Back to Journals » Patient Preference and Adherence » Volume 17
What Do Seniors Believe About Medication Adherence? A Qualitative Study Among Seniors with Chronic Conditions in Yogyakarta, Indonesia
Authors Widyakusuma NN ![]() , Suryawati S, Wiedyaningsih C, Probosuseno
, Suryawati S, Wiedyaningsih C, Probosuseno
Received 17 March 2023
Accepted for publication 25 May 2023
Published 8 June 2023 Volume 2023:17 Pages 1381—1392
DOI https://doi.org/10.2147/PPA.S412981
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Niken Nur Widyakusuma,1,2 Sri Suryawati,1 Chairun Wiedyaningsih,2 Probosuseno1
1Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia; 2Faculty of Pharmacy, Universitas Gadjah Mada, Yogyakarta, Indonesia
Correspondence: Niken Nur Widyakusuma, Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada, Jl. Farmako Sekip Utara, Yogyakarta, 55281, Indonesia, Tel +62 274 560300, Fax +62 274 581876, Email [email protected]
Purpose: This qualitative study elicited beliefs about medication adherence among hypertensive seniors with polypharmacy.
Methods: Twenty-one participants aged 60 or older with hypertension and other chronic conditions, with or without their family caregivers, residing surrounding Yogyakarta province, using five medicines or more routinely, were semi-structuredly interviewed by one researcher or one research assistant in January to April 2022. Behavioral, normative, and control beliefs were elicited using an interview guideline which was developed based on the Theory of Planned Behavior approach. Thematic analysis was applied.
Results: The participants believed that taking medicines routinely was advantageous because the medicines kept their body in good condition and prevented disease worsening. However, there were concerns about the medications’ harmful effects on kidneys, gastric, and the whole body, and that the medicines would not be effective anymore. Prescribers, family, and friends would likely approve of medication adherence. However, non-prescriber doctors, family, and neighbors, mainly those with experience with complementary/alternative medicines, would likely disapprove of medication adherence. Good physical and cognitive function, help from family and technology, mealtime regularity, a simple regimen and easy-to-read medication labeling, and good communication with prescribers were among the facilitators of medication adherence. Physical and cognitive decline, mealtime irregularity, tablets that must be cut before taken, insurance that does not cover all medicines, change in dosage regimen, and hard-to-tear-off medication packaging were among the barriers to medication adherence.
Conclusion: Understanding these beliefs yields insights into the health communication approaches to improving seniors’ medication adherence.
Keywords: polypharmacy, medication adherence, theory of planned behavior
Introduction
Indonesia entered an aging population era in 2020, marked by the percentage of people aged 60 and older reaching 10% of the total population.1 This demographic transition results in a shift of disease patterns from infectious diseases to non-communicable diseases. In Indonesia, 63.2% of people aged 65–74 suffer from hypertension.2 At that age, about 26% have two morbidities, and 33% have three morbidities. The most common are hypertension and diabetes mellitus, chronic hypertension and stroke, and hypertension and chronic ischemic heart disease.3 Meanwhile, in Yogyakarta, an Indonesian province with the highest population of seniors,4 the prevalence of hypertension is 11.01% or higher than the national figure, where hypertension is 8.8%.5
Unfortunately, the adherence to hypertension treatment among seniors in Indonesia and some Asian countries tends to be low,6–8 probably because they often have several health conditions which require polypharmacy and might suffer from potential cognitive deficits. Non-adherence and misuse of medications may result in undesirable outcomes, such as lack of drug efficacy, emergency visits, hospitalizations, low quality of life, or increased healthcare costs.9,10
Understanding the underlying reason for non-adherence is essential to improve medication adherence. Many factors, such as patient-related factors, condition-related factors, therapy-related factors, healthcare provider factors, system-based factors, and socioeconomic factors, influence medication adherence.11–14 Horne and Weinman showed that medication beliefs are associated with medication adherence and may offer greater predictability than other clinical or social factors.15
It was also known that medication beliefs differ among cultural groups. Beliefs about the disease, approach to self-management, and medications can be influenced by culture, family experiences, and individual preferences.16 Patients who had stronger beliefs in the effectiveness of traditional Chinese medication were found to be less adherent to self-management and medication.17,18 A study in Saudi Arabia found that people who perceived that God controls their health and illness have good medication adherence. Meanwhile in Indonesia, since beliefs underlying medication adherence among hypertensive seniors were scarcely studied, we aimed to elicit beliefs about medication adherence among hypertensive seniors with polypharmacy.
Materials and Methods
Study Approach and Reporting
A qualitative study with phenomenology approach was conducted to elicit the beliefs about medication adherence among polypharmacy seniors using the Theory of Planned Behavior (TPB) framework. This study is reported according to the Consolidated criteria for Reporting Qualitative research (COREQ) checklist to enhance the transparency of the study approach, execution, analysis, and reporting of research data,19 (Supplementary File 1).
Study Participants and Sampling Strategy
We semi-structuredly interviewed seniors aged 60 and older with hypertension and chronic conditions who lived at home and took five prescribed medicines or more routinely. We purposively recruited seniors with a wide variety of background (age, education level, urban/rural area of living, living arrangement, number of daily medicines used, and duration of the disease) to see whether this background variation also shows a variation in the beliefs expressed. Participants were recruited from two locations: one community pharmacy in Yogyakarta, which serves a national referral program (Program Rujuk Balik), and one pharmacy in a type-A hospital in Yogyakarta, which provides a geriatric clinic service. Yogyakarta is considered as the province with the highest percentage of the senior population in Indonesia and covers urban and rural areas. Pharmacists at these institutions indicated which patients met the inclusion criteria. Patients with communication barriers were excluded from the study.
Instrument and Data Collection
A semi-structured interview guide was constructed based on TPB framework.20 According to this theory, behavior is guided by three kinds of considerations: beliefs about the advantages and disadvantages of doing the behavior (behavioral beliefs), beliefs about the normative expectations and behaviors of significant others (normative beliefs), and beliefs about the factors that may facilitate or impede doing the behavior (control beliefs).21 The interview guide therefore consisted of questions about the advantages and disadvantages of taking medications routinely as prescribed, the individuals or groups who would think that participants should and should not take medications routinely as prescribed, and the circumstances that enable and prevent participants from taking the medication routinely as prescribed. The guide was created in Bahasa Indonesia and Javanese since seniors around Yogyakarta province were more accustomed to speak in Javanese and it was considered politer. However, sometimes it is more convenient for the younger family to speak in Bahasa Indonesia. The researcher and research assistant piloted the interview guide to the first two participants.
The interviewers were either NNW as the researcher (a female medical Ph.D. student with a pharmacy background) or a research assistant (a female B. Pharm pharmacist with approximately five years of experience in the community). Both have been involved in some qualitative studies in recent years. A short briefing of approximately 30 minutes was conducted to prepare the research assistant for interview techniques before the data collection. The translation of Bahasa Indonesia to Javanese was done directly and spontaneously at interview sites based on the interviewer’ consideration who can speak both languages. In approaching participants, the interviewer informed the patients about the study and invited them to participate. No relationship was established with participants before study commencement. All patients who consented to participate were interviewed face-to-face.
Data were collected between January to April 2022 in the study sites or the patients’ homes based on the participant’s preferences, and a family member could be present at the interview. The interviews were audio-recorded, and each interview lasted for about 25 minutes until one hour. During the interviews, the interviewers could make notes and take photographs. Data was considered saturated when we found a repetition of categorization in the data analysis.
Ethics Approval
The study was conducted according to the principles outlined in the Declaration of Helsinki.22 Information for participants was explained, and written informed consent was collected from all participants. Informed consent included voluntary participation, confidentiality, and publication of anonymized responses. The questions and approach to sampling were approved by the Medical and Health Research Ethics Committee at Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada, with reference number KE/FK/1299/EC/2021. Given local cultural expectations, a paper bag containing a face mask and hand sanitizer was given as a small gift to each participant on completion of the interview.
Data Analysis
Interviews were transcribed verbatim and checked against the audio recording for accuracy. The interviewers’ field notes and photographs were added to provide better contextual information and enhance interpretation. Thematic analysis23 was applied to the data in Bahasa Indonesia or Javanese before the data was translated to English. Potential meaning units were searched from each line of the transcripts. From these meaning units, codes were then generated. The codes can be added, reduced, changed, or merged according to the addition of new transcript data. These codes were then reorganized into sub-themes and themes that have been pre-determined into behavioral, normative, and control beliefs of medication adherence (deductive approach) by three data coders. Quotations that illustrate these themes are provided. Additions to words were placed in square brackets to facilitate understanding of the quotations. A qualitative research software NVivo12® was used to track the coding and manage the data.
Results
In total, 27 people were approached to participate in the study, but only 21 were interviewed (Table 1). Four people did not participate because their family members were busy, were in a rush, or left contact numbers but had yet to respond when being contacted. Two other people were found to be in the end stage of stroke; thus, we could not assess their beliefs and did not take any data from their families or caregivers.
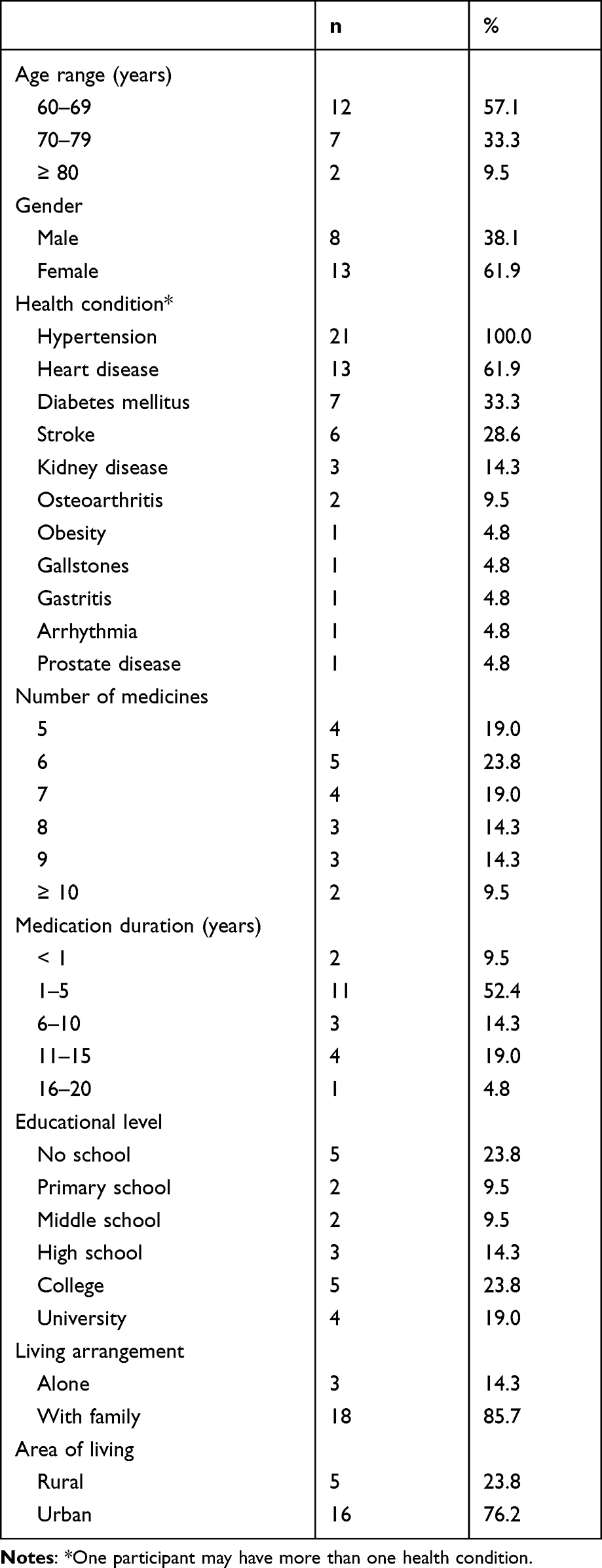 |
Table 1 Characteristics of the 21 Participants |
The themes identified from the study were classified into behavioral beliefs, normative beliefs, and control beliefs (Table 2). These beliefs are antecedents to understanding the behavior of medication adherence among seniors with polypharmacy, as shown in the schema of the TPB framework in Figure 1.
 |
Table 2 Themes, Sub-Themes, Codes, and Number of Participants Who Indicated the Codes at Least Once |
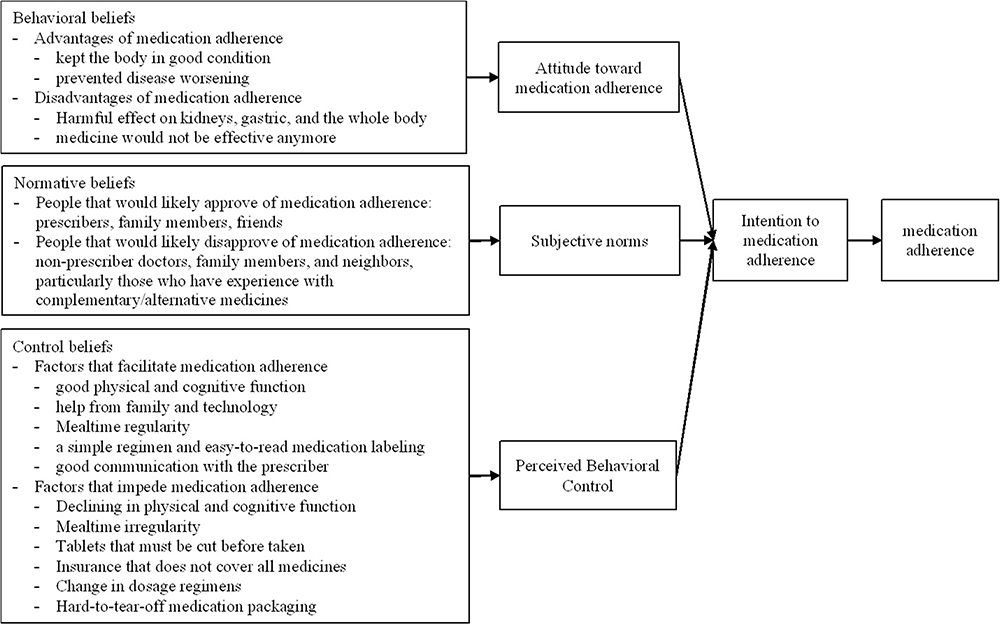 |
Figure 1 Schema of the TPB framework to understand the behavior of medication adherence among hypertensive seniors with polypharmacy. |
Behavioral Beliefs
Advantages of Medication Adherence
The participants believed that taking medicines routinely was advantageous because the medicines kept their body in good condition. These were interpreted from the following quotations.
Yes, at least, insya Allah [God willing], you can keep the body in a stable condition.
Yes, to be healthy, right? Because I will go hajj this year. Well, in fact, the blood pressure decreased, right?
They also believed that taking medicines routinely prevents them from disease worsening.
My neighbor does not take the medicines, then [it worsens to] kidney disease instead, then sorry, Miss, he is on dialysis now.
However, the participants also thought the risk of medication non-adherence was still tolerable, and missing doses sometimes was all right. Some intentionally did not take antihypertensive or lipid-lowering medicines for one or two days but retook them the next day.
If I go out, I forget, I do not take the medicines. But that is okay. Not taking the medicines one or two days is okay.
Disadvantages of Medication Adherence
The participants also showed concern about taking medicines every day. They reported that they feared medications’ harmful effects on the kidney, gastric, or whole body, because medicines poison the body. To counter this, they drink more water or sometimes coconut water to detox the body from any harmful effects of medications. Some participants reported these activities but still routinely took medicines from doctors.
Lha [exclamation in Javanese], what I am afraid of taking medications is clearly it will affect my kidney. That is why I drink a lot of water. Sometimes every two weeks I buy coconut ice water, I drink the coconut water, to let the medicine wear off. That is it.
Usually, I ask if I take many medicines, will it cause stomach problems or not?
Otherwise, in the sense that the target [of the medication] is not right, it is not advantageous. It is just drinking a poison. Just poisoning the body.
One participant added that his concern was that after some time, his body would be resistant to medicines (the medicines would not be effective anymore), which was implied from the interview.
Interviewer:Do you have any concerns about this, sir? About you taking these medicines all the time?
Participant:Yes, I am afraid of, what is it called? What is it? Resistance.
Interviewer:Oh, did you get antibiotics, sir?
Participant:There are no antibiotics, Miss.
Interviewer:Oh, resistance means the medicines will not work anymore?
Participant:[Nodding] Yes, there will be no effect again on my body.
Interviewer:Are you feeling that resistance, sir?
Participant:No, not yet.
Normative Beliefs
People Who Would Likely Approve of Medication Adherence
It was implied in society that seniors with a chronic disease (particularly those with high education, health education, and a family living with/near them) should accept their condition because everything has been written by God, including their illness. This acceptance would be shown by the regular clinic or hospital check-ups, obedience to doctor’s instructions, and taking their medications as prescribed. Therefore, prescribers, family members, and friends were among the people who would likely approve of medication adherence, which was interpreted from the following sentences.
If I stop [the medication], I am afraid, the doctor used to say, anyway, unless the doctor says to stop, continue this [the medication]. I am afraid. I take them, never stop.
[I live with] three [members of the family], yes, with daughter-in-law. She helps when the medicine runs out or what, she already knows, Miss. “Oh, you must do this, Mom, you must do that”.
I have been motivated by a friend, Miss, it [taking medicines] is like eating peanuts.
People Who Would Likely Disapprove of Medication Adherence
On the other hand, non-prescriber doctors, family members, and neighbors, particularly who had experience with complementary/alternative medicines, were among the people who would likely disapprove of medication adherence. Reducing or not taking “chemical drugs” and using traditional/alternative medicines instead, was also considered good in society, which may risk medication adherence. One of the participants was proud of only taking propolis during the Covid pandemic and did not get Covid-19. However, she confessed that she still takes the daily medicines for her hypertension and cardiac disease. Some of the participants reported that their friends, even the non-prescriber doctors, are “mocking” them as “moving the pharmacy counter home” or “reselling the medicines” because they receive so many medicines in one hospital visit.
Yes, it is doctor R that also [say] that. “Wow, ma’am, you are going to reselling medicine, ma’am, open a pharmacy in Magelang, right?” Yes, I answered, I am.
Yes, that is it. It is like I am influenced, yes, by the neighbor. [Imitating what the neighbor said], “Why should we take medicine? It is normal. You do not have to take medicines. Just let it go. The important thing is to pray”.
Some participants also shared about family members that encouraged them not to take some or all of those medicines, as indicated in one of the interviews.
Participant:My child in Jakarta [forbidding from taking medicines]. Just herbs. Lha [exclamation in Javanese, showing disagreement], if I want to go on Hajj, [my disease] should be controlled, I said to my child.
Interviewer:Your child in Jakarta did not allow you to take all medicines?
Participant:Not allowed. Do not take medicines.
Interviewer:Then how?
Participant:Only herbs. Habbatussauda and honey, and what is it, olive oil. But yes, I just said yes (despite the disagreement), that is all.
Control Beliefs
Factors That Facilitate Medication Adherence
The participants implied they can take medications routinely because they still have a good physical and cognitive functions, which was interpreted from the following sentence.
Oh, I have memorized it [the regimen], Miss. I have memorized it for years. I am not dementia, right?
Another participant confessed that she did not understand medicines because she did not attend school, and the family member explained that she was illiterate. As she needs help from the family member to prepare her medications, help from the family facilitates her adherence.
Daughter:Has my mother prepared [the medicine] by herself? Did you ever prepare [the medicine] by yourself [asking her mother]?
Participant:No, it should be prepared [by a family member].
Daughter:[nodding] Yes, should be prepared [by family member].
Participant:Otherwise, I do not want [to swallow the medicines]. I might make a mistake.
Daughter:Yes.
Participant:I am afraid of preparing the medicines myself. If they forget [to prepare my medicines], I will call my oldest son, “come here, I have not had my medicines yet”.
Not only helps from family but one participant also used technology to help them adhering medications.
[I was] reminded: medicine, medicine! I also have a timer on my phone, set by my daughter. Her father also [reminds me]: do not forget the medicines, do not forget the medicines.
As many medicines were directed to be taken after meals, some participants and their families admitted that the mealtime regularity is a factor that facilitates them to take medicine as prescribed. If they were late taking meals, they would be late taking medicines.
Yes, meals on time, right, Miss?
From the medicine-related factor, simple medication regimens and easy-to-read medication labeling facilitated patients to take medicine routinely, as indicated in the following sentences.
Yes. if only once a day, no [not confused]. If it used to be that much, and three times a day, I thought [it would be] difficult, hehe [smiling], to take the medicines. But Alhamdulillah [praise to God] it gets better, [now all the medicines are] once a day, once a day, once a day [pointing each medicine].
Yes, there are labels to read, these are [to be taken] before meals, these are right when eating the meals, and these are to be taken after meals. Then there are medicines to be taken one hour before meals at night.
Some participants said they were not worried about taking medicines routinely as they communicated well with the prescriber doctor, as implied in the following sentences.
Yes, sometimes if there is, anu [word to say someone is thinking in Javanese], that I am not feeling well, I immediately say it, I immediately say that to the doctor. I stopped [the medicine] myself. Later when I do a control visit, I will immediately say, “why I do not feel well taking this drug, doc?” “Oh yes, then just stop it, I will change the drug later”.
I can have a discussion with doctor X. Oh, it can be a long discussion. If something is happening, I will discuss it with doctor X.
Factors That Impede Medication Adherence
On the other hand, participants were aware that declining physical and cognitive function would prevent them from being adherent.
Actually, at first, when I had to take a large number of medicines a day, there was not any real difficulty. But later, with the development of my physical condition, including memory problems and so on, sometimes I might forget to take medicines.
Many participants rely very much on meal timing to take medications. This is acceptable in diabetes mellitus patients, where the administrations of antidiabetic drugs depend on mealtime. However, some participants also referred to meal timing before they administered antihypertensive or antihyperlipidemic medications. Whenever they feel their stomach is full, they will delay their mealtime. Thus, the schedule of taking medications would also be late.
Here when I have not eaten [my meals], I have not taken medicines, yes later on. I am still full. I am still full, I will eat later. The most important is I still feel good.
Two participants showed their hardship with tablets needing to be cut before they were taken, either because the dose was too big or the size of the tablets was too big.
It is funny if they tell you to take it a quarter [tablet]. How do you do that?
When it is [the tablet] too big, it is difficult to swallow. So you need to cut it sometimes. Sometimes I do not cut it. But I go on [to cut it], it is okay. [to swallow]
Some participants also showed hardship when they found the insurance did not cover some medicines. As charging the insurance participants is against the law, these patients are usually requested to buy the medicines elsewhere.
Participant:My complaint is when I was asked to buy it myself because they just give half or a third of it [the prescribed medicines]. Oh there was a third of it [looking at his medications in the plastic bag].
Interviewer:What about the rest?
Participant:Buy [them] myself [elsewhere].
From the medication factor, a change in medication regimens would impede the participant from taking medicine routinely as prescribed.
Yes, that is because the regimen has been changed. It was twice a month, but this month only once. Well, it is a change in the regimen that makes you forget.
There was also difficulty in opening the medication package.
[It is difficult] to open the package, Miss. What is the name, blister? [Later, it was revealed that he meant aluminum foil instead of blister when he showed his medicines]. Oh yes, it is difficult to open. You have to use scissors.
Discussion
Using the TPB approach, this study revealed beliefs about taking many medications daily as prescribed among hypertensive seniors with polypharmacy in Yogyakarta province and its surrounding. The TPB is a framework for predicting and explaining behavior in various domains. It has been widely used to understand some health-related behavior, such as condom use among young people,24 parents’ intention to reduce childhood fever with medications,25 and nonprescribed antibiotics use.26 Since medication adherence is also a patient’s medication-taking behavior, understanding these beliefs can be a key to improving adherence.
In general, most participants reported they were adherent to medication because they understood the benefit of taking medication routinely to their bodies. However, they had concerns about the harmful effect of the medications, although they did not feel the side effects they were worried about. Similarly, in some previous studies, patients often have concerns about taking medication out of fear of drug dependence or side effects.27,28 What is new in this finding is that participants tend to eliminate this perceived side effect by drinking a lot of water or coconut water. Although many participants believe in the detoxification effect of coconut water, there is almost no study yet to prove this effect.
There was also concern that the medicines would not be effective anymore. Although it was unclear which medication led to this perceived belief, drug tolerance may occur in antihypertensive agents.29,30 Therefore, healthcare professionals should be aware of these common concerns and may address them to maintain medication adherence.
On the one hand, some participants perceived that their significant others, such as prescribers, family members, and friends, approved of them taking all prescribed medicines as the prescriber said. On the other hand, participants perceived that non-prescriber doctors, family members, and neighbors might also disapprove of medication adherence, by encouraging them to lessen the number and frequency of the medication use, mocking the participants with a large number of medications, or providing other alternatives such as herbal use. The last strategy was usually suggested by people who have experienced herbal use. However, this encouragement of non-adherence generally referred to all medications, not only particular routine medications such as antihypertensive or antidiabetic agents. Patients perceived people around them expected that having fewer “chemical” medicines and using herbal medicines instead is better.
Concerning herbal use, a previous study showed that the most common complementary/alternative medicine (CAM) therapy used by type 2 diabetes mellitus patients in Indonesia was herbs. These users had positive attitudes toward CAM, but most chose not to disclose their CAM use to their healthcare providers.31 In a recent study, even the majority of participating general practitioners demonstrated a favorable view towards traditional Indonesian herbal medicines’ role in conventional care.32 So, as part of a society where traditional or herbal medicine is trusted, this indeed affects patient perception of the medication prescribed. Dismissive this belief might widen the gap between traditional and modern medication, while encouraging that traditional medicines could work complementary with the prescribed medicine, surely with the prescriber’s supervision, might encourage medication adherence. In the case of drinking coconut water and taking herbal medicines, health professionals might encourage patients to do so after two or two and a half hours of taking the prescribed medicines to prevent the risk of drug interactions.
Non-adherence behaviors are classified into intentional non-adherence and unintentional non-adherence. Intentional non-adherence is when individuals decide not to follow the treatment recommendations, possibly because of concerns about the drug’s effectiveness, side effects, and discomfort in using the drug according to the timing and frequency of using the drug as directed.33 Intentional non-adherence occurs when a patient decides not to take the treatment as instructed. Weintraub also termed this as intelligent noncompliance, which describes the situation in which a patient does not take the medication as prescribed but at a dose and on a schedule that is beneficial to the patient, because of valid and rational reasons.34 Meanwhile, unintentional non-adherence is when an individual wants to follow treatment recommendations but cannot do so due to cognitive problems, poor management skills, polypharmacy, and difficulty accessing medication.32 However, intentional and unintentional may sometimes overlap each other. For example, a patient may forget to take their medicine but refuse to set the alarm or receive help to set the alarm. From this study, some participants implied that they wanted to follow the treatment recommendations but were hindered due to physical and cognitive decline, insurance that does not cover all medicine, a change in dosage regimens, or hard-to-tear-off medication packaging. Nevertheless, some participants were considered intelligent noncompliant by arranging their medication regimen based on their schedule and understanding.
For seniors, the family turned out to be significant in medication adherence, with or without using technology. Some quotations showed that the participants expected and received support from their family members to manage the medications. One participant even shared that her daughter helped her set the timer on the phone or install a mobile application to know the weight of the rice she should eat. Therefore, a healthcare professional might address medication adherence issues among seniors through their family members and by using technology.
Plenty of studies found the benefit of family support to hypertension medication adherence35–39 and the benefit of using technology for chronic conditions management such as text messaging and mobile apps.40–42 But it should be noted that despite the increasing need of technology, seniors might have difficulty in using mobile phone or navigating through an app. When available, healthcare professionals might introduce some apps that are seniors-friendly, but the help of family members in using the technology may also be required.
However, it should be realized that friends and family members may not always approve of medication adherence. They may have different beliefs and give inappropriate advice and opinions which negatively influence adherence and self-management behaviors.43 The healthcare professionals must then be sensitive to the particular beliefs when assessing the seniors’ treatment adherence issues.
This study yields insights into a health communication approach to seniors. As a health professional, understanding patients’ perceptions is essential. Physicians and pharmacists, for example, must be sensitive to patients’ beliefs regarding medications and address these beliefs while encouraging medication adherence and providing health education to society. Only attempting to increase adherence without consideration of the reasons for non-adherence can lead to other problems. As patients can choose not to follow their prescribed therapy and may know their body best,44 bidirectional communication and adherence assessment become critical.34
This study has a strength in terms of the diverse social background the participants purposively selected. The findings are considered robust to describe common beliefs about medication adherence among seniors with hypertension and chronic conditions in Yogyakarta and its surroundings. However, this study also has limitations. First, as pharmacists conducted the interviews, there might be an interview bias where patients tend to show their adherence and conceal non-adherence behaviors, influencing the beliefs they expressed. Second, the sampling strategy from a pharmacy or a hospital might introduce selection bias, since participants who were routine visitors might have already adhered to their medications. People who were non-adherent might not show up to health centers to do check-ups or refill prescriptions and may express different beliefs.
Conclusion
This study elicited what seniors believe about medication adherence. Health professionals should incorporate these beliefs in the communication approach to improving medication adherence in seniors.
Acknowledgments
The authors would like to acknowledge the participants, the pharmacists in study sites (Rumah Sehat dan Apotek UGM and RSUP Dr. Sardjito), Chintya Gilang Ghaisani as the interviewer assistant, and Faculty of Pharmacy Universitas Gadjah Mada for the license of QSR’s NVivo 12 Pro software.
Author Contributions
SS, CW, NNW, and P developed the concept of the research. NNW and one research assistant interviewed participants. NNW transcribed the original language (Bahasa Indonesia and Javanese). All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Final Project Recognition Grant Universitas Gadjah Mada number 3550/UN1.P.III/Dit-Lit/PT.01.05/2022.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pusat Analisis Determinan Kesehatan. Analisis Kebijakan Mewujudkan Lanjut Usia Sehat Menuju Lanjut Usia Aktif [Policy Analysis to Materializing Healthy Aging Towards Active Aging]. Kementerian Kesehatan Republik Indonesia; 2019.
2. Kementerian Kesehatan Republik Indonesia. Hasil Utama Riskesdas 2018 [Main Results of Basic Health Research 2018]. Kementerian Kesehatan Republik Indonesia; 2018.
3. Husnayain A, Ekadinata N, Sulistiawan D, Chia-Yu Su E. Multimorbidity patterns of chronic diseases among Indonesians: insights from Indonesian National Health Insurance (INHI) sample data. Int J Environ Res Public Health. 2020;17(23):8900. doi:10.3390/ijerph17238900
4. Girsang APL, Ramadani KD, Nugroho SW, Sulistyowati NP, Putrianti R, Wilson H. Statistik Penduduk Lanjut Usia 2021 [The Statistics of Senior Citizens 2021]. Fungsi Statistik Pendidikan Dan Kesejahteraan Sosial, Ed.. Badan Pusat Statistik; 2021.
5. Dinas Kesehatan Daerah Istimewa Yogyakarta. Profil Kesehatan D.I. Yogyakarta Tahun 2020 [Health Profile of D.I. Yogyakarta in 2020]. Dinas Kesehatan Daerah Istimewa Yogyakarta; 2021.
6. Lo LSHS, Chau JPC, Woo J, Thompson DR, Choi KC. Adherence to antihypertensive medication in older adults with hypertension. J Cardiovasc Nurs. 2016;31(4):296–303. doi:10.1097/JCN.0000000000000251
7. Razak R, Laksono A, Kusumawati L, Wijayanti K. Hypertension among elderly in Indonesia: analysis of the 2018 Indonesia basic health survey. Med Legal Update. 2021;21:78–86. doi:10.37506/mlu.v21i3.2967
8. Mahmood S, Jalal Z, Hadi MA, Khan TM, Haque MS, Shah KU. Prevalence of non-adherence to antihypertensive medication in Asia: a systematic review and meta-analysis. Int J Clin Pharm. 2021;43(3):486–501. doi:10.1007/s11096-021-01236-z
9. Zelko E, Klemenc-Ketis Z, Tusek-Bunc K. Medication adherence in elderly with polypharmacy living at home: a systematic review of existing studies. Mater Sociomed. 2016;28(2):129–132. doi:10.5455/msm.2016.28.129-132
10. Burnier M, Polychronopoulou E, Wuerzner G. Hypertension and drug adherence in the elderly. Front Cardiovasc Med. 2020;7:49. doi:10.3389/fcvm.2020.00049
11. Management Sciences for Health. MDS-3: Managing Access to Medicines and Health Technologies. Management Sciences for Health; 2012.
12. Van der Laan DM, Elders PJM, Boons C, Beckeringh JJ, Nijpels G, Hugtenburg JG. Factors associated with antihypertensive medication non-adherence: a systematic review. J Hum Hypertens. 2017;31(11):687–694. doi:10.1038/jhh.2017.48
13. Yap AF, Thirumoorthy T, Kwan YH. Medication adherence in the elderly. J Clin Gerontol Geriatr. 2016;7(2):64–67. doi:10.1016/j.jcgg.2015.05.001
14. Hugtenburg JG, Timmers L, Elders PJM, Vervloet M, van Dijk L. Definitions, variants, and causes of nonadherence with medication: a challenge for tailored interventions. Patient Prefer Adherence. 2013;7:675–682. doi:10.2147/PPA.S29549
15. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–567. doi:10.1016/s0022-3999(99)00057-4
16. McQuaid EL, Landier W. Cultural issues in medication adherence: disparities and directions. J Gen Intern Med. 2018;33(2):200–206. doi:10.1007/s11606-017-4199-3
17. W-W L, Stewart AL, Stotts N, Froelicher ES. Cultural factors associated with antihypertensive medication adherence in Chinese immigrants. J Cardiovasc Nurs. 2006;21(5):354–362. doi:10.1097/00005082-200609000-00005
18. Eh K, McGill M, Wong J, Krass I. Cultural issues and other factors that affect self-management of Type 2 Diabetes Mellitus (T2D) by Chinese immigrants in Australia. Diabetes Res Clin Pract. 2016;119:97–105. doi:10.1016/j.diabres.2016.07.006
19. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
20. Ajzen I. Constructing a theory of planned behavior questionnaire; 2019. Available from: https://people.umass.edu/aizen/pdf/tpb.measurement.pdf.
21. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
22. World Medical Association. World Medical Association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. DOI:10.1001/jama.2013.281053
23. Braun V, Clarke V. Thematic analysis. In: APA Handbook of Research Methods in Psychology, Vol. 2: Research Designs: Quantitative, Qualitative, Neuropsychological, and Biological. American Psychological Association; 2012:57–71.
24. Reinecke J, Schmidt P, Ajzen I. Birth control versus AIDS prevention: a hierarchical model of condom use among young people. J Appl Soc Psychol. 1997;27(9):743–759. doi:10.1111/j.1559-1816.1997.tb00657.x
25. Walsh A, Edwards H, Fraser J. Attitudes and subjective norms: determinants of parents’ intentions to reduce childhood fever with medications. Health Educ Res. 2009;24(3):531–545. doi:10.1093/her/cyn055
26. Widayati A, Suryawati S, de Crespigny C, Hiller JE. Beliefs about the use of nonprescribed antibiotics among people in Yogyakarta City, Indonesia: a qualitative study based on the theory of planned behavior. Asia Pac J Public Health. 2015;27(2):NP402–NP413. doi:10.1177/1010539512445052
27. Mukhtar O, Weinman J, Jackson SHD. Intentional non-adherence to medications by older adults. Drugs Aging. 2014;31(3):149–157. doi:10.1007/s40266-014-0153-9
28. Markotic F, Cerni Obrdalj E, Zalihic A, et al. Adherence to pharmacological treatment of chronic nonmalignant pain in individuals aged 65 and older. Pain Med. 2013;14(2):247–256. doi:10.1111/pme.12035
29. Gavras HP. Issues in hypertension: drug tolerability and special populations. Am J Hypertens. 2001;14(4S):231S–236S. doi:10.1016/S0895-7061(01)02132-X
30. Struthers AD, Murphy MB, Dollery CT. Glucose tolerance during antihypertensive therapy in patients with diabetes mellitus. Hypertension. 1985;7(6_pt_2):II95. doi:10.1161/01.hyp.7.6_pt_2.ii95
31. Sari Y, Anam A, Sumeru A, Sutrisna E. The knowledge, attitude, practice and predictors of complementary and alternative medicine use among type 2 diabetes mellitus patients in Indonesia. J Integr Med. 2021;19(4):347–353. doi:10.1016/j.joim.2021.04.001
32. Rahayu YYS, Araki T, Rosleine D, Purwaningtyas RM. General practitioners’ attitudes toward traditional Indonesian herbal medicine and integrative care in the universal health coverage system. Glob J Health Sci. 2022;14(4):1–82. doi:10.5539/gjhs.v14n4p82
33. Mair A, Fernandez-Llimos F, Alonso A, et al. Polypharmacy Management by 2030: A Patient Safety Challenge.
34. Weintraub M. Compliance in the elderly. Clin Geriatr Med. 1990;6(2):445–452. doi:10.1016/S0749-0690(18)30627-X
35. Woodham N, Taneepanichskul S, Somrongthong R, Auamkul N. Medication adherence and associated factors among elderly hypertension patients with uncontrolled blood pressure in rural area, Northeast Thailand. J Health Res. 2018;32(6):449–458. doi:10.1108/JHR-11-2018-085
36. Johnson J, Vijayakumar K, Nujum ZT, Thankamoniamma PM. Compliance and its determinants to pharmacologic management of hypertension. Indian J Community Health. 2019;31(1):63–72.
37. Wang J, Zhao X. Family functioning and social support for older patients with depression in an urban area of Shanghai, China. Arch Gerontol Geriatr. 2012;55(3):574–579. doi:10.1016/j.archger.2012.06.011
38. Sheilini M, Hande HM, George A. Family support and medication nonadherence among elderly on antihypertensives. Indian J Public Health Res Dev. 2019;10:294–298. doi:10.5958/0976-5506.2019.00706.X
39. Nurannisa D, Febtrina R, Zul’Irfan M, Kharisna D. Family support increases the hypertension medication adherence in the elderly at public health center of simpang Tiga Pekanbaru. Sci Midwifery. 2022;10(5):4246–4253. doi:10.35335/midwifery.v10i5.1010
40. Ma Y, Cheng HY, Cheng L, Sit JWH. The effectiveness of electronic health interventions on blood pressure control, self-care behavioural outcomes and psychosocial well-being in patients with hypertension: a systematic review and meta-analysis. Int J Nurs Stud. 2019;92:27–46. doi:10.1016/j.ijnurstu.2018.11.007
41. Tam HL, Leung LYL, Wong EML, Cheung K, Chan ASW. Integration of text messaging interventions into hypertension management among older adults: a systematic review and meta-analysis. Worldviews Evid Based Nurs. 2022;19(1):16–27. doi:10.1111/wvn.12549
42. Wong EML, Leung DYP, Tam HL, et al. Effectiveness of a nurse-led support programme using a mobile application versus phone advice on patients at risk of coronary heart disease - a pilot randomized controlled trial. Risk Manag Healthc Policy. 2022;15:597–610. doi:10.2147/RMHP.S355554
43. Ding W, Li T, Su Q, Yuan M, Lin A. Integrating factors associated with hypertensive patients’ self-management using structural equation modeling: a cross-sectional study in Guangdong, China. Patient Prefer Adherence. 2018;12:2169–2178. doi:10.2147/PPA.S180314
44. Wertheimer AI, Smith MC. Pharmacy Practice: Social and Behavioral Aspects Third Edition. Williams & Wilkins; 1989.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Observational Cohort Study to Evaluate the Impact of a Tailored Medicines Optimisation Service on Medication Use, Accident and Emergency Department Visits, and Admissions Among Patients Identified with Medication Support Needs in Secondary Care
Harrap N, Wells J, Howes K, Kayyali R
Patient Preference and Adherence 2022, 16:2947-2961
Published Date: 28 October 2022
Prevalence of Multiple Chronic Conditions in Older Adults with Undiagnosed Mild Cognitive Impairment and Alzheimer’s Disease and Related Dementias in Primary Care
Summanwar D, Owora AH, Ben Miled Z, Dexter PR, Kulshreshtha A, Strunk S, Jiang B, Coppedge K, Disla S, Galvin JE, Boustani M, Fowler NR
Clinical Interventions in Aging 2025, 20:1799-1809
Published Date: 24 October 2025
Implementation and Evaluation of a Real-Time Prescription Alert System to Optimize Antiretroviral Therapy and Medication Adherence in People Living with HIV. SANPAT PROJECT
Morillo-Verdugo R, Solis-Martin C, Marquez-Saavedra E, Robustillo-Cortes MDLA, Romero Gil E, Contreras-Macias E
Patient Preference and Adherence 2025, 19:3493-3508
Published Date: 7 November 2025
Therapeutic Adherence and Potentially Inappropriate Prescribing in Older Adults with Polypharmacy in Primary Health Care
Lafuente González M, Calleja Hernández MA, Ferrit Martín M
Patient Preference and Adherence 2025, 19:3849-3860
Published Date: 1 December 2025
Impact of a CMO-Based Pharmaceutical Care Model on 3-HIT Criteria in Older People Living with HIV: The DIS3HIT Project
Roldán Galnares M, Morillo-Verdugo R, Robustillo-Cortes MDLA, Vélez-Díaz-Pallarés M, Company Albir MJ, Proy Vega B, Losa López L, Marín Ventura L, Ferris Villanueva M, Mora Atorrasagasti O, Gutiérrez E
Patient Preference and Adherence 2026, 20:569460
Published Date: 30 January 2026