Back to Journals » Journal of Pain Research » Volume 16
Challenges in Palliative Care Provision in Ethiopia: An Exploratory Qualitative Study
Authors Negasa EH, Human SP, Roro AG ![]()
Received 30 April 2023
Accepted for publication 25 September 2023
Published 5 October 2023 Volume 2023:16 Pages 3405—3415
DOI https://doi.org/10.2147/JPR.S415866
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amitabh Gulati
Endalew Hailu Negasa,1 Sarie Petronella Human,2 Ameyu Godesso Roro3
1Department of Nursing, Institute of Health, Jimma University, Jimma, Oromiya, Ethiopia; 2Department of Health Studies, College of Human Science, University of South Africa (UNISA), Pretoria, South Africa; 3Department of Sociology, College of Social Sciences and Humanities, Jimma University, Jimma, Oromiya, Ethiopia
Correspondence: Endalew Hailu Negasa, Email [email protected]
Background: The prevalence of chronic illnesses is increasing at an alarming rate in Ethiopia. However, the existing palliative care service is not adequate to address the palliative care need of the patients and their families. This demands the need to explore, among other things, the challenges in palliative care provision. Thus, this article aimed to examine the challenges of palliative care provision in Ethiopia.
Methods: The study considered Ethiopia as a case and examined the topic using a qualitative exploratory design. The data used in the study were collected through 29 in-depth interviews and 5 focus group discussions with health professionals and other stakeholders and analyzed using thematic analysis technique with ATLAS-ti 7.0 computer software.
Results: This study explored patient-related, provider-related, health system-related and partnership-related challenges/gaps in palliative care in Ethiopia. Patient-related factors include, delay in seeking medical care, lack of awareness of disease conditions, discontinuation of treatment due to inability to pay, a lack of follow-up care by considering cancer diagnosis as end of life/death and preferring dying at home. Provider-related challenges include lack of awareness of palliative care, lack of pre-service/in-service training for health professionals, absence of palliative care in the curricula of health programs and scarcity of research information on palliative care in Ethiopia. Health-system challenges include lack of drug, reagent shortage, limited chemotherapy and radiotherapy services, and weak facility-community linkage. Finally, lack of collaborators between governmental and non-governmental organizations was seen as a challenge to the provision of palliative care in Ethiopia.
Conclusion: The study revealed that the challenges to palliative care provision in Ethiopia include patient-related factors, provider-related factors, health facility-related factors and partnership-related factors. Therefore, it is vital to take these challenges into account in order to improve the current palliative care service provision in Ethiopia.
Keywords: challenges, exploration, palliative care, Ethiopia
Introduction
Palliative care is an approach to improve the quality of life of patients with life-threatening illnesses through pain prevention, assessment and treatment of physical, psychological, and spiritual needs of the patients and their families.1 As the world’s population ages and the prevalence of cancer and other non-communicable diseases, including life-threatening diseases, continues to rise in low- and middle-income countries, the global, regional, and national needs for palliative care are increasing. As such, palliative care is considered as a basic human right.2,3
Palliative care should begin with early diagnosis of a life-threatening illness and continue through the course of treatment. It is offered in combination with other therapies.4 It is an integral part of a comprehensive healthcare system. Research shows that integrating disease-oriented care, such as palliative care, is important to optimizing patient care. However, access to pain relief and palliative care is low or non-existent for most patients in low- and middle-income countries.3 In other words, in many developing countries, palliative care is either lacking, or it is not properly integrated into the existing healthcare systems. Therefore, countries with resource limited prioritize infectious diseases prevention of rather than to palliative care. This problem can, of course, be associated with certain challenges that hinder the creation and delivery of effective palliative care.
However, palliative care provision presents with many challenges. For example, research shows that financial estimates are required to drive the expansion and sustainability of palliative care services.5 According to this study, costs of care include direct costs that measure the resources spent in treating diseases, such as expenses for staff time, radiotherapy, chemotherapy, and the cost of advanced imaging. Indirect costs, on the other hand, typically include costs that usually measure lost productivity (patients or family members take time off work or school). This study found that access to available palliative care services, in low-income settings, comes at a high cost that low-income households cannot afford. The same study argues that palliative care should be a strategy to reduce the direct, indirect and societal costs that terminal illness can cause, such as fragile health care system, a lack of insurance schemes and social support programs.
Studies conducted in Malawi, Kenya, Rwanda, Uganda and Zambia found that families prioritized the urgent need for curing their ill family members over saving money for future household expenses. It turns out that as clinical staffs are reluctant to deal with bad news, the progression of the incurable diseases leaves families more vulnerable to both direct and indirect costs.5 Furthermore, weak health care systems, and lack of the safety nets from insurance schemes and social support programs are the top challenges identified in the study findings. To overcome cost-related issues, study findings have shown that integrating palliative care with curative services is the most cost-effective pathway to quality healthcare.6 Palliative care models should therefore be integrated into all healthcare systems in the provision of primary, secondary and tertiary palliative care to reduce both direct and indirect costs.7
The literature highlights that carefully designed palliative care programs reduce both direct and indirect costs. Palliative care is also more cost-effective when provided in conjunction with curative services. A context-specific palliative care model is important for this. However, challenges such as cost-related and other types that impede the provision of available palliative care services should be identified and appropriately addressed in the development of palliative care models. As shown in a previous article, there is a threshold-level palliative care in Ethiopia (eg Hospice Ethiopia). Therefore, the challenges of the country are this early-stage palliative care need to be considered. As a result, this study seeks to explore the challenges hindering palliative care provision in Ethiopia.
Methods
Study Setting
The setting of this study is one city administration and one zonal administration in Ethiopia. Ethiopia is located in the Horn of Africa, sharing borders with Eritrea, Kenya, Djibouti, Somalia, Sudan and South Sudan as shown in Figure 1. When this study was conducted, the country had Nine Regional States (Afar, Amhara, Benishangul-Gumuz, Gambella, Harar, Oromia, Somali, Southern Nations Nationalities and Peoples and Tigray). There were also two city administrations: Addis Ababa and Dire Dawa.
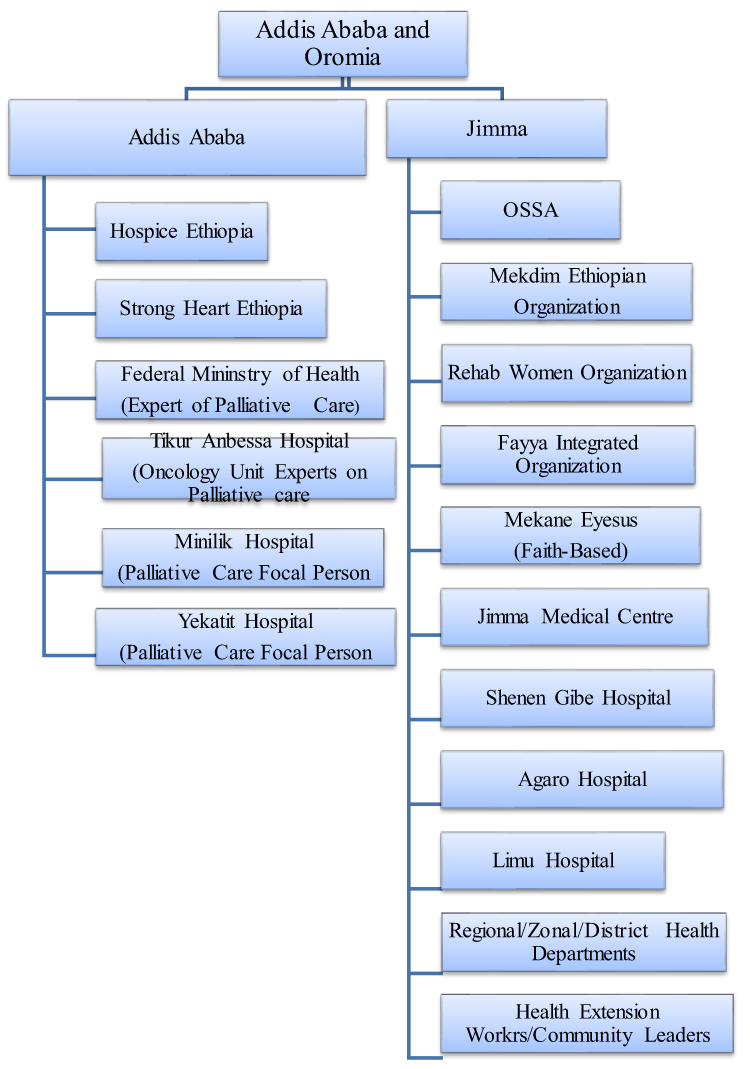 |
Figure 1 Sampling for in-depth interview. |
The study was conducted in Addis Ababa (the capital city of Ethiopia and Oromia) and Jimma Zone from the Oromia Region. Addis Ababa was selected as it has some palliative care providing institutions including the Ministry of Health and different NGOs. In the city are several palliative care-related policy makers and experts affiliated with several public hospitals. Based at Tikur Anbessa Hospital, the only cancer (Oncology) center is Addis Ababa that offers specialized services such as radiotherapy. Hospice Ethiopia and Strong Hearts Ethiopia are also located based in Addis Ababa city.
Oromia Region was selected since it is the largest region in Ethiopia and nearly a third of the country’s population lives in this region. Jimma zone is one of the zones in Oromia. The study focused on four public hospitals from Jimma Zone (Jimma University Medical Centre, Shenen Gibe Hospital, Limu Genet Hospital and Agaro Hospital) which were chosen as specific sites for study. Of these, Jimma University Medical Center and Shenen Gibe Hospitals are found in Jimma town, whereas Limu Genet and Agaro hospitals are located in Jimma District. Care-providing and faith-based organizations that support patients with chronic illnesses were part of the study.
Research Design
Qualitative research is used to study how people see their world and how they interact with each other to construct their social reality.8,9 It also helps answer questions focused on exploring processes and unpacking the meanings that people associate activities, and situations.8 Qualitative research is deemed appropriate for palliative care medicine because it has been employed to researching the same in the African context.10 The study employed a qualitative, exploratory based on data collected through in-depth interviews and focus group discussions to examine the challenges facing palliative care provision in Ethiopia.
Therefore, in this study based on data from policymakers, program managers, health workers, community representatives and organizations engaged in delivering palliative care in Ethiopia (Addis Ababa and Jimma Zone). Data were also collected using focus group discussions conducted with nurses who were working in chronic illness wards of four hospitals. Qualitative approach was thus employed to elaborate the participants’ experiences regarding the challenges associated with palliative care provision in the health facilities with which they are affiliated.
Study Participants and Data Collection Methods
Data were collected through key informant interviews (KII) and focus group discussions (FGDs) to explore the challenges that hinder palliative care delivery in Ethiopia. Study participants were from the Ethiopian Federal Ministry of Health, non-governmental organizations, faith-based organizations, hospitals, zonal health departments and health extension workers units. Purposively selected nurses working in chronic illness clinics in the four hospitals in Jimma Zone were participated in the focus group discussions. Interviews involved stakeholders currently providing palliative care to chronically ill patients and health professionals with at least six months of experience providing palliative care services in chronic care clinics.
Sampling
Purposive sampling is often used in qualitative studies.10 Here, data saturation is the primary determinant of sample size, ie, sampling should be ceased if no new information is emerged from the new unit.11 The purpose of the study, its specific objectives and the characteristics of the study population (such as size and diversity) also determine which and how many people to sample.12 In this study, the participants were purposively selected as shown by Figure 1 as they were believed to have rich knowledge and first hand experiences of the palliative care challenges in Ethiopia. Besides, the participants had at least 6 months of work experience in chronic illness clinics.
Thus, 29 interviews were conducted with informants taken from Addis Ababa and Jimma Zone. This includes policy makers, hospice managers and program coordinators ranging from the federal level to the districts (health workers and community representatives). Religious figures were also interviewed due to their rich knowledge of the challenges of palliative care provision in Ethiopia. In addition, the interview involved heads or representatives of five non-governmental organizations and four faith-based organizations that support palliative care in Jimma Zone. A detailed sampling plan for the in-depth interview is shown in Figure 1 and Table 1.
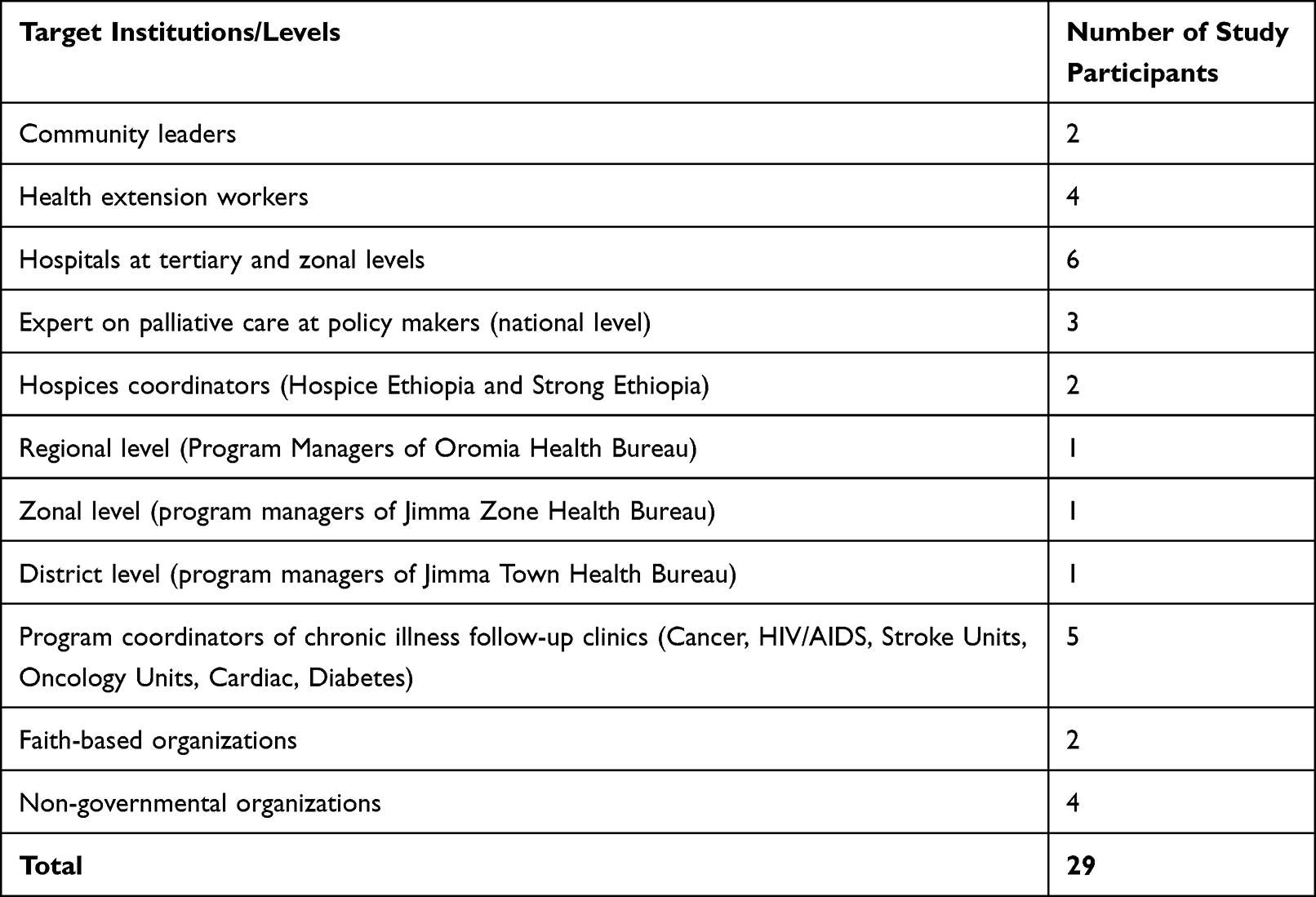 |
Table 1 Detailed Sampling Scheme for Key Informant Interviews |
Secondly, 30 nurses working in chronic illness wards off our hospitals in Jimma Zone participated in FGDs. As noted above, these participants were selected purposively based on their understanding of the challenges faced in providing palliative care to patients with life-threatening illnesses. A total of five FGDs were conducted with nurses working in five chronic illness clinics of Jimma University Medical Center (JUMC), Agaro hospital, Limu hospital, Shenen Gibe Hospital as well as in Oncology Unit of JUMC. Each group consisted of six nurses.
Inclusion Criteria
The study participants were purposively included stakeholders and health professionals who fulfilled the following inclusion criteria: Stakeholders who were involved in palliative care provision/support to patients with chronic illness in the country for 2 years or more. Besides, health professionals who had at least six months work experience on rendering palliative care services to their patients in chronic clinic were eligible to participate.
Exclusion Criteria
The stakeholders or health care professionals who were on maternity leave were excluded from the study.
Data Collection Procedures
Data for the study were collected through KII and FGD conducted by the researcher and a trained research assistant. An interview guide was developed in English based on the literature and was later translated into and implemented in Amharic. Amharic is a commonly used language in Ethiopia. The in-depth interview guide was then thoroughly evaluated by experts, who had a great deal of experiences in qualitative research. The guide has also been pretested in Jimma University Medical Center with the Surgical and Medical Department heads to check its appropriateness. Following this, minor corrections were made in its wording and construction. The pilot interview was audio-recorded and took 35 to 60 minutes, which was also the case for the main study.
Similarly, the researcher and the assistant data collector used a pretested FGD guide, supplemented with clear oral explanations and directions, to carry out the focus FGDs. The principles of objectivity, impartiality, reflective thinking, a critical appraisal of the data collector’s role and influence on the discussion process were adhered to in conducting the FGD. Focus group discussions were taped and notes were taken to supplement their coded data.
Data Management and Analysis
In this study, the data were analyzed thematically. Audio-transcripts were read multiple times and assigned codes. A code structure was also created. Unit of meanings derived from the data were assigned to specific codes. This was followed by axial and selective coding to develop higher codes (categories and sub-themes). First, we converted the transcribed data to a text file. After that, they were imported into ATLAS-ti software for coding and other subsequent products to facilitate data management and interpretation of the findings. Data were managed by breaking the narrative information into smaller, more manageable units. Finally, a deductive coding approach was applied and pre-existing coding framework was used. The pre-existing coding frame-work takes challenges of palliative care provision at its center and has a link with patient-related challenges, health-professionals related challenges, policy-related challenges and partnership-related challenges. Under each sub-links to the palliative care provision challenges, there are various challenges. Categories and subcategories were developed into themes for each participant and across different participants. Finally, the meaning of the theme was interpreted. And issues of trustworthiness, ie, credibility, dependability, transferability and conformability, were also carefully addressed.13
Ethical Considerations
A study, regardless of the approach, must follow ethical principles.14 The following ethical issues were addressed in this study: First ethical clearance was obtained from the Research and Ethics Committee of the Department of Health Studies of the University of South Africa (UNISA). Then, letters support was obtained from Addis Ababa City Administration and Oromia Region Health Bureaus, giving permission to conduct the study. Additionally, the following ethical principles were adhered. Therefore, participation in the study was voluntary and informed consent was obtained. Also, the participants were consented on the publication of their anonymized response. Codes were also used to anonymize the study participants. Care was also taken to protect the participants from harm through the principles of beneficence, non-maleficence and justice.
Results
In exploring the challenges of providing palliative care services in Ethiopia, the study identified these challenges related to patients, health care providers, research, health systems and partnerships. In general, there were 1072 primary codes, 32 categories and 7 main themes emerged from the analysis of 5 focus group discussions and 29 Key informants. Here below are the detailed results:
Patient-Related Challenges
Study participants described patient-related challenge as a common barrier to the delivery of palliative care services. These include delayed visit to a health care facility, lack of awareness of medical conditions, poverty, treatment discontinuation of treatment, drop of clinical follow-up because cancer diagnosis is considered as death /end of life and loss of hope.
Regarding this, FGD participants noted that most of the patients made a visit to the health facilities after the disease had already advanced and after they had visited private health institutions and traditional healers. In this discussion, it was noted as in the excerpt below:
There is often little awareness in our community of the importance of follow-up to the care for life long illness. So, a patient shows up after the problem becomes complicated. One example, terminal cancer. This is due to a lack of awareness in the community and sometimes reliance on traditional healers. And, they visiting different types of health institutions and treated for other opportunistic diseases. [FGD2, 26 years clinical nurse]
In addition, KII participants shared similar views on how delays in patient visits to health care facilities affect palliative care.
Most of the time, they are late. When you take a cancer patient, they come here after the disease has progressed. They stay at home when the disease t has no-specific manifestation, and t take analgesics but, come here when the diseases advance. They come here with referral or without referral paper. [40 years internist from a hospital]
In fact, the problem is rooted in other factors. For example, a clinical nurse said the lack of patients’ awareness, considering cancer as a deadly disease and losing hope were some of the challenges. This is highlighted in the following excerpt:
Patients lack quality of life due to a variety of factors. Viewing cancer as deadly disease, loss of hope and lack of interest to stay at hospital and even prefer to die at home. Psychosocial distress and financial crisis are the main problems for most of our patients. [A 28-year old, FGD 1]
Other participants emphasised why patients discontinued their medication and no longer available for follow-up:
… Sometimes, they [patients] started taking medications, but then stopped them. They [patients]) say that “holy water” “praying”, “du’a” heal us and then stop their medication. Of course, we often teach them [patients] not to stop taking medication and to use both together. [24 –year-old, health officer, FGD4]
In general, there are patient-related barriers to providing palliative care, as the above results demonstrated. This includes, being late to a health facility to receive palliative care services. After trying various options such as herbal remedies and spiritual healers, patients may visit a health facility. They sometimes discontinued follow-up losing hope. In addition, lack of awareness of the medical conditions, poverty and treatment dropout was identified as other challenges associated with patients.
Provider-Related Challenges
Health care providers play an important role in providing palliative care to patients with life-threatening illnesses. Therefore, this study examined provider -related factors that may hinder the delivery of palliative care in the study settings. In this regard, the study found the following issues: lack of palliative care awareness among health professionals, lack of in-service and pre-service palliative care training and lack of palliative care in the various health disciples training curricula. For instance, one key informant said that:
The main thing that is seen as an obstacle is the very low level health provider’s professionalism. If the knowledge and attitude of the healthcare professionals is good, I the healthcare managers can create a system that would improve the palliative care. Awareness creating training should be given for the management personnel and healthcare providers, so that palliative care can be provided appropriately. [KII9, a 41- year-old, oncologist working in a tertiary hospital]
The following quote also strengthens the above truth:
I think most of our staff are not trained and do not have enough knowledge about this [palliative care]. So, the main thing is that this is not included in pre-service training. There are also few in-service trainings. Palliative care knowledge, attitude and practice are generally low. [KII 940, a hospital manager]
As detailed below, the manner in which healthcare providers provide care services is another provider related-challenge.
Another issue is the cost and the willingness of the professionals to give these analgesics is also another problem. When we take pethidine, most of the professionals are not willing to give because the patients may develop addiction. They believe that they don’t deserve these analgesics. [KII 940, hospital manager]
Health professionals are only focused on prescribing medications. Even palliative care is not only for patients, but also for families or caregivers, but we are more focused on medications and even where palliative care is provided. It is more focused on patients. I have not seen any palliative care guidelines here in our facility, we did not also have palliative care standards, but I have pain management guideline in soft copy. [FGD, 27 year-old]
Overall, the above findings are consistent with a lack of knowledge about palliative care among health professionals, unwillingness to provide the adequate care services, and lack of palliative care guidelines in health facilities were the provider-related challenges to the delivery of palliative care services. These challenges are also related to the lack of palliative care content in the curricula of most health education curricula. Therefore, this is thus one of the factors which are hindering palliative care delivery in Ethiopia.
Research-Related Challenges
Participants reported that research studies focused on communicable diseases are very limited in Ethiopia. This is shown in the following quote:
In our country, research on palliative care is very limited. You can count them and say one, two. There was a study conducted by a person named, Dr. Nicolas; in 2012 at AAU and published. It was on morphine dosage and how it was started in Ethiopia Apart from this, I think, research on this issue is limited. So, if universities study such topics, and train palliative care professionals, it will help our country. [KII 11, 36 year-old internist in one of Jimma Zone Hospital]
The following response also supports the above one:
I do not recall any research being conducted on this topic [palliative care] when I was doing my research. When I say policy in addition to training, it must be one thematic area for researchers. But, it is not the thematic area of must researchers; even if it is thematic area, most researchers are not interested in doing research on this area. They are doing their research areas related diseases like hypertension, DM and others. [KII11, a36 year-old internist in one of Jimma Zone Hospitals]
Research-oriented knowledge is essential effective palliative care delivery. However, the participants in this study reported that there was limited research on the topic in Ethiopia. Experience also shows there is still too little research on palliative care in the country. This problem obviously hinders the delivery of effective palliative care services to patients with life-threatening patients.
Health System-Related Challenges
This study further explored the healthcare systems’ - challenges to the delivery of palliative care. As such, challenges such as shortage of human resources, drugs, reagents, chemotherapy, and radiotherapy were limited. For example, one FGD participant said that:
Two physicians and some nurses have attended the training on palliative, but I have already mentioned that, there is high turnover of staff turnover and there are no trained nurses here. We have shortage of professionals, despite the high number of unemployed health professionals in the country. If the government would m and assign send them, they could play a key in reaching out to out-of-hospital patients. For this reason, strengthening health extension services are needed. Because it is the only effective one in town. The other problem is the supply of essential drugs like morphine. Even when it is available, its supply is intermittent. Another issue here is the cost and the willingness of the professionals to these drugs. [FGD3, 35 year-old nurse]
Another participant also described the problem as follows:
Additionally, there are financial challenges to providing service. Drugs are expensive. Some patients cannot afford them. So they must pass through process which helps them to take the treatment until that patients are suffering due to pain. We are doing one analysis of pain treatments in cancer patients that include morphine, and there are sometimes shortage of morphine. [FGD3, 30 year-old nurses from Chronic Clinic]
The following assertions are also associated with scarcity and high cost of chemotherapy drugs:
The main problem is interruption of the supply of chemotherapy drugs and opioids, especially morphine. The main issue with the supply with the supply chain, there are gaps in the PFSA as well, because there were times when chemotherapy drugs are available in central PFSA, but not in our setting. Moreover, there is financial issue while providing the service; drugs are expensive, there are patients who cannot afford it and have to go through a process that helps them get treatment, until then they are in pain. [KII 19, physician at Oncology Unit]
As shown above, some healthcare system-related challenges are affecting the provision of palliative care delivery in Ethiopia. These include shortage of human resources and scarcity of drugs and absence of facility-community linkage. This problem, along with other challenges, worsens the hindrances to palliative care provision in Ethiopia.
Partnership-Related Challenges
One key informant from the Federal Ministry of Health (FMOH) explained that there are no non-governmental organizations dealing with palliative care. According to this participant, more attention is being paid to communicable diseases, especially treatment and prevention.
There are very few organizations in our country that deal with non-communicable diseases, but dealing communicable diseases. They are taking about prevention and communicable diseases, so it has become difficult for us to talk about centers for disease control and prevention (CDC). So none is working with Ministry of Health. [KII2, 36 year-old, FMOH]
This study also showed weak linkage between health facilities and -community. An instance is shown in the following transcript:
For example, we did not provide end-of-life care because there are challenges in the community that make it difficult to provide; We are only providing services not the level of outreach. [FGD 5, 32 year-old nurse from chronic clinic]
This study identified various local non-governmental and faith-based organizations in Jimma Zone and explored the extent to which they provide palliative care services. Based on this, the people working the following local non-governmental organizations were interviewed: Mekdem Ethiopia, Organization for Social Service Health and Development, Fayya Integrated Development Organization, and Ethiopian Evangelical Church Mekane Yesus Social Service/Jimma Branch (FOBs).
The interviews revealed that the majority of the organizations provide palliative care to HIV/AIDS patients. Most of the local NGOs and FBOs coordinators emphasized in the interviews that they are far fewer donors supporting patients than in the previous times. Also, there was mismatch between demand and supply. The number of patients requiring support is very high. All the study participants indicated that their projects relied largely on external sources to sustain their services. This dependence obviously limits the operation and hinders the sustainability of palliative care capacity. All the interviewed participants mentioned the existence of this challenge.
In conclusion, the study found that limited partnership with national and international stakeholders is one of the challenges for providing palliative care in Ethiopia. Additionally, a lack reliable local resources, exclusive dependence on external donors have been found to exacerbate the problems associated with providing palliative care. The weak links between health facilities have also exacerbated the challenges of palliative care provision.
Discussion
The study findings of the study have demonstrated that the challenges faced by health faculties for providing effective palliative care. The two main challenges facing health professionals are the lack of clear policy and appropriate strategic implementation plans and guidelines. On policy level, the existing health policy of the government focuses on communicable diseases, while neglects the non-communicable diseases. As a result, a dearth of fund has always been a stumbling block for effective and efficient palliative care. This study findings are consistent with a study describing the palliative care pathways in Kenya and Uganda. Policy limitations and regulatory failure, lack of funding and trained professionals, and lack of integrating palliative care in public and private health care systems major gaps and challenges related to palliative care provisions.15
The study also demonstrated that there was a scant research publication on palliative care in Ethiopia, which is consistent, the findings of previous studies.16 In fact, the Federal Ministry of Health (FMOH) has been provided with an advisory on palliative care. However, a lack of research focus on palliative care also poses challenges to strengthening palliative care system in the Ethiopian context. Similar observations were reported by Rhee et al.16
One of the challenges that affecting palliative care delivery in Ethiopia is the lack of adequate financial support. Most palliative care services are provided by non-governmental, faith-oriented, or community-based organizations with no self-reliable and sustainable funding system. This study showed that there was no specific funding allocated or palliative care by the FMOH, and this affects establishment of palliative care model and its delivery. Furthermore, there is no strong and organized support for palliative care activities from international non-governmental organizations or foreign governments that could found it in Ethiopia. This agrees with the findings of a study by Lucas,17 who found that palliative care in Africa has faced financial challenges as it relies on funding from external donors.
Another challenge faced in providing palliative care in Ethiopia is related to the patients. These include lack of awareness about their disease conditions, delayed access to health facilities, misconceptions about cancer, loss of hope, discontinuity in follow-up care, resorting to other treatment options such as traditional healing, and poverty. These findings are in agreement with those of previous studies.18,19 These challenges obviously contributed to the difficulties faced by palliative care endeavors in Ethiopia.
Provider-related factors are other challenges to the provision palliative care in Ethiopia. Health professionals play a key role in improving palliative care service for patients with life-threatening illnesses. To this end, factors pertaining to provides which affect palliative care provision must be significantly minimized. However, this study identified provider-related challenges and how they have impeded the proper delivery of palliative care to patients with life-threatening illnesses. The challenges include lack of palliative care knowledge and practice, particularly at zonal and regional levels, lack of a multi-disciplinary team approach, greater emphasis on disease treatment with medications only, and high turnover of trained health professionals. The findings corroborate findings of a study conducted by Ddungu,15 that recommend that the governments should provide a holistic care based on patients’ need and raise awareness among patients and their families.
A final challenge influencing palliative care delivery identified in this study relates to healthcare system challenges. Inadequate man power, lack of funding allocated to providing palliative care, failure to include palliative in the hospital strategic plan, scarcity of cancer and radiotherapy centers are some of these setbacks. Drugs, reagents, chemotherapy and radiotherapy were in short supply. And links between health facilities and community were weak. This finding is supported by a systematic review done by Hammoda, Alex and Justina,20 which showed that knowledge deficits of healthcare providers about palliative care, inadequate number of trained work force, limited physical infrastructure and insufficient drugs for symptoms relief were challenges seen in the provision of palliative care to cancer patients in low- and middle-income countries.
Strengths and Limitations
The strengths of this study include that the sample size of the study was adequate. Both FGD and in-depth interview were used as data collection methods complementing the weakness of each other. Thus, the finding of this study can be used by the concerned bodies to improve the existing palliative care provision in Ethiopia. But the study has not included the existing opportunity for palliative care provision.
Conclusion
The provision of palliative care in Ethiopia is still in its early stages. These challenges can also have complex relationships that complicate the burden of available palliative care. Appropriate palliative care strategies that address these issues are therefore of great importance for advancing palliative care provision in Ethiopia.
Data Sharing Statement
Data supporting this research will be available upon request from the corresponding author.
Acknowledgment
We would also like to extend my thanks to the University of South Africa, Oromia Regional Health Bureau and Jimma University for arranging me this opportunity to carry out this thesis and offering me the Ethical clearances to carry out this study. Our thanks also goes to Jimma University for funding this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Jimma University funded this research solely for the data collection purpose. Otherwise, the funder has no contribution in this research work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Gwyther L, Chb MB, Brennan F, Obs D, Harding R. Advancing palliative care as a human right. J Pain Symptom Manage. 2009;38(5):767–774. doi:10.1016/j.jpainsymman.2009.03.003
2. Brennan F. Palliative care as an international human right. J Pain Symptom Manage. 2007;33(5):494–499. doi:10.1016/j.jpainsymman.2007.02.022
3. Knaul FM, Farmer PE, Krakauer EL, et al. Alleviating the access abyss in palliative care and pain relief—an imperative of universal health coverage: the Lancet Commission report. Lancet. 2018;391(10128):1391–1454. doi:10.1016/S0140-6736(17)32513-8
4. Brereton L, Clark J, Ingleton C, et al. What do we know about different models of providing palliative care? Findings from a systematic review of reviews. Palliat Med. 2017;31(9):781–797. doi:10.1177/0269216317701890
5. Anderson RE, Grant L. What is the value of palliative care provision in low-resource settings? BMJ Global Health. 2017;2(1):2016–2018. doi:10.1136/bmjgh-2016-000139
6. Currow DC, Clark J. Notes from the editor why smart emerging economies will invest in excellent palliative care, if palliative care services do their part. J Palliat Med. 2018;21(3):276–277. doi:10.1089/jpm.2018.0007
7. Reid EA, Kovalerchik O, Jubanyik K, Brown S, Hersey D, Grant L. et alIs palliative care cost-effective in low-income and middle-income countries? A mixed-methods systematic review BMJ Support Palliat Care. 2019;9(2):120–129. doi:10.1136/bmjspcare-2018-001499
8. Devi BCR, Tang TS, Corbex M. A model of palliative care programme integrating rural with hospital care: Sarawak, Malaysia. Prog Palliat Care. 2010;18(1):31–36. doi:10.1179/096992610X12624290276269
9. Ntizimira CR, Nkurikiyimfura JL, Mukeshimana O, Ngizwenayo S, Mukasahaha D, Clancy C. Palliative care in Africa: a global challenge. Ecancermedicalscience. 2014;8:1–4.
10. Downing J, Boucher S, Daniels A, Nkosi B. Paediatric palliative care in resource-poor countries. Children. 2018;5(2):27. doi:10.3390/children5020027
11. Polit DF, Beck CT. Essentials of Nursing Research: Appraising Evidence for Nursing Practice.
12. Shenton AK. Strategies for ensuring trustworthiness in qualitative research projects. Educ Inform. 2004;22:63–75.
13. Hancock B. An introduction to qualitative research authors. Qual Res. 2006;4:504.
14. Creswell WC. Research Design: Qualitative, Quantitative and Mixed Methods Designs.
15. Ddungu H. Palliative care: what approaches are suitable in developing countries ? Br J Haematol. 2011;154(6):728–735. doi:10.1111/j.1365-2141.2011.08764.x
16. Rhee JY, Luyirika E, Namisango E, et al. APCA atlas of palliative care in Africa; 2017.
17. Lucas S. Palliative care: issues and challenges. World Health Organization; 2002.
18. Kassa H, Murugan R, Zewdu F, Hailu M, Woldeyohannes D. Assessment of knowledge, attitude and practice and associated factors towards palliative care among nurses working in selected hospitals. BMC Palliat Care. 2014;13(1):1–11. doi:10.1186/1472-684X-13-6
19. Haileselassie W, Mulugeta T, Tigeneh W, Kaba M, Labisso WL. The situation of cancer treatment in Ethiopia. Challenges Opportunities. 2019;24(1):33–42.
20. Maltoni M, Jiang Y, Dinkel A, Abu-Odah H. Hammoda Abu-Odah1, 2, Alex Molassiotis1, 3 and Justina Yat Wa Liu1; 2023.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Challenges of Access to Oral Morphine Medicine: Palliative Care at a Crossroads for Cancer Patients in Ethiopia
Fentie AM, Belete A, Selam MN
Journal of Pain Research 2023, 16:1829-1833
Published Date: 31 May 2023
Palliative Care Practice and Associated Factors Among Nurses Working in Chronic Care Units of Tertiary Hospitals in Ethiopia: A Cross-Sectional Study
Gembe M, Tariku T, Tesfaye T, Hailu EH
Nursing: Research and Reviews 2024, 14:45-58
Published Date: 8 February 2024
Unpacking Multi-Layered Challenges in Palliative Care Transitions: A Descriptive Qualitative Study of Multidisciplinary Teams in China
Tang J, Li J, Wang X, Xiao M, Zhang Y, Tao H, Jiang Y, Yan Y, Zhao Q
Journal of Multidisciplinary Healthcare 2026, 19:605455
Published Date: 26 May 2026