Back to Journals » Patient Preference and Adherence » Volume 19
Implementation and Evaluation of a Real-Time Prescription Alert System to Optimize Antiretroviral Therapy and Medication Adherence in People Living with HIV. SANPAT PROJECT
Authors Morillo-Verdugo R ![]() , Solis-Martin C, Marquez-Saavedra E, Robustillo-Cortes MDLA, Romero Gil E, Contreras-Macias E
, Solis-Martin C, Marquez-Saavedra E, Robustillo-Cortes MDLA, Romero Gil E, Contreras-Macias E
Received 11 July 2025
Accepted for publication 22 October 2025
Published 7 November 2025 Volume 2025:19 Pages 3493—3508
DOI https://doi.org/10.2147/PPA.S549933
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ramón Morillo-Verdugo,1 Cecilia Solis-Martin,1 Esther Marquez-Saavedra,1 Maria de las Aguas Robustillo-Cortes,1 Eloy Romero Gil,1 Enrique Contreras-Macias2
1Pharmacy Hospital Service, Hospital Universitario de Valme, Área de Gestión Sanitaria Sur de Sevilla, Sevilla, Spain; 2Pharmacy Hospital Service, Hospital San Juan de Dios, Sevilla, Spain
Correspondence: Ramón Morillo-Verdugo, Pharmacy Hospital Service, Hospital Universitario de Valme, Área de Gestión Sanitaria Sur de Sevilla, Sevilla, Spain, Tel +34 955 015 467, Email [email protected]
Purpose: To evaluate the clinical and implementation impact of “Alert System for New Prescriptions and Therapeutic Adherence Monitoring” (SANPAT), a real-time prescription alert system embedded in a structured pharmaceutical care model, aimed at optimizing antiretroviral therapy (ART) and improving medication adherence in people living with HIV (PLWH).
Patients and Methods: A quasi-experimental, before-and-after study was conducted in a hospital outpatient pharmaceutical care unit in Andalusia, Spain. Patients aged ≥ 50 years receiving ART were included if they had polypharmacy (≥ 6 concurrent medications) or demonstrated poor adherence. The pre-intervention period (Feb 2023–Jan 2024) relied on standard care without alerts. The post-intervention period (Feb 2024–Jan 2025) incorporated SANPAT, enabling pharmacists to receive real-time alerts for new prescriptions and adherence risks. Pharmaceutical interventions were classified using a validated Capacity-Motivation-Opportunity (CMO)-based taxonomy, and implementation was evaluated using the Reach, Effectiveness, Adoption, Implementation y Maintenance (RE-AIM) framework.
Results: A total of 153 patients were included (84 pre- and 69 post-intervention). The number of pharmacist interventions increased markedly post-intervention (from 84 to 877 events), especially in adherence support (0.0% to 47.2%) (p< 0.001) and medication error prevention (0.0% to 34.7%) (p< 0.001). The frequency of polypharmacy and major polypharmacy increased, while immunovirological risk markers improved (CD4 cell count< 200 cells/μL decreased from 15.0% to 4.3%; detectable viral load from 20.3% to 3.6%) (p< 0.001). The RE-AIM evaluation demonstrated broad reach, high adoption, improved implementation metrics, and early signs of long-term sustainability.
Conclusion: SANPAT significantly enhanced the timely identification and resolution of pharmacotherapeutic risks in PLWH, supporting personalized interventions and optimizing ART management. Its integration within existing electronic prescribing populations.platforms and structured care models represents a scalable strategy to improve medication safety in aging and complex patients.
Keywords: HIV, antiretroviral therapy, clinical decision support system, medication adherence, pharmaceutical care, real-time alerts, RE-AIM, polypharmacy
Introduction
Human immunodeficiency virus (HIV) infection has undergone a radical transformation over the past decades.1 While initially associated with high morbidity and mortality, the introduction of antiretroviral therapy (ART) has enabled it to become a manageable chronic disease.2 Due to the advent and widespread use of ART, HIV has transformed into a chronic condition, leading to an aging people living with HIV (PLWH) population with increased life expectancy.3 Consequently, these patients exhibit a higher burden of comorbidities, resulting in increased polypharmacy, a greater risk of drug-drug interactions, and challenges in medication adherence.4–8
Polypharmacy, defined as the concurrent use of six or more medications, is highly prevalent among older adults with HIV due to the need to manage multiple comorbidities, including cardiovascular disease, diabetes, renal impairment, and mental health disorders. While ART regimens are highly effective, their complexity—stemming from the presence of multiple drug classes and pharmacokinetic profiles—further complicates medication management.9–11 Drug-drug interactions (DDIs) between ART and concomitant therapies can lead to treatment failure, increased toxicity, and adverse clinical outcomes. Moreover, poor adherence to ART and co-medications has been widely recognized as a major barrier to optimal long-term disease management.12–14
Pharmaceutical interventions play a crucial role in mitigating the risks associated with polypharmacy and improving adherence.15,16 Hospital pharmacists are essential in identifying clinically significant DDIs, optimizing ART regimens, and implementing strategies to support medication adherence.17,18 Also, in Spain PLWH receive their ART exclusively through hospital pharmacies, regardless of hospitalization status. Traditional pharmaceutical care (PC) models rely on scheduled consultations and retrospective medication reviews, which may lead to delays in detecting new prescriptions and potential DDIs.19 Therefore, innovative approaches are required to enhance real-time intervention and prevent adverse outcomes.
The Capability-Motivation-Opportunity (CMO) model has been proposed as an effective framework to improve pharmaceutical interventions in chronic patients, and for PLWH is considered the standard for monitoring according to current guidelines in Spain.20,21 Within this model, opportunity refers to the availability of tools and systems that facilitate proactive interventions. In the context of HIV pharmacotherapy, technological solutions can enhance PC by ensuring early identification of prescribing risks and adherence issues.22,23
In recent years, digital health tools have demonstrated their potential in optimizing pharmacotherapy, particularly through clinical decision support systems (CDSS) and real-time prescription alerts.24,25 The integration of automated alert systems within electronic prescribing platforms has been shown to enhance medication safety, improve adherence, and reduce DDIs in other therapeutic areas (e.g oncology or chronic conditions).26–29 While CDSS have demonstrated efficacy in various therapeutic areas, their specific impact on ART adherence in PLWH has not been extensively evaluated in clinical studies.
Given the increasing complexity of ART regimens and the prevalence of polypharmacy, it is imperative to explore the effectiveness of real-time digital tools in optimizing HIV treatment. The objective of this study is to evaluate the utility of a real-time prescription alert system for monitoring new prescriptions and adherence to optimize ART in HIV-infected patients within a hospital PC setting.
Materials and Methods
Study Design
A quasi-experimental before-and-after study was conducted in the outpatient PC unit of a public general hospital in Andalusia, Spain. The study was structured into two periods:
- Pre-Intervention Period: From February 1, 2023, to January 31, 2024, PC relied on in-person consultations at the hospital pharmacy or direct patient communication via telephone regarding new prescriptions issued by non-infectious disease specialists. No computerized alerts were available.
- Post-Intervention Period: From February 1, 2024, to January 31, 2025, an alert system was activated, allowing pharmacists to intervene proactively in real-time through electronic prescribing.
Population and Inclusion Criteria
Patients included in the study met the following criteria: Confirmed diagnosis of HIV infection, active antiretroviral therapy (ART), Age ≥ 50 years and regular follow-up in the hospital’s PC unit.
Additionally, patients had to meet at least one of the following criteria:
1) Polypharmacy (≥6 concurrent medications) or high pharmacotherapeutic complexity during the study period;
2) Confirmed poor adherence to concomitant medications prescribed alongside ART, assessed using two measurement methods: a multi-interval dispensing ratio (MDR) <90% based on pharmacy refill data and non-adherent classification according to the Simplified Medication Adherence Questionnaire (SMAQ), a validated tool for PLWH.
Patients were excluded if they participate in clinical trials involving active pharmacological interventions during the study period or were transfer to another hospital or had incomplete clinical records.
During this period prescriptions originated from both infectious disease specialists and other specialties (internal medicine, primary care, and other hospital units), reflecting real-world conditions.
Development and Implementation of the Alert System
The computerized alert system, named in Spanish “Sistema de Alerta de Nuevas Prescripciones y Adherencia Terapeutica” and in English: “Alert System for New Prescriptions and Therapeutic Adherence Monitoring” (SANPAT), was developed and integrated into “Receta XXI” the official electronic prescribing platform of the Andalusian Health Service.
The process was developed in several phases.
- Alert System Design and Integration:
Alerts were configured and linked to patients’ pharmacotherapeutic records within Receta XXI.
- Validation and Pilot Testing:
Technical validation was performed with hospital pharmacists.
A pilot test was conducted with a subset of patients to assess usability and system impact, followed by adjustments based on identified challenges.
- Clinical Implementation:
SANPAT was introduced for clinical use in February 2024. Healthcare personnel were trained.
Functionality of the SANPAT System
The tool consists of several operational modules (Figures 1 and 2)
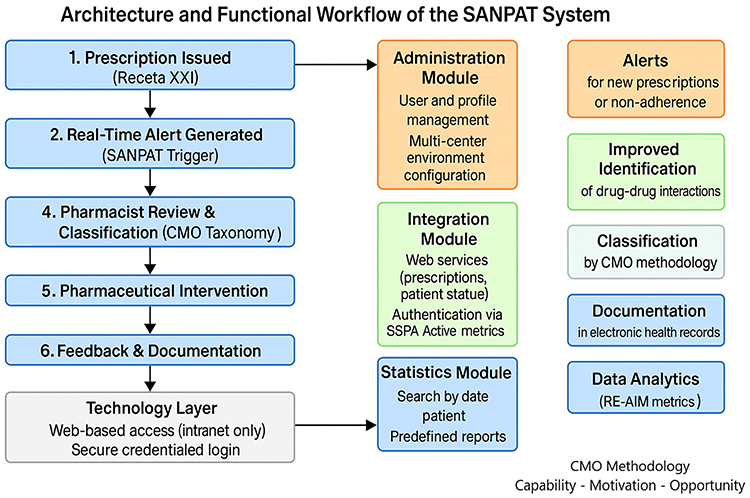 |
Figure 1 Architecture and functional workflow of SANPAT. |
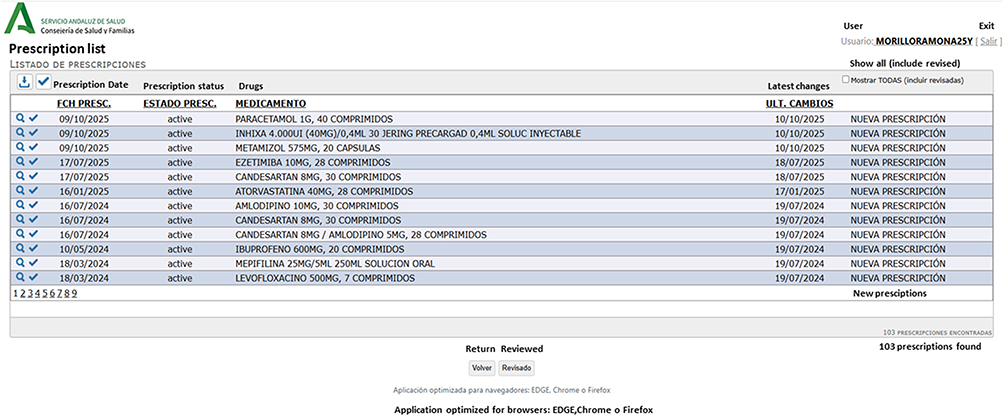 |
Figure 2 Original Spanish-language interface of the SANPAT (Prescription Alert and Adherence Monitoring System) tool (English translations of key fields are provided below for clarity). |
Administration Module
This module manages general system functionalities, such as: User and profile, management of the system’s master tables and parameter and configuration. The system was designed to operate in multi-center environments within the Andalusian Health Service (SSPA).
Patient Management and Monitoring Module
This module allows the definition and management of the selected patient cohort for monitoring, as well as defining how and to whom notifications should be sent in case of prescription changes. It includes a rapid search system for patients using key fields directly from the Unified Database (BDU). Supports patient monitoring management (add, modify, deactivate, activate/deactivate monitoring, monitoring type, notifications to stakeholders, etc). Enables traceability of prescription changes for each patient (history of changes). Patient grouping: to facilitate monitoring and associated notifications, the system organizes patients into categories, forming various monitoring groups.
Integration Module
This module was developed in alignment with the standardized electronic prescription and dispensing methodology of the Andalusian Health Service (Servicio Andaluz de Salud, SSPA), which provided the infrastructure required for SANPAT’s integration with corporate and clinical information systems. To ensure optimal functionality, the module incorporates:1 a web service for prescription messaging;2 a web service for monitoring patient status changes (eg, death notifications); and3 integration with SSPA’s authentication and access control systems. Authentication is performed against the SSPA’s Active Directory (DMSAS), and user permission profiles are structured according to assignment to specific DMSAS groups.
Statistics Module
This module gathers all the data required for reporting purposes: features a search system by date and/or patient. Offers a series of predefined reports for patient monitoring.
Technical Requirement and Technological Environment
The project was developed using web technology to ensure the application is accessible from any internal SSPA network device via a web browser, without requiring installation on client devices. To ensure information security, access was controlled by credential validation (username and password) against the database. Unauthorized users cannot access the application.
The tool was registered with an intellectual property record under number: 2404297818177–37VUTS.
Data Collection and Analysis
Baseline characteristics (dependent variables) of the patients were collected, including sex, current age at diagnosis, route of HIV acquisition (sexual, parenteral, or vertical), detectable viral load status, CD4 level (less than 200 cells/mcL or greater than or equal to 200 cells/mcL), AIDS advanced HIV disease (CD4 <200 cells/µL or AIDS-defining condition), comorbidities and their patterns (cardiovascular, neuropsychiatric, COPD-hepatic, sexually transmitted diseases, AIDS-related events, or general health). Additionally, data were collected on the number of concomitant medications with ART, polypharmacy, and major polypharmacy defined as ≥630 and ≥10 medications concurrently used. Patterns of polypharmacy included psychogeriatric, cardiometabolic, mechanical-obese-thyroid, or mixed categories.31 ART regimens were categorized into four groups: nucleoside reverse transcriptase inhibitors (NRTIs) + non-nucleoside reverse transcriptase inhibitors (NNRTIs), NRTIs +protease inhibitors (PIs), NRTIs + integrase inhibitors (INIs), and others.The interventions recorded during the study period were classified according to the taxonomy published for the CMO methodology in PLWH.32
Patient stratification according to the CMO framework was performed using predefined criteria, including comorbidity burden, pharmacotherapeutic complexity, and adherence profile, following published models for PLWH.33
RE-AIM Evaluation Framework
To comprehensively evaluate the implementation, the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework was applied. This model assesses a multidimensional perspective of intervention performance in real-world settings.
Implementation outcomes were assessed using the RE-AIM framework, following established methodological recommendations for digital health interventions. For each domain, specific indicators were selected a priori based on RE-AIM planning guidelines and adapted to the PLWH PC context. Table 1 summarizes these indicators along with their operational definitions and rationale.
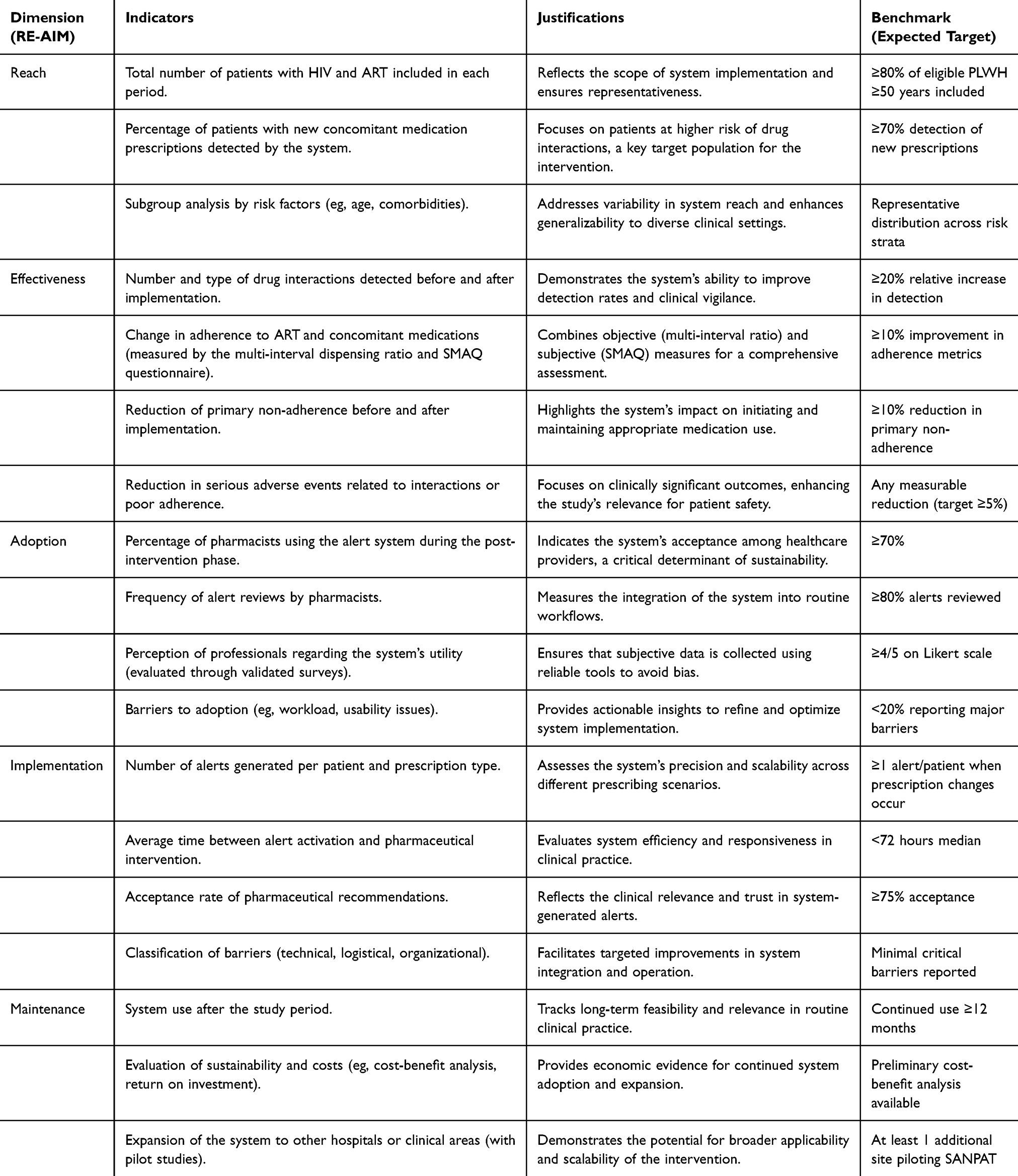 |
Table 1 RE-AIM Dimensions, Indicators, Justifications, and Predefined Benchmarks |
Reach was measured as the number and proportion of eligible PLWH receiving ART who were captured by SANPAT, with subgroup analyses stratified by age, comorbidity burden, and polypharmacy status.
Effectiveness focused on improvements in clinical outcomes (CD4 cell counts, viral suppression) and adherence metrics. These were assessed through standard clinical records and patient self-reports.
Adoption included the proportion of pharmacists actively using SANPAT, the rate of alert review, and usability perceptions collected through structured surveys based on validated instruments.
Implementation indicators comprised the number and type of alerts, response times, intervention acceptance rates, and recorded barriers categorized as technical, operational, or organizational.
Maintenance was evaluated through continued system use post-study, presence of scaling plans across institutions, and preliminary cost-benefit assessments.
For each indicator, a percentage score was calculated by comparing the observed value to a predefined target, either based on literature benchmarks or consensus among a multidisciplinary panel of experts in implementation science and clinical pharmacy.
Data for the RE-AIM evaluation were collected using multiple sources. System usage data (alerts generated, intervention types, time-to-action, and acceptance rates) were extracted directly from SANPAT’s internal activity logs. Adoption metrics, including pharmacist engagement and perceived usability, were assessed through a structured, self-administered questionnaire developed by the research team based on validated implementation science constructs. The questionnaire was piloted internally to ensure face and content validity prior to deployment.
For each RE-AIM indicator, an expected value or benchmark was defined a priori based on published literature where available. In the absence of validated thresholds, consensus values were established by a multidisciplinary panel of five experts in PC and implementation science using a modified nominal group technique. Table 1 summarizes the RE-AIM dimensions, indicators, operational definitions, rationale, and the predefined benchmarks used to guide interpretation of the results. This approach ensured methodological rigor and contextual relevance when calculating domain-specific percentage scores.
Statistical Analysis
The sample size was initially calculated to detect an expected improvement in the intervention rate of 20 percentage points, from a baseline rate of 47% (pre-intervention period) to 67% (post-intervention period), with a two-sided α error of 0.05 and a target power of 80%. This estimation indicated a requirement of 60 patients per group. However, given the prospective nature of the study and its implementation within routine clinical practice, the recruitment process was influenced by real-world constraints. Additionally, no adjustments for dropout were necessary, as complete follow-up data were available for all participants.
A descriptive and inferential statistical analysis was performed to evaluate the differences in clinical and pharmacotherapeutic variables before and after the implementation of the SANPAT system. Quantitative variables were summarized using means, standard deviations, and 95% confidence intervals, while categorical variables were presented as percentages.
For the comparison of continuous variables between the pre- and post-intervention periods, Student’s t-test for independent samples was applied when normality was assumed; otherwise, the Mann–Whitney U-test was used. Categorical variables were compared using the Chi-square test or Fisher’s exact test, as appropriate. The normal distribution of variables was assessed via normal probability plots and skewness/kurtosis coefficients.
Additional exploratory analyses were conducted using stratified subgroups (eg, comorbidity patterns, ART regimen types, geriatric classification) to identify differential effects. Given the exploratory nature of this quasi-experimental study, no correction for multiple comparisons was applied. All analyses were performed using SPSS (v29) and RStudio (v1.1.456), with a significance threshold set at p < 0.05.
Ethics
The study was carried out according to the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use and the Declaration of Helsinki. The study protocol and any other information that required prior approval was reviewed and approved by the ethics committee of the research center Comité de Ética de Investigación Sevilla Sur (0682-N-22). All participants provided written informed consent prior to enrollment.
Results
Patient Characteristics
A total of 153 PLWH and receiving ART were included in the study, with 84 patients in the pre-intervention group and 69 in the post-intervention group. Baseline characteristics are summarized in Table 2. The median age of participants increased slightly between periods (56 vs 64 years, p < 0.001). No significant differences were observed in sex distribution (p = 0.210), but statistically significant changes were identified in most clinical variables, including AIDS staging, CD4 count, viral load, and comorbidity profiles (p < 0.05 for all).
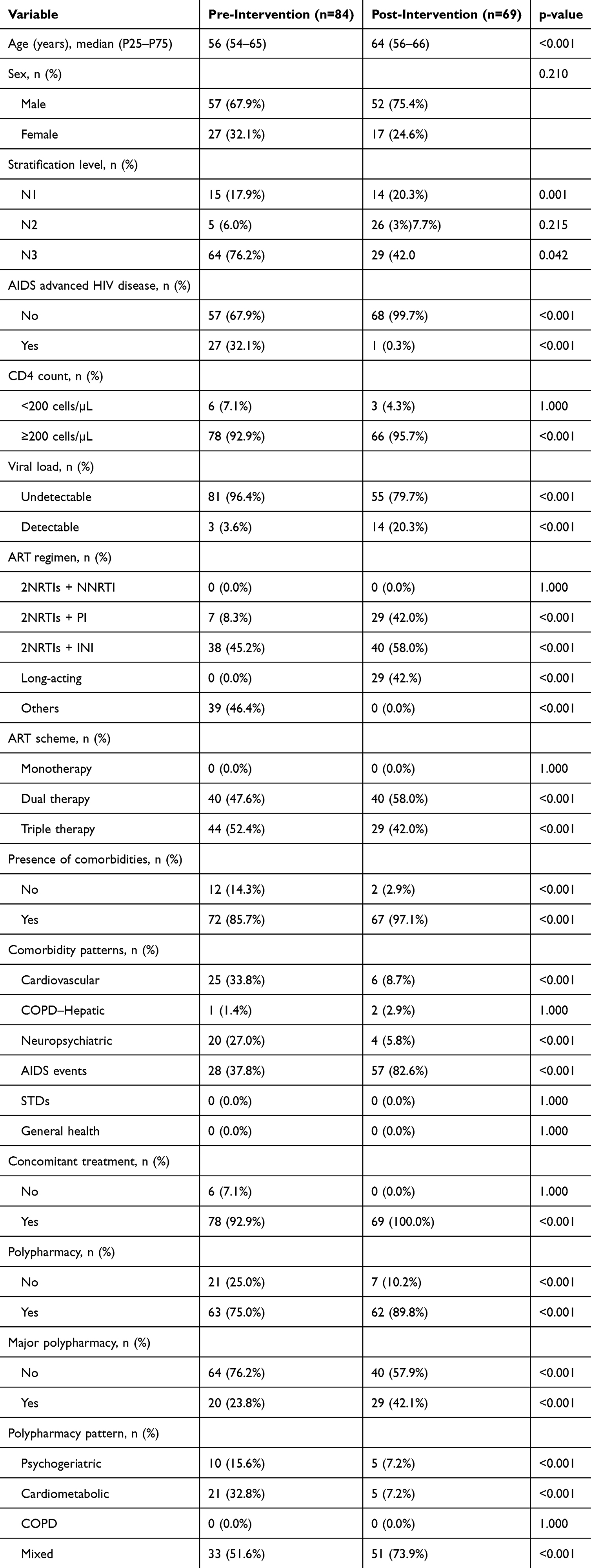 |
Table 2 Baseline Characteristics of the Study Population |
Stratification of patients according to the CMO model revealed a significant shift in complexity levels post-intervention, with a marked increase in level 2 patients (from 6.0% to 37.7%, p = 0.001) and a concomitant decrease in level 3 cases (from 76.2% to 42.0%, p = 0.042).
Interventions Characteristics
Key areas of intervention included medication error prevention—defined as pharmacist interventions aimed at identifying inappropriate prescriptions, duplications, or incorrect dosages at the point of prescribing—interaction review, and enhancement of primary and secondary adherence and those related to renal impairment (Table 3).
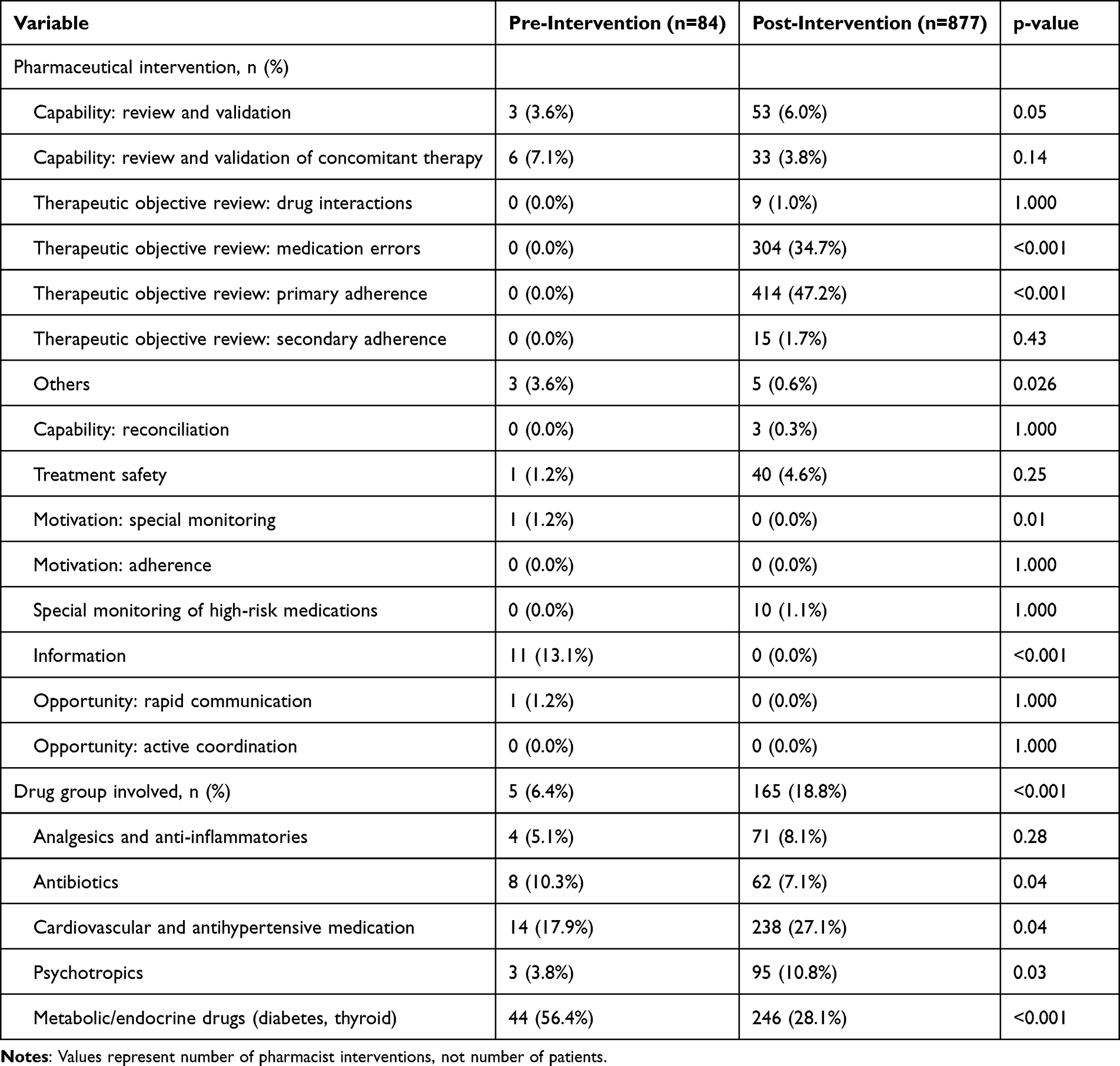 |
Table 3 Pharmaceutical Interventions and Involved Drug Groups |
Regarding drug groups implicated, there was a marked increase in the identification of issues related to cardiovascular and psychotropic medications, which rose from 17.9% and 10.3% in the pre-intervention period to 27.1% and 10.8%, respectively, post-intervention. This suggests an enhanced capacity to detect potentially inappropriate prescribing and drug-drug interactions, particularly in comorbid older adults.
Significantly, the increase in pharmaceutical interventions was especially prominent among patients classified as level 2, suggesting enhanced responsiveness in intermediate-complexity profiles.
The implementation of the SANPAT system was associated with significant improvements in key pharmacotherapeutic and clinical variables. The average number of pharmaceutical interventions increased markedly from 1.0 to 6.1 per patient (p < 0.001), reflecting enhanced pharmacist activity enabled by real-time alerting. The prevalence of polypharmacy and major polypharmacy rose from 75.0% to 89.8% and from 23.8% to 42.1%, respectively, likely due to the aging profile of the cohort (p < 0.01 and p < 0.001) as detailed in Table 4.
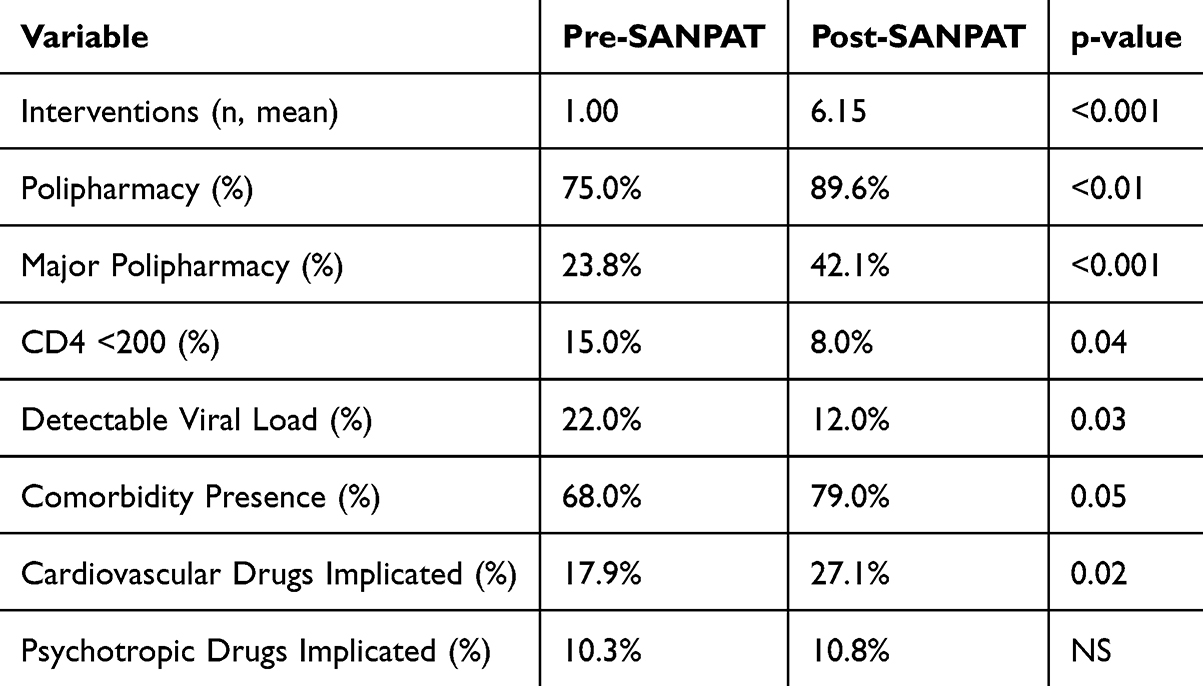 |
Table 4 Comparison of Key Outcomes Before and After SANPAT Implementation |
Interventions related to psychotropic drugs slightly increased post-intervention (from 10.3% to 10.8%), although this change did not reach statistical significance (p > 0.05), possibly due to limited sample size.
Implementation outcomes were assessed across the five RE-AIM dimensions (Table 5), with performance metrics summarized in Figure 3 and detailed below.
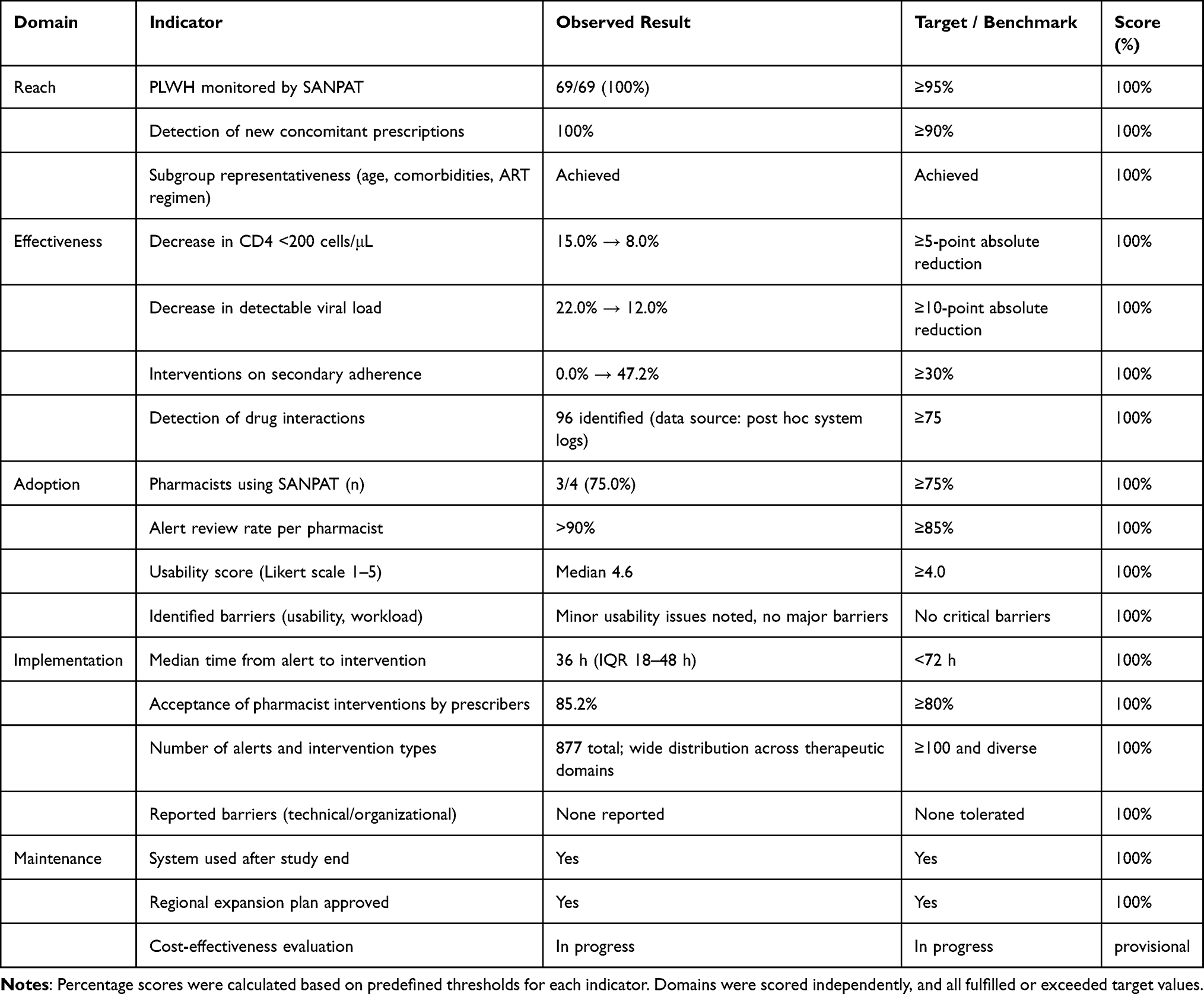 |
Table 5 RE-AIM Framework Evaluation of the SANPAT System Implementation |
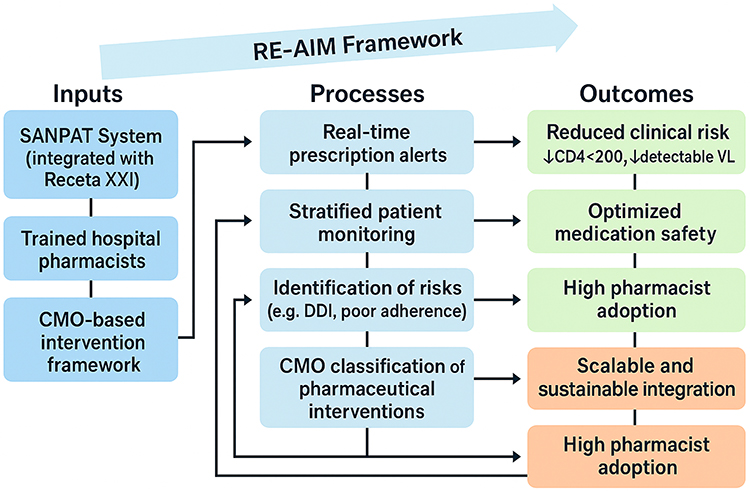 |
Figure 3 Conceptual Framework of SANPAT Implementation. This model illustrates how the SANPAT system, supported by trained pharmacists and a CMO-based intervention framework, enables real-time monitoring, identification of pharmacotherapeutic risks, and personalized interventions, ultimately improving safety, adherence, and implementation sustainability, within the RE-AIM evaluation framework. |
Reach was optimal, with 100% of eligible patients monitored by SANPAT during the post-intervention period (n = 69). The system successfully captured all new prescriptions and adherence-related events among patients ≥50 years old with polypharmacy or pharmacotherapeutic complexity. Subgroup analyses confirmed representativeness across comorbidity profiles, ART regimens, and levels of clinical risk.
Effectiveness was reflected in both clinical and behavioral indicators. The proportion of patients with CD4 <200 cells/μL declined from 15.0% to 8.0% (p = 0.04), and detectable viral load rates fell from 20.3% to 3.6% (p = 0.03). In parallel, the number of pharmacist interventions addressing secondary adherence rose from 0.0% to 47.2% (p < 0.001), supporting the hypothesis of SANPAT’s clinical utility.
Adoption was high: 83.3% (5/6) of pharmacists in the outpatient unit actively engaged with SANPAT, consistently reviewing alerts and recording interventions. The median alert review rate per pharmacist exceeded 90%. Usability was rated favorably by all respondents (median global satisfaction score: 4.6/5), based on structured feedback collected via an internally validated implementation survey.
Implementation outcomes showed robust system performance. The average time from alert generation to pharmacist intervention was 36 hours (IQR 18–44 h), and the intervention acceptance rate by prescribers reached 85.2%. Pharmacist actions spanned 877 events, with a broad distribution across therapeutic domains, demonstrating scalability and operational efficiency. Technical and workflow-related barriers were minimal, with no system downtimes reported during the study period.
Overall, RE-AIM scores surpassed predefined thresholds in all dimensions, confirming SANPAT’s dual capacity to generate measurable clinical benefits while achieving high adoption and feasibility within routine pharmaceutical care workflows.
Discussion
This study is the first to demonstrate the feasibility and impact of integrating a real-time prescription alert system (SANPAT) into a structured PC model for PLWH. Its main contribution lies in showing how digital tools can shift HIV pharmacotherapy from a reactive to a proactive model of care. SANPAT not only enabled timely identification of new prescriptions and adherence concerns, but also facilitated a significant increase in personalized pharmaceutical interventions—particularly in high-risk, aging patients with polypharmacy. This dual focus on clinical effectiveness and implementation success, evaluated through the RE-AIM framework, distinguishes this work from previous studies and positions SANPAT as a replicable model for digital transformation in HIV care. SANPAT notably enhances the “opportunity” dimension of the CMO model by enabling pharmacists to engage proactively at the point of prescribing, thereby facilitating timely, personalized interventions that would be unlikely under conventional care models.
While CDSS have been widely studied in other therapeutic domains, their use in HIV care remains limited. Prior implementations have often been isolated from structured care models and lacked integration into routine workflows. This study addresses those gaps by demonstrating how SANPAT, when linked to Receta XXI—the Andalusian public health e-prescribing platform—achieves both clinical relevance and operational feasibility. Furthermore, our use of the RE-AIM framework offers a comprehensive lens to evaluate the system’s impact across dimensions often overlooked in traditional trials. Compared to previous evidence focused on pharmacist adherence support or medication reconciliation, SANPAT expands the field by integrating digital automation with personalized clinical decision-making.
The marked increase in pharmaceutical interventions—from 84 to 877—speaks to the system’s ability to enhance pharmacists’ capacity without increasing workload. Notably, interventions addressing secondary adherence (47.2%) and medication errors (34.7%) underscore SANPAT’s value in mitigating risks that frequently go undetected in retrospective review models. Improvements in key clinical indicators, such as a reduction in CD4 <200 cells/μL and detectable viral load, further validate the intervention’s potential to contribute to better patient outcomes.
The observed rise in polypharmacy and major polypharmacy post-intervention likely reflects the natural aging of the cohort, yet also highlights the system’s role in identifying and addressing prescribing complexity.34–37 Increased interventions related to cardiovascular and psychotropic medications reinforce SANPAT’s utility in navigating comorbidities often under-prioritized in HIV care. These results are especially relevant given the known association between polypharmacy and adverse health outcomes in aging PLWH.38–40 In this way, the personalization of PC interventions was achieved through the validation of SANPAT alerts by pharmacists, in combination with the CMO stratification methodology, including motivational interviewing adapted to the pharmacotherapeutic objectives established at each moment, which allowed the interventions to be adapted to comorbidities, the ART regimen, the burden of polypharmacy, adherence patterns, and the overall level of complexity of each patient. In adittion, the unusually high RE-AIM scores observed, particularly in reach and adoption, likely reflect the specific context of implementation in a single highly motivated and specialized unit, where strong pharmacist engagement and close integration with existing workflows facilitated optimal performance; such results may not be directly reproducible in broader, less controlled settings. It should be acknowledged that predefined RE-AIM benchmarks were intentionally conservative, which may partly explain the uniformly high success rates observed.
Future studies should incorporate patient-reported outcomes, hospitalization rates, and long-term virologic suppression to fully capture the clinical and economic value of SANPAT.
This study has several methodological strengths. It was conducted prospectively under real-world conditions, ensuring high external validity. The classification of interventions using a validated CMO-based taxonomy and the RE-AIM framework added analytical depth beyond traditional outcome metrics.41 Full patient follow-up and integration into the existing digital infrastructure (Receta XXI) further support reproducibility.
However, several limitations must be acknowledged. The quasi-experimental before-and-after design limits causal inference, as secular trends or external factors may have influenced the outcomes. The study was conducted at a single site, potentially limiting generalizability—although the platform’s integration into a regional prescribing system strengthens scalability. In addition, the analysis focused on process measures (eg, intervention frequency, alert response), and did not assess hard clinical outcomes such as hospitalizations, quality of life, or long-term virologic suppression.
Additionally the quasi-experimental before–after design is inherently vulnerable to secular trends and unmeasured confounding, which may have influenced the observed outcomes. Second, the unequal sample sizes between the pre- and post-intervention groups reflect real-world implementation constraints and may have introduced bias. Third, given the exploratory nature of the study, no correction for multiple comparisons was applied; therefore, the risk of type I error cannot be excluded. These statistical findings should be interpreted with caution, as the final sample size did not reach the initially estimated target and no correction for multiple comparisons was applied. Additionally, a Hawthorne effect cannot be excluded, as both patients and clinicians may have modified their behavior due to awareness of being observed, potentially inflating adherence or safety outcomes.
Finally, although the study was conducted in a single center with a comprehensive patient cohort, the generalizability of the findings may be limited, and future multicenter studies with longer follow-up periods are needed to assess sustainability and scalability.
Future studies should pursue randomized controlled designs to isolate the causal impact of real-time interventions on clinical outcomes. Expanding SANPAT’s reach across multiple sites would strengthen external validity and assess implementation barriers at scale. Moreover, integration of artificial intelligence and machine learning may enable dynamic prioritization of alerts and predictive modeling based on patient history, adherence patterns, and pharmacogenomic data. Cost-effectiveness analyses will also be critical to inform broader policy adoption and health system planning.
Conclusion
This study shows the feasibility of integrating a real-time prescription alert system (SANPAT) into PC for PLWH. The system markedly increased detection and resolution of pharmacotherapeutic risks and supported personalized interventions, particularly in older patients with polypharmacy, while also improving key immunovirological markers. SANPAT should be considered a fundamental tool in the follow-up of these patients and holds promise for application in other chronic conditions in the future.
Acknowledgments
The authors would like to thank the Pharmacy Service staff and IT department at Hospital Universitario Virgen de Valme for their support in implementing the SANPAT system, specially Jose Maria Perez Gata and Agustin Vera. Special thanks to Alba Galindo Pineda. The SANPAT system was developed and implemented using internal resources from the Hospital Pharmacy Service at Hospital Universitario Virgen de Valme.
Author Contributions
RMV was responsible for drafting the original manuscript. The remaining authors reviewed and contributed to the text. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, data acquisition, analysis and interpretation, or all these areas. They all participated in drafting, revising, or critically reviewing the article, approved the final version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. HIV/AIDS. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids.
2. Milic J, Russwurm M, Cerezales Calvino A, Brañas F, Sánchez-Conde M, Guaraldi G. European cohorts of older HIV adults: POPPY, AGE(h)IV, GEPPO, COBRA and FUNCFRAIL. Eur Geriatr Med. 2019;10:247–257. doi:10.1007/s41999-019-00170-8
3. Antiretroviral therapy cohort C, May MT, Vehreschild -J-J. Survival of HIV-positive patients starting antiretroviral therapy between 1996 and 2013: a collaborative analysis of cohort studies. Lancet HIV. 2017;4:e349–e56. doi:10.1016/S2352-3018(17)30066-8
4. Guaraldi G, Pintassilgo I, Milic J, Mussini C. Managing antiretroviral therapy in the elderly HIV patient. Expert Rev Clin Pharmacol. 2018;11(12):1171–1181. doi:10.1080/17512433.2018.1549484
5. Mazzitelli M, Trunfio M, Scaglione V, et al. Association between anticholinergic burden and sleep quality in people living with HIV. Br J Clin Pharmacol. 2025. doi:10.1002/bcp.70272
6. Kim J, Nam HJ, Kim JY, et al. Aging with HIV: the burden of comorbidities, polypharmacy, and drug interactions in Korean people living with HIV aged ≥50 years. Infect Chemother. 2024;56(4):534–543. doi:10.3947/ic.2024.0132
7. Fernández-Castro I, Casar-Cocheteux C, Pernas-Pardavila H, Losada-Arias E, Antela A. Cross-sectional analysis of a cohort of people over 65 years of age living with HIV. Enferm Infecc Microbiol Clin. 2024;42(6):317–320. doi:10.1016/j.eimce.2024.04.001
8. Justice AC, Gordon KS, Skanderson M, et al. Nonantiretroviral polypharmacy and adverse health outcomes among HIV-infected and uninfected individuals. AIDS. 2018;32:739–749. doi:10.1097/QAD.0000000000001756
9. Justice AC, Gordon KS, Romero J, et al. Polypharmacy-associated risk of hospitalisation among people ageing with and without HIV: an observational study. Lancet Healthy Longev. 2021;2(10):e639–e650. doi:10.1016/S2666-7568(21)00206-3
10. Allavena C, Marzolini C. Polypharmacy and risk of admission to hospital in people ageing with HIV: what is the contribution of drug-drug interactions? Lancet Healthy Longev. 2021;2(10):e606–e607. doi:10.1016/S2666-7568(21)00227-0
11. Milinkovic A, Pereira B, Mazziteli M, et al. Delivering specialised care to people ageing with HIV in the UK: experience and evolution of services from 2009 to 2019. Lancet HIV. 2022;9(Suppl 1):S1. doi:10.1016/S2352-3018(22)00066-2
12. Zheng C, Meng J, Xiao X, Xie Y, Zhao D, Wang H. Polypharmacy, medication-related burden and antiretroviral therapy adherence in people living with HIV aged 50 and Above: a cross-sectional study in Hunan, China. Patient Prefer Adherence. 2022;16:41–49. doi:10.2147/PPA.S340621
13. Vinuesa-Hernando JM, Gimeno-Gracia M, Malo S, et al. Potentially inappropriate prescriptions and therapeutic complexity in older HIV patients with comorbidities. Int J Clin Pharm. 2021;43(5):1245–1250. doi:10.1007/s11096-021-01242-1
14. Marin S, Quiñones C, Codina-Jiménez C, et al. The management of polypharmacy in people living with HIV. AIDS Rev. 2023;25(1):27–40. doi:10.24875/AIDSRev.M23000059
15. Ahmed A, Abdulelah Dujaili J, Rehman IU, et al. Effect of pharmacist care on clinical outcomes among people living with HIV/AIDS: a systematic review and meta-analysis. Res Social Adm Pharm. 2022;18(6):2962–2980. doi:10.1016/j.sapharm.2021.07.020
16. McNicholl IR, Gandhi M, Hare CB, Greene M, Pierluissi E. A pharmacist-led program to evaluate and reduce polypharmacy and potentially inappropriate prescribing in older HIV-positive patients. Pharmacotherapy. 2017;37(12):1498–1506. doi:10.1002/phar.2043
17. Cope RJ, Fischetti BS, Kavanagh RK, Lepa TM, Sorbera MA. Safety and efficacy of weight-loss pharmacotherapy in persons living with HIV: a review of the literature and potential drug-drug interactions with antiretroviral therapy. Pharmacotherapy. 2019;39(12):1204–1215. doi:10.1002/phar.2342
18. Morante-Ruiz M, Sanabria-Giron PC, Rubio-Martin R, et al. A perspective on frailty and its predisposing factors among people living with HIV. Curr HIV Res. 2024;22(6):349–353. doi:10.2174/011570162X335757241111062709
19. Hepler CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. 1990;47:533–543.
20. Morillo-Verdugo R, Robustillo-Cortes MLA, Navarro-Ruiz A, et al. Clinical impact of the capacity-motivation-opportunity pharmacist-led intervention in people living with HIV in Spain, 2019-2020. J Multidiscip Healthc. 2022;15:1203–1211. doi:10.2147/jmdh.S361305
21. Morillo-Verdugo R, Lazaro-Lopez A, Alonso-Grandes E, et al. Patient experience evaluation of the CMO-based pharmaceutical care model vs usual care in people living with HIV. J Multidiscip Healthc. 2022;15:2991–3003. doi:10.2147/JMDH.S392398
22. Li H, Naqvi IA, Strobino K, Malhotra S. Clinical telepharmacy: addressing care gaps in diabetes management for an underserved urban population using a collaborative care model. Telemed J E Health. 2024;30(7):e1923–e1926. doi:10.1089/tmj.2023.0589
23. Worrall C, Shirley D, Bullard J, Dao A, Morrisette T. Impact of a clinical pharmacist-led, artificial intelligence-supported medication adherence program on medication adherence performance, chronic disease control measures, and cost savings. J Am Pharm Assoc. 2024;17:102271. doi:10.1016/j.japh.2024.102271
24. Dohrn A, Hoskins R, Collier L, Kennelty K. Evaluation of a telehealth-based pharmacist led chronic care management program. J Pharm Pract. 2024;37(4):933–939. doi:10.1177/08971900231196624
25. Bektay MY, Buker Cakir A, Gursu M, Kazancioglu R, Izzettin FV. An assessment of different decision support software from the perspective of potential drug-drug interactions in patients with chronic kidney diseases. Pharmaceuticals. 2024;17(5):562. doi:10.3390/ph17050562
26. Bektay MY, Seker Z, Eke HK, Turk HM, Izzettin FV. Comparison of different decision support software programs in perspective of potential drug-drug interactions in the oncology clinic. J Oncol Pharm Pract. 2023;29(5):1178–1186. doi:10.1177/10781552221104814
27. Newton N, Bamgboje-Ayodele A, Forsyth R, Tariq A, Baysari MT. How Are clinicians’ acceptance and use of clinical decision support systems evaluated over time? A systematic review. Stud Health Technol Inform. 2024;310:259–263. doi:10.3233/SHTI230967
28. Grechuta K, Shokouh P, Alhussein A, et al. Benefits of clinical decision support systems for the management of noncommunicable chronic diseases: targeted literature review. Interact J Med Res. 2024;13:e58036. doi:10.2196/58036
29. Pawloski PA, Brooks GA, Nielsen ME, Olson-Bullis BA. A systematic review of clinical decision support systems for clinical oncology practice. J Natl Compr Canc Netw. 2019;17(4):331–338. doi:10.6004/jnccn.2018.7104
30. Delara M, Murray L, Jafari B, et al. Prevalence and factors associated with polypharmacy: a systematic review and Meta-analysis. BMC Geriatr. 2022;22(1):601. Erratum in: BMC Geriatr. 2022 Sep 12;22(1):742. doi: 10.1186/s12877-022-03388-7. doi:10.1186/s12877-022-03279-x
31. Prados-Torres A, Poblador-Plou B, Calderón-Larrañaga A, et al. Multimorbidity patterns in primary care: interactions among chronic diseases using factor analysis. PLoS One. 2012;7:e32190. doi:10.1371/journal.pone.0032190
32. Morillo Verdugo R, Villarreal Arevalo AL, Alvarez De Sotomayor M, Robustillo Cortes ML. Development of a taxonomy for pharmaceutical interventions in HIV+ patients based on the CMO model. Farm Hosp. 2016;40(n06):544–568. English. doi:10.7399/fh.2016.40.6.10567
33. Glasgow RE, Harden SM, Gaglio B, et al. RE-AIM planning and evaluation framework: adapting to new science and practice with a 20-year review. Front Public Health. 2019;7:64. doi:10.3389/fpubh.2019.00064
34. Sutton RT, Pincock D, Baumgart DC, Sadowski DC, Fedorak RN, Kroeker KI. An overview of clinical decision support systems: benefits, risks, and strategies for success. NPJ Digit Med. 2020;3:17. doi:10.1038/s41746-020-0221-y
35. Gordon NP, Hornbrook MC. Differences in access to and preferences for using patient portals and other ehealth technologies based on race, ethnicity, and age: a database and survey study of seniors in a large health plan. J Med Internet Res. 2016;18(3):e50. doi:10.2196/jmir.5105
36. Oluoch T, Katana A, Kwaro D, et al. Effect of a clinical decision support system on early action on immunological treatment failure in patients with HIV in Kenya: a cluster randomised controlled trial. Lancet HIV. 2016;3(2):e76–84. doi:10.1016/S2352-3018(15)00242-8
37. Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. 1999;89(9):1322–1327. doi:10.2105/ajph.89.9.1322
38. Mugavero MJ, Amico KR, Horn T, Thompson MA. The state of engagement in HIV care in the United States: from cascade to continuum to control. Clin Infect Dis. 2013;57(8):1164–1171. doi:10.1093/cid/cit420
39. Budak JZ, Scott JD, Dhanireddy S, Wood BR. The impact of COVID-19 on HIV care provided via telemedicine-past, present, and future. Curr HIV/AIDS Rep. 2021;18(2):98–104. doi:10.1007/s11904-021-00543-4
40. Kemp CG, Velloza J. Implementation of eHealth interventions across the hiv care cascade: a review of recent research. Curr HIV/AIDS Rep. 2018;15(6):403–413. doi:10.1007/s11904-018-0415-y
41. Cooper JB, Scotti A, Carr ML. Implementing medicare education for medication access: a review of the literature using the RE-AIM framework. Res Social Adm Pharm. 2023;19(1):16–27. doi:10.1016/j.sapharm.2022.08.013
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Experiences of Antiretroviral Therapy Initiation Among HIV-Positive Adults in Ethiopia: A Descriptive Phenomenological Design
Tefera E, Mavhandu-Mudzusi AH
HIV/AIDS - Research and Palliative Care 2022, 14:243-254
Published Date: 24 May 2022
Risk Factors for Suboptimal Adherence Identified by Patient-Reported Outcomes Assessments in Routine HIV Care at 2 North American Clinics
Short D, Wang X, Suri S, Hsu TK, Jones B, Fredericksen RJ, Crane HM, Musten A, Bacon J, Wang Y, Gough KA, Ramgopal M, Berry J, Lober WB
Patient Preference and Adherence 2022, 16:2461-2472
Published Date: 5 September 2022
An Observational Cohort Study to Evaluate the Impact of a Tailored Medicines Optimisation Service on Medication Use, Accident and Emergency Department Visits, and Admissions Among Patients Identified with Medication Support Needs in Secondary Care
Harrap N, Wells J, Howes K, Kayyali R
Patient Preference and Adherence 2022, 16:2947-2961
Published Date: 28 October 2022
Virological Outcomes After Switching to Abacavir/Lamivudine/Dolutegravir Combined with Adherence Support in People Living with HIV with Poor Adherence: A Phase IV, Multicentre Randomized Prospective Open Label Study (TriiADD-CTN 286)
Klein MB, Young J, Ortiz-Paredes D, Wang S, Walmsley S, Wong A, Martel-Laferrière V, Pick N, Conway B, Angel J, Baril JG, Fraser C, Lebouché B, Tan DH, Sandre R, Trottier S, Peiris H, Jayaraman J, Singer J
Patient Preference and Adherence 2022, 16:3267-3281
Published Date: 13 December 2022
Impact of a CMO-Based Pharmaceutical Care Model on 3-HIT Criteria in Older People Living with HIV: The DIS3HIT Project
Roldán Galnares M, Morillo-Verdugo R, Robustillo-Cortes MDLA, Vélez-Díaz-Pallarés M, Company Albir MJ, Proy Vega B, Losa López L, Marín Ventura L, Ferris Villanueva M, Mora Atorrasagasti O, Gutiérrez E
Patient Preference and Adherence 2026, 20:569460
Published Date: 30 January 2026