")
Back to Journals » Cancer Management and Research » Volume 11
Treatment of non-metastatic castration-resistant prostate cancer: focus on apalutamide
Authors Gul A, Garcia JA, Barata PC
Received 19 April 2019
Accepted for publication 15 July 2019
Published 1 August 2019 Volume 2019:11 Pages 7253—7262
DOI https://doi.org/10.2147/CMAR.S165706
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Harikrishna Nakshatri
Anita Gul,1 Jorge A Garcia,1 Pedro C Barata2
1Department of Hematology/Medical Oncology, Cleveland Clinic Taussig Cancer Institute, Cleveland, OH, USA; 2Tulane University, New Orleans, LA, USA
Abstract: Androgen deprivation therapy (ADT) is an important component of systemic therapy in advanced prostate cancer; however, resistance to ADT is inevitable. Three large studies demonstrated the efficacy of novel androgen receptor (AR)-targeted therapies in prolonging metastasis-free survival and time to symptomatic progression in patients with non-metastatic castration-resistant prostate cancer (nmCRPC). Enzalutamide and apalutamide have been approved by the FDA in the nmCRPC setting. This review discusses the role of AR and ADT in prostate cancer, mechanism of ADT resistance and the nmCRPC stage. In addition, pharmacologic characteristics and clinical development of apalutamide, role of apalutamide in nmCRPC, and ongoing clinical studies of apalutamide in different stages of prostate cancer are discussed.
Keywords: androgen receptor, non-metastatic castration-resistant prostate cancer, apalutamide, ARN-509, Phase III trials
Introduction
Prostate cancer is one of the most commonly diagnosed cancer in men in the United States with an estimated 164,690 new cases and 29,430 deaths in 2018.1 Most prostate cancer patients are diagnosed at a localized stage and are treated with definite radiotherapy, radical prostatectomy (RP), or active surveillance.2–4 About 40–50% of patients, who initially present with the localized disease eventually progress.5,6 Biochemical recurrence (BCR) is a clinical stage of prostate cancer in which patients present with a rising prostate-specific antigen (PSA) level, after initial definite local therapy and no evidence of metastasis on conventional imaging like radionuclide bone imaging, computed tomography (CT) scan or magnetic resonance imaging (MRI). Systemic treatment with androgen deprivation therapy (ADT) has an important role in the management of patients with BCR who are not candidate of salvage prostatectomy, salvage radiation therapy or who have BCR recurrence after salvage treatment. Early initiation of ADT in BCR reduces PSA level and delays time to metastatic disease.7 However, randomized controlled trials are lacking to demonstrate the impact of early ADT on overall survival (OS), prostate cancer-specific survival, and quality of life (QoL) in patients with BCR. Many patients who receive ADT for BCR eventually progress. The median duration of response to ADT in patients with non-metastatic prostate cancer is 19 months, after which many men progress to non-metastatic castrate-resistant prostate cancer (nmCRPC).8 The disease state in which patients have PSA recurrence only while on ADT without evidence of metastasis on conventional imaging including radionuclide bone imaging, CT scan, or MRI is defined as nmCRPC.9
This review discusses the role of AR in prostate cancer, mechanism of resistance to ADT, nmCRPC stage, the clinical development of apalutamide, pivotal trials evaluating apalutamide, enzalutamide, and darolutamide in nmCPRC, and the active clinical trials evaluating the role of apalutamide in different stages of prostate cancer.
Role of the androgen receptor (AR) and ADT in prostate cancer
The AR mediates the action of androgens by acting as a transcription factor.10 The AR consists of N-terminal domain, central DNA binding domain, and C terminal ligand binding domain (LBD).10 Testosterone, a weak ligand is converted by 5-alpha reductase to potent dihydrotestosterone (DHT) in prostate cells. When DHT binds to C terminal LBD of AR, conformational changes occur in AR and heat shock protein dissociates from AR.10 The androgen-AR complex forms a dimer and enters the nucleus where it binds to specific DNA sequences called androgen responsive elements and activates transcription.10,11 Charles and Huggins first recognized that prostate cancer cells thrive on androgens (testosterone and DHT) and ablation of androgens cause prostate cancer cells to undergo apoptosis and the cells who survive are arrested in the G1 phase of cell cycle.12 Since then, ADT has been the critical component of the management of prostate cancer for the last several decades which is achieved by suppression of gonadal androgens by gonadotrophin-releasing hormone (GnRH) agonist. Several mechanisms of ADT resistance have been proposed including incomplete blockade of AR, ligand activation by intra-tumoral androgen which activates AR signaling pathway despite castrate level of testosterone, amplification of AR gene, AR mutation, ligand-independent activation of ARr by oncogenes such as ERBB2 or HRAS which can cause increased mitogen-activated protein kinase signaling, and activation of other survival pathways including PI3K pathway.13–17
Non-metastatic castrate resistant prostate cancer
The incidence of nmCRPC in the United States is about 50,000–60,000 cases per year.18 Prostate Cancer Working Group 3 defines nmCRPC as rising PSA level with 25% increase above the nadir level (considering a starting value of ≥1ng/mL) with minimum rise of 2 ng/mL, no evidence of local recurrence or distant metastases on conventional imaging including radionuclide bone imaging, CT scan or MRI, and serum testosterone level <50 ng/mL (castrate level). The value of rising PSA should be confirmed on the second measurement, 3 weeks apart.9 The average metastasis-free survival (MFS) in patients with nmCRPC is about 25–30 months.19 Approximately, one-third of patients with nmCRPC develop bone metastasis in 2 years.19,20 PSA doubling time (PSA-DT) (estimated time required for the PSA level to double) <10 months is associated with a significant risk of progression to metastasis in patients with nmCRPC.21 nmCRPC is a challenging disease for the development of therapeutic strategies due to the lack of radiologic evidence of metastatic disease and the absence of clinical symptoms. Until recently, the standard of care for nmCRPC was continuation of GnRH agonist, addition of first-generation AR antagonist (nilutamide, flutamide or bicalutamide) to GnRH agonist, increasing the dose of bicalutamide, switching to other AR antagonist, AR antagonist withdrawal, or other hormonal therapies with no significant impact on OS.22–28
A known limitation of conducting studies in localized prostate cancer is the long-term follow-up required to assess the impact of the therapeutic intervention on OS which in some cases exceeds a decade. This paradigm changed about 2 years ago when Intermediate Clinical Endpoints in Cancer of the Prostate study (ICECap), a meta-nalysis of 28 randomized trials with localized prostate cancer, found a strong correlation between change in MFS and change in OS (Kendall’s t correlation, 0.91). MFS (as per ICECaP study) is the time measured from the date of random assignment to the date of the first evidence of metastases confirmed by imaging or histologic evidence – or death from any cause.29 Consequently, MFS was recognized as a surrogate marker for OS in patients with prostate cancer based on ICECaP study.29 This endpoint was considered for all confirmatory Phase III studies in nmCRPC setting and will be discussed later. In 2011, the FDA recognized MFS as a reasonable clinical endpoint as the development of the metastatic disease is a clinically relevant event that can be associated with pain and need for additional interventions.30,31
Pharmacologic properties of apalutamide
Apalutamide (ARN-509) is a synthetic beryl thiohydantoin that retains full AR antagonist activity in the setting of increased AR expression.32 Apalutamide is a novel, second-generation AR antagonist which demonstrated seven to ten fold greater affinity to AR than bicalutamide in vivo and animal models.33 Apalutamide inhibits nuclear translocation of AR and inhibits binding of AR to androgen response like elements in the context of AR expression.33 Apalutamide did not exhibit agonist activity in prostate cancer cell lines which were made to overexpress AR as in metastatic castration-resistant prostate cancer. Apalutamide caused ≥50% tumor regression in eight of ten castrate immunodeficient mice harboring LNCaP/AR xenograft tumors, whereas bicalutamide caused ≥50% tumor regression in only one of ten mice.33 Clerg et al compared the dosage of enzalutamide and apalutamide in the murine xenograft model of human CRPC and showed that maximal therapeutic response of apalutamide was achieved at 30 mg/kg/day, whereas the same response required 100 mg/kg/d of enzalutamide and higher steady-state plasma concentration.33 Enzalutamide and apalutamide have low affinity for the GABA receptor in the brain. However, the steady-state level of apalutamide was four fold lower than enzalutamide, suggesting lower seizurogenic potential and less CNS adverse effects as compared to enzalutamide.33
Clinical development of apalutamide: Phase I, II, and III data
The first in human, Phase I trial of apalutamide enrolled 30 patients with progressive metastatic castrate-resistant prostate cancer (mCRPC). The primary objective of this trial was to assess the pharmacokinetics (PK), safety, tolerability, and to define the recommended Phase II dose (RP2D).34 A total of 30 patients with a median age of 68 years (45–81), baseline median PSA of 42 ng/mL (2.3–326.6) were included. The patients were assigned sequentially to escalating dose levels of apalutamide following a traditional 3+3 design, in a 28-day cycle. The starting dose of apalutamide was 30 mg once daily. The most common adverse effects of any cause were fatigue (47%), back pain (30%), diarrhea (30%), arthralgia (24%), nausea (26%), and dyspnea (29%), all of them were grade 1–2. Only three patients (9%) had grade 3 adverse effects including abdominal pain, nausea, and arthralgia. At 12 weeks, 14 (46.7%) of 30 patients had a ≥50% decline in PSA as compared with baseline. The median PSA change from baseline at 12 weeks was −43.2% (range, −98.6% to 120.6%), and the maximum median decline on the study was −62.7% (range, −99.8% to 16.7%). Five (50%) of the ten patients who had baseline measurable soft tissue disease showed stable disease >6 months. One patient (10%) experienced disease progression and four patients (40%) had an indeterminate response. Apalutamide was rapidly absorbed, with peak plasma concentrations in 2–3 hrs after administration. Peak concentrations of apalutamide and AUCs were dose proportional. The RP2D dose of apalutamide was 240 mg daily.34 Based on these data, a Phase II multicenter, multicohort study was initiated with three distinct sets of patients 1) high-risk nmCRPC, 2) chemotherapy-naive and abiraterone acetate/prednisone-naive mCRPC, and 3) progressive mCRPC after abiraterone acetate plus prednisone.35,36 In the high-risk nmCRPC cohort (PSA≥8 ng/mL, PSA-DT≤10 months or both), 51 patients were enrolled. Apalutamide was given at the dose of 240 mg orally daily. The primary endpoint was post treatment percentage change in PSA relative to baseline at 12 weeks (or earlier for those who discontinued therapy) and maximal change at any time on the study. The secondary endpoints were time to PSA progression (TTPP) and MFS. The median age of the enrolled patients was 71 years (51–88), 57% of patients had Gleason score ≤7, 35% had Gleason score 8–10, baseline PSA level was 10.7 ng/mL (0.5–201.7), and 45% of patients had PSA-DT was ≤10 months. At 12 weeks, 89% had a PSA decline of ≥50%. The median TTPP was 24 months (95% CI, 16.3 months – not reached); median MFS was not reached (95% CI 33.4 months – not reached). Apalutamide was discontinued in 22% of patients due to disease progression and in 18% of patients due to adverse effects. The most common adverse effect was fatigue (61%); however, only 4% of patients experienced grade 3 fatigue.36 The positive results in the high-risk nmCRPC cohort led to the international Phase III, double-blind, placebo-controlled trial (SPARTAN) which evaluated apalutamide in patients with high-risk nmCRPC with PSA-DT of ≤10 months.37 The primary endpoint was MFS. Secondary endpoints were time to metastasis, progression-free survival (PFS), time to symptomatic progression, OS, and time to the initiation of cytotoxic chemotherapy. Exploratory endpoints included TTPP (defined as time from randomization to PSA progression according to Prostate Cancer Working Group 2 criteria),38 PSA response rate, patient-reported outcomes, and second PFS. The second PFS was defined as the time from randomization to investigator-assessed disease progression (PSA progression, detection of metastatic disease on imaging, symptomatic progression, or any combination thereof) during the first subsequent treatment for metastatic castration-resistant disease or death from any cause.
A total of 1207 patients were randomized in 2:1 fashion to receive apalutamide 240 mg daily (807 in the apalutamide arm) or placebo (401 in the placebo arm) and ADT was continued in both arms during the study. The patients were stratified by PSA-DT (<6 months or ≥6 months), use of bone-sparing agents and classification of nodal status as N0 or N1. The median age of the patients was 74 years (range, 48–97), 71.3% had a PSA-DT ≤6 months, 10.0% used a bone-sparing agent, and 83.6% had N0 nodal status. Most of the patients (73.1%) had previously used a first-generation AR antagonist. At the planned primary analysis, apalutamide demonstrated significant improvement in MFS compared with placebo (40.5 vs 16.2 months; HR for death or metastasis: 0.28, 95% CI 0.23–0.35; p<0.001). Similarly, median PFS was 40.5 months in the apalutamide arm vs 14.7 months in the placebo arm (HR: 0.29; 95% CI 0.24–0.36; p<0.001). Of the other exploratory endpoints, apalutamide was associated with improved TTPP (HR: 0.06; 95% CI 0.05–0.08; p<0.0001), time to symptomatic progression (HR: 0.45; 95% CI 0.32–0.63; p<0.001), and time to initiation of cytotoxic chemotherapy (HR: 0.44; 95% CI 0.29–0.66). PSA response rate (≥50% decline) was observed in 90% of patients in the apalutamide group as compared to 2% in the placebo group. The patients in the apalutamide arm reported stable overall health-related QoL as did the patients in the placebo arm. The second PFS was significantly longer in the apalutamide arm than the placebo arm (HR: 0.49; 95% CI 0.36–0.66). Of note, the OS data were not mature at the time of publication but apalutamide showed a trend toward improved OS with HR of 0.70. Notably, an exploratory landmark analysis in the SPARTAN trial suggested an association between MFS and OS in high-risk nmCRPC who develop metastases at 6, 9, and 12 months (Spearman’s correlation coefficient: 0.62; p<0.0001).39
The most common adverse effects of any grade in the apalutamide group versus the placebo group were fatigue (31.3% vs 21.4%), hypertension (39.1% vs 31.6%), rash (29% vs 5.8%), diarrhea (21.3% vs 15.6%), and falls (17.3% vs 9.8%). Significant (grade 3 or 4) adverse events were observed in 45.1% of patients in the apalutamide group compared with 34.2% in the placebo group. Due to adverse effects, 10.6% of patients discontinued apalutamide as compared to 7% in the placebo group.39 The treatment-related mortality rate in the apalutamide group was 1.2% as compared to 0.3% in the placebo group. Based on the improvement in MFS, FDA approved apalutamide on 14 February 2018 for the treatment of patients with nmCRPC.40
Genomic data and apalutamide resistance
Despite the activity of apalutamide in CRPC, resistance to apalutamide eventually develops and associated with specific mutations in the AR gene. The most studied example includes F877L mutation, a missense mutation at AR LBD. F877L mutation was found to be associated with a lack of antitumor activity in castrated immunodeficient mice injected with LNCaP cell lines expressing F877 L mutation.41 In a Phase I study of apalutamide, 3 (10.3%) of the 29 enrolled patients showed F877L mutation in circulating tumor DNA samples after treatment with apalutamide with no evidence of F877 L mutation in pretreatment samples suggesting acquired treatment resistance to apalutamide.41 A different Phase II study by Rathkopf et al showed that only 2 (2.2%) of 93 patients analyzed had the F877L mutation at baseline suggesting that other mechanisms may play a role in resistance to apalutamide including AR splice variant within the N-terminal domain, increase steroidogenesis, development of androgen-independent tumor and/or activation of the PI3K signaling pathway.42–44 Further studies are needed to detect de-novo and acquired mutations in patients exposed to apalutamide which would help to optimally use apalutamide in sequence or in combination with other AR signaling targeting agents.
Treatment options for patients with nmCRPC
In addition to apalutamide, two other novel AR-targeted therapies – enzalutamide and darolutamide were evaluated in nmCRPC and are briefly discussed here.
Enzalutamide is a second-generation AR antagonist which inhibits binding of androgen to AR, inhibits AR translocation to the nucleus, impairs DNA binding to androgen response elements, and recruitment of coactivators.45 Enzalutamide has five to eight fold affinity than bicalutamide for AR and unlike bicalutamide, it does not appear to switch from antagonist to agonist.46 Two large multicenter Phase III trials (PREVAIL and AFFIRM) established the safety and efficacy of enzalutamide in patients with metastatic prostate cancer while PROSPER study evaluated the efficacy of enzalutamide in nmCRPC setting.47–49 PROSPER involved 1401 nmCRPC patients with PSA-DT of ≤10 months and randomized them to receive enzalutamide 160 mg daily or placebo, ADT was continued in both arms.49 The median MFS was 36.6 months in the enzalutamide group versus 14.7 months in the placebo group (HR for metastasis or death, 0.29; 95% CI 0.24 −0.35; p<0.001). In the interim analyses of secondary or exploratory endpoints, TTPP, PSA response rate, time to the first use of subsequent antineoplastic therapy was longer in the enzalutamide group than in the placebo group. The median OS was not reached in either group. The most common adverse effects of any grade in the enzalutamide group as compared to placebo were fatigue (36% vs 15%), hot flashes (13% vs 8%), nausea (11% vs 9%), hypertension (15% vs 7%), fall (12% vs 5%), dizziness (10% vs 4%), major adverse cardiovascular events (5% vs 3%), and mental impairment disorders (5% vs 2%), respectively. Enzalutamide had a higher adverse effect-related mortality rate as compared to placebo (3% vs 1%). The rate of discontinuation for adverse eventswas 10% with enzalutamide versus 6% with placebo.49
Darolutamide is a non-steroidal second-generation AR antagonist which inhibits androgen-induced translocation of AR to the nucleus, thus decreasing activation of genes required for prostate cancer cell growth. Darolutamide and its metabolites have exhibited tighter binding to AR than enzalutamide and apalutamide.50 Darolutamide has shown to retain full AR antagonist activity in the presence of AR mutations which can cause a switch of AR antagonist to agonist; F877 L mutation can cause enzalutamide and apalutamide to become an agonist, W742L and T878A mutations can cause bicalutamide to act as an agonist.50,51 Darolutamide showed lower affinity of γ-aminobutyric acid type A receptors in the brain and lower blood-brain penetration than enzalutamide and apalutamide in pre-clinical models.52 Darolutamide showed antitumor activity and safety in Phase I and II studies in patients with metastatic prostate cancer which led to the evaluation of darolutamide in Phase III (ARAMIS) trial in patients with nmCRPC.53,54 ARAMIS enrolled 1509 patients with nmCRPC and PSA-DT of ≤10 months and randomized them to received darolutamide plus ADT or placebo plus ADT. The primary endpoint was MFS. Secondary endpoints were OS, time to pain progression (assessed by Brief Pain Inventory Short Form), time to first symptomatic skeletal event, and time to first cytotoxic chemotherapy. Exploratory endpoints included PFS (defined as the time from randomization to evidence of any radiographic disease progression, including local relapse or new pathologic lymph nodes, or death from any cause, whichever occurred first), time to first prostate cancer-related invasive procedure, time to initiation of subsequent antineoplastic therapy, PSA progression and response, deterioration in ECOG performance status, and QoL. QoL was assessed by the European Organization for Research and Treatment of Cancer QoL Prostate Cancer module (EORTC-QLQ-PR25) at baseline and every 16 weeks until the end of treatment. Darolutamide plus ADT was associated with improved MFS as compared to placebo plus ADT (40.4 vs 18.4 months; HR: 0.41, 95% CI 0.34–0.50; p < 0.001). At the time of interim analyses, darolutamide showed improvement in secondary and exploratory endpoints as compared to placebo.55 The OS data were not mature at the time of publication of results.55 The most common adverse effects of any grade in the darolutamide group as compared to the placebo group were fatigue (12.1% vs 0.9%), back pain (8.8% vs 9%), arthralgia (8.1% vs 9.2%), and hypertension (6.6% vs 5.2%) respectively. The rate of side effects of any grade was 83.2% in patients treated with darolutamide and 76.9% in those who received a placebo. Grade 3 or 4 adverse effects of any cause were 24.7% in the darolutamide group versus 19.5% in the placebo group. Notably, darolutamide was not associated with a higher incidence of falls (4.2% vs 4.7%), seizure (0.2% vs 0.2%), or fractures (4.2% vs 3.6%) as compared to the placebo group. There was one treatment-related death in the darolutamide group (0.4%) vs 3 deaths (0.2%) in the placebo group. The rate of treatment discontinuation due to adverse effects was 8.9% in the darolutamide group as compared to 8.7% in the placebo group.55
Recent updated analysis showed that darolutamide significantly delayed pain progression as compared to placebo (40.3 vs 25.4 months; HR: 0.65; 95% CI 0.53–0.79; p<0.001). The delay in pain progression with darolutamide was maintained beyond end of the study treatment. Darolutamide was associated with delayed time to deterioration of EORTC-QLQ-PR25 outcomes for urinary symptoms (25.8 vs 14.8 months; HR: 0.64; 95% CI 0.54–0.76; p<0.01) and for hormonal treatment-related symptoms as compared to placebo (18.9 vs 18.4 months; HR: 1.06; 95% CI 0.88–1.27; p=0.52).56
Role of apalutamide beyond nmCRPC
Several trials are currently underway to evaluate the role of apalutamide in early and advanced stages of prostate cancer. During ASCO 2019 meeting, the results of the TITAN trial were presented. TITAN was a Phase III trial which assessed the efficacy of apalutamide plus ADT versus placebo plus ADT in patients with metastatic hormone-sensitive prostate cancer. The patients who previously received docetaxel for advanced prostate cancer (11%) were also enrolled. The primary endpoints were radiologic progression-free survival (rPFS) and OS. At the time of first interim analysis, apalutamide plus ADT was associated with improved rPFS as compared to placebo plus ADT (HR: 0.48; 95% CI 0.39–0.60; p<0.001).57 OS survival data were not mature at the time of the first interim analysis. Grade 3–4 adverse effects were 42.2% in the apalutamide plus ADT arm vs 40.8% in the placebo plus ADT arm.57
ACIS is a Phase III, randomized, placebo-controlled, double-blind study which is evaluating apalutamide in combination with abiraterone and prednisone (AAP) versus AAP alone as first-line treatment in patients with mCRPC, with rPFS as the primary endpoint.58 Secondary endpoints are OS, time to long-term opioid use, time to initiation of cytotoxic chemotherapy, time to pain progression, and time to skeletal-related events.58 Another smaller Phase II study is investigating the same combination in two cohorts of Caucasian and African American men (PANTHER study, NCT03098836).59 LACOG 0415 is a Phase II, randomized, a three-arm study evaluating the role of abiraterone acetate plus ADT versus apalutamide versus abiraterone and apalutamide in patients with advanced prostate cancer with non-castrate testosterone. The primary endpoint of the study is undetectable PSA levels (below 0.2 ng/mL) at week 25, aiming for 65% of undetectable PSA at week 25. Secondary endpoints are PSA progression and PSA response (50% and 80%) at week 25, rPFS, safety, health QoL, and correlation of serum androgen levels with response.60 PILLAR, a Phase II study is comparing apalutamide with stereotactic body radiation therapy (SBRT) versus apalutamide alone in patients with mCRPC. The patients will receive apalutamide for 52 weeks in both arms. The primary endpoint is to determine if the proportion of patients with an undetectable serum PSA at 6 months following cessation of apalutamide is higher with the addition of SBRT to prostate-specific membrane antigen -avid oligometastatic sites of disease compared to the group of patients receiving apalutamide monotherapy.61 A three-arm Phase II study is evaluating apalutamide in combination with abiraterone acetate and prednisone (AAP) in patients with mCRPC either with ipilimumab or carboplatin and cabazitaxel. In this open-label study, the patients will be randomized in 1:1:1 fashion into three treatment arms: control arm consisting of apalutamide and AAP, experimental arm consisting of apalutamide, AAP and ipilimumab, and other experimental arm consisting of apalutamide, AAP, carboplatin, and cabazitaxel. The primary outcome of the study is OS in each arm.62
ATLAS, a Phase III, randomized double-blind placebo-controlled trial is evaluating the role of apalutamide in combination with GnRH agonist compared with GnRH agonist alone in patients with high risk, localized or locally advanced prostate cancer who are receiving radiation therapy as initial definite therapy.63 The primary endpoint is MFS.
A Phase III is evaluating the role of apalutamide in men with biochemically recurrent prostate cancer who have PSAD-T≤9 months. In this three-arm, open-label study, the patients will be randomized in 1:1:1 fashion into one of three treatment arms: control arm consisting of degarelix monotherapy, experimental arm consisting of apalutamide in combination with degarelix, and another experimental arm consisting of apalutamide, AAP and degarelix.64 The patients will be treated for a maximum duration of 52 weeks. The primary endpoint of the study is PSA PFS in the intent-to-treat patient population. Secondary endpoints include PSA PFS in testosterone-evaluable population, 36-month PSA PFS rate in both intent-to-treat and testosterone-evaluable populations, time to testosterone recovery, time to castration resistance, MFS, QoL, and safety. A Phase II trial is evaluating neoadjuvant apalutamide in patients with intermediate to high-risk prostate cancer followed by radical prostatectomy. The patients will receive apalutamide for 12 weeks. The primary endpoints are pathologic down staging and biochemical response (to achieve PSA level <0.03 µg/L) after neoadjuvant apalutamide followed by RP.65 A Phase II randomized, multicenter trial is evaluating active surveillance with or without apalutamide in low-risk prostate cancer. The patients will receive apalutamide for 6 months. The primary endpoint is time to initiate local treatment.66 Table 1 summarizes the ongoing Phase III trials with apalutamide in different stages of prostate cancer.
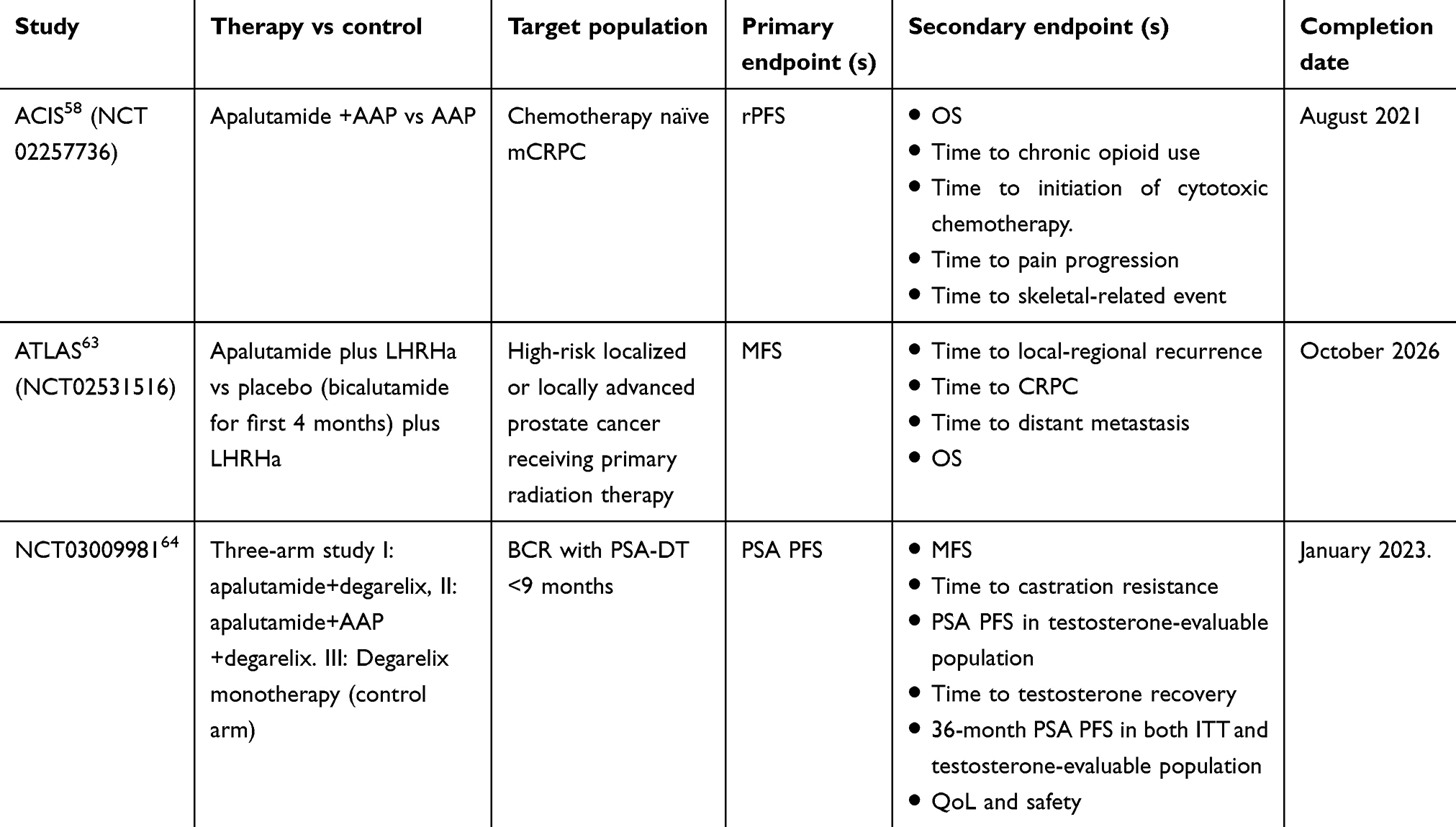 |
Table 1 Phase III trials of apalutamide in prostate cancer |
Conclusion
The treatment landscape of prostate cancer is dramatically changing, with the incorporation of novel AR-targeted therapies early in the course of the disease. Apalutamide was the first drug that demonstrated a delay in the development of metastasis as detected on conventional imaging in patients with nmCRPC. Other mechanistically similar therapies – enzalutamide and darolutamide have also shown to delay time to metastatic disease in patients with nmCRPC.
Apalutamide and enzalutamide have received FDA approval in the nmCRPC setting. It is very clear from the previous data that patients with nmCRPC with rapidly rising PSA level (PSA-DT <10 months) are at increased risk of developing bone metastases and would benefit from novel AR-targeted therapies. The benefit of novel AR-targeted therapies in patients with longer PSA-DT has yet to determined.
It is noteworthy that none of the novel AR-targeted agent has demonstrated OS benefit in the nmCRPC setting. In our opinion, the adverse effect profile would most likely influence the selection of the individual agent in the nmCRPC setting. In addition, the emerging use of sensitive molecular imaging will probably impact the use of novel AR-targeted therapies in the nmCRPC setting. Future studies will help to determine the mechanism of resistance to apalutamide, therapeutic ways to circumvent this resistance and the role of apalutamide as monotherapy or with other therapies in different stages of prostate cancer.
Abbreviations
CRPC, castration-resistant prostate cancer; LHRHa, luteinizing hormone-releasing hormone agonist; ADT, androgen deprivation therapy; mCRPC, metastatic castration-resistant prostate cancer; MFS, metastasis-free survival; mHSPC, metastatic hormone-sensitive prostate cancer; OS, overall survival; rPFS, radiographic progression-free survival; BCR, biochemical recurrence; PFS, progression-free survival; ITT, intention to treat; QoL, quality of life; AAP, abiraterone and prednisone.
Disclosure
Dr Garcia has disclosed to be a paid consultant/speaker for Clovis, Sanofi, Merck, Janssen, Eisai, Bayer and received institutional research support from Genentech, Merck, Clovis, and Pfizer. Dr Barata disclosed to be a paid consultant to Bayer, BMS, EMD, and Pfizer and received institutional research support from Blue Earth Diagnostics. Dr Gul reports no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7–30. doi:10.3322/caac.21442
2. Bolla M, Maingon P, Carrie C, et al. Short androgen suppression and radiation dose escalation for intermediate- and high-risk localized prostate cancer: results of EORTC trial 22991. J Clin Oncol. 2016;34(15):1748–1756. doi:10.1200/JCO.2015.64.8055
3. Garisto JD, Klotz L. Active surveillance for prostate cancer: how to do it right. Oncology (Williston Park, NY). 2017;31(5):333–340, 345.
4. Roehl KA, Han M, Ramos CG, Antenor JA, Catalona WJ. Cancer progression and survival rates following anatomical radical retropubic prostatectomy in 3,478 consecutive patients: long-term results. J Urol. 2004;172(3):910–914. doi:10.1097/01.ju.0000134888.22332.bb
5. Amling CL, Bergstralh EJ, Blute ML, Slezak JM, Zincke H. Defining prostate specific antigen progression after radical prostatectomy: what is the most appropriate cut point? J Urol. 2001;165(4):1146–1151.
6. Lee WR, Hanks GE, Hanlon A. Increasing prostate-specific antigen profile following definitive radiation therapy for localized prostate cancer: clinical observations. J Clin Oncol. 1997;15(1):230–238. doi:10.1200/JCO.1997.15.1.230
7. Pinover WH, Horwitz EM, Hanlon AL, Uzzo RG, Hanks GE. Validation of a treatment policy for patients with prostate specific antigen failure after three-dimensional conformal prostate radiation therapy. Cancer. 2003;97(4):1127–1133. doi:10.1002/cncr.11166
8. Sharifi N, Dahut WL, Steinberg SM, et al. A retrospective study of the time to clinical endpoints for advanced prostate cancer. BJU Int. 2005;96(7):985–989. doi:10.1111/j.1464-410X.2005.05798.x
9. Scher HI, Morris MJ, Stadler WM, et al. Trial design and objectives for castration-resistant prostate cancer: updated recommendations from the prostate cancer clinical trials working group 3. J Clin Oncol. 2016;34(12):1402–1418. doi:10.1200/JCO.2015.64.2702
10. Gelmann EP. Molecular biology of the androgen receptor. J Clin Oncol. 2002;20(13):3001–3015. doi:10.1200/JCO.2002.10.018
11. Edwards J, Bartlett JM. The androgen receptor and signal-transduction pathways in hormone-refractory prostate cancer. Part 2: androgen-receptor cofactors and bypass pathways. BJU Int. 2005;95(9):1327–1335. doi:10.1111/j.1464-410X.2005.05527.x
12. Huggins C, Hodges CV. Studies on prostatic cancer. I. The effect of castration, of estrogen and androgen injection on serum phosphatases in metastatic carcinoma of the prostate. CA Cancer J Clin. 1972;22(4):232–240.
13. Titus MA, Schell MJ, Lih FB, Tomer KB, Mohler JL. Testosterone and dihydrotestosterone tissue levels in recurrent prostate cancer. Clin Cancer Res. 2005;11(13):4653–4657. doi:10.1158/1078-0432.CCR-05-0525
14. Visakorpi T, Hyytinen E, Koivisto P, et al. In vivo amplification of the androgen receptor gene and progression of human prostate cancer. Nat Genet. 1995;9(4):401–406. doi:10.1038/ng0495-401
15. Taplin ME, Bubley GJ, Shuster TD, et al. Mutation of the androgen-receptor gene in metastatic androgen-independent prostate cancer. N Engl J Med. 1995;332(21):1393–1398. doi:10.1056/NEJM199505253322101
16. Craft N, Shostak Y, Carey M, Sawyers CL. A mechanism for hormone-independent prostate cancer through modulation of androgen receptor signaling by the HER-2/neu tyrosine kinase. Nat Med. 1999;5(3):280–285. doi:10.1038/6495
17. Bitting RL, Armstrong AJ. Targeting the PI3K/Akt/mTOR pathway in castration-resistant prostate cancer. Endocr Relat Cancer. 2013;20(3):R83–R99. doi:10.1530/ERC-12-0394
18. Scher HI, Solo K, Valant J, Todd MB, Mehra M. Prevalence of prostate cancer clinical states and mortality in the United States: estimates using a dynamic progression model. PLoS One. 2015;10(10):e0139440. doi:10.1371/journal.pone.0139440
19. Smith MR, Kabbinavar F, Saad F, et al. Natural history of rising serum prostate-specific antigen in men with castrate nonmetastatic prostate cancer. J Clin Oncol. 2005;23(13):2918–2925. doi:10.1200/JCO.2005.01.529
20. Smith MR, Cook R, Lee KA, Nelson JB. Disease and host characteristics as predictors of time to first bone metastasis and death in men with progressive castration-resistant nonmetastatic prostate cancer. Cancer. 2011;117(10):2077–2085. doi:10.1002/cncr.25762
21. Smith MR, Saad F, Oudard S, et al. Denosumab and bone metastasis-free survival in men with nonmetastatic castration-resistant prostate cancer: exploratory analyses by baseline prostate-specific antigen doubling time. J Clin Oncol. 2013;31(30):3800–3806. doi:10.1200/JCO.2012.44.6716
22. Taylor CD, Elson P, Trump DL. Importance of continued testicular suppression in hormone-refractory prostate cancer. J Clin Oncol. 1993;11(11):2167–2172. doi:10.1200/JCO.1993.11.11.2167
23. Crawford ED, Eisenberger MA, McLeod DG, et al. A controlled trial of leuprolide with and without flutamide in prostatic carcinoma. N Engl J Med. 1989;321(7):419–424. doi:10.1056/NEJM198908173210702
24. Schellhammer P, Sharifi R, Block N, et al. A controlled trial of bicalutamide versus flutamide, each in combination with luteinizing hormone-releasing hormone analogue therapy, in patients with advanced prostate cancer. Casodex combination study group. Urology. 1995;45(5):745–752. doi:10.1016/s0090-4295(99)80077-6
25. Miyake H, Hara I, Eto H. Clinical outcome of maximum androgen blockade using flutamide as second-line hormonal therapy for hormone-refractory prostate cancer. BJU Int. 2005;96(6):791–795. doi:10.1111/j.1464-410X.2005.05766.x
26. Klotz L, Drachenberg D, Singal R, et al. An open-label, phase 2 trial of bicalutamide dose escalation from 50 mg to 150 mg in men with CAB and castration resistance. A Canadian urology research consortium study. Prostate Cancer Prostatic Dis. 2014;17(4):320–324. doi:10.1038/pcan.2014.24
27. Sartor AO, Tangen CM, Hussain MH, et al. Antiandrogen withdrawal in castrate-refractory prostate cancer: a Southwest oncology group trial (SWOG 9426). Cancer. 2008;112(11):2393–2400. doi:10.1002/cncr.23473
28. Small EJ, Baron AD, Fippin L, Apodaca D. Ketoconazole retains activity in advanced prostate cancer patients with progression despite flutamide withdrawal. J Urol. 1997;157(4):1204–1207.
29. Xie W, Regan MM, Buyse M, et al. Metastasis-free survival is a strong surrogate of overall survival in localized prostate cancer. J Clin Oncol. 2017;35(27):3097–3104. doi:10.1200/JCO.2017.73.9987
30. AdvisoryCommittee FCfDEaROD. FDA center for drug evaluation and research. Oncologic Drugs AdvisoryCommittee. Available from: https://www.fda.gov/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/OncologicDrugsAdvisoryCommittee/default.htm.
31. Beaver JA, Kluetz PG, Pazdur R. Metastasis-free survival - a new end point in prostate cancer trials. N Engl J Med. 2018;378(26):2458–2460. doi:10.1056/NEJMp1805966
32. Jung ME, Ouk S, Yoo D, et al. Structure-activity relationship for thiohydantoin androgen receptor antagonists for castration-resistant prostate cancer (CRPC). J Med Chem. 2010;53(7):2779–2796. doi:10.1021/jm901488g
33. Clegg NJ, Wongvipat J, Joseph JD, et al. ARN-509: a novel antiandrogen for prostate cancer treatment. Cancer Res. 2012;72(6):1494–1503. doi:10.1158/0008-5472.CAN-11-3948
34. Rathkopf DE, Morris MJ, Fox JJ, et al. Phase I study of ARN-509, a novel antiandrogen, in the treatment of castration-resistant prostate cancer. J Clin Oncol. 2013;31(28):3525–3530. doi:10.1200/JCO.2013.50.1684
35. Rathkopf DE, Antonarakis ES, Shore ND, et al. Safety and antitumor activity of apalutamide (ARN-509) in metastatic castration-resistant prostate cancer with and without prior abiraterone acetate and prednisone. Clin Cancer Res. 2017;23(14):3544–3551. doi:10.1158/1078-0432.CCR-16-2509
36. Smith MR, Antonarakis ES, Ryan CJ, et al. Phase 2 study of the safety and antitumor activity of apalutamide (ARN-509), a potent androgen receptor antagonist, in the high-risk nonmetastatic castration-resistant prostate cancer cohort. Eur Urol. 2016;70(6):963–970. doi:10.1016/j.eururo.2016.04.023
37. Smith MR, Saad F, Chowdhury S, et al. Apalutamide treatment and metastasis-free survival in prostate cancer. N Engl J Med. 2018;378(15):1408–1418. doi:10.1056/NEJMoa1715546
38. Scher HI, Halabi S, Tannock I, et al. Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: recommendations of the prostate cancer clinical trials working group. J Clin Oncol. 2008;26(7):1148–1159. doi:10.1200/JCO.2007.12.4487
39. Smith MR, Mehra M, Nair S, Lawson J, Small EJ. Association of metastasis-free survival (MFS) and overall survival (OS) in nonmetastatic castration-resistant prostate cancer (nmCRPC). J Clin Oncol. 2018;36(15_suppl):5032.
40. FDA approves apalutamide for non-metastatic castration-resistant prostate cancer. https://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm596796.htm.
41. Joseph JD, Lu N, Qian J, et al. A clinically relevant androgen receptor mutation confers resistance to second-generation antiandrogens enzalutamide and ARN-509. Cancer Discov. 2013;3(9):1020–1029. doi:10.1158/2159-8290.CD-13-0226
42. Rathkopf DE, Smith MR, Ryan CJ, et al. Androgen receptor mutations in patients with castration-resistant prostate cancer treated with apalutamide. Ann Oncol. 2017;28(9):2264–2271. doi:10.1093/annonc/mdx283
43. Shafi AA, Yen AE, Weigel NL. Androgen receptors in hormone-dependent and castration-resistant prostate cancer. Pharmacol Ther. 2013;140(3):223–238. doi:10.1016/j.pharmthera.2013.07.003
44. Watson PA, Arora VK, Sawyers CL. Emerging mechanisms of resistance to androgen receptor inhibitors in prostate cancer. Nature Rev Cancer. 2015;15(12):701–711. doi:10.1038/nrc4016
45. Tran C, Ouk S, Clegg NJ, et al. Development of a second-generation antiandrogen for treatment of advanced prostate cancer. Science (New York, NY). 2009;324(5928):787–790. doi:10.1126/science.1168175
46. von Klot CA, Kuczyk MA, Merseburger AS. No androgen withdrawal syndrome for enzalutamide: a report of disease dynamics in the postchemotherapy setting. Eur Urol. 2014;65(1):258–259. doi:10.1016/j.eururo.2013.09.036
47. Beer TM, Armstrong AJ, Rathkopf DE, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med. 2014;371(5):424–433. doi:10.1056/NEJMoa1405095
48. Scher HI, Fizazi K, Saad F, et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med. 2012;367(13):1187–1197. doi:10.1056/NEJMoa1207506
49. Hussain M, Fizazi K, Saad F, et al. Enzalutamide in men with nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2018;378(26):2465–2474. doi:10.1056/NEJMoa1800536
50. Fizazi K, Smith MR, Tombal B. Clinical development of darolutamide: a novel androgen receptor antagonist for the treatment of prostate cancer. Clin Genitourin Cancer. 2018;16(5):332–340. doi:10.1016/j.clgc.2018.07.017
51. Moilanen AM, Riikonen R, Oksala R, et al. Discovery of ODM-201, a new-generation androgen receptor inhibitor targeting resistance mechanisms to androgen signaling-directed prostate cancer therapies. Sci Rep. 2015;5:12007. doi:10.1038/srep12007
52. Zurth C, Sandmann S, Trummel D, Seidel D, Gieschen H. Blood-brain barrier penetration of [14C]darolutamide compared with [14C]enzalutamide in rats using whole body autoradiography. J Clin Oncol. 2018;36(6_suppl):345.
53. Fizazi K, Massard C, Bono P, et al. Activity and safety of ODM-201 in patients with progressive metastatic castration-resistant prostate cancer (ARADES): an open-label phase 1 dose-escalation and randomised phase 2 dose expansion trial. Lancet Oncol. 2014;15(9):975–985. doi:10.1016/S1470-2045(14)70240-2
54. Shore ND, Tammela TL, Massard C, et al. Safety and antitumour activity of ODM-201 (BAY-1841788) in chemotherapy-naive and CYP17 inhibitor-naive patients: follow-up from the ARADES and ARAFOR trials. Eur Urol Focus. 2018;4(4):547–553. doi:10.1016/j.euf.2017.01.015
55. Fizazi K, Shore N, Tammela TL, et al. Darolutamide in nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2019. doi:10.1056/NEJMoa1815671
56. Fizazi K, Shore ND, Tammela T, et al. Impact of darolutamide (DARO) on pain and quality of life (QoL) in patients (Pts) with nonmetastatic castrate-resistant prostate cancer (nmCRPC). J Clin Oncol. 2019;37(15_suppl):5000. doi:10.1200/JCO.2019.37.15_suppl.5000
57. Chi KN, Agarwal N, Bjartell A, et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N Engl J Med. 2019. doi:10.1056/NEJMoa1903307
58. ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). Identifier NCT02257736, An efficacy and safety study of Apalutamide (JNJ-56021927) in combination with abiraterone acetate and prednisone versus abiraterone acetate and prednisone in participants with chemotherapy-naive metastatic castration resistant prostate cancer (mCRPC); [
59. ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US. Identifier ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US. Identifier NCT02867020. Apalutamide and Abiraterone Acetate in African American and Caucasian Men With Metastatic Castrate Resistant Prostate Cancer (PANTHER) 2017 April 4;
60. ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US. Identifier NCT02867020, A Phase II Randomized Study of Abiraterone Acetate Plus ADT Versus APALUTAMIDE Versus Abiraterone and APALUTAMIDE in Patients With Advanced Prostate Cancer With Non-castrate Testosterone; 2016 August 15 [
61. ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). Identifier Identifier: NCT03503344. Apalutamide With or Without Stereotactic Body Radiation Therapy in Treating Participants With Castration-Resistant Prostate Cancer (PILLAR); 2018, April 19 [
62. ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). Identifier NCT02703623. A Dynamic Allocation Modular Sequential Trial of Approved and Promising Therapies in Men With Metastatic Castrate Resistant Prostate Cancer; 2016 March 9 [
63. ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). Identifier NCT02531516, An efficacy and safety study of JNJ-56021927 (Apalutamide) in high risk prostate cancer subjects receiving primary radiation therapy: ATLAS; 2015 August 24 [
64. ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US. Identifier NCT 03009981, A Study of Androgen Annihilation in High-Risk Biochemically Relapsed Prostate Cancer; 2017 January 4 [
65. Prostate Cancer. April 21, 2017 [
66. ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). Identifier NCT03088124. Active Surveillance With or Without Apalutamide Treatment in Low Risk Prostate Cancer; 2017 Available from: https://clinicaltrials.gov/ct2/show/NCT03088124.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.