Back to Journals » ClinicoEconomics and Outcomes Research » Volume 18
The Socioeconomic Impact of Long-Acting Injectable Buprenorphine
Authors Rasche SE, Batchelor GOW, Montgomery C, Sumnall HR ![]() , Mogford D
, Mogford D ![]()
Received 20 December 2025
Accepted for publication 3 April 2026
Published 20 May 2026 Volume 2026:18 590462
DOI https://doi.org/10.2147/CEOR.S590462
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Samuel E Rasche,1 George OW Batchelor,1 Catharine Montgomery,2 Harry R Sumnall,2 Daniel Mogford3
1Edge Health, London, UK; 2School of Psychology, Liverpool John Moores University, Liverpool, UK; 3Camurus Ltd., Cambridge, UK
Correspondence: Samuel E Rasche, Email [email protected]
Purpose: To assess the socioeconomic impact of increased uptake of long-acting injectable buprenorphine (LAIB) for opioid use disorder (OUD) in England.
Materials and Methods: A cost–benefit analysis was conducted from a societal perspective over a one-year time horizon. An economic model compared existing standard of care for OUD with a scenario in which a proportion of individuals switched to LAIB and additional individuals not currently in treatment initiated care with LAIB, based on uptake and retention assumptions. Areas of impact (e.g., crime, healthcare, and employment) were identified and quantified using a targeted literature review and published unit cost estimates.
Results: Assuming approximately 30,000 people could receive LAIB, the annual cost is estimated at £ 77 million, while the projected benefits total £ 236 million, resulting in a benefit–cost ratio of 3.1. The greatest savings are expected to be derived from reductions in crime and incarceration, followed by socioeconomic gains through increased employment, improved quality of life, prevented fatalities, decreased healthcare burden, and reduced social care costs.
Conclusion: Despite higher acquisition costs than current standard treatments, LAIB was estimated to be cost-beneficial, with potential to improve outcomes for individuals while generating substantial value for society.
Keywords: opioids, disorders due to use of opioids, long-acting injectable buprenorphine, methadone, sublingual buprenorphine
Introduction
Opioid use disorder (OUD) is a complex and chronic condition that is characterised by compulsive use of opioids, such as heroin, prescription medicines, and synthetic opioids.1 The condition is associated with a societal burden, as individuals with OUD experience disproportionately high rates of morbidity, mortality, and social harms, such as unemployment and having a housing related need.2,3 Family relationships may also suffer, with OUD associated with parental neglect, care orders, and intergenerational cycles of substance use.4 Furthermore, non-medical opioid use is controlled under the Misuse of Drugs Act,5 and associated acquisitive offences lead to criminal justice involvement.6,7 The combined impact of these factors reinforces marginalisation and stigma, making recovery challenging.8,9
Pharmacological treatments, most prominently opioid agonist therapies (OAT) such as methadone and sublingual buprenorphine, have proven to be effective in managing OUD.1,10 These treatments differ in their pharmacological profiles, and access and prescriptions are covered by different regulatory requirements internationally. They require daily dosing, are often subject to restrictive dispensing arrangements, and may involve regular monitoring. In England, current guidance recommends daily supervised consumption for people entering treatment for a minimum of three months, after which the level of supervision is determined by individual clinical assessment.10,11 Some of these treatment practices, such as observed dosing, frequent attendance requirements, and urine drug screening, may be perceived as intrusive or burdensome by some individuals.12–14 This can create barriers to treatment entry or result in unplanned treatment exit.15,16 With an estimated unmet treatment need of 61% for opioid use, 45% for co-use of opioids and crack in England (2023/24), and the proportion of unplanned treatment exits at 37% (2024/25),17 engaging and retaining people in treatment is a public health priority.
The UK government’s From Harm to Hope 10-year drugs strategy set out an ambition to rebuild treatment services, with the aim of supporting an additional 24,000 people into long-term recovery.18 The strategy also linked recovery to broader socioeconomic outcomes, including reduced crime, increased sustained employment, and access to secure housing, while aiming to prevent nearly 1000 drug-related deaths. It included an ambition to increase the provision of long-acting injectable buprenorphine (LAIB). Use of this medication can potentially overcome some of the challenges associated with existing OAT, such as daily medication management, and the risk of diversion.19–21 LAIB is administered once per week or month depending on the formulation, thereby reducing the treatment burden and potentially increasing retention. It was first made available in the UK in 2019,22 but uptake has remained limited; in 2022, approximately 2.1% of people receiving OAT in the UK were prescribed LAIB, with variation across UK nations,23 but precise figures for England specifically are not routinely reported. In other countries, however, greater uptake has been observed. The introduction of LAIB in Australia, alongside broader policy and service delivery changes, was associated with a steady increase in OAT uptake.24 Similar increases have been observed in Finland,25 suggesting that LAIB can reach individuals who might otherwise not engage with treatment services.
Increased engagement and sustained retention in treatment may, in turn, contribute to several broader health, social, and economic benefits. Receiving OAT has been associated with reductions in crime,26,27 foster care placements,28 and drug-related fatalities.29–32 Studies have also shown that receiving treatment for OUD leads to significant improvements in quality of life, reflected in the quality-adjusted life year (QALY) metric.33 When considering LAIB specifically in comparison to other OAT, it has been associated with higher QALY gains compared to methadone and sublingual buprenorphine (approximately 0.02 incremental QALYs over 24 weeks)34 and reduced healthcare utilisation.35 Benefits of LAIB have also been observed in correctional settings, with reports of reduced recidivism36 and lower staffing demands due to reduced dosing frequency, supervision requirements, and escorting.37–40 Furthermore, by removing the daily requirement of managing treatment, it may reduce time and logistical burdens, which could facilitate workforce participation for some individuals with OUD.19,41–45 Finally, LAIB has also been associated with more stable plasma concentrations,46 reduced risk related to managing take-home doses such as loss, misuse, or diversion,19–21 and greater dosing flexibility.41
Overall, these studies suggest that LAIB may generate a range of individual and societal benefits. However, LAIB has higher acquisition costs than daily oral OATs such as methadone or sublingual buprenorphine, which are the current standard of care. It is therefore important to evaluate whether these additional costs are justified by the benefits. This study presents a health and socioeconomic cost–benefit analysis of increased uptake of LAIB in England to address this question.
Method
Design and Model Overview
To estimate the costs and benefits of implementing LAIB in England, an analytic model was developed in Microsoft Excel. The analysis was structured as a cost–benefit analysis from a societal perspective. In line with economic evaluation practice,47,48 the analysis involved three steps: (a) identifying the areas in which LAIB could generate costs or benefits, (b) estimating the expected change in these outcomes associated with increased uptake of LAIB, drawing on published evidence; and (c) assigning monetary values to each outcome using unit costs from publicly available sources and academic literature in order to calculate total costs and benefits. The time horizon of the model was set to one year.
Target Population and Comparators
The model compared LAIB with the current standard of care in England, defined as existing OATs (predominantly methadone and sublingual buprenorphine) and their treatment pathways. For individuals currently not engaged in treatment, the comparison was between remaining untreated versus initiating LAIB.
The target population who could receive LAIB was defined in three stages. First, prevalence rates of OUD, obtained from the literature, were applied to Office for National Statistics (ONS) population estimates for England49 to calculate the total number of people with OUD. Next, published data from the Office for Health Improvement & Disparities (OHID) on the number of individuals currently in treatment for OUD3 was used to divide the population into in-treatment and out-of-treatment groups.
Having determined the number of people receiving treatment and not receiving treatment, the next step was to determine how many individuals in each group could receive LAIB. Estimating this figure required several assumptions. Firstly, not all of those in the in-treatment group are expected to switch to LAIB. There are various reasons for this, including personal preference, clinical decision-making and need for clinical support.19,21 Based on real-world data from Australia, where approximately 25% of people in treatment were receiving LAIB in 2022,24 we assumed that 25% of people currently in OAT in England could switch to LAIB. It should be noted that this observed uptake reflects a policy and service delivery context specific to Australia. Uptake could potentially be higher, as illustrated by Finnish data, where reports suggest that 60–65% of people on OAT are receiving LAIB.23 We adopted the lower Australian estimate as a conservative assumption. To further avoid overstating the number of people likely to switch in the English context, we applied an additional adjustment using a retention rate of 70% at one year of LAIB treatment, which was derived from a mix of randomised controlled trials (RCT), open-label trials, and observational studies.35,44,50 Finally, to model the type of OAT from which individuals would switch, we used the current treatment distribution in England, where approximately 70% of people in OAT receive methadone and 30% receive sublingual buprenorphine.10
To capture the potential engagement of people currently not in treatment, uptake estimates of LAIB were again derived from Bharat et al24 and applied to the English population (0.8 per 100,000 per month), yielding an estimate of new LAIB treatment initiations. The combined in-treatment switchers and out-of-treatment initiators formed the total estimated number of people receiving LAIB in a given year.
Outcomes and Cost Estimation
Evidence to inform model structure, parameter values and unit costs was obtained through a targeted review of the academic and grey literature. The following areas where LAIB could have an impact were identified: employment, criminal justice, social care, healthcare, fatalities, and quality of life (Table 1). The outcomes were costed by applying the appropriate unit costs, resulting in a total estimate of the costs (or costs saved) of each outcome. Where multiple estimates existed, conservative values were chosen. Costs were inflated to 2024 GBP if necessary, using the HM Treasury GDP deflator.51 Using the target population estimate, the potential impact of LAIB was assessed by mapping the relevant subpopulation to the identified outcomes. That is, not all benefits apply to the entire population; for example, some may relate specifically to people who are currently not receiving treatment.
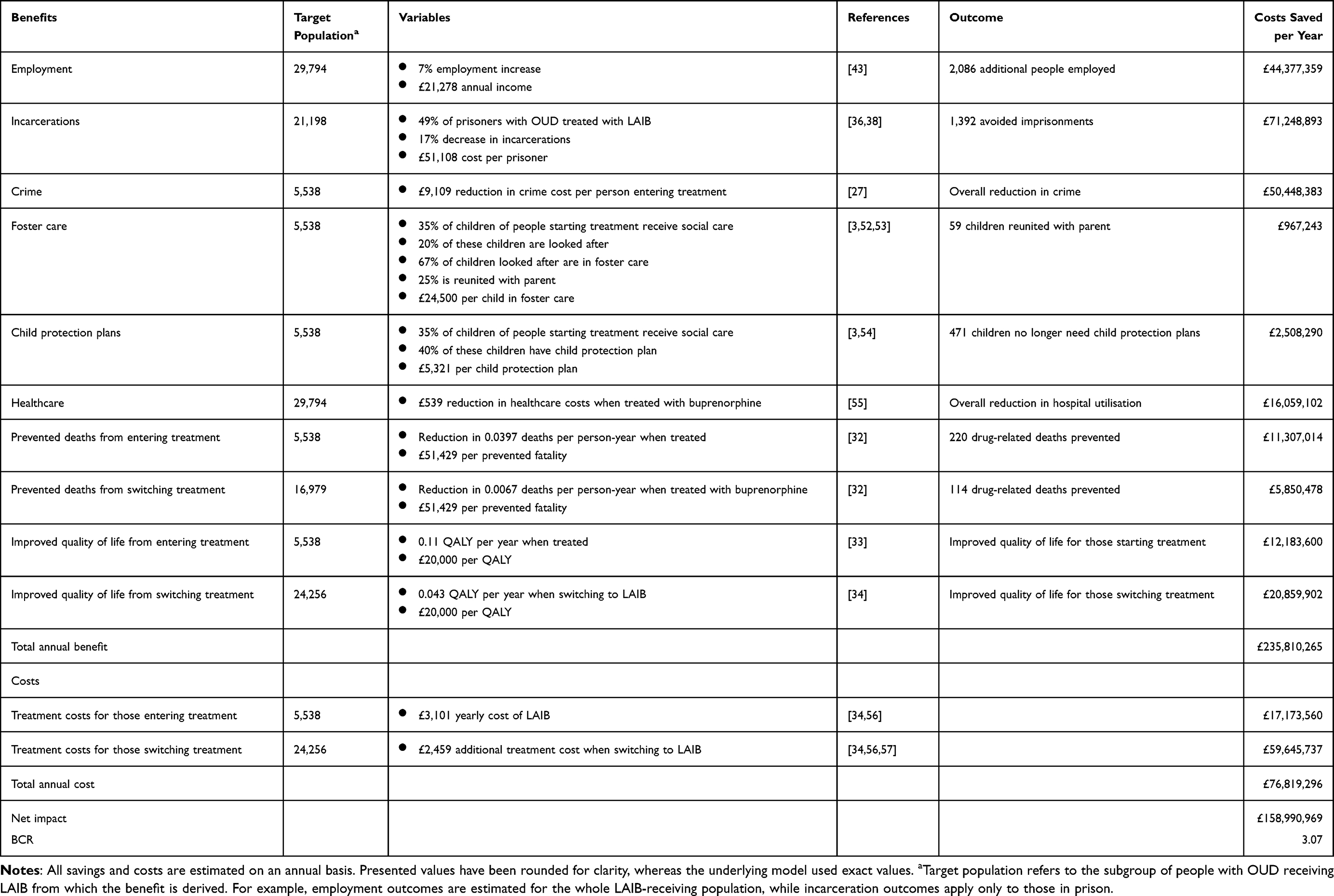 |
Table 1 Estimated Annual Benefits and Costs of LAIB |
Employment
To estimate the income that could be generated by individuals with OUD who become employed following LAIB treatment, several assumptions were required. It was assumed that the benefit of LAIB regarding employment applies to all individuals receiving LAIB treatment, because both out-of-treatment and in-treatment OUD cases may benefit from the removal of daily doses. Improved employment rates with LAIB were obtained from clinical trial evidence, including a Phase 3 randomised, double-blind, placebo-controlled trial42,44 and a subsequent open-label extension study without an active comparator.43 It should be noted that no studies to date, to our knowledge, have directly compared employment outcomes between LAIB and other OAT. The unit cost for employment was defined as gross income, which was assumed to be lower than average (60% of the median UK income) as many people with OUD are likely to have employment gaps, limited education or work experience, hold criminal records, and experience public and structural stigma.58
Criminal Justice
Treating OUD in prison with any buprenorphine formulation can help reduce recidivism.36,59 In a recent study, Mlilo et al36 found that 21% of inmates treated with LAIB were re-incarcerated, compared to 38% of those treated with sublingual buprenorphine. Based on this, the model assumed a 17% reduction in re-incarcerations associated with LAIB. Furthermore, data from Forth Valley Prisons in Scotland indicated that, with ready availability and system support, 49% of prisoners in OAT were treated with LAIB.38 A similar uptake was assumed for England. These figures were applied to the prison population currently receiving OAT, enabling an estimate of the number of prison sentences potentially avoided with wider LAIB implementation. For unit costs, a yearly average cost of £51,108 per prisoner was used in the calculation.60 Note that this does not consider sentence length or prison type due to lack of more granular data. Other potential benefits associated with LAIB in prison settings, such as staff resource savings,37–40 were not included.
To estimate the impact of LAIB on crime, only people entering treatment were considered, as the impact of LAIB on crime compared to other treatments is yet to be determined (see Marsden et al34 for preliminary findings). Casey et al27 found a reduction in crime costs of £6,189 per individual with OUD in treatment for a year, which was used as the unit cost (after correcting for inflation). Similar figures (£5,132-£7,321) were estimated by Godfrey et al,61 which were used in the sensitivity analysis (Table S1). To test the reliability of the results, offence rates obtained from Lind et al26 were used; they reported reductions in robberies by 12%, domestic burglary by 57%, and vehicle theft by 56% among individuals receiving treatment compared to no treatment. These reduction rates were multiplied by the population entering treatment and the corresponding UK offence costs (£11,320 for robbery, £5,930 for burglary, £10,290 for vehicle theft, obtained from Heeks et al).62
Social Care
Receiving treatment for substance misuse has been associated with improved family dynamics and an increased likelihood of reunification of the family.63 The availability of LAIB, which is assumed to increase the number of people receiving treatment, may therefore help reduce the burden on child social care.28
First, the impact of LAIB on foster care was assessed. This benefit was assumed to be derived from out-of-treatment individuals who are brought into treatment with the availability of LAIB, as studies comparing the impact of different treatments on social care have yet to be conducted. Data on the parental status of people starting treatment and on children requiring help was obtained from OHID.3 The following rates were applied: 32% of individuals starting treatment were assumed to be parents, with an average of 1.9 children per parent. 35% of children of people starting treatment are in contact with social care; of these, 20% are children looked after, and 67% of children looked after are in foster care.3,52 These figures apply to all individuals in substance misuse treatment but are applied here to those with OUD due to the lack of more granular data. It was also assumed that 25% of people entering treatment are reunited with their child.53 Unit costs of £24,500 annually per child in foster care were used.64 Other types of placements were not costed.
Beyond foster care, the burden on social care can also be decreased by reducing the need for child protection plans. Of the children receiving help (that is, 35% of children of people starting treatment), 40% have child protection plans, which are estimated to cost £5,321 per child.3,54 The assumption was made that protection plans are no longer needed when receiving LAIB treatment.
Healthcare
Acute healthcare utilisation is significantly reduced when treated with methadone, sublingual or long-acting buprenorphine.65,66 Buprenorphine has been associated with lower healthcare costs compared to methadone.35,55,67 It was therefore assumed that LAIB may lead to a reduced burden on healthcare and significant cost savings by (a) having more people enter treatment, and (b) by treating more people with LAIB instead of other treatments.
Unit costs were obtained from Domzaridou et al,55 who reported a £539 reduction in healthcare costs per person-year when treated with buprenorphine instead of methadone. However, since recent real-world evidence has shown even greater cost savings with LAIB specifically compared to other treatments,35 and entering treatment is also associated with reduced hospital utilisation,65,66 the unit cost was applied to the entire cohort treated with LAIB, rather than just those switching from methadone.
Drug-Related Deaths
Exact drug mortality rates differ per study; we therefore used estimates from a meta-analysis by Ma et al,32 who reported all-cause mortality rates of 0.92 per 100 person-years when receiving treatment, and 4.89 per 100 person-years when not receiving treatment. The difference (0.0397 deaths per person-year) was applied to the number of people entering treatment to estimate the number of prevented fatalities. Mortality also depends on treatment type; deaths are significantly higher among methadone recipients than those receiving buprenorphine.68 Ma et al32 estimated all-cause mortality rates of 0.38 per 100 person-years for buprenorphine and 1.05 per 100 person-years for methadone. On this basis, switching from methadone to buprenorphine was assumed to reduce mortality by 0.0067 deaths per person-year. Unit costs were estimated using a “value of a prevented fatality” (VPF) of £1.8m, which is regarded as conservative.69 To obtain yearly figures, the VPF value was divided by the additional years lived when recovered (35 years), based on the average age of opioid-related fatalities (approximately 45 years70) and average life expectancy in the general population (80 years).
Quality of Life
Studies have shown that receiving treatment for OUD leads to significant improvements in quality of life, reflected in the QALY metric. Schackman et al33 found that receiving buprenorphine treatment resulted in 1.58 QALYs over a 24-month period, compared to 1.36 QALYs for those not receiving treatment. We therefore assumed a 0.11 QALY gain per year when entering treatment. More recently, Marsden et al34 found that LAIB specifically was associated with higher QALY gains (increase of 0.02) compared to other OAT in a 24-week period. This estimate was scaled up to a yearly value assuming linear gains; a QALY gain of 0.043 per year was used for those switching treatment. For unit costs, we applied the lower threshold of £20,000 per QALY.71
Treatment Costs
Treatment costs were calculated for (a) individuals entering treatment with LAIB and (b) individuals switching from existing OATs to LAIB, with incremental costs applied in the latter case. Based on the UK list price, the assumed monthly cost of LAIB was £239.70 plus £18.72 in associated administration costs, whereas current treatment options were estimated at £36.00 per month plus £17.50 monitoring costs, assuming a daily dose of 100 mL methadone or 16 mg sublingual buprenorphine.34,56,57 Note that these figures exclude supervised pick-up or pharmacy dispensing fees.
All quantified benefits were summed to calculate the total gross benefit. Having estimated the benefits and costs, a benefit–cost ratio (BCR) was calculated as:
A ratio lower than 1 indicates that costs exceed the benefits, while a ratio above 1 indicates that the intervention generates more value than costs. Finally, a sensitivity analysis was conducted to assess the robustness of the findings; parameters were varied within plausible ranges derived from the literature. This is shown in Table S1.
Results
Population
Using mortality data, Jones et al72 estimated an overall OUD prevalence of 0.82% among 15–64-year-olds in England. Applying this rate to the current 15–64-year-olds population (N = 36,964,892),49 resulted in an estimate of 303,112 cases of OUD in England (Figure 1). Other studies have found similar, though slightly lower, estimates of OUD in 2016/201773 and 2018/2019.74 The latter source also suggests that opioid use in England is increasing over time, supporting the plausibility of our estimate. Furthermore, based on data indicating that 138,604 people are currently receiving treatment for OUD in England,3 it was estimated that approximately 54% of individuals with OUD (N = 164,508) are currently not engaged in treatment (Figure 1).
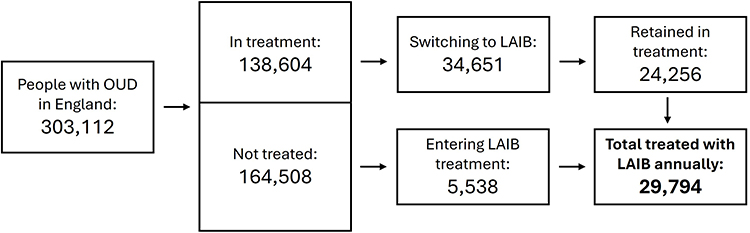 |
Figure 1 Projected uptake of LAIB in England. This figure illustrates the estimated OUD population in England and, based on the presented model, the expected annual uptake of LAIB in England. Bold text denotes the total estimated annual LAIB treatment population. |
Next, we estimated that 24,256 people currently in treatment could switch to LAIB over the course of a year (Figure 1), which was derived from an assumed uptake rate of 25%24 and a retention rate of 70%,35,44,50 applied to the current treated population (N = 138,604).3 Finally, it was calculated that 5,538 additional people per year are expected to be treated with LAIB from the OUD population who are currently out of treatment (Figure 1). This was based on figures obtained from Bharat et al;24 in line with how the rate is reported in the Australian population, the rate was applied to the whole population of England (N = 57,690,300).49
By combining the number of people in treatment switching to LAIB and those out of treatment starting LAIB treatment, the total number of people who could be treated with LAIB in a year was estimated to be 29,794 in England (Figure 1).
Impact and Cost Estimates of Identified Outcomes
After determining the population who could potentially be treated with LAIB, areas where benefits and costs may arise were identified. These included employment, crime and incarceration, child social care, healthcare, drug-related deaths, quality of life, and treatment costs.
Impact on Employment
Based on a single-arm study by Ling et al,43 an increase of 7% in employment with LAIB was assumed; this was applied to the entire treatment cohort (N = 29,794) at an income of £21,278 per year, resulting in an estimated £44.4m in gross income generated by employment (Table 1).
Impact on the Justice System
With 21,198 people treated for OUD in prison, and 78.5% receiving pharmacological treatment, it was estimated that 8,200 prisoners could be treated with LAIB (21,198 × 0.785×0.492).38,75 Using the reduction rate of 17% in re-incarcerations with LAIB,36 a cost saving of £71.2m in avoided prison sentences was estimated (Table 1).
The expectation that the availability of LAIB increases the number of people with OUD entering treatment (N = 5,538) leads to significant cost savings through the acknowledged positive impact of treatment on crime costs; using the estimate of Casey et al27 suggests cost savings of £50.4m after correcting for inflation (£6189 × 1.47 = £9,109 saved per person entering treatment) (Table 1). The alternative estimation approach, based on crime reduction rates obtained from rates from Lind et al,26 resulted in a comparable estimate of savings (£58.2m).
Impact on Social Care
Among the people newly entering treatment (N = 5,538), the model estimated that they have 3,367 children, of whom 1,178 require support. Of these, 236 children were estimated to be in state care, with 158 in foster care. Applying the reunification rate of 25%53 suggests that 59 children could be reunited with a parent, 39 of whom are currently in foster care. This corresponds to an estimated annual saving of £1.0m due to reduced foster care use with the availability of LAIB. Furthermore, an estimated 471 children would no longer require child protection plans, resulting in £2.5m costs saved. Taken together, £4.6m could potentially be saved in child social care when increasing the engagement with LAIB treatment (Table 1).
Impact on Hospitalisations
Using the estimated per-person cost saving of £539,55 and applying this to the 29,794 individuals who could be treated with LAIB, the model estimated an annual healthcare cost reduction of £16.1m (Table 1).
Impact on Drug-Related Deaths
Applying a rate of 0.0397 deaths per person-year32 to 5,538 individuals entering treatment suggests that approximately 220 deaths could be avoided annually, corresponding to savings of £11.3m. Moreover, applying the reduced mortality rate related to switching from methadone treatment (0.0067 deaths per person-year32) to 16,979 people equated to 114 deaths prevented annually, with associated cost savings of £5.9m. Taken together, LAIB could potentially prevent 334 drug-related deaths in one year, with cost savings of £17.2m (Table 1).
Improved Quality of Life Due to Treatment
A QALY gain of 0.11 was used to estimate quality of life improvements related to entering treatment (N = 5,538),33 resulting in £12.2m. Assuming a 0.043 QALY gain per year for those switching treatment,34 a benefit of 20.9m was found for the switching cohort (N = 24,256). Taken together, the estimated QALY gains associated with LAIB translated into annual savings of £33.0m (Table 1).
Additional Treatment Costs
As the number of people receiving treatment is expected to increase with LAIB, so too does the overall cost of treatment. The yearly cost of LAIB was estimated at £3,101 (including administration costs), resulting in a total treatment cost of £17.2m per year for new entrants (N = 5,538). In addition, LAIB was found to have a higher medicine acquisition cost than methadone or sublingual buprenorphine. For those switching treatment (N = 24,256), the average annual cost for current treatments of methadone or sublingual buprenorphine was estimated at £642 (including administration costs); hence a cost difference of £2,444 between LAIB and current regimens resulted in a total cost of £59.6m for those switching treatment. Taken together, the additional treatment costs associated with LAIB were estimated at £76.8m (Table 1).
Benefit–Cost Ratio
The overall BCR was calculated by dividing total benefits of £235.8m by total costs of £76.8m, yielding a BCR of 3.1. This indicates that increased LAIB uptake in England could deliver substantial socioeconomic benefits while improving treatment outcomes, representing a cost-beneficial strategy.
Assumptions were based on what appeared most reasonable given the current emerging evidence base. However, it is valuable to explore how the BCR might vary under different assumptions. Therefore, a sensitivity analysis was conducted (Table S1), which showed a BCR ranging from 2.8 to 3.6 showing that LAIB was cost-beneficial under more strict scenarios as well as a potential for greater benefit.
Discussion
This study estimated the socioeconomic and health impact of increasing the uptake of LAIB as a treatment for OUD in England. Despite higher treatment costs compared with traditional therapies such as methadone or sublingual buprenorphine, LAIB was associated with substantial potential benefits, including reduced crime and incarcerations, increased employment, fewer fatalities and hospitalisations, reduced burden on social care, and improved quality of life. The annual cost of implementing LAIB was estimated at £76.8m, while the projected assumed annual benefits amounted to £235.8m, resulting in a net annual benefit of £159.0m and a BCR of 3.1. These findings suggest that LAIB may represent an economically viable public health investment in England while improving outcomes for individuals.
Among the various domains evaluated, the most substantial benefits stem from reduced criminal justice costs. These were estimated based on reductions in recidivism and crime, but such outcomes can also lead to fewer police interventions, court appearances, and imprisonments, which are particularly relevant given the current pressures on the justice system.76 While LAIB may not directly influence imprisonment rates (which are largely determined by sentencing and justice policy), it can contribute to broader criminal justice savings by reducing reoffending and the burden on staff in correctional settings.36–40
By reducing the need for frequent supervised dosing and regular attendance at treatment services, LAIB may enable individuals to engage more easily in structured activities,19,21 including employment,42–44 which was estimated to contribute the second largest share of economic benefit. LAIB may also facilitate the fulfilment of family responsibilities by reducing disruption to daily routines, potentially supporting greater stability in caregiving and family functioning, which may in turn influence the need for child welfare interventions.28,63 Another interesting consideration with reduced service contact through LAIB are changes in the nature of the therapeutic relationship. While some healthcare staff have expressed concerns that reduced frequency of treatment attendance with LAIB could lead to fewer opportunities for social support,20 this could enable a greater emphasis on supplementary psychosocial and recovery interventions.77 In addition, less frequent attendance and supervised dosing may help reduce treatment-related stigma.19,78
Finally, healthcare benefits contributed significantly to the economic model. In line with the UK government’s From Harm to Hope 10-year drugs strategy to reduce drug-related deaths,18 recent UK policy has expanded access to naloxone, an emergency antidote for opioid overdoses,79 and introduced a “synthetic opioid preparedness plan” to address the growing threat from novel synthetic opioids.80 LAIB has the potential to complement these strategies; the model estimated that over 300 deaths could be prevented annually by increasing the number of people in treatment and by switching from methadone to buprenorphine. This aligns with previous research demonstrating that engagement with opioid agonist therapy significantly reduces all-cause and overdose mortality.29–32 In addition to prevented fatalities, reduced healthcare utilisation and an improved quality of life were significant contributors to the overall benefit.
Costs beyond additional treatment costs associated with LAIB that could be quantified were not identified. It is, however, important to recognise that this does not mean that there are none; although counselling costs are expected to remain the same, system-level investments may be needed to scale up LAIB delivery, such as infrastructure development, workforce training, obtaining UK Home Office licenses for drug storage, and service redesign.23 LAIB requires administration by trained healthcare professionals, and inappropriate administration carries potential risks, which in some settings may lead to additional regulatory controls and could introduce logistical challenges. Nevertheless, these system-level changes should only be applicable in the initial phase of treatment rollout, and may, perhaps, lead to long-term cost savings. It should also be noted that daily sublingual buprenorphine or methadone incur their own ongoing costs related to supervised dosing, daily dispensing, and staff time.34,81,82
Although made on reasonable assumptions, the results of this evaluation are consistent with previous costing models of LAIB; other studies similarly reported positive benefit–cost relationships, particularly through reductions in healthcare utilisation,35 efficiencies in prison-based settings,37–40 and lower overall treatment delivery costs despite higher drug acquisition prices.81,82 Taken together, this suggests that the present model aligns with a growing literature supporting LAIB as a cost-beneficial addition to opioid dependence treatment services.
The findings should be interpreted in the context of the approach taken with this work. The modelling relies on a range of transparent assumptions, an emerging evidence base, and limited data in some areas. For example, there is limited availability of real-world evidence on LAIB use. As a result, many estimates were derived from clinical trial data, which may not fully capture the complexity of real-world settings. Another limitation is the model’s time coverage, which is set to one year. This means that long-term costs and benefits, and the impact of changes over time such as future developments in drug treatment, justice, or health and social care policy, are not captured. Finally, it is important to note that a proportion of the estimated benefits arises from increased treatment uptake among individuals not currently engaged in care, for whom engagement in any effective OAT would be expected to improve outcomes.
Conclusion
The findings of this study suggest that LAIB is a cost-beneficial intervention that has the potential to improve outcomes for individuals with OUD while delivering significant value to society. Increasing access to LAIB could therefore be considered as part of a broader strategy to enhance treatment engagement and reduce the wider health, social, and economic burden associated with opioid dependence in England.
Implementation will, however, require consideration of system-level factors that may influence the pace and extent of uptake, including potential shifts in the wider delivery of treatment, such as greater integration of psychosocial and mental health support alongside pharmacological interventions.
Further research is needed to strengthen the evidence base, particularly through real-world studies evaluating long-term outcomes, comparative effectiveness with other OAT treatments, and impacts across different population subgroups. In addition, more robust evidence on outcomes such as employment and social functioning would help to refine future economic evaluations. Nevertheless, these findings support LAIB as a valuable addition to OUD treatment services.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Camurus AB which developed Buvidal®. Daniel Mogford is an employee of Camurus and participated in this research as a co-author. Apart from Daniel Mogford’s specific contributions detailed in the “Author Contributions” section, the funder had no role in this work.
Disclosure
Samuel Rasche and George Batchelor were commissioned by Camurus to conduct this study. Catharine Montgomery and Harry Sumnall have received consultancy fees from Camurus. Daniel Mogford is employed at Camurus. The authors declare no other conflicts of interest in this work.
References
1. Strang J, Volkow ND, Degenhardt L, et al. Opioid use disorder. Nat Rev Dis Primers. 2020;6(1):3. doi:10.1038/s41572-019-0137-5
2. Aldridge RW, Story A, Hwang SW, et al. Morbidity and mortality in homeless individuals, prisoners, sex workers, and individuals with substance use disorders in high-income countries: a systematic review and meta-analysis. Lancet. 2018;391(10117):241–12. doi:10.1016/S0140-6736(17)31869-X
3. Office for Health Improvement & Disparities. Adult substance misuse treatment statistics 2022 to 2023: report. 2023.
4. Romanowicz M, Vande Voort JL, Shekunov J, et al. The effects of parental opioid use on the parent–child relationship and children’s developmental and behavioral outcomes: a systematic review of published reports. Child Adolesc Psychiatr Ment Health. 2019;13(1):5. doi:10.1186/s13034-019-0266-3
5. Misuse of drugs act. 1971.
6. Winkelman TNA, Chang VW, Binswanger IA. Health, polysubstance use, and criminal justice involvement among adults with varying levels of opioid use. JAMA Network Open. 2018;1(3):e180558. doi:10.1001/jamanetworkopen.2018.0558
7. Pierce M, Hayhurst K, Bird SM, et al. Insights into the link between drug use and criminality: lifetime offending of criminally-active opiate users. Drug Alcohol Depend. 2017;179:309–316. doi:10.1016/j.drugalcdep.2017.07.024
8. Garpenhag L, Dahlman D. Perceived healthcare stigma among patients in opioid substitution treatment: a qualitative study. Subst Abuse Treat Prev Policy. 2021;16(1):81. doi:10.1186/s13011-021-00417-3
9. Carlisle VR, Maynard OM, Bagnall D, et al. Should I stay or should I go? A qualitative exploration of stigma and other factors influencing opioid agonist treatment journeys. Int J Environ Res Public Health. 2023;20(2):1526. doi:10.3390/ijerph20021526
10. Department of Health & Social Care. Oral methadone and buprenorphine: recommendations. 2024.
11. National Institute for Health and Care Excellence. Methadone and buprenorphine for the management of opioid dependence. 2007. Available from: www.nice.org.uk/guidance/ta114.
12. Jones M, Guirguis A, Watkins A, Bradshaw C, Mohamed L, Schifano F. Obstacles to treatment retention in opioid use disorder: an international substance use disorder treatment worker survey. Hum Psychopharmacol Clin Exp. 2023;38(5):e2882. doi:10.1002/hup.2882
13. Monwell B, Bülow P, Johnson B. The pros and cons of supervised urine tests in opioid replacement therapy: a study of patients’ experiences. Heroin Addict Relat Clin Probl. 2018;20(6):5–15.
14. Mackey K, Veazie S, Anderson J, Bourne D, Peterson K. Barriers and facilitators to the use of medications for opioid use disorder: a rapid review. J Gen Intern Med. 2020;35(S3):954–963. doi:10.1007/s11606-020-06257-4
15. Frank D, Mateu-Gelabert P, Perlman DC, Walters SM, Curran L, Guarino H. “It’s like ‘liquid handcuffs”: the effects of take-home dosing policies on methadone maintenance treatment (MMT) patients’ lives. Harm Reduct J. 2021;18(1):88. doi:10.1186/s12954-021-00535-y
16. Benyamina A, Stöver H. Barriers to treatment access and informed patient choice in the treatment of opioid dependence in Europe. Heroin Addict Relat Clin Probl. 2012;14(4):65–80.
17. National Drug Treatment Monitoring System. Unmet treatment need indicator. 2025. Available from: https://www.ndtms.net/.
18. HM Government. From harm to hope: a 10-year drugs plan to cut crime and save lives. 2021.
19. Barnett A, Savic M, Lintzeris N, et al. Tracing the affordances of long-acting injectable depot buprenorphine: a qualitative study of patients’ experiences in Australia. Drug Alcohol Depend. 2021;227:108959. doi:10.1016/j.drugalcdep.2021.108959
20. Nordgren J, Monwell B, Johnson B, Gunnarsson NV, Capusan AJ. Healthcare staff’s perspectives on long-acting injectable buprenorphine treatment: a qualitative interview study. Addiction Sci Clin Pract. 2024;19(1):25. doi:10.1186/s13722-024-00458-6
21. Johnson B, Flensburg OL, Capusan AJ. Patient perspectives on depot buprenorphine treatment for opioid addiction – a qualitative interview study. Subst Abuse Treat Prev Policy. 2022;17(1):40. doi:10.1186/s13011-022-00474-2
22. National Institute for Health and Care Excellence. Opioid dependence: buprenorphine prolonged-release injection (Buvidal): evidence review. 2019.
23. Rolland B, Matheson C, Kaski A, Kosim M, Roncero C, Vorspan F. Compared implementation of the long-acting buprenorphine treatment buvidal in four European countries. Expert Opin Drug Deliv. 2024;21(5):809–815. doi:10.1080/17425247.2024.2369756
24. Bharat C, Chidwick K, Gisev N, Farrell M, Ali R, Degenhardt L. Trends in use of medicines for opioid agonist treatment in Australia, 2013–2022. Int J Drug Policy. 2024;123:104255. doi:10.1016/j.drugpo.2023.104255
25. Prami T, Pölkki M, Ruotsalainen J, Nordbeck EB, Meyner S, Kaski A. Reasons for not entering opioid agonist treatment: a survey among high-risk opioid users in Finland. Nord Stud Alcohol Drugs. 2024;41(2):200–211. doi:10.1177/14550725231204723
26. Lind B, Chen S, Weatherburn D, Mattick R. The effectiveness of methadone maintenance treatment in controlling crime: an australian aggregate-level analysis. Br J Criminol. 2005;45(2):201–211. doi:10.1093/bjc/azh085
27. Casey J, Hay G, Godfrey C, Parrot S. Assessing the scale and impact of illicit drug markets in Scotland. Scottish Government Soc Res. 2009.
28. Bullinger LR, Wang V, Feder KA. Effects of opioid treatment programs on child well-being. Ann Am Acad Pol Soc Sci. 2022;703(1):79–105. doi:10.1177/00027162221142644
29. Santo T, Hickman M, Padmanathan P, Degenhardt L. The impact of opioid agonist treatment delivered in different settings on all-cause mortality and specific causes of death: a systematic review and meta-analysis. JAMA Psychiatry. 2021;78(9):979–993. doi:10.1001/jamapsychiatry.2021.0976
30. Sordo L, Barrio G, Bravo MJ, et al. Mortality risk during and after opioid substitution treatment: systematic review and meta-analysis of cohort studies. BMJ. 2017;357. doi:10.1136/bmj.j1550
31. Hickman M, Steer C, Tilling K, et al. The impact of buprenorphine and methadone on mortality: a primary care cohort study in the United Kingdom. Addiction. 2018;113(8):1461–1476. doi:10.1111/add.14188
32. Ma J, Bao YP, Wang RJ, et al. Effects of medication-assisted treatment on mortality among opioids users: a systematic review and meta-analysis. Mol Psychiatry. 2019;24(12):1868–1883. doi:10.1038/s41380-018-0094-5
33. Schackman BR, Leff JA, Polsky D, Moore BA, Fiellin DA. Cost-effectiveness of long-term outpatient buprenorphine-naloxone treatment for opioid dependence in primary care. J Gen Intern Med. 2012;27(6):669–676. doi:10.1007/s11606-011-1962-8
34. Marsden J, Kelleher M, Gilvarry E, et al. Superiority and cost-effectiveness of monthly extended-release buprenorphine versus daily standard of care medication: a pragmatic, parallel-group, open-label, multicentre, randomised, controlled, phase 3 trial. EClinicalMedicine. 2023;66:102311. doi:10.1016/j.eclinm.2023.102311
35. Gauffin E, Marques Franca A, Pizzaro Ferrero E, et al. Reduced need for inpatient care following introduction of long-acting injectable buprenorphine. BMC Health Serv Res. 2025;25(1):1–10. doi:10.1186/s12913-025-13607-7
36. Mlilo K, Fatema K, Poudel P, Harjanto R, Whitton G. Comparing the effectiveness of depot buprenorphine (buvidal injection) and buprenorphine/naloxone (suboxone) treatment following custody release - a retrospective cohort study. J Subst Use. 2025;30(3):414–421. doi:10.1080/14659891.2024.2342313
37. Ling R, White B, Roberts J, et al. Depot buprenorphine as an opioid agonist therapy in New South Wales correctional centres: a costing model. BMC Health Serv Res. 2022;22(1):1326. doi:10.1186/s12913-022-08687-8
38. Sayers C, Mogford D. Patient satisfaction and resource utilization following introduction of long-acting injectable buprenorphine (LAIB) in Scottish Prisons. Subst Abuse Rehabil. 2025;Volume 16:83–93. doi:10.2147/SAR.S510467
39. Stöver H, Keppler K. Opioidsubstitutionsbehandlung im Justizvollzug: der Vergabeaufwand von Buprenorphin-Depot im Vergleich zu anderen Substitutionsmedikamenten – eine gesundheitsökonomische Modellrechnung. Das Gesundheitswesen. 2023;85(06):573–577. doi:10.1055/a-1842-7164
40. Wong JSH, Masson S, Huang A, et al. Cost analysis of buprenorphine extended-release injection versus sublingual buprenorphine/naloxone tablets in a correctional setting. J Correctional Health Care. 2022;28(6):368–371. doi:10.1089/jchc.21.07.0063
41. Neale J, Tompkins CNE, Strang J. Prolonged-release opioid agonist therapy: qualitative study exploring patients’ views of 1-week, 1-month, and 6-month buprenorphine formulations. Harm Reduct J. 2019;16(1):25. doi:10.1186/s12954-019-0296-4
42. Ling W, Nadipelli VR, Solem CT, et al. Patient-centered outcomes in participants of a buprenorphine monthly depot (BUP-XR) double-blind, placebo-controlled, multicenter, Phase 3 study. J Addict Med. 2019;13(6):442–449. doi:10.1097/ADM.0000000000000517
43. Ling W, Nadipelli VR, Solem CT, et al. Effects of monthly buprenorphine extended-release injections on patient-centered outcomes: a long-term study. J Subst Abuse Treat. 2020;110:1–8. doi:10.1016/j.jsat.2019.11.004
44. Haight BR, Learned SM, Laffont CM, et al. Efficacy and safety of a monthly buprenorphine depot injection for opioid use disorder: a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2019;393(10173):778–790. doi:10.1016/S0140-6736(18)32259-1
45. Neale J, Cassidy J, Cosgrove S, Strang J. Patient satisfaction with long-acting injectable buprenorphine: what needs to be measured from the patient’s perspective? Drugs. 2025;1–10. doi:10.1080/09687637.2025.2506415
46. Ling W, Shoptaw S, Goodman-Meza D. Depot buprenorphine injection in the management of opioid use disorder: from development to implementation. Subst Abuse Rehabil. 2019;10:69–78. doi:10.2147/SAR.S155843
47. HM Treasury. The Green Book: Central Government Guidance on Appraisal and Evaluation. Hm Treasury; 2022.
48. Michael D, Sculpher MJ, Karl C, Stoddart GL, Torrance GW. Methods for the Economic Evaluation of Health Care Programmes. Oxford University Press; 2015.
49. Office for National Statistics. Population estimates for England and Wales: mid-2023. 2024.
50. Frost M, Bailey GL, Lintzeris N, et al. Long-term safety of a weekly and monthly subcutaneous buprenorphine depot (CAM2038) in the treatment of adult out-patients with opioid use disorder. Addiction. 2019;114(8):1416–1426. doi:10.1111/add.14636
51. HM Treasury. GDP deflators at market prices, and money GDP June 2025 (Quarterly national accounts). 2025.
52. Department for Education. Children Looked after in England Including Adoption: 2023 to 2024. 2024.
53. Harwin J, Alrouh B, Broadhurst K, McQuarrie T, Golding L, Ryan M. Child and parent outcomes in the london family drug and alcohol court five years on: building on international evidence. Int J Law Policy Family. 2018;32(2):140–169. doi:10.1093/lawfam/eby006
54. Conti G, Pizzo E, Morris S, Melnychuk M. The economic costs of child maltreatment in UK. Health Econ. 2021;30(12):3087–3105. doi:10.1002/hec.4409
55. Domzaridou E, Allen T, Carr MJ, Millar T, Webb RT, Ashcroft DM. Healthcare utilisation and associated costs for methadone versus buprenorphine recipients: examination of interlinked primary and secondary care electronic health records in England. Drug Alcohol Rev. 2024;43(7):1845–1855. doi:10.1111/dar.13933
56. National Institute for Health and Care Excellence. Buprenorphine. 2025.
57. National Institute for Health and Care Excellence. Methadone Hydrochloride. 2025.
58. Bauld L, Hay G, McKell J, Carroll C. Problem drug users’ experiences of employment and the benefit system. 2010.
59. Evans EA, Wilson D, Friedmann PD. Recidivism and mortality after in-jail buprenorphine treatment for opioid use disorder. Drug Alcohol Depend. 2022;231:109254. doi:10.1016/j.drugalcdep.2021.109254
60. HM Prison & Probation Service. Costs per place and costs per prisoner by individual prison. 2024.
61. Godfrey C, Stewart D, Gossop M. Economic analysis of costs and consequences of the treatment of drug misuse: 2-year outcome data from the national treatment outcome research study (NTORS). Addiction. 2004;99(6):697–707. doi:10.1111/j.1360-0443.2004.00752.x
62. Heeks M, Reed S, Tafsiri M, Prince S. The economic and social costs of crime second edition. home office research report 99. 2018.
63. Green BL, Rockhill A, Furrer C. Does substance abuse treatment make a difference for child welfare case outcomes? A statewide longitudinal analysis. Child Youth Serv Rev. 2007;29(4):460–473. doi:10.1016/j.childyouth.2006.08.006
64. National Fostering Group. Foster care pay and allowances. Available from: https://www.nfa.co.uk/thinking-about-fostering/support-and-benefits-for-foster-carers/financial-support/.
65. Wakeman SE, Larochelle MR, Ameli O, et al. Comparative effectiveness of different treatment pathways for opioid use disorder. JAMA Network Open. 2020;3(2):e1920622. doi:10.1001/jamanetworkopen.2019.20622
66. Yarborough BJH, Stumbo SP, Janoff SL, Keast EM, Leo MC, Leitz SJ. Reduced emergency department use among insured individuals receiving extended-release buprenorphine in a health system setting. Drug Alcohol Dependence Reports. 2024;11:100233. doi:10.1016/j.dadr.2024.100233
67. Roncero C, Dorado ML, Orengo T, et al. PMH70 direct healthcare costs for the management of patients with opioid use disorder treated with methadone and buprenorphine/naloxone in real-world setting in Spain. COSTEDOPIA study. Value Health. 2019;22:S693. doi:10.1016/j.jval.2019.09.1544
68. Bell JR, Butler B, Lawrance A, Batey R, Salmelainen P. Comparing overdose mortality associated with methadone and buprenorphine treatment. Drug Alcohol Depend. 2009;104(1–2):73–77. doi:10.1016/j.drugalcdep.2009.03.020
69. Thomas P. Minimum sample size for the survey measurement of a wealth-dependent parameter with the UK VPF as exemplar. Measurement. 2020;150:107044. doi:10.1016/j.measurement.2019.107044
70. Office for National Statistics. Deaths related to drug poisoning in England and Wales: 2023 registrations. 2024.
71. National Institute for Health and Care Excellence. How NICE measures value for money in relation to public health interventions. 2013.
72. Jones HE, Harris RJ, Downing BC, et al. Estimating the prevalence of problem drug use from drug-related mortality data. Addiction. 2020;115(12):2393–2404. doi:10.1111/add.15111
73. Hay G, Rael Dos Santos A, Reed H, Hope V. Estimates of the prevalence of opiate use and/or crack cocaine use, 2016/17: sweep 13 report. 2019.
74. Office for Health Improvement and Disparities, UK Health Security Agency. Estimates of opiate and crack use in England: main points and methods. 2023.
75. Office for Health Improvement & Disparities. Alcohol and drug treatment in secure settings 2022 to 2023: report. 2024.
76. Ministry of Justice & HM Prison and Probation Service. New change to some offenders’ automatic release dates. 2024. Available from: https://www.gov.uk/guidance/new-change-to-some-offenders-automatic-release-dates.
77. Fish R, Mateus C, Maiden H, Lawson E, Limmer M. Long acting injectable buprenorphine: perspectives from service-users, staff and stakeholders. Drug Alcohol Dependence Reports. 2025;15:100328. doi:10.1016/j.dadr.2025.100328
78. Somaini L, Vecchio S, Corte C, et al. Prolonged-release buprenorphine therapy in opioid use disorder can address stigma and improve patient quality of life. Cureus. 2021. doi:10.7759/cureus.18513
79. Department of Health and Social Care. Supplying take home naloxone without a prescription. 2025. Available from: https://www.gov.uk/guidance/supplying-take-home-naloxone-without-a-prescription.
80. Home Office. Local preparedness for synthetic opioids in England. 2025. Available from: https://www.gov.uk/government/publications/local-preparedness-for-synthetic-opioids-in-england/local-preparedness-for-synthetic-opioids-in-england-accessible.
81. Phillips-Jackson H, Hallam C, Cullen N, et al. Budget impact analysis of the introduction of injectable prolonged-release buprenorphine on opioid use disorder care resource requirements. Clinicoecon Outcomes Res. 2020;12:233–240. doi:10.2147/CEOR.S242984
82. Pedersen MH, Danø A, Gibbons C, Jensen R. Administration and patient-incurred costs associated with opioid agonist treatment in Norway. Curr Med Res Opin. 2022;38(11):1959–1965. doi:10.1080/03007995.2022.2129230
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Multimodal Acute Pain Management in the Parturient with Opioid Use Disorder: A Review
Koltenyuk V, Mrad I, Choe I, Ayoub MI, Kumaraswami S, Xu JL
Journal of Pain Research 2024, 17:797-813
Published Date: 29 February 2024