Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Treatment Patterns for Chronic Obstructive Pulmonary Disease (COPD) in the United States: Results from an Observational Cross-Sectional Physician and Patient Survey
Authors Mannino D ![]() , Siddall J, Small M, Haq A
, Siddall J, Small M, Haq A ![]() , Stiegler M
, Stiegler M ![]() , Bogart M
, Bogart M
Received 23 September 2021
Accepted for publication 28 February 2022
Published 6 April 2022 Volume 2022:17 Pages 749—761
DOI https://doi.org/10.2147/COPD.S340794
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
David Mannino,1 James Siddall,2 Mark Small,2 Adam Haq,2 Marjorie Stiegler,3 Michael Bogart3
1Department of Medicine, University of Kentucky, Lexington, KY, USA; 2Respiratory DSP Franchise, Adelphi Real World, Bollington, UK; 3US Value Evidence and Outcomes, GlaxoSmithKline plc, Durham, NC, USA
Correspondence: Michael Bogart, US Value Evidence and Outcomes, GlaxoSmithKline plc, 5 Moore Dr, Research Triangle Park, Durham, NC, USA, Tel +19198897413, Email [email protected]
Purpose: There is a high prevalence of chronic obstructive pulmonary disease (COPD) in the United States (US). Although guidelines are available for the treatment of COPD, evidence suggests that management of COPD in clinical practice is not always aligned with this guidance. This study aimed to further understand the current use of COPD maintenance medication in the US.
Patients and Methods: This study was an analysis of data from the Adelphi Respiratory Disease Specific Programme (DSP™) 2019. Point-in-time data were collected from participating US physicians and their COPD patients. Physicians were either primary care physicians (PCPs) or pulmonologists, with a minimum workload of ≥ 3 COPD patients per month. Patients were aged ≥ 18 years with a physician-confirmed diagnosis of COPD.
Results: In total, 171 physicians completed the survey (92 PCPs and 79 pulmonologists). Mean patient age was 66.4 years, 45% were female, with moderate COPD in 49.4% of patients and severe/very severe in 19.3%. Pulmonologists more frequently prescribed dual bronchodilation and triple therapy than PCPs, whereas inhaled corticosteroid/long-acting β2-agonist was more frequently prescribed by PCPs than pulmonologists. For both physician types, the most common reason for prescribing their patients’ current treatment was 24-hour symptom relief. The majority of PCPs (70.1%) and pulmonologists (71.9%) reported referring to COPD guidelines when making treatment decisions.
Conclusion: Prescribing patterns for COPD patients were found to differ between PCPs and pulmonologists. Improved physician understanding of how to tailor treatment for each patient, based on current symptoms and exacerbation risk, could help optimize patient care in COPD.
Keywords: COPD, inhaled corticosteroids, long-acting β2-agonist, long-acting muscarinic antagonist, maintenance therapy, survey
Plain Language Summary
Patients with COPD are usually treated by a primary care physician (PCP) and/or a specialist doctor (pulmonologist). These doctors typically follow guideline recommendations on how to choose the best treatment based on symptoms and frequency/severity of exacerbations experienced by each of their patients with COPD. We designed a study using data from a survey completed by pulmonologists and PCPs to understand what COPD treatments they prescribe and whether they follow guidelines when selecting treatments for their patients.
In total, 171 doctors completed the survey (92 PCPs and 79 pulmonologists) and provided anonymous information about 800 of their patients with COPD. The survey showed that patients treated by pulmonologists are more often prescribed combination treatments that have more recently been introduced and are now recommended by guidelines. Patients being treated by PCPs are more often prescribed an inhaled corticosteroid combined with a long-acting bronchodilator, irrespective of the patients’ current COPD symptoms and risk of having an exacerbation. Both types of doctor indicated that their most common reason for prescribing a treatment was to provide patients with 24-hour symptom relief. Most PCPs (70.1%) and pulmonologists (71.9%) reported referring to COPD guidelines when deciding on a treatment for their patients.
The study results suggest that some doctors may not follow guideline recommendations exactly when personalizing treatment regimens for patients with COPD. Personalizing the medication choice to properly treat each patient is important, and these guidelines can help doctors choose the best treatment that will control COPD and improve patients’ daily lives.
Introduction
Despite the availability of international and national treatment guidelines for chronic obstructive pulmonary disease (COPD), evidence suggests that available therapies may not be utilized to their full potential to optimize disease management and outcomes for patients.1–3 COPD treatment guidelines are frequently updated, which presents a challenge for physicians managing patients with COPD. Furthermore, several new COPD medications have been approved in recent years.4,5 Current recommendations from the Global Initiative for Chronic Obstructive Lung Disease (GOLD) indicate that each treatment regimen needs to be individualized, as the relationship between symptom severity, airflow limitation, and severity of exacerbations differs between patients.4 Pharmacotherapy based on the patient’s GOLD group (symptom severity and number/severity of exacerbations in the last year) can include a long-acting muscarinic antagonist (LAMA) or long-acting β2-agonist (LABA), alone or in combination, with addition of an inhaled corticosteroid (ICS) if indicated by the patient’s exacerbation history in the past year (≥2 moderate or resulting in hospitalization). Triple inhaled therapy of LABA, LAMA, and ICS (ie LABA/LAMA/ICS) improves lung function, symptoms, health status, and reduces exacerbations compared with LABA/ICS, LAMA/LABA, or LAMA monotherapy.4
To ensure optimal management and outcomes for patients with COPD, it is important to understand how treatment guidelines are translated into real-world clinical practice and identify barriers to the implementation of best practice. Historical data from observational studies have shown that COPD management in routine clinical practice is not always aligned with guideline recommendations.6–11
COPD has a high prevalence in the US. During 2014–2015, 5.9% of adults (more than 15.9 million) reported having been told by their healthcare professional that they have COPD, and the average age-adjusted mortality rate for COPD was 39.7 per 100,000 population.12 There is a lack of published evidence on current treatment patterns in real-world clinical practice in the US, and how these prescribing patterns align with COPD guidelines, such as GOLD.4 In addition, little information is available on the reasoning behind prescribing behaviors for specific COPD medications and classes by US primary care physicians (PCPs) and pulmonologists.
This observational study used data from a 2019 survey of US PCPs and pulmonologists, and their patients, to better understand the current use of COPD maintenance medication and the factors guiding treatment choices.
Methods
Study Design
This analysis utilized secondary data created from a survey of COPD patients and their physicians in the US – the Respiratory Disease Specific Programme (DSP)TM (2019 version). The DSP is an independent, multi-subscriber, point-in-time physician and (voluntary) patient survey. The DSP methodology has been published and validated previously.13 The DSPs are established, large, observational surveys of routine clinical practice, designed to capture cross-sectional real-world data, that accurately reflect current disease burden, patient characteristics, care pathways, and associated treatment practices for a range of common chronic diseases, including COPD.1,14,15
The DSP surveys were completed between July and December 2019. Each participating physician completed a patient record form for consecutive COPD patients. The patients were asked to complete a COPD Assessment Test (CAT) questionnaire, in which they provided their CAT score on the survey date. This score was used to derive their GOLD classification (A–D). No other patient-reported data were included in this analysis. Other information was recorded on the survey date from available medical history. No follow-up data were collected. Importantly, all data analyzed in this study were collected prior to the emergence of COVID-19.
The DSP survey was conducted in accordance with the amended Declaration of Helsinki, adhering to the ICC/ESOMAR International code on observational research, and Health Insurance Portability and Accountability Act (HIPAA) guidelines. The survey received ethical exemption determination by the Western Institutional Review Board, a central international review board for the US (Study Number: 1-1211337-1). Patients provided written consent before completing the questionnaire. All data from physicians and patients were anonymized.
Physician and Patient Criteria
Data were collected from US PCPs and pulmonologists, and their patients. Target physicians were identified by Adelphi preferred and audited local US DSP fieldwork team from public lists of healthcare professionals according to pre-defined selection criteria. PCPs and pulmonologists were required to manage ≥3 COPD patients per month and be actively involved in the management of COPD patients. This screening criteria threshold was chosen to ensure that data were collected from a sample of physicians who regularly treat patients with COPD, whilst not limiting the sample of physicians to those who have a very high COPD workload/specialism. Patients were required to be aged ≥18 years with a physician-confirmed diagnosis of COPD (including emphysema and/or chronic bronchitis). Note, International Classification of Disease (ICD) codes were not captured in this study. Patients with a concomitant asthma diagnosis (as confirmed by the physician) were excluded from this analysis, as were patients currently enrolled in a clinical study. To avoid selection bias, physicians were asked to provide data for a consecutive series of patients; this was a pragmatic sample as the program criteria did not require patient samples to be representative of the population in terms of race, income, social class, or age.
Study Outcomes and Data Sources
The analytical considerations for each of the research objectives are described below. The primary objective was to describe the current prescribing patterns for US PCPs and pulmonologists and their reasons for prescribing specific classes of COPD therapy. Data were extracted from the DSP dataset on the treatments prescribed to COPD patients by PCPs and pulmonologists, and the reasons, or combinations of reasons, given for prescribing each specific therapy class. Descriptive statistics were generated, and data tables produced showing the frequency and percentage of patients within each response. Patients could be treated by multiple physician types; however, the data on current treatments were grouped according to the physician type (PCP or pulmonologist) that provided data in the survey.
The secondary objectives were 1) to describe the patient types prescribed each class of COPD therapy and 2) to assess which treatment guidelines US physicians refer to, and whether their treatment choices are aligned with guideline recommendations. Data were extracted from the DSP dataset from physician-completed surveys, which provided demographic and clinical characteristics on the patients included. Where appropriate and depending on the variable, the timeframe for collection of information was either the survey date (for age, sex, employment status, physician-perceived severity of COPD) or based on available medical records (comorbidities, body mass index; Charlson comorbidity index, clinical COPD assessments).
To assess whether physicians align to guideline recommendations, physician responses to the following two questions in the DSP were extracted: “Have you referred to guidelines when treating COPD patients?”, with a nominal response of 1) Yes or 2) No. Those answering yes were asked a follow-up question: “What is the name of the guidelines you have referred to?”, with an open response requested in the survey. A subgroup of physicians was provided with four patient profiles related to symptom presentation and exacerbation history/risk and asked to provide their most likely treatment choice for each of the patients.
Results
Study Population Demographics and Disease Characteristics
Figure 1 shows the overall sample captured in the Respiratory DSP 2019 survey. Invitations to participate in the DSP were sent to 118 PCPs and 198 pulmonologists; 171 physicians completed the survey (n = 92 PCPs, n = 79 pulmonologists). In total, PCPs and pulmonologists completed record forms for 408 and 392 patients, respectively. Of the total sample of 800 patients, 451 (PCP: 255, pulmonologist: 196) completed the voluntary patient self-completion questionnaire. Table 1 summarizes patient demographics and disease characteristics for the overall patient population (N = 800) and according to the class of COPD treatment received. The overall mean age of the population was 66.4 years and 45% of participants were female. In total, 56% of patients were retired and 87% were current or former smokers. Almost half of the patients were judged by their physician to have moderate COPD (49.4%; Table 1), with severe/very severe in 19.3%. The physician-perceived severity of COPD (Table 2) was worse for pulmonologist patients than for PCP patients (more patients perceived as severe or very severe). Patient characteristics according to the physician type also showed that employment was affected by COPD in a higher proportion of pulmonologist patients than PCP patients (Table 2).
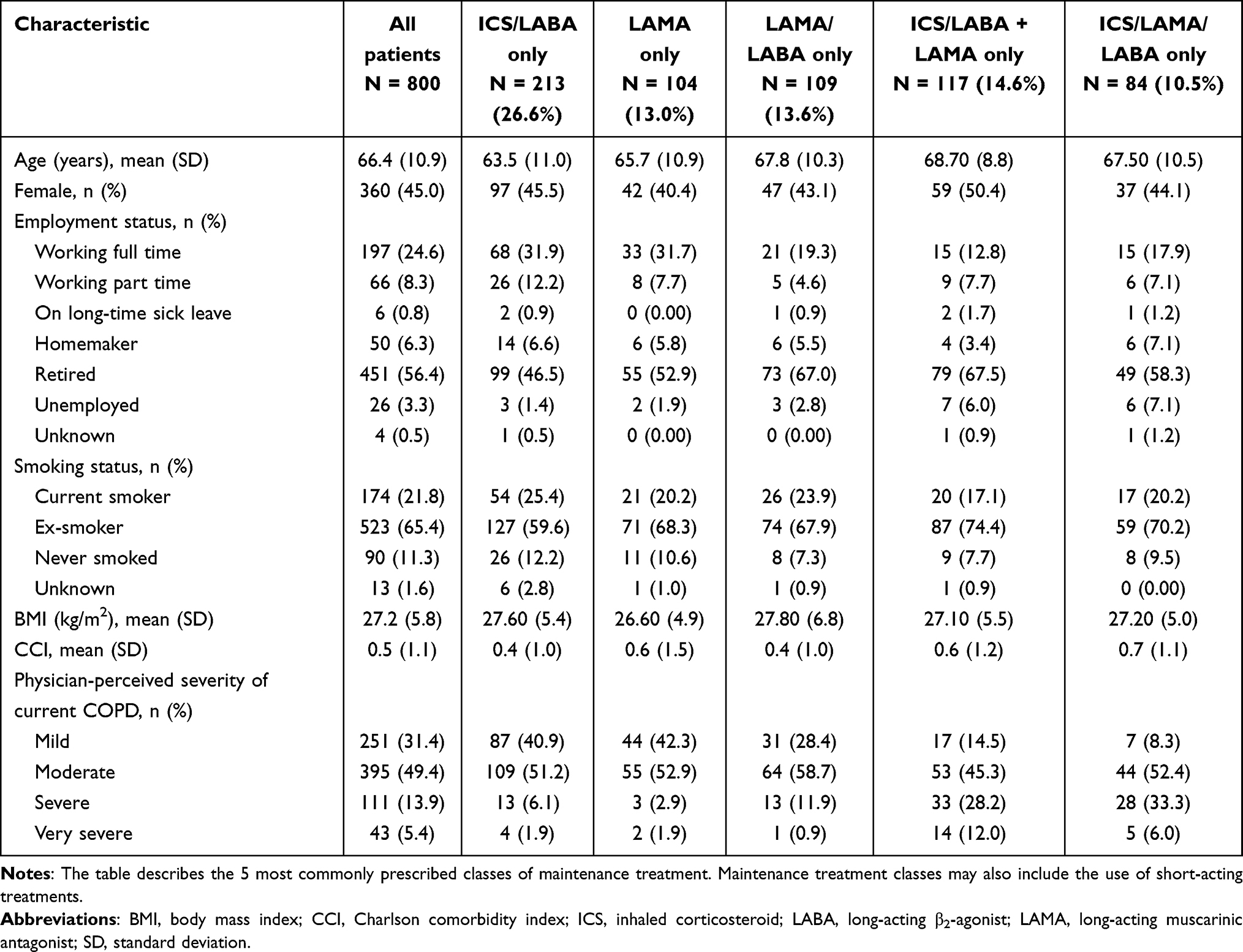 |
Table 1 Patient and Disease Characteristics According to the Class of COPD Treatment Received |
 |
Table 2 Patient and Disease Characteristics According to Physician Type Providing Data in the Survey |
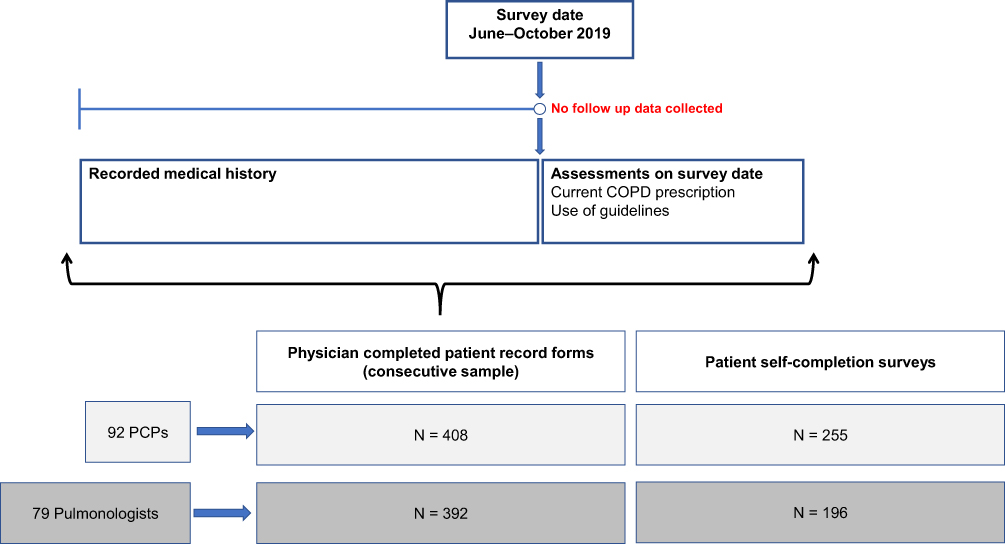 |
Figure 1 Respiratory DSP survey: population sampled and data captured. Abbreviations: COPD, chronic obstructive pulmonary disease; DSP, Disease Specific Programme; PCP, primary care physician. |
In total, 40.9% and 42.3% of patients on ICS/LABA only or LAMA only, respectively, were reported as having mild disease (Table 1). Table S1 shows further details provided by physicians on their patients’ COPD characteristics according to COPD treatment received.
COPD Medications Prescribed According to Physician Type
Table 3 summarizes the COPD medications that patients were receiving, according to physician type. A lower proportion of patients consulting a pulmonologist were prescribed ICS/LABA only, than those consulting a PCP (21.7% vs 31.4% of patients). Compared with PCPs, pulmonologists prescribed for a higher proportion of their patients LAMA/LABA only (16% vs 12% of patients), single-inhaler ICS/LAMA/LABA triple therapy (14.0% vs 7.1% of patients), and ICS/LABA + LAMA triple therapy (13.7% vs 15.6% of patients). Prescription of LAMA monotherapy was similar between patients treated by PCPs and pulmonologists (14.5% vs 11.5% of patients, respectively).
 |
Table 3 COPD Medications Prescribed by Pulmonologists and Primary Care Physicians |
PCPs and pulmonologists provided information on the current COPD treatment regimens received by their patients and identified the type of provider initiating the treatment. Figure 2 shows the prescriber type initiating the current treatment regimens received by patients. The majority of patients (58.8%) consulting a PCP had their current COPD treatment regimen initiated by a PCP. Current treatment regimens were initiated by a pulmonologist in only 31.9% of patients consulting a PCP. In total, 87.2% of patients consulting a pulmonologist had their current treatment regimen initiated by a pulmonologist, and 8.2% of these patients had their treatment initiated by a PCP. According to subjective evaluation by PCPs and pulmonologists, PCPs reported that 70.3% of their patients were very or completely adherent to their current treatment regimen, compared with 69.9% of pulmonologist patients (Figure 3).
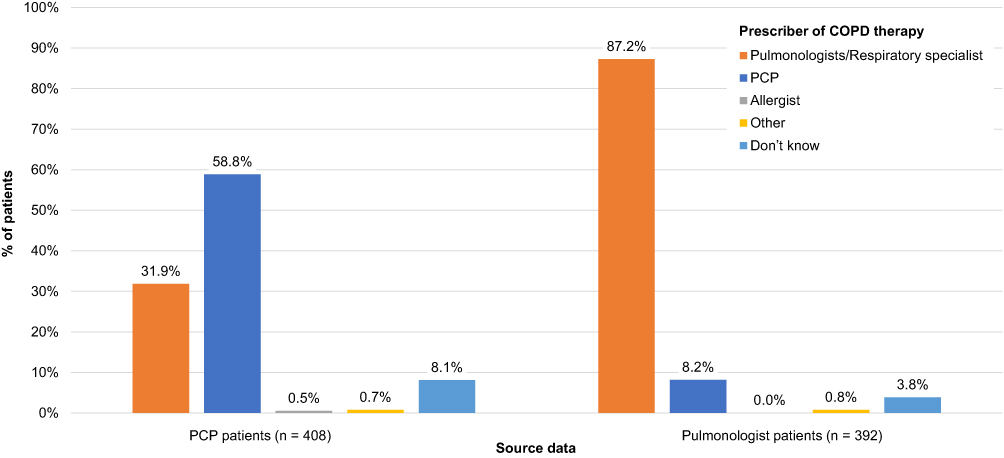 |
Figure 2 Prescriber of patients’ current COPD treatment regimen. Abbreviations: COPD, chronic obstructive pulmonary disease; PCP, primary care physician. Note: As patients could be treated by multiple physician types, the figure refers to the physician type (PCP or pulmonologist) who provided data in the survey. |
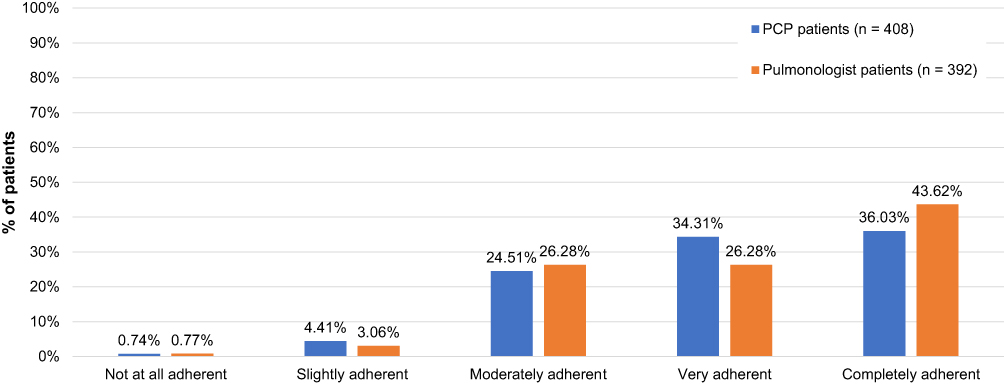 |
Figure 3 Patient adherence to prescribed COPD treatment (physician reported). Abbreviations: COPD, chronic obstructive pulmonary disease; PCP, primary care physician. |
Factors Influencing Physician’s COPD Treatment Choices
The most common reasons given by pulmonologists and PCPs for their current treatment choice (Figure 4A) were symptom relief, including 24-hour symptom relief (80% of PCP-treated patients; 76% of pulmonologist-treated patients), improvement of shortness of breath (69% and 69%, respectively), and daytime symptom relief (59% and 64%, respectively).
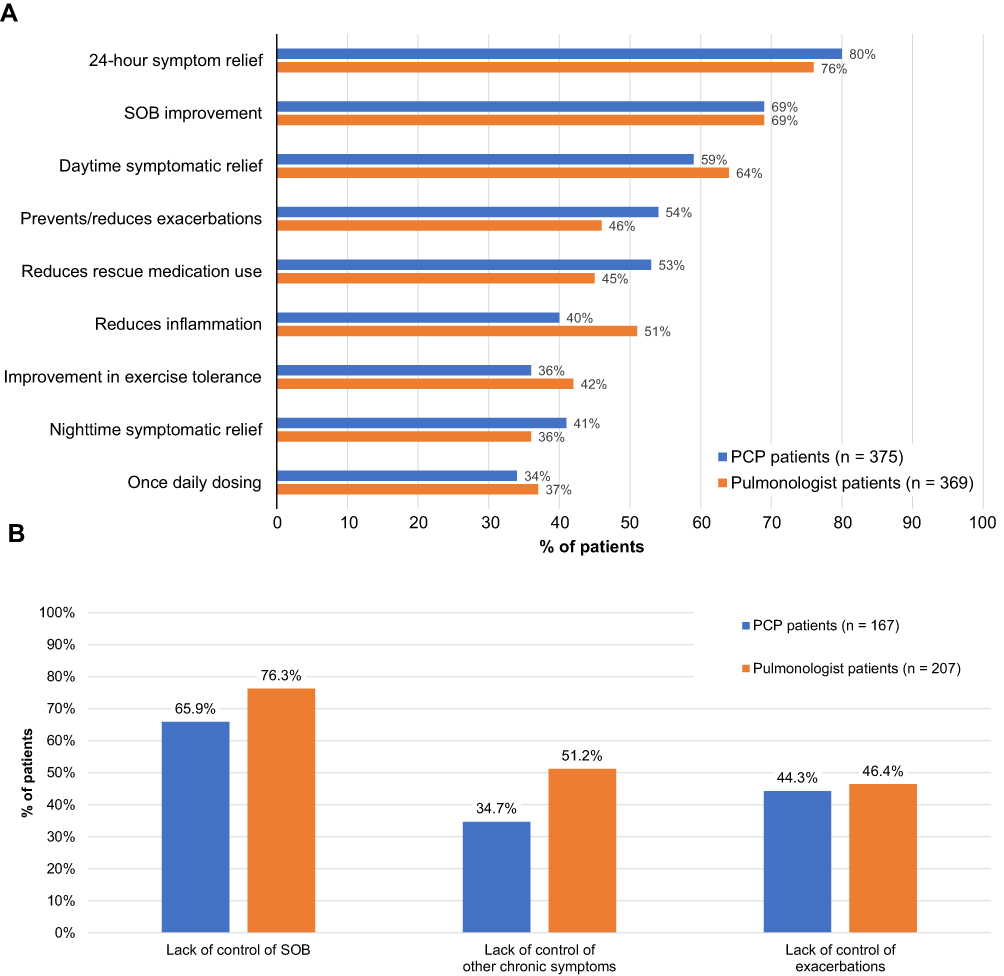 |
Figure 4 Most common reasons (>25% of responses) cited by PCPs and pulmonologists for (A) choice of current prescribed treatment and (B) a change to current treatment. Abbreviations: COPD, chronic obstructive pulmonary disease; PCP, primary care physician; SOB, shortness of breath. |
The most common reason for a change to a patient’s current treatment (Figure 4B) was lack of control of shortness of breath with the previous treatment (65.9% of PCP-treated patients and 76.3% of pulmonologist-treated patients).
Treatment Decisions According to Treatment Guidelines and Patient Profiles
A randomly assigned subset of physicians (n = 43 PCPs, n = 32 pulmonologists) were surveyed about their use of COPD treatment guidelines and treatment choices for different patient profiles. Physicians were presented with four patient profiles: patient 1: maintenance-naïve, symptomatic COPD (no asthma), significant exacerbation risk; patient 2: maintenance-naïve, symptomatic COPD (no asthma), recent exacerbation history; patient 3: symptomatic COPD (no asthma), no exacerbations in the past 12 months, moderate dyspnea; patient 4: symptomatic COPD (no asthma), no exacerbations in the past 12 months, severe dyspnea. Table 4 shows the most common treatment choices selected by PCPs and pulmonologists when presented with these four different profiles. Pulmonologists’ treatment choices differed markedly across the four patient profiles. By contrast, PCPs most frequently selected ICS/LABA for each of the four patient profiles.
 |
Table 4 Patient Profiles and Most Frequently Selected Classes of COPD Therapy (in >5% of Patients in Either Arm) |
Among physicians responding to questions about their use of treatment guidelines (Figure 5), 79.1% of PCPs and 71.9% of pulmonologists reported that they refer to guidelines when making treatment decisions. The majority of physicians who reported referring to guidelines stated that they most frequently consult the GOLD guidelines (PCPs 79.4%; pulmonologists 91.3%).
 |
Figure 5 Physician-reported referral to COPD guidelines. Responses from PCPs (n = 43) and pulmonologists (n = 32) surveyed. Abbreviations: ATS, American Thoracic Society; COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease. Note: The righthand figure includes responses from the 34 PCPs and 23 pulmonologists who said they referred to guidelines when treating COPD patients. |
Discussion
This study analyzed a real-world dataset of physicians and their patients with COPD and provides new insights into the use of COPD maintenance therapies in the US. COPD treatment patterns were found to vary by prescriber type: pulmonologists were more likely to prescribe dual bronchodilation and triple therapy than PCPs. This difference in prescribing patterns is perhaps explained by the fact that pulmonologists likely deal with a more severe caseload of COPD patients.
GOLD treatment guidelines currently recommend the use of ICS treatment in combination with one or two long-acting bronchodilators, only in patients with a history of severe exacerbations and those with ≥2 moderate COPD exacerbations during the last year. ICS is, however, also recommended for patients whose symptoms are suggestive of asthma and for patients with a COPD and asthma overlap. For COPD patients with dyspnea, guidelines recommend the use of a LAMA/LABA combination over LABA or LAMA monotherapy. Guidelines recommend escalation to triple therapy with ICS/LAMA/LABA in patients with a history of one or more severe exacerbations in the past year.4,5 Despite these guideline recommendations, our study shows that an ICS-containing regimen was prescribed for the majority of patients and at a similar rate by PCPs and pulmonologists. This could be due to the PCPs’ familiarity and experience using ICS/LABAs, which have been long-standing treatment options in COPD, or possibly an uncertainty among PCPs in applying symptoms/exacerbation history to guide treatment choice or use of newer treatment options.
For most patients consulting a PCP at the survey date, their current COPD treatment was initiated by a PCP, rather than a pulmonologist, indicating that COPD patients in the US are more likely to be seen outside of specialist care. Many PCPs do not have easy access to pulmonary function testing to aid in the diagnosis and classification of COPD patients. The uptake of tools for patient-reported outcomes, such as the CAT or modified Medical Research Council scale, may also be low among PCPs. Therefore, they may not have the information needed to stratify patients and comply with best-practice treatment from evidence-based guidelines.4
The drivers of treatment decisions among the physicians sampled were related to sustained symptomatic control and improvement; improvement of dyspnea was a frequent reason identified by physicians for the current treatment choice and also for a change to a current treatment. It was surprising that exacerbation was not more highly used as a factor guiding treatment decisions, as a patient’s exacerbation history is an important factor in predicting and managing their future exacerbation risk.4 This highlights a potential need for further education among physicians on the importance of proactively managing exacerbation risk to provide continued protection from exacerbations. Current guidelines recommend that physicians should direct treatment to the predominant 'treatable COPD trait' rather than COPD severity.4 This highlights the importance of treatment based upon individual patient factors and uncovers another potential educational gap. Medication cost should also be considered, as treatment affordability may also play a role in treatment decisions, however, in this study, cost was not included in the list of factors influencing COPD treatment choices provided to the physicians. As well as physician factors, for example awareness of guideline recommendations, patient factors may also influence the management of their disease. In some cases, patients may be resistant to a change in COPD medication, possibly due to poor understanding of their disease or the severity of their symptoms.16 Treatment adherence is also an issue. Patients using their medication sporadically and lack of education on inhaler technique have been identified as possible factors contributing to clinical inertia in COPD.16
The results of this study also suggest a potential disconnect between physician perception of adherence to guidelines, and their actual prescribing patterns. The high rate of ICS use suggests that the guidelines are not being closely adhered to, despite many physicians reporting referral to guidelines in treatment.
Results from the patient profile scenarios also confirmed that treatment decisions, particularly by PCPs, do not always align with treatment guidelines. Pulmonologists’ treatment choices differed markedly across the four patient profiles, whereas PCPs most frequently selected ICS/LABA for each of the four patient profiles, irrespective of whether the patient was treatment-naïve, had symptom presentation, and had exacerbation risk. This suggests that further education among PCPs may be needed to highlight the importance of understanding of patient types when prescribing the most appropriate COPD therapy. It should also be noted that all four of the patient profile scenarios were classified as 'symptomatic COPD, no asthma'. However, as previously mentioned, a 'no asthma' characterization may not be clear cut in a real-world clinical practice setting. For example, patients may have a large degree of bronchodilator responsiveness, large variability in symptoms, or other characteristics that are suggestive of asthma and COPD overlap, or comorbid asthma.
This study has provided valuable insights into current treatment practices and adherence to guidelines among US physicians treating patients with COPD. In the future, it may be of value to repeat the survey at multiple time points to monitor new prescribing trends and further explore the barriers to optimizing care for patients with COPD, especially as new treatments are approved.
This study has a few limitations that should be mentioned. Patient and physician participation in the survey was not truly random; a willingness to participate and pragmatic geographical considerations may have influenced the sample. As a result, patients participating in the DSP may not reflect the general COPD population. Exclusion of patients with comorbid asthma also limits the generalizability of the findings. In addition, although COPD diagnosis was confirmed by a physician, spirometry testing was not confirmed, and it is possible that a small number of patients were incorrectly diagnosed. Physicians were asked to provide data for a consecutive series of patients to avoid selection bias; however, no formal patient selection verification procedures were in place. Finally, missing data on the clinical history of COPD and treatment history limit the conclusions that can be drawn about factors influencing treatment choices.
Conclusions
Prescribers utilize treatments for COPD at different rates; pulmonologists were more likely to prescribe dual bronchodilation and triple therapy than PCPs. When considering patient profiles, choices differed markedly for pulmonologists, whereas ICS/LABA was chosen by the highest proportion of PCPs regardless of patient symptom presentation and exacerbation risk. Physician education and improved understanding of patient types that benefit from each treatment pathway could help optimize patient care in COPD, particularly in the primary care setting.
Abbreviations
BMI, body mass index; CAT, COPD assessment test; CCI, Charlson comorbidity index; COPD, chronic obstructive pulmonary disease; DSP, Disease Specific Programme; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HIPAA, Health Insurance Portability and Accountability Act; ICD, International Classification of Disease; ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; LRA, leukotriene receptor antagonist; OCS, oral corticosteroid; PCP, primary care physician; PDE4i, phosphodiesterase-4 inhibitor; SABA, short-acting bronchodilator; SD, standard deviation.
Data Sharing Statement
The datasets supporting the results reported in this manuscript are not publicly available. Access to the raw data may be granted on reasonable request to the corresponding author dependent on the intended use and subject to third-party agreements.
Ethics Approval and Informed Consent
The survey received ethical exemption determination by the Western Institutional Review Board (study number: 1-1211337-1). Patients provided written consent before completing the voluntary patient self-completion. The survey was conducted in accordance with the amended Declaration of Helsinki and adhered to the ICC/ESOMAR International code on observational research, and Health Insurance Portability and Accountability Act (HIPAA) guidelines.
Acknowledgments
Editorial support (in the form of writing assistance, including preparation of the draft manuscript under the direction and guidance of the authors, collating and incorporating authors’ comments for each draft, assembling tables and figures, grammatical editing and referencing) was provided by Fiona Goodwin and Rebecca Cunningham of Aura, a division of Spirit Medical Communications Group Limited and was funded by GlaxoSmithKline. Trademarks are property of their respective owners. These data have previously been presented in abstract/poster form at the American College of Chest Physicians Congress 2020 (Mannino D, et al. Cross-sectional survey to assess chronic obstructive pulmonary disease (COPD) medication use by United States (US) physicians. CHEST 2020;158(4):A1776). doi:10.1016/j.chest.2020.08.1550.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by GlaxoSmithKline plc (study number 209577). The sponsor was involved in study conception and design, data interpretation, and the decision to submit the article for publication. The sponsor was also given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
Disclosure
The authors declare the following conflicts of interest during the last three years in relation to this article: DM is a former employee of GlaxoSmithKline and holds stocks/shares in GlaxoSmithKline; reports royalties from UptoDate and personal fees as a consultant for AstraZeneca. JS, M Small, and AH are employees of Adelphi Real World. Adelphi Real World received research funds from GlaxoSmithKline in relation to this study. M Stiegler and MB are employees of GlaxoSmithKline and hold stocks/shares in GlaxoSmithKline. The authors report no other conflicts of interest in this work.
References
1. Vestbo J, Vogelmeier CF, Small M, Siddall J, Fogel R, Kostikas K. Inhaled corticosteroid use by exacerbations and eosinophils: a real-world COPD population. Int J Chron Obstruct Pulmon Dis. 2019;14:853–861. doi:10.2147/COPD.S189585
2. Wallace AE, Kaila S, Bayer V, et al. Health care resource utilization and exacerbation rates in patients with COPD stratified by disease severity in a commercially insured population. J Manag Care Spec Pharm. 2019;25(2):205–217. doi:10.18553/jmcp.2019.25.2.205
3. Diette GB, Dalal AA, D’Souza AO, Lunacsek OE, Nagar SP. Treatment patterns of chronic obstructive pulmonary disease in employed adults in the United States. Int J Chron Obstruct Pulmon Dis. 2015;10:415–422. doi:10.2147/COPD.S75034
4. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease; 2021. Available from: https://goldcopd.org/gold-reports/.
5. Nici L, Mammen MJ, Charbek E, et al. Pharmacologic management of chronic obstructive pulmonary disease. An official American Thoracic Society clinical practice guideline. Am J Respir Crit Care Med. 2020;201(9):e56–e69. doi:10.1164/rccm.202003-0625ST
6. Fitch K, Iwasaki K, Pyenson B, Plauschinat C, Zhang J. Variation in adherence with Global Initiative for Chronic Obstructive Lung Disease (GOLD) drug therapy guidelines: a retrospective actuarial claims data analysis. Curr Med Res Opin. 2011;27(7):1425–1429. doi:10.1185/03007995.2011.583230
7. Asche CV, Leader S, Plauschinat C, et al. Adherence to current guidelines for chronic obstructive pulmonary disease (COPD) among patients treated with combination of long-acting bronchodilators or inhaled corticosteroids. Int J Chron Obstruct Pulmon Dis. 2012;7:201–209. doi:10.2147/COPD.S25805
8. Price D, West D, Brusselle G, et al. Management of COPD in the UK primary-care setting: an analysis of real-life prescribing patterns. Int J Chron Obstruct Pulmon Dis. 2014;9:889–905. doi:10.2147/COPD.S62750
9. Vestbo J, Vogelmeier C, Small M, Higgins V. Understanding the GOLD 2011 strategy as applied to a real-world COPD population. Respir Med. 2014;108(5):729–736. doi:10.1016/j.rmed.2014.03.002
10. Lopez-Campos JL, Navarrete BA, Soriano JB, et al. Determinants of medical prescriptions for COPD care: an analysis of the EPOCONSUL clinical audit. Int J Chron Obstruct Pulmon Dis. 2018;13:2279–2288. doi:10.2147/COPD.S160842
11. Gruffydd-Jones K, Brusselle G, Jones R, et al. Changes in initial COPD treatment choice over time and factors influencing prescribing decisions in UK primary care: a real-world study. NPJ Prim Care Resp Med. 2016;26:16002. doi:10.1038/npjpcrm.2016.2
12. Sullivan J, Pravosud V, Mannino DM, Siegel K, Choate R, Sullivan T. National and state estimates of COPD morbidity and mortality — United States, 2014-2015. Chronic Obstr Pulm Dis. 2018;5(4):324–333. doi:10.15326/jcopdf.5.4.2018.0157
13. Anderson P, Benford M, Harris N, Karavali M, Piercy J. Real-world physician and patient behaviour across countries: disease-specific programmes – a means to understand. Curr Med Res Opin. 2008;24(11):3063–3072. doi:10.1185/03007990802457040
14. Ding B, Small M. Treatment trends in patients with asthma-COPD overlap syndrome in a COPD cohort: findings from a real-world survey. Int J Chron Obstruct Pulmon Dis. 2017;15(12):1753–1763. doi:10.2147/COPD.S136314
15. Higgins V, Piercy J, Roughley A, et al. Trends in medication use in patients with type 2 diabetes mellitus: a long-term view of real-world treatment between 2000 and 2015. Diabetes Metab Syndr Obes. 2016;9:371–380. doi:10.2147/DMSO.S120101
16. Cooke CE, Sidel M, Belletti DA, Fuhlbrigge AL. Review: clinical inertia in the management of chronic obstructive pulmonary disease. COPD. 2012;9(1):73–80. doi:10.3109/15412555.2011.631957
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.