Back to Journals » Veterinary Medicine: Research and Reports » Volume 10
Trigeminal-mediated headshaking in horses: prevalence, impact, and management strategies
Authors Roberts V
Received 13 August 2018
Accepted for publication 16 November 2018
Published 9 January 2019 Volume 2019:10 Pages 1—8
DOI https://doi.org/10.2147/VMRR.S163805
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Young Lyoo
Veronica Roberts
Bristol Vet School, Faculty of Health Sciences, University of Bristol, Langford, North Somerset BS40 5HB, UK
Abstract: Trigeminal-mediated headshaking is a little-understood neuropathic facial pain condition of the horse. The condition may affect around 1% of the equine population to a degree of severity sufficient to require veterinary attention. As a pain condition, this represents a significant welfare issue. Horses are usually more severely affected at exercise which can leave them unable to perform, or even dangerous to ride and handle. With little known about the condition and variable response to treatments, severely affected horses are often euthanized. This review article considers the literature on trigeminal-mediated headshaking, focusing on what is known, and indeed not known, about the prevalence of the condition and its impact. The current published management options are considered, along with their challenges and limitations.
Keywords: neurology, neurological disorder, neuropathic pain, facial pain, welfare
Introduction
Occasional shaking of the head is a normal equine behavior. However, where the headshaking is any or all of frequent, violent, accompanied by flicks or jerks of the head, accompanied by signs of nasal irritation (such as snorting, sneezing, rubbing the nose, striking the nose), accompanied by signs of distress, or affects riding or handling the horse, then a pathological process must be considered.1 Conditions which can cause headshaking may include ear mite infestation, otitis interna, cranial nerve dysfunction, cervical injury, ocular disease, guttural pouch mycosis, dental periapical osteitis,2 protozoal myeloencephalitis,3 and sinusitis4 as well as a behavioral or rider issue.1 However, where shaking was such that referral veterinary advice was required, there was a 98% chance that no physical cause could be determined, leading to a diagnosis of idiopathic headshaking.2 As knowledge of this condition has developed, it is likely that most of these horses were suffering what is now termed trigeminal-mediated headshaking.1
Trigeminal-mediated headshaking appears to be an acquired disorder of the horse. Clinical signs are usually of predominantly vertical headshaking, which may be violent.1 These movements are often accompanied by sharp vertical flicks and signs of nasal irritation.2 Typically, signs are worst at exercise,2,5,6 with only some horses being affected at rest also. Seasonality of clinical signs is usually reported in ~60% of headshaking horses, with the majority of these being spring/summer affected,5,7 although a more recent study found that owner’s reported horses were only completely free of signs seasonally in 25% cases (unpublished data). Even in nonseasonally affected horses, signs may vary with an apparent correlation to weather conditions.2,5,7
The clinical signs of trigeminal-mediated headshaking are consistent with neuropathic pain of the trigeminal nerve. Although this was suspected even in the 19th century,8,9 there have been many other theories, with trigeminal involvement being only recently confirmed.10,11 These studies demonstrated that the infraorbital branch of the trigeminal nerve of affected horses was sensitized, with a lower threshold for activation than unaffected horses. Somatosensory-evoked potentials were recorded under general anesthesia. These determined the threshold for activation for control horses to be >10 mA, but <5 mA for affected horses. There were no differences in the neurophysiological characteristics of the action potentials. Additionally, there were no differences between left and right sides, consistent with bilateral involvement of the trigeminal nerve. One seasonally affected horse was tested out of season and returned normal threshold activations, but was not tested when showing clinical signs, to see if then, threshold was abnormal. Should clinical signs be shown to change as threshold changes, then not only would that confirm causation but also suggest a potentially reversible condition. Further work is required in this area.
The reason for the sensitization of the trigeminal nerve remains unknown. While herpes virus is involved in the pathogenesis of some human neuropathic pain syndromes, the virus was not involved in the pathogenesis of trigeminal-mediated headshaking.12 While trigeminal nerve root demyelination is the most frequent cause of trigeminal neuralgia, a neuropathic facial pain syndrome in people,13 no histopathological abnormality of the nerve has been discovered.14 Despite the apparent clinical similarities between trigeminal neuralgia and trigeminal-mediated headshaking, this result was not inconsistent with signs as human trigeminal neuralgia sufferers are usually unilaterally affected and would have abnormal conduction patterns.13 It can be considered to be a potentially positive result, as this condition would be less likely to be reversible. The results of these studies suggest a functional, rather than structural abnormality of the nerve, leading to the potential for developing a treatment which reverses the functional abnormality.
This summarizes the limited current knowledge of the causes and mechanisms of trigeminal-mediated headshaking. Advances in treatment for trigeminal-mediated headshaking will remain limited until more is understood of the etiopathogenesis of the condition. There may be more than one cause with the same clinical manifestation, leading to different response rates to treatment. It is recognized in human medicine that response to treatment for neuropathic pain varies among individuals, even with the same diagnosis.32 Therefore, even if all trigeminal-mediated headshakers have the same underlying condition, response to the same treatment may vary.
It is against this challenging background that this article considers the prevalence, impact, and current management strategies for trigeminal-mediated headshaking. There is a need for further research into this condition to allow progression in treatment and even prevention. Establishing prevalence and welfare and economic impacts contributes to determining research priority for this condition, as does an understanding of the limited success of current treatments. This review considers and consolidates the current literature in these areas.
Prevalence
Knowledge of the prevalence of headshaking in the worldwide population is fundamental to understanding the scale of the welfare issue that is trigeminal-mediated headshaking. While there are reports of horses with signs consistent with trigeminal-mediated headshaking from many developed countries, only the UK horse population has been used for prevalence studies. There may be a complex interaction with environment in this acquired condition of unknown etiology. For this reason, further information as to whether there is a difference in prevalence between countries, and in particular between developed and developing countries, would be of interest.
The prevalence of headshaking in the UK equine population was first reported by Slater33 in 2013 as part of a general equine health survey. The prevalence of horses reported to have shaken their heads on a particular day of the year was reported to be between 1% and 1.5%. A dedicated study into the prevalence of headshaking in the UK equine population was published in 2018.15 Owners reported that 4.6% of their horses had shaken their heads in the last year, with 6.2% at any time point since ownership was considered. However, veterinary advice was required in only 30% of these horses. This suggests that medically significant headshaking can be expected to affect some 2% of UK horses. Assuming an approximate UK horse population of about one million31 then some 20,000 of those horses could be suffering from significant neuropathic facial pain.
The study by Ross et al15 did not identify an association of sex or breed but median age was 12 years. There are further studies considering signalment. From this, it appears that the condition usually affects the adult horses first in the prime of their lives, with median ages of onset varying from 67 to 10 years.16 Geldings appear to be overrepresented, comprising 63%7 to 71.5%5 cases. All breeds appear susceptible7 (V Roberts, University of Bristol, personal communication, June, 2018). There are no longitudinal studies following disease progression, although there is a suggestion that some 5% of horses may enter spontaneous long-term remission.5
While trigeminal neuropathy is recognized in small animals, there appears to be limited clinical overlap with trigeminal-mediated headshaking. To the author’s knowledge, there are only isolated anecdotal reports of clinical signs consistent with trigeminal-mediated headshaking, without investigation, in zebra and donkeys (V Roberts, personal communication, June, 2012). There may be potential to explore why horses might be affected but other Equidae not or rarely so, as this could potentially give some information as to etiology.
Impact
Impact encompasses morbidity, mortality, and economic burden.34 For trigeminal-mediated headshaking, this requires consideration of welfare and economic effects of the condition on the individual horse, the individual owner, and the equine industry as a whole. The potential for translational research should also be considered.
Horses suffering trigeminal-mediated headshaking are considered to have a neuropathic facial pain condition, and presence of pain has a negative impact on welfare. The degree of this negative impact can arguably be assumed to correlate with the severity of pain. Human patients with neuropathic pain may report signs varying from tingling up to unbearable electric shock-like pain, with quality of life significantly reduced with increasing pain.17 Severity of clinical signs in horses are likely to be our best indicator of severity of pain and severity of headshaking signs commonly vary between and within individuals. A variety of grading systems have been used to quantify severity of headshaking signs.6,18,19 The system used by Talbot focuses mostly on the effect of signs on the horse’s behavior, that by Roberts on the utility of the horse to the owner, and that by Newton is a combination (Table 1). An agreed methodology could be useful for more accurate monitoring of disease progression, treatment efficacy, and comparison of published studies,1 although incorporating both a horse and owner perspective may be of use. It could be inferred that disease of a severity such that horses meet grade 1/5 on Newton’s scale, 1/3 on Talbot’s scale, and 1/3 on Roberts’ scale has minimal impact on welfare and utility to the owner, and therefore minimal economic impact to the equine industry. Significant welfare and economic impact could be expected at the higher grades, with horses being retired or even euthanized if they cannot perform in their intended discipline. Of note are horses which would be classified as 3/3 on Roberts’ scale. These horses suffer even at rest and so can have no respite. For these horses, even retirement is not an option, which may leave only euthanasia if treatment options fail.
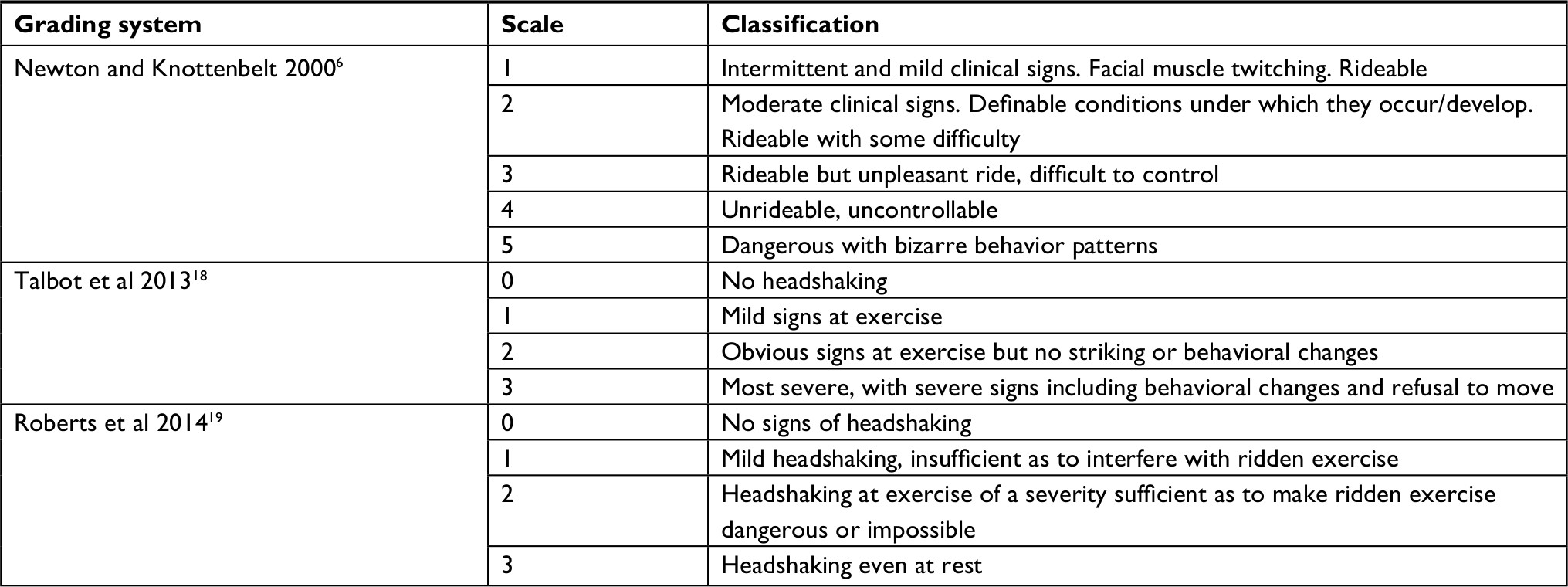 | Table 1 Grading systems |
There is at present no data considering the proportions of affected horses meeting each grading classification. These data would allow us to better assess scale of impact, by calculating the proportion of horses with significant welfare compromise, those retired and euthanized and from that, the cost of wastage to the equine industry.
There is potential for translational research, with clinical similarities being present between trigeminal-mediated headshakers and people suffering neuropathic pain. This potential may, however, be limited, as there does not appear to be an exact parallel condition between people and horses. Trigeminal neuralgia is a neuropathic facial pain condition in people, usually sudden in onset in late middle age and affecting a greater proportion of women.20 Sufferers usually report repeated paroxysms of unilateral facial pain, varying from tingling, through “pins and needles” to unbearable electric-shock pain. Episodes may be triggered by certain actions, such as light touch to the face. Causes of trigeminal neuralgia can be considered to fall into five categories, with the greatest proportion of cases being a result of unilateral focal demyelination at the trigeminal nerve root.13 There are obvious clinical differences with trigeminal-mediated headshakers, where geldings are more commonly affected and signs are bilateral. These differences were supported by one of the researchers working with this author,14 where no demyelination was identified at the trigeminal nerve root of trigeminal-mediated headshakers. Another cause of trigeminal neuralgia in people and of postherpetic neuralgia is latent infection of herpes virus in the trigeminal ganglia. However, no evidence for an association with latent equine herpes virus-1 has been identified in horses.12 A small amount of work has also been published on the use of electroacupuncture in horses presumed to be trigeminal-mediated headshakers.21 There has been more extensive recent work in trigeminal-mediated headshakers, into the use of neuromodulation22 and (Roberts et al, unpublished data) using percutaneous electrical nerve stimulation which is used for the management of neuropathic pain in people. Very little is known about neuromodulation, and there is potential to expand this work using horses to improve our knowledge, which could impact on the management of neuropathic pain in people. Otherwise, determining the etiology of trigeminal-mediated headshaking may open more doors for translational research.
Management strategies
With trigeminal-mediated headshaking neither the pathology nor the cause of the condition is known, presenting the greatest challenge to finding effective treatment. It is possible that there is more than one cause with the same clinical manifestation, leading to different response rates to treatment. It is recognized in human medicine that response to treatment for neuropathic pain varies among individuals, even with the same diagnosis.32 Therefore, even if all trigeminal-mediated headshakers have the same underlying condition, response to the same treatment may vary.
To review the literature surrounding management strategies, reliability of diagnosis, the mechanism of assessment of response used, and the placebo effect must be considered. Assessment of response to treatment can be challenging. Horses can vary from day to day and season to season in the severity of their signs and interpretation of these signs is heavily influenced by the placebo effect.18,23 The most objective measure currently available is classification of success as being return to ridden work at the previous level.22 Should data consistently demonstrate sensitization of the infraorbital in trigeminal-mediated headshakers, the next stage for research would be to determine whether the horses judged to have trigeminal-mediated headshaking responded to treatment, and threshold potentials have returned to normal. This could allow measurement of threshold potentials before and after treatment to give an objective measure of response to treatment. However, the procedure requires general anesthesia which may limit its practical application.1
Diagnosis of trigeminal-mediated headshaking is currently made by exclusion, allowing potential for misdiagnosis. Some papers’ populations rely mostly on interpretation of clinical signs and even owner-led diagnosis. Again, further work demonstrating consistency of lowered infraorbital nerve threshold potentials could allow for this to be the gold standard for diagnosis but would always be limited by the requirement for general anesthesia. It would still be important to show there was no gross pathology leading to sensitization to complete a diagnosis.
There is a considerable placebo effect when interpreting results of treatments for headshaking.18,23 Where possible, trials of treatments for headshaking should include placebo or control group. However, this is not always possible due to welfare considerations in a group of horses suffering a painful condition.
This review will consider published treatments. There are many unpublished treatments used by owners of headshakers (Roberts et al 2018, unpublished data). Assessment of efficacy of unpublished treatments is particularly challenging; it is not known if a veterinary diagnosis was made, or whether the criteria for success are sufficiently robust as to compensate for placebo effect of the owner. Without published data, they are not further considered in this review. Published treatments are best considered in two categories: scientifically proved treatments and those with no effective results, even with apparent placebo effect.
The recent advances suggesting possibly reversible sensitization, may give opportunity for advance in therapy, although these remain limited and early in their inception. The rationale behind more established therapies with some evidence of success appears to reduce sensory input from the trigeminal nerve, intended or not, even before sensitization was shown to occur.
Scientifically proven treatments
Nose net
This, shown in Figure 1, is the first treatment to try as it is cheap, noninvasive, risk-free, and is allowed in most competition at most levels. It is reported to give up to 70% relief in 25% cases.6 The mechanism by which a nose net may work is likely to be similar to (but not the same as it does not travel through the spinal cord) gate control theory. This treatment is noninvasive, affordable, and accepted in most by many, but not all, competition regulatory bodies.
 | Figure 1 Horse wearing a nose net. |
Pharmaceuticals
There are drugs available for the treatment of neuropathic pain in people and some of these have been used in trigeminal-mediated headshakers to see if their neuropathic pain could be managed this way. Even in people with neuropathic pain, these drugs have inconsistent results and may confer side effects including drowsiness. A challenge to the efficacy of neuropathic pain is the heterogeneity of the mechanisms of neuropathic pain, and therefore heterogeneity is the best way to target its treatment.24 Of first-line drugs used for neuropathic pain in people, use of gabapentin has been published in the horse25 but not in cases of trigeminal-mediated headshaking, although it is trialed in some cases (personal observation). Gabapentin is an anti-convulsant acting at calcium channels, which are expressed in the spinal cord, and it is this which gives them its analgesic properties; indeed, the number of voltage-gated calcium channels can increase in cases of neuropathic pain.24 Pharmacology and therefore dosing regimen of neuropathic pain pharmaceuticals in the horse is often uncertain, although there is work on gabapentin (Dirikolu et al, 2007).35 Carbemazepine, a sodium-channel blocking anticonvulsant, can be effective to treat some cases of trigeminal neuralgia in people.20 Mechanism of action is again to reduce central nerve conduction. Not all sufferers respond, some respond only for a short-term but even a short-term response can aid diagnosis, and some experience side effects.20 The use of carbamazepine alone, or in combination with cyproheptadine, a centrally acting antihistamine and serotonin antagonist (serotonin plays a role in pain sensation), is published in trigeminal-mediated headshakers.5,6 Results are mixed, and as with people, occasionally a positive response is merely short-term. Some horses may be affected by drowsiness, so there may be a need to consider whether they are safe to ride/handle. It is the author’s interpretation of these results that, as some individuals can respond well, these drugs can be worth trying as long as expectations are managed. It should be noted that use of these medications would not be allowed in competition, and this fact may be sufficient to limit further research in this area.
Homeopathy
About 93.3% owners felt their horses improved following homeopathic treatment of varying regimes, as part of a larger study into homeopathy.26
Sodium cromoglycate eye drops
Stalin et al27 published a short communication where administration of sodium cromoglycate (a mast cell stabilizer) eye drops was effective in three seasonally affected horses, returning them to ridden exercise. This could suggest allergic conjunctivitis as an etiology. Unfortunately, it appears that conventional allergy is not the cause in the majority of headshaking cases and the author has been unable to replicate these results, although trialing treatment is low risk.
Surgery
Bilateral infraorbital neurectomy16 was effective in 3 out of 19 horses with serious side effects being common; however, it was important in that it added to the weight of evidence of involvement of the trigeminal nerve.
Caudal ablation of the infraorbital nerve via coil compression had better results,28,29 with about a 50% success rate in 57 horses but 26% relapsed with a median time of 9 months (range 2 months to 5 years). Most horses developed side effects of nose rubbing which were short-term in most cases but 4 out of 58 were euthanized due to severity or nonresolution of these side effects.
EquiPENS™ neuromodulation
This technique, demonstrated in Figure 2, was translated from percutaneous electrical nerve stimulation neuromodulation, a minimally invasive procedure which can have efficacy for the management of neuropathic pain in people. Potentially, the procedure is effective by normalizing neural function, but no basic science has been performed to investigate the mechanism of action. An initial trial, using an electrical protocol based on humans and an initial three procedure course, was published in 2016.22 This demonstrated that the procedure was possible to perform understanding sedation, had minimal risk of side effects, and returned five of seven horses to ridden work. More recent unpublished data on 168 trigeminal-mediated headshakers receiving EquiPENS™ neuromodulation (530 procedures) have followed this work. The complication rate was 8.8% of procedures. In all but one case, complications were mild and transient, with no self-trauma. Remission of headshaking following the initial course occurred in 53% (72 out of 136) of horses. Median length of time recorded in remission was 9.5 weeks (range 2 days to 156 weeks ongoing). Where signs recurred, most horses went back into remission following future procedures usually for longer time than the previous procedure. No predictors for outcome were determined. Should these data be published, it may suggest that EquiPENS™ neuromodulation, while clearly carrying limitations, is a good first-line treatment for horses which do not respond to a nose net. Refinement of this procedure will remain limited not only until we understand the etiopathogenesis of trigeminal-mediated headshaking but also the mechanism of action of neuromodulation, about which only little is currently known.
 | Figure 2 Horse undergoing EquiPENS™ neuromodulation. |
Electroacupuncture
Electroacupuncture was attempted for the treatment of trigeminal-mediated headshaking, following the initial indication of possible success of EquiPENS™ neuromodulation and resulted in success in a small group of cases.21 As we do not understand the mechanism of action of neuromodulation or electroacupuncture, the only way to make a comparison is to compare the use of a uniform electroacupuncture technique to EquiPENS™ over a similar number of appropriately diagnosed horses.
Treatments with no effective results
Feed supplement
Talbot et al18 published a double-blinded placebo controlled trial of a commercial herbal feed supplement, marketed for treatment of headshaking. There was no real effect of the supplement or the placebo as judged by vets, but there was significant placebo effect of both the supplement and the placebo to the owner, who “felt their horses were improved”. This demonstrates the importance of using as objective a measure of success as is possible.
Gonadotropin-releasing hormone vaccine23
The use of this vaccine was investigated as the condition may be more common in geldings. In a study of 15 horses, there was no actual improvement as judged by vets but again one-third of owners felt their horses improved. Vaccination reactions were reported in 4 out of 15 cases.
Pulsed high-dose dexamethasone
Consistent with the above statement that conventional allergy is not a common cause of trigeminal-mediated headshaking, pulsed high-dose dexamethasone was not effective for treatment.30
Various other treatments
Madigan and Bell5 performed a survey of owners of headshaking horses. While limited by owner-reported diagnosis and outcomes, with success of treatment judged by owner impression of improvement, no treatment – antihistamines, antimicrobials, corticosteroids, NSAIDs, melatonin, chiropractic treatment, acupuncture – stood out as more successful.
Conclusion
Trigeminal-mediated headshaking in horses is a condition with both welfare and economic implications. Further research is required to fully demonstrate proportions of horses affected worldwide and proportions of horses of each degree of severity, which would best indicate overall welfare and economic impact. There is also an absence of longitudinal data which would reveal whether and how the condition may be expected to progress and in what fashion, as well as the proportion of horses which may be expected to experience spontaneous resolution. Without this information, the detailed full scale of the problem to the population is unknown.
Even in the absence of this information, impact of the individual horse and horse owner can be severe, even resulting in the euthanasia of the horse and all that implies to the owner. There is no one safe and effective treatment and even if aiming for management rather than cure, results are variable. While there are advances being made in understanding the condition and in progressing new treatments, major progress is unlikely until the etiopathogenesis is fully understood. In the meantime, the author recommends a thorough investigation to be as sure as possible of diagnosis, followed by logical trials of published treatments. Where horses are affected at rest and do not respond to treatment, euthanasia may be the only humane option.
Acknowledgments
The University of Bristol receives a fee, in majority for use to fund headshaking research, from training other centers in the use of EquiPENS™.
Disclosure
The author reports no conflicts of interest in this work.
References
Pickles K, Madigan J, Aleman M. Idiopathic headshaking: is it still idiopathic? Vet J. 2014;201(1):21–30. | ||
Lane JG, Mair TS. Observations on headshaking in the horse. Equine Vet J. 1987;19(4):331–336. | ||
Moore LA, Johnson PJ, Messer NT, Kline KL, Crump LM, Knibb JR. Management of headshaking in three horses by treatment for protozoal myeloencephalitis. Vet Rec. 1997;141(11):264–267. | ||
Fiske-Jackson AR, Pollock PJ, Witte TH, Woolford L, Perkins JD. Fungal sinusitis resulting in suspected trigeminal neuropathy as a cause of headshaking in five horses. Equine Vet Educ. 2012;24(3):126–133. | ||
Madigan JE, Bell SA. Owner survey of headshaking in horses. J Am Vet Med Assoc. 2001;219(3):334–337. | ||
Newton SA, Knottenbelt DC, Eldridge PR. Headshaking in horses: possible aetiopathogenesis suggested by the results of diagnostic tests and several treatment regimes used in 20 cases. Equine Vet J. 2000;32(3):208–216. | ||
Mills DS, Cook S, Taylor K, Jones B. Analysis of the variations in clinical signs shown by 254 cases of equine headshaking. Vet Rec. 2002;150(8):236–240. | ||
Williams WL. Involuntary twitching of the head relieved by trifacial neurectomy. J Comp Med Vet Arch. 1897;18:426–428. | ||
Williams WL. Involuntary shaking of the head and its treatment by trifacial neurectomy. Am Vet Rev. 1899;23:321–326. | ||
Aleman M, Williams DC, Brosnan RJ, et al. Sensory nerve conduction and somatosensory evoked potentials of the trigeminal nerve in horses with idiopathic headshaking. J Vet Intern Med. 2013;27(6):1571–1580. | ||
Aleman M, Rhodes D, Williams DC, Guedes A, Madigan JE. Sensory evoked potentials of the trigeminal nerve for the diagnosis of idiopathic headshaking in a horse. J Vet Intern Med. 2014;28(1):250–253. | ||
Aleman M, Pickles KJ, Simonek G, Madigan JE. Latent equine herpesvirus-1 in trigeminal ganglia and equine idiopathic headshaking. J Vet Intern Med. 2012;26(1):192–194. | ||
Love S, Coakham HB. Trigeminal neuralgia: pathology and pathogenesis. Brain. 2001;124(Pt 12):2347–2360. | ||
Roberts VL, Fews D, McNamara JM, Love S. Trigeminal nerve root demyelination not seen in six horses diagnosed with trigeminal-mediated headshaking. Front Vet Sci. 2017;15(4):72. | ||
Ross SE, Murray JK, Roberts VLH. Prevalence of headshaking within the equine population in the UK. Equine Vet J. 2018;50(1):73–78. | ||
Mair TS. Assessment of bilateral infra-orbital nerve blockade and bilateral infra-orbital neurectomy in the investigation and treatment of idiopathic headshaking. Equine Vet J. 1999;31(3):262–264. | ||
Dermanovic Dobrota V, Hrabac P, Skegro D, et al. The impact of neuropathic pain and other comorbidities on the quality of life in patients with diabetes. Health Qual Life Outcomes. 2014;12:171. | ||
Talbot WA, Pinchbeck GL, Knottenbelt DC, Graham H, McKane SA. A randomised, blinded, crossover study to assess the efficacy of a feed supplement in alleviating the clinical signs of headshaking in 32 horses. Equine Vet J. 2013;45(3):293–297. | ||
Roberts V. Idiopathic headshaking: is it still idiopathic? Vet J. 2014;201(1):7–8. | ||
Zakrzewska JM, Linskey ME. Trigeminal neuralgia. BMJ Clin Evid. 2014;2014:1207. | ||
Devereux S. Electroacupuncture as an additional treatment for headshaking in six horses. Equine Vet Educ. 2017;27:1–10 | ||
Roberts VL, Patel NK, Tremaine WH. Neuromodulation using percutaneous electrical nerve stimulation for the management of trigeminal-mediated headshaking: a safe procedure resulting in medium-term remission in five of seven horses. Equine Vet J. 2016;48(2):201–204. | ||
Pickles KJ, Berger J, Davies R, Roser J, Madigan JE. Use of a gonadotrophin-releasing hormone vaccine in headshaking horses. Vet Rec. 2011;168(1):19. | ||
Fornasari D. Pharmacotherapy for neuropathic pain: a review. Pain Ther. 2017;6(Suppl 1):25–33. | ||
Davis JL, Posner LP, Elce Y. Gabapentin for the treatment of neuropathic pain in a pregnant horse. J Am Vet Med Assoc. 2007;231(5):755–758. | ||
Mathie RT, Baitson ES, Hansen L, Elliott MF, Hoare J. Homeopathic prescribing for chronic conditions in equine veterinary practice in the UK. Vet Rec. 2010;166(8):234–237. | ||
Stalin CE, Boydell IP, Pike RE. Treatment of seasonal headshaking in three horses with sodium cromoglycate eye drops. Vet Rec. 2008;163(10):305–306. | ||
Roberts VL, McKane SA, Williams A, Knottenbelt DC. Caudal compression of the infraorbital nerve: a novel surgical technique for treatment of idiopathic headshaking and assessment of its efficacy in 24 horses. Equine Vet J. 2009;41(2):165–170. | ||
Roberts VLH, Perkins JD, Skärlina E, et al. Caudal anaesthesia of the infraorbital nerve for diagnosis of idiopathic headshaking and caudal compression of the infraorbital nerve for its treatment, in 58 horses. Equine Vet J. 2013;45(1):107–110. | ||
Tomlinson JE, Neff P, Boston RC, Aceto H, Nolen-Walston RD. Treatment of idiopathic headshaking in horses with pulsed high-dose dexamethasone. J Vet Intern Med. 2013;27(6):1551–1554. | ||
British Equestrian Trade Association. National Equestrian Survey; 2015. Available from: http://www.beta-uk.org/pages/industry-information/market-information.php. Accessed November 30, 2018. | ||
Neuropathic pain in adults: pharmacological management in non-specialist settings Clinical guideline [CG173]; 2013. Available from: https://www.nice.org.uk/guidance/cg173/chapter/1-Recommendations. Accessed April, 2018. | ||
Slater J. National equine health survey; 2013. Available from: http://www.bluecross.org.uk/80135/national-equine-health-survey-html. Accessed November 30, 2018. | ||
World Health Organisation. Guide to identifying the economic consequences of disease and injury; 2018. Available from: http://www.who.int/choice/publications/d_economic_impact_guide.pdf?ua=1. Accessed November 30, 2018. | ||
Dirikolu L, Dafalla A, Ely KJ, Connerly AL, Jones CN, ElkHoly H, Lehner AF, Thompson K, Tobin T. Pharmacokinetics of gabapentin in horses. J Vet Pharmacol Ther. 2008;31(2):175–7. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.