Back to Journals » International Journal of Women's Health » Volume 18
Trajectories of Perinatal Depressive Symptoms from the Second Trimester to Three Months Postpartum and Their Dynamic Relationship with Social Support: A Prospective Cohort Study in Beijing, China
Authors Wang C ![]() , Hou J, Li A, Chen Y
, Hou J, Li A, Chen Y
Received 30 November 2025
Accepted for publication 27 February 2026
Published 13 March 2026 Volume 2026:18 570352
DOI https://doi.org/10.2147/IJWH.S570352
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Chen Wang,1 Jinqin Hou,2 Anning Li,3 Yi Chen1
1Department of Perinatal Medicine, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, Beijing, People’s Republic of China; 2Department of Special Education and Psychology, National Institute of Education Sciences, Beijing, People’s Republic of China; 3The National Clinical Research Center for Mental Disorders & Beijing Key Laboratory of Mental Disorders, Beijing Anding Hospital, Capital Medical University, Beijing, People’s Republic of China; Advanced Innovation Center for Human Brain Protection, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Yi Chen, Department of Perinatal Medicine, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, No. 251 Yaojiayuan Road, Chaoyang District, Beijing, People’s Republic of China, Tel +86 186 1194 2798, Email [email protected]
Purpose: Social support has long been recognised as one of the most important extrinsic factors influencing perinatal depressive symptoms, yet few cohort studies have simultaneously tracked changes in both domains. This study aimed to identify heterogeneous trajectories of depressive symptoms and to examine their dynamic association with social support across the perinatal period.
Patients and Methods: A prospective cohort study was conducted in Beijing, enrolling participants at 15 gestational weeks. Depressive symptoms were assessed using the Edinburgh Postnatal Depression Scale (EPDS), and social support was measured with the Social Support Rating Scale (SSRS) at five time points from enrolment to three months postpartum. A total of 1416 women completed at least three assessments. The overall trajectory of depressive symptoms was estimated using LGCM, and LCGM was used to identify heterogeneous subgroups. The association between depressive symptoms and social support over time was examined using a parallel-process growth model.
Results: The overall EPDS trajectory showed a progressive increase from mid-pregnancy to three months postpartum. Two latent trajectories were identified: an ascending–low symptom group (72.2%) with initially low but gradually increasing symptom levels, and a persistently elevated symptom group (27.8%) with persistently elevated symptoms. After accounting for social support, the overall trajectory flattened into a stabilized linear pattern. In subgroup analyses, higher symptom levels were observed in both groups in models not accounting for social support; notably, the formerly ascending–low symptom group transformed into a stable linear trajectory at a higher level.
Conclusion: From 15 weeks of gestation to three months postpartum, perinatal depressive symptoms showed an overall increasing trend. However, substantial heterogeneity was observed: approximately 70% of women followed an ascending–low symptom trajectory, whereas about 30% exhibited persistently elevated symptoms with minimal change over time. Higher social support was associated with less worsening of depressive symptoms over the perinatal period, and this association appeared stronger during pregnancy than postpartum, particularly among women with lower initial symptom levels. These findings suggest that strengthening social support across pregnancy and the postpartum period may contribute to mitigating symptom worsening and promoting improved maternal mental health.
Keywords: perinatal depression, social support, trajectory, latent growth curve, cohort study
Introduction
Epidemiology and Temporal Patterns of Perinatal Depressive Symptoms
Perinatal depression (PND) refers to depressive symptoms occurring during pregnancy (antenatal depression, AND) and up to one year postpartum (postpartum depression, PPD).1 PND—among the most common obstetric complications—adversely affects both maternal and child well-being. Over the past several decades, epidemiological research on perinatal depressive symptoms has received substantial global attention. However, much of the existing evidence has been derived from screening-based assessments and cross-sectional designs. Prevalence estimates therefore vary widely across countries and regions, partly owing to differences in social, economic, and cultural contexts, as well as variation in assessment timing, measurement instruments, and cutoff thresholds. During pregnancy, the prevalence of depressive symptoms ranges from 7% to 20% in high-income countries and exceeds 20% in many low- and middle-income countries; postpartum depressive symptoms are estimated to affect 7–30% of women globally and up to 45% in some low-resource settings.2 In China, a recent meta-analysis reported pooled prevalence estimates of 16.3% for PND, 19.7% for AND, and 14.8% for PPD.3 While these prevalence figures underscore the substantial public health burden of perinatal depressive symptoms, single time-point estimates provide limited insight into how symptoms change across pregnancy and the postpartum period. In recent years, research has increasingly adopted repeated assessments to characterize symptom trajectories over time. Such approaches better capture dynamic fluctuations and help identify critical periods of change, as well as factors associated with symptom persistence or progression. Evidence to date suggests that symptom dynamics may differ across settings. Early studies from Europe and the United States have reported a generally decreasing pattern from pregnancy to several months postpartum,4–6 whereas a recent study in China observed a progressive increase from mid-pregnancy to three months postpartum with a curvilinear pattern.2 These cross-context differences highlight the importance of examining temporal patterns rather than relying solely on static prevalence estimates. Moreover, population-average trends may mask meaningful individual differences, highlighting the need to investigate heterogeneous trajectories of perinatal depressive symptoms among different groups of women.7,8
Heterogeneous Trajectories of Perinatal Depressive Symptoms
Beyond population-average trends, substantial heterogeneity has been observed in perinatal depressive symptoms across the perinatal period. Women differ not only in overall symptom severity but also in the timing of onset, trajectory shape, and persistence of symptoms. This recognition has led to increasing use of trajectory-based analytic approaches, which allow researchers to identify clinically meaningful subgroups rather than relying solely on average symptom patterns. To date, most trajectory research has focused primarily on postpartum depressive symptoms, often initiating assessments in late pregnancy or the early postpartum weeks and extending follow-up into the first year after childbirth. Across studies, the most frequently identified pattern is a persistently low-symptom trajectory encompassing the majority of women, accompanied by smaller subgroups demonstrating increasing, decreasing, or fluctuating symptom courses. A minority of women typically exhibit persistently moderate-to-high symptom levels across follow-up, with symptom changes often most pronounced during the early postpartum months before stabilizing thereafter.7–9
In contrast, heterogeneity in antenatal depressive symptoms has received comparatively less attention, and many studies have relied on limited assessments during pregnancy. Evidence from Europe and North America suggests that antenatal symptom trajectories often differ primarily in overall severity (eg, low-, moderate-, and high-symptom groups), with relatively modest change across pregnancy.10–13 Studies from less-resourced settings remain limited, but available data from regions such as India and South Korea have described additional increasing and decreasing antenatal patterns.14,15 Notably, a study from southern China with more intensive repeated measurements reported more pronounced symptom fluctuations across pregnancy and into the postpartum period,16 indicating variability in trajectory patterns across settings. Together, these findings highlight the need to examine heterogeneous trajectories spanning both pregnancy and postpartum, particularly in settings where sociocultural and healthcare environments may shape symptom patterns in distinct ways. These observations underscore the importance of considering contextual influences when investigating changes in perinatal depressive symptoms over time.
Social Support in Relation to Perinatal Depressive Symptom Trajectories
A substantial body of research has consistently identified social support as one of the most influential contextual factors associated with variations in perinatal depressive symptoms.17,18 Social support is commonly conceptualized as operating through stress-buffering and resource-related mechanisms, including emotional reassurance, practical assistance, and informational guidance. To date, both domestic and international studies have underscored its beneficial role,10,19,20 with evidence spanning diverse nationalities, cultural contexts, socioeconomic strata, and even vulnerable populations such as immigrants, adolescents, and women living with HIV.21–25 More recently, since the onset of the COVID-19 pandemic, numerous studies have reported rising rates of perinatal depressive symptoms in parallel with reduced social support resulting from lockdowns, isolation, and other public-health measures.20,26–29
Although a considerable body of research has identified associations between social support and perinatal depressive symptoms, most prior studies have relied on cross-sectional designs.18,20–22,30–38 Wikman10 and Khanlari11 demonstrated that lower spousal involvement in household and childcare responsibilities was associated with postpartum depressive symptoms.39 In certain cultural contexts—including China, other parts of Asia, and the Middle East—support provided by mothers-in-law has been identified as an important correlate of perinatal depressive symptoms.34,40 In contrast, relatively few studies have incorporated repeated measurements across pregnancy and postpartum, and most have focused primarily on the postpartum phase rather than examining social support as a dynamic correlate across the perinatal period. Choi et al34 reported that women with low social support, measured at a single time point, were more likely to belong to “worsening depression” and “persistent depression” trajectories. Similarly, Ahmed et al35 found that inadequate social support increased the likelihood of both antenatal and postpartum depression trajectories. Although these studies adopted trajectory-based approaches, both relied on categorical indicators of support availability rather than standardized quantitative measures. More recent studies have begun to use validated scales to quantify social support and have reported broadly consistent findings. Al-Abri,32 Bhushan,15 Fuhr,38 and Matsumura39 have utilized validated scales to quantify social support, reporting broadly consistent findings. Al-Abri32 assessed support levels dynamically from late pregnancy to 8 weeks postpartum but did not explicitly examine whether temporal changes in social support were associated with depressive symptom trajectories. Fuhr38 noted that women with greater support during late pregnancy were more likely to experience spontaneous remission of postpartum depressive symptoms, while Matsumura39 and Hagaman40 reported that antenatal social support was associated with a reduced likelihood of postpartum depressive symptoms up to one year after childbirth. In China, research on perinatal depressive symptom trajectories and their correlates remains scarce, and the limited longitudinal evidence has largely focused on point-to-point associations between social support and depressive symptoms rather than trajectory-based approaches. For instance, Zheng et al41 assessed social support and depressive symptoms at three postpartum time points (day 3, month 3, and month 6), providing important descriptive evidence but without modelling distinct symptom trajectories or examining whether within-person changes in support were associated with trajectory patterns. Gao37 examined cross-lagged associations during the postpartum period, emphasizing bidirectional relationships rather than heterogeneity in symptom trajectories across the full perinatal window.
These studies differ markedly in sample size, study populations, cultural and socioeconomic settings, forms of support, and measurement instruments. Despite these differences, most studies have conceptualized social support as a static exposure, overlooking its inherently dynamic nature during the perinatal transition. Yet this period is characterized by continuous social and relational adjustments, during which the relevance and impact of support may change. Consequently, single time-point assessments may fail to capture how support relates to evolving depressive symptoms across pregnancy and postpartum. Moreover, compared with many Western settings, social support in China is often more family-centered, relatively less flexible in structure. During pregnancy, women often receive structured antenatal care and sustained professional monitoring; after childbirth, however, support tends to shift toward more task-oriented assistance within intensified caregiving demands. Under such conditions, mothers’ physical discomfort and psychological needs may receive comparatively less explicit attention. In addition, the availability and integration of educational, community-based, and welfare supports for postpartum women may warrant further development. Taken together, these gaps highlight the need for a cohort study that repeatedly measures both depressive symptoms and social support across the perinatal period, to clarify how dynamic changes in support relate to heterogeneous depressive symptom trajectories, particularly in the Chinese context.
Accordingly, the present study aimed to: (1) characterize the overall trajectory of perinatal depressive symptoms from 15 weeks of gestation to 3 months postpartum; (2) identify distinct latent trajectories of perinatal depressive symptoms; and (3) repeatedly assess social support and examine how changes in social support are associated with these symptom trajectories.
Materials and Methods
This study was embedded within an ongoing prospective perinatal cohort at Beijing Obstetrics and Gynecology Hospital, Capital Medical University, which has supported multiple research aims addressing different perinatal health factors. A prior publication from this cohort examined perinatal depressive symptom trajectories in relation to sleep quality, whereas the present study focuses on the dynamic association between depressive symptom trajectories and social support across the perinatal period.
This cohort study was conducted in the Department of Perinatal Medicine at Beijing Obstetrics and Gynecology Hospital, Capital Medical University, China. From January 2020 to June 2021, pregnant women attending their first prenatal visit at 15–16 gestational weeks were consecutively recruited. Participants were eligible if they were aged ≥18 years, were able to read and understand the questionnaires, and provided written informed consent prior to participation. Women were excluded if they had a documented history of severe mental disorders (eg, bipolar disorder or psychotic disorders), had serious medical conditions that precluded participation, or were unable to complete the follow-up assessments.
Procedure
Participants were recruited during routine antenatal care visits at Beijing Obstetrics and Gynecology Hospital and were enrolled at 15–16 gestational weeks after providing written informed consent. The participants’ sociodemographic characteristics, past medical history (PMH), family history, and obstetric history were collected at enrollment (15–16 gestational weeks). Subsequently, the Chinese versions of the EPDS and SSRS were administered at five time points: three during pregnancy—15–18 weeks (T1), 28–32 weeks (T2), and 36–37 weeks (T3)—and two postpartum, at six weeks (T4) and 3–4 months (T5).
All questionnaires were administered via a purpose-built mobile-compatible online survey platform. The system automatically distributed questionnaires at the prespecified gestational weeks and postpartum time points, and participants were required to complete all items before submission to minimize missing data. To enhance data quality, “attention-check” items (eg, “If you have read and answered all questions truthfully, please select option A”) were embedded at random positions in each survey. Responses were considered valid only if participants answered all attention-check items correctly, otherwise, the survey was excluded. For the present analyses, we included women who completed at least three assessments starting from T1 (N = 1416).
Measures
Sociodemographic Characteristics, PMH, Family History, and Obstetric History
Participants’ sociodemographic information included age, occupation, educational background, marital status, smoking status, and monthly household income. Occupation was scored on a 1–5 scale, ranging from “temporary worker or unemployed” to “senior professional manager, personnel, or supervisor”. Educational background was scored on a 1–7 scale, ranging from “no schooling” to “doctoral degree or above”. Past medical history (PMH) included participants’ previous acute or chronic physical and mental conditions, particularly any history of depression. Participants with psychiatric disorders other than depression were excluded. Information on family history of depressive disorders among first-degree relatives was collected. Obstetric history data included parity, planned versus unplanned pregnancy, and any previous pregnancy loss, including spontaneous abortion, stillbirth, fetal malformation, or neonatal death.
Depressive Symptoms
Depressive symptoms were assessed using the validated Chinese version of the Edinburgh Postnatal Depression Scale (EPDS), a widely used screening instrument for perinatal depressive symptoms; in Chinese populations, a score of 10 or higher is commonly used as a threshold to indicate elevated symptoms.42 In the present study, EPDS total scores were analyzed as a continuous variable to capture the full spectrum of symptom severity across both subclinical and clinically relevant levels. Cronbach’s alpha coefficients ranged from 0.80 to 0.87, indicating good internal consistency.
Social Support
Social support was measured using the Social Support Rating Scale (SSRS)43 originally developed by Xiao Shuiyuan in 1986. The SSRS comprises 10 items across three dimensions: objective support (3 items), subjective support (4 items), and utilization of social support (3 items). Higher scores reflect higher levels of perceived social support. In this study, the total SSRS score was treated as a continuous variable to assess its association with perinatal depressive symptoms. The internal consistency of the SSRS in this sample ranged from 0.83 to 0.86.
Sample Size Consideration
Because no universally accepted formula exists for determining sample size in latent growth and latent class growth models, sample size was considered based on repeated measurements, model complexity, and class size. The analytic sample included 1416 participants with at least three assessments across five time points. The smallest latent class comprised 27.8% of the sample, supporting stable estimation and classification for the planned LGCM, LCGM, and parallel-process LGCM analyses.
Statistical Analysis
All statistical analyses were conducted in three stages. First, descriptive statistics were computed for participants’ sociodemographic characteristics, psychiatric history, obstetric history, and depressive symptoms at each time point using SPSS version 25.0. Second, a latent growth curve model (LGCM) was fitted using Mplus version 8.3 to estimate the overall trajectory of depressive symptoms from mid-pregnancy to three months postpartum. Model fit was evaluated using χ2, Comparative Fit Index (CFI), Tucker–Lewis Index (TLI), and Root Mean Square Error of Approximation (RMSEA), with CFI/TLI ≥ 0.90 and RMSEA ≤ 0.08 indicating acceptable model fit. Third, a latent class growth model (LCGM) was applied to identify heterogeneous trajectories of depressive symptoms. Model fit indices included Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), adjusted BIC (aBIC), Entropy, Lo–Mendell–Rubin likelihood ratio test (LMR–LRT), and Bootstrap likelihood ratio test (BLRT). Lower AIC/BIC/aBIC values and Entropy > 0.80 indicated better model quality and reliable classification. Finally, a parallel-process LGCM was conducted to examine the association between the growth processes of depressive symptoms and social support.
Missing Data
Missing data were handled using full information maximum likelihood (FIML), which estimates model parameters using all available data under the assumption that data are missing at random (MAR), without imputing missing values. All latent growth models were fitted in Mplus version 8.3 using maximum likelihood estimation with robust standard errors (MLR).
Results
Participants’ Characteristics
Figure 1 illustrates the recruitment process and response rates across different time points. A total of 1416 participants completed at least three assessments and were included in the final analyses. The mean age of participants was 31.5 ± 3.9 years. The median occupation score was 3 (IQR: 3–3), and the median education score was 5 (IQR: 5–5). The median monthly household income was 20,000 CNY (IQR: 15,000–32,750). Other sociodemographic, medical, and obstetric characteristics, including parity, pregnancy planning, and previous pregnancy loss, are presented in Table 1.
 |
Table 1 Participants’ Sociodemographic Characteristics (N = 1416) |
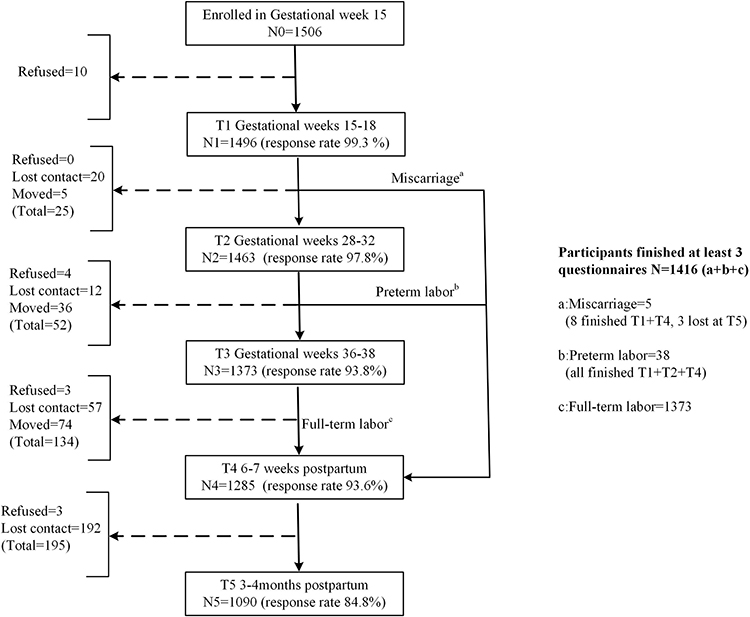 |
Figure 1 Participant recruitment process and response rates across assessment time points. |
Overall Trajectory of Perinatal Depressive Symptoms
Across the cohort, depressive symptoms increased from mid-pregnancy to three months postpartum (Figure 2). The latent growth curve model (LGCM) demonstrated acceptable model fit (χ2 = 2614.4, CFI = 0.987, TLI = 0.978, RMSEA = 0.063). Detailed model parameters are provided in the figure legend.
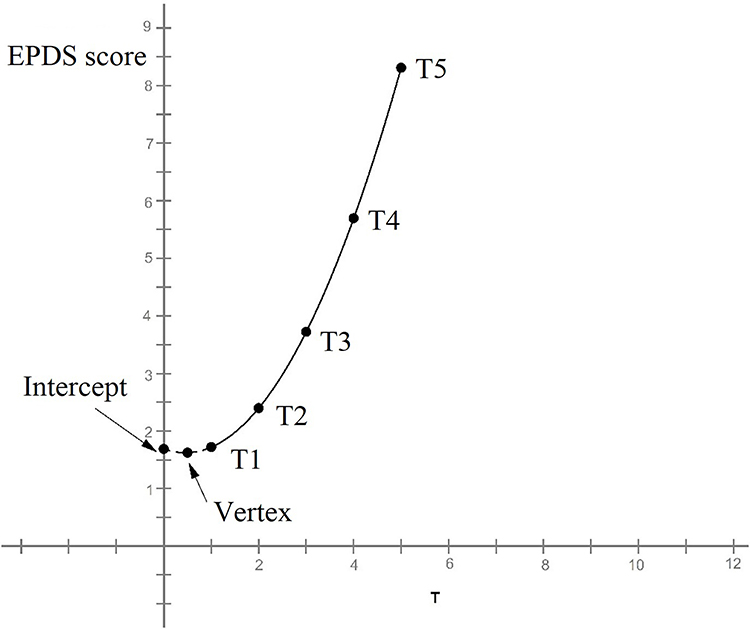 |
Figure 2 Overall trajectory of perinatal depressive symptoms (G). The figure was generated using Mplus version 8.3. Model parameters: Intercept = 1.687 (p < 0.001); Slope = –0.29 (p < 0.05); Quadratic coefficient = 0.323 (p < 0.001). Abbreviations: EPDS, Edinburgh Postnatal Depression Scale; PND, perinatal depressive symptoms. |
Latent Trajectories of Perinatal Depressive Symptoms
To capture heterogeneity in symptom change over time, latent class growth modeling (LCGM) identified two distinct depressive symptom trajectories among the 1416 participants (Figure 3). The 2-class solution was selected based on a significant LMR-LRT (1435.61, p<0.001), acceptable classification quality (entropy=0.826), and model parsimony; the LMR-LRT was not significant for the 3-class and 4-class models (p=0.131 and 0.385, respectively). The 2-class model also showed favorable fit indices (AIC=33,167.5; BIC=33,267.4; aBIC=33,207.0). Group 1, the ascending–low symptom group (G1; n = 1023; 72.2%) exhibited a progressively increasing curvilinear trajectory from T1 to T5, but with relatively low overall symptom levels. Group 2, the persistently elevated symptom group (G2; n = 393; 27.8%) displayed a relatively stable linear trajectory, showing minimal change from T1 to T5, yet maintaining consistently higher symptom levels throughout the observation period.
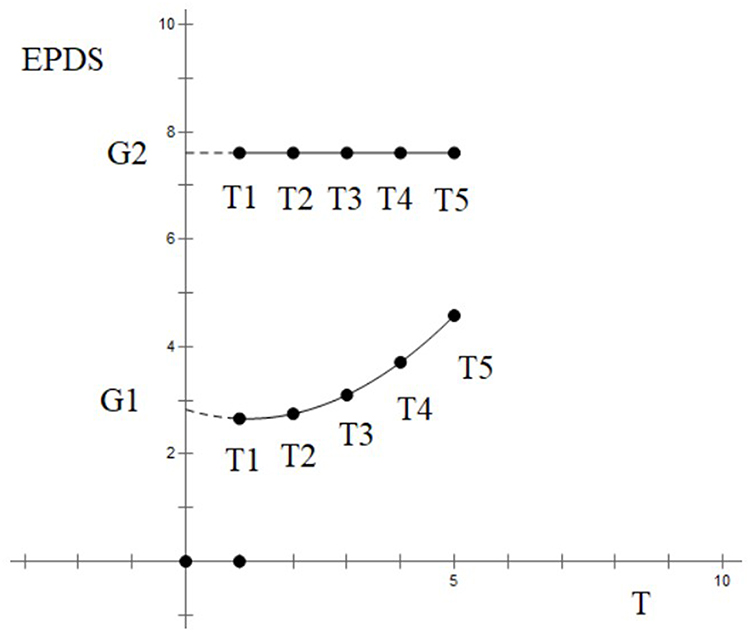 |
Figure 3 Latent trajectories of perinatal depressive symptoms. The figure was generated using Mplus version 8.3. Group 1 (G1; ascending–low symptom group, n = 1023; 72.2%): Intercept = 2.83 (p < 0.001); Slope = –0.30 (p < 0.05); Quadratic coefficient = 0.31 (p < 0.05). Group 2 (G2; persistently elevated symptom group, n = 393; 27.8%): Intercept = 7.61 (p < 0.001); Slope = –1.20 (p > 0.10); Quadratic coefficient = 0.36 (p > 0.05). Abbreviation: EPDS, Edinburgh Postnatal Depression Scale. |
Association of Social Support with Overall and Latent Depressive Symptom Trajectories
To examine whether social support was related to depressive symptom change over time, SSRS scores were incorporated into the growth models as covariates. The overall trajectory was refitted using a latent growth curve (LGC) model (GZ). After controlling for social support, the refitted LGCM also showed acceptable fit (χ2 = 87.38, CFI = 0.98, TLI = 0.96, RMSEA = 0.045). As shown in Figure 4, the adjusted overall trajectory (GZ) was compared with the original unadjusted trajectory (G, previously presented in Figure 2). After controlling for social support, the estimated growth pattern followed a relatively stable linear pattern across the perinatal period.
 |
Figure 4 Comparison between the original overall trajectory (G) and the adjusted overall trajectory (GZ) after accounting for social support. The figure was generated using Mplus version 8.3. Model parameters (GZ): Intercept = 4.659 (p < 0.001); Slope = 0.999 (p > 0.10); Quadratic coefficient = 3.76 (p > 0.05). Abbreviation: EPDS, Edinburgh Postnatal Depression Scale. |
To further examine subgroup-specific patterns, the LCGM was refitted with SSRS scores as a covariate. As illustrated in Figure 5, the adjusted latent trajectories (G1Z and G2Z) were compared with their corresponding original trajectories (G1 and G2, previously presented in Figure 3). The shapes of the two subgroups changed as follows: G2Z (adjusted G2) — The original persistently elevated symptom trajectory group maintained its flat trajectory over time, but with slightly higher depressive symptom levels compared with the unadjusted model. G1Z (adjusted G1) — The original ascending–low symptom group shifted from a progressively increasing curvilinear trajectory to a relatively stable linear pattern, with symptom levels also elevated relative to the unadjusted model.
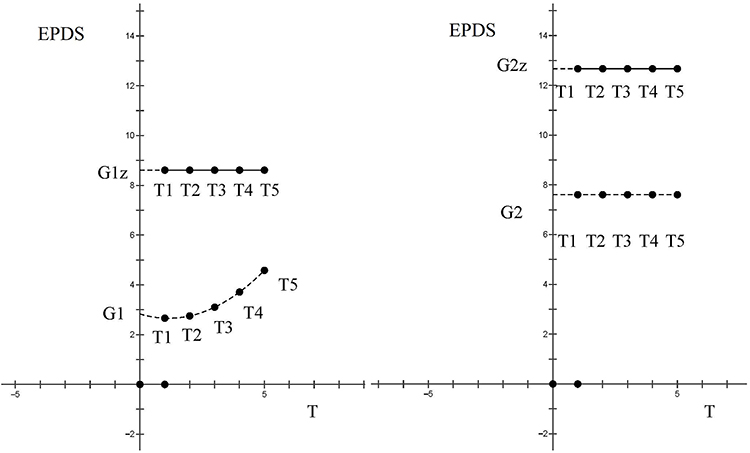 |
Figure 5 Comparison of depressive symptom trajectories after adjusting for social support (G1Z, G2Z) and the original trajectories (G1, G2). The figure was generated using Mplus version 8.3. Model parameters: G1Z: Intercept = 12.67 (p < 0.001); Slope = 0.83 (p > 0.05); Quadratic coefficient = 0.05 (p > 0.05). G2Z: Intercept = 8.61 (p < 0.001); Slope = 0.53 (p > 0.05); Quadratic coefficient = 0.12 (p > 0.05). Abbreviation: EPDS, Edinburgh Postnatal Depression Scale. |
Discussion
The Overall and Latent Trajectories of Perinatal Depressive Symptoms
This study showed that depressive symptoms increased from mid-pregnancy to three months postpartum, while also exhibiting meaningful heterogeneity across individuals. Using latent class growth modeling, we identified two distinct patterns: the ascending–low symptom group, comprising over 70% of participants, demonstrated a gradual increase in symptoms but remained at relatively low levels overall, whereas the persistently elevated symptom group (fewer than 30%) maintained higher symptom levels with minimal change over time. These findings are broadly consistent with most previous studies, although some differences were noted. Research from Europe and North America has indicated that while the severity of perinatal depressive symptoms varies among women, the dynamic changes over time are generally minor.10–13 By contrast, studies conducted in less developed regions have reported more pronounced fluctuations. For instance, Badiya44 in India and Choi34 in Korea identified not only persistently low and persistently high trajectories but also ascending and descending patterns. Similarly, Yu45 in Hubei, China, identified additional subgroups that differentiated between antenatal and postpartum depression. Such variation may reflect differences in sample size and the timing and density of assessments, as well as contextual influences related to ethnicity, socioeconomic conditions, and cultural practices. In the present study, two assessment windows—late pregnancy and six weeks postpartum—captured major physiological and psychosocial transitions surrounding childbirth, which may improve sensitivity to symptom fluctuation during this period. More broadly, the observed symptom patterns are likely shaped by multiple intersecting factors operating across biological, psychological, and sociocultural levels during the perinatal transition.
The Dynamic Influence of Social Support on Perinatal Depressive Trajectories
Social support was associated with patterns of change in perinatal depressive symptoms across pregnancy and postpartum. Higher levels of support corresponded to a less pronounced increase in symptoms over time, and this association appeared stronger during pregnancy than in the postpartum period. To the best of our knowledge, this is the first study to investigate the influence of social support as a dynamic, time-varying factor on perinatal depressive trajectories. Unlike previous studies that evaluated social support at a single time point or applied non-standardized classifications, this study employed a standardized scale and modeled social support as a continuous construct measured repeatedly over time, enabling an evaluation of how support related to changes in symptoms across the perinatal period. Our findings indicated that social support was associated with both the overall symptom trajectory and subgroup-specific patterns. After accounting for social support, the overall trajectory changed from a progressively increasing curve to a more stable linear pattern. Within latent subgroups, symptom levels in the persistently elevated symptom group increased slightly, whereas the ascending–low symptom group shifted from a progressively increasing curvilinear pattern to a relatively stable linear trajectory, albeit, at a higher overall level. Taken together, these results suggest that social support was an important correlate of perinatal depressive symptoms over time and was associated with less symptom worsening, although its buffering association appeared relatively stronger during pregnancy and less pronounced postpartum. Notably, the association between support and symptom course was most apparent among women with initially lower symptom levels, in whom higher support coincided with a flatter trajectory and less escalation over time. This is consistent with the theoretical perspectives of Fuhr38 and Matsumura,39 who suggested the association between social support and symptom course may be stronger among women with lower symptom levels in late pregnancy.
Multilevel Mechanisms Linking Social Support and Perinatal Depressive Symptoms in China
Our findings indicate that perinatal depressive symptoms followed both overall and heterogeneous trajectories, and that higher social support was associated with a buffering effect against symptom worsening—particularly among women with initially lower symptom levels—while this buffering association appeared less pronounced postpartum than during pregnancy.
From a biological perspective, the transition to postpartum involves abrupt hormonal withdrawal,46 sleep disruption,2 intensive caregiving demands, and persistent physical discomfort. For some women, these stressors may be compounded by pregnancy complications (eg, hypertensive disorders of pregnancy and gestational diabetes) and postpartum conditions (eg, pain and anemia) that delay recovery Although such challenges are universal, their psychological salience may be amplified in contexts where postpartum recovery receives comparatively less structured clinical attention. In urban Chinese settings, the contrast between highly structured antenatal monitoring and comparatively procedural postpartum follow-up may be particularly pronounced. In addition, the traditional practice of zuoyuezi remains common, even in major cities. When implemented rigidly—such as restricting bathing, limiting mobility, promoting high-fat diets, or constraining environmental comfort—confinement may intensify discomfort and prolong recovery, potentially increasing susceptibility to postpartum complications (eg, puerperal infection, subinvolution of the uterus, and venous thromboembolism)47,48 Thus, cultural practices intended to facilitate recovery may, under certain conditions, inadvertently contribute to increased vulnerability during the postpartum transition.
Psychologically, the postpartum period often entails a rapid shift in role expectations and social attention. As the infant becomes the primary focus, mothers’ exhaustion, emotional needs, and physical recovery may receive comparatively less explicit attention. Within most Chinese households, postpartum support is primarily provided by older-generation female relatives and tends to be practical and directive, while spousal support may at times be limited or not fully aligned with mothers’ emotional needs. Although such assistance may increase the measurable level of support, it may not consistently address emotional needs and may be experienced as controlling when accompanied by strong prescriptions regarding feeding or caregiving practices. In this context, the structure of support may prioritize functionality over emotional attunement. Under these conditions, the perceived quality of support—its emotional responsiveness and respect for maternal autonomy—may become more salient than its quantity. When autonomy is constrained, support may function less as a buffer and more as an additional interpersonal demand. This distinction between the availability of support and its perceived usability may be particularly relevant within family-centered support systems.
At the social and structural level, support networks in China are often highly family-centered and relatively less flexible. In addition, traditional social expectations surrounding the ideal of a “competent” mother may contribute to heightened self-doubt and interpersonal tension. When family relationships are strained or expectations conflict, alternative sources of support may be limited. Beyond the immediate family, support systems may be relatively less diversified. Access to evidence-based parenting resources and standardized postpartum services remains uneven, and regulatory oversight of confinement care services varies. At the same time, many women face pressure to balance early motherhood with return-to-work expectations. Although maternity protections exist, their implementation may differ across settings, and perceived career penalties may persist beyond the early postpartum months. These structural conditions may sustain stress during a period of heightened vulnerability.
Finally, stigma may further reduce the usability of support.38 Pregnancy and childbirth are often framed as inherently joyful, discouraging disclosure of distress. Stigma surrounding mental health and emotional distress can distort public understanding of perinatal depression, with women labeled as “weak” or “unfit”, which may heighten shame, suppress emotional expression, and delay help-seeking.38,49 Even when support is structurally “present”, stigma and limited low-threshold, nonjudgmental pathways can make it effectively inaccessible. Consistent with this, inadequate support may both exacerbate symptoms and create barriers to help-seeking.50,51
Taken together, intensified physical strain, shifting psychological needs, a family-centered support system that is often practical yet not consistently emotionally attuned—alongside stigma and structural gaps in accessible care—may help explain why symptoms rise after childbirth and why the buffering role of social support appears stronger during pregnancy than postpartum in this cohort. These contextual features may help explain why social support showed a weaker buffering association postpartum than during pregnancy in this Chinese cohort. By contrast, among women in the persistently elevated symptom group, the buffering association of social support appeared less evident, possibly reflecting the more entrenched nature of depressive symptoms in this subgroup, which may be less responsive to contextual influences alone.
Clinical and Public Health Implications
The present findings and contextual interpretation suggest that strengthening social support across the perinatal period may represent an important target for mitigating the progression of depressive symptoms. Practical efforts should address both women’s physical recovery and psychological adjustment, as these domains may jointly influence vulnerability to symptom worsening during pregnancy and after childbirth. At the clinical level, alongside standardized antenatal care, obstetric and community healthcare services may incorporate routine assessment of psychosocial well-being and provide timely support beginning in pregnancy and continuing postpartum. Culturally tailored education—such as promoting more evidence-based zuoyuezi practices—may help improve physical recovery and emotional well-being. In addition, integrating feasible mental health screening and referral pathways into routine perinatal care across multiple time points may facilitate earlier identification of women experiencing elevated depressive symptoms and improve access to appropriate support. At the community level, accessible education addressing perinatal emotional well-being, postpartum recovery, and infant care may help families better understand women’s needs throughout the perinatal period. Programs delivered through antenatal education, primary care, and community platforms may promote supportive responses that combine practical assistance with emotional understanding. Such efforts may help reduce interpersonal stress and strengthen coping resources. Reducing stigma also remains essential. Public education that normalizes emotional distress during pregnancy and postpartum may encourage help-seeking and improve the usability of available support. Low-threshold support options, such as confidential counseling services or digital platforms, may further improve access to timely care. At the service level, efforts to improve the quality and continuity of perinatal care services may further support maternal recovery and psychological adjustment. Collectively, these clinical and community-based strategies may contribute to a more supportive perinatal environment and improved maternal mental health outcomes.
Limitations and Future Directions
This study has several limitations. First, it was conducted at a single centre in Beijing, where participants had relatively homogeneous socioeconomic backgrounds, which may limit the generalisability of the findings to other regions or populations. Second, data from the first trimester were unavailable because participants were enrolled at 15–16 weeks of gestation. Future multicentre studies with larger and more diverse samples, beginning in early pregnancy and including repeated assessments, are warranted to capture symptom fluctuations more comprehensively. Third, although this study examined the association between social support and depressive symptom trajectories, it did not further explore the determinants or risk profiles underlying differences between the identified latent trajectory groups. Future research should investigate these intergroup variations to better understand their underlying mechanisms and clinical implications.
Conclusion
From 15 weeks of gestation to three months postpartum, perinatal depressive symptoms showed an overall increasing trend. However, substantial heterogeneity was observed: approximately 70% of women followed an ascending–low symptom trajectory, whereas about 30% exhibited persistently elevated symptoms with minimal change over time. Higher social support was associated with less worsening of depressive symptoms over the perinatal period, and this association appeared stronger during pregnancy than postpartum, particularly among women with lower initial symptom levels. These findings suggest that strengthening social support across the perinatal period may contribute to mitigating symptom worsening and promoting improved maternal mental health.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation as well as with the Helsinki Declaration of 1975, as revised in 2008. This study was approved by the ethical institutional review board of Beijing Obstetrics and Gynecology Hospital (2019-KY-095-02).
Acknowledgments
We dedicate our appreciation to all study participants. Additionally, we owe gratitude to our colleagues from the Department of Perinatal Medicine, Beijing Obstetrics and Gynecology Hospital, Capital Medical University for lending assistance with respect to the recruitment, follow-up, and data collection processes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Beijing Obstetrics and Gynecology Hospital, Capital Medical University (Grant No.FCYYGL201902). The funding organization played no role in the study design, data collection, data analysis, data interpretation, or writing of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Power J, Watson S, Chen W, Lewis A, van Ijzendoorn M, Galbally M. The trajectory of maternal perinatal depressive symptoms predicts executive function in early childhood. Psychol Med. 2023;53(16):7953–15. doi:10.1017/S0033291723002118
2. Wang C, Hou J, Li A, Kong W. Trajectory of perinatal depressive symptoms from the second trimester to three months postpartum and its association with sleep quality. Int J Womens Health. 2023;15:711–723. doi:10.2147/IJWH.S408347
3. Carter EA, Bond MJ, Wickham RE, Barrera AZ. Perinatal depression among a global sample of Spanish-speaking women: a sequential-process latent growth-curve analysis. J Affect Disord. 2019;243:145–152. doi:10.1016/j.jad.2018.09.006
4. Grekin R, Brock RL, O’Hara MW. The effects of trauma on perinatal depression: examining trajectories of depression from pregnancy through 24 months postpartum in an at-risk population. J Affect Disord. 2017;218:269–276. doi:10.1016/j.jad.2017.04.051
5. Vanwetswinkel F, Bruffaerts R, Arif U, Hompes T. The longitudinal course of depressive symptoms during the perinatal period: a systematic review. J Affect Disord. 2022;315:213–223. doi:10.1016/j.jad.2022.06.087
6. Baron E, Bass J, Murray SM, Schneider M, Lund C. A systematic review of growth curve mixture modelling literature investigating trajectories of perinatal depressive symptoms and associated risk factors. J Affect Disord. 2017;223:194–208. doi:10.1016/j.jad.2017.07.046
7. Santos H Jr, Tan X, Salomon R. Heterogeneity in perinatal depression: how far have we come? A systematic review. Arch Womens Ment Health. 2017;20(1):11–23. doi:10.1007/s00737-016-0691-8
8. Ji QQ, Wang MY. Epidemiology, pathophysiology, and interventions for postpartum depression: systematic review. World J Clin Cases. 2025;13(29):110948. doi:10.12998/wjcc.v13.i29.110948
9. Zarroug M, Altaf MF, Shaikh S, et al. The prevalence and risk factors of postpartum depression among Saudi Arabian women: a systematic review and meta-analysis. Healthcare. 2025;13(16):2040. doi:10.3390/healthcare13162040
10. Wikman A, Axfors C, Iliadis SI, Cox J, Fransson E, Skalkidou A. Characteristics of women with different perinatal depression trajectories. J Neurosci Res. 2020;98(7):1268–1282. doi:10.1002/jnr.24390
11. Khanlari S, Eastwood J, Barnett B, Naz S, Ogbo FA. Psychosocial and obstetric determinants of women signalling distress during Edinburgh Postnatal Depression Scale (EPDS) screening in Sydney, Australia. BMC Pregnancy Childbirth. 2019;19(1):407. doi:10.1186/s12884-019-2565-3
12. Kovacheva K, de la Fe Rodriguez-Munoz M, Gomez-Baya D, Dominguez-Salas S, Motrico E. Relationship between social support and perinatal depression during the COVID-19 pandemic. J Reprod Infant Psychol. 2025;43(1):167–180. doi:10.1080/02646838.2023.2230585
13. Li J, Imam SZ, Jing Z, Wang Y, Zhou C. Suicide attempt and its associated factors among women who were pregnant as adolescents in Bangladesh: a cross-sectional study. Reprod Health. 2021;18(1):71. doi:10.1186/s12978-021-01127-6
14. Marsland S, Treyvaud K, Pepping CA. Prevalence and risk factors associated with perinatal depression in sexual minority women. Clin Psychol Psychother. 2022;29(2):611–621. doi:10.1002/cpp.2653
15. Bhushan NL, Stockton MA, Harrington BJ, et al. Probable perinatal depression and social support among women enrolled in Malawi’s Option B+ Program: a longitudinal analysis. J Affect Disord. 2022;306:200–207. doi:10.1016/j.jad.2022.03.017
16. Stevenson K, Fellmeth G, Edwards S, et al. The global burden of perinatal common mental health disorders and substance use among migrant women: a systematic review and meta-analysis. Lancet Public Health. 2023;8(3):e203–e216. doi:10.1016/S2468-2667(22)00342-5
17. Mohammad KI, Sabbah H, Aldalaykeh M, et al. Effects of social support, parenting stress and self-efficacy on postpartum depression among adolescent mothers in Jordan. J Clin Nurs. 2021;30(23–24):3456–3465. doi:10.1111/jocn.15846
18. Orsolini L, Pompili S, Mauro A, Salvi V, Volpe U. Fear and anxiety related to COVID-19 pandemic may predispose to perinatal depression in Italy. Front Psychiatry. 2022;13:977681. doi:10.3389/fpsyt.2022.977681
19. Alfayumi-Zeadna S, Bina R, Levy D, Merzbach R, Zeadna A. Elevated perinatal depression during the COVID-19 pandemic: a national study among Jewish and Arab women in Israel. J Clin Med. 2022;11(2):349. doi:10.3390/jcm11020349
20. Żyrek J, Klimek M, Apanasewicz A, et al. Social support during pregnancy and the risk of postpartum depression in Polish women: a prospective study. Sci Rep. 2024;14(1):6906. doi:10.1038/s41598-024-57477-1
21. Steward CE, Claridge AM, Beeson T, Feeney SL. Persistent postpartum depression during the COVID-19 pandemic and the role of social supports. J Community Psychol. 2025;53(4):e70018. doi:10.1002/jcop.70018
22. Keles E, Bilge Y, Kumru P, Celik Z, Cokeliler I. Association between perceived social support, marital satisfaction, differentiation of self and perinatal depression. North Clin Istanb. 2023;10(2):181–188. doi:10.14744/nci.2023.79923
23. Bedaso A, Adams J, Peng W, Sibbritt D. The relationship between social support and mental health problems during pregnancy: a systematic review and meta-analysis. Reprod Health. 2021;18(1):162. doi:10.1186/s12978-021-01209-5
24. Friedman LE, Gelaye B, Sanchez SE, Williams MA. Association of social support and antepartum depression among pregnant women. J Affect Disord. 2020;264:201–205. doi:10.1016/j.jad.2019.12.017
25. Fukuzawa RK, Park CG. Role of intrapartum social support in preventing postpartum depression. J Perinat Educ. 2023;32(2):104–115. doi:10.1891/JPE-2022-0003
26. Shoaib N, Abbasi HUB, Rizvi SA, Ali ST. Social support and multifactorial predictors of perinatal depression: insights from a hospital-based cross-sectional survey in Karachi, Pakistan. BMJ Open. 2025;15(9):e091200. doi:10.1136/bmjopen-2024-091200
27. Linde K, Treml J, Lehnig F, Nagl M, Stepan H, Kersting A. Maternal mental health: a longitudinal study of depression and anxiety across pregnancy and postpartum. Midwifery. 2025;149:104571. doi:10.1016/j.midw.2025.104571
28. Dutta I, Sharma D. Mothers at risk of postpartum depression and its determinants: a perspective from the urban Jharkhand, India. J Family Med Prim Care. 2025;14(7):2853–2860. doi:10.4103/jfmpc.jfmpc_303_25
29. Meng W, Shalayiding S, Wang X, Sailike B, Jiang T. Relationship between prenatal anxiety, depression, pregnancy stress and their social determinants. BMC Psychol. 2025;13(1):905. doi:10.1186/s40359-025-03237-3
30. Shahzad J, Nazim L, Hussain L, et al. Unveiling barriers to maternal mental health in Pakistan: knowledge, attitudes and stigmas toward postpartum depression in social support systems. Front Public Health. 2025;13:1527847. doi:10.3389/fpubh.2025.1527847
31. Niimura J, Yamasaki S, Nakanishi M, et al. Investigating the association between the number of interpersonal supporters during first-time pregnancy and postpartum depression symptoms. Epidemiol Psychiatr Sci. 2025;34:e34. doi:10.1017/S2045796025000241
32. Al-Abri K, Edge D, Armitage CJ. Prospective analysis of factors associated with perinatal depression. Midwifery. 2024;128:103871. doi:10.1016/j.midw.2023.103871
33. Fleischman EK, Connelly CD, Calero P. Depression and anxiety, stigma, and social support among women in the postpartum period. Nurs Womens Health. 2022;26(2):95–106. doi:10.1016/j.nwh.2022.01.008
34. Choi C, Mersky JP, Janczewski CE, Goyal D. Advancing research on perinatal depression trajectories: evidence from a longitudinal study of low-income women. J Affect Disord. 2022;301:44–51. doi:10.1016/j.jad.2022.01.026
35. Ahmed A, Feng C, Bowen A, Muhajarine N. Latent trajectory groups of perinatal depressive and anxiety symptoms from pregnancy to early postpartum and their antenatal risk factors. Arch Womens Ment Health. 2018;21(6):689–698. doi:10.1007/s00737-018-0845-y
36. Sun JW, Li JH, Zhang X, et al. Perinatal depression: data-driven subtypes derived from life history and mindfulness and personality. J Affect Disord. 2020;276:335–344. doi:10.1016/j.jad.2020.07.040
37. Gao YM, Wang J, Xu JL, et al. Relationship between perinatal depression, loneliness, and social support among puerperal women: a cross-lagged analysis. J Nurs Sci. 2020;37(7):29–32, 65.
38. Fuhr DC, Sikander S, Vanobberghen F, et al. Predictors of spontaneous remission and recovery among women with untreated perinatal depression in India and Pakistan. Glob Ment Health. 2023;10:e34. doi:10.1017/gmh.2023.26
39. Matsumura K, Hamazaki K, Tsuchida A, et al; Japan Environment and Children’s Study Group. Causal model of the association of social support during pregnancy with a perinatal and postpartum depressive state: a nationwide birth cohort. J Affect Disord. 2022;300:540–550. doi:10.1016/j.jad.2021.12.117
40. Hagaman A, LeMasters K, Zivich PN, et al. Longitudinal effects of perinatal social support on maternal depression: a marginal structural modelling approach. J Epidemiol Community Health. 2021;75(10):936–943. doi:10.1136/jech-2020-215836
41. Zheng X, Morrell J, Watts K Changes in maternal self-efficacy, postnatal depression symptoms and social support among Chinese primiparous women during the initial postpartum period: a longitudinal study. Midwifery. 2018;59:39–46.
42. Liu Y, Zhang L, Guo N, Ai Y. Advances in the application of the Edinburgh Postnatal Depression Scale for screening perinatal depression in China. Chin J Mod Nurs. 2021;27(36):5026–5031.
43. Xiao SY. Rating scales for mental health. In: Theoretical Basis and Research Application of the Social Support Rating Scale. Nanjing: Chinese Mental Health Journal Press; 1994:98–100. Chinese.
44. Badiya PK, Siddabattuni S, Dey D, et al. Identification of clinical and psychosocial characteristics associated with perinatal depression in the South Indian population. Gen Hosp Psychiatry. 2020;66:161–170. doi:10.1016/j.genhosppsych.2020.08.002
45. Yu M, Li H, Xu DR, Wu Y, Liu H, Gong W. Trajectories of perinatal depressive symptoms from early pregnancy to six weeks postpartum and their risk factors: a longitudinal study. J Affect Disord. 2020;275:149–156. doi:10.1016/j.jad.2020.07.005
46. Lin YH, Chen CM, Su HM, et al. Association between postpartum nutritional status and postpartum depression symptoms. Nutrients. 2019;11(6):1204. doi:10.3390/nu11061204
47. Yang X, Qiu M, Yang Y, Yan J, Tang K, Marano G. Maternal postnatal confinement practices and postpartum depression in Chinese populations: a systematic review. PLoS One. 2023;18(10):e0293667. doi:10.1371/journal.pone.0293667
48. Neupane M, Bartaula M, Pradhan S, et al. Postpartum depression among mothers in a maternity hospital in Kathmandu, Nepal: a mixed-method study. JNMA J Nepal Med Assoc. 2024;62(277):575–581. doi:10.31729/jnma.8746
49. Hu Y, Huang S, Xiao M, et al. Barriers and facilitators of psychological help-seeking behaviors for perinatal women with depressive symptoms: a qualitative systematic review based on the Consolidated Framework for Implementation Research. Midwifery. 2023;122:103686. doi:10.1016/j.midw.2023.103686
50. Robinson KA, Hemphill TE, Atlas RO. A quasi-experimental study: social support in group prenatal care’s impact on postpartum depression in Black and Hispanic women. Int J Environ Res Public Health. 2025;22(7):9876. doi:10.3390/ijerph22071046
51. Yang L, Nan Y, Zhou J, et al. The effectiveness of a nurse-assisted digital Thinking Healthy program for postpartum depression: a randomized controlled trial. Psychiatry Res. 2025;351:116639. doi:10.1016/j.psychres.2025.116639
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.