Back to Journals » International Journal of Women's Health » Volume 18
Thread-Embedding versus Manual Acupuncture for Overactive Bladder in Postmenopausal Women: Randomized Controlled Trial
Received 17 November 2025
Accepted for publication 6 March 2026
Published 19 March 2026 Volume 2026:18 582171
DOI https://doi.org/10.2147/IJWH.S582171
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Su-Ji Choi,1 Jang-Kyung Park2
1Department of Obstetrics and Gynecology, College of Korean Medicine, Dong-eui University, Busan-si, Republic of Korea; 2Department of Korean Medicine Obstetrics and Gynecology, School of Korean Medicine, Pusan National University, Yangsan-si, Republic of Korea
Correspondence: Su-Ji Choi, Department of Obstetrics and Gynecology, College of Korean Medicine, Dong-eui University, 52-57 Yangjeong-ro, Busanjin-gu, Busan, 47227, Republic of Korea, Tel +82 51 850 8660, Fax +82 505 182 6883, Email [email protected]
Objective: Overactive bladder (OAB) is a common condition in older women, characterized by urinary urgency, frequency, and nocturia. This study compared the efficacy and safety of thread-embedding acupuncture (TEA) and sham TEA in postmenopausal women with OAB.
Methods: In this multicenter, randomized, controlled trial, 68 postmenopausal women with OAB were allocated in a 1:1 ratio to receive TEA or sham TEA (manual acupuncture without thread embedding) once weekly for 8 weeks, followed by an 8-week follow up. The primary outcome was the mean daily voiding frequency over 3 days. Secondary outcomes included other bladder diary parameters, the Overactive Bladder Symptom Score (OABSS), and the King’s Health Questionnaire score.
Results: At week 8, both groups showed reductions in 24-hour micturition frequency; however, after adjustment for baseline values using ANCOVA, no significant between-group difference was observed in the primary outcome. Repeated measures analysis demonstrated no significant group-by-time interactions for secondary outcomes, although significant improvements over time were observed in both groups. At follow-up, nighttime voiding remained significantly reduced from baseline in the TEA group, whereas this reduction was not statistically significant in the sham group; however, the between-group difference did not reach statistical significance. No serious adverse events were reported.
Conclusion: TEA and manual acupuncture were effective and safe in reducing OAB symptoms in postmenopausal women, with no significant differences between interventions. Larger, long-term studies are needed to clarify specific benefits of TEA.
Plain Language Summary: Overactive bladder (OAB) is a common condition in postmenopausal women, often causing frequent urination, sudden urges, and sometimes leakage. Medicines are usually the first treatment, but they can cause side effects and are not always effective. Acupuncture is a non-drug option that may help. This study looked at a special form of acupuncture called thread-embedding acupuncture (TEA), where a small thread is left under the skin at acupuncture points to give longer-lasting stimulation.
We conducted a randomized controlled trial with 68 women who had OAB. Half received TEA, and the other half received manual acupuncture (MA), where the needles were inserted in the same way but without the thread. Both groups received weekly treatments for eight weeks and were followed for another two months.
Both TEA and MA significantly reduced urinary frequency and other OAB symptoms. On average, women in both groups urinated about two fewer times per day after treatment, and these improvements lasted for 2 months. Quality-of-life scores also improved. However, there was no meaningful difference between the TEA and MA groups, suggesting that the benefit may come mainly from acupuncture itself rather than the thread.
No serious side effects were reported, and both treatments were well tolerated.
In summary, this study suggests that acupuncture—whether with or without thread embedding—can safely improve OAB symptoms in postmenopausal women. Larger, longer studies are needed to see whether TEA has unique long-term advantages over MA.
Keywords: overactive bladder, menopause, frequent urination, quality of life, acupuncture
Introduction
Overactive bladder (OAB) is a prevalent and distressing condition characterized by urinary urgency, frequency, nocturia, and, in some cases, urgency incontinence, in the absence of other pathological causes such as urinary tract infection or structural bladder abnormalities.1 OAB particularly affects older adults, with prevalence rising from approximately 20.8% in the general population to 27.9% among those over the age of 60.2 This increase has a disproportionate impact on women, as postmenopausal hormonal changes and aging contribute to a higher incidence of bladder dysfunction, which significantly impairs quality of life.3 Among women aged 40 years and older, the prevalence of OAB increases with age, and one study reported that about 43% of women in this group experience the condition.4,5
Despite the availability of pharmacological treatments such as anticholinergics and beta-3 adrenergic agonists, long-term use is associated with adverse effects, including dry mouth, constipation, and cognitive impairment with antimuscarinics, as well as hypertension and tachycardia with beta-3 agonists.6 Moreover, many patients are reluctant to continue medical therapy because of these side effects or limited efficacy.7 Consequently, alternative therapies have gained attention, particularly in traditional medicine. Acupuncture has been applied extensively to manage OAB symptoms, including reducing urinary urgency and frequency by stimulating specific acupoints related to bladder function.8–10 Both electroacupuncture and traditional acupuncture have shown promise in alleviating OAB symptoms; however, these therapies often require frequent and prolonged treatment sessions, which may be burdensome in terms of time and cost.
Thread-embedding acupuncture (TEA) offers a potentially more efficient approach. This technique involves inserting bioabsorbable threads into acupuncture points, providing sustained stimulation over time. As a result, TEA may reduce the need for frequent clinic visits while maintaining therapeutic efficacy.11 By lowering treatment frequency while offering similar benefits to traditional acupuncture, TEA could improve patient adherence.11 Sustained stimulation of acupoints frequently used in OAB management may enhance bladder control and reduce detrusor overactivity.
However, while acupuncture, including thread-embedding techniques, has been widely used for bladder dysfunction in Traditional Chinese Medicine, rigorous evidence supporting the efficacy and safety of TEA in postmenopausal women with OAB is still limited. This gap highlights the need for well-designed clinical trials to validate the therapeutic benefits of TEA and assess its safety profile.
Therefore, in this study designed as a randomized controlled clinical trial with a sham TEA control group, we aimed to rigorously evaluate the efficacy and safety of TEA treatment for OAB in postmenopausal women.
Methods
Study Design and Setting
This multicenter, randomized, controlled, double-blind, parallel-group clinical trial was conducted at Dong-eui University Korean Medicine Hospital and Busan National University Korean Medicine Hospital. Sixty-eight participants with OAB were randomly assigned in a 1:1 ratio to receive either TEA or sham TEA. The study lasted 16 weeks, consisting of 8 weeks of active treatment followed by an 8-week follow-up. The timeline for enrollment, intervention, and assessment is shown in Supplementary Table 1.
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and complied with the international standards of Good Clinical Practice. The study protocol followed the Consolidated Standards of Reporting Trials and Standards for Reporting Interventions in Clinical Trials of Acupuncture guidelines.
Ethical Approval and Study Registration
The study protocol was approved by the Institutional Review Boards of the Dong-eui University Korean Medicine Hospital (DH 2023–07) and Busan National University Korean Medicine Hospital (PNUKHIRB 2023–11-001). All participants provided written informed consent before enrollment. The protocol was registered with the Clinical Research Information Service (CRIS), Republic of Korea (KCT0009905).
Participants
Postmenopausal women were recruited through advertisements in outdoor areas and on hospital websites. Eligibility was initially assessed by the primary researchers according to the inclusion and exclusion criteria. Eligible participants were women aged ≥ 40 years, postmenopausal for at least 1 year since the last menstruation, and not receiving hormone replacement therapy within the past 6 months. Additional inclusion criteria required symptoms of urinary urgency and frequency for at least 3 months before enrollment, with an OAB Symptom Score (OABSS) of 3 or higher. Exclusion criteria included urinary tract infection, pure stress urinary incontinence, neurogenic bladder disorders, a history of pelvic or bladder surgery, or the presence of a pacemaker or other implantable medical devices. Patients were withdrawn if they became unwilling to continue participation. Those who failed to attend at least six sessions were also excluded.
Randomization and Blinding
An independent statistician generated the randomization sequence using R. Allocation sequences were sealed in opaque envelopes and distributed to each participating research center, where they were securely stored in a double-locked cabinet. At the initial visit (visit 1), the investigator enrolled eligible participants and assigned them in a 1:1 ratio to the TEA or sham TEA group according to the predetermined block randomization.
Practitioners could not be blinded but were excluded from outcome assessments. To minimize bias, outcome analyses were conducted by researchers not involved in randomization or treatment. Participant blinding was maintained by using eye patches during treatment, which prevented them from visually detecting whether threads were embedded. Both participants and outcome assessors remained blinded to group assignments. The success of blinding was evaluated at the final session (visit 8) using blinding index.12
Interventions
Participants were randomly assigned to TEA or sham TEA, administered once weekly for 8 weeks (Figure 1). Licensed Korean medicine practitioners with at least 1 year of clinical experience in acupuncture, trained in the study protocol, performed all procedures. Patient adherence was encouraged through interviews and telephone consultations, and no additional OAB treatments were permitted during the trial.
 |
Figure 1 Study flowchart. |
TEA was delivered using disposable needles (30G × 25 mm) at CV3 (Zhongji), BL33 (Zhongliao), and BL35 (Huiyang). This technique involves inserting absorbable threads to provide sustained stimulation. Needles were inserted to a depth of approximately 20–25 mm with standard manual manipulation, and absorbable polydioxanone (PDO) threads were released within the tissue. Sham TEA involved inserting identical needles at the same acupoints but without thread embedding, thereby mimicking acupuncture only.
Acupoints were selected based on a structured review of the literature on acupuncture for overactive bladder.13 Candidate points included CV3, SP6, KI3, BL33, and BL35. An internal feasibility assessment was conducted during protocol development to evaluate the tolerability and technical suitability of thread embedding at the candidate sites. Based on this assessment, ankle-region acupoints (KI3 and SP6) were excluded due to limited subcutaneous tissue depth and increased procedural discomfort. The final protocol included CV3 and bilateral BL33 and BL35.
Sample Size
Based on a preliminary clinical trial,14 which demonstrated a significant reduction in average 24-hour micturition frequency from baseline to visit 8, the estimated mean difference for this study was conservatively set at half the observed change (−1.27) with a standard deviation of 1.64. With a significance level of 0.05 and a power of 80%, the required sample size was calculated as 27 participants per group. Allowing for a 20% dropout rate, the total sample size was set at 68 participants.
Outcome Measures
Efficacy was evaluated using a 3-day bladder diary, the OABSS, and the King’s Health Questionnaire (KHQ). Participants completed bladder diaries before treatment, after treatment, and during the 8-week follow-up period. They documented urination patterns for 3 consecutive days before each follow-up visit, noting the time of each urination and urgency level using a 5-point Urgency Rating Scale (URS), where 1 indicates no urgency and 5 indicates urgent urinary incontinence (UUI).
The OABSS assesses four domains of OAB bladder symptoms (daytime frequency, nocturia, urgency, and UUI), with total scores of 0–15.15 The KHQ measures quality of life in relation to OAB symptoms and includes 10 domains: general health perception, incontinence impact, role limitations, physical limitations, social limitations, personal relationships, emotions, sleep/energy, severity measures, and symptom severity. Validated Korean versions of both questionnaires were used.16,17
The primary outcome was the change in average 24-h voiding frequency from baseline (visit 1) to the end of treatment (visit 8), as recorded in the 3-day bladder diary.
Secondary outcomes included additional parameters from the 3-day bladder diary: daytime and nighttime urination frequency, total number of urgency episodes (URS score ≥3), total urgency scores over 3 days, and total number of UUI episodes. Furthermore, participants completed the Korean versions of the OABSS and KHQ at baseline, post-treatment (visit 8), and at follow-up (visit 10).
Safety and Data Management
All participants were monitored for adverse events (AEs), defined as any undesirable or unintentional signs, symptoms, or diseases that occurred post-intervention, regardless of causality. At each visit, investigators assessed participants’ vital signs and evaluated any AEs, which were classified by severity, seriousness, and relationship to the intervention. All AEs were documented and monitored according to institutional standards. Data were collected using electronic case report forms, secured with password protection. Data were anonymized and periodically reviewed by independent clinical experts and statisticians.
Statistical Analysis
The primary analysis was conducted using the full analysis set (FAS), consistent with the intention-to-treat principle. Participants were excluded from the FAS only if they met prespecified criteria, including violation of eligibility criteria, use of prohibited concomitant medications, or absence of the baseline assessment for the primary outcome. A secondary per-protocol (PP) analysis was also performed.
Continuous variables were summarized as mean, standard deviation, median, minimum, and maximum, and categorical variables as frequencies and percentages. The primary outcome was analyzed using analysis of covariance (ANCOVA), with baseline values included as covariates. Secondary outcomes measured at multiple time points were analyzed using repeated measures analysis of variance (RM-ANOVA), with time as the within-subject factor and group as the between-subject factor. The group × time interaction was used to evaluate differences between groups over time. All statistical tests were two-sided with a significance level of 5%. Missing data were handled using the Last Observation Carried Forward method.
Result
Participants
In total, 68 participants were enrolled and randomly assigned to the intervention group (n = 34) or the control group (n = 34). All 34 participants in the intervention group were included in the full analysis set (FAS) population. In the control group, two participants were found, after allocation of randomization numbers but prior to initiation of the intervention, to have violated predefined exclusion criteria (history of urinary stone surgery and prior urinary incontinence surgery). They were excluded from the FAS population, leaving 32 participants in the control group for analysis (Figure 1).
All participants who received at least one intervention were included in the safety analysis set. Baseline demographic and clinical characteristics, including height, weight, body mass index, sex, smoking status, and alcohol consumption, were collected for participants in the FAS set. Participant demographics are summarized in Table 1.
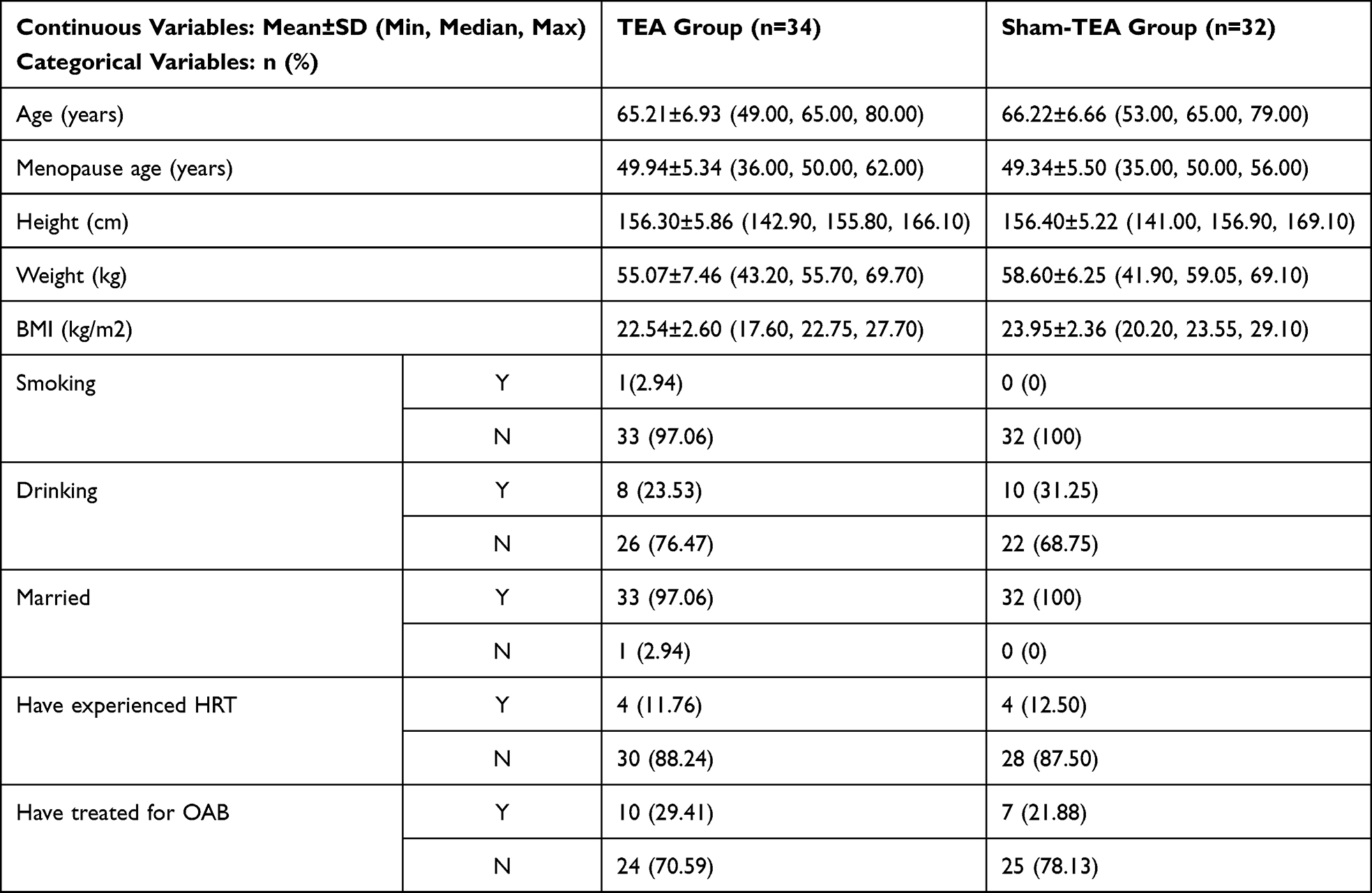 |
Table 1 Demographic Characteristics |
Primary Outcome Analysis
In the FAS analysis, the mean 24-h micturition frequency decreased from 12.06 ± 2.06 at baseline to 10.00 ± 2.07 at visit 8 in the intervention group, and from 11.81 ± 2.78 to 9.84 ± 2.36 in the control group (Figure 2). After adjustment for baseline values using analysis of covariance (ANCOVA), the between-group difference in the change from baseline to visit 8 was not statistically significant in the FAS population (p = 0.9579). Similar results were observed in the PP analysis (p = 0.8798) (Table 2).
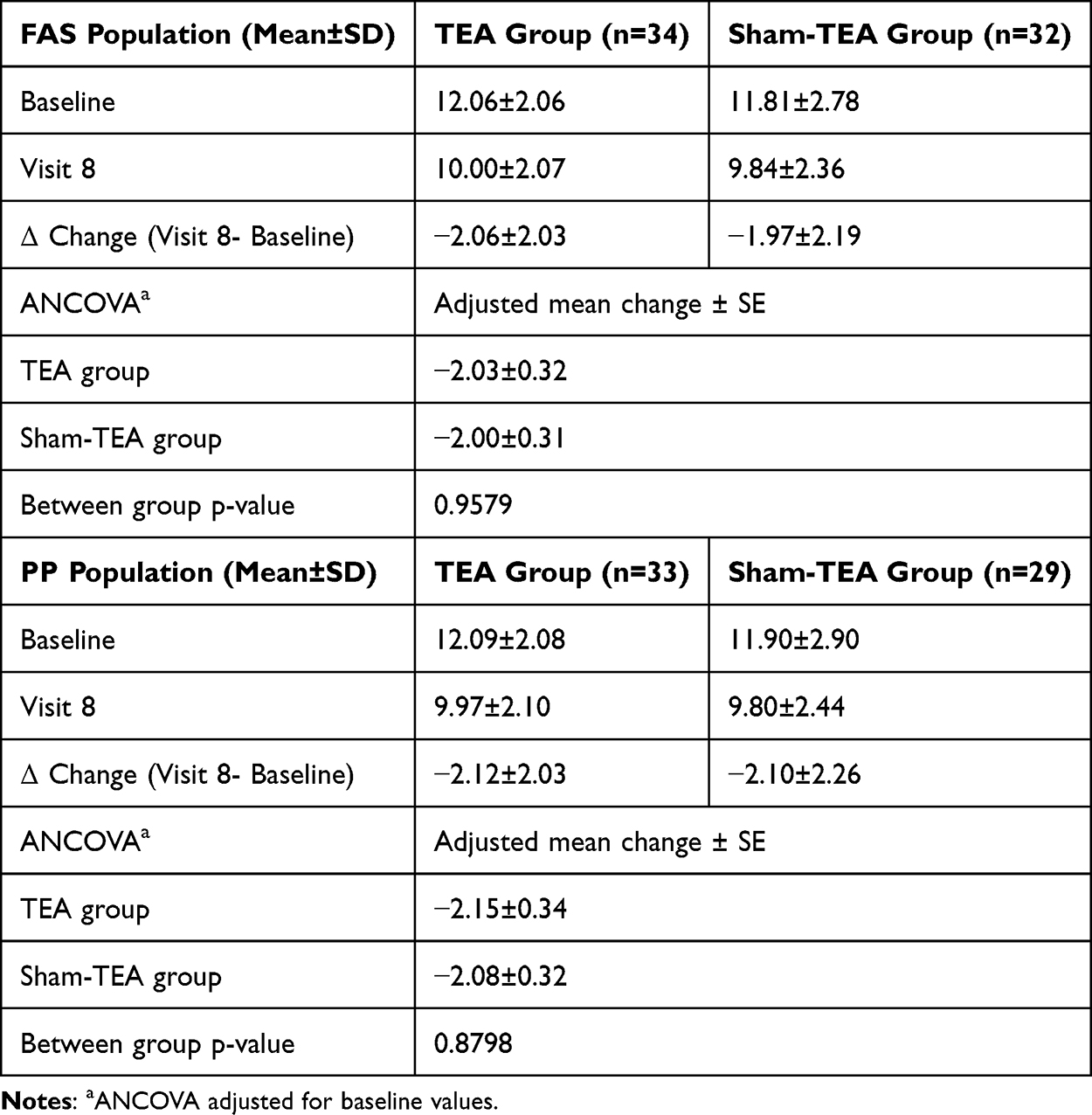 |
Table 2 Primary Outcome Analysis of 24-Hour Voiding Frequency |
 |
Figure 2 Mean voiding frequency by timepoint and group. |
Secondary Outcome Analysis
Changes in Voiding Frequency
Repeated measures ANOVA showed no significant group-by-time interaction for 24-h or daytime micturition frequency, indicating no differential treatment effect over time between groups. However, a significant main effect of time was observed (p < 0.0001), suggesting overall improvement over time in both groups (Supplementary Table 2).
For nocturnal micturition frequency, there was no significant group effect or group-by-time interaction. A significant main effect of time was observed, reflecting improvement over time in both groups. Although the change from baseline at visit 10 reached statistical significance only within the intervention group, the between-group difference remained non-significant (p = 0.8490) (Figure 2, Supplementary Table 2).
Changes in Urgency
There were no significant group effects or group-by-time interactions for urgency episodes or urgency urinary incontinence episodes. A significant main effect of time was observed (p < 0.0001), indicating symptom improvement over time in both groups (Supplementary Table 2).
Changes in OABSS and KHQ Scores
Repeated measures ANOVA demonstrated no significant group effects or group-by-time interactions for OABSS or KHQ scores. However, a significant main effect of time was observed for both outcomes (p < 0.0001), indicating progressive improvement across visits in both groups (Supplementary Table 3).
Safety Analysis
No serious AEs occurred during the trial. AEs were reported in 23 participants (34.85%), totaling 27 events: 12 participants (35.29%, 14 events) in the TEA group and 11 participants (34.38%, 13 events) in the sham TEA group (Table 3). Among these 23 participants, three events were assessed as “possibly related” to the intervention: two in the TEA group (16.67%) and one in the sham TEA group (9.09%). In the TEA group, two events (16.67%) were classified as “probably not related”, and the remaining events were deemed “definitely not related”: eight participants (66.67%) in the TEA group and ten (90.91%) in the sham TEA group.
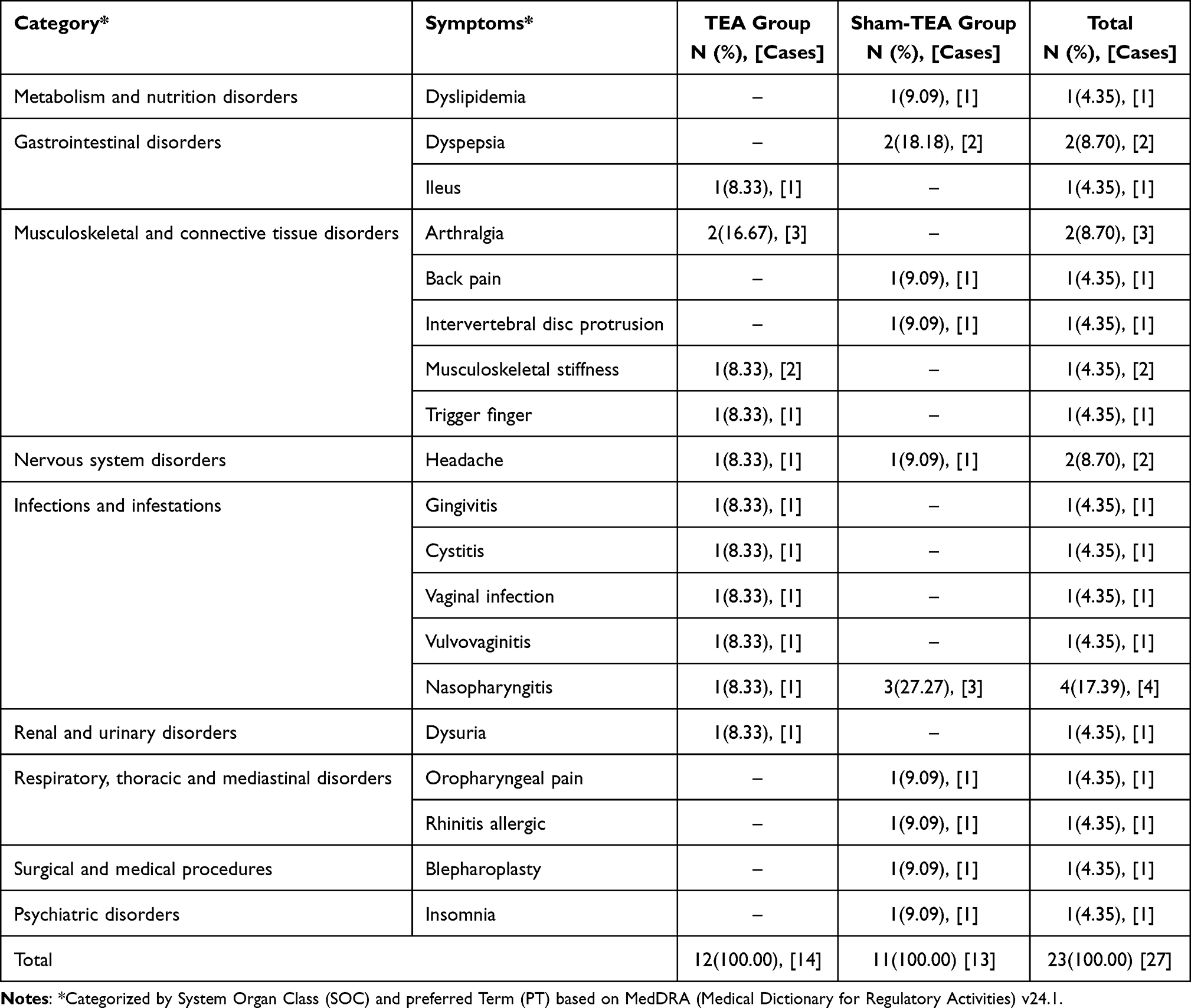 |
Table 3 Reported Adverse Events |
Discussion
This study describes a randomized controlled trial evaluating the potential benefits of TEA for managing OAB symptoms in postmenopausal women. Unlike traditional pharmacological treatments, which can cause side effects or have contraindications, TEA offers a nonpharmacological alternative that may provide sustained symptom relief through continuous acupoint stimulation.
The focus on postmenopausal women reflects the high prevalence of OAB in this demographic and the limitations of current treatment options. Traditional acupuncture has shown promise in alleviating similar symptoms; however, TEA may enhance efficacy and patient compliance by reducing the frequency of treatment sessions.
Accordingly, we compared TEA with sham TEA (manual acupuncture without thread embedding) to isolate effects of the thread itself. To minimize confounding factors, rigorous blinding procedures, including the use of eye masks, were implemented. Assessment using the Blinding Index (BI) confirmed that blinding was effectively maintained.
The selected acupoints (CV3, BL33, and BL35) are among those frequently reported in acupuncture studies targeting bladder dysfunction. These points are anatomically located in the lower abdomen and sacral region, areas closely associated with bladder innervation and pelvic floor regulation. Their use in the present study is consistent with previously reported therapeutic strategies for modulating lower urinary tract function.
The 8-week treatment duration was determined based on previous acupuncture studies7,18 in postmenopausal women with OAB. The intervention period falls within the commonly employed treatment range and was considered sufficient to allow therapeutic response while maintaining clinical practicality.
In total, 68 participants were equally allocated to the intervention and control groups. Both groups experienced an approximate reduction of two micturitions per day over the 2-month treatment period, and this improvement persisted at the 2-month follow-up. A reduction of approximately 1.5 or more voids per 24 h is generally considered clinically meaningful based on previous literature.19 However, the between-group difference was not statistically significant.
After 8 weeks of treatment, daytime micturition frequency decreased by approximately 1.6 episodes in both groups, while nighttime frequency decreased by approximately 0.4 episodes. At the 2-month follow-up, the nighttime micturition reduction remained significant in the intervention group (−0.41 episodes; p < 0.05), whereas the control group showed a reduction of −0.35 episodes, which was not statistically significant. Since nocturia occurring more than twice per night is associated with reduced quality of life, the reduced to less than twice per night can be considered clinically meaningful.20
The OABSS decreased by approximately four points from baseline to visit 10 in both groups, with no statistically significant difference between groups. A change of three points or more on the OABSS has been suggested as the minimal threshold for a clinically meaningful improvement.21 Both groups achieved a therapeutic effect exceeding this threshold at the end of treatment and at follow-up.
In this trial, both MA and TEA produced statistically and clinically significant improvements in urinary frequency and other OAB symptoms compared with baseline, sustained for 2 months post-treatment. However, no significant between-group differences were observed, reflecting the specific effect attributable to the embedded thread.
Two factors may explain the lack of intergroup differences. First, the study duration may have been insufficient to detect the sustained differential effect of the embedded thread. Previous studies indicate that inserted threads can persist in the body for approximately 3–6 months. Therefore, long-term evaluation—with follow-up extending at least 3 months after the final treatment—may be necessary to fully assess the unique contribution of the thread. In this study, the follow-up period was limited to 2 months after treatment, during which both groups showed sustained symptom improvement without divergence in effect.
Second, the weekly treatment frequency may have been sufficient for MA alone to produce therapeutic effects comparable to those of TEA, reducing the detectable difference between the interventions. To better isolate the effect of thread insertion, future trials should consider extending the interval between treatment sessions while maintaining long-term follow-up.
Clinically, these findings suggest that regular acupuncture, even without thread embedding, can yield meaningful improvements in OAB symptoms when administered at a fixed frequency over a defined treatment period. This insight may guide patient selection when considering TEA versus MA.
Regarding safety, no serious AEs related to the interventions were observed up to 2 months after treatment, supporting the relative safety of both TEA and MA in this patient population.
Previous studies indicate that acupuncture is highly safe, with a low incidence of adverse effects, and produces moderate to large improvements in OAB symptoms, significantly enhancing patients’ quality of life and well-being.22 In addition, clinical trials have investigated related interventions, such as moxibustion and electroacupuncture, confirming their efficacy and safety. Combined acupuncture and moxibustion have demonstrated greater effects than acupuncture alone,23 and trials comparing electroacupuncture with manual acupuncture are ongoing.24 However, to date, no studies have evaluated TEA. Therefore, this study addresses this gap by providing preliminary evidence on the efficacy and safety of TEA for OAB.
This study has limitations. The relatively small sample size, limited follow-up duration, and restricted number of participating centers may limit the generalizability of the findings and reduce statistical power to detect modest between-group differences, particularly for secondary outcomes and long-term effects. While validated symptom-based measures and bladder diary parameters were used in accordance with international clinical trial standards for OAB, the absence of urodynamic assessments may limit the exploration of underlying physiological mechanisms. Future studies incorporating both symptom-based and physiological parameters could provide complementary insights into treatment effects. Finally, due to the lack of previous studies on TEA for OAB, comparisons with existing evidence are limited, highlighting the need for larger, multicenter trials with longer follow-up and more diverse outcome measures.
Future research should address several factors. First, longer-term evaluations of TEA, particularly with less frequent treatment intervals, are needed to assess its sustained efficacy. Second, detailed subgroup analyses incorporating relevant clinical factors—such as disease duration and comorbidities—should be performed to identify patient characteristics predictive of greater benefit. Third, refinement of the sham TEA control is warranted. In this study, sham TEA involved needle insertion at identical acupoints without thread placement, which may have produced therapeutic effects from acupuncture alone, limiting its validity as an inert placebo.
In conclusion, while no significant differences were observed between TEA and MA, both interventions were effective and safe for symptom alleviation in postmenopausal women with OAB. Further large-scale, long-term studies are needed to confirm the specific benefits, cost-effectiveness, and sustained safety of TEA.
Data Sharing Statement
The data generated and analyzed during the current study are not publicly available due to ethical restrictions but may be made available from the corresponding author upon reasonable request.
Acknowledgments
The study protocol was presented as an oral presentation at the 19th World Congress on Menopause (Dates: 18~22, October 2024; Location: [Melbourne, Australia]) hosted by the International Menopause Society.
Funding
This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: RS-2022-KH127717).
Disclosure
The authors report no competing interests in this work.
References
1. Haylen BT, De Ridder D, Freeman RM, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn. 2010;29(1):4–11. doi:10.1002/nau.20798
2. Chuang Y-C, Liu S-P, Lee K-S, et al. Prevalence of overactive bladder in China, Taiwan and South Korea: results from a cross-sectional, population-based study. Low Urin Tract Symptoms. 2019;11(1):48–55. doi:10.1111/luts.12193
3. Lee Y-S, Lee K-S, Jung JH, et al. Prevalence of overactive bladder, urinary incontinence, and lower urinary tract symptoms: results of Korean EPIC study. World J Urol. 2011;29(2):185–190. doi:10.1007/s00345-009-0490-1
4. Sang JH, Park HM. Survey on the prevalence of overactive bladder in healthy Korean postmenopausal women. J Korean Soc Menopause. 2012;18(1):60. doi:10.6118/jksm.2012.18.1.60
5. Sexton CC, Coyne KS, Thompson C, et al. Prevalence and effect on health-related quality of life of overactive bladder in older Americans: results from the epidemiology of lower urinary tract symptoms study. J Am Geriatr Soc. 2011;59(8):1465–1470. doi:10.1111/j.1532-5415.2011.03492.x
6. Vouri SM, Kebodeaux CD, Stranges PM, et al. Adverse events and treatment discontinuations of antimuscarinics for the treatment of overactive bladder in older adults: a systematic review and meta-analysis. Arch Gerontol Geriatr. 2017;69:77–96. doi:10.1016/j.archger.2016.11.006
7. Hargreaves E, Baker K, Barry G, et al. Acupuncture for treating overactive bladder in adults. Cochrane Database Syst Rev. 2022;9(9):CD013519. doi:10.1002/14651858.CD013519.pub2
8. Zhao Y, Zhou J, Mo Q, et al. Acupuncture for adults with overactive bladder: a systematic review and meta-analysis of randomized controlled trials. Medicine. 2018;97(8):e9838. doi:10.1097/MD.0000000000009838
9. Mak TC, Chen HY, Cho WC. Acupuncture for overactive bladder in adults: a systematic review and meta-analysis. Acupunct Med. 2019;37(6):321–331. doi:10.1136/acupmed-2017-011528
10. Lee JJ, Heo JW, Choi TY, et al. Acupuncture for the treatment of overactive bladder: a systematic review and meta-analysis. Front Neurol. 2022;13:985288. doi:10.3389/fneur.2022.985288
11. Kazemi AH, Adel-Mehraban MS, Jamali Dastjerdi M, et al. A comprehensive practical review of acupoint embedding as a semi-permanent acupuncture: a mini review. Med Baltim. 2024;103(23):e38314. doi:10.1097/MD.0000000000038314
12. Bang H, Ni L, Davis CE. Assessment of blinding in clinical trials. Control Clin Trials. 2004;25(2):143–156. doi:10.1016/j.cct.2003.10.016
13. Cho SI, Kim DI, Choi SJ. A Review of Acupuncture Treatment Methods for Urinary incontinence and Overactive bladder in Postmenopausal Women. J Korean Obstet Gynecol. 2022;35(4):121–142. doi:10.15204/jkobgy.2022.35.4.121
14. Choi SJ, Lee H, Kim DI. Thread embedding acupuncture in postmenopausal women with overactive bladder: a prospective, single-arm, before-after study. Int J Womens Health. 2024;16:2287–2296. doi:10.2147/IJWH.S494135
15. Homma Y, Yoshida M, Seki N, et al. Symptom assessment tool for overactive bladder syndrome—overactive bladder symptom score. Urology. 2006;68(2):318–323. doi:10.1016/j.urology.2006.02.042
16. Jeong SJ, Homma Y, Oh S-J. Korean version of the overactive bladder symptom score questionnaire: translation and linguistic validation. Int Neurourol J. 2011;15(3):135–142. doi:10.5213/inj.2011.15.3.135
17. Oh S-J, Choo M-S, Kim HS, et al. Psychometric properties of the Korean version of the King’s health questionnaire in women with stress urinary incontinence. J Korean Continence Soc. 2005;9(2):115–123. doi:10.5213/jkcs.2005.9.2.115
18. Noh EJ, Choi SJ, Kim DI, et al. Effectiveness and safety of electroacupuncture and manual acupuncture in postmenopausal women with overactive bladder: a multicenter, randomized, controlled, parallel clinical trial. Acupuncture Med. 2025;43(6):316–329. doi:10.1177/09645284251399237
19. van Kerrebroeck P, Chapple C, Drogendijk T, et al. Combination therapy with solifenacin and tamsulosin oral controlled absorption system in a single tablet for lower urinary tract symptoms in men: efficacy and safety results from the randomised controlled Neptune trial. Eur Urol. 2013;64(6):1003–1012. doi:10.1016/j.eururo.2013.07.034
20. Tikkinen KAO, Johnson TM II, Tammela TLJ, et al. Nocturia frequency, bother, and quality of life: how often is too often? A population-based study in Finland. Eur Urol. 2010;57(3):488–496. doi:10.1016/j.eururo.2009.03.080
21. Gotoh M, Homma Y, Yokoyama O, et al. Responsiveness and minimal clinically important change in overactive bladder symptom score. Urology. 2011;78(4):768–773. doi:10.1016/j.urology.2011.06.020
22. Ma J, Ren F, Lu S, et al. Acupuncture therapy of overactive bladder: an umbrella review and meta-analysis. Arab J Urol. 2025;23(1):75–83. doi:10.1080/20905998.2024.2400628
23. Guo X, Guo X, Hu P, et al. Evaluation of the effect of acupuncture combined with cross-moxibustion in the treatment of patients with severe overactive bladder. Urologia. 2025;92(3):536–543. doi:10.1177/03915603251327833
24. Wang H-Y, Ji Y, Zhang S, et al. Effectiveness of electroacupuncture for the treatment of refractory overactive bladder disease in women: study protocol for a randomised controlled clinical trial. BMJ Open. 2025;15(7):e101864. doi:10.1136/bmjopen-2025-101864
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of Overactive Bladder Symptoms in Patients Recovering from Post-Acute COVID-19 Syndrome
Zachariou A, Sapouna V, Kaltsas A, Dimitriadis F, Douvli E, Champilomatis I, Kounavou C, Papatsoris A, Tsounapi P, Takenaka A, Sofikitis N
Journal of Multidisciplinary Healthcare 2022, 15:2447-2452
Published Date: 26 October 2022
Thread Embedding Acupuncture in Postmenopausal Women with Overactive Bladder: A Prospective, Single-Arm, Before-After Study

Choi SJ, Lee H, Kim DI
International Journal of Women's Health 2024, 16:2287-2296
Published Date: 23 December 2024
Integrated Western and Traditional Chinese Medicine Approaches for Herpes Zoster and Post-Herpetic Neuralgia: A Narrative Review
Li L, Xu J, Al-Danakh A, Xing Q
Drug Design, Development and Therapy 2026, 20:570847
Published Date: 13 January 2026