Back to Journals » International Journal of Women's Health » Volume 15
Trajectory of Perinatal Depressive Symptoms from the Second Trimester to Three Months Postpartum and Its Association with Sleep Quality
Authors Wang C ![]() , Hou J, Li A, Kong W
, Hou J, Li A, Kong W ![]()
Received 13 February 2023
Accepted for publication 5 May 2023
Published 9 May 2023 Volume 2023:15 Pages 711—723
DOI https://doi.org/10.2147/IJWH.S408347
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Chen Wang,1 Jinqin Hou,2 Anning Li,3 Weimin Kong4
1Department of Perinatal Medicine, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, Beijing, People’s Republic of China; 2Department of Special Education and Psychology, China National Academy of Educational Sciences, Beijing, People’s Republic of China; 3The National Clinical Research Center for Mental Disorders & Beijing Key Laboratory of Mental Disorders, Beijing Anding Hospital, Capital Medical University, Beijing, People’s Republic of China; 4Department of Gynecological Oncology, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, Beijing, People’s Republic of China
Correspondence: Weimin Kong, Department of Gynecological Oncology, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, No. 251, Yaojiayuan Road, Chaoyang District, Beijing, People’s Republic of China, Tel +8618611942798, Email [email protected]
Purpose: Few studies have explored the association between sleep quality and depressive symptoms in perinatal women from the second trimester to the postpartum period. This study aims to explore this relationship using a longitudinal design.
Patients and Methods: Participants were enrolled at 15 gestational weeks. Demographic information was collected. Perinatal depressive symptoms were measured using the Edinburgh Postnatal Depression Scale (EPDS). Sleep quality was measured employing the Pittsburgh Sleep Quality Index (PSQI) at five timepoints from enrollment to three months postpartum. Overall, 1416 women completed the questionnaires at least thrice. A Latent Growth Curve (LGC) model was performed to identify the relationship between the trajectories of perinatal depressive symptoms and sleep quality.
Results: Of the participants, 23.7% screened positive at least once on the EPDS. The perinatal depressive symptoms trajectory, fitted by the LGC model, decreased at early pregnancy and increased from 15 gestational weeks to three months postpartum. The intercept of sleep trajectory positively affected the intercept of perinatal depressive symptoms’ trajectory; the slope of sleep trajectory positively affected both the slope and the quadratic coefficient of perinatal depressive symptoms’ trajectory.
Conclusion: The trajectory of perinatal depressive symptoms increased from 15 gestational weeks to three months postpartum following a quadratic trend. Poor sleep quality was associated with depression symptoms beginning at the onset of pregnancy. Moreover, rapidly declining sleep quality could be a significant risk factor for perinatal depression (PND). These findings call for greater attention to perinatal women who report poor and persistently deteriorating sleep quality. Additional sleep-quality evaluations, depression assessments, and referrals to mental health care providers may benefit these women and support PND prevention, screening, and early diagnosis.
Keywords: perinatal depression, sleep quality, trajectory, latent growth curve model
Introduction
Perinatal Depression (PND) includes the depressive symptoms occurring during pregnancy (ie, antenatal depression [AND]) and up to one year postpartum (ie, postpartum depression [PPD]).1 PND is among the most common obstetric complications and it adversely affects both maternal and child wellbeing.2 However, it is difficult to recognize because women often do not observe changes in their mood or are reluctant to report them. If left untreated, PND can have devastating effects on women, infants, and families. More specifically, AND is thought to be related to low birth weight, decreased fetal growth, and preterm birth.3 Whereas, PPD has adverse consequences on the infant’s wellbeing and development, and is associated with cognitive, behavioral, and emotional problems in childhood and adolescence.4 Additionally, PND can lead to suicide which surpasses hemorrhage and hypertensive disorders as a cause of maternal mortality.5
PND’s incidence varies across different countries and regions owing to social, economic, and cultural backgrounds; survey timepoints; and survey tools and criteria. During pregnancy, the prevalence of depressive symptoms’ ranges from 7% to 20% in high-income countries and exceeds 20% in numerous low- and middle-income countries; furthermore, PPD is estimated to affect 7–30% of women globally and 45% of women in some low-resource settings.6 In the United States, the prevalence of major and minor depression during pregnancy and the first postpartum year are (reportedly) 8.5–11% and 6.5%–12.9%, respectively; however, some evidence indicates that racial and ethnic differences contribute to PND prevalence rates.7,8 A recent article suggested that in China, the pooled prevalence of PND, AND, and PPD are 16.3%, 19.7%, and 14.8%, respectively.9 Moreover, PND’s incidence in China was significantly higher than normal during the COVID-19 (Corona Virus Disease 2019) outbreak.10 However, no published studies have hitherto examined the prevalence of PND in Beijing, the capital of China.
The Trajectory of Depressive Symptoms During the Perinatal Period
In the last decade, instead of employing only a single assessment at non-standardized timepoints as a proxy for the entire perinatal period, the trajectories of depressive symptoms and risk factors from the prenatal period to the years postpartum have attracted the interest of an increasing number of researchers.11–14 As most of these studies started the assessment in the later stages of pregnancy or a few months postpartum, data on the course of PND symptoms from the first or second trimester through childbirth are still sparse.
Recently, several studies have assessed the progression of depressive symptoms from the first or second trimester for a better understanding of when women are most at risk and what factors are associated with the disorder’s onset, severity, and chronicity.15–19 These studies described trajectories based on severity levels: some trajectories are described as time-stable with a linear trend,15,17 while other studies reported symptom trajectory trends with variability—a quadratic trend.16,18–21 Some studies only traced the trajectory during pregnancy,17 while others merely described rough trajectories, missing the data of either the second trimester15 or after 36 weeks (right before labor).16,18,20,21 Meanwhile, most of the samples were from high-income countries, with limited attention paid to relatively low-income populations. Research with a larger sample size, at shorter intervals, and in more diverse settings is still needed in order to inform services and policies regarding how and when to effectively identify women at high risk of PND.
Sleep Quality During the Perinatal Period
Worsening sleep quality and increases in sleep disturbances, which are well-documented complaints from mothers during the perinatal period, have been suggested as important modifiable risk factors for developing PND.3,22–30 Mothers’ subjective sleep quality is disturbed as early as the first trimester of pregnancy23,28 and deteriorates as pregnancy progresses.31–34 The proportion of women defined as poor sleepers as per the Pittsburgh Sleep Quality Index (PSQI)—those with scores at or above the cutoff of “5”—has increased significantly.35 In the postpartum period, sleep problems frequently persist, peaking during the first postpartum months and remaining elevated thereafter.3,35,36 However, most studies examining sleep quality during pregnancy have only considered one or two timepoints, with most using one time period after 20 weeks’ gestation and another in late pregnancy or the post-partum period.24,25,27,34,37–39 Relative evidence before 20 gestation weeks remains scarce and inconsistent.31,33,35,40
Recently, several longitudinal studies have attempted to map out a rough sleep pattern during the perinatal period.22,23,35,41 While Sivertsen et al found an overall pattern indicating stable or increased sleep problems from late pregnancy to immediately after birth (eight weeks),41 Gueron-Sela et al assessed only the maternal postpartum sleep pattern.22 Meanwhile, Tomfohr et al35 and Solomonova et al23 tracked the dynamic maternal-sleep trajectory from early pregnancy to the postpartum period employing relatively small sample sizes, but the data of the late pregnancy period was missing. To gain a better understanding of the dynamic change in perinatal sleep quality as a risk factor for PND, first- or second-trimester-to-postpartum period assessments with larger samples are needed.
Association Between Perinatal Sleep Quality and Depressive Symptoms
The association between sleep quality and depressive symptoms has long been discussed. However, the exploration of the relationship between sleep quality and perinatal depressive symptoms has only recently gained increasing attention.3,28,39,42 According to a few cross-sectional studies, poor sleep quality is associated with PND across different timepoints.25,27,30 Longitudinal studies have demonstrated that disturbed sleep is associated with the emergence of perinatal depressive symptoms; specifically, sleep disturbances in the first and/or second trimester predict depressive symptoms during the later pregnancy period.23,37 Meanwhile, subjective assessments of sleep disturbances in the second and/or third trimester also indicate that sleep disturbances are a predictor of PPD symptoms.22–24,38,42–48 Other findings have suggested that the effects of poor sleep quality on depressive symptoms persist even after delivery.26,29,49,50 Most of the existing studies have proven the association between sleep quality and depressive symptoms during the third trimester and postpartum period.39,42 However, evidence concerning the second trimester or earlier is scarce and inconsistent.34,37 Only a few studies have shed light on the early stage of pregnancy (before 20 gestation weeks).20,23,35,51,52
Moreover, most of the studies have first assessed sleep quality and depressive symptoms at one or two timepoints during the perinatal period, followed by an examination of the sleep quality’s immediate and/or prolonged impacts on depressive symptoms (ie, the effects at the same and/or later timepoints).24,26,29,34,37,38,43–45,47–50 Only a few studies have traced different trajectories of depressive symptoms and then either explored the quality of sleep as a risk factor—how sleep quality at one timepoint influenced each trajectory20,22 or interpreted the association between perinatal sleep quality and depressive symptoms in process models.23,53 Longitudinal studies which have drawn associations, by tracking both sleep quality and depressive symptoms changes from the time before 20 gestation weeks to the postpartum period, are lacking.
Both depressive symptoms and sleep quality fluctuate throughout the perinatal period; therefore, identifying the variations in their trajectories and interpreting the relationship between them is crucial. In this study, we aimed to explore: (1) the incidence of PND in Beijing Obstetrics and Gynecology Hospital, (2) the overall depressive symptoms’ trajectory from 15 gestation weeks to 3 months postpartum, and (3) how poor sleep quality dynamically impacts depressive symptoms during the perinatal period.
Materials and Methods
This study is part of “The study of risk factors, perinatal outcome, assessment, and management of PND in Beijing Obstetrics and Gynecology Hospital, Capital Medical University” (GRANT NO FCYYGL201902). The protocol was approved by the Ethics Committee of the Beijing Obstetrics and Gynecology Hospital, Capital Medical University (2019-KY-095-02).
Setting and Participants
In this cohort study, participants were enrolled during their first registered clinic visit (15–16 gestational weeks) in the Perinatal Department of Beijing Obstetrics and Gynecology Hospital of China in the period of January 2020 to June 2021. All participants signed the consent form and could understand the questionnaire’s meaning.
Procedure
The participants’ sociodemographic information was collected at the beginning of their enrollment (15–16 gestational weeks). Thereafter, the Chinese editions of the Postnatal Depression Scale (EPDS) and PSQI were administered at five timepoints; three times during pregnancy as follows: gestational weeks 15–18 (T1), weeks 28–32 (T2), weeks 36–37 (T3); and two after delivery: six-weeks postpartum (T4) and 3–4 months postpartum (T5).
The questionnaires were administered through an online survey platform for mobile phones that was specifically designed for this study. The questionnaires were automatically administered to the participants through the platform during their designated gestation weeks. Subsequently, participants were reminded—by the research group’s members and via auto-reminders delivered by the platform—to complete their questionnaires on time.
To ensure the questionnaires’ completeness, each participant was required to answer all the questions before submitting the questionnaire. “Lie detector questions”, such as “If you have read and answered all the questions truthfully, please select the following answer A (B, C, or D)”, were included randomly within each timepoint. The survey results were considered “valid” only if the participants answered all the “lie detector questions” correctly and finished at least three questionnaires from the T1 in sequence (N = 1416).
Measures
Sociodemographic Status
Participants’ sociodemographic data included their age, socioeconomic status (SES), marital status, and family’s monthly income; SES was weighted by occupation and educational background.54 The occupation was graded 1–5 points ranging from “Temporary workers or unemployed” to “Senior Professional Manager, Personnel, or Supervisor”. Educational background was graded 1–7 points ranging from “No schooling” to “Doctor or above”. Table 1 outlines the detailed scoring method. The two scores’ sum was recorded as the participants’ SES score ranging from 2 to 12.
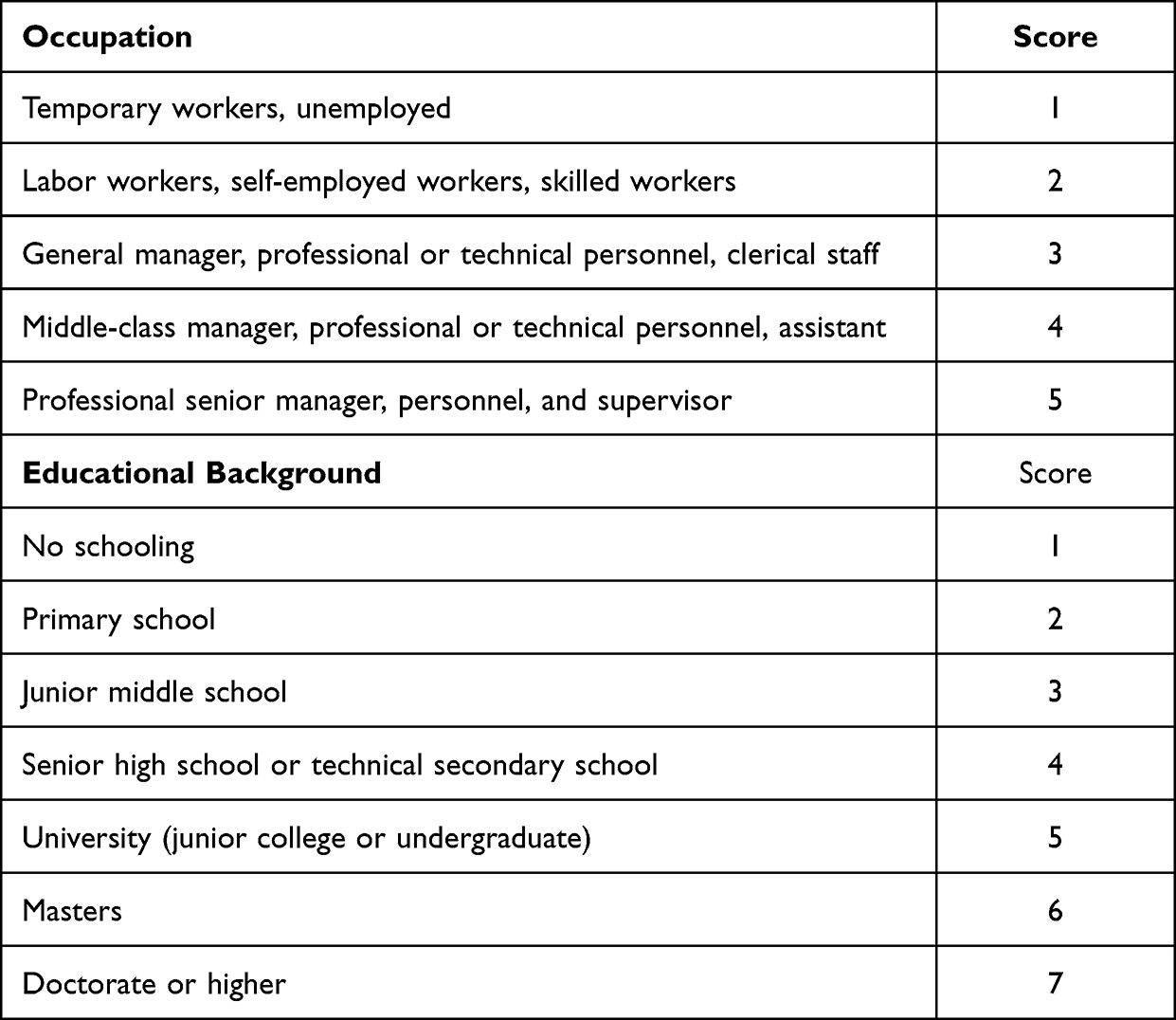 |
Table 1 Scoring for Socioeconomic Status: Occupation and Educational Background |
Depressive Symptoms
Participants’ depressive symptoms were assessed using the EPDS’ Chinese edition55 with 10 as the cutoff point.56 The scores’ total sum was used as a continuous variable for statistical analysis to produce a comprehensive measure at both clinical and subclinical levels. The Cronbach’s alphas ranged from 0.80 to 0.87, representing satisfactory internal reliability.
Sleep Quality
The PSQI is a self-report scale used to evaluate sleep quality. We evaluated study participants’ sleep quality using the PSQI’s Chinese edition; a score of 5 was the cutoff point.57 The total score was used as a continuous variable for further statistical analysis to interpret the association with the EPDS scores. The Cronbach’s alphas ranged from 0.80 to 0.84, representing satisfactory internal reliability.
Statistical Analysis
Statistical analyses were performed in three steps. First, SPSS 25.0 software was used to analyze the participants’ sociodemographic information, and depressive symptom incidences at each timepoint. Second, the latent growth curve (LGC) model was employed to explore depressive symptoms’ overall trajectory from early pregnancy to three months postpartum, using the Mplus 8.3 software. Finally, the LGC model with parallel processes model was utilized to analyze the association between the trajectories of depressive symptoms and sleep quality.
Missing Data
Missing data were treated by the full information maximum likelihood procedure (FIML), which processes estimated parameters iteratively based on complete cases instead of imputing them. The LGC model was fitted by Mplus 8.3 using maximum likelihood estimation with robust standard errors.
Results
Participants’ Sociodemographic Characteristics
Figure 1 is a flowchart of the study procedure; it presents the timeline of the study and the number of participant dropouts during each timepoint and the reasons for dropout. The average age of participants was 31.5 ±3.9 years, and the SES score was 8.2 ±1.0. The median monthly income was 20,000 (15,000–32,750) China Yuan (CNY). Of all the participants, 1411 cases (99.6%) were married while only 5 cases (0.4%) were single. No statistically significant difference regarding age (t = 1.283, p = 0.95, ns) or SES (t = 2.290, p = 0.46, ns) was noted between the participants who finished at least three measurements (N = 1416) and those who completed two or fewer measurements (n = 90).
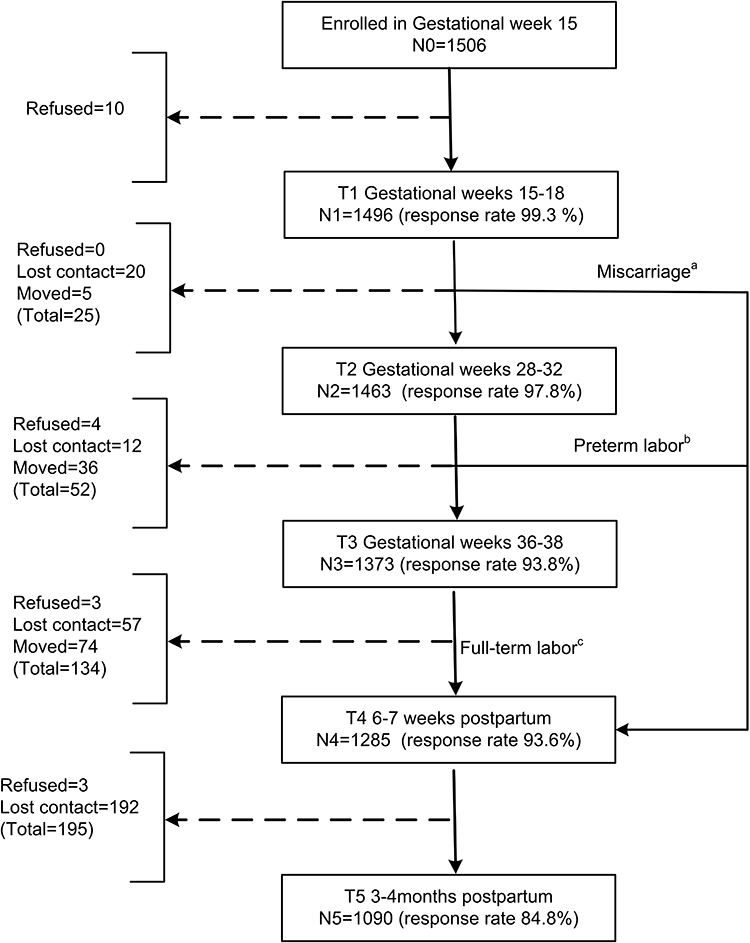 |
Figure 1 Flowchart of the study procedure. Participants finished at least 3 questionnaires N = 1416 (a + b + c). aMiscarriage = 5 (8 finished T1 + T4, 3 lost at T5). bPreterm labor = 38 (all finished T1 + T2 + T4). cFull-term labor = 1373. |
The Incidence of PND and Poor Sleep Quality at Different Timepoints
With 10 as the cutoff point of EPDS, the incidence of depressive symptoms was 7.9%, 6.6%, and 6.2% from T1–T3 (during pregnancy), respectively, and 11.4% and 11.5% from T4–T5 (postpartum), respectively. Overall, 336 cases (23.7%) screened positive at least once, while 1080 cases (76.3%) were below the cut-off value at all timepoints.
With 5 as the cutoff point of PSQI, the incidence of poor sleep quality was 35.6%, 37.2%, and 42.8% from T1–T3 (during pregnancy), respectively; thereafter, it went up to 55.1% at T4 (six weeks postpartum) and slightly descended to 47.3% at T5 (three months postpartum).
Trajectory of Perinatal Depressive Symptoms
The EPDS scores indicate that from T1 to T5, the progression of the trajectory of perinatal depressive symptoms follows a quadratic trend. The perinatal depressive symptoms trajectory fitted by the LGC model across the perinatal period followed a presumed U-shape trajectory, as presented in Figure 2. The depression model’s parameters were as follows: intercept = 1.687, p < 0.001; slope = −0.29, p < 0.05; quadratic coefficient = 0.323, p < 0.001. No association has been found between maternal age and all parameters (intercept, slope, or quadratic coefficient) of the trajectory when included as a potential confounder in the model (p > 0.05).
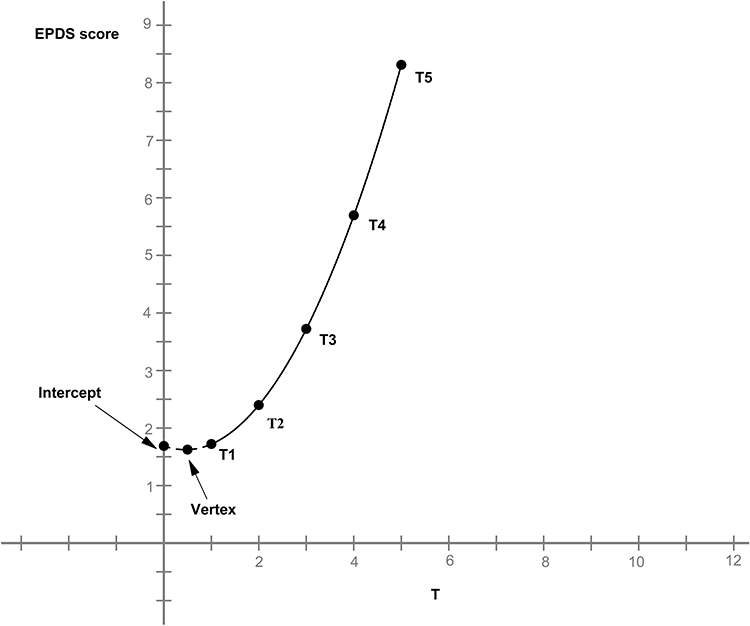 |
Figure 2 Trajectory of PND. The depression model’s parameters: Intercept = 1.687, p < 0.001; Slope = −0.29, p < 0.05; Quadratic coefficient = 0.323, p < 0.001. The presumed vertex (lowest point) of the parabola (coordinates X = 0.45, Y = 1.62) came before the T1. Abbreviations: EPDS, Edinburgh Postnatal Depression Scale; PND, Perinatal depression; CFI, Comparative Fit Index; TLI, Tucker-Lewis Index; RMSEA, Root Mean Square Error of Approximation. Notes: This figure was prepared using Mplus 8.3. The measures of the goodness-of-fit are as follows: χ2 = 2614.4, CFI = 0.987, TLI = 0.978, RMSEA = 0.063 (95% CI: 0.045–0.082). |
As illustrated in Figure 2, the presumed vertex (lowest point) of the parabola (coordinates X = 0.45, Y = 1.62) came before the T1 timepoint, and the scores of the EPDS from T1–T5 ascended progressively. The estimated EPDS mean score was 1.72 at early pregnancy (T1), increasing to 2.39 in the third trimester (T2), and continuing to increase to 3.70 before delivery (T3). After birth, the mean EPDS score was 5.65 at six weeks postpartum (T4), which increased to 8.36 at three months postpartum (T5).
Association Between the Trajectories of PND and Sleep Quality
The parallel processes model depicting the associations between the trajectories of depressive symptoms and sleep quality are presented in Figure 3. The figure depicts impacts of the intercept, slope, and quadratic coefficient of the perinatal depressive symptoms’ trajectory on each EPDS score. The effects of the intercept and slope of the sleep quality trajectory on different PSQI scores are also presented. Maternal age, which was included in the model as a possible confounder, only positively affected the intercept of sleep quality.
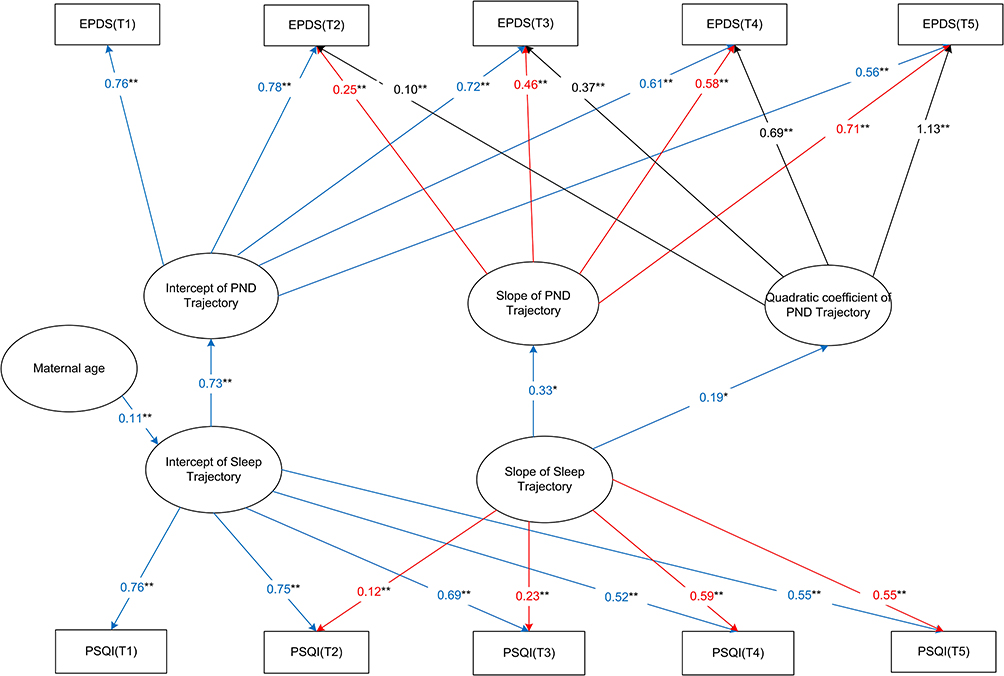 |
Figure 3 Parallel process model depicting associations between the trajectory of depressive symptoms and sleep quality. Abbreviations: EPDS, Edinburgh Postnatal Depression Scale; PND, PND; PSQI, Pittsburgh Sleep Quality Index; CFI, Comparative Fit Index; TLI, Tucker-Lewis Index; RMSEA, Root Mean Square Error of Approximation. Notes:This Figure was prepared using Mplus 8.3. *p < 0.05; **p < 0.001. The measures of the goodness-of-fit: χ2 = 5857.2, CFI = 0.950, TLI = 0.931, RMSEA = 0.072 (95% CI: 0.065–0.079). |
Regarding the association between perinatal sleep quality and depressive symptoms, three major results can be seen in Figure 3: 1) The intercept of sleep trajectory positively affects the intercept of depressive symptoms (β = 0.73, p < 0.001); thus, at the onset of the pregnancy, women with poorer sleep quality were more likely to exhibit more severe depressive symptoms. 2) The slope of sleep interacted with the slope of depression (β = 0.33, p < 0.05) such that a higher slope of sleep was followed by a higher the slope of depression. This implies that with progression of time, the rate of reduction of sleep quality increased; the likelihood that the participant would suffer more severe depressive symptoms also increased. 3) The slope of sleep positively affected the quadratic coefficient of depression (β = 0.19, p < 0.05). In other words, the higher the slope of sleep, the more likely that the x coordinate of the depression vertex would shift to the left. Again, our results showed that as time progressed, the more rapidly the reduction of sleep quality became, and the sooner a sudden deterioration of depressive symptom was likely to occur.
Discussion
Incidence and Trajectory of Perinatal Depressive Symptoms
To the best of our knowledge, this is the first study conducted in China to explore the association between sleep and perinatal depressive symptoms. In this study, participants were recruited from relatively developed regions of the country with higher SES. Compared with previous literature, the incidence of depressive symptoms at each timepoint in this study was lower than the incidence in developing countries and close to that in developed countries; nevertheless, the overall incidence of the entire perinatal period is in accordance with previous studies6–8 and is slightly higher than that of other reports in China.9 This indicates that nearly one in every five women might experience depression at least once during their perinatal period, which is a concern that should not be ignored.
Although the incidence of depressive symptoms descends slightly from T2–T3 and ascends after delivery, perinatal depressive symptoms’ trajectory—based on the EPDS scores—increases progressively with a quadratic trend from 15 gestation weeks to three months postpartum. The presumed vertex (lowest point) of the parabola exists before T1, which implies that the depressive symptoms might presumably be relieved in early pregnancy. Even though maternal age is often considered a relative risk factor for developing depressive symptoms, no relationship has been found between maternal age and the depression trajectory in this study. This reason for this could be due to all participants being in childbearing age (31.5 ±3.9 years old), meaning that there were not big age differences in the sample to allow us to observe the effect of maternal age on depression.
The trajectory described in this study is partly consistent with most previous literature, which included at least one continuously increasing trajectory from the second trimester to a few months postpartum.16,20,21,58 However, the trajectory in our study is not consistent with Figueiredo and Conde, who stated that depressive symptoms showed a significant decrease from the first to second trimesters, but the changes afterward were not significant.18 The differences might have occurred due to the different sample size, the cultural background of the participants, and the timepoints of the assessment (our study included the timepoint of 36–37 gestation weeks and 8 weeks postpartum, whereas Figueiredo and Conde set one different timepoint, which was at childbirth).
The Dynamic Relationship Between Sleep Quality and Depressive Symptoms
The sleep trajectory’s intercept affects the sleep quality from T1–T5, which indicates that entering pregnancy with elevated PSQI scores is associated with significantly worse sleep quality throughout the perinatal period. These results partly confirm the findings of prior studies.35 To our knowledge, this is one of the few studies interpreting the dynamic relationship between depressive symptoms and sleep quality with multi-point questionnaires from the second trimester to the postpartum period. Our findings contribute to the evidence in the literature regarding the association between poor sleep quality and PND.
According to the results of this study, poor sleep quality was associated with depressive symptoms from as early as the beginning of pregnancy. This is consistent with the results of previous studies.23,35,52 Our results are similar to those of Solomonova et al23 and Gueron-Sela et al.22 Solomonova et al reported that sleep disturbances in early pregnancy directly predict depressive symptoms in late pregnancy, and Gueron-Sela et al established that poor sleep quality in late pregnancy is associated with more depressive symptoms from 3 to 18 months postpartum. However, in this study, we prove—with a relatively larger sample size compared to previous studies—that sleep quality positively affects depressive symptoms from the beginning of a pregnancy to the postpartum period. Moreover, to our knowledge, this study is the first to interpret how the slope of the sleep quality trajectory affects the changes in depressive symptoms during the perinatal period. Our results indicate that as time progresses and sleep quality rapidly deteriorates, perinatal women are likely to experience more severe depressive symptoms, and their condition may deteriorate suddenly and rapidly. This means that a minor change in sleep quality might be a normal side effect of pregnancy; however, major decreases in sleep quality may be a significant risk factor of PND. This was partly in agreement with Tomfohr et al, who investigated sleep trajectories and their relationship with PND, and further predicted a potential threshold of change in sleep quality, indicating new-onset depression.35
PND’s etiology remains poorly understood but is assumed to be the result of a complex interaction involving genetics, epigenetics, the neuroendocrine hypothalamic-pituitary-adrenal (HPA) axis, and environmental and social factors.59,60 Research on other biological factors precipitating PND include the following: systemic inflammation, immune system dysregulation, alterations in cortisol and amylase, intrauterine artery resistance, thyroid dysregulation, alterations in oxytocin, and prolactin.47,61
Although the mechanisms linking sleep disturbances and depressive symptoms remain unclear, several mechanisms can underlie these processes. First, there is evidence that both sleep disturbances and depressive symptoms during pregnancy have been associated with the augmentation of inflammatory responses and changes in immune function.22 Okun et al have found that poor sleep quality is associated with higher circulating and stimulated levels of interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α). Such elevated levels of inflammatory markers have also been found in patients with depression;62,63 furthermore, insufficient sleep during pregnancy may disrupt the typical course of inflammatory “switch off”, leading to unfavorable maternal outcomes,64 including PND. Another likely contributing factor is the dramatic change in hormone levels.4,42 Reproductive hormones, especially estrogen and progesterone, are considered responsible for maintaining sleep quality in menopausal women.65,66 Relevant evidence obtained during the perinatal period is still sparse and disputed. However, the available evidence suggests that the interaction between poor sleep/insomnia and a dramatic decrease in hormones following childbirth may augment the risk of PND.4 Additionally, the impact of sleep disturbance on emotion regulation is another potential mediator. Disruptions in circadian/ultradian rhythms have been linked to alterations in emotional reactivity and the increased likelihood of perceiving ambiguous information as threatening, which may eventually lead to the emergence of a depressed mood.67 Finally, physiological hyperarousal, a known biomarker for sleep disorders, is also associated with depression and anxiety disorders.22
Despite the strong association between poor sleep and PND, routine sleep quality evaluation has not been included in prenatal visits and postpartum follow-ups. To date, most obstetric health providers still consider poor sleep quality during the perinatal period as attributable to normal pregnancy and postpartum changes; thus, its role as a PND risk factor is often overlooked. Interventions to improve perinatal sleep quality are not readily available and have rarely been studied. This study provides evidence that obstetric care providers, including obstetricians, midwives, pediatricians, psychiatrists, and general practitioners, should be more attentive to poor sleep quality in patients from early pregnancy through the postpartum period. Patient care standards should include an additional sleep quality evaluation for perinatal women with persistent complaints of poor sleep quality. Moreover, maternal care for those with rapidly deteriorating sleep quality should include depression assessments and referrals to mental health care providers, as these patients may benefit from prevention, screening, and early diagnosis of PND. Tailored interventions for poor sleep quality may relieve perinatal women from more severe sleep problems and depressive symptoms later during the perinatal period.
Limitations and Future Directions
This study had several limitations. Firstly, this was a single-centered study, in which most participants came from Chaoyang District, Beijing and has a similar SES; therefore, this should be considered when generalizing these results to other samples. Secondly, a score of “5” was used as the cut-off in the PSQI, which is in accordance with previous studies; however, that cutoff might not be valid for pregnant participants due to changes during pregnancy. Thirdly, the participants were first enrolled near the beginning of their second trimester (15–18 weeks) at their first routine visit, and evaluations ended at 3-months postpartum. Therefore, the data from the first trimester and from 3 to 12 months postpartum were not included in our analysis.
Regarding future research, we look forward to conducting multi-centered studies with larger sample sizes. To understand the fluctuation of depressive symptoms more specifically and thoroughly, we suggest a multi-centered study conducted with a larger sample, using repeated assessments at shorter intervals (especially starting at the beginning of/before pregnancy and ending at 1 year postpartum). Such a study may yield a more nuanced understanding of the trajectory. A topic to discuss in future articles are studies aiming to interpret the latent trajectory groups such as time-stable, linear trajectory or draw.
Conclusion
The trajectory of depressive symptoms, from 15 gestation weeks to three months postpartum, increases progressively with a quadratic trend. Poor sleep quality might be associated with depressive symptoms as early as the beginning of the pregnancy. Rapid reduction of sleep quality could be a significant risk factor of PND. As time progresses and sleep quality rapidly deteriorates, perinatal women are likely to experience more severe depressive symptoms, and their condition may deteriorate suddenly and rapidly. This evidence should serve to alert all obstetric care providers, including obstetricians and midwives, as well as pediatricians, psychiatrists, and general practitioners to the importance of poor sleep quality among women from early pregnancy through the postpartum period. Additionally, further evaluation of sleep quality should be advised for all perinatal women with persistent complaints of poor sleep quality. Those with rapidly deteriorating sleep quality may benefit from an assessment of depression and referral to mental healthcare providers for the prevention, screening, and early diagnosis of PND. Moreover, tailored interventions for poor sleep quality in perinatal women can prevent the development of more severe sleep problems and depressive symptoms later in the perinatal period.
Abbreviations
PND, Perinatal depression; AND, Antenatal Depression; PPD, postpartum depression; COVID-19, Corona Virus Disease 2019; EPDS, Edinburgh Postnatal Depression Scale; PSQI, Pittsburgh Sleep Quality Index; SES, socioeconomic status; LGC, latent class growth curve; FIML, full information maximum likelihood procedure; CNY, China Yuan; HPA, hypothalamic-pituitary-adrenal; IL-6, interleukin-6; TNF-α, tumor necrosis factor-α; CFI, Comparative Fit Index; TLI, Tucker-Lewis Index; RMSEA, Root Mean Square Error Of Approximation.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation as well as with the Helsinki Declaration of 1975, as revised in 2008. This study was approved by the ethical institutional review board of Beijing Obstetrics and Gynecology Hospital (2019-KY-095-02).
Acknowledgments
We dedicate our appreciation to all study participants. Additionally, we owe gratitude to our colleagues from the Department of Perinatal Medicine, Beijing Obstetrics and Gynecology Hospital, Capital Medical University for lending assistance with respect to the recruitment, follow-up, and data collection processes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Beijing Obstetrics and Gynecology Hospital, Capital Medical University (Grant No. FCYYGL201902). The funding organization played no role in the study design, data collection, data analysis, data interpretation, or writing of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Obstetrics Group CS of O and GCMA. Expert consensus on screening and diagnosis of perinatal depression. Chin J Obstet Gynecol. 2021;56(8):521–527.
2. Berry OO, Babineau V, Lee S, et al. Perinatal depression prevention through the mother-infant dyad: the role of maternal childhood maltreatment. J Affect Disord. 2021;290:188–196. doi:10.1016/j.jad.2021.04.068
3. Lawson A, Murphy KE, Sloan E, Uleryk E, Dalfen A. The relationship between sleep and postpartum mental disorders: a systematic review. J Affect Disord. 2015;176:65–77. doi:10.1016/j.jad.2015.01.017
4. Emamian F, Khazaie H, Okun ML, Tahmasian M, Sepehry AA. Link between insomnia and perinatal depressive symptoms: a meta-analysis. J Sleep Res. 2019;28(6). doi:10.1111/jsr.12858
5. American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 757: screening for perinatal depression. Obstet Gynecol. 2018;132(5):e208–e212. doi:10.1097/AOG.0000000000002927
6. Butler MS, Young SL, Tuthill EL. Perinatal depressive symptoms and breastfeeding behaviors: a systematic literature review and biosocial research agenda. J Affect Disord. 2021;283:441–471. doi:10.1016/j.jad.2020.11.080
7. Lenze SN, Potts MA, Rodgers J, Luby J. Lessons learned from a pilot randomized controlled trial of dyadic interpersonal psychotherapy for perinatal depression in a low-income population. J Affect Disord. 2020;271:286–292. doi:10.1016/j.jad.2020.03.084
8. Dagher RK, Bruckheim HE, Colpe LJ, Edwards E, White DB. Perinatal depression: challenges and opportunities. J Women's Health. 2021;30(2):154–159. doi:10.1089/jwh.2020.8862
9. Nisar A, Yin J, Waqas A, et al. Prevalence of perinatal depression and its determinants in Mainland China: a systematic review and meta-analysis. J Affect Disord. 2020;277:1022–1037. doi:10.1016/j.jad.2020.07.046
10. Sun G, Wang Q, Lin Y, et al. Perinatal depression of exposed maternal women in the COVID-19 pandemic in Wuhan, China. Front Psychiatry. 2020;11. doi:10.3389/fpsyt.2020.551812
11. Santos H, Tan X, Salomon R. Heterogeneity in perinatal depression: how far have we come? A systematic review. Arch Women's Ment Health. 2017;20(1):11–23. doi:10.1007/s00737-016-0691-8
12. Baron E, Bass J, Murray SM, Schneider M, Lund C. A systematic review of growth curve mixture modelling literature investigating trajectories of perinatal depressive symptoms and associated risk factors. J Affect Disord. 2017;223:194–208. doi:10.1016/j.jad.2017.07.046
13. Kiviruusu O, Pietikäinen JT, Kylliäinen A, et al. Trajectories of mothers’ and fathers’ depressive symptoms from pregnancy to 24 months postpartum. J Affect Disord. 2020;260:629–637. doi:10.1016/j.jad.2019.09.038
14. Matijasevich A, Murray J, Cooper PJ, et al. Trajectories of maternal depression and offspring psychopathology at 6 years: 2004 Pelotas cohort study. J Affect Disord. 2015;174:424–431. doi:10.1016/j.jad.2014.12.012
15. Dekel S, Ein-Dor T, Ruohomäki A, et al. The dynamic course of peripartum depression across pregnancy and childbirth. J Psychiatr Res. 2019;113:72–78. doi:10.1016/j.jpsychires.2019.03.016
16. Ahmed A, Feng C, Bowen A, Muhajarine N. Latent trajectory groups of perinatal depressive and anxiety symptoms from pregnancy to early postpartum and their antenatal risk factors. Arch Women's Ment Health. 2018;21(6):689–698. doi:10.1007/s00737-018-0845-y
17. Lim HA, Chua TE, Malhotra R, et al. Identifying trajectories of antenatal depression in women and their associations with gestational age and neonatal anthropometry: a prospective cohort study. Gen Hosp Psychiatry. 2019;61:26–33. doi:10.1016/j.genhosppsych.2019.09.001
18. Figueiredo B, Conde A. Anxiety and depression symptoms in women and men from early pregnancy to 3-months postpartum: parity differences and effects. J Affect Disord. 2011;132(1–2):146–157. doi:10.1016/j.jad.2011.02.007
19. Yu M, Li H, Xu D, Wu Y, Liu H, Gong W. Trajectories of perinatal depressive symptoms from early pregnancy to six weeks postpartum and their risk factors—a longitudinal study. J Affect Disord. 2020;275:149–156. doi:10.1016/j.jad.2020.07.005
20. Wikman A, Axfors C, Iliadis SI, Cox J, Fransson E, Skalkidou A. Characteristics of women with different perinatal depression trajectories. J Neurosci Res. 2020;98(7):1268–1282. doi:10.1002/jnr.24390
21. Christensen AL, Stuart EA, Perry DF, Le HN. Unintended pregnancy and perinatal depression trajectories in low-income, high-risk Hispanic immigrants. Prev Sci. 2011;12(3):289–299. doi:10.1007/s11121-011-0213-x
22. Gueron-Sela N, Shahar G, Volkovich E, Tikotzky L. Prenatal maternal sleep and trajectories of postpartum depression and anxiety symptoms. J Sleep Res. 2021;30(4):e13258. doi:10.1111/jsr.13258
23. Solomonova E, MacKinnon AL, Gold I, et al. Disordered sleep is related to delusional ideation and depression during the perinatal period. Sleep Health. 2020;6(2):179–184. doi:10.1016/j.sleh.2020.01.001
24. Gao M, Hu J, Yang L, et al. Association of sleep quality during pregnancy with stress and depression: a prospective birth cohort study in China. BMC Pregnancy Childbirth. 2019;19(1). doi:10.1186/s12884-019-2583-1
25. Lin W, Wu B, Chen B, et al. Sleep conditions associate with anxiety and depression symptoms among pregnant women during the epidemic of COVID-19 in Shenzhen. J Affect Disord. 2021;281:567–573. doi:10.1016/j.jad.2020.11.114
26. Lewis BA, Gjerdingen D, Schuver K, Avery M, Marcus BH. The effect of sleep pattern changes on postpartum depressive symptoms. BMC Women's Health. 2018;18(1). doi:10.1186/s12905-017-0496-6
27. Gelaye B, Addae G, Neway B, et al. Poor sleep quality, antepartum depression and suicidal ideation among pregnant women. J Affect Disord. 2017;209:195–200. doi:10.1016/j.jad.2016.11.020
28. Bei B, Coo S, Trinder J. Sleep and mood during pregnancy and the postpartum period. Sleep Med Clin. 2015;10(1):25–33. doi:10.1016/j.jsmc.2014.11.011
29. Okun ML, Mancuso RA, Hobel CJ, Schetter CD, Coussons-Read M. Poor sleep quality increases symptoms of depression and anxiety in postpartum women. J Behav Med. 2018;41(5):703–710. doi:10.1007/s10865-018-9950-7
30. Khadka R, Hong SA, Chang YS. Prevalence and determinants of poor sleep quality and depression among postpartum women: a community-based study in Ramechhap District, Nepal. Int Health. 2019;12(2):125–131. doi:10.1093/inthealth/ihz032
31. Hedman C, Pohjasvaara T, Tolonen U, Suhonen-Malm AS, Myllylä VV. Effects of pregnancy on mothers’ sleep. Sleep Med. 2002;3(1):37–42. doi:10.1016/S1389-9457(01)00130-7
32. Mindell JA, Cook RA, Nikolovski J. Sleep patterns and sleep disturbances across pregnancy. Sleep Med. 2015;16(4):483–488. doi:10.1016/j.sleep.2014.12.006
33. Sedov ID, Cameron EE, Madigan S, Tomfohr-Madsen LM. Sleep quality during pregnancy: a meta-analysis. Sleep Med Rev. 2018;38:168–176. doi:10.1016/j.smrv.2017.06.005
34. Polo-Kantola P, Aukia L, Karlsson H, Karlsson L, Paavonen EJ. Sleep quality during pregnancy: associations with depressive and anxiety symptoms. Acta Obstet Gynecol Scand. 2017;96(2):198–206. doi:10.1111/aogs.13056
35. Tomfohr LM, Buliga E, Letourneau NL, Campbell TS, Giesbrecht GF. Trajectories of sleep quality and associations with mood during the perinatal period. Sleep. 2015;38(8):1237–1245. doi:10.5665/sleep.4900
36. Kang AW, Pearlstein TB, Sharkey KM. Changes in quality of life and sleep across the perinatal period in women with mood disorders. Qual Life Res. 2020;29(7):1767–1774. doi:10.1007/s11136-020-02437-1
37. Eichler J, Schmidt R, Hiemisch A, Kiess W, Hilbert A. Gestational weight gain, physical activity, sleep problems, substance use, and food intake as proximal risk factors of stress and depressive symptoms during pregnancy. BMC Pregnancy Childbirth. 2019;19(1). doi:10.1186/s12884-019-2328-1
38. Tham EKH, Tan J, Chong YS, et al. Associations between poor subjective prenatal sleep quality and postnatal depression and anxiety symptoms. J Affect Disord. 2016;202:91–94. doi:10.1016/j.jad.2016.05.028
39. González-Mesa E, Cuenca-Marín C, Suarez-Arana M, et al. Poor sleep quality is associated with perinatal depression. A systematic review of last decade scientific literature and meta-analysis. J Perinat Med. 2019;47(7):689–703. doi:10.1515/jpm-2019-0214
40. Osnes RS, Eberhard-Gran M, Follestad T, Kallestad H, Morken G, Roaldset JO. Mid-pregnancy insomnia is associated with concurrent and postpartum maternal anxiety and obsessive-compulsive symptoms: a prospective cohort study. J Affect Disord. 2020;266:319–326. doi:10.1016/j.jad.2020.01.140
41. Sivertsen B, Hysing M, Dørheim SK, Eberhard-Gran M. Trajectories of maternal sleep problems before and after childbirth: a longitudinal population-based study. BMC Pregnancy Childbirth. 2015;15:129. doi:10.1186/s12884-015-0577-1
42. Okun ML. Disturbed sleep and postpartum depression. Curr Psychiatry Rep. 2016;18(7):66. doi:10.1007/s11920-016-0705-2
43. Zhou H, Li W, Ren Y. Poor sleep quality of third trimester exacerbates the risk of experiencing postnatal depression. Psychol Health Med. 2020;25(2):229–238. doi:10.1080/13548506.2018.1549738
44. Koutra K, Vassilaki M, Georgiou V, et al. Pregnancy, perinatal and postpartum complications as determinants of postpartum depression: the Rhea mother-child cohort in Crete, Greece. Epidemiol Psychiatr Sci. 2018;27(3):244–255. doi:10.1017/S2045796016001062
45. Obeysekare JL, Cohen ZL, Coles ME, et al. Delayed sleep timing and circadian rhythms in pregnancy and transdiagnostic symptoms associated with postpartum depression. Transl Psychiatry. 2020;10. doi:10.1038/s41398-020-0683-3
46. Okun ML. Sleep and postpartum depression. Curr Opin Psychiatry. 2015;28(6):490–496. doi:10.1097/YCO.0000000000000206
47. Maghami M, Shariatpanahi SP, Habibi D, et al. Sleep disorders during pregnancy and postpartum depression: a systematic review and meta-analysis. Int J Dev Neurosci. 2021;81(6):469–478. doi:10.1002/jdn.10118
48. Pietikäinen JT, Polo-Kantola P, Pölkki P, Saarenpää-Heikkilä O, Paunio T, Paavonen EJ. Sleeping problems during pregnancy—a risk factor for postnatal depressiveness. Arch Women's Ment Health. 2019;22(3):327–337. doi:10.1007/s00737-018-0903-5
49. Okun ML, Luther J, Prather AA, Perel JM, Wisniewski S, Wisner KL. Changes in sleep quality, but not hormones predict time to postpartum depression recurrence. J Affect Disord. 2011;130(3):378–384. doi:10.1016/j.jad.2010.07.015
50. Creti L, Libman E, Rizzo D, et al. Sleep in the postpartum: characteristics of first-time, healthy mothers. Sleep Disord. 2017;2017:8520358. doi:10.1155/2017/8520358
51. Yu Y, Li M, Pu L, et al. Sleep was associated with depression and anxiety status during pregnancy: a prospective longitudinal study. Arch Women's Ment Health. 2017;20(5):695–701. doi:10.1007/s00737-017-0754-5
52. Okun ML, Kline CE, Roberts JM, Wettlaufer B, Glover K, Hall M. Prevalence of sleep deficiency in early gestation and its associations with stress and depressive symptoms. J Women's Health. 2013;22(12):1028–1037. doi:10.1089/jwh.2013.4331
53. Saxbe DE, Schetter CD, Guardino CM, et al. Sleep quality predicts persistence of parental postpartum depressive symptoms and transmission of depressive symptoms from mothers to fathers. Ann Behav Med. 2016;50(6):862–875. doi:10.1007/s12160-016-9815-7
54. Lin N, Bian Y. Getting ahead in Urban China. Am J Sociol. 1991;97(3):657–688. doi:10.1086/229816
55. Wang Y, Guo X, Lau Y, Chan KS, Yin L, Chen J. Psychometric evaluation of the Mainland Chinese version of the Edinburgh Postnatal Depression Scale. Int J Nurs Stud. 2009;46(6):813–823. doi:10.1016/j.ijnurstu.2009.01.010
56. Xiayu F, Xiong C, Yunzhi Z. Cut-off value analysis of Edinburgh postnatal Depression Scale in prenatal depression screening of women in third trimester. Chin J Clin Obstetr Gynecol. 2018;19:2.
57. Fabbri M, Beracci A, Martoni M, Meneo D, Tonetti L, Natale V. Measuring subjective sleep quality: a review. Int J Environ Res Public Health. 2021;18(3):1–57. doi:10.3390/ijerph18031082
58. Mora PA, Bennett IM, Elo IT, Mathew L, Coyne JC, Culhane JF. Distinct trajectories of perinatal depressive symptomatology: evidence from growth mixture modeling. Am J Epidemiol. 2008;169(1):24–32. doi:10.1093/aje/kwn283
59. Dickens MJ, Pawluski JL. The HPA axis during the perinatal period: implications for perinatal depression. Endocrinology. 2018;159(11):3737–3746. doi:10.1210/en.2018-00677
60. van Niel MS, Payne JL. Perinatal depression: a review. Cleve Clin J Med. 2020;87(5):273–277. doi:10.3949/ccjm.87a.19054
61. McEvoy K, Payne JL, Osborne LM. Neuroactive steroids and perinatal depression: a review of recent literature. Curr Psychiatry Rep. 2018;20(9). doi:10.1007/s11920-018-0937-4
62. Okun ML, Coussons-Read ME. Sleep disruption during pregnancy: how does it influence serum cytokines? J Reprod Immunol. 2007;73(2):158–165. doi:10.1016/j.jri.2006.06.006
63. Okun ML, Hall M, Coussons-Read ME. Sleep disturbances increase interleukin-6 production during pregnancy: implications for pregnancy complications. Reprod Sci. 2007;14(6):560–567. doi:10.1177/1933719107307647
64. Okun ML. Sleep disturbances and modulations in inflammation: implications for pregnancy health. Soc Personal Psychol Compass. 2019;13(5):e12451. doi:10.1111/spc3.12451
65. Saletu-Zyhlarz G, Anderer P, Gruber G, et al. Insomnia related to postmenopausal syndrome and hormone replacement therapy: sleep laboratory studies on baseline differences between patients and controls and double-blind, placebo-controlled investigations on the effects of a novel estrogen-progestogen combination (ClimodienR, LafammeR) versus estrogen alone. J Sleep Res. 2003;12(3):239–254. doi:10.1046/j.1365-2869.2003.00356.x
66. Hachul H, Bittencourt LRA, Andersen ML, Haidar MA, Baracat EC, Tufik S. Effects of hormone therapy with estrogen and/or progesterone on sleep pattern in postmenopausal women. Int J Gynaecol Obstet. 2008;103(3):207–212. doi:10.1016/j.ijgo.2008.07.009
67. Baglioni C, Spiegelhalder K, Lombardo C, Riemann D. Sleep and emotions: a focus on insomnia. Sleep Med Rev. 2010;14(4):227–238. doi:10.1016/j.smrv.2009.10.007
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Sleep Quality and Self-Efficacy Trajectories Among Pregnant Women: A Parallel Process Latent Growth Curve Model
Mei X, Li Y, Wu X, Liang M, Chen Q, Kang L, Ye Z
Nature and Science of Sleep 2025, 17:1405-1419
Published Date: 19 June 2025
Trajectories of Perinatal Depressive Symptoms from the Second Trimester to Three Months Postpartum and Their Dynamic Relationship with Social Support: A Prospective Cohort Study in Beijing, China
Wang C, Hou J, Li A, Chen Y
International Journal of Women's Health 2026, 18:570352
Published Date: 13 March 2026