Back to Journals » Clinical Interventions in Aging » Volume 20
Traditional Chinese Medicine Constitution and Cognitive Frailty in Older Adults: Prediction Models and Sleep-Quality Mediation Pathway from a Multicenter Study in China
Authors Qiao M ![]() , Yang S, Ma Y, Chen C, Xu M, Gan H, Wu W
, Yang S, Ma Y, Chen C, Xu M, Gan H, Wu W ![]()
Received 1 August 2025
Accepted for publication 11 December 2025
Published 16 December 2025 Volume 2025:20 Pages 2607—2625
DOI https://doi.org/10.2147/CIA.S548401
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Mengyuan Qiao,1 Sixiang Yang,1 Yuping Ma,2 Chongli Chen,1 Manru Xu,1 Hanyue Gan,1 Wenbin Wu1
1Department of Geriatrics, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 2Department of Nephropathy Medicine, Affiliated Hospital of Panzhihua University, Panzhihua, Sichuan, People’s Republic of China
Correspondence: Wenbin Wu, Department of Geriatrics, Hospital of Chengdu University of Traditional Chinese Medicine, No. 39 Shi-er-qiao Road, Chengdu, Sichuan, 610072, People’s Republic of China, Email [email protected]
Purpose: To investigate the predictive value of Traditional Chinese Medicine Constitution (TCMC) in cognitive frailty (CF) among older adults and explore its potential influencing pathways.
Patients and Methods: From 2021 to 2023, a total of 905 older participants were recruited from three geographic regions in China: Southwest (Sichuan), East (Shanghai), and North (Beijing). A multidimensional survey (including TCMC assessment) was conducted. Prediction models were developed using nomogram and C5.0 decision tree algorithms. Internal and external validations were performed. The KHB method was applied for mediation analysis.
Results: Logistic regression identified Qi-stagnation constitution (QSC) and Qi-deficiency constitution (QDC) as important risk factors for CF (P < 0.01). Both the C5.0 decision tree model and Nomogram model based on TCMC demonstrated strong predictive performance (AUC=0.824 and 0.812, respectively). External validation indicated superior extrapolability of the C5.0 model (AUC=0.810 vs 0.772). Mediation analysis revealed that sleep quality partially mediated the association between QSC and CF (P < 0.05), with a mediation proportion of 22.7%.
Conclusion: QSC and QDC were identified as modifiable risk factors for CF. Prediction models based on TCMC demonstrated strong predictive performance and generalizability. Furthermore, QSC may worsen CF progression through its detrimental effects on sleep quality, identifying its clinical applicability as both a risk stratification factor and a prevention focus for CF.
Keywords: cognitive frailty, Traditional Chinese Medicine Constitution, prediction model, mediation effects analysis
Introduction
With the accelerated aging of the global population, the prevention and management of age-related syndromes have become a public health priority. In this context, Cognitive Frailty (CF), a non-dementia syndrome characterized by the co-occurrence of physical frailty and cognitive impairment, is gaining increasing clinical significance.1 According to World Health Organization projections, the global population aged 60 and above will double by 2050, a trend that will substantially expand the at-risk population for CF, positioning it as a critical target in healthy aging strategies. A unique feature of CF is its dual nature. On one hand, research confirms its role as a precursor to dementia and functional decline; on the other hand, its potential reversibility offers a valuable window for intervention.2,3 Effective treatments for dementia remain limited. As CF represents a critical window for early intervention, current research focuses on its modifiable factors - including physical frailty components, cognitive impairment drivers, and their dynamic interactions. Targeting these factors may not only mitigate CF progression but also potentially delay or even prevent dementia onset.4
Current CF screening faces significant limitations, relying either on time-intensive clinical assessments (eg, Fried Frailty Phenotype combined with MoCA and CDR scales requiring specialized administration) or risk prediction models with constrained clinical utility. Only 31.8% of existing models have undergone external validation, risking overfitting, while many incorporate complex biomarkers (eg, SNPs, protein markers) or opaque machine learning algorithms (25% of models). While these approaches demonstrate promising theoretical efficacy (AUC 0.86–0.88), their clinical adoption in community or primary care settings remains challenging due to limited interpretability, operational complexity, and restricted generalizability (eg, being primarily validated in chronic disease subgroups).5,6 To address these gaps, we developed a dual-model system combining interpretable nomograms for individualized risk assessment in community, senior residence, and outpatient settings with optimized machine learning algorithms for efficient population screening.
The concept of Traditional Chinese Medicine Constitution (TCMC) was proposed by Wang Qi in 1994 and has been widely used in the prevention, management, and treatment of diseases.7 The theory of TCMC posits that body constitution represents inherent and relatively stable characteristics in an individual’s morphological structure and physiological functions. Contemporary TCM classifies constitutions into balanced type (healthy state) and eight imbalanced types. The relationship between TCMC and health is akin to soil and plants: balanced constitution is fertile soil, while imbalanced constitutions resemble nutrient-deficient soil. The unbalanced constitutions exhibit disease-specific correlations and can guide precision medicine approaches. Constitution-based regulation (eg, through environmental regulation, lifestyle modification, psychological adjustment, and TCM therapies) may enhance internal homeostasis, thereby conferring both disease-preventive and health-promoting effects.
However, current evidence remains insufficient to establish associations between constitutional types and CF, substantially limiting the clinical utility of constitutional theory in CF screening and intervention. Moreover, extant research has consistently demonstrated an inverse correlation between imbalanced TCMC and sleep quality.8–11 Separately, the role of sleep disturbances as precipitating factors for CF is also well-established.12–14 Nevertheless, whether constitutional deviations influence CF progression partially through sleep quality-mediated pathways remains mechanistically undefined.
Building upon the constitution as a modifiable personalized determinant, this study aims to: (1) investigate the potential of TCMC as an independent predictive factor for CF risk stratification; and (2) elucidate the underlying mechanistic pathways, with particular emphasis on evaluating the hypothesized mediating role of sleep quality.
Materials and Methods
Study Design
This multicenter observational study was conducted in three phases. First, from 2021 to 2022, we recruited 478 older adults from Sichuan Province in southwestern China. After applying exclusion criteria (>10% missing questionnaire data [n=49], severe audiovisual impairment [n=2], or Alzheimer’s disease diagnosis [n=1]), 426 eligible participants were included as the primary study cohort and stratified into cognitive frailty (CF, n=120) and non-CF (n=306) groups. Second, using this primary cohort from Sichuan, we developed predictive models for CF using both Nomogram and C5.0 boosted decision tree algorithms, with TCMC as the primary predictor. Third, we externally validated these models in independent cohorts from Beijing (Northern China, n=255; 2022–2023) and Shanghai (Eastern China, n=224; 2021–2023). Finally, we employed the KHB method to examine sleep quality as a potential mediator between TCMC and CF, thereby elucidating its predictive value and potential influencing pathways. The research flowchart is shown in Figure 1.
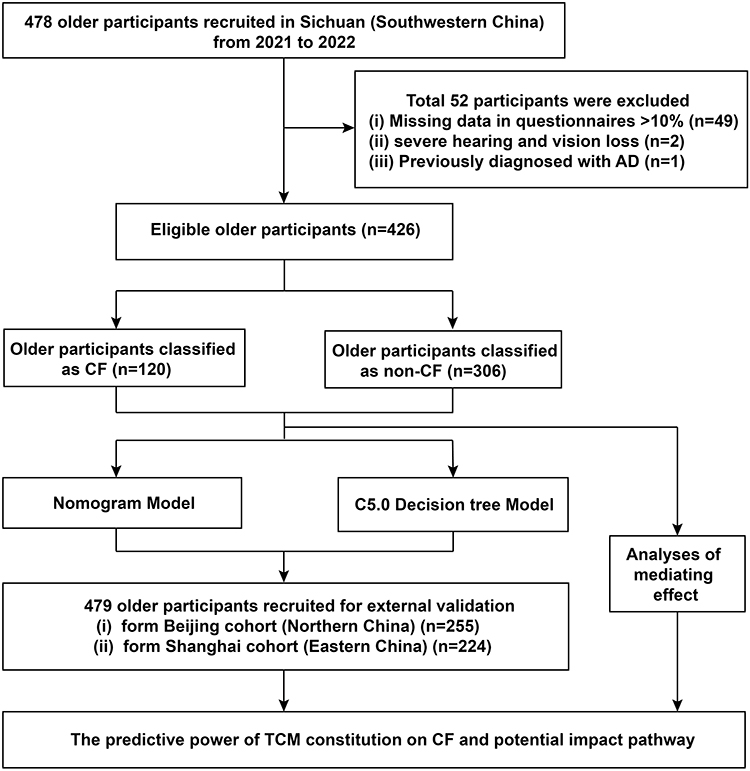 |
Figure 1 Study flowchart. |
Participants
The study enrolled participants meeting the following inclusion criteria: aged 60 years or older, capable of independent daily living and communication (Barthel Index [BI] score ≥75), willing to provide written informed consent, and able to comply with study procedures and follow-up requirements. Exclusion criteria comprised: (1) diagnosed dementia of any type; (2) severe visual or hearing impairment precluding study participation; (3) severe systemic diseases including cardiac, cerebral, renal, hepatic or other major organ dysfunction; (4) acute neurological impairment or ongoing cardiovascular events; and (5) severe neuropsychiatric disorders such as major depression or schizophrenia. These criteria ensured the selection of cognitively evaluable participants without significant multimorbidity that might confound cognitive frailty assessment.
Variables and Measurement
The data were collected by strictly trained investigators using structured questionnaires and standardized procedures.
Demographic Characteristics, Clinical Factors, and Multimorbidity
The assessed variables included: age (from birth date), sex, education, residence (1=home, 2=senior residence), living arrangement (1=alone, 2=cohabiting), social support (number of close friends providing substantial help; 1=none, 2=1-2, 3=3-5, 4=≥6), smartphone usage (1=daily, 2=no), visual impairment (vision condition including wearing classes; 1=normal, can read books; 2=mild, can watch TV; 3=moderate, blur; 4=severe, light perception or blind), hearing impairment (1=normal; 2=mild, requires slowed speech or raised volume to hear clearly; 3=moderate, mostly inaudible; 4=severe, completely inaudible), masticatory function (1=no difficulty, 2=mild, 3=moderate, 4=severe), living ability (Barthel Index, BI; Instrumental Activities of Daily Living Scale, IADL), sleep quality (Pittsburgh Sleep Quality Index, PSQI), anxiety (Generalized Anxiety Disorder-7 items Scale, GAD-7), depression (Patient Health Questionnaire-9, PHQ-9), nutritional status (Mini Nutritional Assessment Short Form, MNA-SF), and multimorbidity (≥2 chronic diseases; 1=yes, 2=no).
Physical examinations included measurements of dominant-hand grip strength, waist circumference, and body height, all obtained using calibrated instruments. Grip strength was assessed with a handgrip dynamometer; participants were instructed to exert maximal voluntary force, and the highest value from at least two trials was recorded. Measurements were recorded in kilograms (kg) for grip strength and centimeters (cm) for waist circumference and height. The waist-to-height ratio (WtHR) was calculated by dividing waist circumference by height.
Cognitive Frailty
Based on the international consensus by International Academy on Nutrition and Aging (I.A.N.A) and the International Association of Gerontology and Geriatrics (I.A.G.G), the diagnostic criteria for CF must simultaneously fulfill the following conditions: 1) Presence of physical frailty or pre-frailty screened by the FRAIL scale; 2) Presence of mild cognitive impairment by Montreal Cognitive Assessment (MoCA) Changsha version score of <22 and Clinical Dementia Rating (CDR) scale score of 0.5; 3) Exclusion of concurrent Alzheimer’s disease or other dementias. All three conditions were required for a definitive CF diagnosis.1
Traditional Chinese Medicine Constitution (TCMC)
The TCMC was assessed based on the TCM constitution scale for geriatrics.15 The scale includes 33 items, and each item is scored from 1 to 5 points. There are 9 constitutions with its corresponding items: Balanced constitution (Type A: items1, 2, 4, 5, 13), Qi-deficiency constitution (Type B, items 2, 3, 4, 14), Yang-deficiency constitution (Type C: items 11, 12, 13, 29), Yin-deficiency constitution (Type D, items 10, 21, 26, 31), Phlegm-dampness constitution (Type E: items 9, 16, 28, 32), Damp-heat constitution (Type F: items 23, 25, 27, 30), Blood-stasis constitution (Type G: items 19, 22, 24, 33), Qi-stagnation constitution (Type H: items 5, 6, 7, 8), Inherited-special constitution (Type I: items 15, 17, 18, 20). Detailed scoring criteria and classification rules for each TCMC are provided in the Supplementary Material.
Statistical Analysis
Descriptive Statistical Analysis
Statistical analyses were performed using SPSS 25.0 software, including descriptive statistics and binary logistic regression. Continuous variables with normal distribution were presented as mean ± standard deviation, while non-normally distributed data were expressed as median (interquartile range). Categorical variables were reported as counts (percentages). The significance level α was set at 0.05.
Data normality and homogeneity of variance were assessed using the Kolmogorov–Smirnov test. Between-group comparisons were conducted using t-tests for normally distributed data or the Mann–Whitney U nonparametric test for non-normally distributed data. Categorical variables were compared using Chi-square tests, with Yates’ continuity correction applied when at least one expected frequency was between 1 and 5, and Fisher’s exact test used when any expected frequency was less than 1.
Binary Logistic Regression and the Nomogram
The binary logistic regression model was developed using the Forward-Conditional method, with multinomial variables converted to dummy variables. The final model was validated through the Omnibus and Hosmer-Lemeshow tests. The validated model was subsequently transformed into a clinically applicable nomogram (Mnomo) using R software (version 2.2.2), which represents the predictive model for CF in older adults through weighted scoring of significant predictors.
Machine Learning Model Establishment
The decision tree model for CF diagnosis prediction (Mtree) was constructed using the C5.0 algorithm in SPSS Modeler 18.0 visual data mining software. CF was designated as the marker variable, with statistically significant variables from logistic regression analysis and clinically relevant input variables being incorporated into model development. The study cohort was randomly partitioned into training (70%) and testing (30%) sets using a fixed random seed to ensure reproducibility. To enhance predictive performance, we implemented a boosting ensemble algorithm combining multiple decision trees (15 iterations) for classification, with model robustness optimized through 10-fold cross-validation to address data partitioning challenges in limited sample sizes. The algorithm incorporated expert configuration with three key safeguards: (1) pruning severity set at 75% with a minimum of 2 records per sub-branch, (2) global pruning to prevent overfitting, and (3) a clinical reality-informed misclassification cost matrix (false-positive cost = 1.0; false-negative cost = 2.0) to guide pruning decisions. This comprehensive approach balanced statistical rigor with clinical applicability throughout model development.
Model Evaluation and Comparison
Mnomo was evaluated using receiver operating characteristic (ROC) curves, the area under the curve (AUC), decision curve analysis (DCA), and calibration curves. Mtree was assessed with confusion matrices, ROC curves, and AUC. Ultimately, the performance of the two models was compared based on their confusion matrices, ROC curves, and AUC values.
Mediation Effect Analysis
In this part, based on prior evidence,16 we analyzed mediation pathways using the Karlson-Holm-Breen (KHB) method, which addresses scaling limitations in logistic regression when decomposing direct and indirect effects. CF served as the binary outcome variable, with Qi-stagnation constitution scores (continuous; higher values indicating stronger constitutional tendency) as the independent variable and PSQI scores (higher values reflecting poorer sleep quality) as the mediator in the hypothesized pathways. The KHB approach was specifically chosen to overcome comparability issues in nested logistic models, enabling accurate effect decomposition while accounting for the binary nature of CF.17,18 This analytical strategy builds upon established mediation frameworks while addressing the unique requirements of binary health outcomes.
Results
Preliminary Statistics and Demographic Characteristics
This study first included 426 older adults aged ≥60 years in Sichuan, excluding 49 people with >10% missing data completion, two people with severely impaired hearing and vision, and one person who had been definitively diagnosed with Alzheimer’s disease, including 155 (36.4%) males and 271 (63.6%) females, with a mean age of (76.92±7.89) years.
Results of Cognitive Frailty Analysis and Univariate Analysis
As revealed in Table 1, 28.2% of the 426 research participants (120 instances) had cognitive frailty. Comparison of intergroup factor variability between the cognitive frailty group (CF group) and the non-cognitive frailty group (NCF group) indicated that cognitive frailty was associated with age, gender, education, residence, social support, smartphone usage, and visual or hearing impairment (P < 0.01). In terms of geriatric syndromes, participants in the CF group had higher rates of ADL or IADL disability, poor sleep quality, depression, anxiety, nutritional risk, and suffering from multimorbidity than the NCF group (P < 0.05). Given the physiological differences in body measurements between men and women, we performed gender-stratified analyses, which showed that in the CF group, grip strength decreased in both males and females, but only females showed an increase in waist-to-height ratio (P < 0.01).
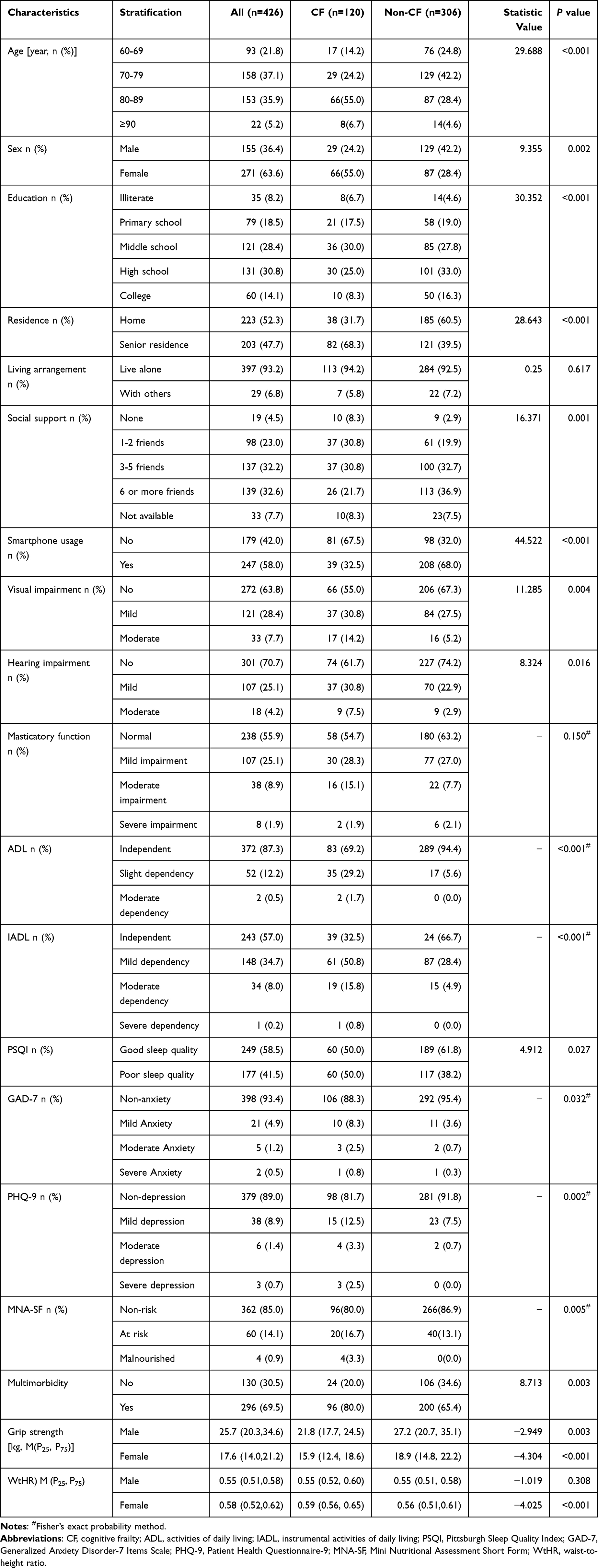 |
Table 1 Characteristics of the Sample According to the Presence of Cognitive Frailty (n = 426) |
Notably, the CF group exhibited a significantly higher proportion of imbalanced TCM constitutions compared to the NCF group (P < 0.001). This was reflected in both the lower prevalence of balanced constitution (P < 0.05) and the higher frequencies of Qi-deficiency (QDC), Yin-deficiency, phlegm-dampness, and Qi-stagnation (QSC) constitutions (all P < 0.05). These findings suggest that a balanced constitution may confer protection against CF, whereas imbalanced constitutions (eg, Qi-deficiency, Yin-deficiency, phlegm-dampness, and Qi-stagnation) may predispose individuals to CF development (Table 2).
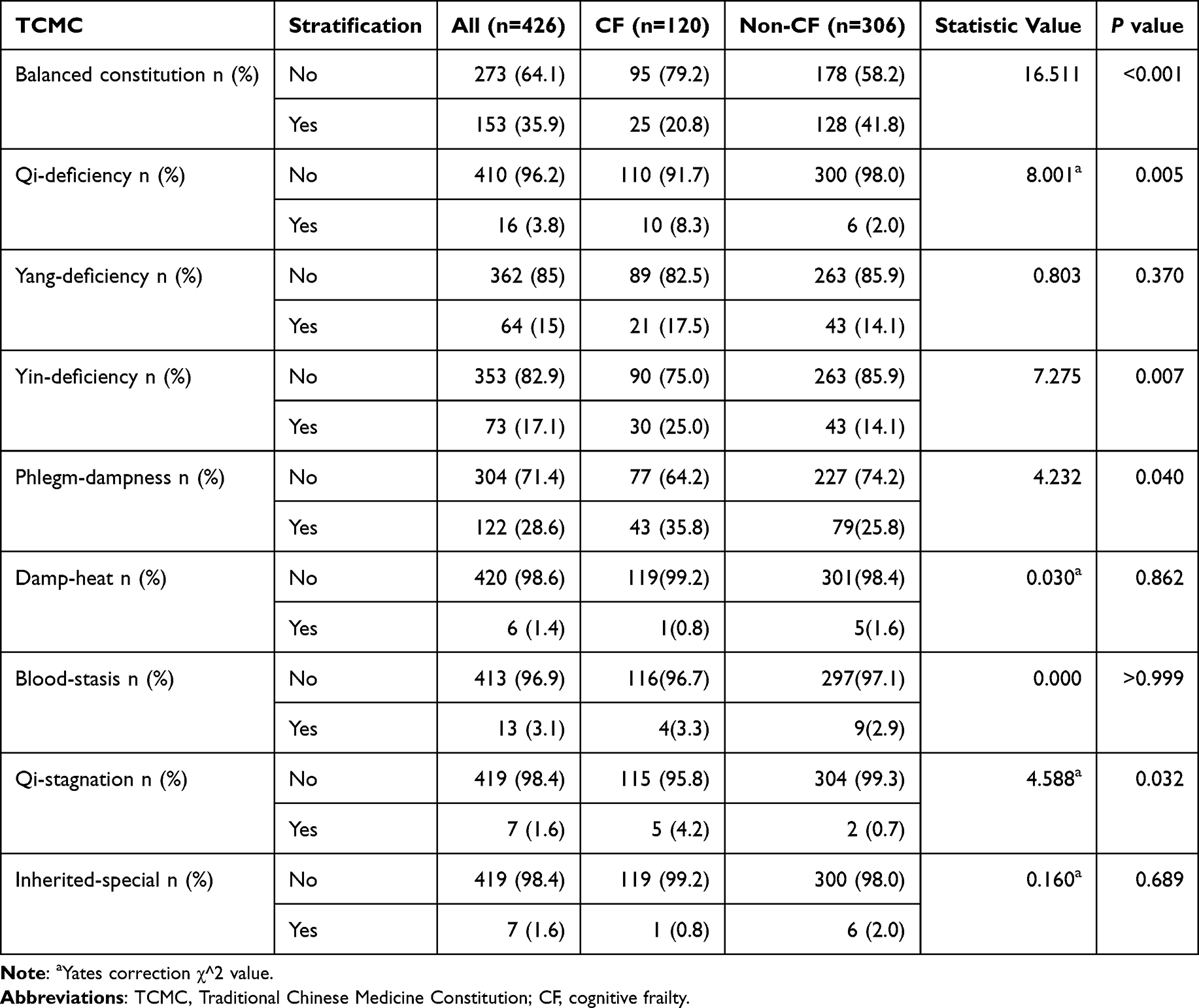 |
Table 2 TCMC of the Sample According to the Presence of Cognitive Frailty (n = 426) |
Binary Logistic Regression Analysis of Independent Risk Factors for Cognitive Frailty
The binary logistic regression analysis identified six significant independent predictors that remained in the final model after adjusting for potential confounders (Table 3 and Figure 2). The model demonstrated excellent overall performance, with a significant omnibus test (P < 0.001) and a non-significant Hosmer-Lemeshow test (P = 0.460), indicating good model fit to the data.
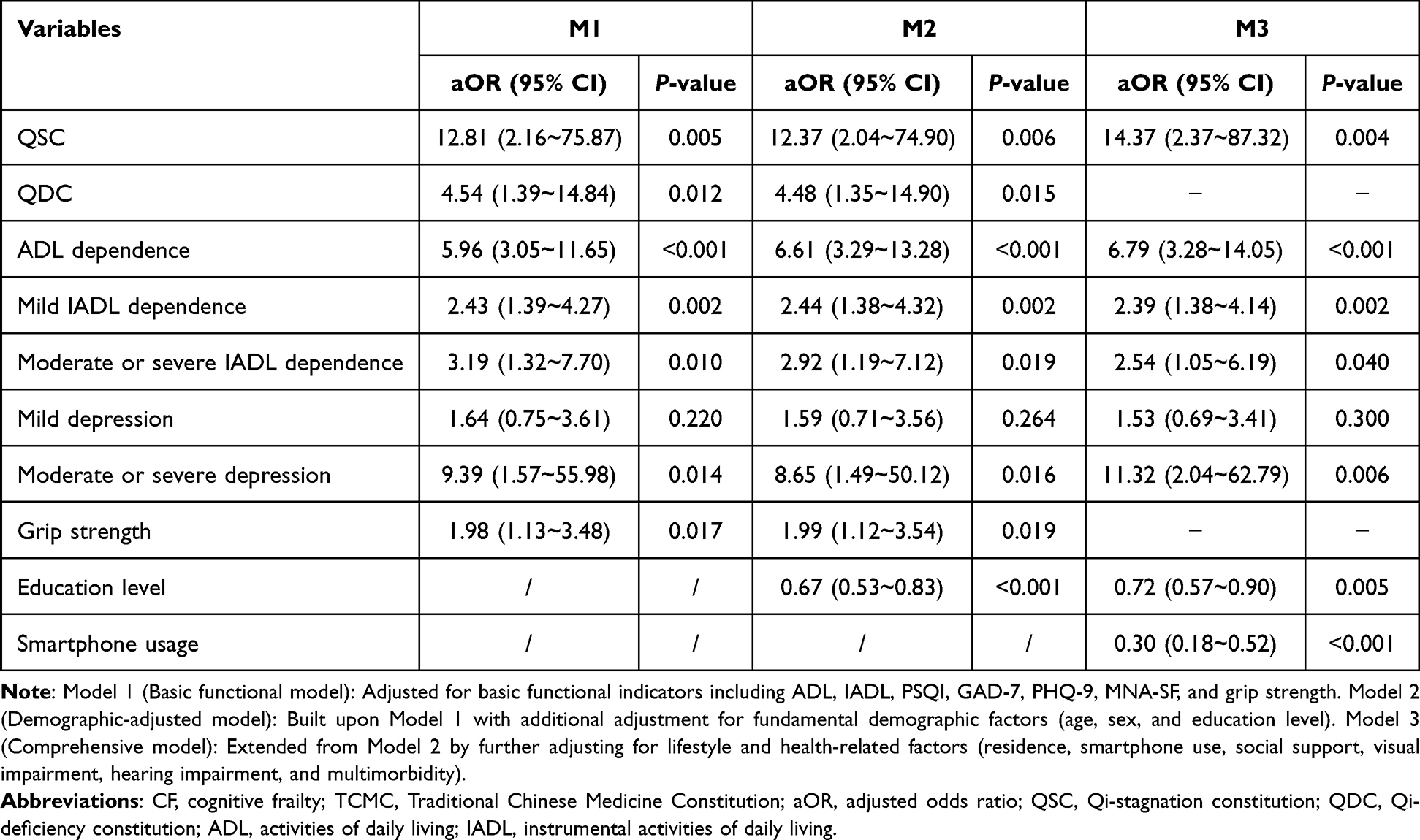 |
Table 3 Association of CF with TCMC and Other Variables (n = 426) |
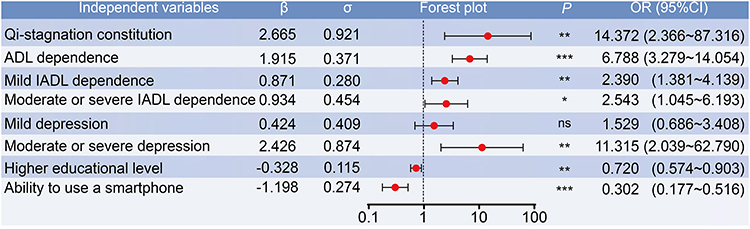 |
Figure 2 Forest plot for the logistic regression analysis showing the independent influences of cognitive frailty (CF). *P<0.05, **P<0.01, ***P<0.001. ns, not significant. |
Logistic regression identified a range of independent risk factors for CF, with QSC showing a particularly strong association (OR=14.37, 95% CI: 2.37–87.32, P=0.004). Other significant risk factors included ADL dependence, IADL dependence, and moderate or severe depression. Meanwhile, higher education level and smartphone usage were identified as independent protective factors. In addition to the above independent influences, it is noteworthy that QDC (OR=4.48, 95% CI: 1.35–14.90, P=0.015) and grip strength remained significant in the M2 after adjustments for common geriatric syndromes, grip strength, age, gender, and education level, which suggests that QDC and grip strength also have a meaningful effect on CF.
Given that senior residence may be closely associated with functional measures, we conducted a sensitivity analysis based on Model 3 (the comprehensive model) by including senior residence as a covariate while removing ADL and IADL to assess potential overadjustment. As shown in Table S1, the significant association between QSC and CF remained robust (aOR = 11, p = 0.009), indicating that the key finding from our primary models is stable and not biased by overadjustment.
Construction and Evaluation of Prediction Models for Cognitive Frailty
The Nomogram Prediction Model
In order to evaluate the predictive potential of TCMC in CF, we constructed a Nomogram graph prediction model (Mnomo) based on the results of logistic regression analysis with QDC, ADL, IADL, depression, education, and smartphone usage as predictors (Figure 3a). We also converted the graphical results of the nomogram model into a scale for easier clinical application (Table 4). The nomogram plot more visually shows the important role of QSC in the above indicators, followed by moderate or severe depression and ADL dependence.
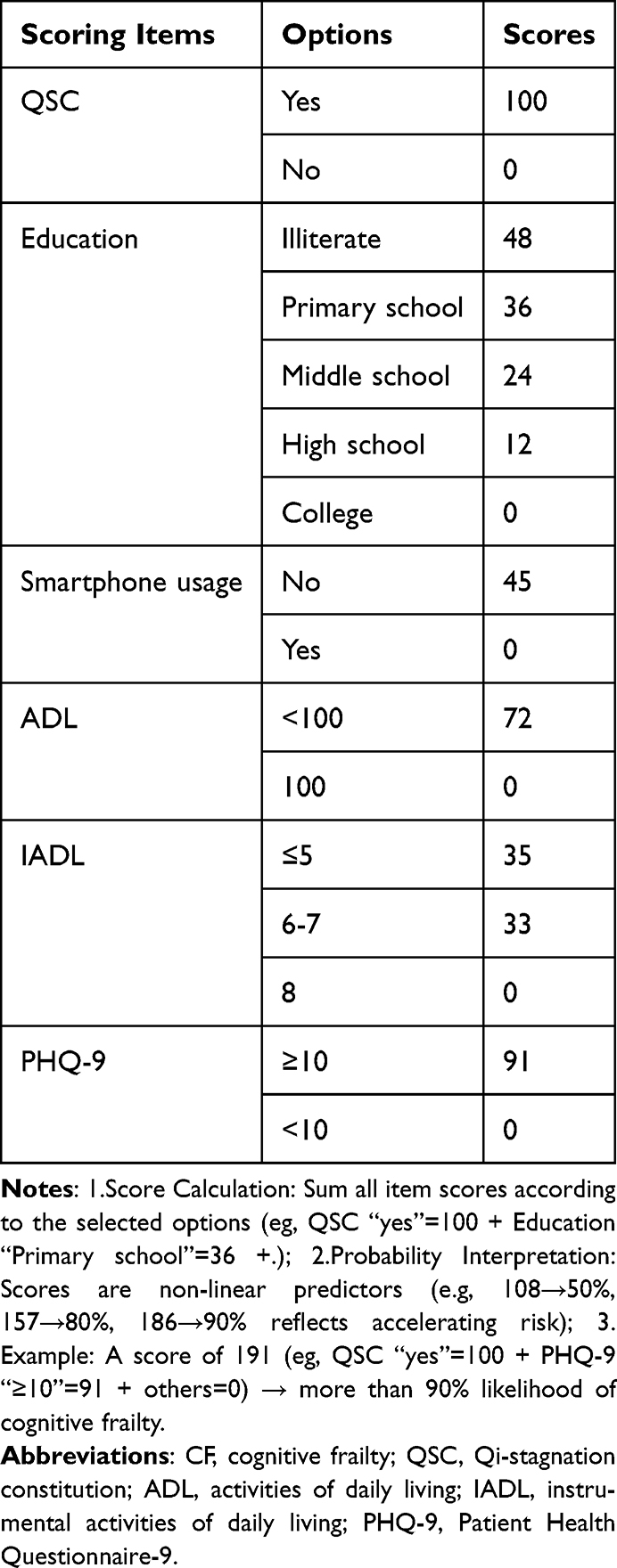 |
Table 4 A Nomogram-Based Scale for CF Prediction |
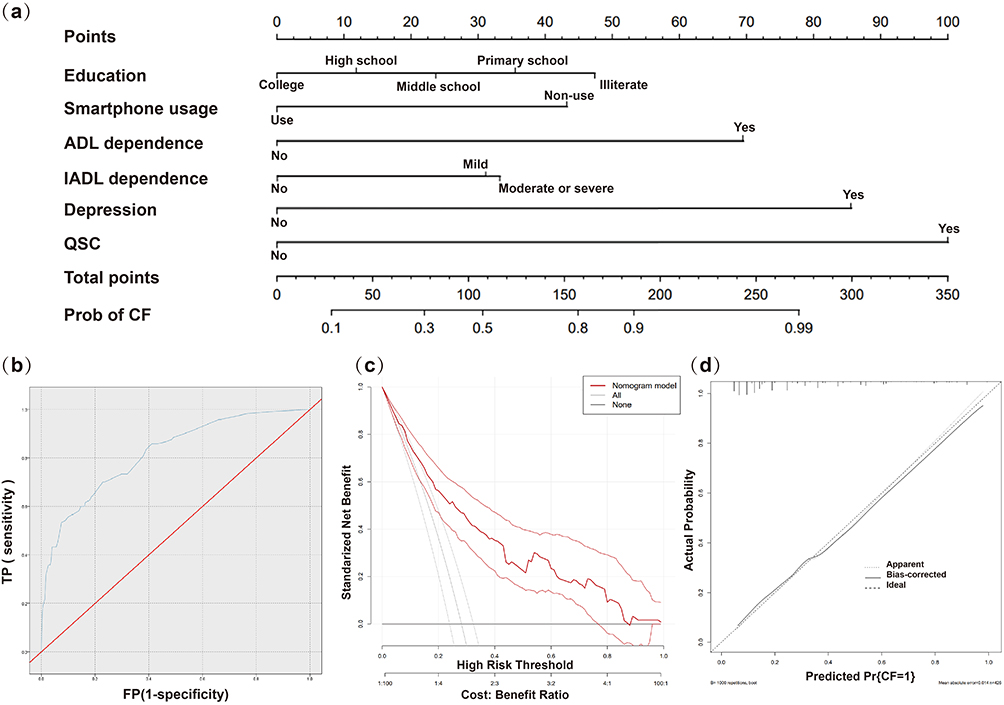 |
Figure 3 Nomogram for cognitive frailty prediction (a) and its validation through ROC curve (b), decision curve analysis (c), and calibration plot (d). |
The Mnomo was validated using receiver operating characteristic (ROC) curve analysis, decision curve analysis (DCA) curve, and calibration curve assessment. The results showed an AUC (area under curve) of 0.812 (95% CI: 0.767–0.858) for the ROC, which indicated that the Mnomo had good discrimination, and the prediction was accurate and statistically significant (P < 0.001; Figure 3b). Furthermore, the DCA curve revealed good clinical utility across a wide threshold range, showing favorable net clinical benefit (Figure 3c). The calibration curve similarly confirmed that the model was well calibrated (Figure 3d).
The C5.0 Integrated Decision Tree Model
We used the C5.0 integrated decision tree algorithm in machine learning for predictive model construction. We selected variables for modeling based on stepwise regression results, existing literature, and our clinical observations.19,20 Consequently, QDC and grip strength, both of which were significant variables in the M2 model, were included. In total, eight predictor variables were used in this section. We divided the 426 study cases from Sichuan (SC) into a train set (SCtrain) and a test set (SCtest) according to the ratio of 7:3, and the results of SCtest were used as the internal validation of the model. After iteration, a total of 15 rule sets were generated. The final protective result was judged by the algorithm synthesizing the results of these rule sets.
Finally, the C5.0 integrated decision tree model (Mtree) was evaluated by ROC and confusion matrix for comparison with Mnomo. The Mtree showed an AUC of 0.824 in the internal validation of the SCtest (Figure 4), which is slightly higher than the Mnomo (0.812). Similarly, the Mtree showed higher accuracy (ACC), sensitivity, precision, and NPV (Negative Predictive Value) than the Mnomo, and only the specificity was slightly lower than the Mnomo (Table 5). Therefore, it can be determined that the Mtree outperformed the Mnomo in terms of predictive performance.
 |
Table 5 Internal and External Validation Results for Each Model |
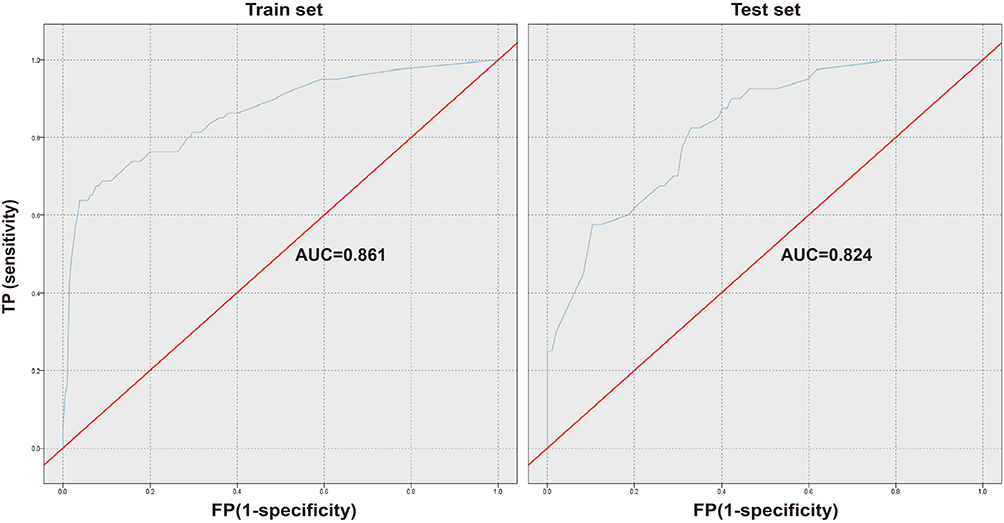 |
Figure 4 Receiver operating characteristic (ROC) curve of the C5.0 integrated decision tree model (Mtree) for cognitive frailty prediction. |
External Validation of Predictive Models of CF
Next, we collected a total of 479 older adults in the eastern (Shanghai, SH) and northern (Beijing, BJ) regions of China, as the external validation to evaluate the extrapolation performance of the two models constructed in the previous section. A comparison of the baseline situation of older adults in the three sites is shown in Table 6, which reveals differences in age, education, and smartphone usage among these seniors. AUC and a confusion matrix were used for predictive performance evaluation. The results showed that both the tree Mtree and Mnomo achieved an AUC greater than 0.7 in the two external validation sets. Among them, the Mtree achieved an AUC of 0.810 for the SH, which is the best result in the external validation sets. For the Mtree, the ACC in both validation sets were higher than 70% (75.89% in SH, 70.59% in BJ). For the Mnomo, the ACC in SH is also higher than 70%, while that in BJ is only 59.22%. It can be seen that both models have good extrapolation in external validation sets, while combining all the metrics, the Mtree had better extrapolation performance (Table 5 and Figure 5).
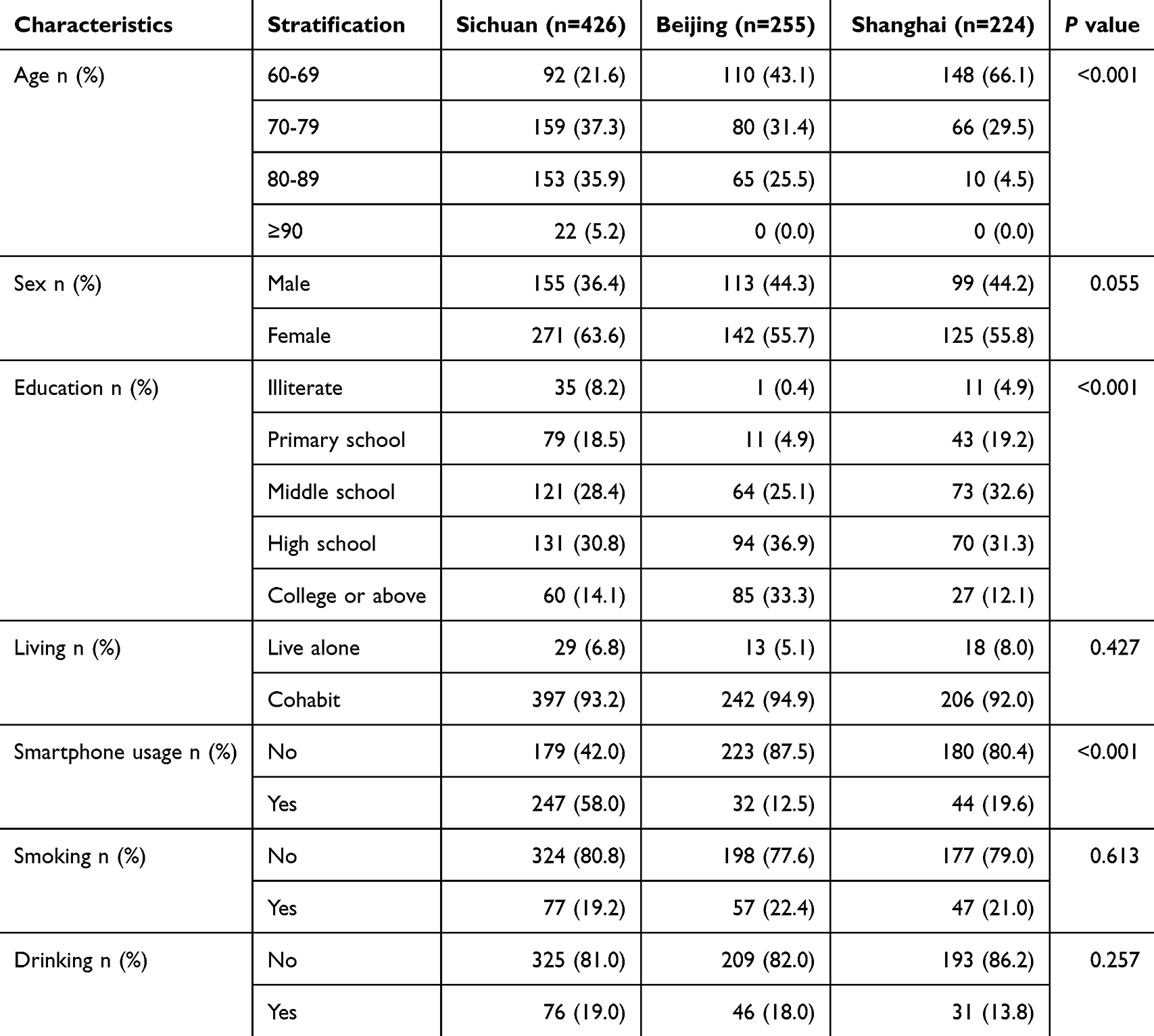 |
Table 6 Baseline Comparison of Internal and External Validation Among Different Areas |
 |
Figure 5 Comparison of ROC curves for internal and external validation of nomogram (Mnomo) and decision tree (Mtree) models. |
Analysis of the Mediating Effects Between TCMC and CF
Based on the regression results and TCMC theory, we constructed a mediated effects model using the KHB method with QSC (score) as the independent variable, sleep quality (PSQI score) as the mediator variable, and CF (binary variable as yes or no) as the dependent variable. The results showed that the total effect of QSC on CF was 0.163 (95% CI: 0.065–0.261, P=0.001), and the direct effect was 0.125 (95% CI: 0.026–0.225, P=0.013). And the mediating effect of sleep quality between QSC and CF was 0.037 (95% CI: 0.010–0.065, P=0.008<0.01). The mediation effect ratio for sleep quality was 22.7% (0.037/0.163), suggesting that QSC may contribute to the development of CF by reducing sleep quality in older adults (Figure 6).
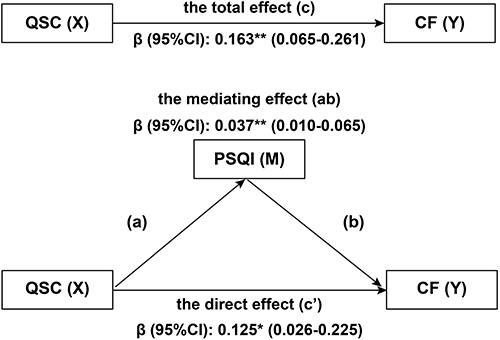 |
Figure 6 Mediation effect of sleep quality on the association between Qi-stagnation constitution (QSC) and cognitive frailty (CF). The mediating effect (ab) was significant (ab = 0.037, 95% CI [0.010, 0.065]), accounting for 22.7% of the total effect. The direct (c’ = 0.125) and total (c = 0.163) effects were also significant, consistent with partial mediation. *P < 0.05, **P < 0.01. Abbreviation: CI, confidence interval. |
Discussion
With the accelerating global aging process, CF has emerged as a major challenge in older adult health management. This was a multicenter study that elaborated the epidemiological evidence relationship between TCMC and CF at the level of influential factors, predictive value, and impact pathway. This study employed dual validation through both nomogram and machine learning-based clinical prediction models, first revealing that QSC serves as a robust predictor of CF, with cross-regional applicability confirmed by external validation. Our findings demonstrated that sleep quality mediates 22.7% of the effect pathway, indicating that QSC not only directly impacts CF but also indirectly influences CF occurrence through the mediating effect of sleep quality. These results provide clinically actionable early prevention perspectives and tools for CF screening and intervention.
Our results support QSC as an independent risk factor for CF, aligning with TCM theory that constitution represents the soil of disease onset. It has been demonstrated by preceding studies that TCMC plays a pivotal role in the genesis and progression of chronic diseases from a variety of vantage points. In the context of disease associations, significant correlations were identified between Yin-deficient constitution and sarcopenia, Yang-deficient/phlegm-dampness/blood-stasis constitution and mild cognitive impairment, and phlegm-dampness constitution and metabolism-related fatty liver.21–23 In terms of predictive value, similar to our results, QSC not only predicted cognitive decline and physical frailty in older adults, but was also strongly associated with migraine, depression, psychological disorders mediated by childhood trauma.24–29 Intervention studies have further demonstrated that TCMC modification (eg, improving damp-heat constitution) may improve health outcomes through mechanisms such as regulating intestinal flora.30 The present study revealed the important roles of TCMC and QDC in CF, which not only supports the theory of TCMC as the basis of disease susceptibility, but also provides new ideas for early intervention in CF. Further exploration is warranted into the clinical application value of TCMC in cognitive health management in forthcoming studies.
This study developed two different predictive models for CF: the first model (Mnomo) incorporated six key predictors (QSC, depression, ADL/IADL dependency, education level, and smartphone usage), while the ML model (Mtree) additionally combined QDC and grip strength as significant contributing factors. The models constructed in this study demonstrate methodological rigor and practical advantages. In contrast to the models reviewed by Ren et al, where only 18.1% underwent external validation, our approach employed a rigorous validation process based on a multicenter sample (external validation n = 479).6
Mtree exhibited robust performance in the Shanghai validation cohort (AUC = 0.810), approaching the mean AUC of externally validated models reported (pooled AUC = 0.841).6 Critically, both models achieved AUCs exceeding the clinical utility threshold (AUC > 0.70) in external cohorts from both geographical regions.31 This multi-center, multi-region validation strategy effectively addresses the prevalent issue of limited generalizability in previous research.32
Technically, this study innovatively established a dual-model system adaptable to diverse application scenarios, where Mtree is ideal for high-throughput screening scenarios, whereas Mnomo is optimized for rapid assessment in routine clinical or institutional settings. This “precision screening and rapid assessment” architecture offers a promising solution to the research-practice gap highlighted by Ren, providing customizable solutions for settings with varying resources. In addition, whereas previous studies primarily focused on community-dwelling older adults or specific clinical populations (like individuals with renal disease or hypertension), incorporating high-risk institutionalized older adults into our predictive model ensures greater applicability.
While existing research predominantly relies on nomograms with only limited adoption of machine learning (ML) models, our findings corroborate the superior performance of ML approaches over traditional models. The Mtree model demonstrated enhanced adaptability to regional heterogeneity, leveraging ML algorithms to effectively capture complex data patterns intrinsic to diverse populations. In contrast, Mnomo provides efficient assessment comparable to community screening tools through minimal routine indicators, but innovatively integrates TCMC.
Furthermore, our study identified QSC, QDC, and smartphone usage behavior as important key predictors of risk stratification for CF. This not only confirms Bai’s assertion about the value of nontraditional factors, but also does not rely exclusively on basic demographics and other burdensome comprehensive assessments of aging.33 Our findings support Rivan’s claims for multidimensional interventions and establish an assessment paradigm that is responsive to the digital health needs of aging populations.34
This study further explored the mechanism by which QSC influences the occurrence of CF through sleep quality. People with QSC are not only at high risk of CF, but they may also have poorer sleep quality and be more likely to experience it. QSC is a TCMC state characterized by introversion, emotional instability, depression, vulnerability, sensitivity, and suspicion due to long-term emotional distress and stagnation of Qi. Common manifestations of QSC include: a melancholic outlook, boredom and unhappiness, fullness and pain in the chest and hypochondrium, frequent sighing and hiccups, or a foreign body sensation between the pharynx, or breast distension and pain, poor sleep, and loss of appetite. Previous studies have shown that QSC is the main TCMC constitution for physical frailty, as well as an important risk factor for mild cognitive impairment (MCI).35,36 Clinical and basic research has revealed that QSC patients exhibit reduced cerebral oxygen metabolism and that QSC-induced cellular peroxidation and free radical accumulation can impair learning and memory functions.37,38 Furthermore, TCM formulas have been shown to improve cognitive scores by addressing these pathologies.39 Moreover, chronic stress-induced persistent activation of the hypothalamic-pituitary-adrenal (HPA) axis, exacerbated systemic inflammation, neurotransmitter imbalances, and concomitant adverse lifestyle factors (eg, sedentary behavior and social isolation) may collectively contribute to the progression of CF through both direct and indirect pathways.40–45
Our study demonstrated a negative correlation between QSC and sleep quality, with QSC individuals exhibiting poorer sleep quality - a finding consistent with both QSC characteristics and prior research.8–11 Furthermore, we found sleep quality to be significantly associated with CF, corroborating existing evidence.12–14 Sleep quality, primarily determined by subjective perception (including sleep duration and satisfaction), was assessed using the PSQI, evaluating seven components: subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, hypnotic medication use, and daytime dysfunction.46 Existing evidence suggests two potential biological pathways linking impaired sleep quality to CF: (1) compromised insulin metabolism leading to reduced cerebral glucose utilization efficiency, and (2) oxidative stress-induced neuronal damage.47–50
This study provides important tools and targets for the early identification and clinical intervention of CF. We have developed two risk prediction models: a simplified clinical assessment model for rapid screening of high-risk individuals in medical institutions, and a large-scale screening model offering efficient solutions for community-based early detection. Building upon previous research, we particularly emphasized the clinical application value of TCM constitutions as a modifiable factor in our predictive model. Compared to non-modifiable factors like age or education level, constitutions such as Qi-stagnation can be improved through TCM interventions and lifestyle adjustments, demonstrating greater clinical applicability.
The proposed targeted interventions include:
- Environmental regulation: Maintaining quiet living spaces free from excessive noise.
- Lifestyle modification: Balancing activity and rest while increasing outdoor exposure to nature.
- Psychological adjustment: Proactively participating in social and recreational activities while cultivating hobbies.
- TCM therapies: Utilizing traditional approaches including medicinal teas, herbal cuisine, foot baths, moxibustion, and acupoint massage.
We recommend that primary healthcare institutions integrate constitution assessment into routine check-ups and implement stepped management for QSC/QDC individuals: initial lifestyle and psychological interventions, supplemented by TCM external therapies for suboptimal responders, and herbal medication for refractory cases. Communities could leverage public health platforms to establish comprehensive intervention systems incorporating environment optimization, exercise guidance, social engagement promotion, and TCM healthcare. This integrated model, combining modern screening techniques with traditional regimen methods, offers a TCM-characterized solution for CF prevention and management.
This study has several notable strengths. First, we employed a comprehensive analytical approach by combining traditional regression methods with nomogram visualization and machine learning (decision tree model) for predictive model construction. The consistent demonstration of TCM constitutions’ predictive value for CF across multiple modeling approaches enhances the robustness and generalizability of our findings. Second, our multicenter design incorporated internal and external validation across northern, eastern, and southwestern China, ensuring good geographical representativeness and clinical applicability of the prediction models.
Several limitations should be acknowledged. First, the cross-sectional design restricts causal inferences between identified risk factors and CF outcomes-future prospective cohort studies are needed to verify these temporal relationships. Second, while our models showed good performance in the derivation and validation cohorts, there is still a need for further optimized model calibration using independent populations to further extend clinical utility. Third, our study has limitations in the measurement of certain variables. Specifically, the assessment of multimorbidity was based on a single self-report question rather than a validated index. While practical, this approach does not capture the severity of conditions and may have led to an underestimation of the true burden. Additionally, some potentially influential factors, like detailed socioeconomic status or dietary patterns, were not included due to data availability. Future studies should incorporate validated comorbidity index, such as the Charlson Comorbidity Index, and explore these missing variables to provide a more comprehensive understanding of the factors influencing cognitive frailty.
Despite these limitations, our study provides valuable evidence for CF prediction by innovatively integrating TCM with modern analytical approaches. The multicenter design and dual-model strategy (clinical-friendly vs population-screening) offer flexible implementation pathways for different healthcare settings.
Conclusion
This study demonstrated that QSC and QDC served as modifiable risk factors for CF. The predictive model incorporating TCMC exhibited satisfactory discriminative ability and generalizability. QSC may contribute to CF both directly and indirectly through poorer sleep quality. These findings highlight the dual utility of TCMC: (1) as a screening indicator for early CF detection, and (2) as a modifiable target for non-pharmacological interventions. The established models provided practical tools for implementing precision prevention strategies in clinical practice.
Abbreviations
ACC, accuracy; ADL, activities of daily living; AUC, area under the curve; BI, Barthel Index; BJ, Beijing; CDR, Clinical Dementia Rating scale; CF, cognitive frailty; DCA, decision curve analysis; GAD-7, Generalized Anxiety Disorder-7 items Scale; HPA, hypothalamic-pituitary-adrenal; IADL, instrumental activities of daily living; I.A.G.G., International Association of Gerontology and Geriatrics; I.A.N.A., International Academy on Nutrition and Aging; KHB, Karlson-Holm-Breen method; MCI, mild cognitive impairment; ML, machine learning; MNA-SF, Mini Nutritional Assessment Short Form; MoCA, Montreal Cognitive Assessment; NPV, negative predictive value; PHQ-9, Patient Health Questionnaire-9; PPV, positive predictive value; PSQI, Pittsburgh Sleep Quality Index; QDC, Qi-deficiency constitution; QSC, Qi-stagnation constitution; ROC, receiver operating characteristic curves; SC, Sichuan; SH, Shanghai; SNPs, single nucleotide polymorphisms; TCM, Traditional Chinese Medicine; TCMC, Traditional Chinese Medicine Constitution; TNR, true negative rate; TPR, true positive rate; WtHR, waist-to-height ratio.
Ethics Approval and Consent to Participate
The study protocol received ethical approval from the Ethics Committee of the Hospital of Chengdu University of Traditional Chinese Medicine (Approval No. 2021KL-055). Prior to study commencement, all participants provided written informed consent. The investigation was conducted in full compliance with both the ethical guidelines established by the reviewing institutional board and the principles outlined in the Declaration of Helsinki. All study procedures, including data collection and analysis, strictly adhered to institutional ethical standards for human subjects research, ensuring participant confidentiality and welfare throughout the study duration.
Acknowledgments
We sincerely appreciate the hospitals and community healthcare centers in Sichuan, Beijing, and Shanghai for their collaboration and data support. We are also grateful to all investigators for their valuable contributions to this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the National Key Research and Development Program of China (grant numbers: 2024YFC3506305 and 2020YFC2003104).
Disclosure
The authors report no conflicts of interest in this work.
References
1. K E, C M, C M, et al. Cognitive frailty: rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. J Nutr Health Aging. 2013;17(9):726–734. doi:10.1007/s12603-013-0367-2
2. Ruan Q, Yu Z, Chen M, Bao Z, Li J, He W. Cognitive frailty, a novel target for the prevention of elderly dependency. Ageing Res Rev. 2015;20:1–10. doi:10.1016/j.arr.2014.12.004
3. Ruan Q, Xiao F, Gong K, et al. Prevalence of cognitive frailty phenotypes and associated factors in a community-dwelling elderly population. J Nutr Health Aging. 2020;24(2):172–180. doi:10.1007/s12603-019-1286-7
4. Holland C, Dravecz N, Owens L, et al. Understanding exogenous factors and biological mechanisms for cognitive frailty: a multidisciplinary scoping review. Ageing Res Rev. 2024;101:102461. doi:10.1016/j.arr.2024.102461
5. Huang J, Zeng X, Hu M, et al. Prediction model for cognitive frailty in older adults: a systematic review and critical appraisal. Front Aging Neurosci. 2023;15:1119194. doi:10.3389/fnagi.2023.1119194
6. Ren M, Guo H, Guo Y, Guo W, Zhu L. The risk prediction models for cognitive frailty in the older people in China: a systematic review and meta-analysis. BMC Geriatr. 2025;25:365. doi:10.1186/s12877-025-05961-2
7. Wang Q. The present situation and prospects for the research on TCM constitution theory. J Shandong Univ Tradit Chin Med. 1994;(2):74–82.
8. Liu Z, Cao L, Wu J, et al. Association of qi-stagnation constitution and subjective sleep characteristics with mild cognitive impairment among elderly in community: a cross-sectional study. Eur J Integr Med. 2023;59:102232. doi:10.1016/j.eujim.2023.102232
9. Yang JJ, Wang Q, Jiang W. Harmonizing the mind and body: the interrelationship between traditional Chinese medicine body constitution, mental health and sleep quality. World J Psychiatry. 2025;15(3):103033. doi:10.5498/wjp.v15.i3.103033
10. Han Y, Wang Y, Shi MY, Liu Y, Cheng XD, Zhou Y. Integrating traditional Chinese medicine constitutions into insomnia management: findings from a cross-sectional study. J Integr Med. 2025;S2095–4964(25)00066–4. doi:10.1016/j.joim.2025.05.004
11. Xie B, Ma C, Chen Y, Wang J. Prevalence and risk factors of the co-occurrence of physical frailty and cognitive impairment in Chinese community-dwelling older adults. Health Soc Care Community. 2021;29(1):294–303. doi:10.1111/hsc.13092
12. Hsieh LL, Chang SF, Tsai HC. Physiological indexes, psychological resilience, sensory functions, and sleep quality on the cognitive function of older adults with pre-frailty: a predictive study. J Mens Health. 2022;18(12):12–23. doi:10.22514/jomh.2022.006
13. Griffiths J, Seesen M, Sirikul W, Siviroj P. Malnutrition, depression, poor sleep quality, and difficulty falling asleep at night are associated with a higher risk of cognitive frailty in older adults during the COVID-19 restrictions. Nutrients. 2023;15(13):2849. doi:10.3390/nu15132849
14. Ma X, Yao G, Wan X, et al. Relationship between sleep and cognitive frailty in older adults: a systematic review and meta-analysis. J Adv Nurs. 2025. doi:10.1111/jan.17081
15. Liu X. Development and Preliminary Application Analysis of the “Geriatric Version of Traditional Chinese Medicine Constitution Classification and Determination” Scale [dissertation]. Beijing: Beijing University of Traditional Chinese Medicine; 2013.
16. Cui G, Li S, Yin Y, Chen L, Liu X, Chen L. Mediating effect of abnormal TCM-based constitution on the association between sedentary behavior and cognitive frailty in elderly people. Chin Gen Pract. 2021;24(18):2297–2302.
17. Karlson KB, Holm A, Breen R. Comparing regression coefficients between same-sample nested models using logit and probit: a new method. Sociol Methodol. 2012;42(1):286–313. doi:10.1177/0081175012444861
18. Breen R, Karlson KB, Holm A. Total, direct, and indirect effects in logit and probit models. Sociol Methods Res. 2013;42(2):164–191. doi:10.1177/0049124113494572
19. Fritz NE, McCarthy CJ, Adamo DE. Handgrip strength as a means of monitoring progression of cognitive decline–a scoping review. Ageing Res Rev. 2017;35:112–123. doi:10.1016/j.arr.2017.01.004
20. Grande G, Triolo F, Nuara A, Welmer A-K, Fratiglioni L, Vetrano DL. Measuring gait speed to better identify prodromal dementia. Exp Gerontol. 2019;124:110625. doi:10.1016/j.exger.2019.05.014
21. Shen T, Wang S, Wang Z, et al. Association between the traditional Chinese medicine constitution and metabolic dysfunction-associated fatty liver disease in older people: a cross-sectional study. Heliyon. 2024;10(3):e24905. doi:10.1016/j.heliyon.2024.e24905
22. Wang C, Zhang H, Nie X, et al. Traditional Chinese medicine constitution and sarcopenia: a cross-sectional study. Front Public Health. 2024;12:1368933. doi:10.3389/fpubh.2024.1368933
23. Deng X, Teng J, Nong X, et al. Characteristics of TCM constitution and related biomarkers for mild cognitive impairment. Neuropsychiatr Dis Treat. 2021;17:1115–1124. doi:10.2147/NDT.S290692
24. Yap SY, Ng FL, Subramaniam M, Lim YM, Foo CN. Traditional Chinese medicine body constitutions as predictors for depression: a systematic review and meta-analysis. Behav Sci Basel Switz. 2022;12(11):423. doi:10.3390/bs12110423
25. Xinzhu W, Yuanchun H. Qi stagnation and qi deficiency are associated with depression in college students. Front Public Health. 2024;12:1444237. doi:10.3389/fpubh.2024.1444237
26. Sun Z, Ping P, Li Y, et al. Relationships between traditional Chinese medicine constitution and age-related cognitive decline in chinese centenarians. Front Aging Neurosci. 2022;14:870442. doi:10.3389/fnagi.2022.870442
27. Zhang Z, Chuang Y, Ke X, et al. The influence of TCM constitutions and neurocognitive function in elderly Macau individuals. Chin Med. 2021;16(1):32. doi:10.1186/s13020-021-00441-2
28. Ma X, Tang H, Zeng J, et al. Traditional Chinese medicine constitution is associated with the frailty status of older adults: a cross-sectional study in the community. Evid-Based Compl Altern Med ECAM. 2022;2022:8345563. doi:10.1155/2022/8345563
29. Duan S, Xia H, Zheng T, et al. Development and validation of non-invasive prediction models for migraine in Chinese adults. J Headache Pain. 2023;24(1):148. doi:10.1186/s10194-023-01675-1
30. Chen J, Cheng J, Li F, et al. Gut microbiome and metabolome alterations in traditional Chinese medicine damp-heat constitution following treatment with a chinese patent medicine and lifestyle intervention. Phytomedicine Int J Phytother Phytopharm. 2024;131:155787. doi:10.1016/j.phymed.2024.155787
31. Tseng SH, Liu LK, Peng LN, Wang PN, Loh CH, Chen LK. Development and validation of a tool to screen for cognitive frailty among community-dwelling elders. J Nutr Health Aging. 2019;23(9):904–909. doi:10.1007/s12603-019-1235-5
32. Navarro-Pardo E, Facal D, Campos-Magdaleno M, Pereiro A, Juncos-Rabadán O. Prevalence of cognitive frailty, do psychosocial-related factors matter? Brain Sci. 2020;10(12):968. doi:10.3390/brainsci10120968
33. Bai A, Zhao M, Zhang T, et al. Development and validation of a nomogram-assisted tool to predict potentially reversible cognitive frailty in Chinese community-living older adults. Aging Clin Exp Res. 2023;35(10):2145–2155. doi:10.1007/s40520-023-02494-9
34. Rivan NFM, Shahar S, Rajab NF, et al. Incidence and predictors of cognitive frailty among older adults: a community-based longitudinal study. Int J Environ Res Public Health. 2020;17(5):1547. doi:10.3390/ijerph17051547
35. Qin Z, Zhan X. An overview of the emotional pathogenesis of mci and the cognitive neuropsychological research ideas of MCI caused by the constitution of qi-stagnation. Mod Tradit Chin Med Mater Medica. 2024;26(9):2305–2313.
36. Gu X, Wang W, Wang X, et al. Traditional Chinese medicine constitution characteristics and relatedrisk factors of elderly patients with physicalfrailty. Geriatr Health Care. 2024;30(3):590–598.
37. Yu M. The Study of Theory and Clinic about the Relativity between Stagnation of Liver-energy and Dementia [Dissertation]. Jinan: Shandong University of Chinese Medicine; 2007.
38. Zhu Y, Shi Y, Cao C, et al. Jia-wei-kai-xin-san, an herbal medicine formula, ameliorates cognitive deficits via modulating metabolism of beta amyloid protein and neurotrophic factors in hippocampus of Aβ1-42 induced cognitive deficit mice. Front Pharmacol. 2019;10:258. doi:10.3389/fphar.2019.00258
39. Liu Z, Zhan X, Liu Y. Effects of xiaoyao pill on magnetic resonance spectroscopy of mild cognitive impairment patients with liver qi stagnation syndrome. J Tradit Chin Med. 2018;59(17):1489–1493.
40. Xie X, Wu F, Zhuang Z, Xu A. The bidirectional relationships between social isolation and cognitive function among older adults in China: separating between-person effects from within-person effects. Sci Rep. 2024;14(1):31832. doi:10.1038/s41598-024-83130-y
41. Wen X, Wang L, Hou T, Li Y. Exploring the mechanism of acupuncture in treating depression based on the neuro-endocrine-immune network. J Shaanxi Univ Chin Med. 2022;45(3):143–146.
42. Pape K, Tamouza R, Leboyer M, Zipp F. Immunoneuropsychiatry - novel perspectives on brain disorders. Nat Rev Neurol. 2019;15(6):317–328. doi:10.1038/s41582-019-0174-4
43. Sun ZW, Wang X, Zhao Y, et al. Blood-brain barrier dysfunction mediated by the EZH2-claudin-5 axis drives stress-induced TNF-α infiltration and depression-like behaviors. Brain Behav Immun. 2024;115:143–156. doi:10.1016/j.bbi.2023.10.010
44. Švob Štrac D, Pivac N, Mück-šeler D. The serotonergic system and cognitive function. Transl Neurosci. 2016;7(1):35–49. doi:10.1515/tnsci-2016-0007
45. Raichlen DA, Aslan DH, Sayre MK, et al. Sedentary behavior and incident dementia among older adults. JAMA. 2023;330(10):934–940. doi:10.1001/jama.2023.15231
46. Nelson KL, Davis JE, Corbett CF. Sleep quality: an evolutionary concept analysis. Nurs Forum. 2022;57(1):144–151. doi:10.1111/nuf.12659
47. Gulec M, Ozkol H, Selvi Y, et al. Oxidative stress in patients with primary insomnia. Prog Neuropsychopharmacol Biol Psychiatry. 2012;37(2):247–251. doi:10.1016/j.pnpbp.2012.02.011
48. Donga E, van Dijk M, van Dijk JG, et al. A single night of partial sleep deprivation induces insulin resistance in multiple metabolic pathways in healthy subjects. J Clin Endocrinol Metab. 2010;95(6):2963–2968. doi:10.1210/jc.2009-2430
49. Jennings JR, Muldoon MF, Hall M, Buysse DJ, Manuck SB. Self-reported sleep quality is associated with the metabolic syndrome. Sleep. 2007;30(2):219–223. doi:10.1093/sleep/30.2.219
50. Doyle P, Cusin I, Rohner-Jeanrenaud F, Jeanrenaud B. Four-day hyperinsulinemia in euglycemic conditions alters local cerebral glucose utilization in specific brain nuclei of freely moving rats. Brain Res. 1995;684(1):47–55. doi:10.1016/0006-8993(95)00402-C
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Machine Learning and Traditional Chinese Medicine Constitution–Based Prediction Model for Mild Cognitive Impairment in Community-Dwelling Older Adults
Xu Q, Huang Z, Su W, Cai A, Chen Z, Zhou W, Li J, Chen X
Neuropsychiatric Disease and Treatment 2026, 22:608660
Published Date: 17 June 2026