")
Back to Journals » Journal of Pain Research » Volume 16
Ultrasound-Guided Modified Thoracolumbar Fascial Plane Block in Tianji Robot-Assisted Lumbar Internal Fixation: A Prospective, Randomized, and Non-Inferiority Study
Authors Hu L , Shen Z, Pei D, Sun J, Zhang B, Zhu Z , Yan W, Zhou H , An E
Received 1 November 2022
Accepted for publication 13 February 2023
Published 18 February 2023 Volume 2023:16 Pages 543—552
DOI https://doi.org/10.2147/JPR.S395677
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ellen M Soffin
Li Hu,1,2,* Zhuoer Shen,3,* Daqing Pei,1,2 Jintao Sun,4 Bin Zhang,1 Zhipeng Zhu,1 Weiwei Yan,1 Hongmei Zhou,1– 3 Erdan An1,2
1Department of Anesthesiology, The Second Affiliated Hospital of Jiaxing University, Jiaxing City, People’s Republic of China; 2Key Laboratory of Basic Research and Clinical Transformation of Perioperative Precision Anesthesia, Jiaxing City, People’s Republic of China; 3Department of Anesthesiology, Bengbu Medical College, Bengbu City, People’s Republic of China; 4Jiaxing University Master Degree Cultivation Base, Zhejiang Chinese Medical University, Hangzhou City, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hongmei Zhou; Erdan An, Department of Anesthesiology, The Second Affiliated Hospital of Jiaxing University, Huancheng Strasse 1518, Jiaxing, 314000, People’s Republic of China, Tel +86 13867300139 ; +86 13515733732, Fax +86 573 82080930, Email [email protected]; [email protected]
Purpose: Ultrasound-guided modified thoracolumbar fascial plane block (MTLIP) has been reported effective for postoperative pain control following lumbar surgery. Although trauma of the Tianji robot-assisted lumbar internal fixation is reduced, the degree of pain cannot be ignored.MTLIP may improve operation efficiency and reduce puncture complications.This study aimed to explore whether MTLIP is not inferior to thoracolumbar fascial plane block (TLIP) in the treatment of lumbar internal fixation.
Methods: This prospective double-blinded, non-inferiority randomized trial enrolled patients underwent Tianji robot-assisted lumbar internal fixation between April and August 2022 to either MTLIP or TLIP. The primary outcome was an effective dermatomal block area after 30 min. Secondary outcomes included the numeric rating scale (NRS) scores, nerve block operation time, puncture times, image clarity, patient satisfaction, intraoperative opioid consumption, complications/adverse reactions, and Oswestry Disability Index (ODI).
Results: Sixty participants were randomized to MTLIP (n=30) and TLIP (n=30). The effective dermatomal block area 30 min after block was non-inferior in the MTLIP group (283.6 ± 62.6 cm2) compared with the TLIP group (261.4± 53.2 cm2) (P=0.145; estimated mean difference: − 22.17, 95% CI: − 52.19, 7.85; smaller than the non-inferiority margin of 39.5). Compared with TLIP, MTLIP showed shorter operation time, smaller puncture times, and better target definition and satisfaction scores (all P< 0.001). Sufentanil amount, remifentanil amount, PCIA sufentanil dosage, parecoxib amount, NRS scores (increased with time in the two groups but without inter-group differences), and complications were not significantly different between the two groups (all P> 0.05).
Conclusion: This non-inferiority trial supports the hypothesis that MTLIP yields a non-inferior effective dermatomal block area compared with TLIP for Tianji robot-assisted lumbar internal fixation.
Clinical Trials Registration: Chinese Clinical Trial Registry (ChiCTR2200058687);.
Keywords: local anesthetics, regional anesthesia, lumbosacral plexus, lumbar internal fixation, robotic surgical procedures
Introduction
Lumbar fixation can be required for patients with spondylolisthesis, vertebral fracture, or lumbar spinal stenosis.1–3 Such procedures involve high trauma and postoperative pain. With the development of spinal surgical techniques and internal fixation devices, Tianji robot-assisted (Tinavi, Tianji robot, Beijing, China) lumbar internal fixation is emerging in clinical practice.4 This surgical method can assist surgeons in locating implants accurately with sub-millimeter accuracy. It can reduce intraoperative radiation doses by more than 70%, improve surgical efficiency, and reduce blood loss and intraoperative tissue trauma, but perioperative pain still exists with this surgical method.4
In the past, patient-controlled intravenous analgesia (PCIA),5 incision local analgesia,6 and epidural analgesia were the main methods for postoperative analgesia of the lumbar spine. Opioids are often used in PCIA, which has the advantage of convenient use, but it also has obvious disadvantages and adverse reactions, such as hypotension, respiratory depression, nausea and vomiting, and poor analgesic effect.7,8 The perioperative use of non-opioid strategies to reduce opioid use has also been shown to reduce long-term mortality.9 Incision local analgesia only blocks the local anesthesia around the incision, the blocking effect is not accurate, and the blocking time is not good. A meta-analysis highlighted that the effect of incision local analgesia is limited.10 Many clinical studies have shown that epidural analgesia is better than PCIA, but the epidural block can affect the muscle strength of the patients’ lower limbs, and there is a risk of total spinal anesthesia, which limits its clinical use.11–13
Hand et al14 were the first to describe ultrasound-guided thoracolumbar fascial plane block (TLIP). Later, Ahiskalioglu et al15 proposed the ultrasound-guided modified thoracolumbar fascial plane block (MTLIP), in which the block point was changed from multifidus and longissimus to between the iliocostal and longissimus muscles. The location is superficial and easy to locate under ultrasound, and the adjacent muscles, ribs, and pleura imaging are very clear. The puncture direction is also changed from the inside out. A study showed that ultrasound-guided MTLIP could improve postoperative pain in lumbar spine surgery.16 Although the optimal analgesic technique for pain management following Tianji robot-assisted lumbar internal fixation has not yet been determined, it is important to validate alternative analgesic regimens and list their relative advantages and disadvantages.
Therefore, this study aimed to explore whether the effective dermatomal block area 30 min after MTLIP block was not inferior to that of TLIP and explore the efficacy and safety of MTLIP and TLIP in the treatment of lumbar internal fixation.
Materials and Methods
Study Design and Participants
This randomized, double-blinded, non-inferiority trial was conducted at the Second Affiliated Hospital of Jiaxing University between April and August 2022. The study was registered before enrolment of the first patient at the Chinese Clinical Trial Registry (www.chictr.org.cn/) database (ChiCTR2200058687, registered April 14, 2022). This study was approved by the Ethics Committee of Second Affiliated Hospital of Jiaxing University. All participants signed the informed consent form. This manuscript adheres to the applicable CONSORT guidelines.
The inclusion criteria were 1) patients with American Society of Anesthesiologists (ASA) class I–III, 2) 18–65 years of age, 3) body mass index (BMI) of 19–30 kg/m2, and 4) planning to undergo Tianji robot-assisted lumbar internal fixation. The exclusion criteria were 1) patients with a history of chronic opioid or steroid consumption, 2) coagulopathy or therapeutic anticoagulation, or 3) pregnancy.
Randomization and Blinding
The participants were randomized 1:1 to the MTLIP and TLIP groups by the random envelope method, which involved sequentially numbered sealed envelopes. Before performing the block, an envelope was opened by the attending anesthesiologist. The envelope was then resealed and returned to the participant research binder labeled with the medical record number. They were reopened at the end of the study for statistical analysis. The participants, anesthesiologists, data collectors, physicians performing the follow-up, and data analysts were blinded to group allocation. Blinding was maintained until the completion of the final analyses.
Preoperative Management
The participants received oral celecoxib 200 mg as part of the preoperative multimodal analgesia. The participants fasted for 8 h and were not allowed to drink for 2 h before anesthesia. After intravenous cannula insertion, the participants were connected to routine monitors (ECG, non-invasive blood pressure, pulse oximetry) and received supplemental oxygen (2 L/min) via a nasal cannula in the preparation room. Intravenous sedation consisted of 1–2 mg midazolam and 50 µg fentanyl. All blocks were performed by one of the three anesthesiologists from our regional anesthesiology team. All of them had more than 5 years of experience in regional anesthesia. Blinding was enhanced by scanning all participants regardless of group allocation (MTLIP or TLIP) with a low-frequency (3–5 MHz) curvilinear ultrasound transducer just above the intercristal line from the anterior to posterior direction.
Lumbar Plexus Block
In the MTLIP group, the participants were placed in the prone position with the surgical side up. As described in the literature,17 after the probe was covered with a sterile ultrasonic sleeve, the third lumbar spinous process was scanned at the long axis of the patient’s posterior median, and the probe was rotated 90° to the horizontal position of the short axis and moved 2–3 cm laterally until the paraspinous multifidus, longissimus, and iliac ribs exposed the intramuscular fascia. Using an in-plane technique, the needle was inserted from the inside out when the tip reached the longissimus and iliocostal muscles on both sides. The water separation technique was used to confirm the position of the needle tip, and 0.375% ropivacaine (AstraZeneca, Ropivacaine Hydrochloride Injection, London, United Kingdom) 20 mL was injected into the fascia space after back-pumping to confirm the absence of blood and cerebrospinal fluid (Figure 1).
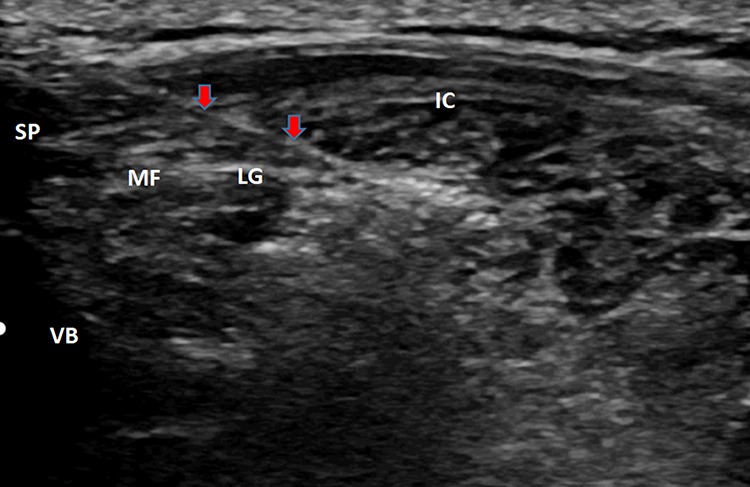 |
Figure 1 Modified thoracolumbar fascial plane block (MTLIP) anatomical process image in ultrasound. The red arrows show the puncture needle. Abbreviations: SP, spinous process; VB, vertebral body; MF, multifidus muscle; LG, longissimus muscle; IC, iliac costal muscle. |
In the TLIP group, after the probe was covered with a sterile ultrasonic sleeve, the third lumbar spinous process was scanned at the long axis of the participants’ posterior median, and the probe was rotated 90° to the horizontal position of the short axis and moved 2–3 cm laterally until the paraspinous multifidus, longissimus, and iliac ribs exposed the intramuscular fascia. Using an in-plane technique, the needle was inserted from the outside in when the tip reached the multifidus and longissimus muscles on both sides. The water separation technique was used to confirm the position of the needle tip, and 0.375% ropivacaine (AstraZeneca, Ropivacaine Hydrochloride Injection, London, United Kingdom) 20 mL was injected into the fascia space after back-pumping to confirm the absence of blood and cerebrospinal fluid. The successful mark of block evaluation 30 minutes after injection is the disappearance of acupuncture pain around the spine.All blocks were successful.
Perioperative Care
After sufficient oxygenation and nitrogen removal, the two groups received the same scheme of intravenous inhalation combined with endotracheal intubation general anesthesia: propofol 50–80 μg·kg-1·min-1 and remifentanil 0.05–0.15 μg·kg-1·min-1 intravenous pumping, and sevoflurane 1–2% inhalation maintenance. According to the administration time and muscle relaxation in the operation area, 0.1 mg/kg atracurium CIS sulfonate and 5 μg sufentanil were added intermittently to maintain a bispectral index (BIS) value of 45–60, and the fluctuations of blood pressure (BP) and heart rate (HR) were within 20% of the baseline value. Both groups were given 5 mg of tropisetron intravenously after the operation. After surgery, the participants were transferred to the post-anesthesia care unit (PACU), where they achieved complete anesthesia recovery before transfer to the surgical ward.
Collectible 200 mg was given orally every 12 h. After tracheal extubation, PCIA was administered 48 h after surgery. The PCIA formulae were sufentanil 100 μg and tropisetron 10 mg, diluted to 100 mL with 0.9% normal saline; the background dose was 1 mL/h, the controlled additional dose (PCA) was 2 mL, and the locking time was 10 min. In addition, parecoxib sodium 40 mg was injected intravenously into patients with a numeric rating scale (NRS) score of ≥5. Patients who developed undesirable opioid side effects (nausea and vomiting) were given tropisetron 5 mg intravenously every 6 h.
Endpoints and Measurement
The primary outcome was the effective area of block 30 min after block, calculated using Adobe Photoshop CS2 software (Adobe, San Jose, CA, USA). At 30 min after TLIP or MTLIP, the area of pain sensation loss due to acupuncture in the posterior part of the thoracolumbar segment was evaluated. The movements were evaluated from the axillary midline at the injection level to the contralateral axillary midline, and the range of disappearance of acupuncture pain sensation was marked. The evaluation range was three lumbar segments above and below the injection level.
The secondary outcomes included 1) nerve block operation time (starting from the ultrasound probe touching the skin of the effective area to the end of the puncture), 2) puncture times (needle back surface skin to reposition number), 3) ultrasound image of puncture clarity score (0: completely invisible; 1: barely visible; 2: visible; 3: very visible and clear), 4) patient satisfaction score (1: dissatisfied; 2: generally satisfied; 3: satisfied; 4: very satisfied), 5) intraoperative dosage of sufentanil and remifentanil, 6) NRS (from 0=“no pain” to 10=“worst possible pain”)18 during movement and rest at 2, 6, 24, and 48 h, 7) amount of sufentanil used by PCIA, 8) amount of parecoxib analgesic rescue, 9) postoperative complications related to nerve block (nerve injury, local hematoma, strayed into spinal canal or epidural, and infection at puncture site), 10) postoperative adverse reactions (nausea, vomiting, and hypotension), and 11) the Oswestry Disability Index (ODI)19 to assess lumbar function before and 3 months after surgery.
All data were collected by the experimental recorder of the research team, who was proficient in anesthesia knowledge and mastered Adobe Photoshop CS2 software. This recorder was blinded to group allocation and anesthetic management. Preoperative general data and surgical information, age, sex, BMI, ASA grade, operation section, anesthesia time, operation time, and intraoperative blood loss were collected for each participant.
Sample Size
The sample size was calculated using PASS 15.0. The study was designed to assess the non-inferiority of MTLIP to TLIP for the primary outcome. The sample size was based on a pilot study with 10 patients in the two groups. The mean effective area of the block 30 min after the block was 280.6±39.2 cm2 with TLIP and 288.1±39.7 cm2 with MTLIP. An acceptable non-inferiority margin was defined as 39.45 cm2, which was determined by 1/2 SD of the effective dermatomal block area 30 min after block in the pilot study. Based on these data, the sample size was calculated as 27 patients per group for 80% power and an alpha error of 0.05. We recruited 33 patients per group to account for potential attrition.
Statistical Analysis
The analysis was performed according to the intention-to-treat principle. Continuous data with a normal distribution were described as means ± standard deviation, and the data with a skewed distribution were described as medians (interquartile range). Inter-group comparisons were performed using the independent-samples t-test for normally distributed data and the Mann–Whitney U-test for non-normally distributed data. Categorical data were expressed as n (%). The inter-group comparison was performed using the chi-square test or Fisher’s exact test. Continuous measurement data were analyzed with one-way ANOVA. P-values <0.05 were considered statistically significant. SPSS 22.0 (IBM, Armonk, NY, USA) was used for statistical analysis.
Results
Characteristics of the Participants
Sixty participants were randomized to MTLIP (n=30) and TLIP (n=30) for Tianji robot-assisted lumbar internal fixation between April and August 2022 (Figure 2). The general information of the participants is listed in Table 1.
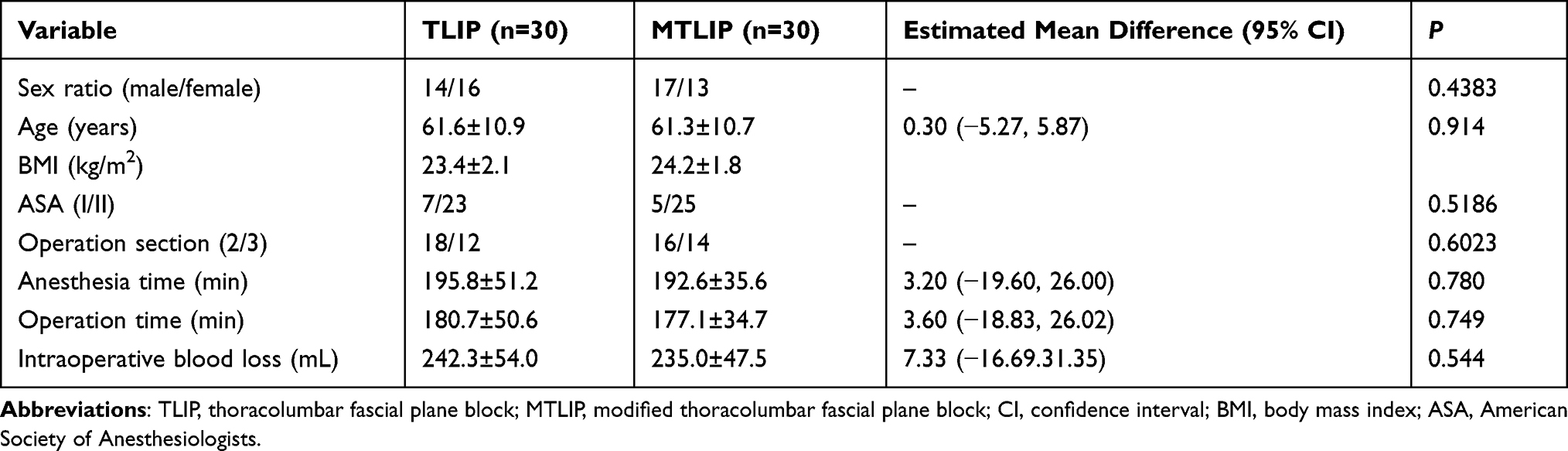 |
Table 1 Characteristics of the Participants |
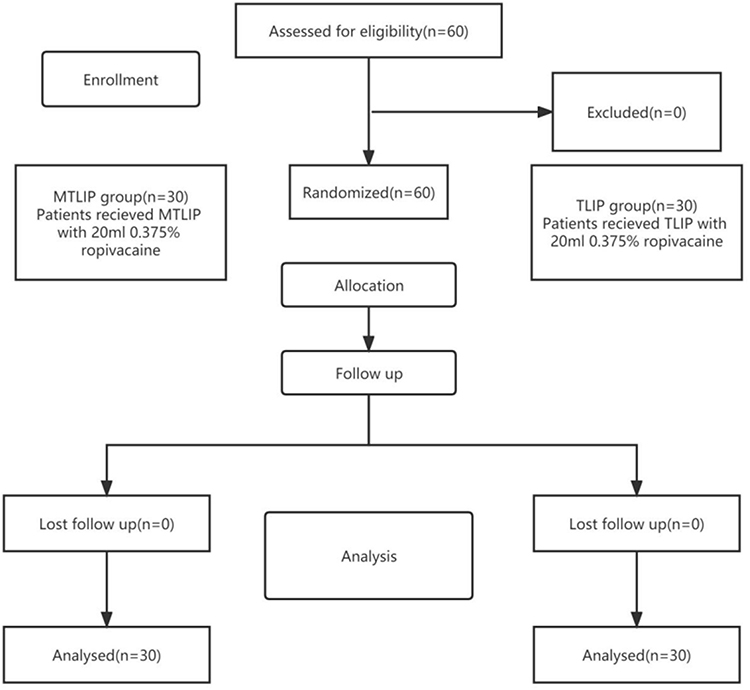 |
Figure 2 Participant flowchart. |
Primary Endpoint
The effective dermatomal block area 30 min after block was non-inferior in the MTLIP group (283.6 ± 62.6 cm2) compared with the TLIP group (261.4±53.2cm2) (P=0.75; estimated mean difference: −22.17, 95% CI: −52.19, 7.85; smaller than the non-inferiority margin).
Secondary Endpoints
The operation time was shorter in the MTLIP group (621.5±191.9 s) compared with the TLIP group (904.5±177.5 s) (P<0.001). The puncture time was lower in the MTLIP group compared with the TLIP group (3±1 vs 4±1, P=0.001). The target definition score and satisfaction score in the MTLIP group were higher than in the TLIP group (P<0.001) (Table 2).
 |
Table 2 Clinical Comparison of Nerve Block Between the Two Groups |
The amount of sufentanil used during operation (P=0.722), the amount of remifentanil used (P=0.760), the number of effective PCIA sufentanil dosages (P=0.687), and the amount of parecoxib were not significantly different between the two groups (Table 3).
 |
Table 3 Comparison of Intraoperative Sufentanil and Remifentanil Dosage, Postoperative PCIA Sufentanil Dosage, and Parecoxib Salvage Volume Between the Two Groups |
The NRS scores at rest were not significantly different between the two groups (P=0.329) but increased with time in both groups (P<0.001); there was no group×time interaction (P=0.662). The NRS scores when moving were not significantly different between the two groups (P=0.064) but increased with time in both groups (P<0.001); there was no group×time interaction (P=0.898) (Table 4).
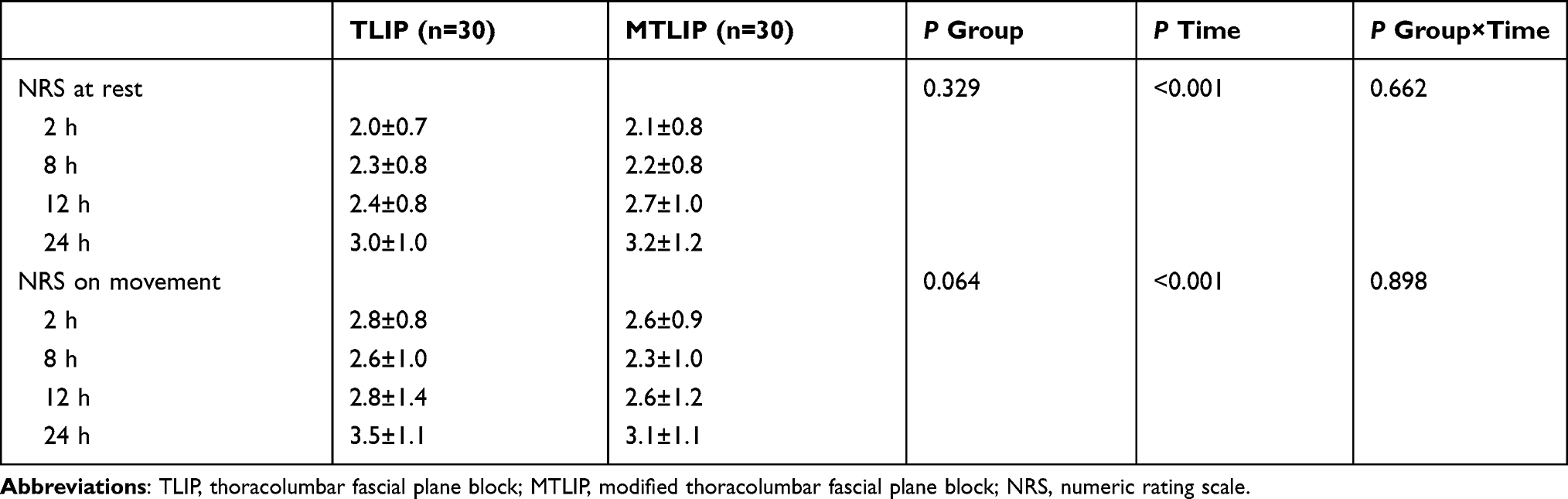 |
Table 4 Comparison of NRS Scores Between the Two Groups at Different Time Points |
There were no significant differences in complications related to nerve block (nerve injury, local hematoma, accidental entry into spinal canal or epidural, puncture site infection), the incidence of nausea and vomiting, respiratory depression, hypotension, and ODI score between the MTLIP and TLIP groups (all P>0.05) (Table 5).
 |
Table 5 Comparison of Postoperative Adverse Reactions and ODI Scores Before and 3 Months After Operation Between the Two Groups |
Discussion
This non-inferiority trial supports the hypothesis that MTLIP yields a non-inferior effective dermatomal block area compared with TLIP for Tianji robot-assisted lumbar internal fixation.
Nowadays, enhanced recovery after surgery (ERAS) is the medical community consensus for managing postoperative patients.20 It puts forward a series of optimization measures to reduce postoperative complications and accelerate the speed of recovery and rehabilitation.20 Eltaher et al21 found that TLIP combined with general anesthesia can make the hemodynamics of patients more stable during operation, achieve good postoperative pain control, and reduce potential postoperative complications. Therefore, ultrasound-guided TLIP is an important part of modern spinal surgery, but data about nerve blocks for Tianji robot-assisted lumbar internal fixation is very scarce. A retrospective study by Morgenstern et al22 suggested that TLIP block can significantly improve the prognosis of patients undergoing lumbar interbody fusion through intervertebral foramen without needing opioids after the operation. The study by Ye et al23 showed that TLIP block was superior to wound infiltration regarding opioid consumption. Hu et al24 conducted a meta-analysis that proved that applying TLIP in postoperative analgesia for lumbar surgery is effective.
This study was a non-inferiority trial of TLIP and MTLIP applied to Tianji robot-assisted lumbar internal fixation. The dermatomal block area of MTLIP at 30 min was not lower than that of TLIP, although this result cannot determine the quality of the analgesic effect of these two blocking methods. However, there were no differences in the use of sufentanil and remifentanil during operation, sufentanil in PCIA after the operation, and parecoxib rescue, and there were no differences in static and dynamic NRS scores at 2, 8, 12, and 24 h after the operation. Most patients after posterior lumbar surgery have a large demand for analgesics within 24 h after operation.25 A retrospective analysis by Kurnutala et al26 concluded that an ERAS protocol in patients undergoing lumbar surgery under regional anesthesia with MTLIP for lumbar laminectomy led to a significant reduction in opioid administration for lumbar laminectomy and spinal fusion. Ekinci et al27 showed that MTLIP could provide effective analgesia in the first 24 h after lumbar disc surgery and replace wound infiltration for pain management. Ciftci et al28 believed that ultrasound-guided vertical spinal muscle block (ESPB) and MTLIP can effectively control pain after discectomy, but there was a non-optimality between the ESPB and MTLIP groups. Their findings also suggested that MTLIP can indeed be used for lumbar surgery analgesia, but there was no comparison with TLIP in terms of blocking effect, so it is impossible to confirm the difference of blocking effect between the two blocking methods.
Bicak et al29 suggested that the application of MTLIP block for postoperative analgesia was not better than local anesthetic infiltration, but their baseline data were uneven; the operation time of MTLIP was longer than that of the incision analgesia group, and the VAS scores at 1, 4, and 8 h after operation were significantly smaller than that of the incision analgesia group, which was not enough to prove that the analgesic effect of MTLIP was not due to local anesthetic infiltration. Ozmen et al30 reported that the postoperative pain score, opioid consumption, and QoR-40 value of MTLIP were better than for TLIP, while the present study confirmed that there were no significant differences in analgesic effect between the two methods. The purpose of the two methods was to block the posterior branch of the spinal nerve, which will be further discussed in an autopsy study to be carried out later.
In addition, the puncture time of MTLIP was significantly shorter than that of TLIP, and the puncture times of MTLIP were also significantly less than that of TLIP. The image quality of MTLIP on ultrasound was better than that of the TLIP group, which is similar to the results by Ciftci et al,31 which might be due to the superficial position of the fascia space between the longissimus muscle and the iliac costal muscle, which is farther away from the vertebral body and is highlighted under ultrasound. At the same time, this study also confirmed that the target area recognition of MTLIP was higher because the imaging of the vertebral body, muscle, and fascia adjacent to the iliac costal and longissimus muscles was very clear, with stronger visibility and easier positioning.31 Kim et al32 showed that a shorter operation time could increase patient satisfaction and reduce anxiety, while faster puncture speed and fewer puncture times might improve the satisfaction score, which is consistent with the results of this study.
The puncture site of TLIP is deep, and the ultrasound recognition is not high, which is easy to injure the muscles and nerves by mistake, and even carries the risk of entering the spinal canal by mistake. Therefore, the puncture of TLIP under ultrasound guidance is difficult and risky, and the target area is not clear, resulting in repeated puncture, which is also easy to reduce the patient’s satisfaction or even lead to intolerance or rejection of nerve block. The puncture target of ultrasound-guided MTLIP is changed from multifidus muscle and longissimus muscle to between iliac costus and longissimus muscles, and the puncture direction is changed from inside to outside. Nevertheless, there was no difference in nerve block-related complications between the two blocking methods in this study. It may be that the operating anesthesiologists in this study were experts skilled in the two blocking methods, or it might be due to the small sample size of this study. In the follow-up, it will be necessary to increase the sample size to evaluate whether the improved thoracolumbar fascia plane block under ultrasound guidance is safer.
Although the best nerve block scheme for Tianji robot-assisted lumbar internal fixation analgesia has not been determined, ultrasound-guided MTLIP can provide a 30 min dermatomal block area that is not inferior to TLIP. There were no differences between NRS scores at rest and when moving within 24 h between the two groups, but the NRS scores increased in the two groups over 24 h, indicating no differences between the two methods but that the blocking effect disappeared with time. If the block time is prolonged, it might be necessary to perform a continuous block with indwelling a catheter in the target area.
Li et al33 suggested that MTLIP might be safer to perform than TLIP, but there were no significant differences in the incidence of complications related to the two nerve block methods and complications after general anesthesia in the present study. There were no significant differences in ODI index between the two groups before and 3 months after the operation, suggesting that ultrasound-guided MTLIP did not increase the risk of complications related to nerve block and general anesthesia compared with TLIP. It had no adverse effects on the surgical effect of Tianji robot-assisted lumbar internal fixation.
This study had some limitations. Measuring a dermatomal block may not reflect analgesia, in our follow-up study, we also need to carry out autopsy study to identify the nerves infiltrated by these two types of nerve blocks.The duration of a single nerve was limited, and the postoperative analgesic effect was not as good as a continuous nerve block. Continuous improved thoracolumbar interfascial block for perioperative analgesia in posterior lumbar decompression and fusion surgery needs further study. Meanwhile, the current perioperative analgesia was mainly multi-mode analgesia. Multi-mode analgesia based on improved thoracolumbar interfascial block guided by continuous ultrasound needs further study.
Conclusion
Compared with TLIP, MTLIP provides a non-inferior dermatomal block range, reduces operation time, and improves patient satisfaction. It can effectively inhibit the perioperative pain of Tianji robot-assisted lumbar internal fixation. MTLIP is simple, has high patient satisfaction, a low incidence of related complications, and high safety. It is an optimized analgesic method for Tianji robot-assisted lumbar internal fixation.
Data Sharing Statement
All the processed data were included in the current study. If reviewers or readers have any questions regarding our published data, they can contact the corresponding author [e-mail, [email protected]] for access to the original data.
Ethics Approval
The protocol was approved by the Research Ethics Committee of Second Affiliated Hospital of Jiaxing University. (The approval number:JXEY-2019YJ004).
Acknowledgments
We thank all the researchers and the subjects.
Funding
This work was supported by grants from the Zhejiang Medical and Health Science and Technology Plan (2022ZH013), and the Open Project Program of Jiaxing Key Laboratory of Basic Research and Clinical Transformation of Perioperative Precision Anesthesia (JXMZKL2022B01).
Disclosure
The authors report no conflicts of interest.
References
1. Alfieri A, Gazzeri R, Prell J, Röllinghoff M. The current management of lumbar spondylolisthesis. J Neurosurg Sci. 2013;57(2):103–113.
2. McCarthy J, Davis A. Diagnosis and management of vertebral compression fractures. Am Fam Physician. 2016;94(1):44–50.
3. Kreiner DS, Shaffer WO, Baisden JL, et al. An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spinal stenosis (update). Spine J. 2013;13(7):734–743. doi:10.1016/j.spinee.2012.11.059
4. Zhang TT, Wang ZP, Wang ZH, et al. [Clinical application of Orthopedic Tianji Robot in surgical treatment of thoracolumbar fracture]. Zhongguo Gu Shang. 2021;34(11):1034–1039. doi:10.12200/j.issn.1003-0034.2021.11.010
5. Costantini R, Affaitati G, Fabrizio A, Giamberardino MA. Controlling pain in the post-operative setting. Int J Clin Pharmacol Ther. 2011;49(2):116–127. doi:10.5414/cp201401
6. Loizides S, Gurusamy KS, Nagendran M, Rossi M, Guerrini GP, Davidson BR. Wound infiltration with local anaesthetic agents for laparoscopic cholecystectomy. Cochrane Database Syst Rev. 2014;(3):CD007049. doi:10.1002/14651858.CD007049.pub2
7. Ramirez MA, Ramirez JM, Murthi AM. Multimodal local infiltration analgesia in total shoulder replacement. Pain Manag. 2013;3(4):253–255. doi:10.2217/pmt.13.17
8. Jitpakdee T, Mandee S. Strategies for preventing side effects of systemic opioid in postoperative pediatric patients. Paediatr Anaesth. 2014;24(6):561–568. doi:10.1111/pan.12420
9. Kehlet H, Holte K. Effect of postoperative analgesia on surgical outcome. Br J Anaesth. 2001;87(1):62–72. doi:10.1093/bja/87.1.62
10. Kjærgaard M, Møiniche S, Olsen KS. Wound infiltration with local anesthetics for post-operative pain relief in lumbar spine surgery: a systematic review. Acta Anaesthesiol Scand. 2012;56(3):282–290. doi:10.1111/j.1399-6576.2011.02629.x
11. Schenk MR, Putzier M, Kügler B, et al. Postoperative analgesia after major spine surgery: patient-controlled epidural analgesia versus patient-controlled intravenous analgesia. Anesth Analg. 2006;103(5):1311–1317. doi:10.1213/01.ane/0000247966.49492.72
12. Gessler F, Mutlak H, Tizi K, et al. Postoperative patient-controlled epidural analgesia in patients with spondylodiscitis and posterior spinal fusion surgery. J Neurosurg Spine. 2016;24(6):965–970. doi:10.3171/2015.8.SPINE15415
13. Park SY, An HS, Lee SH, Suh SW, Kim JL, Yoon SJ. A prospective randomized comparative study of postoperative pain control using an epidural catheter in patients undergoing posterior lumbar interbody fusion. Eur Spine J. 2016;25(5):1601–1607. doi:10.1007/s00586-016-4385-8
14. Hand WR, Taylor JM, Harvey NR, et al. Thoracolumbar interfascial plane (TLIP) block: a pilot study in volunteers. Can J Anaesth. 2015;62(11):1196–1200. doi:10.1007/s12630-015-0431-y
15. Ahiskalioglu A, Yayik AM, Alici HA. Ultrasound-guided lateral thoracolumbar interfascial plane (TLIP) block: description of new modified technique. J Clin Anesth. 2017;40:62. doi:10.1016/j.jclinane.2017.04.015
16. Farag E, Seif J. Thoracolumbar interfascial block (TLIP): a new technique of interfascial plane blocks. J Clin Anesth. 2020;61:109640. doi:10.1016/j.jclinane.2019.109640
17. Karmakar MK, Li JW, Kwok WH, Hadzic A. Ultrasound-guided lumbar plexus block using a transverse scan through the lumbar intertransverse space: a prospective case series. Reg Anesth Pain Med. 2015;40(1):75–81. doi:10.1097/AAP.0000000000000168
18. Thong ISK, Jensen MP, Miró J, Tan G. The validity of pain intensity measures: what do the NRS, VAS, VRS, and FPS-R measure? Scand J Pain. 2018;18(1):99–107. doi:10.1515/sjpain-2018-0012
19. Arpinar VE, Gliedt JA, King JA, Maiman DJ, Muftuler LT. Oswestry Disability Index scores correlate with MRI measurements in degenerating intervertebral discs and endplates. Eur J Pain. 2020;24(2):346–353. doi:10.1002/ejp.1490
20. Brindle M, Nelson G, Lobo DN, Ljungqvist O, Gustafsson UO. Recommendations from the ERAS® Society for standards for the development of enhanced recovery after surgery guidelines. BJS Open. 2020;4(1):157–163. doi:10.1002/bjs5.50238
21. Eltaher E, Nasr N, Abuelnaga ME, Elgawish Y. Effect of ultrasound-guided thoracolumbar interfascial plane block on the analgesic requirements in patients undergoing lumbar spine surgery under general anesthesia: a randomized controlled trial. J Pain Res. 2021;14:3465–3474. doi:10.2147/JPR.S329158
22. Morgenstern C, Ramírez-Paesano C, Juanola Galcerán A, Morgenstern R. Thoracolumbar interfascial plane block results in opioid-free postoperative recovery after percutaneous/endoscopic transforaminal lumbar interbody fusion surgery. World Neurosurg. 2021;153:e473–e480. doi:10.1016/j.wneu.2021.06.152
23. Ye Y, Bi Y, Ma J, Liu B. Thoracolumbar interfascial plane block for postoperative analgesia in spine surgery: a systematic review and meta-analysis. PLoS One. 2021;16(5):e0251980. doi:10.1371/journal.pone.0251980
24. Hu Z, Han J, Jiao B, et al. Efficacy of thoracolumbar interfascial plane block for postoperative analgesia in lumbar spine surgery: a meta-analysis of randomized clinical trials. Pain Physician. 2021;24(7):E1085–E1097.
25. Bajwa SJ, Haldar R. Pain management following spinal surgeries: an appraisal of the available options. J Craniovertebr Junction Spine. 2015;6(3):105–110. doi:10.4103/0974-8237.161589
26. Kurnutala LN, Dibble JE, Kinthala S, Tucci MA. Enhanced recovery after surgery protocol for lumbar spinal surgery with regional anesthesia: a retrospective review. Cureus. 2021;13(9):e18016. doi:10.7759/cureus.18016
27. Ekinci M, Çiftçi B, Çelik EC, Yayık AM, Tahta A, Atalay YO. A comparison of the ultrasound-guided modified-thoracolumbar interfascial plane block and wound infiltration for postoperative pain management in lumbar spinal surgery patients. Lomber spinal cerrahi yapılan hastalarda postoperatif analjezi yönetimi için ultrason eşliğinde yapılan modifiye-torakolomber interfasiyal plan bloğu ve yara yeri infiltrasyonunun karşılaştırılması: prospektif, randomize çalışma. Agri. 2020;32(3):140–146. doi:10.14744/agri.2019.97759
28. Ciftci B, Ekinci M, Celik EC, Yayik AM, Aydin ME, Ahiskalioglu A. Ultrasound-guided erector spinae plane block versus modified-thoracolumbar interfascial plane block for lumbar discectomy surgery: a randomized, controlled study. World Neurosurg. 2020;144:e849–e855. doi:10.1016/j.wneu.2020.09.077
29. Bicak M, Aktas U, Salik F, Akelma H, Bicak EA, Kaya S. Comparison of thoracolumbar interfascial plane block with the application of local anesthesia in the management of postoperative pain in patients with lumbar disc surgery. Turk Neurosurg. 2021;31(5):757–762. doi:10.5137/1019-5149.JTN.33017-20.2
30. Ozmen O, Ince I, Aksoy M, Dostbil A, Atalay C, Kasali K. The effect of the modified thoracolumbar interfacial nerve plane block on postoperative analgesia and healing quality in patients undergoing lumbar disk surgery: a prospective, randomized study. Medeni Med J. 2019;34(4):340–345. doi:10.5222/MMJ.2019.36776
31. Çiftçi B, Ekinci M. A prospective and randomized trial comparing modified and classical techniques of ultrasound-guided thoracolumbar interfascial plane block. Ultrason eşliğinde yapılan torakolomber interfasiyal plan bloğunun klasik ve modifiye tekniklerini karşılaştıran prospektif ve randomize çalışma. Agri. 2020;32(4):186–192. doi:10.14744/agri.2020.72325
32. Kim KT, Cho DC, Sung JK, et al. Intraoperative systemic infusion of lidocaine reduces postoperative pain after lumbar surgery: a double-blinded, randomized, placebo-controlled clinical trial. Spine J. 2014;14(8):1559–1566. doi:10.1016/j.spinee.2013.09.031
33. Li C, Jia J, Qin Z, Tang Z. The use of ultrasound-guided modified thoracolumbar interfascial plane (TLIP) block for multi-level lumbar spinal surgery. J Clin Anesth. 2018;46:49–51. doi:10.1016/j.jclinane.2018.01.018
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.