Back to Journals » Patient Preference and Adherence » Volume 19
Therapeutic Adherence and Potentially Inappropriate Prescribing in Older Adults with Polypharmacy in Primary Health Care
Authors Lafuente González M ![]() , Calleja Hernández MA, Ferrit Martín M
, Calleja Hernández MA, Ferrit Martín M
Received 11 March 2025
Accepted for publication 18 October 2025
Published 1 December 2025 Volume 2025:19 Pages 3849—3860
DOI https://doi.org/10.2147/PPA.S524773
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Marta Lafuente González,1 Miguel Angel Calleja Hernández,2 Mónica Ferrit Martín3
1Department Medicines for Human Use, Pharmacology and Clinical Assessment Division, Spanish Agency of Medicines and Medical Device, Madrid, Spain; 2Department of Pharmacy, Hospital Universitario Virgen de la Macarena, Seville, Spain; 3Department of Pharmacy. Hospital San Juan de la Cruz, Úbeda, Jaén, Spain
Correspondence: Marta Lafuente González, Email [email protected]
Purpose: Treatment adherence is essential for achieving therapeutic goals and improving patient outcomes. In older adults, polypharmacy and potentially inappropriate prescriptions (PIPs) may negatively affect adherence.
Objective: To assess treatment adherence in older adults with polypharmacy and PIPs in a primary care setting.
Patients and Methods: A descriptive, observational study was carried out in the primary care setting of Toledo, Spain, involving patients aged over 65 who had been taking six or more medications for at least six months. Demographic, clinical, and pharmacological data were collected. Adherence was the primary outcome. PIPs were assessed using the Beers and STOPP criteria. Data were obtained from electronic medical records, prescription systems, and billing records.
Results: The study included 448 patients (mean age: 79 years; 60.9% female). A total of 4413 medications were prescribed, with a mean of 9.9 drugs per patient. Overall adherence was 64.3%. The prevalence of PIPs was 44.0% (STOPP) and 42.6% (Beers). No significant association was found between adherence and PIPs (p = 0.426 for Beers; p = 0.164 for STOPP).
Conclusion: Among older adults with polypharmacy, treatment adherence was 64.3%. The rate of potentially inappropriate prescribing was high, but no significant relationship with adherence was observed. Further studies are needed to explore the impact of PIPs in this population. Pharmaceutical interventions—such as educational programmes for prescribers and patients, and regular medication reviews—may help improve adherence.
Keywords: older adults, polypharmacy, chronic diseases, medication adherence, potentially inappropriate prescribing, primary care
Introduction
Ageing and increased life expectancy have led to a rise in multimorbidity and polypharmacy. The terms pluripathology or multimorbidity refer to the presence of two or more chronic diseases. Polypharmacy describes the simultaneous use of multiple medications.
Treatment adherence — the extent to which patients follow treatment recommendations agreed upon with their healthcare provider — is a key component in managing chronic diseases in older adults with polypharmacy.1 Adherence is essential to achieving treatment goals and improving health outcomes.2
A prescription is considered potentially inappropriate in older adults if the potential adverse effects outweigh the clinical benefits, particularly when a safer alternative are available.3–5 Several tools have been developed to assess the appropriateness of drug therapy in polymedicated older patients, including the Beers criteria,4 and the Screening Tool of Older Person’s Potentially Inappropriate Prescriptions (STOPP) criteria.5,6 Ongoing medication review and monitoring of adherence by primary care professionals provide an opportunity to prevent and identify potentially inappropriate prescriptions (PIPs).
In Spanish primary care, up to 40% of individuals — regardless of age — have three or more chronic diseases, and among these, 94% are polymedicated.7 It is estimated that chronic diseases account for 80% of primary care consultations,7 that 50% of individuals with chronic conditions do not adhere to prescribed treatment,8 and that between 6% and 20% of patients fail to collect their prescribed medications from the pharmacy.9 Previous studies have shown that the prevalence of polypharmacy in older adults ranges from 13% to 92%, depending on the definitions used and the characteristics of the study population.10
Patient-related factors associated with non-adherence include, among others, age, gender, number of chronic diseases and number of medications.8,11,12 Non-adherence results in reduced clinical benefits, diminished treatment efficacy, poorer disease control, and increased risks of morbidity and mortality. It also leads to higher rates of emergency department visits, medical consultations, hospitalisations,13 and overall healthcare costs, while negatively affecting patients’ quality of life. For these reasons, medication adherence is considered major public health priority,8,14 particularly among older adults.
Various methods have been used to estimate therapeutic adherence. Indirect methods are the most commonly employed due to their simplicity and low cost, although they tend to overestimate adherence and are generally less reliable than direct methods.9,15 Currently, there is no single method capable of assessing all factors involved in adherence,14 and the most effective strategy to address non-adherence remains undefined.
Nowadays, electronic prescriptions in Spain plays a crucial role in evaluating adherence.16 In the Spanish National Health System, the primary source of data on outpatient prescriptions is pharmacy billing for officially dispensed medications.
Given that primary care is the cornerstone for managing patients with chronic conditions and functional limitations,7 it is necessary to conduct research in this field, to inform the development of effective and efficient strategies to improve medication adherence and enhance patient safety.
There is limited evidence regarding the level of adherence to medication among older adults with polypharmacy and its potential association with PIPs in primary care. This study aimed to assess medication adherence in older polypharmacy patients in primary care, and to describe their demographic, clinical, and pharmacological characteristics. It also explored potential associations between adherence, PIPs, and other contributing factors.
Materials and Methods
Settings and Design
This was a descriptive, observational study conducted in patients over 65 years of age with chronic diseases and polymedicated who were prescribed seven or more medications for a minimum of six months. The study was carried out in public primary care centres within the Toledo Health Area (Spain). The primary aim was to assess the level of adherence to prescribed pharmacological treatment and to explore whether non-adherence was associated with potentially inappropriate prescriptions (PIPs).
Adherence was evaluated by comparing the medications prescribed by physicians, as recorded in the patients’ electronic medical records, with data on dispensed medications from community pharmacies over the study period.
Inclusion Criteria
- Patients registered in the Public Primary Health Care Area of Toledo, Spain.
- Patients over the age of 65 who are receiving outpatient treatment.
- Patients who have been prescribed at least seven medications for a period of at least six months.
- Patients with electronic medical records and pharmacological prescriptions recorded in the in the computer programmes of Castilla-La Mancha Health Service (Sescam).
- Dispensing drugs at the request of patients by community pharmacy offices during the study period.
- Electronic pharmacy dispensing records available for the study period. These records include data on prescriptions dispensed and invoiced.
Exclusion Criteria
- Hospitalised patients, those in long-term care facilities, end-of-life or palliative care patients, and patients without an assigned general practitioner in the Toledo Health Area.
- Patients with incomplete or missing information in their electronic health records.
- Medications dispensed in hospitals, through private insurance, or without a prescription were excluded.
The study also excluded medical devices, magistral formulations of a medicinal products, enteral nutrition, over-the-counter medications, herbal and homeopathic products, and medications not reimbursed by the Spanish National Health System.
Data Collection and Procedure
Data were collected between August and September 2014 through a review of patients’ electronic medical records and pharmacy dispensing data.
A primary care pharmacist collected demographic data (age, sex, geographic location) and clinical information (chronic conditions and medications). The pharmacist compared the prescribed medications in the electronic health records with those actually dispensed by pharmacies, using official prescription billing data for the two-month study period. Any discrepancies were analysed.
The pharmacist also manually reviewed patients’ clinical records to assess medication adherence and identify PIPs, using the Beers and STOPP criteria.
Sources of Information
Data were obtained from:
- The Sescam electronic health record and prescription system.
- The prescription billing database.
- Information provided by the General Directorate of Care and Quality of Sescam.
- Identify PIPs, using the 2012 Beers Criteria4 and the 2008 STOPP Criteria,5 including the Spanish-adapted 2009 version of the latter.6
Outcome Measures
The primary outcome was the degree of adherence to pharmacological treatment. Non-adherence was assessed based on the number of medication packages that should have been collected from the pharmacy during the two-month study period (August–September 2014), as per electronic prescriptions.
To quantify adherence, the Proportion of Days Covered (PDC)15 was calculated:
- Numerator: Days for which medication was dispensed.
- Denominator: Total number of days in the study period (61 days).
- A PDC ≥80% was classified as adherent.
Only medications classified as chronic treatments were considered.
Secondary variables included:
- Demographic: Age, sex.
- Clinical: Presence of chronic diseases.
- Pharmacological: Medication details (active ingredient, dose, frequency, route of administration, formulation, pharmaceutical form and treatment duration).
- PIPs: Identified using the Beers and STOPP criteria.
Operational Definitions
- Polypharmacy was defined as the concurrent use of at least seven medications, and hyper-polypharmacy as the concurrent use of at least ten medications.17 Polypharmacy was defined as the concurrent use of at least seven medications, and hyper-polypharmacy as the concurrent use of at least ten medications. Data on pharmacological prescriptions were obtained and recorded, covering only the names of the of the active ingredient. The medications were classified according to the World Health Organization’s (WHO) Anatomical Therapeutic Chemical (ATC) Classification System.18
- Chronic medication: Treatments with a prescription duration of six months or more.
- Chronic diseases: Included hypertension, cardiovascular disease (ischemic heart disease, stroke, heart failure), diabetes, respiratory diseases (chronic obstructive pulmonary disease, asthma), osteoporosis, anxiety-depression disorders, schizophrenia, and Alzheimer’s disease and related dementias.
- Multimorbidity: Presence of two or more chronic conditions, classified per 11th revision of the International Classification of Diseases (ICD-11).19
- Therapeutic adherence: Defined as “the extent to which a person’s behaviour corresponds with agreed recommendations from a healthcare provider”.8
- Potentially Inappropriate Prescription (PIPs): A prescription where the risk of harm outweighs the benefit, or safer alternatives are available.4,5
Data Analysis
The sample size was calculated using the formula for infinite sample sizes for means, assuming a standard deviation of 1.5 and a precision of 0.15, with 95% confidence and a 5% alpha error. A minimum sample size of 385 was estimated, accounting for a 10% expected dropout rate. A total of 448 patients were ultimately included.
Data were analysed descriptively, using absolute and relative frequencies and 95% confidence intervals. A result was considered statistically significant if p < 0.05.
A random sample of 448 patients was drawn from the 2598 patients included in the main study, which evaluated pharmacists’ interventions in Primary Care to improve medication prescribing. Patient identities were anonymised, and only the principal investigator had access to identifiable information.
Data were recorded in a structured Microsoft Excel® sheet and analysed using Statistical Package for the Social Sciences© (SPSS) v17.0. Only the principal investigator had access to this information. The dataset included demographic, and clinical data, pharmacological information (ATC-coded drug names, number and types of PIPs per Beers and STOPP criteria), and adherence outcomes. The number of prescription packages was also recorded.
A mixed-methods approach was used: quantitative and qualitative analyses.
- Quantitative analysis: Means and standard deviations for continuous variables; frequencies and percentages for categorical variables.
- Qualitative analysis: Chi-square and Fisher’s exact tests for associations between categorical variables. Student’s t-tests or Mann–Whitney U-tests were used depending on the normality of quantitative data.
Ethical Statement
The research project was approved by the Primary Care Management of Toledo, and the study was reviewed and unanimously approved by the Clinical Research Ethics Committee (CEIm) of the Health Area of Toledo (Spain) (Clinical Research Ethics Committee of the University Hospital Complex of Toledo Approval No. 102; Date: 07 October 2013; at its meeting of 25 September 2013). Informed consent from patients was not required for the conduct of this study. All data were anonymised. Data confidentiality was agreed with the Health Service of Castilla-La Mancha (Sescam). The study was conducted in accordance with current legislation and ethical standards on confidentiality, privacy and data protection. This study did not involve any direct intervention by the investigator on the patient and does not involve any risk to the patients included in the study. The study was conducted in accordance with the ethical guidelines of the Declaration of Helsinki, Good Clinical Practice and local regulations. All records are de-identified and fully comply with patient confidentiality requirements. There are no ethical or legal issues or conflicts of interest.
Results
As of June 2014, a total of 434,547 individuals were enrolled in the healthcare system within the Toledo health district. Of these, 69,787 (16.1%) were aged 65 years or older, and 25,172 (5.8%) were taking seven or more medications. Overall, 36.1% of patients were both aged ≥65 and polymedicated.
Demographic, Clinical, and Pharmacology Characteristics
A total of 448 patients were included in the study. The mean age of the patients was 79.4 ± 7.6 years (range 66–103 years), with 175 (39.1%) male and 273 (60.9%) female participants.
Patients exhibited a high burden of comorbidity: 49.3% had six or more chronic conditions. The most prevalent chronic diseases were cardiovascular (91%), endocrine (58%), ophthalmological (52%), and musculoskeletal disorders (51%). The most common individual diagnoses were arterial hypertension (83.9%), dyslipidaemia (58.5%), and diabetes mellitus (48.9%). Additionally, 34.4% of patients presented with an anxiety-depressive syndrome, 15.0% with chronic kidney disease, 10.4% with cognitive impairment or dementia, and 11.6% with physical disability resulting in immobility.
In terms of pharmacological load, 67% of patients were prescribed 7–10 medications, while 33% were classified as having hiper-polypharmacy (more than 10 medications); 4.9% were taking 15 or more medications. A total of 4413 medications were prescribed during the study period, equating to an average of 9.9 ± 2.4 drugs per patient (range: 7–19).
The most frequently prescribed drug classes were those targeting the cardiovascular system (28.9%), nervous system (23.4%), and alimentary tract and metabolism (21.2%), which together accounted for 73.5% of all prescriptions. The most prescribed therapeutic subgroups were drugs for acid-related disorders (A02, 9.2%), analgesics (N02, 8.1%), antithrombotic agents (B01, 7.6%), and lipid-lowering agents (C10, 7.4%). Antidiabetic medications (A10) and agents acting on the renin-angiotensin system (C09) comprised 7.3% and 7.1% of prescriptions, respectively.
The most commonly prescribed chemical-therapeutic subgroups were A02BC (proton pump inhibitors, 8.8%), C10AA (statins, 6.3%), and B01AC (antiplatelet agents, 6.1%). Among individual drugs, omeprazole was prescribed to 58.3% of patients, acetylsalicylic acid to 49.8%, paracetamol monotherapy to 36.5%, simvastatin to 31.3%, atorvastatin to 24.3%, furosemide to 24.3%, lorazepam to 22.1%, and metamizole to 21.7%.
Therapeutic Adherence
Of the 448 patients included in the study, 160 (35.7%) were considered as non-adherent to their treatment, while 288 (64.3%) were considered adherent (see Table 1). Among non-adherent patients, 100 (62.5%) were female, compared to 173 (60.1%) in the adherent group.
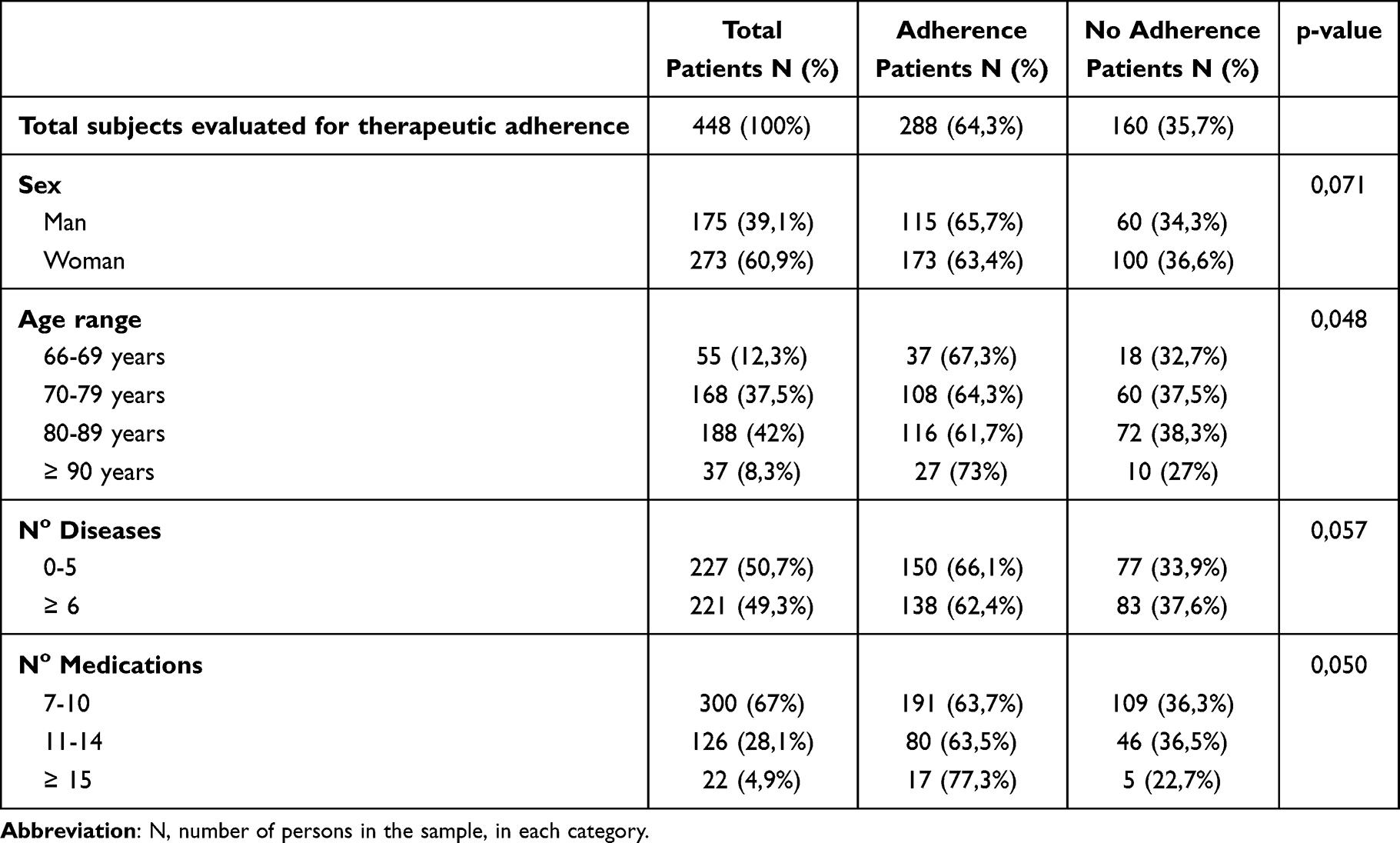 |
Table 1 Demographic and Clinical Variables of the Patients in the Study Related to Therapeutic Adherence and Statistical Significance |
Table 1 summarises the association between adherence and the demographic and clinical variables of the study population, along with their statistical significance.
Based on medication dispensation data from community pharmacies during the study period, 35.7% of patients were deemed non-adherent to the pharmacological treatment prescribed by their primary care physician. 36.6% of women compared to 34.3% of men did not adhere to the prescribed treatment. Adherence rates were slightly lower in women (63.4%) than men (65.7%), although the difference was not statistically significant (p = 0.071).
Age was significantly associated with adherence: patients aged ≥90 years had the highest adherence rates, with 73.0% demonstrating adherence levels above 80%. Similarly, patients prescribed ≥15 medications also showed high adherence: 77.3% of this group had adherence levels exceeding 80%. However, no statistically significant differences were observed between patients taking 7–10 versus 11–14 medications.
No statistically significant associations were found between adherence and sex, number of chronic conditions, or overall number of medications. However, the presence of specific conditions—dermatological (p = 0.031), musculoskeletal (p = 0.0035), respiratory (p = 0.031), neoplastic (p = 0.029), and renal diseases (p = 0.044)—was significantly associated with adherence.
Figures 1 and 2 illustrate the relationship between therapeutic adherence, number of chronic conditions, and number of medications.
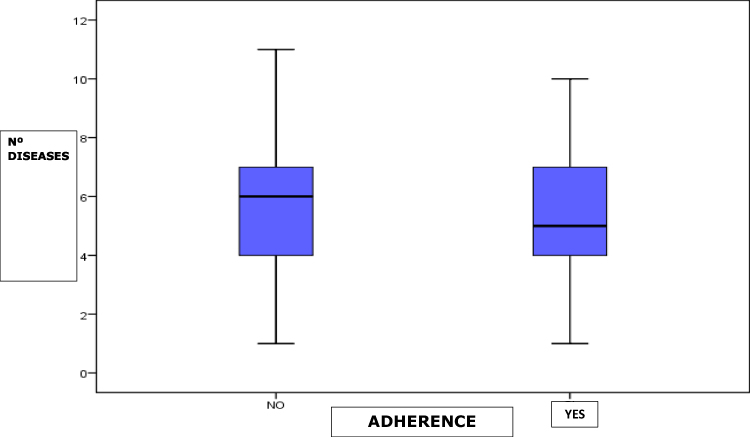 |
Figure 1 Relationship between therapeutic adherence and the number of diseases of the study. (See attached document). |
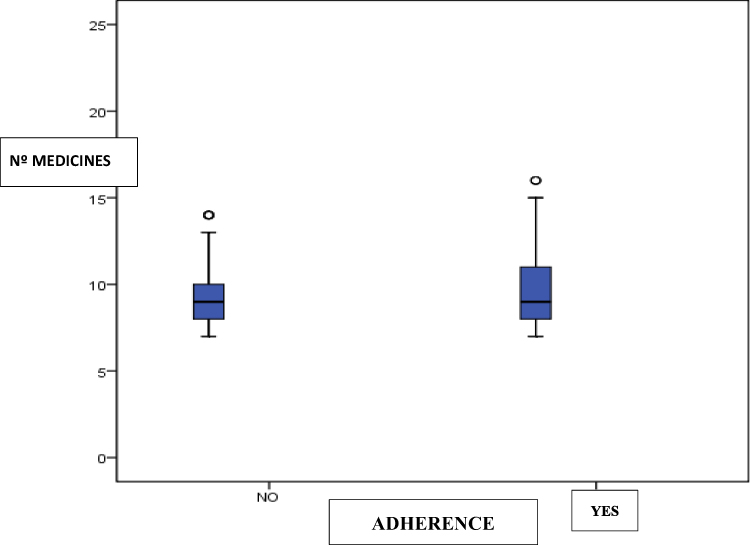 |
Figure 2 Relationship of therapeutic adherence with the number of medications. (See attached document). |
Potentially Inappropriate Prescriptions (PIPs)
Potentially inappropriate prescriptions were identified in 43.1% of patients using the Beers 2012 criteria and in 43.8% using the STOPP 2008 criteria. Interestingly, inappropriate prescribing was less common among patients with poor adherence than among adherent patients. Among those with adequate adherence (≥80%), 44.1% had PIPs according to the Beers criteria and 45.8% according to the STOPP criteria.
PIPs identified via the Beers criteria primarily involved medications affecting the cardiovascular, endocrine, and musculoskeletal systems. Those identified by the STOPP criteria were most frequently related to the central nervous system (eg, benzodiazepines and neuroleptics) and the cardiovascular system.
Table 2 presents the bivariate analysis of therapeutic adherence in relation to the study variables.
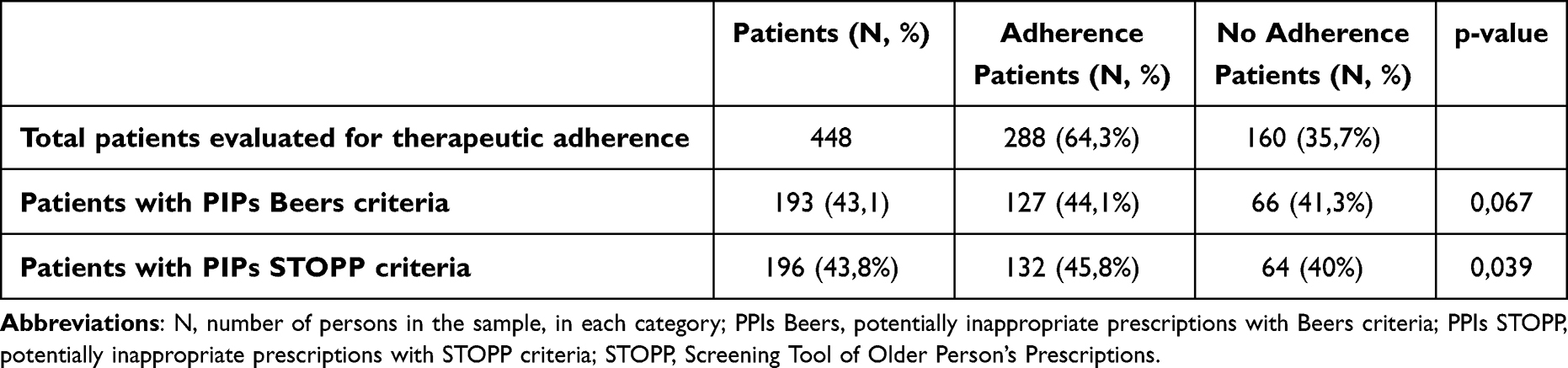 |
Table 2 Study Variables Related to Therapeutic Adherence and Statistical Significance |
Relationship Between PIPs and Adherence
A statistically significant association was observed between the presence of any PIPs (according to the STOPP 2008 criteria) and treatment adherence (p = 0.039). However, no significant association was found between adherence and PIPs identified by the Beers 2012 criteria (p = 0.067) or the prescription of drugs considered to have low therapeutic value (p = 0.093).
Discussion
Study Overview
This study was conducted among community-dwelling older adults. We analysed pharmacotherapy patterns and the degree of treatment adherence in polymedicated patients aged over 65 years who had been prescribed at least seven chronic medications (with a treatment duration of ≥6 months) and who presented with multiple morbidities within the Toledo Primary Care Area.
A total of 448 patients were included, with a mean age of 79 years; 60.9% were female. Notably, 49.3% had six or more chronic conditions. Sixty-seven percent of patients were prescribed between 7 and 10 medications, while 33% received prescriptions consistent with hyper-polypharmacy (ie more than 10 drugs). The mean number of prescribed medications per patient was 9.9, which matched the average number of medications dispensed per patient during the study period, suggesting that patients collected the prescribed treatments during the evaluation timeframe.
Therapeutic Adherence
Studies evaluating therapeutic adherence have reported highly variable results, attributable to differences in populations, disease types, clinical settings, healthcare systems, and methodological approaches. Numerous factors influence adherence.14,20–23 In our study, 64.3% of patients demonstrated adherence rates of ≥80%, though it is important to consider that adherence was measured indirectly, based on pharmacy dispensing data. Published adherence rates vary widely: 43.2% in private clinics,24 49% in urban health centres,25 51.7% in public primary healthcare centres26 and 61.1% in hospitals.25 Higher rates have also been reported: 77.8%27 and 79.7%28 among polymedicated patients in health centres; 86% in hospital hypertension units;29 and 93.8% in patients over 75 years in primary care.30 Prevalence estimates also vary depending on the measurement method: 15.6% using the Batalla test; 34.6% using pill count (in patients with hypertension and diabetes); and 76.8% using the Morinsky-Green test.31
In our study, adherence was significantly higher among older patients (p = 0.048), with the highest level observed in those aged ≥90 years (73%). Other authors have also found increased adherence among older adults, particularly those aged 71–85 years,1,25,32 although some studies have reported the opposite.33 Still other found no significant association between demographic and clinical variables and drug adherence.34
Adherence was slightly higher in men (65.7%) than women (63.4%), though the difference was not statistically significant (p = 0.071). As with age, the literature on gender differences in adherence is inconsistent.25
No statistically significant associations were observed between adherence and the number of chronic conditions or medications. Adherence rates are known to vary by condition; for example, non-adherence rates of up to 75% have been reported in psychiatric disorders, 70% in asthma, 50% in patients with arterial hypertension, diabetes and dyslipidaemia, and 30% in acute conditions.35 However, in our study, certain clinical conditions were significantly associated with adherence: dermatological disease (p = 0.031), musculoskeletal disease (p = 0.0035), pulmonary disease (p = 0.031), neoplasms (p = 0.029) and renal failure (p = 0.044).
Regarding polypharmacy, no statistically significant correlation was found between the number of prescribed medications and adherence (p = 0.050). Some studies suggest that polypharmacy may improve adherence,36 while others have found that it negatively impacts it.37–39
A systematic review noted that advanced age, polypharmacy, comorbidities, and adverse drug reactions are associated with poorer adherence.40–43
In our study, 64.3% of patients were classified as adherent (adherence ≥80%), which is higher than the commonly cited average of 50% in patients with chronic conditions.8,9 One primary care study using the eight-item Morisky-Green scale reported that 49% of patients aged ≥65 had optimal adherence, with men adhering more than women.25 Among those taking 6–10 medications, 36% were adherent; this increased to 42% in those taking >10 medications.25 Another primary care study using the Morisky-Green-Levine questionnaire found adherence in 55.5% of patients.1 In a separate study in Badajoz, Spain, involving polymedicated patients over 65 years taking ≥5 drugs, 77.8% were adherent based on the Morisky-Green test.27
The variability in findings across studies reflects the complexity of medication adherence, which is influenced by a broad range of factors, including patient knowledge and attitudes, family and socioeconomic context, and relationships with healthcare professionals (physicians, nurses, and pharmacists).43–45
Potentially Inappropriate Prescriptions (PIPs)
The study population was at high risk for inappropriate prescribing, given their advanced age, multimorbidity, and polypharmacy. We therefore assessed whether therapeutic adherence was associated with the presence of potentially inappropriate prescriptions (PIPs), using the Beers (2012) and STOPP (2008) criteria—tools familiar to local primary care providers.46 PIPs were identified in 43.1% of patients based on the Beers criteria and in 43.8% based on the STOPP criteria (2008 version and 2009 Spanish adaptation). Beers-related PIPs primarily involved medications targeting the cardiovascular, endocrine, and musculoskeletal systems. The most frequent STOPP-related PIPs involved central nervous system drugs (eg benzodiazepines and neuroleptics) and cardiovascular agents. These findings are consistent with those of other studies examining PIPs in older, polymedicated populations.47,48 Interestingly, PIPs were more prevalent among adherent patients; however, this association was only statistically significant when using the STOPP criteria (p = 0.039). No significant differences were found when PIPs were identified using the Beers criteria (p = 0.067). While some studies similarly found no clear relationship between inappropriate prescribing and adherence, others observed a trend towards higher rates of PIPs among non-adherent patients.30
To our knowledge, no prior studies have jointly addressed polypharmacy, adherence, and potentially inappropriate prescribing in individuals over 65 years of age. These interrelated factors are particularly relevant in this age group, making this study a novel and important contribution.
Strengths and Limitations
Strengths of the study include a robust sample size of 448 patients across 30 health centres, allowing for detailed statistical analysis. Additionally, the simultaneous examination of polypharmacy, adherence, and PIPs in older adults represents a unique and previously unexplored area in the literature.
Limitations include the indirect method of assessing adherence (via pharmacy dispensing data), which may not accurately reflect actual medication intake. Adherence may also vary over time, and the relatively short two-month study period may have limited the detection of statistically significant associations. Another limitation is the use of a pharmacy billing system that lacks diagnostic codes and contextual clinical information relevant to understanding adherence behaviours. Moreover, some statistical tests were conducted without adjusting p-values for multiple comparisons, increasing the likelihood of Type I error. This increases the risk of chance findings. This is a serious limitation.
Finally, as an observational study, the findings should be interpreted with caution and may not be generalisable to other healthcare settings.
Conclusion
Adherence rates of ≥80% were observed in 64.3% of patients, while the prevalence of potentially inappropriate prescribing remained high—44.0% according to the STOPP criteria and 42.6% according to the Beers criteria. However, no statistically significant association was found between therapeutic adherence and inappropriate prescribing.
No significant differences in adherence were observed by sex, number of chronic conditions, or number of prescribed medications. However, patient age was significantly associated with adherence. In addition, therapeutic adherence showed statistically significant associations with the presence of dermatological, musculoskeletal, pulmonary, neoplastic, and renal diseases.
Further research is warranted to better understand the clinical consequences of potentially inappropriate medication use in older patients with polypharmacy.
An interdisciplinary, multifactorial pharmaceutical intervention may help improve adherence among older adults with polypharmacy and potentially inappropriate prescriptions. Such interventions could include educational programmes for prescribers and patients, along with regular, personalised medication reviews.
Abbreviations
ATC, Anatomical, Therapeutic, Chemical Classification System; ICD, International Classification of Diseases; CI, Confidence interval; PDC, Proportion of days covered with prescription; PIP, Potentially inappropriate prescriptions; Sescam, Health Service of Castilla-La Mancha; SNHS, Spanish National Health System; SPSS, Statistical Package for the Social Sciences©; STOPP, Screening Tool of Older Person’s Potentially Inappropriate Prescriptions; WHO, World Health Organization.
Acknowledgments
We would like to thank the Primary Care Management of Toledo, the University of Granada, and all those involved in the doctoral programme in Social Pharmacy for their support.
Disclosure
All authors declare that the research was conducted independently of any commercial or financial relationships that could be perceived as a potential conflict of interest.
References
1. Fernández-Lázaro CI, García-González JM, Adams DP, et al. Adherence to treatment and related factors among patients with chronic conditions in primary care: a cross-sectional study. BMC Fam Pract. 2019;20(1):132. doi:10.1186/s12875-019-1019-3 Spanish.
2. Religioni U, Barrios-Rodríguez R, Requena P, Borowska M, Ostrowski J. Enhancing therapy adherence: impact on clinical outcomes, healthcare costs, and patient quality of life. Medicina. 2025;61(1):153. doi:10.3390/medicina61010153
3. Abdelwahed AA, El-Dahiyat F, Aljawamis D, Al Ajimi J, Bin Rafeea KJ. Potentially inappropriate medications in older adults according to Beers criteria 2019: prevalence and risk factors. Int J Clin Pract. 2021;75(11):e14715. doi:10.1111/ijcp.14715
4. The American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society. The American updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2012;60:616–631. doi:10.1111/j.1532-5415.2012.03923.x
5. Gallagher P, Ryan C, Byrne S, Kennedy J, O’ Mahony D. STOPP (Screening-Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther. 2008;46:72–83. doi:10.5414/cpp46072
6. Delgado E, Muñoz M, Montero B, Sánchez C, Gallagher PF, Cruz-Jentoft A. Prescripción inapropiada de medicamentos en los pacientes mayores: los criterios STOPP/START [Inappropriate prescription in older patients: the STOPP/START criteria]. Rev Esp Geriatr Gerontol. 2009;44(5):273–279. doi:10.1016/j.regg.2009.03.017 Spanish.
7. Ferrer C, Orozco D, Román P. Estrategia para el Abordaje de la Cronicidad en el Sistema Nacional de Salud [Internet] [Strategy for Addressing Chronicity in the National Health System]. Strategy approved by the Interterritorial Council of the National Health System (NHS) on 27 June 2012. Ministerio de Sanidad Servicios Sociales e Igualdad; 2012. España. Spanish. Available from: https://www.sanidad.gob.es/areas/calidadAsistencial/estrategias/abordajeCronicidad/docs/Resumen_Ejecutivo_Estrategia_Abordaje_Cronicidad_ENGLISH_02.pdf.
8. Sabaté E. Adherence to Long-Term Therapies: Evidence for Action. Geneva, Switzerland: WHO, World Health Organization; 2003. doi:10.1111/j.1547-5069.2003.tb00001.x
9. Palop Larrea V, Martínez Mir I. Adherencia al tratamiento en el paciente anciano [Adherence to treatment in the elderly patient]. Inf Ter Sist Nac Salud. 2004;28(5):113–120. Spanish.
10. Taghy N, Cambon L, Cohen JM, Dussart C. Failure to reach a consensus in polypharmacy definition: an obstacle to measuring risks and impacts-results of a literature review. Ther Clin Risk Manag. 2020;11(16):57–73. doi:10.2147/TCRM.S214187
11. Kvarnström K, Westerholm A, Airaksinen M, Liira H. Factors contributing to medication adherence in patients with a chronic condition: a scoping review of qualitative research. Pharmaceutics. 2021;13(7):1100. doi:10.3390/pharmaceutics13071100
12. Gavilán Moral E, Villafaina Barroso A. Pacientes polimedicados frágiles, un reto para el sistema sanitario [Frail polymedicated patients, a challenge for the health system]. Inf Ter Sist Nac Salud. 2011;35:114–123. Spanish.
13. Payero M Á, Martínez López de Castro N, Ucha Samartín M, Martín Vila A, Vázquez López C, Piñeiro Corrales G. Medication non-adherence as a cause of hospital admissions. Farm Hosp. 2014;38(4):328–333. [Spanish]. doi:10.7399/FH.2014.38.4.7660
14. Lorenzo Garmendia A, Pereira Expósito A, Valdésy Llorca C, et al. Proyecto ADHER: libro Blanco de la Adherencia en España [ADHER Project: white Paper on Adherence in Spain]. 2022. Grup OAT y Fundation Weber. ISBN OAT: 978-84-09-47302-1 ISBN Weber: 978-84-124939-4-8. Spanish. Available from: https://www.oatobservatorio.com/wp-content/uploads/2023/02/17.20220404.Proy-Adher.LB_Version-digital-OK.pdf.
15. Orozco-Beltrán D, Carratalá-Munuera C, Gil-Guillén V. Mejorar la adherencia: una de las acciones más eficientes para aumentar la supervivencia de los pacientes en prevención secundaria [Improving Treatment Adherence: one of the Most Effective Ways of Increasing Patient Survival in Secondary Prevention]. Rev Esp Cardiol Supl. 2015;15(E):12–18. doi:10.1016/S1131-3587(16)30004-8.
16. Vejdani M, Meraji M, Varmaghani M, Jamali J, Hooshmand E, Vafaee-Najar A. Electronic prescription system requirements: a scoping review. BMC Med Inform Decis Mak. 2022;22(1):231. doi:10.1186/s12911-022-01948-w
17. Masnoon N, Shakib S, Kalisch-Ellett L, et al. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017;17(1):230. doi:10.1186/s12877-017-0621-2
18. World Health Organization (WHO). WHO Collaborating Centre for Drug Statistics Methodology. ATC index. Available from: http://www.whocc.no/atcdddindex/.
19. Harrison JE, Weber S, Jakob R, Chute CG. ICD-11: an international classification of diseases for the twenty-first century. BMC Med Inf Decis Mak. 2021;21(6):1–10.
20. Lyles A, Culver N, Ivester J, Potter T. Effects of health literacy and polypharmacy on medication adherence. Consult Pharm. 2013;28(12):793–799. doi:10.4140/TCP.n.2013.793
21. Patton DE, Cadogan CA, Ryan C, et al. Improving adherence to multiple medications in older people in primary care: selecting intervention components to address patient-reported barriers and facilitators. Health Expect. 2018;21(1):138–148. doi:10.1111/hex.12595
22. Moreno Juste A, Gimeno Miguel A, Poblador Plou B, et al. Adherencia al tratamiento de hipertensión arterial, hipercolesterolemia y diabetes en población anciana de una cohorte española [Adherence to treatment of hypertension, hypercholesterolaemia and diabetes in an elderly population of a Spanish cohort]. Med Clín. 2018;153(1):1–5.
23. Cebrián-Cuenca AM, Villar-Taibo R, Bellido V, Pinés-Corrales PJ. Consecuencias de la inadecuada adherencia terapéutica en diabetes mellitus y propuestas de mejora [Consequences of the poor therapeutic adherence in diabetes mellitus and improvement recommendations]. Aten Primaria Práctica. 2024;6(4):100207. doi:10.1016/j.appr.2024.100207 ISSN 2605-0730. Spanish.
24. Park KA, Kim JG, Kim BW, et al. Factors that affect medication adherence in elderly patients with diabetes mellitus. Korean Diabetes J. 2010;34(1):55–65. doi:10.4093/kdj.2010.34.1.55
25. Calles Artiaga C. Estudio de la adherencia terapéutica en el paciente crónico mayor de 65 años en un centro de salud urbano [Study of therapeutic adherence in chronic patients over 65 years of age in an urban health center] [dissertation]. Final Degree Project. Course 2020 - 2021. Accra: university of Valladolid. Spanish. Available from: https://uvadoc.uva.es/handle/10324/47397.
26. Group P, Núñez Montenegro AJ, Montiel Luque A, et al. Adherencia al tratamiento en pacientes polimedicados mayores de 65 años con prescripción por principio activo [Adherence to treatment, by active ingredient, in patients over 65 years on multiple medication]. Aten Primaria. 2014;46(5):238–245. doi:10.1016/j.aprim.2013.10.003 Spanish.
27. Lorido Cano I, Hernanz Arroyo B, Cordero Sánchez E, González Huéscar A, Menaya Macías RG, Jesús Gómez Encinas J. Adherencia terapéutica en pacientes polimedicados y factores condicionantes en un grupo de pacientes de Badajoz, España [Therapeutic adherence in Polymedicated Patients and Conditioning Factors in a Group of Patients from Badajoz, Spain]. Arch de Med Fam. 2019;21(2):51–59. Spanish.
28. Ordóñez Arcau A, Miranda Ugarte I, Máñez Giménez A, Gómez Moreno S, Fanlo Colás A, Gimeno Zarazaga J. Adherencia al tratamiento en pacientes polimedicados mayores de 65 años por nivel socioeconómico [Treatment adherence in polymedicated patients over 65 years of age by socioeconomic level]. RSI. Revista Sanitaria de Investigación [Health Research Journal] Abril 2021. Spanish. Available from: https://www.revistasanitariadeinvestigacion.com/adherencia-al-tratamiento-en-pacientes-polimedicados-mayores-de-65-anos-por-nivel-socioeconomico.
29. Fernández Vázquez N, García Zurita A, Felipez Agrelo IM, Castro Dios DJ, Remuiñán Rodríguez B. Factores relacionados en la adherencia terapéutica en pacientes a tratamiento hipertensivo [The prescription of active ingredient influences in the farmacological adherence]. Evidentia. 2019;16:1. Spanish.
30. Rivera Plaza L. Prescripción inadecuada de fármacos y su relación con el cumplimiento terapéutico en pacientes polimedicados [Inappropriate prescription and its relationship with adherence to therapeutic plan in polymedicated patients. Gerokomos. 2018;29(3):123–127. Spanish.
31. García Pérez AM, Prados Torres D, Sánchez de la Cuesta F. Cumplimiento terapéutico en pacientes con hipertensión arterial y diabetes mellitus tipo 2 [Therapeutic compliance in patients with arterial hypertension and type 2 diabetes mellitus. Semergen. 2004;30(2):55–59. [Spanish]. doi:10.1016/S1138-3593(04)74275-6
32. Rubio Fernández E, Rosino Bosch A, Fajas Argemi R, Manresa Domínguez J, Martínez Momblan M, Torres Quintana A. Medición del incumplimiento terapéutico en el paciente crónico complejo y modelo de atención cronicidad avanzada en dos centros de urgencias de atención primaria de la provincia de Barcelona. ROL Revista Rol de Enfermería [Nursing Role Magazine]. 2019;42(4):279–284. Spanish.
33. Jansà M, Hernández C, Vidal M, et al. Multidimensional analysis of treatment adherence in patients with multiple chronic conditions. A cross-sectional study in a tertiary hospital. Patient Educ Couns. 2010;81(2):161–168. [Spanish]. doi:10.1016/j.pec.2009.12.012
34. Bastani F, Haghani H, Maleki M. Evaluation of drug adherence in older adults with polypharmac. JHNM. 2024;34(3):201–210. doi:10.32598/jhnm.34.3.2507
35. Rigueira García A. Cumplimiento terapéutico: qué conocemos de España? [Treatment compliance: what do we know about Spain?]. Aten Primaria. 2001;27(8):559–568. doi:10.1016/s0212-6567(01)78860-9 Spanish.
36. Rozenfeld Y, Hunt JS, Plauschinat C, Wong KS. Oral antidiabetic medication adherence and glycemic control in managed care. Am J Manag Care. 2008;14(2):71–75.
37. Vermeire E, Hearnshaw H, Van Royen P, Denekens J. Patient adherence to treatment: three decades of research. A comprehensive review. J Clin Pharm Ther. 2001;26(5):331–342. doi:10.1046/j.1365-2710.2001.00363.x
38. Nishimura R, Kato H, Kisanuki K, et al. Treatment patterns, persistence and adherence rates in patients with type 2 diabetes mellitus in Japan: a claims-based cohort study. BMJ Open. 2019;9:e025806. doi:10.1136/bmjopen-2018-025806
39. Calderón-Larrañaga A, Diaz E, Poblador-Plou B, Gimeno-Feliu LA, Abad-Díez JM, Prados Torres A. Non-adherence to antihypertensive medication: the role of mental and physical comorbidity. Int J Cardiol. 2016;207:310–316. doi:10.1016/j.ijcard.2016.01.069
40. Conthe P, Márquez Contreras E, Aliaga Pérez A, et al. Adherencia terapéutica en la enfermedad crónica: estado de la situación y perspectiva de futuro [Treatment compliance in chronic illness: current situation and future perspectives]. Rev Clin Esp SEGO. 2014;214(6):336–344. [Spanish]. doi:10.1016/j.rce.2014.03.008
41. Lee CY, Huang CC, Shih HC, Huang KH. Factors influencing antihypertensive medication compliance in Taiwan: a nationwide population-based study. Eur J Prev Cardiol. 2013;20(6):930–937. doi:10.1177/2047487312451252
42. McGovern A, Hinton W, Calderara S, Munro N, Whyte M, de Lusignan S. A class comparison of medication persistence in people with type 2 diabetes: a retrospective observational Study. Diabetes Ther. 2018;9(1):229–242. doi:10.1007/s13300-017-0361-5
43. Saadat Z, Nikdoust F, Aerab-Sheibani H, et al. Adherence to antihypertensives in patients with comorbid condition. Nephrourol Mon. 2015;7(4):e299863. doi:10.5812/numonthly.29863
44. Kardas P, Lewek P, Matyjaszczyk M. Determinants of patient adherence: a review of systematic reviews. Front Pharmacol. 2013;4(91). doi:10.3389/fphar.2013.00091
45. Menditto E, Cahir C, Aza-Pascual-Salcedo M, et al. Adherence to chronic medication in older populations: application of a common protocol among three European cohorts. Patient Prefer Adherence. 2018;12:1975–1987. doi:10.2147/PPA.S164819
46. Galván-Banqueri M, Santos-Ramos B, Vega-Coca MD, Alfaro-Lara ER, Nieto-Martóin MD, Pérez-Guerrero C. Adecuación del tratamiento farmacológico en pacientes pluripatológicos [Suitability of pharmacological treatment in patients with multiple chronic conditions]. Atención Primaria. 2012;45(1):6–18. doi:10.1016/j.aprim.2012.03.011 Spanish.
47. Nuñez-Montenegro A, Montiel-Luque A, Martin-Aurioles E, Garcia-Dillana F, Krag-Jiménez M, González-Correa JA. Evaluation of inappropriate prescribing in patients older than 65 years in primary health care. J Clin Med. 2019;8(3):305. doi:10.3390/jcm8030305
48. Inzitari M, Merino Méndez R, Santaeugenia S, et al. Prescripción potencialmente inadecuada en dos centros sociosanitarios según los criterios START-STOPP [Potentially inappropriate prescription in two social-health centres according to START-STOPP criteria]. Barcelona: agència de Qualitat i Avaluació Sanitàries de Catalunya. Departament de Salut. Generalitat de Catalunya; 2017 (Informes de Evaluación de Tecnologías Sanitarias). Spanish. Available from: https://aquas.gencat.cat/web/.content/minisite/aquas/publicacions/2017/prescripcion_sociosanitarios_START-STOPP_Red_aquas2017.pdf.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Observational Cohort Study to Evaluate the Impact of a Tailored Medicines Optimisation Service on Medication Use, Accident and Emergency Department Visits, and Admissions Among Patients Identified with Medication Support Needs in Secondary Care
Harrap N, Wells J, Howes K, Kayyali R
Patient Preference and Adherence 2022, 16:2947-2961
Published Date: 28 October 2022
What Do Seniors Believe About Medication Adherence? A Qualitative Study Among Seniors with Chronic Conditions in Yogyakarta, Indonesia
Widyakusuma NN, Suryawati S, Wiedyaningsih C, Probosuseno
Patient Preference and Adherence 2023, 17:1381-1392
Published Date: 8 June 2023
Suitability of Measures of Pharmacy-Based Medication Adherence for Routine Clinical Use Among Patients with Chronic Diseases: A Systematic Review
Jannah W, Khoiry QA, Alfian SD, Abdulah R
Patient Preference and Adherence 2025, 19:265-278
Published Date: 30 January 2025
Prevalence of Multiple Chronic Conditions in Older Adults with Undiagnosed Mild Cognitive Impairment and Alzheimer’s Disease and Related Dementias in Primary Care
Summanwar D, Owora AH, Ben Miled Z, Dexter PR, Kulshreshtha A, Strunk S, Jiang B, Coppedge K, Disla S, Galvin JE, Boustani M, Fowler NR
Clinical Interventions in Aging 2025, 20:1799-1809
Published Date: 24 October 2025
Implementation and Evaluation of a Real-Time Prescription Alert System to Optimize Antiretroviral Therapy and Medication Adherence in People Living with HIV. SANPAT PROJECT
Morillo-Verdugo R, Solis-Martin C, Marquez-Saavedra E, Robustillo-Cortes MDLA, Romero Gil E, Contreras-Macias E
Patient Preference and Adherence 2025, 19:3493-3508
Published Date: 7 November 2025