Back to Journals » Journal of Pain Research » Volume 16
Therapeutic Potential of Downregulated Interleukin-6 Signaling for the Treatment of Chronic Pain: A Mendelian Randomization Study
Received 22 June 2023
Accepted for publication 23 November 2023
Published 18 December 2023 Volume 2023:16 Pages 4317—4328
DOI https://doi.org/10.2147/JPR.S424086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Wendy Imlach
Yaodan Bi,1,* Yingchao Zhu,2,* Shuai Tang1
1Department of Anesthesiology, Peking Union Medical College Hospital, Peking Union Medical College and Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 2Department of Anesthesiology, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shuai Tang, Department of anesthesiology, Peking Union Medical College Hospital, Beijing, People’s Republic of China, Email [email protected]
Introduction: While numerous studies have emphasized the pivotal involvement of the Interleukin 6 (IL-6) pathway in the development of chronic pain, the causal nature of this relationship remains uncertain.
Methods: In this study, we opted to include genetic variants situated within the locus of the IL-6 receptor (IL-6R) that exhibited associations with C-reactive protein (CRP) levels. CRP serves as a downstream effector in the IL-6 pathway. Utilizing these variants as genetic proxies, we aimed to modulate IL-6 signaling. Employing a two-sample Mendelian randomization (MR) approach, we investigated the potential link between the genetic proxy and seven distinct subtypes of chronic pain, categorized based on their corresponding body locations. Moreover, we examined the relationship between chronic pain and an alternative instrument of IL-6 signaling that was weighted based on s-IL-6R levels. Furthermore, we conducted exploratory analyses to estimate the plausible causal association between CRP, gp130, and the subtypes of chronic pain.
Results: Our analysis showed that genetic proxied downregulation of IL-6 signaling, weighted on CRP levels, was linked to a reduced risk of chronic back and knee pain. The sensitivity analyses across various MR methods confirmed the consistency of the findings and showed no evidence of horizontal pleiotropy or heterogeneity. Moreover, the results remained robust with different sets of instrument variables. A genetically increased level of s-IL-6R was also negatively associated with chronic back and knee pain. However, there was no causal relationship between CRP and gp130 with chronic pain.
Conclusion: Based on our findings, there is evidence to suggest a potential causal relationship between IL-6 signaling and chronic back and knee pain. Consequently, the downregulation of IL-6 signaling holds promise as a potential therapeutic target for addressing chronic back and knee pain.
Keywords: IL-6 signaling, chronic pain, Mendelian randomization
Introduction
Pain serves as an unpleasant experience that encompasses both sensory and emotional components and functions as an indicator of existing or potentially dangerous harm to the body, thus activating a biological state of alertness.1,2 Pain may be classified according to its etiology, location, or period of manifestation. Chronic pain, which persists for more than three months, either regularly or intermittently, represents a common and severe ailment which leads to various negative consequences, including significant impairments, decreased mobility, falls, anxiety, depression, social isolation, sleep disorders, and sarcopenia.3–7 Chronic pain shares numerous features with chronic low-grade inflammation.8 A wide range of pharmacological options, such as opioids, non-steroidal anti-inflammatory drugs (NSAIDs), and gabapentin, among others, are currently available for the management of chronic pain.9–11 Nevertheless, current treatments remain somewhat limited with over 50% of patients experiencing an inadequate relief of pain that requires the emergence of fresh therapeutic alternatives.12
In the classical cis-signaling pathway, the initiation of the inflammatory response by Interleukin-6 (IL-6) occurs through its binding with glycoprotein-130 (gp130) at the IL-6 receptor locus present on the cell membrane (m-IL-6R). Additionally, IL-6R exists in a soluble form within the circulation (s-IL-6R), and when it forms a complex with gp130, it can exert an inhibitory effect on IL-6 action, thus operating through the trans-signaling pathway.13,14 The classical signaling pathway of IL-6 plays a pivotal role in initiating the production of acute-phase proteins, such as C-reactive protein (CRP) and fibrinogen, by engaging signaling mechanisms that exert wide-ranging effects.14 Numerous previous studies have provided evidence demonstrating a correlation between elevated IL-6 levels and various subtypes of pain, such as chronic neuropathic pain, inflammatory pain, and migraine pain.15 Furthermore, the injection of IL-6 through the intrathecal route results in pain-associated behavior, which implies that IL-6 influences the spinal circuits responsible for pain in rats.16 Mendelian randomization (MR) analysis serves as a valuable alternative to randomized clinical trials by utilizing genetic variations linked to a particular exposure. This approach allows for the evaluation of causal relationships and the identification of potential therapeutic targets, which can subsequently be investigated in clinical trials.17
The primary aim of this study was to investigate the potential causal relationship between the downregulation of IL-6 signaling and chronic pain in various regions of body. To accomplish this, we developed a genetic instrument that served as a proxy for pharmacological inhibition of IL-6R, utilizing summary-level data derived from Genome-Wide Association Studies (GWAS). Subsequently, a two-sample Mendelian Randomization (MR) analysis was conducted to explore the potential causal association between IL-6 signaling downregulation and chronic pain, utilizing data obtained from the UK Biobank. Furthermore, we performed exploratory analyses to develop genetic instruments for CRP, sIL-6R, and gp130 levels, with the aim of evaluating their potential associations with chronic pain.
Method
Study Design
In this study, our objective was to conduct a two-sample Mendelian Randomization (MR) investigation to estimate the effect of downregulated IL-6 signaling on chronic pain. The implementation of this study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology-Mendelian Randomization (STROBE-MR) reporting guidelines (refer to Table S1 for details). The study design is outlined in Figure 1, and comprehensive information regarding the datasets utilized can be found in Table S2.
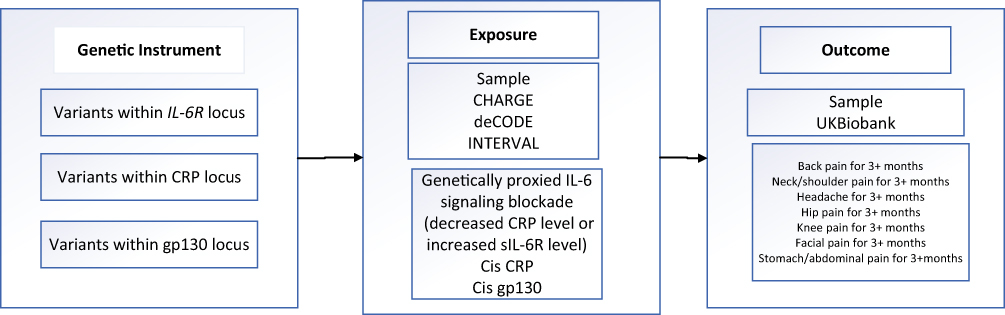 |
Figure 1 Schematic diagram of the present study. |
Outcome
We selected chronic back pain, chronic stomach/abdominal pain, chronic neck/shoulder pain, chronic knee pain, chronic hip pain, chronic facial pain, chronic headache as concerned pain phenotypes. We did not include chest pain as outcome of interest since chest pain is highly mixed with cardiopulmonary disease. Each chronic pain phenotype was established by utilizing self-report answers to the specified questions: Have you had [back pains/neck or shoulder pains/ stomach/abdominal pain/ knee pain/ hip pain/ facial pain/ headache] for more than 3 months? Participants were provided with the options of responding “Yes”, “No”, “Don’t know”, or “Prefer not to answer” to these questions. Individuals who answered “Yes” to a specific question were considered cases for that particular pain phenotype. Number of cases for each GWAS were as follows: back pain (N = 80,588); neck/shoulder pain (N = 72,887); facial pain (N = 3107); hip pain (N= 40,152); knee pain (N=76,910), headache (N=41,719); stomach/abdominal pain (N= 21,711) (Table S2).
Primary IL-6 Signaling Instrument, Weighted on CRP Levels
The IL6R instruments employed in this study were selected based on a recent meta-analysis of a high-sensitivity CRP GWAS conducted on a large cohort of European individuals. The meta-analysis included data from the Cohorts for Heart and Aging Research in Genomic Epidemiology (CHARGE) Consortium and the UK Biobank, encompassing over half a million participants.18 Our main aim was to determine the impact of reduced activity within the IL-6/IL6R pathway. We accomplished this by using independent variants located within 300 kb of IL6R that have an r2-value less than 0.1, which approximated the effect of IL6R. We refer to this approach as “cisIL6R instrument”, which was in line with previous studies.18–21 Our genetic instrument replicated the action of monoclonal antibodies that target IL6R, like tocilizumab, effectively blocking both IL6 classical and trans-signaling pathways. However, it was crucial to acknowledge that the inhibitory effect observed with our genetic instrument was noticeably small compared to the therapeutic inhibition of IL-6R.21 We evaluated the strength of our instrumental variables using F-statistics, (F = beta2 /SE2), the instrument variable was considered robust with F-statistics>10. In order to mitigate the potential issue of overfitting the data due to sample overlap (known as winner’s curse), we opted to utilize the estimated effect sizes of variants solely from the CHARGE dataset, rather than incorporating the UKB-CHARGE meta-analysis. This approach aligns with a previous study conducted in a similar context.18 A total of twenty-six single nucleotide polymorphisms (SNPs) were included in our analysis as instrumental variables (IVs) (Table S3).
Alternative IL-6 Signaling Instrument, Weighted on s-IL-6R Levels
We developed an indirect genetic instrument to investigate IL-6 signaling by utilizing genetic variations associated with s-IL-6R levels, which have been shown to have an inverse correlation with IL-6 signal activity. We identified a set of 34 SNPs located within a 250 kb region of the IL-6R gene that had a consistent association with increased s-IL-6R levels (Table S4). These genetic variants have been widely employed in previous studies for other investigations. The summary-level GWAS data used in our analysis were obtained from the INTERVAL research project.22,23
cisCRP Variants
Our primary genetic instrument consists exclusively of variants located in the vicinity of the IL6R gene. These IVs were developed based on their association with CRP levels, which serve as a proxy for IL-6 function. It’s important to keep in mind that utilizing CRP as the causal biomarker does not necessarily imply that CRP itself is the underlying cause. We sought to determine whether C-reactive protein (CRP) could be a potential target for causal intervention and designed a separate group of cis genetic instruments with the aim of reducing CRP levels. These variants are thought to have an impact on CRP through a pathway that is not related to IL-6 down-regulation. We selected 16 CRP-associated SNPs within a 300kB region of the CRP locus, each SNP having a P-value lower than 5*10-8 and an r2 below 0.1 (Table S5). To perform two-sample MR analyses, we weighted these cis-variants using CHARGE estimates of hsCRP.24
cisgp130 Instruments
The IL-6 receptor is made up of two components, with gp130 (also called IL6ST) serving as the other one that also exists in different cytokine receptors. Although not as well-established as the correlation found between variation at IL6R and specific health outcomes, previous studies have reported phenotypic implications associated with variations in gp130.25,26 We aimed to develop genetic instruments using a recent Genome-Wide Association Study (GWAS) involving 35,287 participants from the DECODE consortium.27 We extracted 24 independent SNPs (with a P-value lower than 5*10−8 and an r2 below 0.1) and linked to gp130 levels within a range of 300 kb of the gp130 area (Table S6).
Statistical Analysis and Sensitivity Analysis
The primary method employed in our analysis was the inverse-variance weighted (IVW) method, which allowed us to derive an overall estimate regarding the causal effect of genetically proxied IL-6 signaling blockade on various subtypes of chronic pain. To ensure the robustness of our findings, we conducted several sensitivity tests to assess the assumptions of Mendelian randomization (MR).
Firstly, we utilized the MR-Egger, simple mode, weighted mode, MR Pleiotropy Residual Sum and Outlier (MR-PRESSO), and weighted median approaches as part of our meta-analytic methods. These tests helped us assess the potential presence of pleiotropy and evaluate the overall consistency of our results. A MR-Egger intercept near zero indicates the absence of directional pleiotropy, further strengthening the validity of our findings.28 With MR-PRESSO global test, we sequentially eliminated SNPs from the regression and evaluated whether there existed a SNP that influenced the association (P-value global test < 0.05).29 This analysis allowed us to identify and address potential outliers or influential SNPs that may have affected our results. Lastly, Cochran’s Q statistic was used to assess heterogeneity among the SNPs. A Cochran’s Q P-value below 0.05 suggests the presence of heterogeneity, indicating that the association between IL-6 signaling blockade and chronic pain may vary across different SNPs. For the causal relationships that reached statistical significance, we employed a systematic approach known as iterative leave-one-out analysis, which involved the sequential exclusion of each SNP from the model and the subsequent recalculation of IVW estimates. This method allowed us to examine the stability and reliability of our findings while assessing the individual contributions of each SNP to the overall estimate. In addition, we investigated whether the SNPs selected for our analysis might have influenced our findings. We reevaluated the results by introducing another set of variants chosen based on the CHARGE data that had previously been employed in identifying causal links among IL-6 and autoimmune arthritis, coronary heart disease, autoimmune disease, and longevity.22,30,31 Furthermore, since some of certain variants of our primary instruments could been viewed as weak instruments based solely on beta values derived from CHARGE data, we repeated the analysis while excluding variants with F-statistics <10 from the subset of variants. Finally, we utilized Asp358Ala SNP (rs2228145), a canonical and well-established single instrument, to run the analysis.32
We set the statistical significance level at P<0.05 for our analysis. To account for multiple testing (ie, multiple exposures), we defined the statistical significance of MR effect estimates as a false discovery rate (FDR) less than 5%. Results were classified as robust (FDR-significant, and consistent across sensitivity analyses), suggestive (P-value<0.05, FDR P-value>0.05, and inconsistent across sensitivity analyses), or not present. All the statistical analyses mentioned above were performed using the “TwoSampleMR” and “MendelianRandomization” packages in R (version 4.1.0). These packages provide robust and reliable tools for conducting Mendelian randomization analyses and were instrumental in our study for assessing causal relationships between IL-6 signaling and chronic pain.
Result
IL-6 Signaling, Weighted by CRP Levels (Primary Instrument)
For each outcome, we performed IVW MR analyses using our instruments weighted by hsCRP separately. Since our instruments were weighted by hsCRP, the odds ratios (ORs) obtained were on the scale of natural log hsCRP decrease. This framework allowed us to quantify the impact of IL6R blockade on the respective outcomes and evaluate the direction and magnitude of the observed effects.
Genetically proxied IL6R blockade was associated with a lower risk of chronic back pain (IVW: OR 0.96, 95% CI 0.94–0.98, P= 0.0002, FDR-corrected P =0.002), and chronic knee pain (IVW: OR 0.96, 95% CI 0.94–0.99, P=0.0009, FDR-corrected P= 0.003). Besides, genetically proxied IL6R blockade was suggestively associated with lower risk of chronic facial pain (IVW: OR 0.89, 95% CI 0.81–0.99, P= 0.03, FDR-corrected P =0.07). Genetically proxied IL6R blockade has no significant effect on chronic headaches (IVW: OR = 0.97, 95% CI = 0.94–1.01, P = 0.11), chronic hip pain (IVW: OR = 0.98, 95% CI = 0.95–1.01, P = 0.21), chronic neck/shoulder pain (IVW: OR = 1.00, 95% CI = 0.98–1.02, P = 0.98), chronic stomach/abdominal pain (IVW: OR = 0.99, 95% CI = 0.96–1.06, P = 0.64).
We observed consistent results across multiple MR methods, as shown in Table S7 and Figure 2. The MR-Egger intercept analysis did not reveal any evidence of pleiotropy, which strengthens the validity of our causal inferences (Table S8). Furthermore, our findings remained robust in the leave-one-out sensitivity analysis, as indicated in Tables S9 and S10. No outlier was identified through MR-PRESSO. Heterogeneity was found in the association between IL6R blockade and chronic headache, no other evidence of heterogeneity or pleiotropy was found (Table S8).
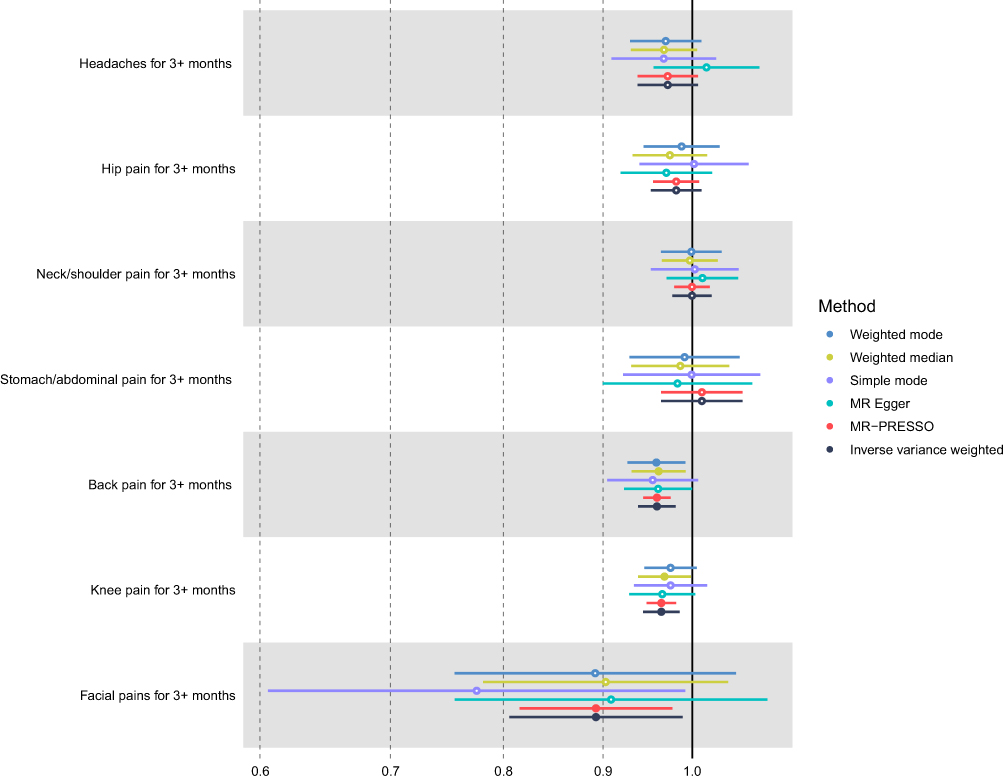 |
Figure 2 Association of genetically proxied IL-6 signaling blockade using main instrument proxied by CRP levels with risk of chronic pain subtypes. Forest plot of odds ratios (OR) are on the scale of natural log CRP decrease. Data are represented as odds ratios (ORs) with 95% confidence intervals (error bars). |
IL-6 Signaling, Proxied by sIL-6R Levels (Alternative Instrument)
As our instruments are weighted by sIL-6R levels, β are on the scale of sIL-6R level per SD increase. As IL-6 signaling negative regulators sIL-6R genetically increased, the risk of chronic back pain (IVW: β −0.003 95% CI −0.005, −0.0004, P=0.02, FDR-corrected P=0.06) and chronic knee pain (IVW: β −0.003 95% CI −0.005, −0.0007, P=0.008, FDR-corrected P=0.06) suggestively decreased, in accordance with main analysis results using direct instrument. Besides, genetically proxied higher sIL-6R level was suggestively associated with lower risk of chronic headache (IVW: β −0.003 95% CI −0.006, −0.0003, P=0.03). Genetically proxied sIL-6R level has no significant effect on chronic hip pain (IVW: β −0.002 95% CI −0.005, 0.001, P=0.18), chronic neck/shoulder pain (IVW: β 0.0004 95% CI −0.002, 0.002, P=0.76), chronic stomach/abdominal pain (IVW: β 0.001 95% CI −0.003, 0.006, P=0.58) and chronic facial pain (IVW: β −0.002 95% CI −0.012, 0.008, P=0.63).
The outcomes obtained from the alternative MR methods exhibited a high degree of consistency, as indicated by the results presented in Table S11 and Figure 3. Notably, the MR-Egger intercept analysis did not reveal evidence of pleiotropy, except in the case of sIL-6R level and its association with chronic stomach/abdominal pain (Table S8). No outlier was identified through MR-PRESSO. No other evidence of heterogeneity or pleiotropy was found (Table S8).
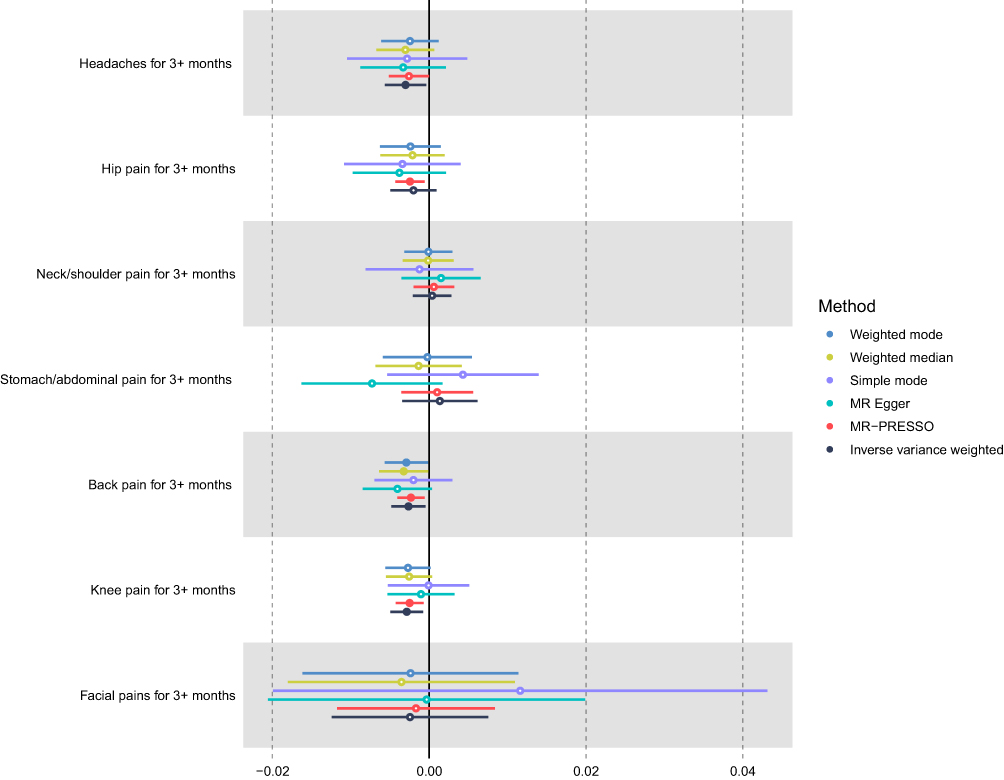 |
Figure 3 Association of genetically proxied IL-6 signaling blockade using alternative instrument proxied by sIL-6R levels with risk of chronic pain subtypes. Forest plot of beta are on the scale of 1 SD sIL-6R increase. Data are represented as beta with 95% confidence intervals (error bars). |
CRP Levels and gp130 Levels
In our IVW MR analyses using the cisCRP instrument, we observed no significant association between genetically predicted CRP levels and the risk of any subtype chronic pain. This suggested that the effects of IL-6 signaling on chronic pain could not be mediated through CRP itself. The results from the analysis of cis variants in gp130 were consistent with these findings. We found no evidence of an effect from gp130 levels on any type of chronic pain. These results are presented in Table S12 and Figure 4 for the cisCRP instrument and Table S13 and Figure 5 for the analysis of gp130 variants.
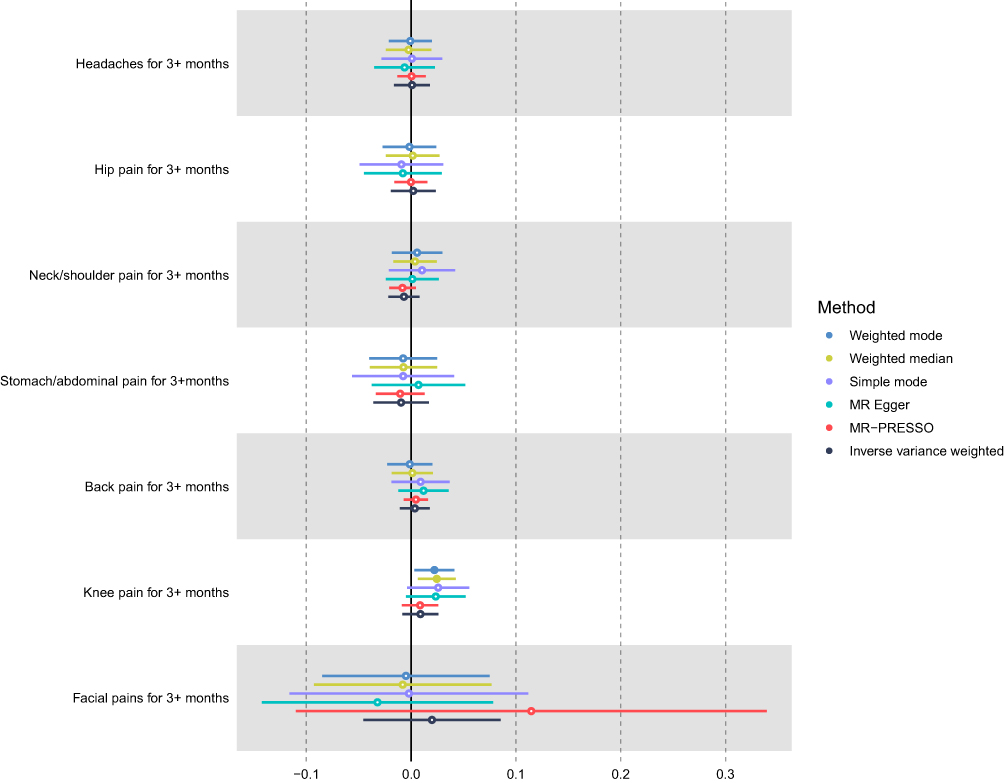 |
Figure 4 Association of genetically proxied CRP with risk of chronic pain subtypes. Forest plot of beta are on the scale of 1 natural log CRP increase. Data are represented as beta with 95% confidence intervals (error bars). |
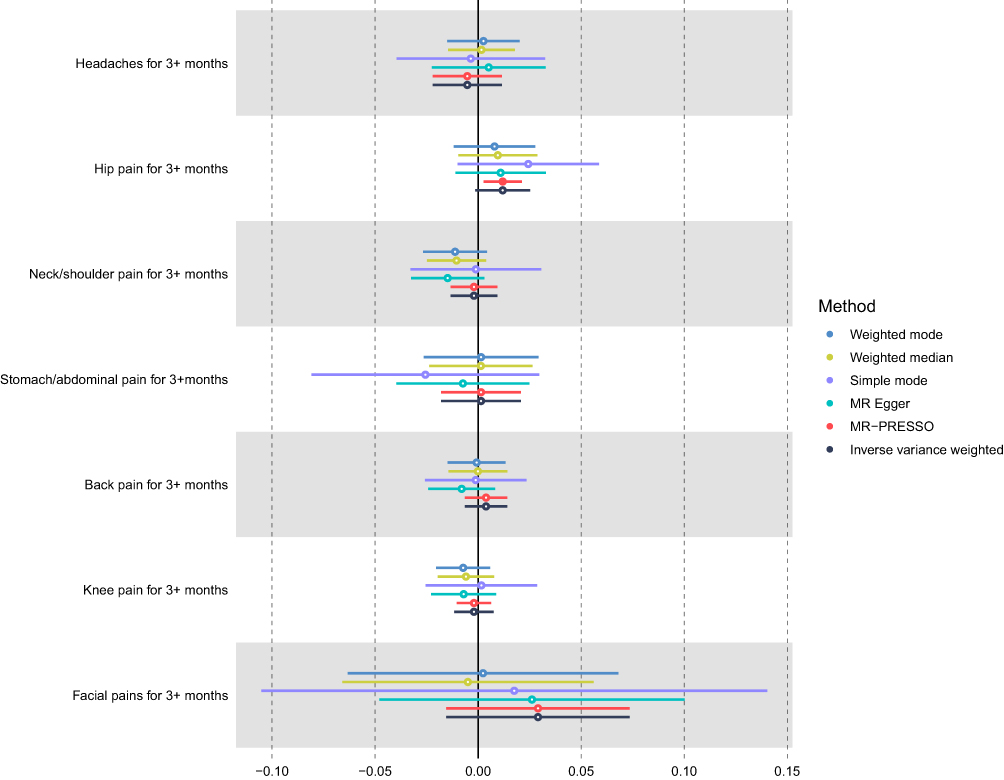 |
Figure 5 Association of genetically proxied gp130 with risk of chronic pain subtypes. Forest plot of beta are on the scale of 1 SD gp130 increase. Data are represented as beta with 95% confidence intervals (error bars). |
Sensitivity Analysis
We performed a comprehensive set of sensitivity analyses assess the robustness of the observed causal link between genetically proxied IL-6R blockade and all subtypes of chronic pain.
Firstly, we employed MR-Egger, weighted mode, simple mode, weighted median, and MR-PRESSO approaches to evaluate the exclusion restriction assumption. MR-PRESSO results were comparable to IVW results, and no outlier was detected by MR-PRESSO except for the association between gp130 and chronic headache. However, the estimates obtained from MR-Egger, weighted mode, simple mode, and weighted median were less precise, with most confidence intervals crossing the null (Tables S7 and S11–13)
Secondly, we conducted additional analyses to assess the potential impact of instrument selection on our results. While all the variants related to IL-6 signaling from the UKB-CHARGE meta-analysis had F-statistics greater than 10, it was noted that some of these variants were considered weak instruments when using beta solely from the CHARGE dataset. To address this concern, we performed a re-analysis excluding variants with F-statistics less than 10. Remarkably, the effects obtained from this subset of instruments were consistent with our primary results, further supporting the robustness of our findings (Table S14). Moreover, we expanded our analysis by incorporating another set of variants selected based on the CHARGE data. The results pertaining to the causal relationship between genetically proxied IL-6R blockade and chronic back pain and chronic knee pain were similar, although the precision of the estimates was slightly reduced due to the smaller number of instruments included (Table S15). Finally, we conducted analyses specifically focusing on the rs2228145 SNP, which is known to have a functional effect on IL6R and downstream signaling. Despite the reduced statistical power resulting from the restricted analysis, the observed effects remained consistent with our primary results, reinforcing the validity of the causal association (Table S16).
Discussion
In this study, we employed a two-sample Mendelian randomization (MR) study to examine the relationship between IL-6 signaling blockade and different subtypes of chronic pain. To estimate the causal effect, we constructed a genetic instrument that served as a proxy for inhibiting IL-6 signaling. This instrument was associated with lower levels of CRP, which is a marker reflecting the classical IL-6 signaling pathway. Our results indicate that downregulation of IL-6 signaling was associated with a reduced risk of chronic back and knee pain. However, we did not find significant associations between IL-6 signaling blockade and other forms of chronic pain. Importantly, these findings were consistent when using an alternative instrument based on s-IL-6R levels, providing additional support for the robustness of our results.
Our study findings indicate that inhibiting CRP was unlikely to have a significant impact on reducing the risk of chronic pain. This suggested that the observed effect was specific to IL-6R variants that influence IL-6 signaling and was not attributable to any direct action of CRP. Moreover, our findings suggest that sgp130’s inhibitory effects on IL-6 trans signaling may not provide protection against chronic pain of any type. The null result obtained could be attributed to the inadequate strength of SNPs used as instrumental variables in this analysis. However, another plausible explanation could be sgp130’s efficacy in inhibiting trans signaling could be limited at normal concentrations because of rapid formation and dissociation of the IL-6/sIL-6R complex.33 Hence, the application of Mendelian randomization method could not accurately capture the inhibitory effects of gp130 in the trans pathway.
Our findings align with previous clinical and experimental studies, adding to the growing body of evidence supporting a potential causal relationship between IL-6 signaling and chronic back or knee pain. In a previous study conducted on male mice, it was demonstrated that Interleukin-6 signaling plays a crucial role in cartilage degradation and pain development in posttraumatic osteoarthritis, a prevalent cause of chronic knee pain.34 A cross-sectional study found that IL-6 was positive correlated with chronic knee pain, although it could not rule out the risk of reverse causation.35 A recent meta-analysis found patients with chronic low back pain had elevated IL-6 level.36 Animal experimentation indicated that injecting IL6/sIL6R into rat knee joints increased spinal neuron responsiveness to mechanical stimulation.37 Moreover, in a previous study, Tocilizumab, a humanized monoclonal antibody targeting the IL-6 receptor (IL6R), was administered epidurally to individuals suffering from sciatica and low back pain. The study revealed that the use of Tocilizumab on the spinal nerve led to more substantial pain relief compared to treatment with dexamethasone, suggesting the potential therapeutic efficacy of IL-6 signaling blockade in alleviating chronic pain associated with these conditions.38
In our study, we did not observe a significant association between IL-6 signaling blockade and a decreased risk of chronic headache, chronic hip pain, chronic stomach/abdominal pain, and chronic neck/shoulder pain. The evidence regarding the impact of IL-6 signaling inhibition on chronic facial pain was not conclusive but suggestive. However, it is important to note that the conclusions drawn for chronic facial pain should be interpreted with caution due to limitations in sample size and statistical power. Future studies with larger sample sizes and increased statistical power are required to validate or refute these findings in a more robust manner.
Pain can have different biological origins across various maladies and body regions. For instance, chronic abdominal pain is predominantly visceral in nature and often characterized by diffuse and challenging localization. A cohort study specifically examining IL-6 polymorphisms revealed no statistically significant difference between individuals with chronic post-cholecystectomy pain and healthy controls. This finding suggested that variations in IL-6 genetic markers may not contribute significantly to the development of chronic pain following cholecystectomy.39 A randomized controlled study investigating the effects of effective low-level laser therapy on patients with temporomandibular disorder, a common of facial pain, did not observe a significant change in IL-6 plasma concentration.40 Besides, a cohort study found no association between IL-6 polymorphism with development of chronic temporomandibular pain.41 A study with 689 participants found no association between IL-6 plasma concentration and chronic hip, shoulder, and neck pain.35
The results of our research suggested that targeting the IL-6 pathway could potentially reduce the risk of developing chronic back and knee pain. It is important to exercise caution when interpreting these findings, as the effects of targeting the IL-6 pathway specifically on chronic pain intensity and duration are still unknown. While the studies mentioned provide insights into the association between IL-6 signaling and certain types of chronic pain, further research is needed to fully understand the potential impact of modulating the IL-6 pathway on the severity and duration of chronic pain. While Monoclonal antibodies that target IL-6 signaling by binding to IL-6R have indeed received FDA approval for the treatment of rheumatoid arthritis,42 the magnitude of the effects observed in our study was much smaller in comparison to reported effects in RA treatments. Additionally, as MR analysis has its limitations, it cannot predict the impact of drugs that may possess a more significant effect over a shorter period. Thus, further investigation into the underlying mechanisms of the relationship between the IL-6 pathway and chronic back/knee pain risk is necessary.
The study was also inevitable of some limitations. MR findings rely on three assumptions that may not always be completely achievable, and RCTs are still needed to infer causality in the future.43 Although IVs could possibly affect the risk of chronic knee or back pain through pathways other than those in the IL-6 cascade, we did not observe any evidence of heterogeneity indicating that IVs operate through a different path. Nonetheless, there may be unknown associations between confounding factors and the risk of chronic back or knee pain, making it still possible. It’s challenging to rule out various effects, such as SNPs impacting chronic pain risk through an unrelated mechanism as our focus was on variants within or near the IL6R. Moreover, genetically proxied down-regulation of IL-6 being linked to reduced likelihood rates of a variety of conditions including cardiometabolic syndrome44, frailty45 and cerebral cortical structure.46 Consequently, identifying the exact mechanism could be difficult. Nonetheless, given the consistency of previous randomized controlled study utilizing IL-6R antibodies for the treatment of chronic back pain,38 as well as the supportive evidence from randomized trial data in inflammatory bowel disease that endorse the use of genetic proxies for IL6R blockade,47,48 along with the consistent results obtained using different sets of SNPs within the IL6R region, we could reasonably infer that alterations in IL6R played a pivotal role in driving the observed effect.
To the best of our knowledge, this study represented the first piece of evidence supporting a plausible causal association between genetically mediated downregulation of IL-6 signaling and chronic pain. The robustness of our findings was bolstered by several strengths inherent in the study design. Firstly, we leveraged coefficients derived from large and well-characterized datasets such as the UK Biobank and CHARGE, enhancing the generalizability of our results. Secondly, we comprehensively assessed various proteins and measures relevant to IL-6 signaling pathways, providing a comprehensive understanding of the underlying mechanisms. Thirdly, we employed multiple approaches to address potential sources of bias, including the evaluation of horizontal pleiotropy, outlier SNPs, and heterogeneity, further strengthening the validity of our conclusions. Lastly, the consistency of outcomes across multiple sets of instrument variables and Mendelian Randomization approaches lends further support to the robustness and reliability of our findings.
In conclusion, our study provides compelling evidence suggesting a potential causal relationship between IL-6 signaling and chronic back and knee pain. The observed associations support the notion that downregulation of IL-6 signaling could hold promise as a treatment target for managing these types of chronic pain. Further research and clinical trials are warranted to explore the clinical implications of targeting IL-6 signaling in pain management strategies.
Data Sharing Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding authors.
Ethics Approval and Consent to Participate
As per the regulations outlined in People’s Republic of China’s “Notice on the Implementation of Ethical Review Measures for Life Science and Medical Research”, our study falls under the exemption criteria specified in Section 4 of the regulation. Therefore, ethics approval was not required for this research, as it met the following conditions:
1. Exemption Premise: The study exclusively utilized publicly available data, specifically summary-level data from GWAS, which does not involve sensitive personal information, pose harm to individuals, or compromise their privacy.
2. Exemption Provision: Our research adheres to the exemption circumstances outlined in Section 4 of the regulation:
- We utilized lawfully obtained publicly available data for our analysis.
- The data used in this study were fully anonymized, ensuring the privacy and confidentiality of individuals.
- Our research focuses on analyzing existing data and does not involve interventions, human biological samples, or activities related to reproductive cloning, genetic manipulation, or germ cells.
Due to the nature of our study and its compliance with the exemption criteria, we did not require explicit ethics approval. While informed consent was not obtained from individual participants since the study involved publicly available data, we ensured that all data accessed and analyzed were fully de-identified and complied with the terms of use and guidelines provided by the data source. We affirm that this research was conducted in accordance with the applicable laws, regulations, and ethical standards.
Acknowledgments
We gratefully acknowledge the authors and participants of all GWASs including UK Biobank, deCODE, CHARGE, and INTERVAL study from which we used summary statistics data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Andrew R, Derry S, Taylor RS, et al. The costs and consequences of adequately managed chronic non-cancer pain and chronic neuropathic pain. Pain Pract. 2014;14:79–94. doi:10.1111/papr.12050
2. Yong RJ, Mullins PM, Bhattacharyya N. Prevalence of chronic pain among adults in the United States. Pain. 2022;163:e328–e332. doi:10.1097/j.pain.0000000000002291
3. Hirase T, Okubo Y, Sturnieks DL, Lord SR. Pain is associated with poor balance in community-dwelling older adults: a systematic review and meta-analysis. J Am Med Dir Assoc. 2020;21:597–603.e598. doi:10.1016/j.jamda.2020.02.011
4. Karimi R, Mallah N, Scherer R, et al. Sleep quality as a mediator of the relation between depression and chronic pain: a systematic review and meta-analysis. Br J Anaesth. 2023;130:747–762. doi:10.1016/j.bja.2023.02.036
5. Attal N, Bouhassira D, Colvin L. Advances and challenges in neuropathic pain: a narrative review and future directions. Br J Anaesth. 2023;131:79–92. doi:10.1016/j.bja.2023.04.021
6. Tsuji H, Tetsunaga T, Misawa H, et al. Association of phase angle with sarcopenia in chronic musculoskeletal pain patients: a retrospective study. J Orthop Surg Res. 2023;18:87. doi:10.1186/s13018-023-03567-1
7. Kim HJ, Ban MG, Yoon KB, et al. Neuropathic-like pain symptoms and their association with muscle strength in patients with chronic musculoskeletal pain. J Clin Med. 2022;12:11. doi:10.3390/jcm12010011
8. Pinto EM, Neves JR, Laranjeira M, Reis J. The importance of inflammatory biomarkers in non-specific acute and chronic low back pain: a systematic review. Eur Spine J. 2023;32:3230–3244. doi:10.1007/s00586-023-07717-1
9. Birkinshaw H, Friedrich CM, Cole P, et al. Antidepressants for pain management in adults with chronic pain: a network meta-analysis. Cochrane Database Syst Rev. 2023;5:Cd014682. doi:10.1002/14651858.CD014682.pub2
10. Falope EO, Appel SJ. Substantive review of the literature of medication treatment of chronic low back pain among adults. J Am Assoc Nurse Pract. 2015;27:270–279. doi:10.1002/2327-6924.12155
11. Chou R, Huffman LH. Medications for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline. Ann Intern Med. 2007;147:505–514. doi:10.7326/0003-4819-147-7-200710020-00008
12. Kelleher JH, Tewari D, McMahon SB. Neurotrophic factors and their inhibitors in chronic pain treatment. Neurobiol Dis. 2017;97:127–138. doi:10.1016/j.nbd.2016.03.025
13. Rose-John S. Interleukin-6 family cytokines. Cold Spring Harb Perspect Biol. 2018;2018:10.
14. Rose-John S. Blocking only the bad side of IL-6 in inflammation and cancer. Cytokine. 2021;148:155690. doi:10.1016/j.cyto.2021.155690
15. Koçer A, Memişoğullari R, Domaç FM, et al. IL-6 levels in migraine patients receiving topiramate. Pain Pract. 2009;9:375–379. doi:10.1111/j.1533-2500.2009.00301.x
16. DeLeo JA, Colburn RW, Nichols M, Malhotra A. Interleukin-6-mediated hyperalgesia/allodynia and increased spinal IL-6 expression in a rat mononeuropathy model. J Interferon Cytokine Res. 1996;16:695–700. doi:10.1089/jir.1996.16.695
17. Bowden J, Holmes MV. Meta-analysis and Mendelian randomization: a review. Res Synth Methods. 2019;10:486–496. doi:10.1002/jrsm.1346
18. Georgakis MK, Malik R, Burgess S, Dichgans M. Additive effects of genetic interleukin-6 signaling downregulation and low-density lipoprotein cholesterol lowering on cardiovascular disease: a 2×2 factorial Mendelian randomization analysis. J Am Heart Assoc. 2022;11:e023277. doi:10.1161/JAHA.121.023277
19. Khandaker GM, Zuber V, Rees JMB, et al. Shared mechanisms between coronary heart disease and depression: findings from a large UK general population-based cohort. Mol Psychiatry. 2020;25:1477–1486. doi:10.1038/s41380-019-0395-3
20. Kappelmann N, Arloth J, Georgakis MK, et al. Dissecting the association between inflammation, metabolic dysregulation, and specific depressive symptoms: a genetic correlation and 2-sample Mendelian randomization study. JAMA Psych. 2021;78:161–170. doi:10.1001/jamapsychiatry.2020.3436
21. Hamilton FW, Thomas M, Arnold D, et al. Therapeutic potential of IL6R blockade for the treatment of sepsis and sepsis-related death: a Mendelian randomisation study. PLoS Med. 2023;20:e1004174. doi:10.1371/journal.pmed.1004174
22. Rosa M, Chignon A, Li Z, et al. A Mendelian randomization study of IL6 signaling in cardiovascular diseases, immune-related disorders and longevity. NPJ Genom Med. 2019;4:23. doi:10.1038/s41525-019-0097-4
23. Sun BB, Maranville JC, Peters JE, et al. Genomic atlas of the human plasma proteome. Nature. 2018;558:73–79. doi:10.1038/s41586-018-0175-2
24. Ligthart S, Vaez A, Võsa U, et al. Genome analyses of >200,000 individuals identify 58 loci for chronic inflammation and highlight pathways that link inflammation and complex disorders. Am J Hum Genet. 2018;103(5):691–706. doi:10.1016/j.ajhg.2018.09.009
25. Gottardo L, De Cosmo S, Zhang YY, et al. A polymorphism at the IL6ST (gp130) locus is associated with traits of the metabolic syndrome. Obesity. 2008;16:205–210. doi:10.1038/oby.2007.28
26. Morieri ML, Passaro A, Zuliani G. Interleukin-6 “Trans-Signaling” and ischemic vascular disease: the important role of soluble gp130. Mediators Inflamm. 2017;2017:1396398. doi:10.1155/2017/1396398
27. Ferkingstad E, Sulem P, Atlason BA, et al. Large-scale integration of the plasma proteome with genetics and disease. Nat Genet. 2021;53:1712–1721. doi:10.1038/s41588-021-00978-w
28. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44:512–525. doi:10.1093/ije/dyv080
29. Verbanck M, Chen C-Y, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nature Genetics. 2018;50:693–698. doi:10.1038/s41588-018-0099-7
30. Hong J, Qu Z, Ji X, et al. Genetic Associations Between IL-6 and the Development of Autoimmune Arthritis Are Gender-Specific. Front Immunol. 2021;2021:12.
31. Georgakis MK, Malik R, Gill D, et al. Interleukin-6 signaling effects on ischemic stroke and other cardiovascular outcomes. Circulation. 2020;13:e002872. doi:10.1161/CIRCGEN.119.002872
32. Wensley F, Gao P, Burgess S, et al. Association between C reactive protein and coronary heart disease: Mendelian randomisation analysis based on individual participant data. BMJ. 2011;342:d548.
33. Baran P, Hansen S, Waetzig GH, et al. The balance of interleukin (IL)-6, IL-6·soluble IL-6 receptor (sIL-6R), and IL-6·sIL-6R·sgp130 complexes allows simultaneous classic and trans-signaling. J Biol Chem. 2018;293:6762–6775. doi:10.1074/jbc.RA117.001163
34. Liao Y, Ren Y, Luo X, et al. Interleukin-6 signaling mediates cartilage degradation and pain in posttraumatic osteoarthritis in a sex-specific manner. Sci Signal. 2022;15:eabn7082. doi:10.1126/scisignal.abn7082
35. Norman KS, Goode AP, Alvarez C, et al. Association of biomarkers with individual and multiple body sites of pain: the Johnston County osteoarthritis project. J Pain Res. 2022;15:2393–2404. doi:10.2147/JPR.S365187
36. Canlı K, Billens A, Van Oosterwijck J, et al. Systemic cytokine level differences in patients with chronic musculoskeletal spinal pain compared to healthy controls and its association with pain severity: a systematic review. Pain Med. 2022;23:1947–1964. doi:10.1093/pm/pnac091
37. Vazquez E, Kahlenbach J, Segond von Banchet G, et al. Spinal interleukin-6 is an amplifier of arthritic pain in the rat. Arthritis Rheum. 2012;64:2233–2242. doi:10.1002/art.34384
38. Ohtori S, Miyagi M, Eguchi Y, et al. Efficacy of epidural administration of anti-interleukin-6 receptor antibody onto spinal nerve for treatment of sciatica. Eur Spine J. 2012;21:2079–2084. doi:10.1007/s00586-012-2183-5
39. Blichfeldt-Eckhardt MR, Olsen DA, Andersen RF, et al. Elevated levels of PGE2-metabolite in cerebrospinal fluid and Cox-2 gene polymorphisms in patients with chronic, post cholecystectomy pain and visceral hyperalgesia compared to healthy controls. A hypothesis-generating pilot study. J Pain Res. 2022;15:3921–3929. doi:10.2147/JPR.S387502
40. Zwiri AM, Ahmad W, Asif JA, et al. A randomized controlled trial evaluating the levels of the biomarkers hs-CRP, IL-6, and IL-8 in patients with temporomandibular disorder treated with LLLT, traditional conservative treatment, and a combination of both. Int J Environ Res Public Health. 2022;20:19. doi:10.3390/ijerph20010019
41. Campello CP, Lima ELS, Fernandes RSM, et al. Genetic polymorphisms of TNF-α, IL-6, and IL-10 in female elderly patients with chronic temporomandibular disorder pain. Spec Care Dentist. 2023;43:144–151. doi:10.1111/scd.12757
42. Rubbert-Roth A, Furst DE, Nebesky JM, et al. A review of recent advances using tocilizumab in the treatment of rheumatic diseases. Rheumatol Ther. 2018;5:21–42. doi:10.1007/s40744-018-0102-x
43. Haycock PC, Burgess S, Wade KH, et al. Best (but oft-forgotten) practices: the design, analysis, and interpretation of Mendelian randomization studies. Am J Clin Nutr. 2016;103:965–978. doi:10.3945/ajcn.115.118216
44. Cupido AJ, Asselbergs FW, Natarajan P, et al. Dissecting the IL-6 pathway in cardiometabolic disease: a Mendelian randomization study on both IL6 and IL6R. Br J Clin Pharmacol. 2022;88:2875–2884. doi:10.1111/bcp.15191
45. Mourtzi N, Georgakis M, Ntanasi E, et al. Genetically downregulated Interleukin-6 signalling is associated with a lower risk of frailty. Age Ageing. 2023;2023:52.
46. Liu C, Zhu S, Zhang J, et al. Inflammatory bowel diseases, interleukin-6 and interleukin-6 receptor subunit alpha in causal association with cerebral cortical structure: a Mendelian randomization analysis. Front Immunol. 2023;14:1154746. doi:10.3389/fimmu.2023.1154746
47. Danese S, Vermeire S, Hellstern P, et al. Randomised trial and open-label extension study of an anti-interleukin-6 antibody in Crohn’s disease (ANDANTE I and II). Gut. 2019;68:40–48. doi:10.1136/gutjnl-2017-314562
48. Parisinos CA, Serghiou S, Katsoulis M, et al. Variation in interleukin 6 receptor gene associates with risk of crohn’s disease and ulcerative colitis. Gastroenterology. 2018;155:303–306.e302. doi:10.1053/j.gastro.2018.05.022
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.