Back to Journals » Infection and Drug Resistance » Volume 16
Trends and Patterns of Antibiotic Prescriptions in Primary Care Institutions in Southwest China, 2017–2022
Authors Li C, Cui Z ![]() , Wei D
, Wei D ![]() , Zhang Q, Yang J, Wang W, Luo X, Chang Y
, Zhang Q, Yang J, Wang W, Luo X, Chang Y ![]()
Received 15 June 2023
Accepted for publication 22 August 2023
Published 5 September 2023 Volume 2023:16 Pages 5833—5854
DOI https://doi.org/10.2147/IDR.S425787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Changlan Li,1,* Zhezhe Cui,2 Du Wei,3,4,* Quan Zhang,5,* Junli Yang,3 Wenju Wang,1 Xiaobo Luo,1 Yue Chang3,4
1School of Public Health, the key Laboratory of Environmental Pollution Monitoring and Disease Control, Ministry of Education, Guizhou Medical University, Guiyang, Guizhou Province, People’s Republic of China; 2Guangxi Key Laboratory of Major Infectious Disease Prevention and Control and Biosafety Emergency Response, Guangxi Zhuang Autonomous Region Center for Disease Control and Prevention, Nanning, Guangxi Province, People’s Republic of China; 3School of Medicine and Health Management, Guizhou Medical University, Guiyang, Guizhou Province, People’s Republic of China; 4Center of Medicine Economics and Management Research, Guizhou Medical University, Guiyang, Guizhou Province, People’s Republic of China; 5Department of Infectious Diseases, The Affiliated Hospital of Guizhou Medical University, Guiyang, Guizhou Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yue Chang, School of Medicine and Health Management, Guizhou Medical University, Guizhou Medical University, University Town, GUI ‘an New District, Guiyang, Guizhou Province, People’s Republic of China, Tel/Fax +86-0851-88308118, Email [email protected] Zhezhe Cui, Guangxi Key Laboratory of Major Infectious Disease Prevention and Control and Biosafety Emergency Response, Guangxi Zhuang Autonomous Region Center for Disease Control and Prevention, 18 Jinzhou Road, Nanning, Guangxi Province, People’s Republic of China, Tel/Fax +86-0771-2518785, Email [email protected]
Purpose: To explore the prescription patterns and usage trends of antibiotics within primary care institutions located in underdeveloped regions of China from 2017 to 2022.
Methods: A retrospective analysis of antibiotic prescriptions was conducted from 25 primary care institutions in Guizhou Province during the period of 2017– 2022. Antibiotic prescriptions were categorized into appropriate and inappropriate use. Appropriate use is further categorized into preferred medication, and antibiotics can be used or substituted. Inappropriate use is further categorized into unnecessary use, incorrect spectrum of antibiotics and combined use of antibiotics. Factors associated with inappropriate use were investigated using generalized estimation equations. Holt-Winters and SARIMA models were employed to predict the number of inappropriate antibiotic prescriptions as the alternative model.
Results: A total of 941,924 prescriptions were included, revealing a decreasing trend in both the number and inappropriate rates of antibiotic prescriptions from 2017 to 2022. Diseases of the respiratory system (70.66%) was the most frequent target of antibiotic use, with acute upper respiratory infections of multiple and unspecified sites representing 52.04% of these cases. The most commonly used antibiotics were penicillins (64.44%). Among all prescriptions, inappropriate antibiotic prescriptions reached 66.19%. Physicians aged over 35, holding the title of associate chief physician and possessing more than 11 years of experience were more likely to prescribe antibiotics inappropriately. The phenomenon of inappropriate antibiotic use was commoner among children aged five or younger. By comparing model parameters, it was determined that the SARIMA model outperforms the Holt-Winters model in predicting the number of inappropriate antibiotic prescriptions among primary care institutions.
Conclusion: The number and inappropriate rates of antibiotic prescriptions in southwest China exhibited a downward trend from 2017 to 2022, but inappropriate prescription remains a serious problem in primary care institutions. Therefore, future efforts should focus on strengthening physician education, training, and clinical practice. Additionally, physicians’ awareness of common misconceptions about inappropriate antibiotic use must be improved, and the prescribing behavior of physicians who fulfill patients’ expectations by prescribing antibiotics needs to be modified.
Keywords: antibiotics, primary care institution, trends, prescription patterns, inappropriate medication
Introduction
The discovery of antibiotics has played a pivotal role in combating bacterial infections and prolonging human life expectancy.1,2 Regrettably, inappropriate prescribing has contributed to the escalating problem of antimicrobial resistance,3–6 which can lead to heightened disease severity, mortality rates, and complications that further burden healthcare systems.7,8
Between 2000 and 2015, global antibiotic consumption witnessed a significant increase of 39%. This surge was primarily observed in middle- and low-income countries.9 An investigation carried out in India revealed a rising tendency in antibiotic usage from 2008 to 2017.10 The utilization of antibiotics in Chinese hospitals witnessed a significant increase of 39.6% from 2011 to 2018, as revealed by a study conducted in China.11 The escalating antibiotic usage is expected to lead to an upsurge in inappropriate antibiotic prescriptions. The World Health Organization (WHO) has emphasized the importance of controlling inappropriate antibiotic prescriptions.12
Worldwide, over 50% of antibiotic prescriptions in hospitals are deemed inappropriate.13–18 In high-income countries like the Netherlands and Qatar, studies have shown that approximately 45% of antibiotics were prescribed inappropriately.16,19 Studies conducted in Italy and the United States estimated that more than 55% of antibiotics were prescribed without any indication.20,21 The inappropriate use of antibiotics is likely to be more prevalent in certain middle- and low-income areas. Studies conducted in Pakistan, Uganda, and Ecuador showed that up to 70.3%, 82.2% and 90.25% of antibiotics were prescribed inappropriately within healthcare institutions.5,18,22 Similarly, studies conducted in India and Ethiopia revealed that approximately half of all antibiotic prescriptions were also used inappropriately.17,23
In China, half a billion of the 1.4 billion people live in rural areas24 and rely primarily on primary care institutions for medical services. According to the National Health Commission’s 2020 report,25 out of a total of 7.74 billion hospital visits nationwide, 4.12 billion individuals (53.23%) sought treatment at primary care institutions24 where antibiotics were frequently prescribed in outpatient settings.26–28 Studies have indicated that over 50% of antibiotic prescriptions in primary care institutions are inappropriate.14,15,29 In the past decade, the Chinese government has implemented a series of policies and measures to address the issue of overuse and misuse of antibiotics.30–32 While these policies aim to target all levels of healthcare institutions, most are better suited for secondary and tertiary hospitals with ample medical resources.27,33–35 The implementation of these policies and measures in primary care institutions is insufficient and impractical.13,15,36
Currently, research on antibiotics primarily centers around prescription patterns and influencing factors,37–39 common types of antibiotics used,2,40,41 analysis of antibiotic resistance42,43 and epidemic trends of antibiotic prescription.10,35,44–46 One study discovered that the growth of antibiotic consumption in middle- and low-income areas was significantly higher than that in high-income countries.9 However, there were few long-term studies on antibiotic prescriptions in in middle- and low-income areas.47 Therefore, our study aims to examine the prescription patterns and usage trends of antibiotics in primary care institutions located in underdeveloped regions of China from 2017 to 2022. It can also establish a theoretical foundation for the development of antibiotic diagnosis and treatment guidelines in primary care institutions located in underdeveloped regions.
Materials and Methods
Study Design
In China, the public hospital is stratified into three levels from top to bottom: tertiary hospitals, secondary hospitals, and primary care institutions. The latter category encompasses township hospitals and community health service centers as described in this study.48 Guizhou, province that has been lagging in development, boasts 1399 primary care institutions. Among them, 132 are utilizing the health information system (HIS) developed by the Guizhou LianKe Weixin Co., LTD. (LWTC). The LWTC is a technology service company primarily focused on the development, promotion, implementation, and operation of medical health information systems in Guizhou Province. It serves nearly 1500 medical institutions, both public and private, including those at the township, community, and some county-levels across nine prefectural-level cities in Guizhou Province.
The study’s inclusion criteria consisted of antibiotics prescribed by general practitioners who maintained their positions in the outpatient department of public primary care institutions in Guizhou Province, China, between 2017 and 2022. Exclusion criteria included prescriptions given for tuberculosis treatment, as it follows a standardized regimen. In the end, a total of 96 physicians from 25 primary care institutions who met these requirements were included in our retrospective observational study.
Data Collection
This study has been authorized by the Information Center of Guizhou Provincial Health Commission, and a data collection agreement has been signed with LWTC. The study data were obtained through the electronic information system’s data port of the primary care institutions, which were authorized by LWTC engineers. The dataset comprises information on outpatient antibiotic prescriptions, patient’s demographic information (including gender, age, disease, and health insurance, etc.). Physician’s characteristics such as sex, age, education level, title and work experience were obtained from the Personnel Management Department of primary care institutions.
Appropriateness of Antibiotic Prescriptions
Currently, the 11th edition of the International Classification of Diseases has been published, but the Guizhou region is still based on the 10th edition of the International Classification of Diseases (ICD-10). Therefore, ICD-10 was used as the classification standard of disease in this study.49 According to the Essential Medicines list published by the WHO,50 in conjunction with China’s clinical application guidelines for antibiotics and the common types of antibiotics used in primary care institutions,14,29,51 this study categorized antibiotics into seven main classes: penicillins, cephalosporins, macrolides, quinolones, lincosamides, nitroimidazoles and aminoglycosides. The focus of this study was on systemic antibiotics, topical antibiotics such as eye drops and ointments were excluded.
According to 1) the 2015 Guiding Principles for Clinical Antibiotic Use issued by the National Health Commission of China,52 2) the United States Centers for Disease Control and Prevention (CDC) Guidelines for antibiotic use,53 3) our previous studies14,29 and 4) the opinions of experts familiar with the situation of domestic primary care institutions, antibiotic prescriptions in primary care institutions were categorized as appropriate or inappropriate use. Appropriate use of antibiotics was further classified into two categories: 1) preferred medication: optimal drug, and 2) antibiotics can be used or substituted: available, not optimal. Inappropriate antibiotic prescriptions based on probable bacterial infections can further be categorized into three types: 1) unnecessary use: prescribing antibiotics to treat viral infections such as acute bronchitis or acute nasopharyngitis, 2) incorrect spectrum of antibiotics, such as prescribing penicillin G for gram-negative bacterial infections or cefotaxime for Pseudomonas aeruginosa infection in patients, 3) combined use of antibiotics: defined as the same physician prescribing different classes of systemic antibiotics to the same patient on the same day without any indication, such as administering penicillin and cefuroxime sodium in combination for gram-positive bacterial infections in single injection.
Data Management and Analysis
The physicians and their patients involved in the study were linked by a unique code. For the purpose of this study, multiple antibiotic prescriptions for the same patient by the same physician on one day were considered as a single visit.
First, cross-tabulation was utilized to analyze the relationship between antibiotic groups and disease categories based on ICD-10 diagnosis codes (take the initial three digits, for example, J02) in order to determine patterns and appropriateness of antibiotic use. In addition, joinpoint regression analysis was employed to examine local trends in antibiotic prescriptions during winter. Joinpoint regression model is to identify the number of join points sufficient to evaluate significant changes in data trends over time and establishing piecewise regression models to assess the changing characteristics of data trends.54 Second, the primary outcome variable in the study was the antibiotic inappropriate rate (AIR), which was calculated by dividing the number of inappropriate antibiotic prescriptions by the total number of antibiotic prescriptions. The Generalized Estimation Equation (GEE) approach was employed to identify independent predictors for inappropriate antibiotic use, in order to elucidate the correlation between antibiotic prescriptions issued by the same physician. Finally, the dataset was partitioned into two subsets: the training set consisted of data from January 2017 to December 2021, while the test set comprised data from January to December 2022. The Holt-Winters and seasonal autoregressive integrated moving average (SARIMA) models were constructed using the number of inappropriate antibiotic prescriptions recorded between January 2017 and December 2021. The determination coefficient (R2), Bayesian information criterion (BIC), rooted mean square error (RMSE), mean absolute percentage error (MAPE) and mean square error (MSE) were used to compare the prediction accuracy of the two models and facilitate optimal model selection. The predicted effect of the optimal model was assessed through relative error and a 95% confidence interval (CI).
The Holt-Winters and SARIMA models are two of the most widely utilized methods for time series prediction. They are applicable to various types of time series data and can effectively capture temporal changes as well as periodic fluctuations in the original data.55,56 The Holt-Winters model, also referred to as the Holt-Winters exponential smoothing method, is a time series analysis and prediction technique that can simultaneously smooth the trend and seasonality of time series, estimate values, trends, and seasonal fluctuations at the current point in time. The smoothness is modulated by the parameters α, β and γ, all of which have values ranging from 0 to 1. The closer a parameter value is to 0, the greater the weight assigned to distant historical data in prediction.57,58 The model includes simple seasonal, additive, and multiplicative models. The SARIMA model is capable of handling seasonal time series data, which is typically represented as ARIMA (p, d, q) × (P, D, Q) s (where p is the autoregressive order, d is the time difference when the sequence is stable, q is the moving average order, P is the seasonal autoregressive order, D is the seasonal difference times, Q is the seasonal moving average order, s is the length of the seasonal cycle).58
A two-sided Type 1 error rate of 0.05 was employed to establish statistical significance in all analyses. Microsoft Excel 2021, R 4.2.1 and IBM SPSS Statistics 26.0 utilized for data management and analysis.
Ethics Statement
The study was approved by the Ethics Review Committee of Guizhou Medical University (Approval Certificate No. 2019 (149)). All participating physicians provided written informed consent to take part in the study. The data accessed complied with relevant data protection and privacy regulations.
Results
This study included 1,009,011 systemic antibiotic prescriptions obtained from the HIS systems of 25 primary care institutions that met the inclusion criteria after excluding 18,970 topical antibiotic prescriptions. For analysis purposes, only the top ten common systemic diseases were considered in this study, which accounted for a total of 941,924 antibiotic prescriptions (93.35%).
A monthly heat map was generated to visualize the trends in antibiotic prescriptions from 2017 to 2022 (Figure 1). The overall number of antibiotic prescriptions exhibited an upward trend during the period of 2017–2019, followed by a significant decline during the years of 2020–2022. In addition, joinpoint regression analysis was performed to examine the trend of antibiotic prescriptions during winter (December–February of the following year). Results indicated an upward trend prior to 2020, followed by a downward trend thereafter.
 |
Figure 1 Monthly variations in antibiotic prescriptions from 2017 to 2022. |
Figure 2 illustrates the distribution and trends in antibiotic appropriateness and AIRs from January 2017 to December 2022. The number of prescriptions and AIRs exhibited a general downward trend, with a significant increase in total prescriptions during winter each year, accompanied by an increase in both the number and rates of inappropriate prescriptions. However, the AIRs have decreased compared to the same period last year since 2021 and has remained low since then until December 2022, when it rebounded clearly. Additionally, there was a significant reduction in AIRs observed between February and July 2018 as well as March and August 2021.
 |
Figure 2 Distribution and trends in antibiotic appropriateness and AIRs from January 2017 to December 2022. |
Table 1 shows the distribution of clinical diagnoses, antibiotic groups, and appropriateness of antibiotic prescriptions. Among all clinical diagnoses, diseases of the respiratory system were the most prevalent (70.62%), with acute upper respiratory infections of multiple and unspecified sites accounting for 52.04%. In the table, “P” represents “Preferred medication”, “A” represents “Antibiotic can be used or substituted”, “I” represents “Incorrect spectrum of antibiotics”, and “U” represents “Unnecessary use”. Inappropriate use of antibiotics was identified in 66.19% (61.04% for I and 5.15% for U) of the 941,924 prescriptions. The highest rate of inappropriate use was observed in patients with diseases of the musculoskeletal system and connective tissue (100%) and symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified (100%), followed by patients with diseases of the skin and subcutaneous tissue (92.01%). Incorrect spectrum of antibiotics was frequently utilized among individuals diagnosed with keratitis (85.96%) and other gastroenteritis and colitis of infectious and unspecified origin (57.84%). Unnecessary use was prevalent across all systemic diseases, and among them, diseases of the musculoskeletal system and connective tissue and symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified reached 100%. The highest rate of appropriate use was found in diseases of pulp and periapical tissues (99.85%), superficial injury of head (99.57%), abscess of anal and rectal regions (99.54%) and acute appendicitis (99.51%). Table 1 shows penicillins accounted for 64.44% of all antibiotic prescriptions followed by cephalosporins (12.32%). The inappropriate use of all antibiotic groups exceeded 60% and aminoglycosides and lincosamides reached 98.66% and 97.76%.
 |
Table 1 Appropriateness Distribution of Clinical Diagnoses, Antibiotic Groups, and Antibiotic Prescriptions |
Figure 3 illustrates the distribution of inappropriate antibiotics in three different systemic diseases. The top three out of ten systemic diseases, namely diseases of the respiratory system, diseases of the digestive system, diseases of the genitourinary system were analyzed based on antibiotic prescription rankings. For diseases of the respiratory system, AIRs exhibited a gradual decline from 2017 to 2019 before experiencing a rebound in 2020 and subsequently decreasing significantly in 2021. In diseases of the digestive system, AIRs remained stable between 2017 and 2020 before experiencing a significant decline after 2021. In diseases of the genitourinary system, there was a marginal increase in AIRs from 2017 to 2022. The average AIRs for diseases of the respiratory system, diseases of the digestive system and diseases of the genitourinary system were recorded at 69.57%, 31.89% and 44.94%, respectively.
 |
Figure 3 Distribution of AIRs in three different systemic diseases. |
Table 2 shows the results of a univariate analysis on inappropriate antibiotic use. In the study, male physicians accounted for 73.42% (691,602), physicians with college degrees or higher made up 46.52% (438,155), and resident physicians comprised 67.13% (632,318). In addition, out of all visits recorded in the study period, men constituted 50.41% (474,870), oral antibiotics were prescribed in 76.63% (721,754) of cases and insurance payments covered treatment costs in 88.93% (837,649) instances. In Table 2, “Combined use of antibiotics” refers to situations where a physician prescribes two or more groups of antibiotics for the same patient in the same visit. The proportions of prescriptions categorized as “preferred medication”, “antibiotic can be used or substituted”, “combined use of antibiotics”, “incorrect spectrum of antibiotics” and “unnecessary use” were 10.21%, 17.46%, 18.56%, 2.15% and 51.60%, respectively. Univariate analysis showed that all variables were statistically significant (P < 0.001), thus all variables were included in the multivariate analysis.
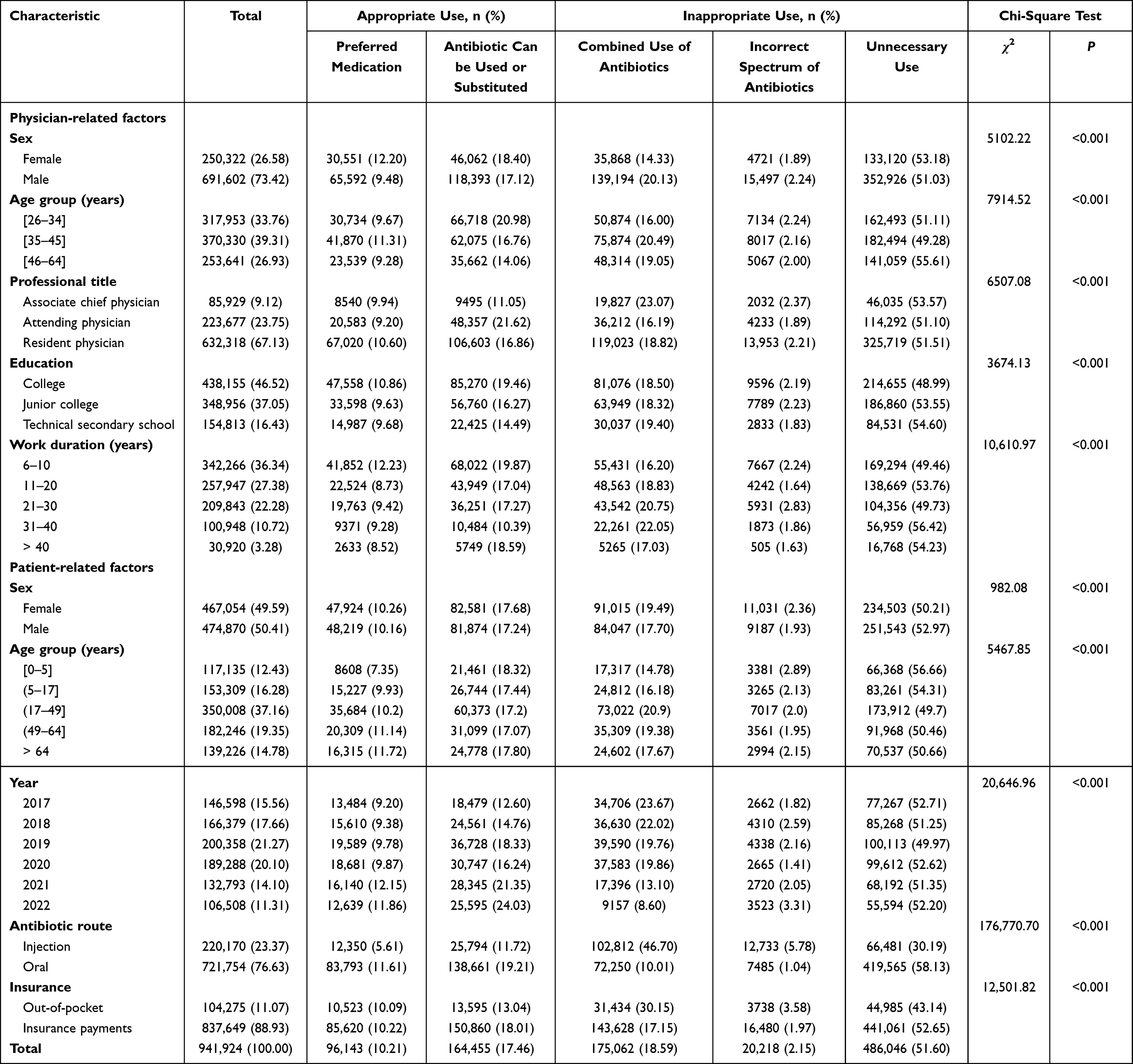 |
Table 2 Factors Associated with Inappropriate Antibiotic Use on Univariate Analysis |
Table 3 shows the results of multivariate analysis on factors associated with inappropriate antibiotic use. Regarding physician-related factors, physicians were more likely to prescribe inappropriate antibiotics if they were male, aged over 35 years old, had less than a college education, had an associate chief physician title, and had over 11 years of service. As for patient-related factors, those aged between 0 and 5, received injections and paid out-of-pocket were more likely to be received inappropriate antibiotics. Furthermore, the inappropriate antibiotic prescriptions were more prevalent in 2017 compared to the period spanning from 2018 to 2022.
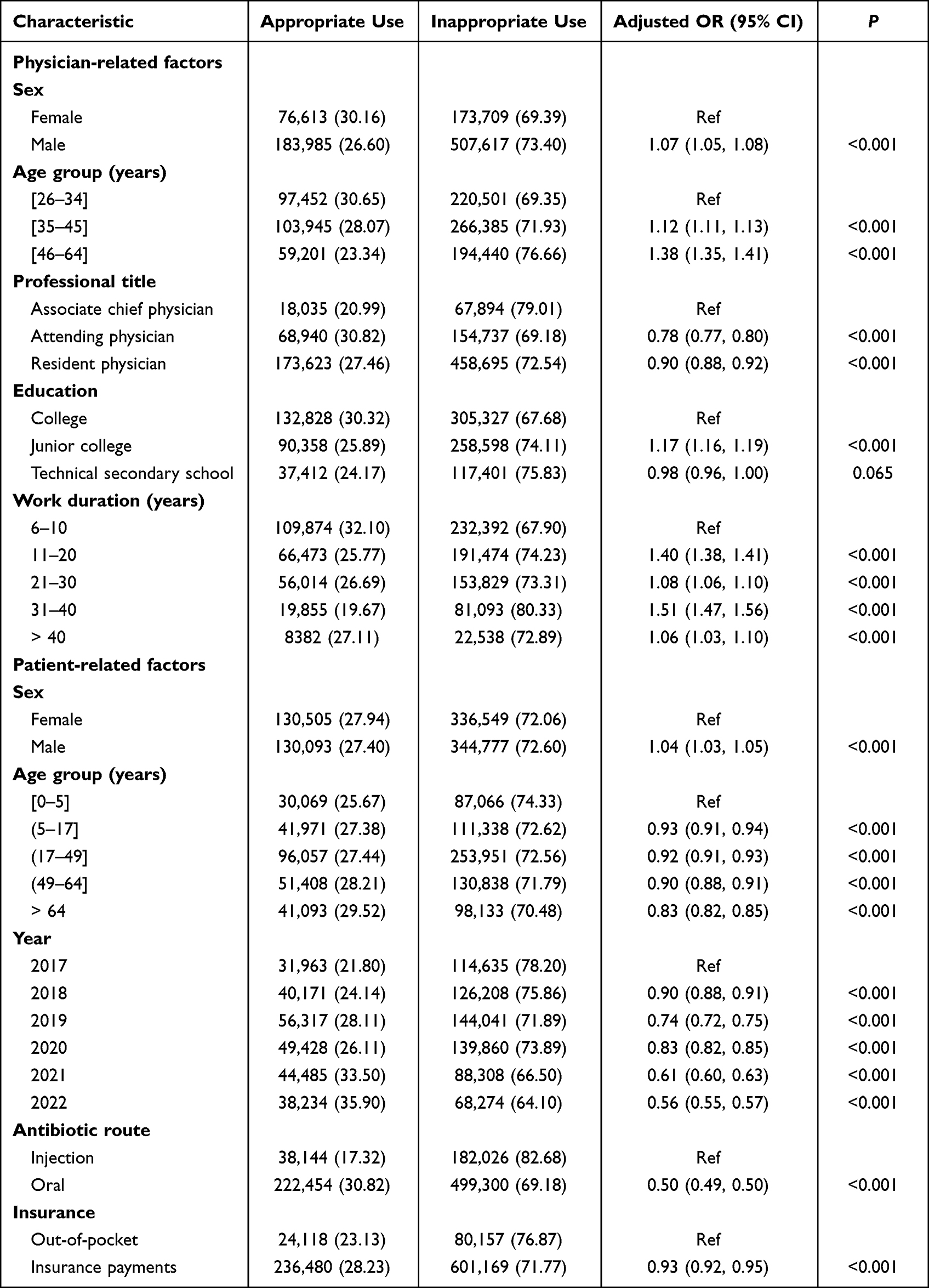 |
Table 3 Results of the GEE Analysis on Factors Influencing Inappropriate Antibiotic Use |
Holt-Winters and SARIMA models were employed to predict inappropriate antibiotic prescription from January to December 2022. The optimal model is determined by selecting the one with the highest R2 and lowest BIC, RMSE, MAPE, and MSE. The optimal Holt-Winters model was a simple seasonal model, and the optimal SARIMA model was ARIMA (0, 1, 0) (1, 1, 0) 12. The Ljung-Box Q test results for the residuals of all optimal models indicated that none of these residuals were autocorrelated, with P-values greater than 0.05. This suggests that the models effectively captured the information from the original series. All model parameter information is included in Tables S1 and S2. The predicted effects of visualization are presented in Figures 4 and 5. As depicted in the figures, the fitting effects of two optimal models during the period between 2017 and 2021 and their predictive performance for the years 2022 were satisfactory. Their predicted values’ 95% confidence intervals all encompass the actual values.
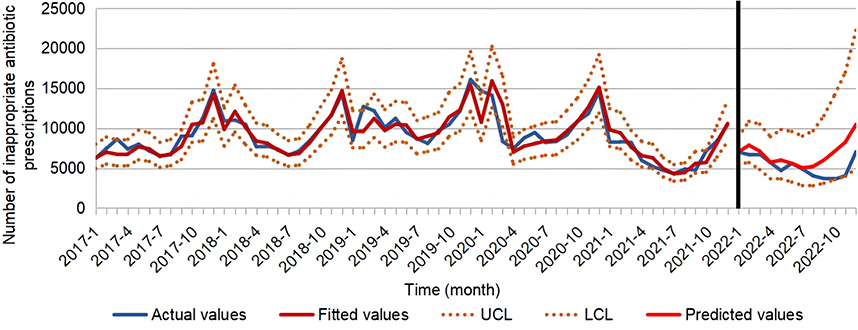 |
Figure 4 The predicted results of the number of inappropriate antibiotic prescriptions by Holt-Winters model. |
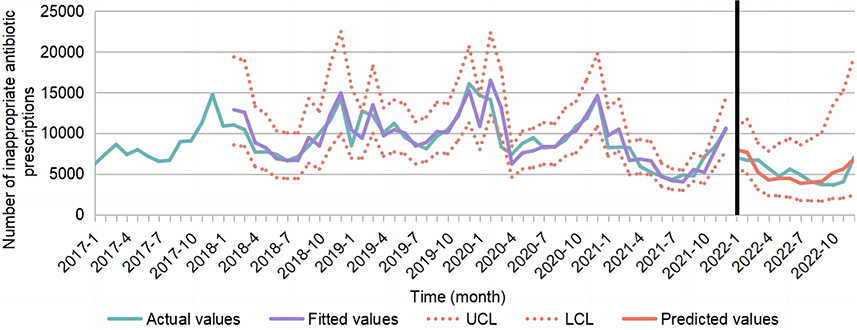 |
Figure 5 The predicted results of the number of inappropriate antibiotic prescriptions by SARIMA model. |
The simple seasonal model exhibited relative errors ranging from 0.07% to 103.11%, with R2 = 0.84, BIC = −5.77, and RMSE, MAPE, and MSE values of 0.05, 0.92%, and 0.04, respectively. The ARIMA (0,1,0) (1,1,0) 12 model displayed relative errors between 1.62% and 42.92%, along with an R2 value of 0.76 and BIC value of −5.22, its corresponding RMSE, MAPE and MSE were calculated as being equal to 0.07, 1.30%, and 0.05, respectively. The SARIMA model predicts an annual relative error of 0.35% in the number of inappropriate antibiotic prescriptions for 2022, which is significantly smaller than the Holt-Winters simple seasonal model’s relative error of 27.65%, as demonstrated in Table 4 and Table 5. The aforementioned data indicate that in comparison to the Holt-Winters model, the ARIMA (0,1,0) (1,1,0) 12 model yields a prediction closer to actual values and exhibits higher accuracy.
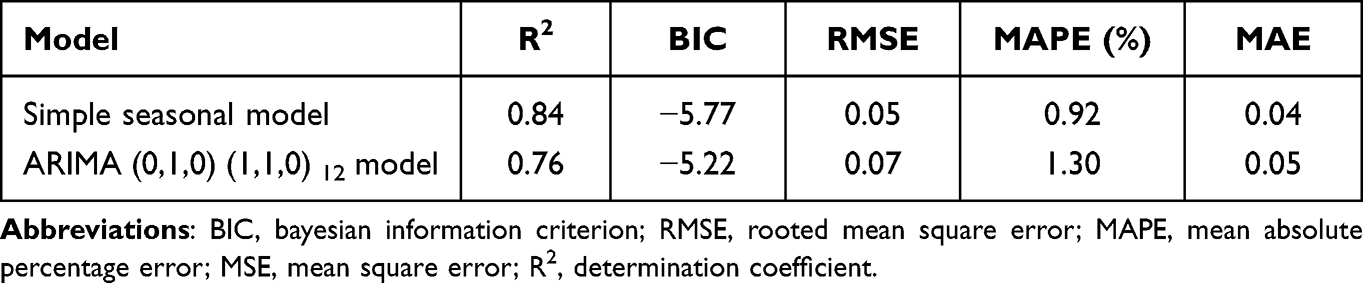 |
Table 4 The Optimal Model Parameter Information |
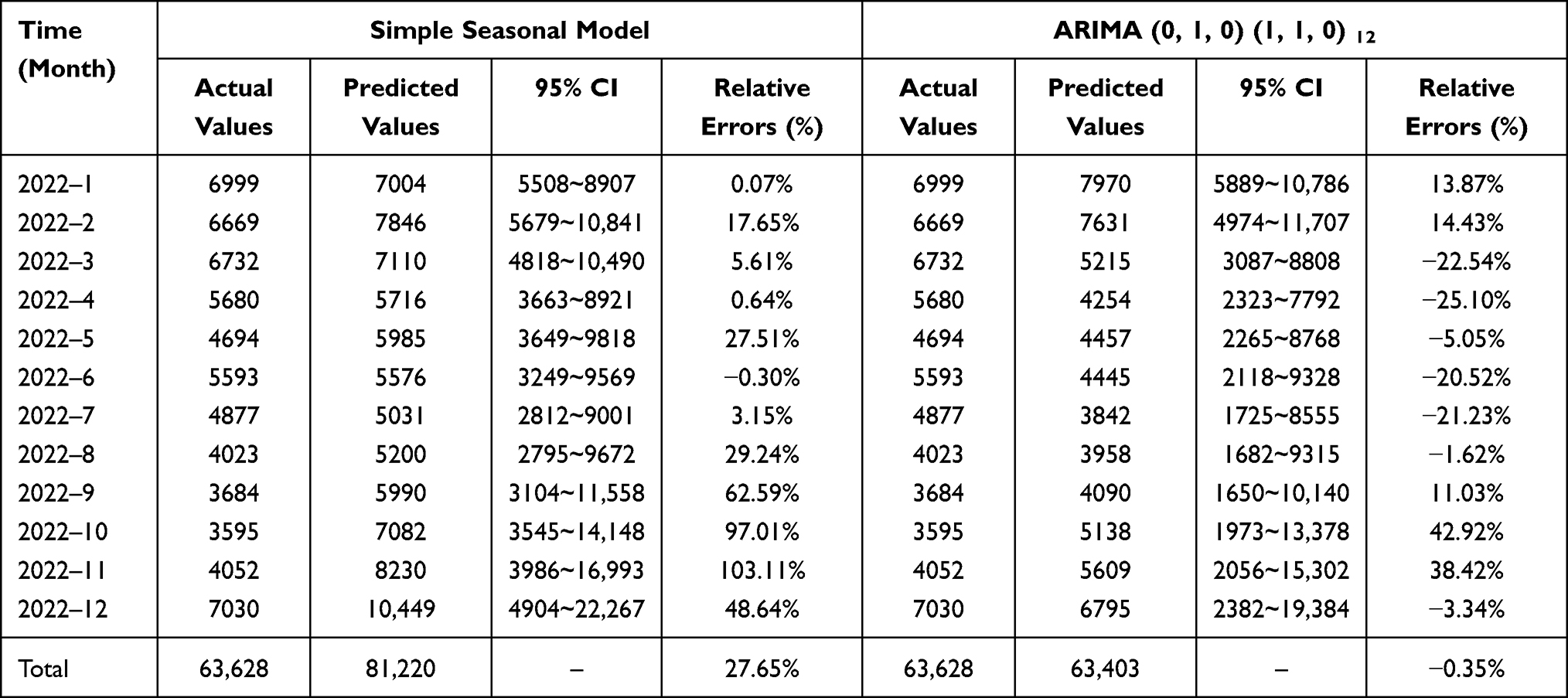 |
Table 5 Comparison of Actual Values and Predicted Values of Inappropriate Antibiotic Prescription from January to December 2022 |
Discussion
In this retrospective study, the trends and patterns of antibiotic prescriptions from 2017 to 2022 were described in 25 primary care institutions in Guizhou Province that met inclusion criteria. The number of antibiotic prescriptions and AIRs generally exhibited a general downward trend. Diseases of the respiratory system accounted for the majority (70.62%) of all system diseases observed, while penicillins were found to be the most commonly prescribed antibiotics. Overall, 66.19% of antibiotic prescriptions were deemed inappropriate. Physicians with less education and over 11 years of work experience were relatively more prone to prescribing antibiotics inappropriately. After comparing the Holt-Winters and SARIMA models for predicting changes in number of inappropriate antibiotic prescriptions, it was found that the SARIMA model outperformed the Holt-Winters model in terms of prediction accuracy.
This study revealed a general declining tendency in antibiotic prescriptions, albeit with a slight increase observed during 2017–2019. A similar trend was reported by a Yinchuan-based investigation.15 Multiple studies have documented significantly reduced antibiotic consumption since 2020 compared to pre-COVID-19 outbreak levels in 2019.59–61 The decline in antibiotic prescriptions may be attributed to the reduced medical seeking behavior of individuals due to the implementation of epidemic prevention and control policies. Additionally, measures such as hand hygiene, widespread mask-wearing, and social distancing have effectively curbed respiratory infectious diseases.59 Furthermore, there was a significant increase in antibiotic prescriptions during the winter prior to 2020, followed by a downward trend thereafter. This could be attributed to a reduction in healthcare-seeking behavior among individuals and respiratory diseases as a result of the COVID-19 pandemic in 2020.
In this study, it was observed that the AIRs dropped from 69.56% in 2017 to 59.74% in 2022, with an average of 66.19% in rural areas of Guizhou Province. A study conducted in Eastern Uganda reported that between 2016 and 2018, approximately 82.6% of antibiotics were prescribed inappropriately.22 A study conducted in China revealed that a proportion of 52.8% (2017–2021) of antibiotic prescriptions issued by primary care institutions were deemed inappropriate.15 Due to variations in research methodologies, data collection, and timeframes across different countries and regions, it is not feasible to directly compare those studies. Although the study found an overall decrease in AIRs in primary care institutions in rural areas, antibiotic inappropriate use remained severe. Evidence suggests that primary care providers practicing in rural areas may be more likely to prescribe antibiotics inappropriately.15,17,62 This is due to the fact that hospital medical inspection equipments and physicians’ clinical experience, which are crucial factors in achieving accurate diagnosis and appropriate prescription, tend to be inferior in rural areas compared to urban areas.63,64 Moreover, the AIRs exhibited a significant decrease during February to July 2018 and March to August 2021, which may be attributed to two six-month feedback interventions conducted by our team targeting inappropriate antibiotic prescribing behavior among primary care physicians during these two periods.65,66 The AIRs continued to decline after 2021 until a significant rebound in December 2022. This may be attributed to the adjustment of China’s COVID-19 prevention and control policy in December 2022, which resulted in a surge of infections and overwhelming visits that led to an increase in inappropriate antibiotic prescriptions prescribed by physicians.
Penicillins were the most used antibiotic in our study (66.44%), probably due to their high availability, safety, affordability, and oral administration. Penicillins was also widely reported as the most commonly prescribed antibiotic in other regions.22,38,67,68 AIRs of all the seven antibiotic groups exceeded 60%, with lincosamides and aminoglycosides reaching 97.76% and 98.66%, respectively. In this study, the majority of lincosamides and aminoglycosides antibiotics were administered for diseases of the respiratory system. Lincosamides were appropriate for treating lower respiratory tract infections caused by Streptococcus pneumoniae, group A hemolytic streptococcus and Staphylococcus aureus. However, in our study, lincosamides were predominantly prescribed for upper respiratory infections that seldom require antibiotic therapy. As for aminoglycosides, their antibacterial effects on Streptococcus pneumoniae and group A hemolytic streptococcus, which are the main pathogens of community-acquired respiratory tract infections, were poor. Additionally, they have significant ear and kidney toxicity. Therefore, it is incorrect to use these drugs for the treatment of common respiratory tract bacterial infections in outpatient settings.52
In the study, the majority of antibiotic prescriptions were for diseases of the respiratory system account for 70.62%, with acute upper respiratory infections of multiple and unspecified sites (J06) accounting for 52.04%. However, the Clinical Guidelines for Antibiotic Use in China52 and the United States CDC53 state that acute upper respiratory infections caused by rhinovirus, coronavirus and influenza virus are the most prevalent community-acquired infections. Typically, these illnesses are self-limiting and do not necessitate antibiotic treatment. The AIRs of diseases of the respiratory system in this study were 69.57%, which was lower than that of Malaysia (87.8%)69 and Ecuador (95.25%),5 but higher than that of the Netherlands (46%) and Italy (66.5%).19,20 Under the antibiotic stewardship system,30–32 the AIRs of diseases of the respiratory system gradually decrease from 2017 to 2019; however, there was a significant rebound observed in 2020, almost reaching the level seen in 2017. This may be associated with the COVID-19 pandemic in 2020. A study revealed that primary care institutions prescribed more antibiotics for respiratory illnesses during the COVID-19 outbreak.60 Between April and September 2021, when our research team implemented the antibiotic prescription intervention, there was a significant reduction in the AIRs related to diseases of the respiratory system. Winter is characterized by an increased prevalence of respiratory illnesses, resulting in higher AIR and antibiotic prescriptions compared to other seasons.
The diseases of the digestive system were the second most common systemic disease in this study, with AIRs accounting for 31.89%. AIRs in diseases of the digestive system remained stable during the 2017–2020 period but showed a significant reduction and maintained a consistent downward trend after the implementation of an antibiotic prescription intervention during the period of April–September 2021. This provided further evidence that interventions targeting antibiotic prescriptions can significantly reduce the AIRs of diseases of the digestive system.
Our study revealed that the AIRs of diseases of the genitourinary system was 44.94%. Despite our team’s antibiotic prescription intervention, we observed a continuous increase in the AIRs of diseases of the genitourinary system during our study period. This may be attributed to the fact that most primary care institutions are general outpatient clinics where physicians lack expertise in diagnosing and treating diseases of the genitourinary system. As a result, most physicians resort to empirical medication or refer patients to specialized clinics at superior hospital.14,70
In this study, the majority of inappropriate antibiotic prescribers were aged over 35 years old, held a high professional title (associate chief physician) and had over 11 years of experience. Most of them possessed only junior college level education and their professional knowledge was not comprehensive nor in-depth. Therefore, it is imperative to provide physicians with more education, training, and clinical practice opportunities to mitigate the overuse of antibiotics in primary care institutions.71 Additionally, our findings indicated a higher likelihood of inappropriate antibiotic prescriptions for children aged 0–5 years, consistent with previous research.15,27,72 This may be attributed to the tendency for rural grandparents to care for young children in this age group who may lack adequate nutrition and have immature immune systems compared to their urban counterparts, rendering them more susceptible to various illnesses. A study has reported that the average child experiences over 40 episodes of morbidity within a 5-year period.72 Furthermore, their guardians are typically poorly educated and unaware of the dangers associated with antibiotic overuse, often requesting physicians to prescribe antibiotics. However, outpatient physicians in primary care institutions frequently prescribe antibiotics empirically or satisfy patients by prescribing them without providing an explanation as to why they are unnecessary.14,62,70
Patients who received intravenous antibiotics were more likely to be prescribed antibiotics inappropriately. This may be attributed to the fact that physicians tend to combine multiple injection antibiotics for patients with serious infections, aiming at promoting early recovery and satisfying patient’s expectations.70 As shown in Table 2, the combined use of antibiotics accounted for 46.70% among the three types of inappropriate injection antibiotics. However, in most cases of bacterial infections, a single antibiotic is sufficient unless otherwise indicated. Furthermore, patients who pay out-of-pocket for medications have a higher likelihood of receiving inappropriate antibiotics in comparison to those with insurance coverage. This finding is in line with the results of two studies conducted in China and the USA.73,74 There are potentially two underlying reasons for this phenomenon. Firstly, the majority of rural residents are covered by basic medical insurance policies with limited payouts. When their medical expenses exceed this limit, patients may defer prescriptions. Conversely, patients who pay out-of-pocket for medications are exempt from insurance limitations so may face an increased risk of receiving inappropriate prescriptions. Secondly, uninsured drugs are less regulated than insured drugs, which means physicians may prescribe them more inappropriately.73
According to the predicted results of Holt-Winters and SARIMA models on the number of inappropriate antibiotic prescriptions in 2022, the fitting effect of Holt-Winters model is better than that of SARIMA model. However, in practical applications, SARIMA exhibits superior prediction accuracy compared to Holt-Winters. Furthermore, in terms of the models, Holt-Winters is suitable for data with a single trend, while SARIMA is more appropriate for predicting data with a stable trend.58 From Figure 5, the number of inappropriate antibiotic prescriptions in winter was significantly higher than in other seasons, exhibiting a relatively stable seasonality. Therefore, based on the comparison of parameters and predicted effects, the SARIMA model appears to be a more appropriate choice for predicting the number of inappropriate antibiotic prescriptions in this study.
The primary strength of this study lies in its large sample of prescription data, which provides an objective assessment of antibiotic utilization in underdeveloped provinces in China. It employs a multifactorial analysis to identify the determinants of inappropriate antibiotic use within primary care institutions. Furthermore, building upon the general prescription pattern study, this study incorporates a diverse range of time series models to forecast future trends and identifies the optimal model as a valuable reference for antibiotic usage trend. However, our study was subject to several limitations. Firstly, it should be noted that primary care institutions in Guizhou province generally do not conduct laboratory tests and physicians tend to administer medication empirically. As a result, we were unable to identify relevant content within the HIS system for further analysis of prescription appropriateness. Secondly, it was possible that the AIRs were overestimated in this study due to the inability to access secondary disease diagnoses for patients from the HIS system.21,51 In China’s primary care institutions, it is uncommon for a secondary diagnosis to be included in prescriptions. Thirdly, the prescription data was sourced solely from primary care institutions in one province. Given the significant regional variations in antibiotic usage, this study may only reflect patterns of antibiotic use within comparable areas of primary care.
Although a gradual decrease in the number of antibiotic prescriptions and inappropriate rates, the prevalence of inappropriate antibiotic prescriptions remains high in primary care institutions in China. This study revealed that 66.19% of prescriptions were deemed inappropriate, with low professional competence among physicians in primary care institutions being a significant contributing factor to this issue. Their antibiotic prescription practices are not evidence-based but rather rely on their own experience and habits. In cases where antibiotics are unnecessary, some physicians even prescribe them to meet patient expectations. Achieving appropriate use of antibiotics across China hinges on promoting their appropriate utilization within primary care institutions. Therefore, in the future, comprehensive training programs should be offered to primary care physicians to enhance their professional competence. Initial training should primarily focus on raising awareness among physicians about diseases or patients for whom antibiotics are often prescribed but should not be used. Subsequently, the second phase of training should focus on changing physicians’ habits of prescribing behavior. Physicians must attentively consider patients’ expectations and when confronted with active requests for unnecessary antibiotic treatment, they should proactively provide clear explanations to justify refusal, thereby effectively reducing instances of inappropriate usage.
Conclusions
From 2017 to 2022, there was a downward trend in both the number of antibiotic prescriptions and AIRs. Despite this progress, inappropriate prescribing practices for antibiotics remain prevalent in primary care institutions, particularly for diseases of the respiratory system. The lack of physician expertise regarding appropriate antibiotic use was a major contributing factor to this issue. Therefore, future efforts should focus on enhancing physician education, training, and clinical practice to effectively address this problem. In addition, future efforts should prioritize two key areas. Firstly, it is imperative to enhance physicians’ awareness in primary care institutions regarding prevalent misconceptions surrounding the inappropriate utilization of antibiotics. Secondly, there is a need to modify the prescribing behavior of physicians who have become accustomed to fulfilling patients’ expectations by prescribing antibiotics.
Abbreviations
AIR, Antibiotic inappropriate rate; WHO, World Health Organization; ICD-10, the 10th Edition of the International Classification of Diseases; CDC, Centers for Disease Control and Prevention; HIS, Hospital Information System; LWTC, LianKe Weixin Co., LTD.; GEE, Generalized estimation equation; SARIMA, Seasonal autoregressive integrated moving average; R2, Determination coefficient; BIC, Bayesian information criterion; RMSE, Rooted mean square error; MAPE, Mean absolute percentage error; MSE, Mean square error; CI, Confidence interval; Ref, Reference group; OR, Odds ratio.
Data Sharing Statement
The original contributions presented in the study are included in the article/Supplementary Material, and further inquiries can be directed to the corresponding authors.
Acknowledgments
We express our gratitude to all participating institutions for their invaluable information and assistance throughout the study. The authors extend their appreciation to all members of the investigational team who diligently collected the data. We would also like to acknowledge Edward McNeil, from Prince of Songkla University in Songkhla, Thailand, for his insightful feedback on improving this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the National Natural Science Foundation of China Grant (71964009) for “Research on feedback intervention mode of antibiotic prescription control in primary care institutions based on the depth graph neural network technology” and the Technology Fund Project of Guizhou Provincial Health Commission Grant (gzwjkj2019-1-218) for “Application Research of Deep Learning Technology in Rational Evaluation and Intervention of Antibiotic Prescription”. Corresponding author YC is the project leader. The funders covered travel expenses incurred during the data collection process, as well as the expert’s fees for providing guidance on study design, technological support, data analysis and interpretation, and manuscript writing assistance.
Disclosure
The authors declare that they have no competing interests.
References
1. Baskaradoss JK, Alrumaih A, Alshebel A, et al. Pattern of antibiotic prescription among dentists in Riyadh, Saudi Arabia. J Investig Clin Dent. 2018;9(3):e12339. doi:10.1111/jicd.12339
2. Machado-Alba JE, Valladales-Restrepo LF, Gaviria-Mendoza A, Machado-Duque ME, Figueras A. Patterns of antibiotic prescription in Colombia: are there differences between capital cities and municipalities? Antibiotics. 2020;9(7):389. doi:10.3390/antibiotics9070389
3. Llor C, Bjerrum L. Antimicrobial resistance: risk associated with antibiotic overuse and initiatives to reduce the problem. Ther Adv Drug Saf. 2014;5(6):229–241. doi:10.1177/2042098614554919
4. Gianino MM, Lenzi J, Bonaudo M, Fantini MP, Ricciardi W, Damiani G. Predictors and trajectories of antibiotic consumption in 22 EU countries: findings from a time series analysis (2000–2014). PLoS One. 2018;13(6):e0199436. doi:10.1371/journal.pone.0199436
5. Sanchez Choez X, Armijos Acurio ML, Jimbo Sotomayor RE. ”Appropriateness and adequacy of antibiotic prescription for upper respiratory tract infections in ambulatory health care centers in Ecuador”. BMC Pharmacol Toxicol. 2018;19(1):46. doi:10.1186/s40360-018-0237-y
6. Farooqui HH, Mehta A, Selvaraj S. Outpatient antibiotic prescription rate and pattern in the private sector in India: evidence from medical audit data. PLoS One. 2019;14(11):e0224848. doi:10.1371/journal.pone.0224848
7. Watkins RR, Bonomo RA. Overview: global and local impact of antibiotic resistance. Infect Dis Clin North Am. 2016;30(2):313–322. doi:10.1016/j.idc.2016.02.001
8. Medina E, Pieper DH. Tackling threats and future problems of multidrug-resistant bacteria. Curr Top Microbiol Immunol. 2016;398:3–33. doi:10.1007/82_2016_492
9. Klein EY, Van Boeckel TP, Martinez EM, et al. Global increase and geographic convergence in antibiotic consumption between 2000 and 2015. Proc Natl Acad Sci USA. 2018;115(15):E3463–E3470. doi:10.1073/pnas.1717295115
10. Damlin A, Sharma M, Marrone G, Stalsby Lundborg C. Antibiotic prescribing among patients with severe infectious diseases in two private sector hospitals in Central India - a time series analysis over 10 years. BMC Infect Dis. 2020;20(1):340. doi:10.1186/s12879-020-05059-7
11. Wushouer H, Zhou Y, Zhang X, et al. Secular trend analysis of antibiotic utilisation in China’s hospitals 2011–2018, a retrospective analysis of procurement data. Antimicrob Resist Infect Control. 2020;9(1):53. doi:10.1186/s13756-020-00709-6
12. O’Neill J. Tackling drug-resistant infections globally: final report and recommendations: the review on antimicrobial resistance; 2016. Available from: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf.
13. Taxifulati Y, Wushouer H, Fu M, et al. Antibiotic use and irrational antibiotic prescriptions in 66 primary healthcare institutions in Beijing City, China, 2015–2018. BMC Health Serv Res. 2021;21(1):832. doi:10.1186/s12913-021-06856-9
14. Wang W, Yu S, Zhou X, et al. Antibiotic prescribing patterns at children’s outpatient departments of primary care institutions in Southwest China. BMC Prim Care. 2022;23(1):269. doi:10.1186/s12875-022-01875-9
15. Zhao H, Wang S, Meng R, et al. Appropriateness of antibiotic prescriptions in Chinese primary health care and the impact of the COVID-19 pandemic: a typically descriptive and longitudinal database study in Yinchuan City. Front Pharmacol. 2022;13:861782. doi:10.3389/fphar.2022.861782
16. Butt AA, Navasero CS, Thomas B, et al. Antibiotic prescription patterns for upper respiratory tract infections in the outpatient Qatari population in the private sector. Int J Infect Dis. 2017;55:20–23. doi:10.1016/j.ijid.2016.12.004
17. Sulis G, Daniels B, Kwan A, et al. Antibiotic overuse in the primary health care setting: a secondary data analysis of standardised patient studies from India, China and Kenya. BMJ Glob Health. 2020;5(9):e003393. doi:10.1136/bmjgh-2020-003393
18. Saleem Z, Saeed H, Hassali MA, et al. Pattern of inappropriate antibiotic use among hospitalized patients in Pakistan: a longitudinal surveillance and implications. Antimicrob Resist Infect Control. 2019;8:188. doi:10.1186/s13756-019-0649-5
19. Dekker AR, Verheij TJ, van der Velden AW. Inappropriate antibiotic prescription for respiratory tract indications: most prominent in adult patients. Fam Pract. 2015;32(4):401–407. doi:10.1093/fampra/cmv019
20. Bianco A, Papadopoli R, Mascaro V, Pileggi C, Pavia M. Antibiotic prescriptions to adults with acute respiratory tract infections by Italian general practitioners. Infect Drug Resist. 2018;11:2199–2205. doi:10.2147/IDR.S170349
21. Young EH, Panchal RM, Yap AG, Reveles KR. National trends in oral antibiotic prescribing in United States physician offices from 2009 to 2016. Pharmacotherapy. 2020;40(10):1012–1021. doi:10.1002/phar.2456
22. Obakiro SB, Napyo A, Wilberforce MJ, et al. Are antibiotic prescription practices in Eastern Uganda concordant with the national standard treatment guidelines? A cross-sectional retrospective study. J Glob Antimicrob Resist. 2022;29:513–519. doi:10.1016/j.jgar.2021.11.006
23. Muhie OA. Antibiotic use and resistance pattern in Ethiopia: systematic review and meta-analysis. Int J Microbiol. 2019;2019:2489063. doi:10.1155/2019/2489063
24. National Bureau of statistics. National health service in China; 2019. Available from: https://data.stats.gov.cn/easyquery.htm?cn=C01.
25. National Health Commission of the People’s Republic of China. Statistical bulletin on China’s health development; 2020. Available from: http://www.nhc.gov.cn/guihuaxxs/s10743/202107/af8a9c98453c4d9593e07895ae0493c8.shtml.
26. Wang J, Wang P, Wang X, Zheng Y, Xiao Y. Use and prescription of antibiotics in primary health care settings in China. JAMA Intern Med. 2014;174(12):1914–1920. doi:10.1001/jamainternmed.2014.5214
27. Zhao H, Wei L, Li H, et al. Appropriateness of antibiotic prescriptions in ambulatory care in China: a nationwide descriptive database study. Lancet Infect Dis. 2021;21(6):847–857. doi:10.1016/S1473-3099(20)30596-X
28. Zhang JS, Liu G, Zhang WS, et al. Antibiotic usage in Chinese children: a point prevalence survey. World J Pediatr. 2018;14(4):335–343. doi:10.1007/s12519-018-0176-0
29. Chang Y, Chusri S, Sangthong R, et al. Clinical pattern of antibiotic overuse and misuse in primary healthcare hospitals in the southwest of China. PLoS One. 2019;14(6):e0214779. doi:10.1371/journal.pone.0214779
30. He P, Sun Q, Shi L, Meng Q. Rational use of antibiotics in the context of China’s health system reform. BMJ. 2019;365:l4016. doi:10.1136/bmj.l4016
31. Xiao Y, Li L. Legislation of clinical antibiotic use in China. Lancet Infect Dis. 2013;13(3):189–191. doi:10.1016/S1473-3099(13)70011-2
32. Xiao Y, Li L. China’s national plan to combat antimicrobial resistance. Lancet Infect Dis. 2016;16(11):1216–1218. doi:10.1016/S1473-3099(16)30388-7
33. Wushouer H, Tian Y, Guan XD, Han S, Shi LW. Trends and patterns of antibiotic consumption in China’s tertiary hospitals: based on a 5 year surveillance with sales records, 2011–2015. PLoS One. 2017;12(12):e0190314. doi:10.1371/journal.pone.0190314
34. Yin J, Li Q, Sun Q. Antibiotic consumption in Shandong Province, China: an analysis of provincial pharmaceutical centralized bidding procurement data at public healthcare institutions, 2012–16. J Antimicrob Chemother. 2018;73(3):814–820. doi:10.1093/jac/dkx469
35. Zhu Y, Qiao Y, Dai R, Hu X, Li X. Trends and patterns of antibiotics use in China’s Urban tertiary hospitals, 2016–19. Front Pharmacol. 2021;12:757309. doi:10.3389/fphar.2021.757309
36. Xiao Y. Antimicrobial stewardship in China: systems, actions and future strategies. Clin Infect Dis. 2018;67(suppl_2):S135–S141. doi:10.1093/cid/ciy641
37. Fossum GH, Lindbaek M, Gjelstad S, Dalen I, Kvaerner KJ. Are children carrying the burden of broad-spectrum antibiotics in general practice? Prescription pattern for paediatric outpatients with respiratory tract infections in Norway. BMJ Open. 2013;3(1):e002285. doi:10.1136/bmjopen-2012-002285
38. Chem ED, Anong DN, Akoachere JKT. Prescribing patterns and associated factors of antibiotic prescription in primary health care facilities of Kumbo East and Kumbo West Health Districts, North West Cameroon. PLoS One. 2018;13(3):e0193353. doi:10.1371/journal.pone.0193353
39. Okoro RN, Nmeka C, Erah PO. Antibiotics prescription pattern and determinants of utilization in the national health insurance scheme at a Tertiary Hospital in Nigeria. Afr Health Sci. 2019;19(3):2356–2364. doi:10.4314/ahs.v19i3.8
40. Almansoori N, Parag N. Antibiotic prescribing patterns in emergency department at Regional Hospital in South Africa. Afr Health Sci. 2021;21(4):1651–1661. doi:10.4314/ahs.v21i4.19
41. Ji L, Yoshida S, Kawakami K. Trends and patterns in antibiotic prescribing for adult outpatients with acute upper respiratory tract infection in Japan, 2008–2018. J Infect Chemother. 2021;27(11):1584–1590. doi:10.1016/j.jiac.2021.07.001
42. Quaegebeur A, Brunard L, Javaudin F, et al. Trends and prediction of antimicrobial susceptibility in urinary bacteria isolated in European emergency departments: the EuroUTI 2010–2016 study. J Antimicrob Chemother. 2019;74(10):3069–3076. doi:10.1093/jac/dkz274
43. Zhao W, Wang B, Yu G. Antibiotic resistance genes in China: occurrence, risk, and correlation among different parameters. Environ Sci Pollut Res Int. 2018;25(22):21467–21482. doi:10.1007/s11356-018-2507-z
44. Bolstad AI, Saetre MM, Aasgaard AS, Bunaes DF. Shift in antibiotic prescription at a University Dental Clinic in Norway 2013–2017. Eur J Oral Sci. 2020;128(6):518–525. doi:10.1111/eos.12741
45. Choi YY, Lee KH. Changes in antibiotic prescription after tooth extraction: a population-based study from 2002 to 2018. Int Dent J. 2021;71(6):491–499. doi:10.1016/j.identj.2021.01.010
46. Zhu NJ, McLeod M, McNulty CAM, Lecky DM, Holmes AH, Ahmad R. Trends in antibiotic prescribing in out-of-hours primary care in England from January 2016 to June 2020 to understand behaviours during the first wave of COVID-19. Antibiotics. 2021;10(1):32. doi:10.3390/antibiotics10010032
47. Wilkinson A, Ebata A, MacGregor H. Interventions to reduce antibiotic prescribing in LMICs: a scoping review of evidence from human and animal health systems. Antibiotics. 2018;8(1):2. doi:10.3390/antibiotics8010002
48. Hang WY, Xue D, Liu SX, Fang PQ. Hospital Administration.
49. World Health Organization. International statistical classification of diseases and related health problems 10th revision. Available from: https://icd.who.int/browse10/2016/en.
50. World Health Organization. WHO Access Watch. Reserve (AWaRe) classification of antibiotics for evaluation and monitoring of use, 2021. Geneva: World Health Organization; 2021. Available from: https://apps.who.int/iris/bitstream/handle/10665/345533/WHO-MHP-HPS-EML-2021.02-eng.pdf.
51. Wang YY, Du P, Huang F, et al. Antimicrobial prescribing patterns in a large tertiary hospital in Shanghai, China. Int J Antimicrob Agents. 2016;48(6):666–673. doi:10.1016/j.ijantimicag.2016.09.008
52. National Health Commission of the People’s Republic of China. Guiding principle of clinical use of antibiotics in 2015; 2015. Available from: http://www.nhc.gov.cn/ewebeditor/uploadfile/2015/09/20150928170007470.pdf.
53. Centers for Disease Control and Prevention. Antibiotic prescribing and use in doctor’s offices; 2017. Available from: https://www.cdc.gov/antibiotic-use/community/for-hcp/outpatient-hcp/adult-treatment-rec.html.
54. Akhtar S, Al-Abkal J, Alroughani R. Joinpoint regression analysis of trends in multiple sclerosis incidence in Kuwait: 1980–2019. Neuroepidemiology. 2020;54(6):472–481. doi:10.1159/000511205
55. Ma S, Liu Q, Zhang Y. A prediction method of fire frequency: based on the optimization of SARIMA model. PLoS One. 2021;16(8):e0255857. doi:10.1371/journal.pone.0255857
56. Swapnarekha H, Behera HS, Nayak J, Naik B, Kumar PS. Multiplicative holts winter model for trend analysis and forecasting of COVID-19 spread in India. SN Comput Sci. 2021;2(5):416. doi:10.1007/s42979-021-00808-0
57. Chatfield C. The holt‐winters forecasting procedure. Appl Stat. 1978;27(3):264–279. doi:10.2307/2347162
58. Wang S, Wei F, Li H, Wang Z, Wei P. Comparison of SARIMA model and Holt-Winters model in predicting the incidence of Sjogren’s syndrome. Int J Rheum Dis. 2022;25(11):1263–1269. doi:10.1111/1756-185X.14417
59. Fukushige M, Ngo NH, Lukmanto D, Fukuda S, Ohneda O. Effect of the COVID-19 pandemic on antibiotic consumption: a systematic review comparing 2019 and 2020 data. Front Public Health. 2022;10:946077. doi:10.3389/fpubh.2022.946077
60. Andrews A, Budd EL, Hendrick A, et al. Surveillance of antibacterial usage during the COVID-19 pandemic in England, 2020. Antibiotics. 2021;10(7):841. doi:10.3390/antibiotics10070841
61. Nicieza Garcia ML, Perez Solis P, Gomez de Ona C, Suarez Gil P, Rolle Sonora V, Suarez Mier B. Consumo de antibióticos en atención primaria en población adulta de Asturias durante el periodo 2014-2020 [Antibiotic consumption in primary care in the adult population of Asturias during 2014–2020 period]. Aten Primaria. 2022;54(3):102261. Romanian. doi:10.1016/j.aprim.2021.102261
62. Yau JW, Thor SM, Tsai D, Speare T, Rissel C. Antimicrobial stewardship in rural and remote primary health care: a narrative review. Antimicrob Resist Infect Control. 2021;10(1):105. doi:10.1186/s13756-021-00964-1
63. Li X, Lu J, Hu S, et al. The primary health-care system in China. Lancet. 2017;390(10112):2584–2594. doi:10.1016/S0140-6736(17)33109-4
64. Xue H, Shi Y, Huang L, et al. Diagnostic ability and inappropriate antibiotic prescriptions: a quasi-experimental study of primary care providers in rural China. J Antimicrob Chemother. 2019;74(1):256–263. doi:10.1093/jac/dky390
65. Chang Y, Sangthong R, McNeil EB, Tang L, Chongsuvivatwong V. Effect of a computer network-based feedback program on antibiotic prescription rates of primary care physicians: a cluster randomized crossover-controlled trial. J Infect Public Health. 2020;13(9):1297–1303. doi:10.1016/j.jiph.2020.05.027
66. Yang J, Cui Z, Liao X, et al. Effects of a feedback intervention on antibiotic prescription control in primary care institutions based on a health information system: a cluster randomized cross-over controlled trial. J Glob Antimicrob Resist. 2023;33:51–60. doi:10.1016/j.jgar.2023.02.006
67. Ahiabu MA, Tersbol BP, Biritwum R, Bygbjerg IC, Magnussen P. A retrospective audit of antibiotic prescriptions in primary health-care facilities in Eastern Region, Ghana. Health Policy Plan. 2016;31(2):250–258. doi:10.1093/heapol/czv048
68. Amaha ND, Berhe YH, Kaushik A. Assessment of inpatient antibiotic use in Halibet National Referral Hospital using WHO indicators: a retrospective study. BMC Res Notes. 2018;11(1):904. doi:10.1186/s13104-018-4000-7
69. Bo ZM, Tan WK, Chong CSC, et al. Respiratory microorganisms in acute pharyngitis patients: identification, antibiotic prescription patterns and appropriateness, and antibiotic resistance in private primary care, central Malaysia. PLoS One. 2022;17(11):e0277802. doi:10.1371/journal.pone.0277802
70. Md Rezal RS, Hassali MA, Alrasheedy AA, Saleem F, Md Yusof FA, Godman B. Physicians’ knowledge, perceptions and behaviour towards antibiotic prescribing: a systematic review of the literature. Expert Rev Anti Infect Ther. 2015;13(5):665–680. doi:10.1586/14787210.2015.1025057
71. Guan X, Tian Y, Song J, Zhu D, Shi L. Effect of physicians’ knowledge on antibiotics rational use in China’s county hospitals. Soc Sci Med. 2019;224:149–155. doi:10.1016/j.socscimed.2019.01.049
72. Fink G, D’Acremont V, Leslie HH, Cohen J. Antibiotic exposure among children younger than 5 years in low-income and middle-income countries: a cross-sectional study of nationally representative facility-based and household-based surveys. Lancet Infect Dis. 2020;20(2):179–187. doi:10.1016/S1473-3099(19)30572-9
73. Zhang Z, Hu Y, Zou G, et al. Antibiotic prescribing for upper respiratory infections among children in rural China: a cross-sectional study of outpatient prescriptions. Glob Health Action. 2017;10(1):1287334. doi:10.1080/16549716.2017.1287334
74. Yaeger JP, Temte JL, Hanrahan LP, Martinez-Donate P. Roles of clinician, patient, and community characteristics in the management of pediatric upper respiratory tract infections. Ann Fam Med. 2015;13(6):529–536. doi:10.1370/afm.1856
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.