his suffering. Instead, he believed that adopting palliative care measures to ensure the patient’s comfort and peace would be sufficient. (Focus Group 2)
Subtheme 3: Distorted Emotional Connection Among Family Members
When a patient with life-limiting illnesses, as a core family member, has been deeply involved in intergenerational support, the profound emotional connection often transform medical decision-making into a means of maintaining family cohesion. Family members often perceive life-sustaining interventions as a form of emotional reciprocation, yet simultaneously experience moral distress when witnessing patient suffering. This distortion of emotional connection reflects traditional family values that conflates “length of life” with “emotional value”, resulting in deviations from the patient’s best interests.
If a patient has made significant contributions to the family during the early stages of life and developed strong connection with family members, such as raising children and educating grandchildren, sacrificing entire life to meet the growth needs of family, the transition to palliative care can disrupt not only the family’s functionality but also tear the entire family apart. Family members may be unwilling to witness the patient’s suffering yet reluctant to cease treatment, hoping that the patient can live longer and remain with the family for a bit more time. (Focus Group 6)
Theme 3: Intrinsic Barriers in Healthcare Provision
Subtheme 1: Institutional Deficits in Palliative Care Literacy
Effective identifying patients with life-limiting illnesses who require palliative care is a prerequisite for facilitating a smooth transition to such care. However, non-palliative care professionals exhibit pervasive conceptual deficiencies regarding palliative care principles. This workforce literacy gap not only hinders their ability to effectively identify and assess patients’ palliative care needs but also leaves desperate patients and families without essential decision-making guidance, perpetuating therapeutic navigation challenges.
Apart from the professionals in the palliative care department, professionals in other departments generally possess a limited understanding of palliative care and lack a comprehensive of it. This deficiency hinders the timely transition of appropriate patients to palliative care. (Focus Group 2)
A cognitive barrier often exists in medical understanding between patients, their families, and healthcare professionals. This suggests that the breadth of knowledge among healthcare professionals directly influences that of patients. Consequently, the awareness and perspectives of healthcare professionals regarding palliative care are crucial. If their understanding of palliative care is limited, the information provided to patients and their families will be even scarcer, potentially leading them to overlook the option of transitioning to palliative care when they feel they have “no way out”. (Focus Group 6)
Subtheme 2: Professional Competence Gaps in Palliative Care Delivery
The robust professional competence of MDT in palliative care as the cornerstone for addressing the complex and diverse needs of patients with life-limiting illnesses. However, palliative care workforce shortages has resulted in ambiguous role definitions and the lack of a certification system, which collectively undermine the operational capacity to meet the transition needs of patients with life-limiting illnesses to palliative care.
Due to the insufficient number of palliative care professionals, many of us are required to assume multiple roles, which ultimately leads to compromise expertise depth. For example, while aromatherapy should ideally be conducted by specialized aromatherapists, it is often the nurses who are tasked with administering this therapy. As a result, there may be a noticeable gap in professional expertise when compared to that of specialized aromatherapists. (Focus Group 6)
The volunteers involved in palliative care are currently operating under an experience-dependent model characterized by low entry thresholds and insufficient training. The absence of standardized certification protocols and systematic training frameworks compromises volunteers’ empathic support competencies, thereby creating service provision gaps that fail to address the multidimensional needs of patients with life-limiting illnesses.
The volunteers in our department are primarily university students, whose life experiences are still developing. For instance, during my training in Taiwan, China, I observed that volunteers engaged in palliative care are not only evaluated based on their educational background but are predominantly retired individuals. These volunteers possess extensive life experiences and are more adept at communicating with patients from an equal perspective, which leads to improved outcomes in volunteer services. Currently, we are facing a significant shortage of such volunteers. (Focus Group 6)
Patients and their family members often face extreme situations as they confront death or the impending loss of a loved one. As a volunteer, I feel that my ability to provide meaningful comfort is limited, and I hesitate to offer casual words of consolation, fearing that they may inadvertently trigger negative emotions. If I were provided with effective training and the necessary qualifications, I believe I could perform volunteer service more effectively. (Focus Group 4)
Subtheme 3: Deficiency in Quality Control System for Palliative Care
The types of institutions providing palliative care and the service scenarios in China are becoming increasingly diverse. However, a standardized system for palliative care tailored to different institutional types and service scenarios has remained incomplete. This lag in the standardization of palliative care development consequently impedes the homogeneous quality assurance of palliative care.
Due to the differing nature of institutions (eg., medical institutions, integrated medical and elderly care institutions, and elderly care institutions) and the varying contexts (eg., hospitals, communities, and homes) in which palliative care, there are notable differences and particularities in the target population, content, and processes of palliative care. To ensure the smooth implementation of palliative care across these diverse institutions and contexts, specific and practical standard guidelines are necessary. (Focus Group 5)
Prognostic survival period serves as a pivotal indicator for evaluating whether patients with life-limiting illnesses should transition to palliative care. Accurate and reliable survival prediction facilitates clarifying treatment goals, optimizing therapeutic regimens, assisting patients and families in decision-making, and rationally arranging subsequent matters. However, when medical and nursing interventions are involved, survival assessment tools represented by the Karnofsky Performance Scale (KPS) still face issues regarding their accuracy and scientific validity, which hinders the precise determination of the optimal timing for transitioning to palliative care.
The Karnofsky Performance Scale is a commonly used clinical tool for assessing survival, primarily predicting a patient’s prognosis based on their physical condition. However, for patients and their families preparing to receive palliative care within an institution, there is often a certain level of medical and nursing care provided, such as oxygenic therapy, sputum suction, and nasogastric feeding, aimed at promoting patient comfort. These seemingly straightforward medical and nursing procedures can significantly influence the patient’s expected survival, resulting in notable discrepancies between estimated and actual survival times. We have encountered several patients whose initial assessments upon admission predicted a survival of less than one month, yet they remained in the department for much longer than anticipated. (Focus Group 3)
Theme 4: Constraints Shaped by Social Environment
Subtheme 1: Insufficient Funding Support for Palliative Care
Funding for palliative care primarily comprises government allocations and social capital. However, inadequate government investment has resulted in heavy reliance on internal subsidies from health institutions, while insufficient social funding prevents operational costs from being offset through market-based mechanisms. This macroscopically impedes the sustainable development of palliative care and, on a micro level, undermines the willingness of patients and their families to opt for palliative care.
The provision of palliative care necessitates financial support; however, local government departments do not offer subsidies to palliative care departments or practitioners. Consequently, hospitals either provide direct financial support or other departments within the hospital utilize their performance bonuses to subsidize palliative care. Given that hospitals must prioritize profitability, they cannot indefinitely sustain reverse subsidies. This situation is undoubtedly not a sustainable long-term solution. (Focus Group 1)
Many services in palliative care are closely associated with humanistic care, exemplified by the frequent purchase of flowers, cakes, photo albums, and cards to fulfill patients’ wishes. However, these expenses often lack financial support from government subsidies or social funds, necessitating departments to independently address the issue through methods such as collecting activity fees from practitioners. (Focus Group 2)
Subtheme 2: Ambiguous Palliative Care Pricing Mechanisms
Although policies has proposed that palliative care can be charged by bed-day or service project, the absence of integration into the healthcare insurance system has led to a lack of detailed and specific pricing standards. Notably, regulatory delays in pricing emerging services such as aromatherapy within the healthcare insurance framework have trapped palliative care implementation in a detrimental cycle of being “operationally viable yet financially unsustainable, desired yet unprofitable”.
Currently, the aromatherapy program, as a part of our palliative care offerings, has shown relatively good efficacy in managing symptoms such as edema and pain in patients. However, it is not covered by healthcare insurance, lacks a clear fee standard, and therefore cannot be charged to patients. (Focus Group 3)
We recognize the value and importance of palliative care and are eager to participate in its implementation. However, palliative care has yet to be integrated into the healthcare insurance system, and the fee standards for palliative care remain ambiguous. As a result, many palliative care initiatives cannot be billed appropriately, leading to a situation where departmental involvement in palliative care is nearly unprofitable. This presents a substantial barrier to the progress of palliative care initiatives. (Focus Group 4)
Subtheme 3: Absence of Practitioner Safeguards in Palliative Care
In comparison to the exploration and implementation of palliative care legislation in the international community, China’s legal documents regarding palliative care require enhancements to ensure the occupational safety of practitioners and to prevent unnecessary disputes.
In the field of palliative care, although numerous relevant policy documents have been issued in mainland China, currently only Shenzhen has enacted legislation concerning living wills. To our knowledge, many countries and regions have already established laws and regulations related to palliative care. Once a patient is determined to be transitioned to palliative care, the specific measures implemented by practitioners, such as symptom control and comfort care, are considered legal. Legal protection is essential, as clearly defined palliative care practices can help resolve many potential medical disputes. (Focus Group 6)
Moreover, palliative care practice constitutes an emotionally, physically, and temporally intensive profession. Yet, practitioners’ specialized efforts fail to translate into equitable economic returns, and the economic value of their labor remains inadequately recognized.
The emotional, temporal, and energetic resources expended in delivering palliative care far exceed those required for routine medical care. For instance, conducting a family conference may take half a day, which is significantly longer than the time a nurse spends administering an injection or sputum suction. While the latter can yield clear economic value, the former can only be documented in medical records as evidence of the physical and psychological care provided to the patient and their family. (Focus Group 3)
Subtheme 4: Socially Entrenched Perceptions of Life and Death
Within the cognitive paradigm of traditional Chinese perspectives on life and death, the public often perceives death as a taboo subject to be avoided. As a result, palliative care, which should be considered a reasonable approach to medical intervention, is relegated to a mere symbol of life’s demise. This relegation places palliative care in a gray area of cultural cognition, rendering it an “other”, shunning and avoiding in collective consciousness.
The public’s perception of life and death can significantly hinder their choices regarding palliative care. Throughout an individual’s life, opportunities to confront death are quite limited, typically arising only through the loss of close friends or family members. When removed from these familiar contexts, death becomes a taboo subject for many, resulting in a reluctance to engage with it actively. This inherent aversion to death causes the public to instinctively resist the concept of palliative care. (Focus Group 1)
Influenced by traditional Chinese perspectives on life and death, the public often perceives “death” as a negative term, representing the conclusion of existence and the absence of hope. Consequently, since palliative care is regarded as a gateway to death, the public tends to resist it. (Focus Group 4)
Discussion
This study was grounded in the social-ecological model and systematically elucidated that the challenges of palliative care transition emerged from four interrelated dimensions, as revealed through multi-perspective qualitative data obtained from multi-center focus groups: individual rights, family fields, healthcare provision, and social environment. This framework not only synthesized the core findings of the study but also offered a cohesive theoretical perspective for interpreting the challenges of palliative care transition across various layers. A scoping review conducted in the United Kingdom reported similar findings, where researchers, utilizing the socio-ecological theoretical framework, identified barriers in the transition to palliative care for children and adolescents with life-limiting illnesses across individual, interpersonal, organizational, community, and societal levels.39 Moreover, the findings observed in this study regarding a certain theme and sub-theme align with those of existing single-perspective studies, such as those from the perspectives of doctors or nurses.40–43 The study incorporated insights from a multidisciplinary palliative care team, which not only corroborated the core conclusions of existing research but also elucidated the differences in the challenges faced during palliative care transition from the perspectives of various stakeholders, thereby providing a more comprehensive empirical foundation for understanding these challenges in the mainland Chinese context.
The life decision-making rights dilemma faced by patients with life-limiting illnesses constitutes a major challenge hindering their transition to palliative care. Firstly, informal sources of information often lead patients to misinterpret palliative care as merely “waiting to die” and “euthanasia”, thereby obstructing rational decision-making regarding palliative care transition. As noted in the study by Hugar et al,44 cancer patients and caregivers often equated palliative care with curative treatment or institutional care based on unverified online sources; similarly, Shalev et al45 highlighted that community-dwelling adults frequently conflated palliative care with euthanasia This phenomenon may be related to the unique amplification mechanisms of misconceptions surrounding palliative care. Firstly, during the early development period of palliative care in mainland China, issues such as inconsistent terminology and conceptual confusion arose, resulting in a lack of unified standards for information dissemination. Secondly, personal social media accounts (eg., Weibo), along with networks of friends and family, serve as the primary sources through which the Chinese individual acquires information about palliative care. The insufficient presence of authoritative information sources exposes the public to biased, emotional, or even erroneous information. Second, the agonizing conflict between prolonging life and preserving quality of life during terminal stages creates decision-making paralysis that impedes palliative care transition. A Chinese study reported similar findings, where inadequate decision-making support triggered helplessness and indecision in patients, resulting in transitional barriers.46
Third, the deprivation of informed consent under protective medical practices, a system that withholds full diagnosis or treatment information from patients with conditions like cancer to mitigate psychological distress,47 exacerbates challenges in autonomous decision-making. In mainland China, although laws such as the “Medical Practitioners Law”, the “Regulations on Handling Medical Accidents”, and the “Implementation Rules for Medical Institution Management Regulations” grant patients the right to be informed, the healthcare system predominantly operates under protective medical practices. Legally, this practice prioritizes informing family caregivers about the patient’s condition “to protect the patient’s interests”, thereby establishing a hierarchical relationship in information disclosure between family caregivers and patients with life-limiting illnesses. Consequently, the information disclosure model in mainland China adopts a family-centered approach.48,49 This model is characterized by family caregivers who communicate on behalf of both patients and physicians. As a result, family caregivers exercise initiative and decision-making power in the process of information disclosure, focusing on the overall interests of the family.48,50 Although designed to safeguard patient interests, such practices paradoxically deprive patients of their autonomy over end-of-life decision-making. The hypothetical benefits of protective medical practices are overshadowed by their tangible harms, as the envisioned “protection” fails to outweigh the evident infringement on patients’ rights.51
Addressing the challenges of dilemmas in individual life decision-making rights requires targeted interventions. Authoritative information dissemination through health institutions and government-endorsed media could rectify misconceptions about palliative care and reduce decision-making conflicts. Furthermore, implementing advance care planning (ACP), a structured process enabling individuals to articulate their values, life goals, and healthcare preferences,52 not only improved the consistency of patients’ future medical decisions but also upholds their autonomy over life,53 serving as a critical measure to resolve life-rights dilemmas in palliative care transitions. The implementation of ACP must take into account the cultural characteristics of Chinese families and establish a shared decision-making model that is both patient-led and family-involved. Such as approach would significantly enhance the acceptability and effectiveness of ACP within the local context.
Family fields refer to the relational network governing interactions among family members, shaped by ethical norms, logical imperatives, and cultural rules (eg., intergenerational dynamics)54 This study reveals that multifaceted constraints within the family fields significantly hinder the transition of patients with life-limiting illnesses to palliative care In Chinese culture, filial piety, rooted in Confucian philosophy, embodies a moral framework emphasizing respect and care for parents55 However, filial piety is socially evaluated, wherein children are judged by whether they provide their parents with what is considered appropriate and proper by societal standards during significant life events, such as life-limiting illnesses. This is often manifested in the overtreatment of parents with life-limiting illnesses, where the decision to treat or not is driven by “face-saving concerns”.56 Consistent with our findings, family members frequently opt for overtreatment to avoid social stigma, thereby delaying palliative care transitions. Reconceptualizing filial piety and recalibrating its application thus emerge as urgent cultural imperatives.
Moreover, cognitive disparities arising from intergenerational values and unequal economic resource allocation within families exacerbate decision-making conflicts. Kirby et al57 similarly identified unresolved familial discord as a dominant barrier to palliative care acceptance. Notably, profound emotional connection among family members can paradoxically fuel irrational medical decision-making. When patients have served as central pillars of intergenerational support, families often perceive life extension, despite observable suffering, as an emotional obligation, even at the cost of prolonging patient distress. The irrational medical decision-making induced by the abnormal reinforcement of familial emotional connections is not merely a result of emotional reactions; rather, it is deeply rooted in the cultural tradition of “family-oriented” values in China. In many Chinese families, a patient’s life is not viewed solely as an individual concern, but rather as a shared responsibility and a symbol of the family’s value.58,59 Consequently, the act of “receiving palliative care” is often perceived by family members as a deviation from familial responsibility, rather than merely a medical choice. This finding underscores that simple interventions related to palliative care information are insufficient to fundamentally alter the logic of family decision-making. It is essential to reconstruct the internal communication patterns and responsibility awareness within families through methods such as family conferences. As an effective communication channel, the family conference serves as a platform for healthcare professionals to convey disease-related information to patients and their families. It not only facilitates a comprehensive assessment of the needs of both patients and their families and provides emotional support, but also enables a joint discussion on care goals and strategies to reach a consensus.60 This approach can be an effective strategy for fostering a shared understanding of palliative care within the family and preventing the distortion of emotional connection among family members.
Systemic barriers in healthcare provision, manifested through institutional deficits in palliative care literacy, professional competence gaps in palliative care delivery, and deficiencies in the quality control system for palliative care, significantly impede patients’ transition to palliative care. This study revealed a widespread lack of palliative care literacy among non-palliative care professionals in health institutions. Studies corroborate this finding,6,14,61,62 documenting that non-palliative care professionals often conflate palliative care concepts, remain uncertain about transition criteria and timing, and delay transitions due to “fear of losing patient management control” or “equating the transition to palliative care with abandoning patients”. Consequently, decisions to discontinue aggressive treatments frequently occur only when death is imminent. Another critical challenge lay in the shortage of trained professionals and suboptimal expertise among existing palliative care professionals. According to the APHN Atlas of Palliative Care in the Asia Pacific Regions 2025, palliative care remains largely absent from compulsory undergraduate medical and nursing curricula, and is often limited to elective training or postgraduate programs without official educational endorsement.63 This deficiency contributes significantly to the inadequate competency of existing palliative care professionals. Therefore, it is crucial to incorporate palliative care as a required component of medical and nursing education and to establish standardized continuing education programs with practitioner certification.6,61,64 Clinicians with expertise in palliative care are well-positioned to spearhead this educational advancement. While standards, guidelines, and guidance aim to standardize clinical protocols,6 this study identified critical gaps in palliative care quality control systems, particularly the underdevelopment of standardized frameworks and insufficient accuracy in survival prediction tools. Studies have reported analogous challenges.41,46,62 The ambiguous admission and discharge criteria across palliative care tiers not only hinder physicians from easily and effectively identifying eligible patients but also result in non-standardized referral pathways and channels for palliative care.46,62 Overestimation of survival prognoses further complicates timely palliative care initiation, as physicians may delay transitions due to prognostic uncertainty.65 It is clear that establishing evidence-based standards, guidelines, and screening tools is essential, not only to effectively bridge the widespread literacy gap in palliative care among healthcare professionals but also to facilitate a more proactive and informed transition to palliative care.40,66
This study identified four constraints shaped by the social environment affecting palliative care transition. First, insufficient government allocations and social capital in palliative care remained a critical barrier. The National Cancer Institute faces similar challenges in other countries, as the majority of funding is concentrated on cancer prevention, diagnosis, and treatment studies. In contrast, less than 1.0% of the total budget is allocated to research in palliative and hospice care services.64 Second, similar to many countries,6,40,62 palliative care has not yet been integrated into the healthcare insurance system, and the fee standards remain unclear, which hinders patients’ transition to palliative care. For instance, a study revealed insufficient coverage of palliative care payments in the United States, where not only is home-based palliative care excluded from coverage, but only 10–15% of insurance companies currently reimburse palliative care costs, collectively deterring patients from transitioning to palliative care.62 Meanwhile, the Gold Standards Framework (GSF) in the United Kingdom, recognized as the first training program aimed at improving the quality of end-of-life patient management, has provided standardized guidance for general practitioners in palliative care practices.67,68 In contrast, China’s palliative care workforce lacks comparable legal and economic safeguards, destabilizing professional retention and palliative care quality. Finally, pervasive cultural taboos surrounding death and dying suppress public expression of palliative care needs.6,69 In China, the pervasive influence of Confucianism, Buddhism, and Taoism philosophies has entrenched rigid societal attitudes toward mortality. Similarly, studies conducted in the United States have highlighted how sociocultural perceptions of death influence palliative care acceptance.6,69 Initiatives like the “Dying Matters initiative” in the United Kingdom demonstrate the value of public death education in normalizing discussions about mortality. To address these challenges, three-pronged systemic reform is imperative. First, it is essential to formulate specific fiscal policies and detailed medical insurance coverage for palliative care. Second, promoting legislation on palliative care and safeguarding the rights of practitioners is crucial. Third, conducting universal death education for the general public is necessary to eliminate the taboo surrounding death.
Limitations
This study has several limitations. Firstly, although this was a multicenter qualitative study drawn all participants from a single city in southwestern China. This limitation may restrict the generalizability of the findings to other regions with differing socioeconomic contexts, healthcare systems frameworks, and aging population profiles. Future research should consider conducting studies across various regions and countries to enhance the representativeness of the results. Secondly, this study adopted a cross-sectional design with data collected within a two-month period. While this approach provides a comprehensive snapshot of MDTs’ perceptions of the challenges in palliative care transitions at the time of data collection, it does not allow for tracking long-term systemic changes in palliative care transition practices. Future research could benefit from employing a longitudinal study design to monitor the challenges of palliative care transitions over time. Thirdly, since this study relied on self-reported experiences from healthcare professionals, the findings may have been influenced by social desirability bias, where participants might provide responses that align with professional norms or organizational expectations. Although confidentiality and voluntary participation were emphasized throughout the study, this bias cannot be entirely eliminated. Future research could enhance the credibility and trustworthiness of findings through strategies such as methodological triangulation, prolonged engagement, and member checking. Finally, although this study focused on a MDT involved in palliative care practice, the overall development level of palliative care in mainland China, particularly in Chongqing, has severely limited the availability of professionals such as volunteers and nutritionists in this field.70,71 Consequently, there is a low representation of these groups in the study sample. This limitation may hinder a comprehensive exploration of the profession-based challenges associated with the transition in palliative care. Future research could specifically target groups such as volunteers and nutritionists to better identify the profession-related challenges encountered during this transition.
Conclusions
Guided by the social ecological model, MDTs offer a unique and comprehensive perspective to assist researchers in identifying challenges during the palliative care transition process. Based on focus group interviews with multidisciplinary palliative care teams from six medical institutions in Chongqing, China, this study demonstrated that palliative care transition faced multi-layered challenges spanning micro to macro systems, including dilemmas in individual life decision-making rights, multiple constraints in the family fields, systemic barriers in healthcare provision, and constraints shaped by the social environment. Notably, novel challenges, such as the protective medical care paradox, external stigma of “unfilial” oppression, and distortion of emotional connection among family members require particular attention and further exploration in countries and regions with similar healthcare and sociocultural contexts.
Based on the findings of this study, we propose a targeted multi-layered intervention prototype that provides specific and feasible strategies for transitioning from problem identification to resolution, thereby promoting the establishment and enhancement of palliative care service systems. The content of the intervention prototype is as follows: At the patient level, short-term interventions can be implemented through ACP consultations within the local context, thereby preserving patients’ rights of end-of-life decision-making. Furthermore, the long-term dissemination of authoritative and accurate palliative care information via media recognized by medical institutions and national governments can enhance awareness of individual end-of-life decision-making rights, thereby establishing a foundation for their future maintenance. At the patients’ families level, short-term initiatives may involve the scientific organization of family conferences aimed at resolving decision-making conflicts and distortions in emotional connection, thereby facilitating the transition to palliative care for patients with life-limiting illnesses. In the long term, it is essential to explore and address the reconceptualization of filial piety and its recalibration to support the transition to palliative care, considering the developmental processes of local palliative care services. At the healthcare institutions level, it is essential for existing palliative care experts to collaboratively establish evidence-based standards, guidelines, and screening tools in the short term to promote the standardization and homogenization of palliative care transitions. In the long term, it is crucial to encourage national government departments to establish standardized continuing education programs with practitioner certification, as well as to incorporate palliative care as a mandatory component of medical and nursing education. At the social environment level, short-term efforts should focus on conducting universal death education for the general public to eliminate the taboo surrounding death. In the long term, national government departments should formulate specific fiscal policies and detailed medical insurance coverage for palliative care, while also establishing laws and regulations that safeguard the rights of palliative care practitioners.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Chongqing Medical University in September 2023 (No. 2023080). Before formally inviting participants, official permission was obtained from the health institutions where the participants were affiliated. All participants signed a written informed consent form, which includes publishing anonymous responses/direct citations. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki (as revised in Helsinki 2024).
Acknowledgments
The authors appreciate the participants in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study is funded by the National Key R&D Program of China (No. 2023YFC3605900/03).
Disclosure
The authors declare no competing interests in this work.
References
1. Sleeman KE, de Brito M, Etkind S, et al. The escalating global burden of serious health-related suffering: projections to 2060 by world regions, age groups, and health conditions. Lancet Glob Health. 2019;7(7):e883–18. doi:10.1016/S2214-109X(19)30172-X
2. World Health Organization. Palliative care. Palliative care: key facts. 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/palliative-care.
3. Haun MW, Estel S, Rücker G, et al. Early palliative care for adults with advanced cancer. Cochrane Pain, Palliative and Supportive Care Group, ed. Cochrane Database Syst Rev. 2017;2017(6). doi:10.1002/14651858.CD011129.pub2
4. Dionne-Odom JN, Azuero A, Lyons KD, et al. Benefits of early versus delayed palliative care to informal family caregivers of patients with advanced cancer: outcomes from the ENABLE III randomized controlled trial. JCO. 2015;33(13):1446–1452. doi:10.1200/JCO.2014.58.7824
5. Hui D, Hannon BL, Zimmermann C, Bruera E. Improving patient and caregiver outcomes in oncology: team-based, timely, and targeted palliative care. CA a Cancer J Clinicians. 2018;68(5):356–376. doi:10.3322/caac.21490
6. Kaasa S, Loge JH, Aapro M, et al. Integration of oncology and palliative care: a lancet oncology commission. Lancet Oncol. 2018;19(11):e588–e653. doi:10.1016/S1470-2045(18)30415-7
7. Coleman EA, Boult C. American geriatrics society health care systems Committee. Improving the quality of transitional care for persons with complex care needs. J Am Geriatr Soc. 2003;51(4):556–557. doi:10.1046/j.1532-5415.2003.51186.x
8. Bennett M, Adam J, Alison D, Hicks F, Stockton M. Leeds eligibility criteria for specialist palliative care services. Palliat Med. 2000;14(2):157–158. doi:10.1191/026921600669491513
9. Thomas K, Noble B. Improving the delivery of palliative care in general practice: an evaluation of the first phase of the gold standards framework. Palliat Med. 2007;21(1):49–53. doi:10.1177/0269216306072501
10. Lynn J, Schall MW, Milne C, Nolan KM, Kabcenell A. Quality improvements in end of life care: insights from two collaboratives. Jt Comm J Qual Improv. 2000;26(5):254–267. doi:10.1016/s1070-3241(00)26020-3
11. Gu X, Cheng W, Chen M, Liu M, Zhang Z. Timing of referral to inpatient palliative care services for advanced cancer patients and earlier referral predictors in mainland China. Pall Supp Care. 2016;14(5):503–509. doi:10.1017/S1478951515001212
12. Xiao YZ, Chen YY. Chinese Cancer Integrated Diagnosis and Treatment Technical Guidelines: Palliative Care. Tianjin, China: Tianjin Science and Technology Press; 2023.
13. ALMouaalamy N, AlMarwani K, AlMehmadi A, et al. Referral time of advance cancer patients to palliative care services and its predictors in specialized cancer center. Cureus. 2020;12(12). doi:10.7759/cureus.12300
14. Quaidoo TG, Adu B, Iddrisu M, et al. Unlocking timely palliative care: assessing referral practices and barriers at a ghanaian teaching hospital. BMC Palliat Care. 2024;23(1):90. doi:10.1186/s12904-024-01411-9
15. Earle CC, Neville BA, Landrum MB, et al. Evaluating claims-based indicators of the intensity of end-of-life cancer care. Int J Qual Health Care. 2005;17(6):505–509. doi:10.1093/intqhc/mzi061
16. Earle CC, Park ER, Lai B, Weeks JC, Ayanian JZ, Block S. Identifying potential indicators of the quality of end-of-life cancer care from administrative data. JCO. 2003;21(6):1133–1138. doi:10.1200/JCO.2003.03.059
17. Mintzer DM, Zagrabbe K. On how increasing numbers of newer cancer therapies further delay referral to hospice: the increasing palliative care imperative. Am J Hosp Palliat Care. 2007;24(2):126–130. doi:10.1177/1049909106297363
18. Binns-Emerick L, Patel P, Deol BB, Kang M. Multidisciplinary palliative care of the older adult: a narrative review. Ann Palliat Med. 2024;13(4):1002–1011. doi:10.21037/apm-23-541
19. Liang M, Liang J, Xu J, Chen Q, Lu Q. Experience of multidisciplinary medical teams on humanistic palliative care in oncology wards: a descriptive qualitative study in Southern China. BMJ Open. 2024;14(2):e074628. doi:10.1136/bmjopen-2023-074628
20. Liu YJ, Wu LP, Wang H, Han Q, Wang SN, Zhang J. The clinical effect evaluation of multidisciplinary collaborative team combined with palliative care model in patients with terminal cancer: a randomised controlled study. BMC Palliat Care. 2023;22(1):71. doi:10.1186/s12904-023-01192-7
21. Palliative Care ProfessionalCommittee of Chinese Nursing Association. Expert consensus on shared care management for adult palliative care patients. Chin J Nurs. 2026;61(1):53–56.
22. Willemsen AM, Mason S, Zhang S, Elsner F. Status of palliative care education in mainland China: a systematic review. Palliat Support Care. 2021;19(2):235–245. doi:10.1017/S1478951520000814
23. Niu J, Feng M, Song C, Xie H. Self-reported knowledge and difficulties towards palliative care among healthcare professionals in rural China: a cross-sectional study. BMC Palliat Care. 2025;24(1):37. doi:10.1186/s12904-025-01674-w
24. Bronfenbrenner U. The Ecology of Human Development: Experiment by Nature and Design. Hlarvard University Press; 1979.
25. Doyle L, McCabe C, Keogh B, Brady A, McCann M. An overview of the qualitative descriptive design within nursing research. J Res Nurs. 2020;25(5):443–455. doi:10.1177/1744987119880234
26. Sandelowski M. What’s in a name? Qualitative description revisited. Research in Nursing & Health. 2010;33(1):77–84. doi:10.1002/nur.20362
27. Carter N, Bryant-Lukosius D, DiCenso A, Blythe J, Neville AJ. The use of triangulation in qualitative research. Oncol Nurs Forum. 2014;41(5):545–547. doi:10.1188/14.ONF.545-547
28. Hudson P. Focus group interviews: a guide for palliative care researchers and clinicians. Int J Palliat Nurs. 2003;9(5):202–207. doi:10.12968/ijpn.2003.9.5.11490
29. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
30. National Bureau of Statistics. The seventh national population census bulletin (No 5.). Available from: http://www.stats.gov.cn/sj/zxfb/202302/t20230203_1901085.html.
31. Benoot C, Hannes K, Bilsen J. The use of purposeful sampling in a qualitative evidence synthesis: a worked example on sexual adjustment to a cancer trajectory. BMC Med Res Methodol. 2016;16:21. doi:10.1186/s12874-016-0114-6
32. Fraser H. Doing narrative research: analysing personal stories line by line. Qual Soc Work. 2004;3(2):179–201. doi:10.1177/1473325004043383
33. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
34. Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: implications for conducting a qualitative descriptive study. Nurs Health Sci. 2013;15(3):398–405. doi:10.1111/nhs.12048
35. Moffat A, Cook EJ, Chater AM. Examining the influences on the use of behavioural science within UK local authority public health: qualitative thematic analysis and deductive mapping to the COM-B model and theoretical domains framework. Front Public Health. 2022;10:1016076. doi:10.3389/fpubh.2022.1016076
36. Maine A, Dickson A, Truesdale M, Brown M. An application of bandura’s “four sources of self-efficacy” to the self-management of type 2 diabetes in people with intellectual disability: an inductive and deductive thematic analysis. Res Dev Disabil. 2017;70:75–84. doi:10.1016/j.ridd.2017.09.004
37. Darrah T, Herbert S, Chambers T. A thematic analysis of alcohol and alcohol-related harm across health and social policy in aotearoa New Zealand. Aust N Z J Public Health. 2024;48(2):100143. doi:10.1016/j.anzjph.2024.100143
38. Krefting L. Rigor in qualitative research: the assessment of trustworthiness. Am J Occup Ther. 1991;45(3):214–222. doi:10.5014/ajot.45.3.214
39. Holder P, Coombes L, Chudleigh J, Harding R, Fraser LK. Barriers and facilitators influencing referral and access to palliative care for children and young people with life-limiting and life-threatening conditions: a scoping review of the evidence. Palliat Med. 2024;38(9):981–999. doi:10.1177/02692163241271010
40. Cole CS, Jackson A, Bennett CR, et al. Nursing home palliative care referral process, barriers, and proposed solutions: a qualitative study. J Appl Gerontol. 2025;44(4):582–590. doi:10.1177/07334648241286326
41. Coombs MA, Addington-Hall J, Long-Sutehall T. Challenges in transition from intervention to end of life care in intensive care: a qualitative study. Int J Nurs Stud. 2012;49(5):519–527. doi:10.1016/j.ijnurstu.2011.10.019
42. Enguidanos S, Cardenas V, Wenceslao M, et al. Health care provider barriers to patient referral to palliative care. Am J Hosp Palliat Care. 2021;38(9):1112–1119. doi:10.1177/1049909120973200
43. Woodrell CD, Mulholland CN, Goldstein NE, Hutchinson CL, Schiano TD, Hansen L. Clinician perspectives on palliative care for people with hepatocellular carcinoma: facilitators of and barriers to referral. Cancers. 2023;15(14):3617. doi:10.3390/cancers15143617
44. Hugar LA, Geiss C, Chavez MN, et al. Exploring knowledge, perspectives, and misperceptions of palliative care: a mixed methods analysis. Urologic Oncol. 2023;41(7):327.e19–327.e26. doi:10.1016/j.urolonc.2023.03.016
45. Shalev A, Phongtankuel V, Kozlov E, Shen MJ, Adelman RD, Reid MC. Awareness and misperceptions of hospice and palliative care: a Population-Based Survey Study. Am J Hosp Palliat Care. 2018;35(3):431–439. doi:10.1177/1049909117715215
46. Liu Y, Xu Y, Kang Y, Wu L, Zhou Y, Yuan L. Experiences and barriers in downward referral decision-making for palliative care patient caregivers under China’s three-tiered linkage model: a qualitative study. Asia PacJ Oncol Nurs. 2025;12:100578. doi:10.1016/j.apjon.2024.100578
47. Yu YS. The introduction of pavlovian theory and the change of the medical system in china in the 1950s: focusing on the construction of the protective medical system. Korean J Med Hist. 2020;29(2). doi:10.13081/kjmh.2020.29.613
48. Liu Q, Xu K. Family resilience habitus: a theoretical tool for understanding the cultural context of terminal illness disclosure. J Hubei Minzu Univer. 2025;43(1):23–33. doi:10.13501/j.cnki.42-1328/c.2025.01.001
49. Zhang HS, Yang LL. Family modelof cancer condition notification. Med Philosophy. 2020;41(9):17–19. doi:10.12014/j.issn.10020772.2020.09.05
50. Sun LP, Li L, Ye ZX. Development of disclosure of cancer diagnosis in cancer patients: the past and the present. J Nurs Sci. 2013;28(11):94–96. doi:10.3870/hlx2z.2013.11.094
51. Li XH, Li M. Protective medicine system and its legalissuesin China. Med Philosophy. 2021;42(2):58–61. doi:10.12014/j.issn.1002-0772.2021.02.12
52. Sudore RL, Lum HD, You JJ, et al. Defining advance care planning for adults: a consensus definition from a multidisciplinary delphi panel. J Pain Sympt Manage. 2017;53(5):821–832.e1. doi:10.1016/j.jpainsymman.2016.12.331
53. Chan CW, Wong MM, Choi KC, et al. What patients, families, health professionals and hospital volunteers told us about advance directives. Asia PacJ Oncol Nurs. 2019;6(1):72–77. doi:10.4103/apjon.apjon_38_18
54. Luo JM. Health communication of family field in the era of new media. Nanchang Univer. 2023. doi:10.27232/d.cnki.gnchu.2022.001601
55. Li WW, Singh S, Keerthigha C. A Cross-Cultural Study of filial piety and palliative care knowledge: moderating effect of culture and universality of filial piety. Front Psychol. 2021;12:787724. doi:10.3389/fpsyg.2021.787724
56. Sun YJ, Chen Y. Pricing priceless parents: economic expenditure and filial piety practice in elderly hospice care. Soc Sci Guangdong. 2025;(2):195–210.
57. Kirby E, Broom A, Good P, Wootton J, Adams J. Families and the transition to specialist palliative care. Mortality. 2014. doi:10.1080/13576275.2014.916258
58. Yang Y, Qu T, Yang J, Ma B, Leng A. Confucian familism and shared decision making in end-of-life care for patients with advanced cancers. Int J Environ Res Public Health. 2022;19(16):10071. doi:10.3390/ijerph191610071
59. Cheng M, Luo Q, Fang C, Comery A, Troyer J. Exploring good death in China: a qualitative study from the perspectives of family members. Soc Sci Med. 2025;367:117727. doi:10.1016/j.socscimed.2025.117727
60. Hudson P, Quinn K, O’Hanlon B, Aranda S. Family meetings in palliative care: multidisciplinary clinical practice guidelines. BMC Palliat Care. 2008;7:12. doi:10.1186/1472-684X-7-12
61. Kavalieratos D, Mitchell EM, Carey TS, et al. “Not the ‘Grim Reaper Service’”: an assessment of provider knowledge, attitudes, and perceptions regarding palliative care referral barriers in heart failure. JAHA. 2014;3(1):e000544. doi:10.1161/JAHA.113.000544
62. Enguidanos S, Lomeli S, Kogan AC, Rahman A, Lewis N. Home-Based palliative care team perspectives on challenges in patient referral and enrollment. J Pain Sympt Manage. 2022;63(5):665–672. doi:10.1016/j.jpainsymman.2022.01.011
63. Monzón L, Tripodoro VA, Hamzah E, et al. APHN atlas of palliative care in the Asia pacific regions 2025. APHN. Available from: https://aphn.org/the-aphn-atlas-of-palliative-care-in-the-asia-pacific-regions-2025/.
64. Knaul FM. Integrating palliative care into health systems is essential to achieve universal health coverage. Lancet Oncol. 2018;19(11):e566–e567. doi:10.1016/S1470-2045(18)30600-4
65. Van Der Stap L, De Nijs EJM, Oomes M, et al. The self-perceived palliative care barriers and educational needs of clinicians working in hospital primary care teams and referral patterns: lessons learned from a single-center survey and cohort study. Ann Palliat Med. 2021;10(3):2620–2637. doi:10.21037/apm-20-1706
66. Shalev A, Phongtankuel V, Lampa K, et al. Examining the role of primary care physicians and challenges faced when their patients transition to home hospice care. Am J Hosp Palliat Care. 2018;35(4):684–689. doi:10.1177/1049909117734845
67. Quinn B, Thomas K. Using the gold standards framework to deliver good end of life care. Nurs Manag. 2017;23(10):20–25. doi:10.7748/nm.2017.e1581
68. Teo SP, Chong JX, Venkatasalu MR. Internationalisation of gold standards framework use in primary health care. Age Ageing. 2018;47(5):762. doi:10.1093/ageing/afy100
69. Disler R, Pascoe A, Luckett T, et al. Barriers to palliative care referral and Advance Care Planning (ACP) for patients with COPD: a cross-sectional survey of palliative care nurses. Am J Hosp Palliat Care. 2022;39(2):169–177. doi:10.1177/10499091211018192
70. National Health Commission of the People ‘s Republic of China. Reply to proposal No. 1103 (Medical and sports category No. 109) at the third session of the 13th national committee of the Chinese people’s political consultative conference. Available from: https://www.nhc.gov.cn/wjw/tia/202101/ca0463ef98d64b21adf1bdf6da2c19da.shtml.
71. Chongqing Health Commission. Reply on the handling of suggestion No. 0883 submitted at the 3rd session of the 6th municipal people’s congress. Available from: https://wsjkw.cq.gov.cn/ztzl_242/rdjyzxta/rdjy/202505/t20250519_14632333_wap.html.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Challenges in Palliative Care Provision in Ethiopia: An Exploratory Qualitative Study
Negasa EH, Human SP, Roro AG
Journal of Pain Research 2023, 16:3405-3415
Published Date: 5 October 2023
Understanding the Support Needs and Challenges Faced by Family Caregivers in the Care of Their Older Adults at Home. A Qualitative Study
Hailu GN, Abdelkader M, Meles HA, Teklu T
Clinical Interventions in Aging 2024, 19:481-490
Published Date: 14 March 2024
Hospital Accreditation Governance in Afghanistan: Challenges and Solutions
Massror AQ, Mosadeghrad AM, Dargahi H, Jaafaripooyan E, Azarakhsh AH
Journal of Healthcare Leadership 2026, 18:561964
Published Date: 17 March 2026