")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Trends in Coprescription Among Taiwanese Children from 2002 to 2012
Authors Tou SI, Lin CL, Huang CY , Yen HR
Received 3 May 2023
Accepted for publication 27 October 2023
Published 29 December 2023 Volume 2023:16 Pages 4307—4320
DOI https://doi.org/10.2147/JMDH.S416892
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sio-Ian Tou,1 Cheng-Li Lin,2,3 Chia-Yu Huang,4,5,* Hung-Rong Yen5– 9,*
1Department of Pediatrics, Chung Kang Branch, Cheng-Ching General Hospital, Taichung, Taiwan; 2Management Office for Health Data, China Medical University Hospital, Taichung, Taiwan; 3College of Medicine, China Medical University, Taichung, Taiwan; 4Department of Family Medicine, Taichung Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Taichung, Taiwan; 5Graduate Institute of Chinese Medicine, School of Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan; 6International Master Program in Acupuncture, College of Chinese Medicine, China Medical University, Taichung, Taiwan; 7Department of Chinese Medicine, China Medical University Hospital, Taichung, Taiwan; 8Research Center for Traditional Chinese Medicine, Department of Medical Research, China Medical University Hospital, Taichung, Taiwan; 9Chinese Medicine Research Center, China Medical University, Taichung, Taiwan
*These authors contributed equally to this work
Correspondence: Hung-Rong Yen, China Medical University, 91 Hsueh-Shih Road, North District, Taichung, 404, Taiwan, Tel +886-4-22053366 ext. 3313, Fax +886-4-22365141, Email [email protected] Chia-Yu Huang, Taichung Tzu Chi Hospital, 88, Sec 1, Fengxing Road, Tanzi Dist, Taichung, 427, Taiwan, Tel +886-4-36060666, Fax +886-4- 36026656, Email [email protected]
Purpose: Coprescription means that patients use different prescription medications at the same time, which can lead to polypharmacy and subsequent complications. In Taiwan, prescriptions can be ordered by Western physicians, traditional Chinese physicians and dentists. It is essential to disclose the trends in coprescription to prevent possible polypharmacy among children.
Patients and Methods: We used the Longitudinal Health Insurance Database 2000 in Taiwan. Children < 18 years old who had coprescription from 2002 to 2012 are included. The odds ratio and 95% confidence interval are estimated by a logistic regression model to evaluate the correlation between basic characteristics and coprescription.
Results: A total of 44,801 children are included in the analysis. The numbers of children with coprescription and the numbers of coprescriptions ordered for children increased with calendar years. Children aged 3– 5 year and 6– 8 years constituted the majority of coprescriptions, while those aged < 3 years constituted the minority of coprescriptions. Compared to those in the Western medication-alone group, aged 3– 5 years and children who lived in central and southern Taiwan are more likely to have coprescription.
Conclusion: Coprescription among Taiwanese children is not uncommon. Healthcare providers, policymakers and parents should be aware of the real coprescription situation among the children.
Keywords: pediatrics, Chinese herbal medicine, polypharmacy, big-data analysis
Introduction
Coprescription means that patients use different prescription medications at the same time, and it can lead to polypharmacy, which is attributed to iatrogenic complications, such as electrolyte imbalance, diarrhea, nausea and conscious change. This topic is well discussed in the context of elderly patients and children because their renal and liver functions are insufficient, leading to potential drug–drug interactions when they have coprescriptions. However, drug–herbal interactions are also noted when patients concurrently used Western medication and local herbal products. In Taiwan, children use Chinese herbal medication (CHM) prescribed by traditional Chinese physicians to treat several types of diseases, including respiratory diseases,1 immunological disorders,2 neurological dysfunction,3 endocrine problems4 and cancers.5
The importance of coprescription is notable when polypharmacy induces drug–drug interactions. Treatment of physiological symptoms is the most common reason to attribute polypharmacy in children. In the United States, polypharmacy was found in 26% of children for controlling chronic musculoskeletal pain during 2000–20136 and 34% of children who needed psychotropic agents from 2012 to 2015; most of them were aged 6–11 years.7 In pediatric intensive care units, 89% and 68.2% children had use ≥5 drugs and ≥10 drugs in a day.8 In general, on average 10 different drugs would be given to children on each admission day.8 The children had with brain tumor are the high-risk group to use polypharmacy in the cancer survivors.9 The prevalence rates of polypharmacy in children have asthma was 33.49%, 15.53% (95%, 12.63% and 5.33%) using 2, 3–4, and 5 medications, respectively.10 Also, the virus could invade respiratory system, such as COVID-19 infection would be found its association with increasing incidence of polypharmacy in children.11 A Korea study report their prevalence of pediatric polypharmacy was 3.7% and medication for respiratory problem, allergic relieving, central nervous system, infection controlling and gastrointestinal discomfort are the major reasons to have polypharmacy.12 These data come from the studies investigating the Western medication. However, in the real-world children and adults concurrently use the Western medication and herbal products.13 Although the prevalence of children taking herbal agents has been investigated, the trends in polypharmacy, including use of herbal products and Western medication, are not as commonly discussed.14
In Taiwan, patients could have prescriptions from three sources, namely, a Western physician,15,16 traditional Chinese physician,17,18 and dentist.19 Since 1995, these medical services have all been reimbursed by the National Health Insurance (NHI) program. More than 99.7% of Taiwanese people are covered by the HNI program, and their medical information is collected into the National Health Insurance Research Database (NHIRD).15,16 On the other hand, the NHIRD is a long-term big-data follow-up tool and is suitable for large-scale investigations that can prevent selection bias.
In 2001, children in Taiwan visited Western physicians, Chinese physicians and dentists 14.55, 0.55, and 1.73 times.20,21 Previous studies disclosed that approximately 2–8% Taiwanese children have used CHM22 and that approximately 5–89% children in Taiwan had visited a dentist for treatment of caries.23 Because coprescription among children is not a rare situation in clinical practice, we aimed to disclose the trends in coprescription among Taiwanese children from three sources of prescriptions: the Western physician, Chinese physician and dentist. Furthermore, basic characteristics, such as age, sex, place of residence and parental financial status, of the children with coprescription are also analyzed.
Materials and Methods
Data Source
We used the Longitudinal Health Insurance Database 2000 (LHID 2000) from the NHIRD which offers the medical records from 2002 to 2012. The LHID 2000 includes a random sample of 1,000,000 subjects out of 23 million beneficiaries of the NHI program in Taiwan.15,16 Through insurance claim records, demographic data, including sex, date of birth, residence, and monthly income, could be extracted from this database. Informed consent from the patient was not necessary because the information from the LHID 2000 was deidentified. All diagnoses in the database are coded according to the International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM).
Study Population
Children are identified from the LHID 2000 and included in the analysis if they met the following inclusion criteria: 1. age <18 years, 2. coprescription from a Western physician (W) and traditional Chinese physician (C), a W and dentist (D), and a C, W and D from 2002 to 2012. The definition of coprescription is children with prescriptions from any two or three of the W, C or D sources and an overlap in prescription use of ≥1 day. When patients have concurrent use W+C+D ≥1 day, they would be included in the W+C+D cohort. If a patient met the criteria of concurrent using W+C and W+D ≥1 day during the follow-up period, the included cohort would be decided depending on the first-time concurrent use is W+C or W+D. When patients did not be moved into the above three cohorts and they meet the criteria of using W alone during 2002–2012 who would be known as W alone cohort. The exclusion criteria are as follows: age ≥18 years, lack of complete data for age and sex, or interruption of health insurance during the follow-up period (Figure 1).
 |
Figure 1 Flowchart of study population selection. A total of 44,801 patients are included: 1,349 patients only used prescriptions from a Western physician (W); 12,259 patients received coprescription from a W and traditional Chinese physician (C); 29,543 patients received coprescription from a W and dentist (D); 1,650 patients received coprescription from a W, C, and D. Abbreviations: W, Western physician; C, traditional Chinese physician; D, dentist; LHID 2000, Longitudinal Health Insurance Database. |
Study Variables
The independent variables are sex, age, region of residence and monthly income. Through the connection of data between children and their parents, we used the monthly income of parents in our study because most children in Taiwan did not have regular income when aged <18 years. Children are categorized into 8 subgroups according to age: ≤1, 1, 2, 3–5, 6–8, 9–11, 12–14 and 15–17 years. Residence in Taiwan is divided into 5 regions: northern Taiwan, central Taiwan, southern Taiwan, eastern Taiwan, and outside islands (Kinmen Islands, Mazu Islands and Penghu Islands). Monthly income (New Taiwan dollar, NTD) is grouped into 3 levels: <20,000, 20,000–39,999 and ≥40,000.
Outcomes Measures
Descriptive statistics are used to present demographic characteristics of children with coprescription. The proportion of children with coprescription, proportion of records of coprescription and proportion of days of coprescription stratified by year are calculated using the number of insured patients in each year, the total number of coprescriptions yearly and the total days of coprescription yearly, respectively. The distributions of sex, age, region of residence and monthly income are presented as the number and percentage in the following four groups: W alone, W+C, W+D and W+C+D. Differences in W+C and W alone, W+D and W alone, and W+C+D and W alone are tested by chi-square tests. The numbers of children and the frequency distributions of the W-alone group and the coprescription W+C, W+D, and W+C+D groups stratified by the major disease categories (ICD-9-CM codes) would be calculated. The numbers of children and the frequency distributions of all participants and the coprescription W+D and W+C+D cohorts stratified by the diagnosis from dentist (ICD-9-CM codes) would be presented, respectively.
Statistical Analysis
The differences of basic characteristics among the 4 cohorts are compared by Pearson chi- squared test and independent Student’s t-test to analyze the descriptive statistics and continuous variables. The demographic characteristics and medical record information are analyzed by SAS statistical software (version 9.4 for Windows; SAS Institute, Inc., Cary, NC, USA). The crude (cOR) and adjusted odds ratio (aOR) with 95% confidence interval (CI) are calculated with a logistic regression model to evaluate the correlation between baseline characteristics and coprescription. The aOR was performed from cOR through correcting sex, age, region and monthly income. Statistical significance was determined using two‐tailed tests (P < 0.05).24
Ethical Considerations
This study was approved by the Research Ethics Committee of China Medical University and Hospital, Taiwan (CMUH104-REC2-115). The NHIRD dataset for this study is encrypted using a random alphanumeric series to protect the privacy of the subjects and adhere to ethical considerations. Research members could not identify any enrollee or facility from the dataset (https://nhird.nhri.org.tw/en/).
Results
A total of 44,801 patients <18 years old with records of prescription ordered by Western physicians are included for the analysis and are included in the noncoprescription group (n = 1,349), W+C group (n = 12,259), W+D group (n = 29,543) and W+C+D group (n = 1,650) (Figure 1). The proportion of children with C increased with year, but the proportion of children with W and D usage remained stable (Figure 2).
 |
Figure 2 The proportions of numbers of children with prescriptions from a W alone indicated by a blue line, C alone indicated by a green line, and D alone indicated by a red line are stratified by year and corrected for the numbers of individuals in the insurance population yearly. Abbreviations: W, Western physician; C, traditional Chinese physician; D, dentist. |
Figure 3A and B show the proportions of numbers of children with coprescription stratified by year and the corrections for the numbers of individuals in each insurance population yearly among the three groups. The trend in the W+C group increased from over 9.03% in 2002 to 10.18% in 2012; that in the W+D group decreased from over 11.48% in 2002 to 8.74% in 2012, and that in the W+C+D group increased from 0.07% in 2002 to over 0.09% in 2012. Supplementary Figure 1A and B shows the proportion of records of coprescriptions stratified by year and corrected for the total number of coprescriptions yearly, and Supplementary Figure 2A and B reveals the proportion of days of coprescription stratified by year and corrected for the total days of prescriptions yearly.
 |
Figure 3 (A) The proportions of numbers of children with prescriptions from W+C group indicated by a green line, and W+D group indicated by a blue line are stratified by year and corrected for the numbers of individuals in the insurance population yearly. (B) The proportions of numbers of children with prescriptions from W+C+D group indicated by a red line are stratified by year and corrected for the numbers of individuals in the insurance population yearly. Abbreviations: W, Western physician; C, traditional Chinese physician; D, dentist. |
The numbers of children with coprescription stratified by age in the three groups are presented in Figure 4A and B. The trend in the W+C group increased from 0 days in the age interval of <1 year to 17,882 days in the age interval of 3–5 years, then decreased to 11,345 days in the age interval of 15–17 years; that in the W+D group increased from 0 days in the age interval of <1 year to 4,694 days in the age interval of 6–8 years, then increased to 1,916 days in the age interval of 12–14 years and increased to 2,301 days in the age interval of 15–17 years; and that in the W+C+D group increased from 0 days in the age interval of <2 years to 142 days in the age interval of 6–8 years, then decreased to 23 days in the age interval of 9–11 years and increased to 68 days in the age interval of 12–14 years, then decreased to 37 days in the age interval of 15–17 years. The numbers of days of coprescription stratified by age and corrected for the number of individuals in each age interval in the three groups are presented in Figure 4C and D. The trend in the W+C group increased from 0 days per person in the age interval of <1 year to 6.5 days per person in the age interval of 2 years then decreased to 2.7 days per person in the age interval of 15–18 years; that in the W+D group increased from 0 days per person in the age interval of <1 year to 0.6 days per person in the age interval of 15–17 years; and that W+C+D group increased from 0 days per person in the age interval of ≤1-year old to 2.7 days per person in the age interval of 3–5 years and decreased to 1.5 days per person in the age interval 9–11-year old, then increased to 3.0 days per person in the age interval 12–14-year old then decreased to 2.1 days per person in the age interval 15–17-year old.
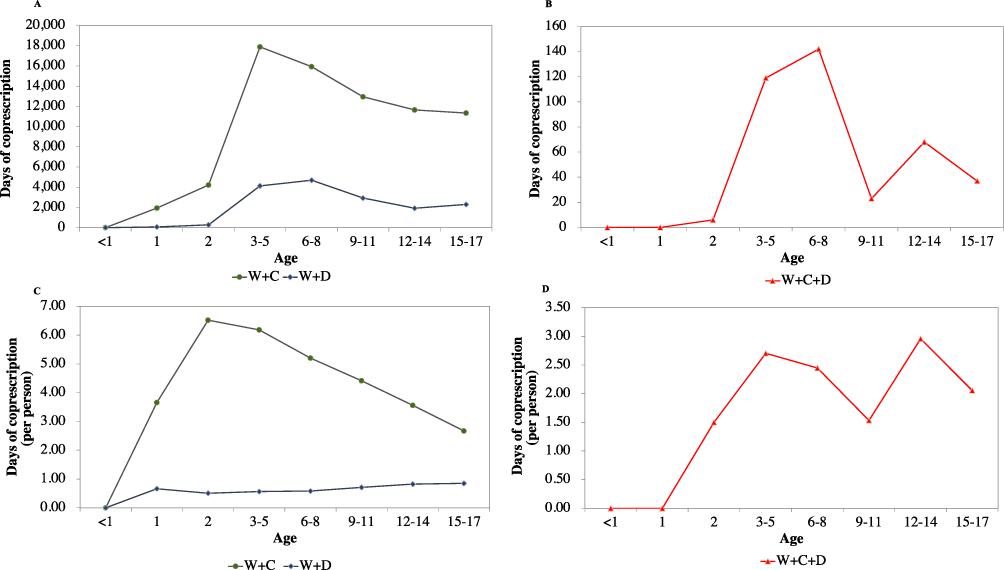 |
Figure 4 (A) The numbers of days of coprescription from W+C group indicated by green line, and W+D group indicated by blue line, and W+C+D group indicated by red line stratified by age. (B) The numbers of days of coprescription from W+C+D group indicated by red line stratified by age. (C) The numbers of days of coprescription from W+C group indicated by green line, and W+D group indicated by blue line, and W+C+ D group indicated by red line stratified by age and corrected for the number of individuals in each age interval. (D) The numbers of days of coprescription from W+C+ D group indicated by blue line stratified by age and corrected for the number of individuals in each age interval. Abbreviations: W, Western physician; C, traditional Chinese physician; D, dentist. |
The numbers of records of coprescription stratified by age in the three groups are presented in Figure 5A and B. The trend in the W+C group increased from 0 in the age interval of <1 year to 13,135 in the age interval of 3–5 years, then decreased to 5,524 in the age interval of 15–17 years; that in the W+D group increased from 0 in the age interval of <1 year to 12,106 in the age interval of 3–5 years, then decreased to 2,934 in the age interval of 12–14 years and increased to 3,505 in the age interval of 15–17 years; and that in W+C+D group increased from 0 in the age interval of <1 year to 59 in the age interval of 6–8 years, then decreased to 15 in the age interval of 9–11 years and increased to 23 in the age interval of 12–14 years, then decreased to 18 in the age interval of 15–17 years. The numbers of records of coprescription stratified by age and corrected for the number of individuals in each age interval in three groups are presented in Figure 5C. The trend in the W+C group decreased from 0 per person in the age interval of <1 year to 3.0 per person in the age interval of 3–5 years then decreased to 1.7 per person in the age interval of 15–17 years; that in the W+D group increased from 0 per person in the age interval of <1 year to 1.7 per person in the age interval of 3–5 years then decreased to 1.3 per person in the age interval of 15–18 years; and that in the W+C+D group increased from 0 per person in the age interval of <1 year to 1.0 per person after the age interval of ≥2 years.
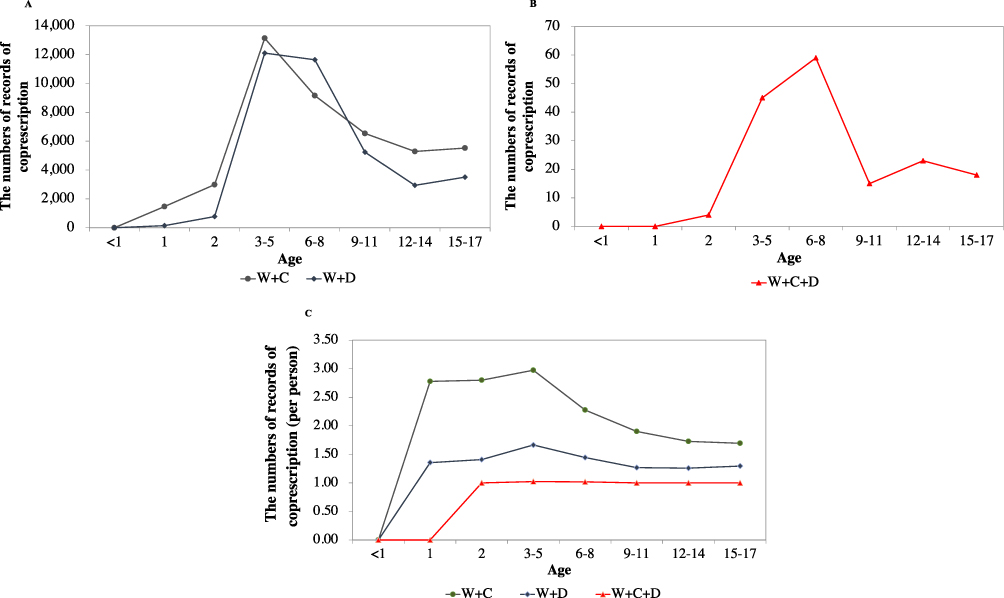 |
Figure 5 (A) The numbers of records of coprescriptions from W+C group indicated by green columns, and W+D group indicated by blue columns, and W+C+D group indicated by red columns are stratified by age. (B) The numbers of records of coprescriptions from W+C+D group indicated by red columns are stratified by age. (C) The numbers of records of coprescriptions from W+C group indicated by green line, W+D group indicated by blue line, and W+C+D group indicated by red line are stratified by age and corrected for the numbers of individuals in each age interval. Abbreviations: W, Western physician; C, traditional Chinese physician; D, dentist. |
The numbers of children with coprescription stratified by age in the three groups are presented in Figure 6A and B. The trend in the W+C group increased from 0 children in the age interval of <1 year to 4,417 children in age interval of 3–5 years, then decreased to 3,059 children in the age interval of 12–14 years and increased to 3,259 children in the age interval of 15–17 years; that in the W+D group increased from 0 children in the age interval of <1 year to 8,063 children in the age interval of 6–8 years, then decreased to 2,329 children in the age interval of 12–14 years and decreased to 2,708 children in the age interval of 15–17 years; and that in the W+C+D group increased from 0 in the age interval of <1 year to 58 children in the age interval of 6–8 years, then decreased to 15 children in the age interval of 9–11 years and increased to 23 in the age interval of 12–14 years then decreased to 18 children in the age interval of 15–17 years. The numbers and percentages of children contributed to Figures 2–6 and Supplementary Figures 1 and 2 are presented in Supplementary Tables 1–7.
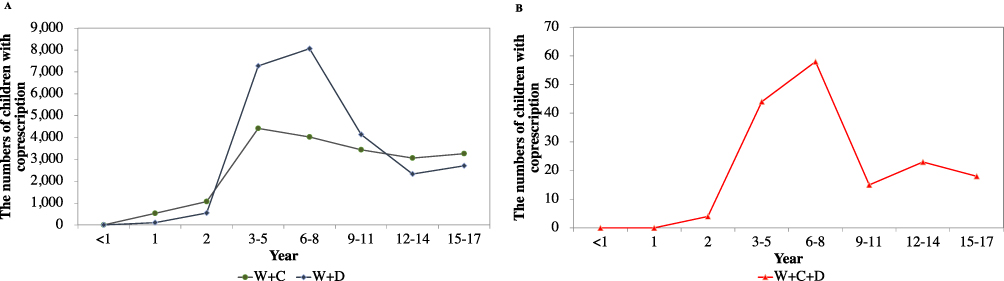 |
Figure 6 (A) The numbers of children with prescriptions from W+C group indicated by green line, and W+D group indicated by blue line are stratified by age. (B) The numbers of children with prescriptions from W+C+D group indicated by a red line are stratified by age. Abbreviations: W, Western physician; C, traditional Chinese physician; D, dentist. |
Table 1 shows the baseline characteristics of the W+C group, W+D group and W+C+D group with distributions of sex, age, regions of residence and parental monthly income that are different from those of the W-alone group. Male children are the predominant group in the coprescription cohorts of W+C and C+W+D. In the W+D coprescription group, female children are predominant. Children aged 6–12 years are the major subgroup to accept coprescription: 23.4% in the W+C group, 40.6% in the W+D group and 50.5% in the W+C+D group. The children who lived in northern Taiwan had a higher opportunity to receive coprescription, and the percentages are 41.8% in the W+C cohort, 51.5% in the W+D cohort and 42.1% in the W+C+D cohort. Parents with a monthly income (NTD) <20,000 had a higher chance of accepting coprescription: 98.3% in the W+C group, 98.4% in the W+D group and 99.1% in the W+C+D group.
 |
Table 1 Baseline Characteristics of Taiwanese Children with Prescriptions from W-Alone Group, and Coprescriptions from W+C Group, W+D Group, and W+C+D Group |
The characteristics associated with the status of coprescription in the W+C group compared with the W-alone group of Taiwanese children are shown in Table 2. Compared to female patients, male patients had a similar adjusted OR (95% CI) for coprescription from W+C sources, at 0.92 (0.90–0.94). Compared to children aged <3 year, those aged 3–5 had higher ORs (95% CI) for coprescription from W+C sources, at 3.38 (1.85–6.19). But there is no difference among children aged <3 year, 6–11, and 12–17 years at 1.07 (0.66, 1.72) and 0.75 (0.47, 1.19), respectively. Compared to children living in Eastern Taiwan+ islands, those living in northern, central and southern Taiwan had higher adjusted ORs (95% CI) for coprescription from W+C sources, at 1.84 (1.40–2.41), 2.46 (1.85–3.27) and 1.91 (1.44–2.52), respectively, and those living in eastern Taiwan had a lower adjusted OR (95% CI) for coprescription from W+C sources, at 0.83 (0.79–0.89). Compared to parents with monthly incomes (NTD) of 20,000–39,999, cohorts with incomes of <20,000 and ≥40,000 had higher and similar adjusted ORs (95% CI) for coprescription from W+C sources, at 12.1 (4.85–30.4) and 2.52 (0.72–8.78), respectively.
 |
Table 2 Adjusted OR and 95% CI for the Characteristics Associated with the Status of Coprescription in the W+C Group Compared with the W-Alone Group of Taiwanese Children |
The characteristics associated with the status of coprescription in the W+D group compared to the W-alone group of Taiwanese children are shown in Table 3. Compared to female patients, male patients had a lower adjusted OR (95% CI) for coprescription from W+D sources, at 0.77 (0.68–0.86). Compared to children aged <3 year, those aged 3–5 and 6–11 had higher ORs (95% CI) for coprescription from W+C sources, at 15.9 (8.80–28.8) and 2.58 (1.62–4.11). However, children aged 12–17 years had a lower OR (95% CI) for coprescription from W+C sources, at 0.50 (0.32–0.79). Compared to children living in northern Taiwan, those living in central Taiwan had higher adjusted ORs (95% CI) for coprescription from W+D sources, at 1.34 (1.16–1.56), and those living in eastern Taiwan+ islands had a lower adjusted OR (95% CI) for coprescription from W+D sources, at 0.54 (0.42–0.71). Compared to parents with monthly incomes (NTD) of 20,000–39,999, groups with incomes of <20,000 and ≥40,000 had higher adjusted ORs (95% CI) for coprescription from W+D sources, at 4.85 (3.44–6.83) and 2.01 (1.19–3.41), respectively.
 |
Table 3 Adjusted OR and 95% CI for the Characteristics Associated with the Status of Coprescription in the W+D Group Compared with the W-Alone Group of Taiwanese Children |
The characteristics associated with the status of coprescription in the W+C+D group compared to the W-alone group of Taiwanese children are shown in Table 4. Compared to female children, the male children had lower similar adjusted OR (95% CI) for coprescription from W+C+D sources, at 0.74 (0.63–0.88). Compared to children aged <3 year, those aged 3–5 and 6–11 years had higher ORs (95% CI) for coprescription from W+C+D sources, at 37.8 (11.8–121.1), and 15.1 (5.03–45.1), respectively, and those aged 12–18 years did not have difference for coprescription from W+C+D sources (P= 0.11). Compared to children living in northern Taiwan, those living in central, southern and eastern Taiwan+ Islands had higher adjusted ORs (95% CI) for coprescription from W+C+D sources, at 4.03 (2.28–7.12), 5.95 (3.33–10.6) and 4.12 (2.31–7.33), respectively. Compared to parents with monthly incomes (NTD) of 20,000–39,999, groups with incomes of <20,000 and ≥40,000 had higher adjusted ORs (95% CI) for coprescription from C+W+D sources, at 12.1 (4.85–30.4) and 2.52 (0.72–8.78), respectively.
 |
Table 4 Adjusted OR and 95% CI for the Characteristics Associated with the Status of Coprescription in the W+C+D Group Compared with the W-Alone Group of Taiwanese Children |
Table 5 presents the numbers of children and the frequency distributions of the W-alone group and the coprescription W+C, W+D, and W+C+D groups stratified by the major disease categories (according to ICD-9-CM codes) in Taiwan. In the W-alone group, diseases of the respiratory system (48.5%), injury and poisoning (12.4%), and diseases of the nervous system and sensory organs (9.93%) are most frequent three major disease categories. In the W+C group, diseases of the respiratory system (55.8%), diseases of the nervous system and sensory organs (9.22%), and injury and poisoning (6.92%) are the most frequent three major disease categories. In the W+D group, diseases of the respiratory system (55.7%), diseases of the nervous system and sensory organs (7.79%), and diseases of the respiratory system (7.70%) are the top three most frequent major disease categories. In the W+C+D group, diseases of the respiratory system (50.8%), diseases of the nervous system and sensory organs (9.82%), and diseases of the skin and subcutaneous tissue (8.97%) are the most frequent major disease categories.
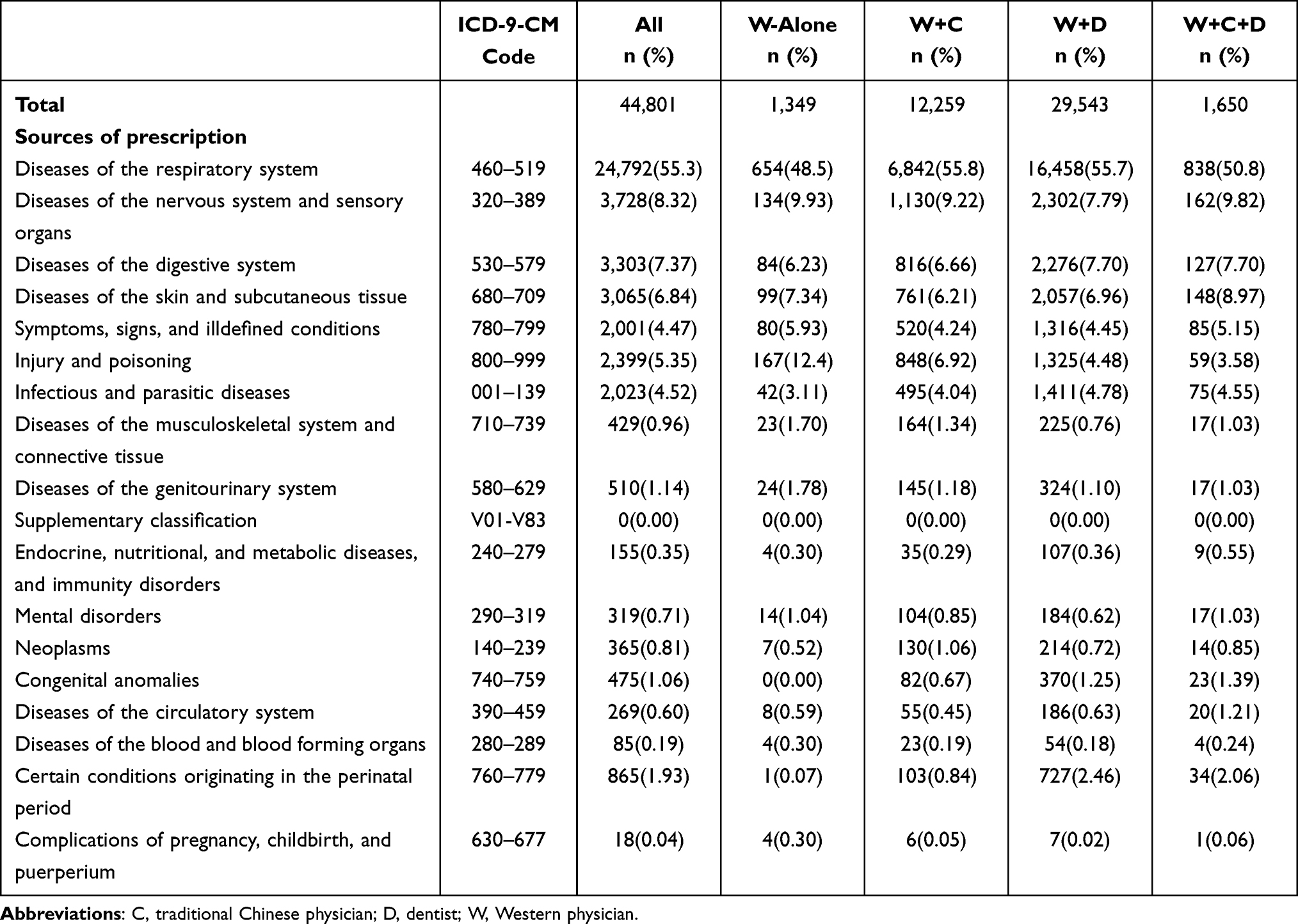 |
Table 5 The Numbers of Children and the Frequency Distributions of the W-Alone Group and the Coprescription W+C, W+D, and W+C+D Groups Stratified by the Major Disease Categories (According to ICD-9-CM Codes) |
Discussion
Our study is the first to reveal the trends in coprescription ordered by Western physicians, traditional Chinese physicians, and dentists among Taiwanese children by big-data analysis. Original prescriptions could be collected completely because of the high health insurance coverage rate in Taiwan.16 Coprescription in children is an important issue because potential risks, such as drug–drug interactions, drug–herbal interactions and polypharmacy, may be increased by coprescription.8,25 Furthermore, concurrent usage of Western medicine and herbal medicine may affect pharmacokinetics and pharmacodynamics. Thus, it is a complicated issue and worthy of investigation.
Herbal medicine is a popular alternative intervention in many countries worldwide, including Taiwan. In the United States and Europe, prescription is not necessary when patients need herbal medicinal products.26,27 A previous study in Jamaica found that the prevalence rates of concurrent use of Western medication and herbal medication at the ages of 0–9 and 10–17 years were 78.2% and 66.8%, respectively.28 Evening primrose oil, Ginkgo biloba, garlic, ginseng, St John’s wort, Echinacea, saw palmetto, and ginger were the commonly and concurrently used herbal medicinal products in the studies of subjects in Europe and the United States.13 However, communication regarding the concurrent usage of Western medication and herbal medicinal agents between Western physicians, traditional Chinese physicians and dentists is not always available.29
In Asian countries such as China, Korea, Japan and Taiwan, CHM is a common medical intervention. The World Health Organization (WHO) published the Traditional Medicine Strategy in 2013 and incorporated traditional Chinese medicine into the eleventh revision of the International Classification of Diseases in 2019, which was helpful toward including CHM in the healthcare system.30 The coprescription of Western medicine and CHM in our analysis is based on their reimbursement by the health insurance program in Taiwan and could be a standard for future reference. In Taiwan, the investigations of coprescription from Western medicine and CHM have been studied in adults with prostate and breast cancer. Most researchers have focused on improving the complications of Western medicine and disease progression.31,32 In Taiwanese adults with cancer, 21–31% patients with coprescription from Western medicine and CHM.31,32 The most common Western medicine in patients with coprescription was acetaminophen. The antibiotic and sedative agents were also listed as most common drugs when cancer patients used coprescription. The characteristics in patients prone to use coprescription were middle-age, living in the northern Taiwan, higher urbanization level regions, insurance amount (NTD) around 20,000–39,000. The similar findings also could be found in Taiwanese being diagnosed as HTN to use coprescription from Western medicine and CHM.33 Only one study performed the analysis to reveal the frequency distributions of the coprescription W+D, stratified by the major disease categories.31 However, the diagnoses (ICD-9 codes 520–529) belong to dentists who have been included into the category of diseases of digestive system (ICD-9 codes 520–579). Because Western physicians and dentists could order pain control agents as acetaminophen, presenting the sources of prescription is necessary and meaningful. However, our results in children are unique and not similar with the above data which reflect the real-world medical behaviors in Taiwanese children and their caregivers. A recent study in Canada recruited children who had concurrent use of natural health products, including herbal medication, and 16% of children were found to have drug–herbal or herbal–herbal interactions, such as bleeding and modified absorption.34
In our study, we found that trends in the proportions of children with coprescription, records of coprescriptions, and numbers of days of coprescription from W+C, and W+C+D sources increased with the calendar year; W+D sources all decreased with the calendar year. The trend of coprescriptions from the W+D sources is compatible with the finding from Korean children.12 Before the age interval of <3 years, the numbers of children with coprescriptions are the lowest. The highest peaks were for children aged 6–8 (W+D and W+C+D cohorts) and 3–5 (W+C cohort) years which is similar with the finding from investigation of polypharmacy in children at Hong Kong.35 The trends in the numbers of coprescriptions from W+C, W+D and W+C+D stratified by age revealed that before the age intervals of <3 years, the numbers of coprescriptions are the lowest. The highest peaks are for children aged 3–5 (W+D and W+C cohorts) and 6–8 (W+C+D cohort) years. After correction for the numbers of children in each age interval, the age intervals of <1 years (W+C, W+D and W+C+D cohorts) and 3–5 years (W+C, W+D cohorts) had lowest and highest numbers of coprescriptions, respectively. After the age intervals of 2 years, the numbers of coprescriptions corrected by numbers of children are the similar.
The lowest proportions of days of coprescriptions from W+C, W+D and W+C+D are at age intervals of <3 years; and the highest proportions of days of coprescriptions from W+C and W+D/W+C+D are at age intervals of 3–5 and 6–8 years, respectively. After correcting numbers of children in each age interval, the lowest proportions of days of coprescriptions from W+C/W+D and W+C+D are at age intervals of <1 and <2 years, respectively; the highest proportions of days of coprescriptions from W+C, W+D and W+C+D are at age intervals of 2, 15–17, and 12–14 years, respectively.
Females are the predominant group with coprescription according to the comparisons of basic characteristics of the W+D groups compared to those of the W-alone group which is not inconsistent from the studies focused on pediatric polypharmacy trends.35 Children in the age interval of 12–17 years are the largest group to use W alone and W+C; the age interval of 6–11 years is the largest group to use prescriptions from W+D and W+C+D. The results of comparisons of W+C, W+D and W+C+D to W alone showed that children aged 3–5 years had higher incidences of coprescription. In the comparisons of W+C, W+D and W+C+D to W alone, patients living in central Taiwan had higher rates of coprescription from W+C and W+D; those in living in southern Taiwan and the outside islands had higher rates of coprescription from W+C+D; children living in eastern Taiwan+ islands had the lowest rate of coprescriptions from W+C; northern Taiwan and eastern Taiwan+ islands had the lowest rate of coprescriptions from W+D; southern Taiwan had the lowest rate of coprescriptions from W+C+D. The findings of W+D/W+C+D to W alone are compatible with the results from the Taiwanese elderly individuals, rather than W+C to W alone. In other words, the regions of central and southern Taiwan are the hot spots to use coprescription.
When parents had a monthly income of <20,000 NTD, a highest incidence of coprescription from C+W, C+D, or C+W+D is found among their children which is not similar with the coprescrition investigation in the elderly individuals in Taiwan. Furthermore, from a Korea study revealed that even their study population most is also covered by national health insurance as Taiwan, the children from higher income family had more risk to accept polypharmacy.36 Taiwanese children born in families with low socioeconomic status may have problems maintaining a healthy status because their parents have limited knowledge to care for them.
The top three categories of children who used W alone and W+C are those with diseases of the respiratory system, injury, and nervous system which could represent that the children seeking W and C for similar diseases. And in the W+D and W+C+D cohorts, respiratory system and nervous system are the top two categories, the third categories are digestive system and skin and subcutaneous tissue, respectively. These findings are compatible with national-wide research investigated in the Korean children. When we reviewed other cohorts, including perceptions from D, the same top three categories from W and D are found in the W+D and W+C+D groups, respectively. This could indicate that the children seeking W and D have similar medical problems when they have coprescription.
There are some limitations in this study. Although Taiwanese can buy Chinese herbs in herbal stores without the need of prescription, the doses and types are for maintaining body health, rather than treating diseases. The definition of coprescription in our study is any two or three prescriptions from each of the three sources with an overlap of ≥1 day. However, this definition may not be clinically meaningful. Clarification of the impact from the cutoff value for the overlap period to outcome evaluation is important in future studies. Another limitation is that the classification of disease categories is a general overview. Some categories, such as symptoms, signs, and ill-defined conditions (ICD-9 codes 789–799) and injury and poisoning (ICD-9 codes 800–999), have been found among the top three disease categories from W or C, but they are difficult to connect directly to clinical problems or diseases. Our database only collected medical information before 2012 and the medical fee may be claimed in 2013 by some healthcare providers, but our topic is observing a long-term medical usage status among Taiwanese children and the sources of prescriptions are fixed since the National Health Insurance Program began in Taiwan. Our study did not belong to any emergent or abundant medical issue, such as COVID-19 pandemic.34,37 The time of our database is not the key obstacle to process our investigation. The claim data of NHIRD could not be validated, and the possible complications from coprescriptions were not disclosed. The specific complication of drug–herbal interaction is not our goal, because the trends of coprescription have not been investigated before and it is hard to hypothesize directly without our results. Our study provides important information about coprescription in children in Taiwan, including real-world data for the detection of coprescription trends ordered by Western physicians, traditional Chinese physicians and dentists in children in Asian countries. It is helpful to design further study to investigate specific drug–herbal interactions in the subgroup of children. Taking Taiwan as an example, healthcare providers and policymakers should be aware of the complexity of coprescription among children. Taiwan’s experience could help the world understand this topic comprehensively.
Conclusion
This study reports the characteristics and distributions of coprescription among children in Taiwan. Children aged 3–5 year and 6–8 years constituted the majority of coprescriptions. Compared to those in the W-alone group, aged 3–5 years and children who live in central Taiwan are more likely to have coprescription. Drug–drug and drug–herb interactions are important safety issues for not only clinical doctors but also children and their parents. The key concepts of coprescription must be introduced to Western physicians, Chinese medical physicians and dentists who may treat children.
Acknowledgement
We thank the funding support from Department of Chinese Medicine and Pharmacy, Ministry of Health and Welfare, Taiwan (M1207118).
Disclosure
Chia-Yu Huang and Hung-Rong Yen are co-correspondence authors for this study. The authors report no conflicts of interest in this work.
References
1. Huang TP, Liu PH, Lien AY, et al. Characteristics of traditional Chinese medicine use in children with asthma: a nationwide population‐based study. Allergy. 2013;68(12):1610–1613. doi:10.1111/all.12273
2. Yen HR, Liang KL, Huang TP, et al. Characteristics of traditional Chinese medicine use for children with allergic rhinitis: a nationwide population-based study. Int J Pediatr Otorhinolaryngol. 2015;79(4):591–597. doi:10.1016/j.ijporl.2015.02.002
3. Liao HH, Yen HR, Muo CH, et al. Complementary traditional Chinese medicine use in Children with cerebral palsy: a nationwide retrospective cohort study in Taiwan. BMC Complement Altern Med. 2017;17(1):155. doi:10.1186/s12906-017-1668-5
4. Huang CY, Wu MY, Wang HC, et al. Chinese herbal medicine decreases incidence of cirrhosis in patients with non-alcoholic fatty liver disease in Taiwan: a propensity score-matched cohort study. J Altern Complement Med. 2021;27(7):596–605. doi:10.1089/acm.2020.0494
5. Huang CY, Wu MY, Kuo YH, et al. Chinese herbal medicine is helpful for survival improvement in patients with multiple myeloma in Taiwan: a Nationwide Retrospective Matched-Cohort Study. Integr Cancer Ther. 2020;19:1–10. doi:10.1177/1534735420943280
6. Gmuca S, Xiao R, Weiss PF, Sherry DD, Knight AM, Gerber JS. Opioid prescribing and polypharmacy in children with chronic musculoskeletal pain. Pain Med. 2019;20(3):495–503. doi:10.1093/pm/pny116
7. Lohr WD, Creel L, Feygin Y, et al. Psychotropic polypharmacy among children and youth receiving Medicaid, 2012–2015. J Manag Care Spec Pharm. 2018;24(8):736–744. doi:10.18553/jmcp.2018.24.8.736
8. Dai D, Feinstein JA, Morrison W, et al. Epidemiology of polypharmacy and potential drug-drug interactions among pediatric patients in intensive care units of US children’s Hospitals. Pediatr Crit Care Med. 2016;17(5):e218.
9. Ewig CLY, Cheng YM, Li HS, et al. Use of chronic prescription medications and prevalence of polypharmacy in survivors of childhood cancer. Front Oncol. 2021;11:642544. doi:10.3389/fonc.2021.642544
10. Xie L, Gelfand A, Murphy CC, et al. Prevalence of polypharmacy and associated adverse outcomes and risk factors among children with asthma in the USA: a cross-sectional study. BMJ Open. 2022;12(10):e064708. doi:10.1136/bmjopen-2022-064708
11. Wood SJ, Ilomäki J, Gould J, et al. Dispensing of psychotropic medications to Australian children and adolescents before and during the COVID-19 pandemic, 2013–2021: a retrospective cohort study. Med J Aust. 2023;219(1):18–25. doi:10.5694/mja2.51948
12. Jeon SM, Park S, Rhie SJ, et al. Prescribing patterns of polypharmacy in Korean pediatric patients. PLoS One. 2019;14(10):e0222781. doi:10.1371/journal.pone.0222781
13. Loh CH. Use of traditional Chinese medicine in Singapore children: perceptions of parents and paediatricians. Singapore Med J. 2009;50(12):1162–1168.
14. Huang TP, Liu PH, Lien ASY, et al. A nationwide population-based study of traditional Chinese medicine usage in children in Taiwan. Complement Ther Med. 2014;22(3):500–510. doi:10.1016/j.ctim.2014.04.002
15. Hsieh CY, Su CC, Shao SC, et al. Taiwan’s national health insurance research database: past and future. Clin Epidemiol. 2019;11:349. doi:10.2147/CLEP.S196293
16. Lin LY, Warren-Gash C, Smeeth L, Chen PC. Data resource profile: the national health insurance research database (NHIRD). Epidemiol Health. 2018;40:e2018062.
17. Wu MY, Lee YC, Lin CL, et al. Trends in use of acupuncture among adults in Taiwan from 2002 to 2011: a nationwide population-based study. PLoS One. 2018;13(4):e0195490. doi:10.1371/journal.pone.0195490
18. Yeh YH, Chou YJ, Huang N, et al. The trends of utilization in traditional Chinese medicine in Taiwan from 2000 to 2010: a population-based study. Medicine. 2016;95(27):e4115. doi:10.1097/MD.0000000000004115
19. Huang CY, Wu MY, Chang CL, et al. Coprescription trends in western medicine, Chinese herbal medicine and dental medicine among older adults in Taiwan from 1997 to 2013. Complement Ther Med. 2021;63:102782. doi:10.1016/j.ctim.2021.102782
20. Lin SW, Yen CF, Chiu TY, et al. New indices for home nursing care resource disparities in rural and urban areas, based on geocoding and geographic distance barriers: a cross-sectional study. Int J Health Geogr. 2015;14(1):28. doi:10.1186/s12942-015-0021-9
21. Yen CF, Lin SW. Justice in dementia care resource allocation: how should we plan for dementia services? Int J Environ Res Public Health. 2019;16(10):1754. doi:10.3390/ijerph16101754
22. Shih CC, Liao CC, Su YC, et al. The association between socioeconomic status and traditional Chinese medicine use among children in Taiwan. BMC Health Serv Res. 2012;12(1):27. doi:10.1186/1472-6963-12-27
23. Tsai AI, Chen CY, Li LA, et al. Risk indicators for early childhood caries in Taiwan. Community Dent Oral Epidemiol. 2006;34(6):437–445. doi:10.1111/j.1600-0528.2006.00293.x
24. LaValley MP. Logistic regression. Circulation. 2008;117(18):2395–2399. doi:10.1161/CIRCULATIONAHA.106.682658
25. Woolf AD. Herbal remedies and children: do they work? Are they harmful? Pediatrics. 2003;112(Supplement 1):240–246. doi:10.1542/peds.112.S1.240
26. Brown AC. An overview of herb and dietary supplement efficacy, safety and government regulations in the United States with suggested improvements. Part 1 of 5 series. Food Chem Toxicol. 2017;107:449–471. doi:10.1016/j.fct.2016.11.001
27. Lazarou R, Heinrich M. Herbal medicine: who cares? The changing views on medicinal plants and their roles in British lifestyle. Phytother Res. 2019;33(9):2409–2420. doi:10.1002/ptr.6431
28. Delgoda R, Younger N, Barrett C, et al. The prevalence of herbs use in conjunction with conventional medicines in Jamaica. Complement Ther Med. 2010;18(1):13–20. doi:10.1016/j.ctim.2010.01.002
29. Welz AN, Emberger-Klein A, Menrad KJ. The importance of herbal medicine use in the German health-care system: prevalence, usage pattern, and influencing factors. BMC Health Serv Res. 2019;19(1):952. doi:10.1186/s12913-019-4739-0
30. Lam WC, Lyu A, Bian Z. ICD-11: impact on traditional Chinese medicine and world healthcare systems. Pharmaceut Med. 2019;33(5):373–377. doi:10.1007/s40290-019-00295-y
31. Wang BR, Chang YL, Chen TJ, et al. Coprescription of Chinese herbal medicine and Western medication among female patients with breast cancer in Taiwan: analysis of national insurance claims. Patient Prefer Adherence. 2014;8:671. doi:10.2147/PPA.S61280
32. Lin YH, Chen KK, Chiu JH. Coprescription of Chinese herbal medicine and Western medications among prostate cancer patients: a population-based study in Taiwan. Evid Based Complement Alternat Med. 2012;2012:147015. doi:10.1155/2012/147015
33. Yang PR, Shih WT, Chu YH, et al. Frequency and co-prescription pattern of Chinese herbal products for hypertension in Taiwan: a Cohort study. BMC Complement Altern Med. 2015;15(1):163. doi:10.1186/s12906-015-0690-8
34. Goldman RD, Rogovik AL, Lai D, et al. Potential interactions of drug-natural health products and natural health products-natural health products among children. J Pediatr. 2008;152(4):521–526. doi:10.1016/j.jpeds.2007.09.026
35. Ewig CLY, Wong KS, Chan PH, et al. Chronic medication use and factors associated with polypharmacy among outpatient pediatric patients. J Pediatr Pharmacol Ther. 2022;27(6):537–544. doi:10.5863/1551-6776-27.6.537
36. Baek YH, Shin JY, Liu G. Trends in polypharmacy over 12 years and changes in its social gradients in South Korea. PLoS One. 2018;13(9):e0204018. doi:10.1371/journal.pone.0204018
37. Huang CY, Kuo YH, Chuang ST, et al. The experience of executing preventive measures to protect a nursing home in Taiwan from a COVID-19 outbreak. Eur Geriatr Med. 2021;22:1–9.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.