")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Uncovering Methods and Outcomes of Palliative Care for Geriatric Patients: A Scoping Review
Authors Haroen H, Harun H, Sari CWM , Witdiawati W
Received 6 July 2023
Accepted for publication 15 September 2023
Published 27 September 2023 Volume 2023:16 Pages 2905—2920
DOI https://doi.org/10.2147/JMDH.S429323
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Hartiah Haroen,1 Hasniatisari Harun,2 Citra Windani Mambang Sari,1 Witdiawati Witdiawati1
1Department of Community Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, Indonesia; 2Department of Medical-Surgical Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, Indonesia
Correspondence: Hartiah Haroen, Department of Community Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Jl Ir. Soekarno KM. 21, Jatinangor, Sumedang, West Java, 45363, Indonesia, Tel +62812-9454-3843, Fax +62 022 7795596, Email [email protected]
Background: Palliative care is an integral part of care for patients with life-limited diseases that focuses on reducing symptoms and maintaining and increasing the quality of life (QoL) for patients and their families. Geriatric patients were more likely to receive palliative care and had unique needs compared to the general population. To improve the quality of palliative care, especially for geriatric patients, it is necessary to have a better understanding of methods and outcomes for geriatric patients when delivering palliative care.
Objective: This study aims to identify the methods and outcomes of palliative care in geriatric patients across the globe.
Methods: This scoping review was guided by Arksey and ‘O Malley’s framework and utilized the Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) checklist for providing transparent reporting to the readers. EBSCO, PubMed, and Scopus databases were used to search the relevant articles with a publication range of 2013– 2023. Thematic analysis was used to identify and summarize palliative care methods and outcomes for geriatric patients in this review.
Results: Twenty-one studies were included in this review, and it was found that there were many types of methods for delivering palliative care to geriatric patients. In both acute care settings and community settings, a wide range of methods for delivering palliative care to geriatric patients were identified. Outcomes of palliative care in geriatric patients in hospitals and community settings, were reduced pain, depressive symptoms and anxiety, edema, constipation, odds of in-hospital death, and increased spiritual well-being, QoL and well-being, being comfortable, patient readiness, place of death, sleep quality, and quality of dying.
Conclusion: Geriatric patients had a variety of methods and outcomes in palliative care. This study suggests that outcomes should be evaluated continuously after implementing methods for delivering palliative care to geriatric patients.
Keywords: aged, methods, outcomes, palliative care
Introduction
According to the World Health Organization (WHO), an estimated 56.8 million people need palliative care annually, including 25.7 million people who are in their last year of life (WHO, 2020). Palliative care refers to a specialized type of medical care that focuses on providing support and improving the quality of life (QoL) for individuals facing life-threatening illnesses.1–3 Palliative care is not limited to end-of-life care (EoLC) or comfort care but extends to all stages of the disease.2 Palliative care begins when a serious illness starts and is provided alongside treatments designed to address the life-limited disease. Meanwhile, end-of-life care (EoLC) or hospice care is a specialized form of palliative care for individuals in their final months of life. It is argued that palliative care should be introduced or integrated as early as possible in the patient’s care when the conventional treatments are not unable to control the disease or symptoms effectively. EoLC involves managing the devastating symptoms, such as pain and any other physical symptoms, and providing physical, psychosocial, and spiritual support to patients.2,4
Palliative care is a crucial public health concern across the globe due to the increase of ageing population including insufficient attention to their multifaceted needs. Currently, the percentage of the population aged 60 and above is set to rise from 1 billion in 2020 to 1.4 billion in 2030.5 By 2050, the population aged 60 and older will reach 2.1 billion.5 Thus, the need for palliative care is growing, especially among older ages who experience chronic illnesses and vulnerability.6
Palliative care has been less accessible to many older adults compared to younger population. Older adults have distinct requirements due to their unique and often more intricate issues than younger people.7 Older people frequently contend with various medical conditions of differing levels of severity.7,8 The collective impact of these conditions can surpass that of individual diseases, resulting in greater impairment and urgent care needs.7 Older ages face a higher risk of adverse drug reactions and iatrogenic illnesses than younger people.7 Minor concerns can disproportionately affect older people’s psychological well-being over time. Acute health issues may overlay physical or mental impairments, financial challenges, and social isolation.7 Therefore, an effective model of palliative care that can effectively meet the needs of older people or geriatric patients is urgently needed. Establishing comprehensive palliative care programs has become an international challenge.9 Although palliative care is recommended by many healthcare professionals and organizations, especially for geriatric patients, there is still a gap in knowledge of its effectiveness among many clinicians. There has been limited studies that investigates the different strategies or methods of palliative care for geriatric patients (add the new cited sources here).10,11 Methods of palliative care refer to the various approaches, techniques, and interventions employed to provide relief, comfort, and support to geriatric patients with serious illnesses. These strategies encompass a wide range of medical, psychological, and emotional interventions tailored to address individual patient needs.
Studies have identified successful outcomes in delivering palliative care to geriatric patients with complex chronic illnesses in their final stages of life residing in Palliative care in Residential Aged Care Facilities (RACFs).12,13 Despite successful outcomes in some interventions and programs, there is a lack of standardized evaluation methods for implementation. This issue hinders rigorous comparisons between different interventions and programs, as well as effective translation and application to different contexts and populations.
There is a gap in the literature regarding the analysis of the available evidence on the various strategies or methods of palliative care for geriatric patients. More specifically, there is a need for a systematic scoping review that examines the various methods and outcomes of palliative care for geriatric patients. This scoping review aims to address this gap in knowledge and provide a comprehensive understanding of the available literature on the subject.
The primary objective of this scoping review is to provide a comprehensive understanding of the different methods and strategies utilized by healthcare professionals across the globe in providing palliative care to geriatric patients and the outcomes associated with these methods. This review aims to identify and map out gaps in the literature, highlighting areas that require further research. It also aims to identify best practices and effective strategies that can be implemented by healthcare practitioners and policymakers in ensuring the provision of effective palliative care services for geriatric patients. Overall, the findings of this scoping review will contribute to the development of a more comprehensive and evidence-based approach towards the provision of palliative care services for geriatric patients particularly for countries with growing older aged population.
Methods
Study Design
We followed Arksey and O’Malley methodological framework for this scoping review.14 This framework allows for the inclusion of an extensive range of study designs to build a comprehensive outline of the research field. Following the Preferred Reporting Item for Systematic Review and Meta-analysis for Scoping Review (PRISMA-ScR),15 this methodology is suitable for this subject because it allows a thorough evaluation of the palliative care interventions available to geriatric patients. The scoping review method began with a broad research question, which was narrowed during the study process to enable in-depth evaluations of the model of palliative care interventions and outcomes for geriatric patients. The initial study question that guided the literature search was “what are the existing palliative care models for geriatric patients, and what outcomes do they produce?”.
Eligibility Criteria
This inclusion criteria followed the Population, Concept, Context (PCC) framework. The eligibility criteria for this study included people with geriatric palliative care needs, Concept and context that focused on palliative care, and studies that reported outcome measures related to palliative care delivery or efficacy. Moreover, the exclusion criteria included: (1) articles that had been published in non-peer-reviewed journals or proceeding (2) preprints (3) article that were not original research (4) Studies beyond the last 10 years (2013–2023) were examined to ensure the relevance of strategies and current conditions.
Search Strategy and Study Selection
A literature search was conducted throughout CINAHL, PubMed, and Scopus databases. The search strategy also used a combination of Medical Subject Headings (MeSH) and relevant keywords to the palliative care interventions available to geriatric patients. Two independent investigators (put initials mba disini) conducted the search activities from February 2023. The search employed the “related articles” feature and hand-searched the reference lists of the included articles to expand the search and identify additional relevant studies. The search terms and MeSH terms included: “Aged” OR “Elderly” OR “Older Adult” OR “Elder” OR “Geriatric” OR “Elderly People” OR “Old People” OR “Senior”) AND (“Palliative Care” OR “End of Life Care” OR “Hospice Care” OR “Palliative Treatment” OR “Palliative Treatments” OR “Palliative Therapy” OR “Palliative Supportive Care” OR “Palliative Surgery” OR “Terminal Care”. The searching strategy in detail can be seen in Supplementary file. We removed duplicate results using a reference tool (Mendeley 19.8) and manually screened the remaining articles after the initial search.
Data Extraction and Analysis
Three authors were involved in the data extraction process. In case of any discrepancies, consensus was reached by the group. The data extraction process was conducted using the PRISMA-ScR guideline, which included identifying duplicates, screening titles and abstracts, and obtaining full texts of relevant studies. The tabulation method was used to manually extract data from the study results, and the data of interest included the author, study location, study design, setting, intervention care model, and its effectiveness. Afterward, this study performed a qualitative thematic analysis of the data extracted from the included studies. Two key themes generated in this review.
Results
Selection Process
The study selection process identified an initial search of 13,198 articles from three databases. After removing duplicates, a total of 12,432 articles were screened by two reviewers using the inclusion criteria. The remaining 173 articles were sought for retrieval, resulting in 41 studies were assessed for full text review.16–36 Of the 41 studies, 20 were excluded, and the remaining 21 studies were included in analysis. The PRISMA flow diagram provides a visual representation of our study selection process (see Figure 1).
 |
Figure 1 PRISMA flow diagram. Notes: Adapted from Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.37 |
Characteristic of Included Studies
The 21 included studies were identified from Europe (Italy, Belgium, Sweden, Switzerland, France, Netherland, UK, Denmark, Poland, Germany), Asia (Japan and China) and North America (the US). The characteristics of the 21 studies included in analysis can be seen in Table 1.16–36 The study design of the selected studies varied, nine were randomized controlled trials,18,19,21–24,30,32,33 one experimental,31 five pilot studies,16,17,25,27,29 one feasibility study,20 two cohort studies,28,34 one observational study,16 one cross-sectional study,36 and one survey.35 The patients included in the studies were having a range of diseases and conditions, such as metastatic non-small cell lung cancer (NSCLC), advanced cancer, colorectal cancer, unsectable advanced gastric cancer, breast cancer, pancreatic adenocarcinoma, dementia, acute gastric problems, and Chronic Obstructive Pulmonary Disease (COPD). The studies were conducted in both hospital and community settings. The modality of intervention applied in the selected studies covered various aspects, including physical, psychological, spiritual, quality of life (QoL), and quality of care. The diversity in study characteristics might be considered in the analysis to provide comprehensive insight into the effectiveness of interventions across a range of contexts and conditions.
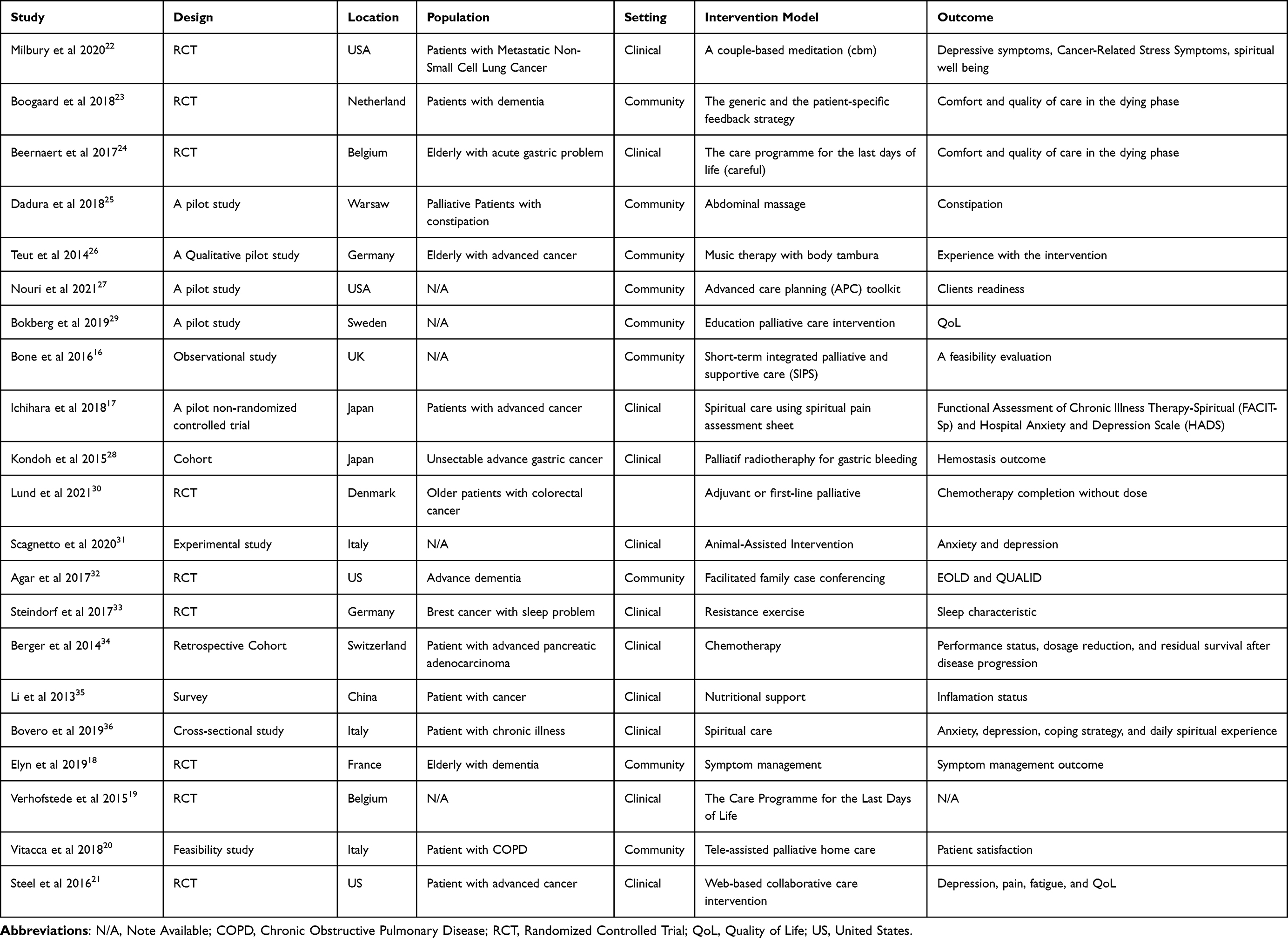 |
Table 1 Characteristics of Included Studies |
Palliative Care Intervention Models
This review concluded with two themes and five ordinate themes. The themes included the model (strategy) of intervention for palliative care for geriatric patients in the hospital and community settings. Ordinate themes included various aspects of physical, psychological, spiritual, QoL, and quality of care regarding EOLC (see Table 2). The strategy of intervention in the hospital setting, including intervention for the physical domain web-based collaborative care intervention, palliative radiotherapy for gastric bleeding, resistance exercise, nutrition support, adjuvant, or first-line palliative, and chemotherapy. The strategy of intervention for the spiritual domain included the use of the spiritual pain assessment sheet, animal-assisted intervention, spiritual care, and CBM. The strategy for improving QoL included the use of the spiritual pain assessment sheet. The strategy of intervention for improving the quality of care was The Care Program for the Last Days of Life (CAREFuL). In the community setting, the strategy of intervention for the physical domain included symptom management, abdominal massage, and music therapy with body tambura. The strategy of intervention for psychological support included facilitated family case conferencing, tele-assisted palliative home care, advanced care planning (APC) toolkit, and short-term integrated palliative and supportive care (SIPS). The strategy for improving quality of life included education palliative care intervention. Finally, the generic and the patient-specific feedback strategy and The Care Program for the Last Days of Life were the modalities of intervention utilized for improving the quality of care regarding EOLC.
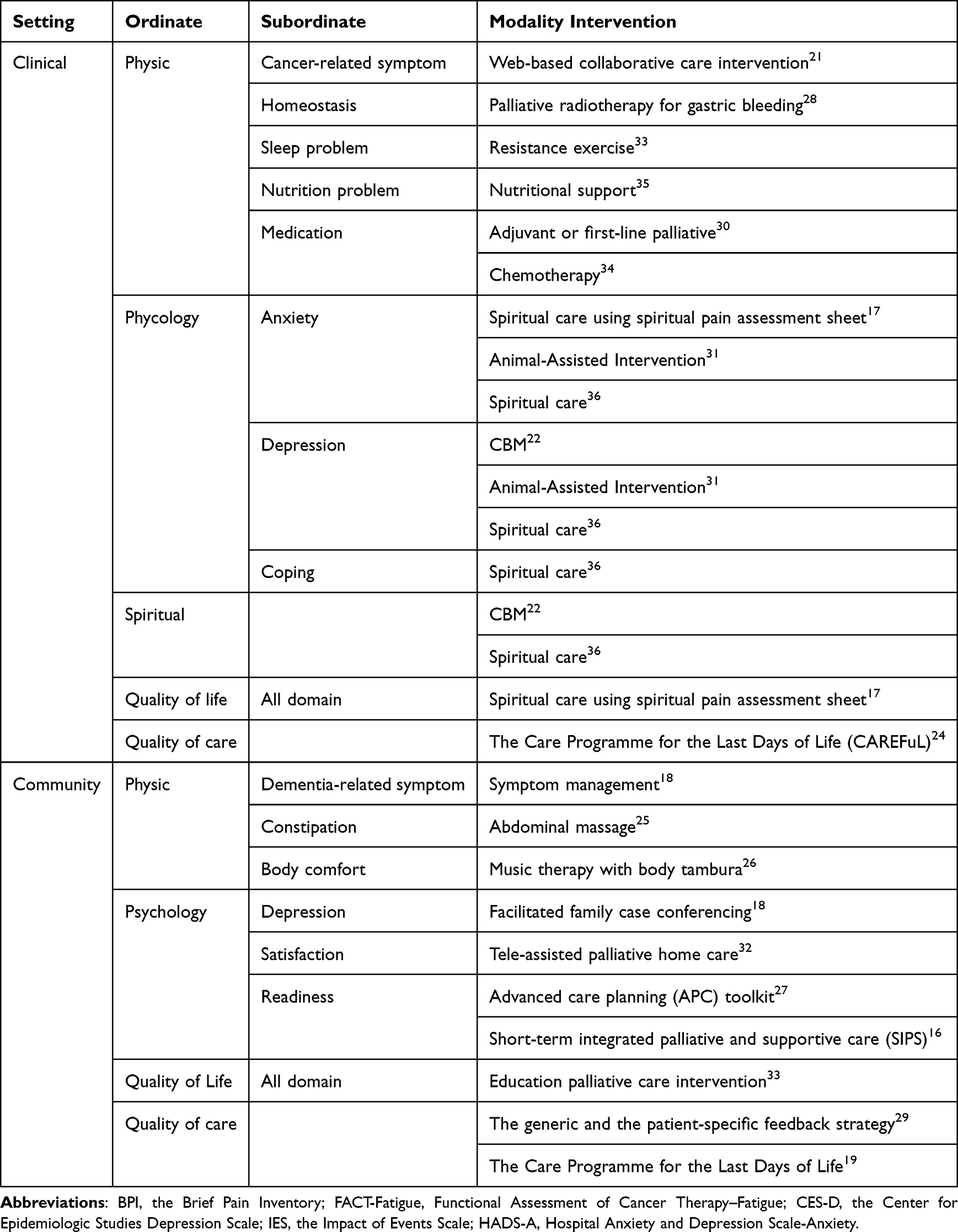 |
Table 2 Themes, Ordinate, Sub-Ordinate Themes, and Modality Intervention |
Outcome of Palliative Care
From the reported intervention modalities in both hospital and community settings, only a few modalities have shown statistically significant better outcomes. In a acute care setting, resistance exercise improves sleep quality,33 nutritional support enhances nutritional status,35 spiritual care reduces anxiety, depression, and spiritual distress while improving coping skills.36 Additionally, The Care Program for the Last Days of Life (CAREFuL) enhances the quality of care for patients with end-of-life.24 Furthermore, definitive therapy such palliative radiotherapy for gastric bleeding increases hemoglobin levels,28 and chemotherapy improves survival rates.34 In a community setting, symptom management reduces pain and pressure ulcers,18 facilitated family case conferencing improves medication,32 and patient feedback enhances satisfaction with palliative care.23 Among all the modalities found in both clinical and community settings, none of them show an improvement in QoL as the primary outcome of palliative care (see Table 3). However, modalities that demonstrate positive results can be integrated into a holistic and continuum palliative care approach to enhance QoL.
 |
Table 3 Study Outcome |
Discussion
Principal Finding
The study found several points, including (1) the results evaluated various intervention palliative care modalities for geriatric in both hospital and community settings. (2) Statistically significant positive outcomes were observed for a few interventions. In the clinical setting, resistance exercise improved sleep quality,33 nutritional support enhanced nutritional status,35 and spiritual care reduced anxiety, depression, and spiritual distress while improving coping skills.36 The Care Program for the Last Days of Life improved the quality of care.24 Palliative radiotherapy for gastric bleeding increased hemoglobin levels, and chemotherapy improved survival rates.28 In the community setting, symptom management reduced pain and pressure ulcers,18 facilitated family case conferencing improved medication,32 and patient feedback enhanced satisfaction with palliative care.23 However, none of the interventions demonstrated an improvement in QoL as the primary outcome.
Resistance exercise has been found to have a positive impact on the physical well-being of geriatric patients in palliative care.33 One significant outcome is the improvement in sleep quality.33 Engaging in regular exercise, tailored to the capabilities of everyone, can help regulate sleep patterns and promote better overall sleep quality. It can reduce restlessness, alleviate physical discomfort, and contribute to a more restful and rejuvenating sleep experience.40 By improving sleep quality, patients may experience increased energy levels, reduced fatigue, and an enhanced sense of well-being.41,42 Sleep is a natural, reversible condition that is governed predominantly by neurobiological processes, and it is a physiological component of human life that is essential for maintaining health and well-being.43–45 Furthermore, nutritional support is another essential aspect of physical care in palliative settings.
Adequate nutrition plays a crucial role in maintaining the strength and overall well-being of geriatric patients.35 In palliative care, individuals may face challenges such as poor appetite, difficulty eating, or weight loss due to the underlying illness or treatment side effects.46,47 Providing appropriate nutritional support helps address these issues and ensures that patients receive the necessary nutrients to meet their nutritional requirements. By enhancing the nutritional status of patients, nutritional support can have several positive outcomes. It can help prevent malnutrition, promote healthy weight maintenance, and support muscle strength and function.48,49 Proper nutrition provides the energy needed for daily activities, enhances the body’s ability to heal and recover, and can contribute to an improved overall quality of life for individuals receiving palliative care. The European Society for Clinical Nutrition and Metabolism (ESPEN) recommendations promote nutritional support for cancer patients. If oral food intake is inadequate despite counseling and Oral Nutritional supplement (ONS) in a patient receiving curative anticancer drugs, additional enteral or, if necessary, parenteral nutrition.50 Anticancer treatment is palliative for unresectable locally advanced or metastatic disease. Due to its survival benefits, chemotherapy is widely used as palliative treatment for advanced cancer.51 Nutritional support for these individuals may improve chemotherapy tolerance and survival.52,53
Palliative radiotherapy especially for gastric bleeding has been found to increase hemoglobin levels in geriatric patients with gastric bleeding.28 By targeting the bleeding site with radiotherapy, it can help control the bleeding, reduce symptoms, and improve overall blood parameters. In certain cases, chemotherapy as a palliative intervention can improve survival rates.30 It is used to manage symptoms, slow disease progression, and extend the lifespan of geriatric patients with advanced or metastatic cancer.
The implementation of spiritual care interventions has shown significant positive effects on the well-being of geriatric patients receiving palliative care. These interventions have been found to effectively reduce anxiety, depression, and spiritual distress, while simultaneously improving patients’ coping skills.36 Spiritual care plays a crucial role in addressing the existential and spiritual needs of individuals facing end-of-life challenges.54,55 It provides a supportive framework that acknowledges and attends to the deeper dimensions of human experience.56 By offering comfort, meaning, and a sense of peace, spiritual care aims to enhance the overall QoL for patients during their end-of-life journey.57–59
Anxiety and depression are common emotional experiences for individuals navigating the complexities of serious illness and mortality.60,61 Spiritual care interventions, such as utilizing spiritual pain assessment sheets, animal-assisted therapy, spiritual counseling, and cognitive-behavioral therapy, have demonstrated their effectiveness in alleviating these psychological burdens. These interventions help geriatric patients find solace, make sense of their circumstances, and develop inner strength and resilience.
In terms of psychological outcome, spiritual care interventions provide support for geriatric patients in managing spiritual distress, which can arise when individuals experience a disconnect or conflict in their core beliefs, values, or sense of meaning. By offering a safe and empathetic space for exploration and reflection, spiritual care interventions empower patients to find greater harmony and acceptance amidst the existential challenges they face.62 By integrating spiritual care into the palliative care framework, healthcare providers can holistically address the diverse needs of patients, recognizing their physical, psychological, and spiritual dimensions.63–66 This comprehensive approach promotes overall well-being, improves emotional resilience, and contributes to a greater sense of comfort and peace for patients as they navigate their end-of-life journey.66–68
The comprehensive care program known as CAREFuL is specifically designed to improve the quality of care provided to geriatric patients nearing the end-of-life.24 This program recognizes the importance of delivering specialized support and attention to individuals during this critical stage of their journey.24 CAREFuL is tailored to address the unique needs of geriatric patients and their families, aiming to enhance their comfort, dignity, and overall experience. It recognizes that end-of-life care requires a multidimensional approach that goes beyond solely focusing on medical interventions. However, the person-centered approach fosters a sense of empowerment and control for patients, allowing them to actively participate in decisions about their care.69
In the community setting, symptom management interventions play a crucial role in palliative care by focusing on reducing pain and alleviating distressing symptoms, such as pressure ulcers.18 These interventions aim to enhance the comfort and well-being of geriatric patients, ultimately contributing to a higher QoL during their remaining time.70 Pain is a prevalent symptom experienced by individuals receiving palliative care.9,71 Effective pain management interventions, such as medication, physical therapies, and complementary approaches like massage or acupuncture, can help alleviate pain and improve patients’ overall comfort.72,73 By managing pain effectively, patients are better able to engage in meaningful activities, maintain their independence, and experience a greater sense of well-being.
Pressure ulcer is a common symptom frequently experience by older adults receiving palliative care and may can predictor as physiological indicators of the approaching end of life. Pressure ulcers, also known as bedsores or pressure sores, are common among patients with limited mobility or those who spend prolonged periods in bed or a seated position.74 These ulcers can cause significant discomfort and pain, and if not managed properly, they can lead to complications and further decline in a patient’s health.75 Symptom management interventions for pressure ulcers may involve regular repositioning, specialized cushions or mattresses, wound care, and the implementation of preventive measures.76 By effectively managing and preventing pressure ulcers, patients can experience relief from discomfort, maintain skin integrity, and improve their overall QoL.
Proper symptom management interventions not only address physical discomfort but also have a positive impact on geriatric patients’ emotional well-being. Uncontrolled pain or distressing symptoms can contribute to feelings of anxiety, depression, and overall distress.39 By effectively managing symptoms, patients may improve psychological well-being, reduce anxiety, and enhance emotional resilience. This, in turn, may allow them to engage more fully in meaningful activities, maintain social connections, and find a sense of peace during their remaining time. The success of symptom management at home undoubtedly involves the active involvement of the patient’s caregiving family members.
Facilitated family case conferencing is a valuable approach that aims to improve medication management for geriatric patients receiving palliative care.32 This intervention recognizes the important role of the patient’s family in the caregiving process and involves them in care discussions and decision-making. By engaging the patient’s family in case conferences, healthcare providers can foster better communication, collaboration, and coordination among all involved parties.38 This collaborative approach ensures that everyone has a shared understanding of the patient’s medication regimen, including dosage, timing, and potential side effects.77 It enables family members to actively participate in medication management, thereby promoting adherence to the prescribed medication regimen. This active involvement improves the safety and effectiveness of medication management, leading to better symptom control and overall care outcomes. Moreover, facilitated family case conferencing provides an opportunity for healthcare providers to educate and empower family members about the medications being used in palliative care.78 With this knowledge, family members can better support the patient in managing their symptoms and make informed decisions about their care.
Collecting feedback from patients is another valuable strategy in improving palliative care.23 By seeking feedback directly from patients, healthcare providers gain insights into the effectiveness of the interventions and services provided. Patient feedback helps identify areas of improvement and ensures that the care delivered is responsive to individual needs and preferences.79 This feedback-driven approach promotes patient-centered care, as it allows healthcare providers to tailor their interventions, communication, and support to meet the specific requirements of each patient. By actively involving patients in their care and addressing their concerns and preferences, healthcare providers can enhance patient satisfaction and contribute to a more positive overall experience for patients receiving palliative care.79
Study Limitation
The scoping review offers a comprehensive overview of the current landscape of palliative care models available for geriatric patients and its outcomes at the global setting. The review result highlights the need for further research and the importance of considering the specific needs and characteristics of this population when designing and implementing palliative care interventions. However, the scoping review has several limitations that should be acknowledged.
The review’s inclusion criteria focused on articles published in peer-reviewed journals, potentially leading to a bias towards studies that have been accepted for publication. Preprints, which may contain relevant information, were excluded from the selection process. Additionally, the review did not apply any other languages, location, or time restrictions, which could introduce the selection bias towards studies conducted in certain regions or published within a specific timeframe.
The review relied on published articles from selected databases, which may introduce publication bias. Positive or statistically significant results are more likely to be published, while studies with negative or non-significant findings may be underrepresented. This bias could affect the overall findings and conclusions of the review. Finally, bias due to generalizability. The scoping review focused specifically on palliative care interventions for geriatric patients. While this provides valuable insights into older population, the findings may not be directly generalizable to other age groups or patient populations receiving palliative care.
Implication to Practice
This study has several implications for nursing practice in palliative care. Firstly, nurses can collaborate with physical therapists and other healthcare professionals to integrate resistance exercise programs into the care plans of patients. By promoting regular exercise, nurses can help improve sleep quality and overall physical well-being. Secondly, nurses play a crucial role in assessing and addressing the nutritional needs of patients. By addressing inadequate nutrition, nurses can help prevent malnutrition and support overall physical function. Thirdly, nurses should recognize the importance of spiritual care and collaborate with spiritual care providers to assess and address spiritual needs, promoting psychological and spiritual well-being. Lastly, nurses can advocate for comprehensive care programs like CAREFuL to improve the quality of care provided to patients nearing the end of life.
Additionally, nurses should prioritize effective symptom management, involving pain control and prevention of pressure ulcers. They should involve family members in care discussions, especially regarding medication management, to ensure coordination and understanding. Seeking patient feedback is also crucial, as it allows nurses to tailor care approaches and enhance patient satisfaction. By incorporating these implications into nursing practice, healthcare providers can deliver holistic, patient-centered care that improves the well-being and QoL for patients in palliative care settings.
The review has implications for further research, particularly in nursing practice. According to the significant results, further research is needed to explore the psychosocial and spiritual dimensions of palliative care. Investigating the impact of psychosocial interventions and spiritual care on patients’ well-being can provide insights into effective strategies for addressing emotional, social, and existential needs. Understanding the role of spirituality and meaning making in palliative care can help healthcare providers develop holistic approaches that support patients’ spiritual well-being and enhance coping mechanisms. Furthermore, further research should focus on the experiences and needs of family caregivers in palliative care. Exploring the challenges, support systems, and interventions that can effectively assist family members in their caregiving role is crucial. By understanding the perspectives and experiences of family caregivers, researchers can identify strategies to enhance their well-being, improve communication, and develop interventions that promote family-centered care. Also, meta-analysis may need to asses size effect of some potential interventions.
Conclusion
The review evaluated various models of palliative care for geriatric patients both in clinical and community settings, addressing physical, psychological, spiritual, QoL, and quality of care aspects. In the clinical setting, interventions such as resistance exercise, nutritional support, spiritual care, and The CAREFuL showed positive outcomes. Palliative care interventions improved sleep quality, enhanced nutritional status, reduced anxiety, depression, and spiritual distress, and improved coping skills. Palliative radiotherapy and chemotherapy also demonstrated benefits in terms of increased hemoglobin levels and improved survival rates. Furthermore, in the community setting, interventions including symptom management, facilitated family case conferencing, tele-assisted palliative home care, and education palliative care intervention had positive effects. These interventions reduced pain and pressure ulcers, improved medication management, and enhanced patient satisfaction with palliative care. However, none of the interventions reviewed showed a significant improvement in QoL as the primary outcome. This highlights the need for further research and development of interventions specifically targeting the enhancement of QoL for geriatric patients receiving palliative care.
While these interventions have shown statistically significant positive outcomes in specific areas, palliative care is a complex and individualized field. The effectiveness of interventions may vary depending on the unique needs and circumstances of each patient. Therefore, a holistic and personalized approach is crucial to provide comprehensive palliative care that improves overall QoL.
Funding
This review is conducted by APC support from Universitas Padjadjaran. Also, we would like to express our sincere gratitude to Dr. Jerico Perdosi from The Queensland University of Technology Australia for his invaluable assistance in proofreading..
Disclosure
The authors declare that they have no conflicts of interest in this study.
References
1. Kelley AS, Morrison RS, Campion EW. Palliative care for the seriously ill. N Engl J Med. 2015;373(8):747–755. doi:10.1056/NEJMra1404684
2. Teoli D, Schoo C, Kalish VB Palliative Care. StatPearls; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537113/.
3. Haroen H, Mirwanti R, Sari CW. Knowledge and attitude toward end-of-life care of nursing students after completing the multi-methods teaching and learning palliative care nursing course. Sustainability. 2023;15(5):4382. doi:10.3390/su15054382
4. Rome RB, Luminais HH, Bourgeois DA, Blais CM. The role of palliative care at the end of life. Ochsner J. 2011;11(4):348–352.
5. World Health Organization. Ageing and health; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.
6. Saracino RM, Bai M, Blatt L, Solomon L, McCorkle R. Geriatric palliative care: meeting the needs of a growing population. Geriatric Nursing. 2018;39(2):225–229. doi:10.1016/j.gerinurse.2017.09.004
7. World Health Organization. Better palliative care for older people world health; 2004. 40. Available from: http://www.euro.who.int/__data/assets/pdf_file/0009/98235/E82933.pdf.
8. Lipman AG. Palliative care for older people: better practices. J Pain Palliat Care Pharmacother. 2012;26(1):81. doi:10.3109/15360288.2011.650361
9. World Health Organization. Palliative care; 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/palliative-care.
10. Goldstein NE, Morrison RS. The intersection between geriatrics and palliative care: a call for a new research agenda. J Am Geriatr Soc. 2005;53(9):1593–1598. doi:10.1111/j.1532-5415.2005.53454.x
11. Hanson LC, Winzelberg G. Research priorities for geriatric palliative care: goals, values, and preferences. J Palliat Med. 2013;16(10):1175–1179. doi:10.1089/jpm.2013.9475
12. Ding J, Johnson CE, Auret K, et al. Comparison of end-of-life care for people living in home settings versus residential aged care facilities: a nationwide study among Australian general practitioners. Health Soc Care Community. 2022;30(1):91–101. doi:10.1111/hsc.13375
13. Penders YWH, Van Den Block L, Deliens L, Donker GA, Onwuteaka-Philipsen B. Comparison of end-of-life care for older people living at home and in residential homes: a mortality follow-back study among GPS in the Netherlands. Br J Gen Pract. 2015;65(640):e724–30. doi:10.3399/bjgp15X687349
14. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol Theory Pract. 2005;8(1):19–32. doi:10.1080/1364557032000119616
15. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
16. Bone AE, Morgan M, Maddocks M, et al. Developing a model of short-term integrated palliative and supportive care for frail older people in community settings: perspectives of older people, carers and other key stakeholders. Age Ageing. 2016;45(6):863–873. doi:10.1093/ageing/afw124
17. Ichihara K, Ouchi S, Okayama S, et al. Effectiveness of spiritual care using spiritual pain assessment sheet for advanced cancer patients: a pilot non-randomized controlled trial. Palliat Support Care. 2019;17(1):46–53. doi:10.1017/S1478951518000901
18. Elyn A, Sourdet S, Morin L, et al. End of life care practice and symptom management outcomes of nursing home residents with dementia: secondary analyses of IQUARE trial. Eur Geriatr Med. 2019;10(6):947–955. doi:10.1007/s41999-019-00234-9
19. Verhofstede R, Smets T, Cohen J, Costantini M, Van Den Noortgate N, Deliens L. Improving end-of-life care in acute geriatric hospital wards using the care programme for the last days of life: study protocol for a Phase 3 cluster randomized controlled trial. BMC Geriatr. 2015;15(1):1–10. doi:10.1186/s12877-015-0010-7
20. Vitacca M, Comini L, Tabaglio E, Platto B, Gazzi L. Tele-assisted palliative homecare for advanced chronic obstructive pulmonary disease: a feasibility study. J Palliat Med. 2019;22(2):173–178. doi:10.1089/jpm.2018.0321
21. Steel JL, Geller DA, Kim KH, et al. Web-based collaborative care intervention to manage cancer-related symptoms in the palliative care setting. Cancer. 2016;122(8):1270–1282. doi:10.1002/cncr.29906
22. Milbury K, Li Y, Durrani S, et al. A mindfulness-based intervention as a supportive care strategy for patients with metastatic non-small cell lung cancer and their spouses: results of a three-arm pilot randomized controlled Trial. Oncologist. 2020;25(11):e1794–802. doi:10.1634/theoncologist.2020-0125
23. Boogaard JA, de Vet HCW, van Soest-Poortvliet MC, Anema JR, Achterberg WP, van der Steen JT. Effects of two feedback interventions on end-of-life outcomes in nursing home residents with dementia: a cluster-randomized controlled three-armed trial. Palliat Med. 2018;32(3):693–702. doi:10.1177/0269216317750071
24. Beernaert K, Smets T, Cohen J, et al. Improving comfort around dying in elderly people: a cluster randomised controlled trial. Lancet. 2017;390(10090):125–134. doi:10.1016/S0140-6736(17)31265-5
25. Dadura E, Stȩpień P, Iwańska D, Wójcik A. Effects of abdominal massage on constipation in palliative care patients - A pilot study. Postep Rehabil. 2017;31(4):19–34.
26. Teut M, Dietrich C, Deutz B, Mittring N, Witt CM. Perceived outcomes of music therapy with body tambura in end of life care - A qualitative pilot study. BMC Palliat Care. 2014;13(1):1–6. doi:10.1186/1472-684X-13-18
27. Nouri SS, Ritchie C, Volow A, et al. A toolkit for community-based, Medicaid-funded case managers to introduce advance care planning to frail, older adults: a pilot study. J Palliat Med. 2021;24(3):428–432. doi:10.1089/jpm.2020.0200
28. Kondoh C, Shitara K, Nomura M, et al. Efficacy of palliative radiotherapy for gastric bleeding in patients with unresectable advanced gastric cancer: a retrospective cohort study. BMC Palliat Care. 2015;14(1):1–6. doi:10.1186/s12904-015-0034-y
29. Bökberg C, Behm L, Ahlström G. Quality of life of older persons in nursing homes after the implementation of a knowledge-based palliative care intervention. Int J Older People Nurs. 2019;14(4):1–11. doi:10.1111/opn.12258
30. Lund CM, Vistisen KK, Olsen AP, et al. The effect of geriatric intervention in frail older patients receiving chemotherapy for colorectal cancer: a randomised trial (GERICO). Br J Cancer. 2021;124(12):1949–1958. doi:10.1038/s41416-021-01367-0
31. Scagnetto F, Poles G, Guadagno C, Notari V, Giacopini N. Animal-assisted intervention to improve end-of-life care: the moderating effect of gender and pet ownership on anxiety and depression. J Altern Complement Med. 2020;26(9):841–842. doi:10.1089/acm.2019.0342
32. Agar M, Luckett T, Luscombe G, et al. Effects of facilitated family case conferencing for advanced dementia: a cluster randomised clinical trial. PLoS One. 2017;12(8):e0181020. doi:10.1371/journal.pone.0181020
33. Steindorf K, Wiskemann J, Ulrich CM, Schmidt ME. Effects of exercise on sleep problems in breast cancer patients receiving radiotherapy: a randomized clinical trial. Breast Cancer Res Treat. 2017;62(3):489–499. doi:10.1007/s10549-017-4141-8
34. Berger AK, Abel U, Komander C, Harig S, Jäger D, Springfeld C. Chemotherapy for advanced pancreatic adenocarcinoma in elderly patients (≥70 years of age): a retrospective cohort study at the national center for tumor diseases Heidelberg. Pancreatology. 2014;14(3):211–215. doi:10.1016/j.pan.2014.03.004
35. Li W, Yang Y, Li Z, Chen W. Effect of malnutrition and nutritional support to reduce infections in elderly hospitalized patients with cancer: a multicenter survey in China. Nutrition. 2023;106:111894. doi:10.1016/j.nut.2022.111894
36. Bovero A, Tosi C, Botto R, Opezzo M, Giono-Calvetto F, Torta R. The spirituality in end-of-life cancer patients, in relation to anxiety, depression, coping strategies and the daily spiritual experiences: a cross-sectional study. J Relig Health. 2019;58(6):2144–2160. doi:10.1007/s10943-019-00849-z
37. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
38. Warner G, Baird LG, McCormack B, et al. Engaging family caregivers and health system partners in exploring how multi-level contexts in primary care practices affect case management functions and outcomes of patients and family caregivers at end of life: a realist synthesis. BMC Palliat Care. 2021;20(1):114. doi:10.1186/s12904-021-00781-8
39. X-M L, Xiao W-H, Yang P, Zhao H-X. Psychological distress and cancer pain: results from a controlled cross-sectional survey in China. Sci Rep. 2017;7(1):39397. doi:10.1038/srep39397
40. Geneen LJ, Moore RA, Clarke C, Martin D, Colvin LA, Smith BH. Physical activity and exercise for chronic pain in adults: an overview of Cochrane reviews. Cochrane Database Syst Rev. 2017;4(4):CD011279. doi:10.1002/14651858.CD011279.pub3
41. Moy S, Kober KM, Viele C, et al. Level of exercise influences the severity of fatigue, energy levels, and sleep disturbance in oncology outpatients receiving chemotherapy. Cancer Nurs. 2022;45(1):3–11. doi:10.1097/NCC.0000000000000875
42. Imanian M, Imanian M, Karimyar M. Sleep quality and fatigue among breast cancer patients undergoing chemotherapy. Int J Hematol Stem Cell Res. 2019;13(4):196–200.
43. Krueger JM, Frank MG, Wisor JP, Roy S. Sleep function: toward elucidating an enigma. Sleep Med Rev. 2016;28:46–54. doi:10.1016/j.smrv.2015.08.005
44. Irwin MR. Why sleep is important for health: a psychoneuroimmunology perspective. Annu Rev Psychol. 2015;66(1):143–172. doi:10.1146/annurev-psych-010213-115205
45. Sejbuk M, Mirończuk-Chodakowska I, Witkowska AM. Sleep quality: a narrative review on nutrition, stimulants, and physical activity as important factors. Nutrients. 2022;14(9):1912. doi:10.3390/nu14091912
46. Fringer A, Stängle S, Büche D, Ott SC, Schnepp W, Fernández-Alcántara M. The associations of palliative care experts regarding food refusal: a cross-sectional study with an open question evaluated by triangulation analysis. PLoS One. 2020;15(4):e0231312. doi:10.1371/journal.pone.0231312
47. National Cancer Institute. Nutrition in cancer care (PDQ®)–patient version – NCI. national cancer institute; 2022. Available from: https://www.cancer.gov/about-cancer/treatment/side-effects/appetite-loss/nutrition-pdq.
48. Cook F, Rodriguez JM, McCaul LK. Malnutrition, nutrition support and dietary intervention: the role of the dietitian supporting patients with head and neck cancer. Br Dent J. 2022;233(9):757–764. doi:10.1038/s41415-022-5107-8
49. Prado CM, Purcell SA, Laviano A. Nutrition interventions to treat low muscle mass in cancer. J Cachexia Sarcopenia Muscle. 2020;11(2):366–380. doi:10.1002/jcsm.12525
50. Arends J, Bachmann P, Baracos V, et al. ESPEN guidelines on nutrition in cancer patients. Clin Nutr. 2017;36(1):11–48. doi:10.1016/j.clnu.2016.07.015
51. Von Hoff DD, Ervin T, Arena FP, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013;369(18):1691–1703. doi:10.1056/NEJMoa1304369
52. Bozzetti F. Nutritional support of the oncology patient. Crit Rev Oncol Hematol. 2013;87(2):172–200. doi:10.1016/j.critrevonc.2013.03.006
53. Sriati A, Rahayuwati L, Komariah M, et al. The balance of spiritual and nutritional needs improves the well-being of cancer patients during chemotherapy. Open Access Maced J Med Sci. 2021;9(T6):138–142. doi:10.3889/oamjms.2021.7321
54. Liefbroer AI, Otten R, Olsman E. Spiritual care in palliative care: a systematic review of the recent European literature. Med Sci. 2019;7(2):5.
55. Best M, Butow P, Olver I. Do patients want doctors to talk about spirituality? A systematic literature review. Patient Educ Couns. 2015;98(11):1320–1328. doi:10.1016/j.pec.2015.04.017
56. Demirsoy N. Holistic care philosophy for patient‐centered approaches and spirituality. Patient Cent Medi. 2017;6. doi:10.5772/66165
57. Taylor EJ. Spiritual screening, history, and assessment. In: Oxford Textbook of Palliative Nursing. Oxford University Press; 2019. doi10.1093/med/9780190862374.003.0034
58. Phelps AC, Lauderdale KE, Alcorn S, et al. Addressing spirituality within the care of patients at the end of life: perspectives of patients with advanced cancer, oncologists, and oncology nurses. J Clin Oncol off J Am Soc Clin Oncol. 2012;30(20):2538–2544. doi:10.1200/JCO.2011.40.3766
59. Chen J, Lin Y, Yan J, Wu Y, Hu R. The effects of spiritual care on quality of life and spiritual well-being among patients with terminal illness: a systematic review. Palliat Med. 2018;32(7):1167–1179. doi:10.1177/0269216318772267
60. Bobo WV, Grossardt BR, Virani S, St Sauver JL, Boyd CM, Rocca WA. Association of depression and anxiety with the accumulation of chronic conditions. JAMA Netw open. 2022;5(5):e229817. doi:10.1001/jamanetworkopen.2022.9817
61. Lee J, Cho Y, Oh J, et al. Analysis of anxiety or depression and long-term mortality among survivors of out-of-hospital cardiac arrest. JAMA Netw open. 2023;6(4):e237809. doi:10.1001/jamanetworkopen.2023.7809
62. Musa AS. Spiritual care intervention and spiritual well-being. J Holist Nurs off J Am Holist Nurses’ Assoc. 2017;35(1):53–61. doi:10.1177/0898010116644388
63. Miller M, Addicott K, Rosa WE. Spiritual care as a core component of palliative nursing. Am J Nurs. 2023;123(2):54–59. doi:10.1097/01.NAJ.0000919748.95749.e5
64. Beaussant Y, Nichipor A, Balboni TA. 1072C17.2Integration of spiritual care into palliative care service delivery models. In: Oxford Textbook of Palliative Medicine. Oxford University Press; 2021. doi10.1093/med/9780198821328.003.0101
65. Haroen H, Mirwanti R, Agustina HR, et al. A qualitative study of perception and experience toward end-of-life care among nursing students who witnessed dying people in their family. J Multidiscip Healthc. 2023;16:2261–2270. doi:10.2147/JMDH.S423198
66. Nursiswati N, Haroen H, Herliani YK, Harun H. Spiritual well-being among women with breast cancer: a scoping review. Malaysian J Med Heal Sci. 2022;18:314–322.
67. Komariah M, Hatthakit U, Boonyoung N. Impact of Islam-based caring intervention on spiritual well-being in Muslim women with breast cancer undergoing chemotherapy. Religions. 2020;11(7):1–13. doi:10.3390/rel11070361
68. Komariah M, Qadous SG, Firdaus MKZH, et al. The psychological experiences of using Islamic philosophy approach among women’s with advanced breast cancer in Indonesia. Open Access Maced J Med Sci. 2021;9(T6):133–137. doi:10.3889/oamjms.2021.7320
69. Pulvirenti M, McMillan J, Lawn S. Empowerment, patient centred care and self-management. Heal Expect an Int J Public Particip Heal Care Heal Policy. 2014;17(3):303–310.
70. Chapman EJ, Pini S, Edwards Z, Elmokhallalati Y, Murtagh FEM, Bennett MI. Conceptualising effective symptom management in palliative care: a novel model derived from qualitative data. BMC Palliat Care. 2022;21(1):17. doi:10.1186/s12904-022-00904-9
71. Yang GM, Ewing G, Booth S. What is the role of specialist palliative care in an acute hospital setting? A qualitative study exploring views of patients and carers. Palliat Med. 2012;26(8):1011–1017. doi:10.1177/0269216311425097
72. Deng G. Integrative medicine therapies for pain management in cancer patients. Cancer J. 2019;25(5):343–348. doi:10.1097/PPO.0000000000000399
73. Singh P, Chaturvedi A. Complementary and alternative medicine in cancer pain management: a systematic review. Indian J Palliat Care. 2015;21(1):105–115. doi:10.4103/0973-1075.150202
74. Witkowski JA, Parish LC, Karadag AS, Parish JL. Pressure Ulcer. Treat Ski Dis Compr Ther Strateg; 2022:181–186. Available from https://www.ncbi.nlm.nih.gov/books/NBK553107/.
75. Horvat VB, Kos M. Dekubitus kao glavni indikator kvalitete zdravstvene njege na neurološkom odjelu [Pressure ulcer as the principal indicator of health care quality at neurology department]. Acta Med Croatica. 2016;70(Suppl 1):17–24. Croatian.
76. Al Aboud AM, Manna B. Wound Pressure Injury Management. StatPearls; 2023. Available from https://www.ncbi.nlm.nih.gov/books/NBK532897/.
77. Manias E, Bucknall T, Hughes C, Jorm C, Woodward-Kron R. Family involvement in managing medications of older patients across transitions of care: a systematic review. BMC Geriatr. 2019;19(1):95. doi:10.1186/s12877-019-1102-6
78. Widera E, Anderson WG, Santhosh L, McKee KY, Smith AK, Frank J. Family meetings on behalf of patients with serious illness. N Engl J Med. 2020;383(11):e71. doi:10.1056/NEJMvcm1913056
79. Wong E, Mavondo F, Fisher J. Patient feedback to improve quality of patient-centred care in public hospitals: a systematic review of the evidence. BMC Health Serv Res. 2020;20(1):530. doi:10.1186/s12913-020-05383-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.