Back to Journals » Advances in Medical Education and Practice » Volume 9
The role of smartphone game applications in improving laparoscopic skills
Authors Chalhoub M, Khazzaka A, Sarkis R, Sleiman Z
Received 22 March 2018
Accepted for publication 23 May 2018
Published 3 August 2018 Volume 2018:9 Pages 541—547
DOI https://doi.org/10.2147/AMEP.S162619
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Marc Chalhoub,1 Aline Khazzaka,1 Riad Sarkis,1 Zaki Sleiman2,3
1Laboratory of Science and Research, Saint Joseph University, Beirut, Lebanon; 2Department of Obstetrics and Gynecology, Lebanese American University Medical Center, Beirut, Lebanon; 3The European Academy for Gynecological Surgery, Leuven, Belgium
Background: Virtual games (VGs) have a positive impact on laparoscopic skills. Time spent playing, the console and the type of game used correlate with the speed of acquisition of laparoscopic skills and their preservation.
Methods: A total of 45 university medical students with no previous surgical experience were divided into three groups: gamers (n=20), control (n=10) and intervention (n=15). They passed the laparoscopic skills testing and training model, developed by the European Academy of Gynecological Surgery, over two sessions. Every 5 intervention participants were asked to play a different smartphone application game daily for 2 months between the two sessions. Scores were calculated at both sessions and used to calculate the evolution ratio between sessions.
Results: Significant advantage was found at session 1 of gamers over non-gamers (p=0.002). No significant difference existed between the two non-gamer groups (p=0.96), or between the three intervention sub-groups (p>0.05). All participants’ performances improved between sessions. No significant difference existed in evolution between control and gamers (p=0.121), nor between intervention and gamers (p=0.189). Significant advantage was found in evolutions of the intervention group over control group (p=0.035).
Conclusion: Previous VG experience is a significant factor in showing better laparoscopic skills when virtual reality simulator is used for the first time. Recent and regular smartphone gaming practice significantly improves laparoscopic skills in non-gamers independently of the type of game practiced. Smartphone gaming practice appears to influence positively some specific laparoscopic skills more than others.
Keywords: virtual games, laparoscopic psychomotor skills, training, smartphone, dry lab
A Letter to the Editor has been received and published for this article.
Introduction
Virtual game (VG) players have a long attention span, rapid mental processing and high level of concentration on tasks.1 They develop better hand-eye coordination and visual motor skills than non-gamers.2 They are also resistant to distraction, more sensitive to information in the peripheral vision and able to count briefly presented objects.3 For that purpose, studies have been conducted to show the positive impact of virtual gaming on laparoscopic training skills. It has been shown that VG players acquire laparoscopic skill faster and make fewer errors than non-gamers.4 Due to their entertaining nature, VGs draw the player into a storyline, which leads to playful and effortless learning.5 Thus, VG experience enables a faster adaptation to perceive a two-dimensional (2D) image as a 3D image, better hand-eye coordination and finer tactile feedback in laparoscopy and endoscopy gamer trainee than in non-gamer trainee. It also facilitates acquiring ambidexterity and tone reflexes.6,7 There is also a positive correlation between the duration of time spent playing on VGs and the acquisition of laparoscopic skills. Prior VG experience and its length were found to be more important than the actual surgical experience when it comes to training on the box, in terms of speed of learning and preservation of the skills.8
Moreover, studies showed different levels of skills and learning curves in different consoles and games used by the resident.9–13 However, to our knowledge, no study has been conducted yet in order to find a correlation between smartphone gaming and laparoscopic skills.
A recent market study showed that the usage of smartphones for professional purposes among physicians in the USA has increased from 68% in 2012 to 84% in 2015.14 The medical community has shown a trend in increasing smartphone dependency, and thus smartphone applications are quickly being integrated into clinical practice.15,16 The number of applications used by medical students, residents and physicians, and the time spent on those applications are on the rise. Furthermore, residents and doctors endorse the development of more smartphone applications to support their knowledge and skills.17,18
The aim of this study is to show that the positive impact of VG practice on laparoscopic skills can include Smartphone games (SGs), and to find a pattern between the types of SGs played and the type of skills acquired.
Methods
Participants
The study was performed by university medical students who have no experience whatsoever in either open or laparoscopic surgery. They have never assisted to nor participated in any kind of surgical experience, training or procedure. Participants were enrolled in the study after filling a pre-designed questionnaire. The questionnaire allowed us to collect demographical data (age and sex), gaming habits and level of surgical or laparoscopic experience. Subjects belonged to the same category of age (22–25 years) and were divided into three groups. The first group (n=20) included VG players (referred to as “gamer group”) who have been playing different games on different consoles for more than 3 years. They were asked not to change their gaming routine and not to introduce any SGs during the conduction of the study. The second group (n=10) included students who have never played VGs or SGs and were asked to not start playing during the conduction of the study (referred to as “control group”). The third group (n=15) included students who have never played VGs or SGs and were asked to start playing a specific SG (Candy Crush Saga – King ©, Temple Run – Imangi Studios ©, or Crazy Balancing Ball – Free App Logic ©) for half an hour daily for a 2-month period (referred to as “intervention group”). Participants of this last group were randomly divided into these three subgroups (n=5) before the first session and were asked to report their gaming time on a daily basis. Any participant who did not meet the inclusion criteria determined in the experimental design was excluded. After the approval of the Ethics Committee of Saint Joseph University, written informed consent was obtained from all participants before initiating the study.
Experimental design
Laparoscopic skills testing and training (LASTT) model was developed by the European Academy of Gynecological Surgery and published in 2008 as a valid method for testing and training laparoscopic skills in gynecology.19 It has been proven as a valid tool for training and measuring different laparoscopic psychomotor skills (LPS) such as laparoscopic camera navigation, depth appreciation from a 2D screen, hand-eye coordination, remote handling of instruments without tactile feedback and fine motor skills. It consists of three different standardized exercises: camera navigation (E1), camera navigation and forceps handling (E2), and forceps handling and bi-manual coordination (E3).19 These exercises aim to specifically measure the following basic LPS: camera navigation, hand–eye coordination and bimanual coordination, respectively.20,21
- E1 evaluates the participants’ ability to navigate a laparoscopic camera by measuring their capacity to identify 14 different targets placed at different sites in the model. The exercise starts by identifying a large symbol on the first target and then a small symbol situated next to it from a close-up viewpoint. This small symbol indicates the next large symbol to be identified. The participant should follow this order until they identify the small symbol on the last target.
- E2 evaluates the participants’ ability to navigate a laparoscopic camera with the non-dominant hand and to handle a pair of laparoscopic forceps with the dominant hand. The participants should grasp and transport six 5×4 mm open cylinders of different colors to six predefined targets/nails of the same colors and introduce them onto the relevant nail.
- E3 evaluates the participants’ ability to handle a pair of laparoscopic forceps simultaneously with the dominant and the non-dominant hand. Participants should grasp 6 objects (10×5 mm push pins with a tail of 10 mm) of different colors with their non-dominant hand, then re-grasp and transport them with their dominant hand to six matching colors targets (20-mm holes).19–21
Each participant received individually a full explanation and a live demonstration of all three tasks at the beginning of the study. He or she was neither allowed to train nor to observe other participants passing the tests. The participant was then asked to perform the test twice; the first time at the beginning of the study (session 1 [s1]) and the second time 2 months later (session 2 [s2]). The exercises were performed in chronological order. Only one try was allowed at each session.
Since the participants had no experience in laparoscopy and only one trial was allowed, we introduced a modified scoring system that only measures performance. Participants were given 120 seconds to identify 14 targets in E1 and 180 seconds to transport 6 objects for E2 and E3. Two variables were recorded: the number of targets identified/transported and the time needed to achieve the tests. Since some were able to achieve their objective in less than the required time while others could not finalize the task, the time to correctly performed exercise was used to calculate the speed of the participant at both sessions. The speed (targets/120 seconds for E1 and targets/180 seconds for E2 and E3) was then calculated over 100 to allow a valid correlation between the three exercises and a valid comparison between s1 and s2. An evolution ratio was then calculated for every participant by dividing the score at s1 over the score at s2.
Statistics
We used the SPSS Statistics Software (version 22.0) to conduct our analysis. Independent t-test was used to compare scores at session 1 (SS1) between groups (gamers, non-gamers, intervention and control), SS1 between subgroups (different type of games) and evolution ratios between these different groups and subgroups as well. We used one-sample t-test to compare evolution ratios between the different exercises (E1, E2 and E3).
Results
A total of 45 participants met the required criteria and were recruited to the study. All of them passed the test during both sessions: s1 and s2. They were divided into three groups; 20 participants belonged to the gamer group. A total of 25 participants belonged to the non-gamer group, of which 10 belonged to the control group, and 15 belonged to the intervention group. Five intervention participants were asked to play Candy Crush 30 minutes daily for 2 months, 5 others were asked to play Temple Run and the remaining 5 were asked to play Crazy Balancing Ball. The male to female ratio was 28/17, and the ratio between groups was as follows: gamers M/F=19/1 and M/F=9/16 for the non-gamers.
Mean scores at s1 and s2 relative to the different groups and sub-groups are displayed in Table 1. A significant advantage was found at s1 of the gamer group over the non-gamer group (p=0.002). No significant difference existed between the two non-gamer groups: control group and intervention group (p=0.96). No significant differences existed between the three intervention sub-groups: Candy Crush, Temple Run, and Crazy Balancing Game: Candy Crush and Crazy Balancing Game (p=0.876), Temple Run and Crazy Balancing Game (p=0.394), Candy Crush and Temple Run (p=0.496).
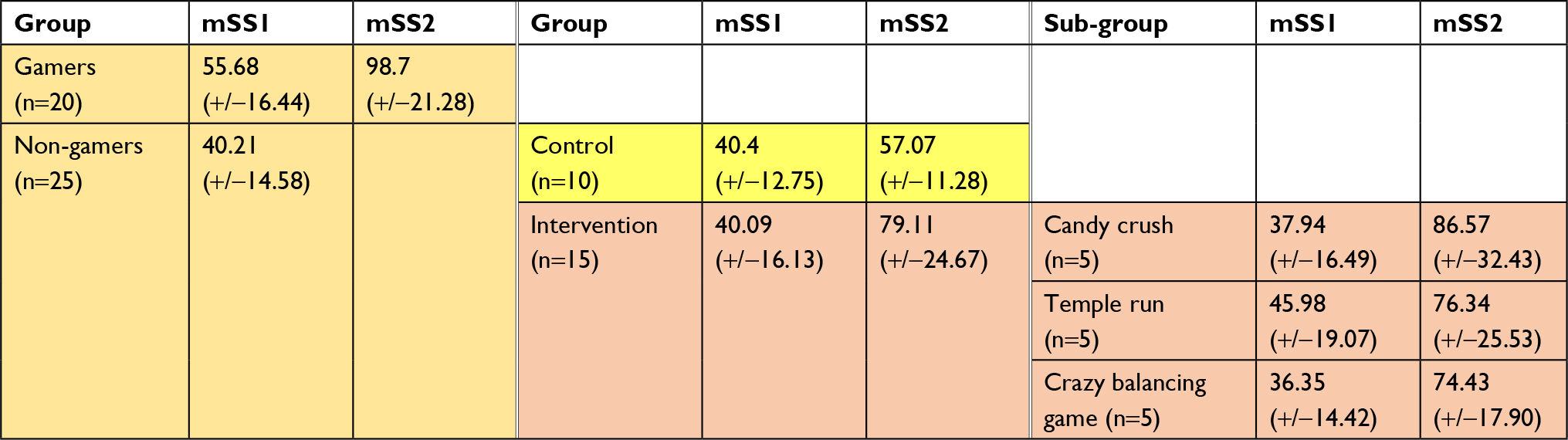 | Table 1 Mean scores (over 100) at session 1 and session 2 of passing LASTT test Abbreviations: LASTT, laparoscopic skills testing and training; mSS1, mean score at session 1; mSS2, mean score at session 2. |
Evolution ratios of different participants are displayed in Figure 1, and mean evolution ratios relative to all groups and sub-groups are displayed in Table 2. The control group scored 1.53 (+/− 0.59) times better in s2 than in s1, while the gamer group scored 1.87 (+/− 0.53) times better. Intervention group’ mean evolution ratio was 2.16 (+/− 0.74), with mean ratios of 2.44 (+/− 0.70), 1.78 (+/− 0.62) and 2.25 (+/− 0.87) for Candy Crush, Temple Run and Crazy Balancing Game respectively. We found a non-significant difference in evolution between control group and gamer group (p=0.121). We found a significant advantage in evolutions of the intervention group over the control group (p=0.035). No significant difference was found between the evolution of the intervention group and evolution of the gamer group (p=0.189). No significant difference was found between the evolution of the three different intervention sub-groups: Candy Crush and Crazy Balancing Game (p=0.710), Temple Run and Crazy Balancing Game (p=0.350), Candy Crush and Temple Run (p=0.149).
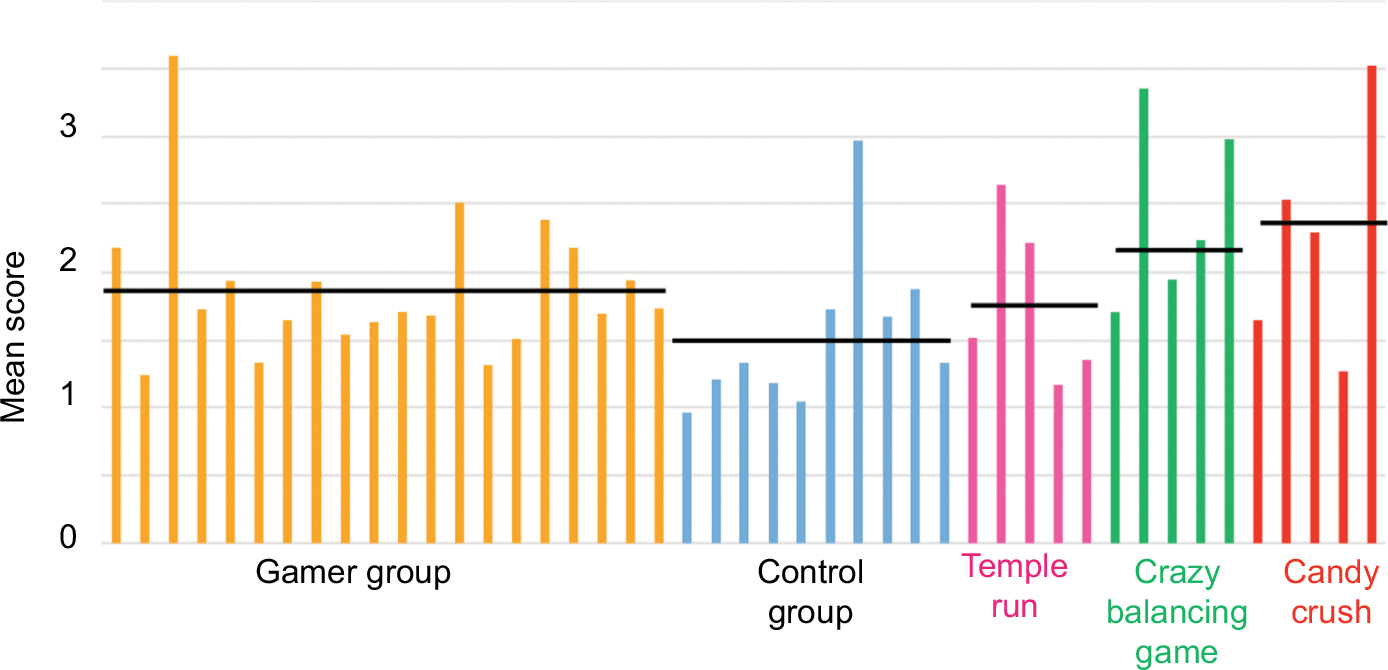 | Figure 1 Distribution of evolution ratio of all participants. Note: In black (horizontal black line) the mean score for every group or sub-group. |
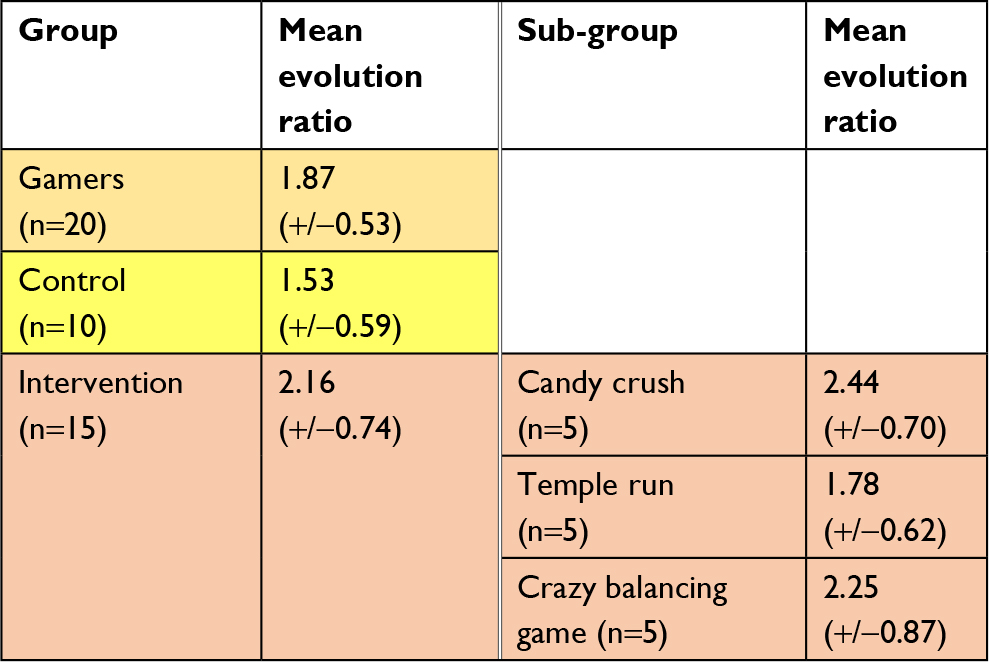 | Table 2 Mean evolution ratio for every group and sub-group |
Mean evolution ratios of the intervention group relative to every exercise were calculated; results are displayed in Table 3. A significant advantage was found in the evolution of the intervention group in exercise 1 (E1) over its evolution in E2 (p=0.000), and in its evolution in E1 over its evolution in E3 (p=0.000). A significant advantage was also found in the evolution of the intervention group in E2 over its evolution in E3 (p=0.000).
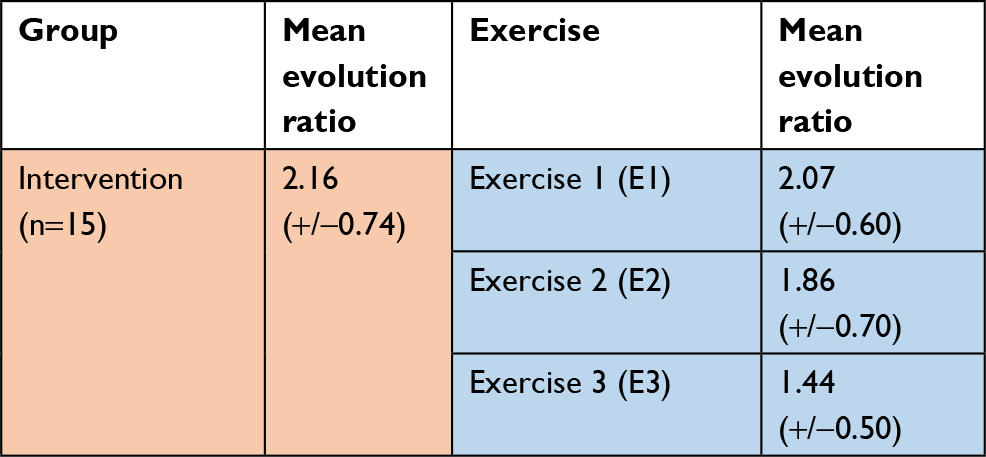 | Table 3 Mean evolution ratio for the intervention group and every exercise relative to this group |
Discussion
In 1992, Satava announced that the burst of laparoscopic surgery was in fact subconscious in the young “video-generation surgeons”. He declared that “Nintendo surgeons” will embrace all kinds of new technologies, ranging from video games to the new laparoscopic surgery.22 It was not until 2003, when Grantcharov et al published the first paper showing evidence of better laparoscopic skills in users of computer games than nonusers. VG players made fewer errors and achieved their tasks faster than non-players.23 Several other reports give evidence that VG players achieve better results in first-time laparoscopic experience than non-players. In a study that included 33 surgery residents, Rosser et al found that gamers made fewer errors and performed faster, with a score better than non-gamers in laparoscopic suturing. This study was the first to find a positive correlation between the time spent on VGs and the laparoscopic skills.4 In 2011, Paschold et al divided 326 Fifth-year undergraduate medical students with no surgical experience into two groups. Participants attended a standardized virtual reality laparoscopy training. Evolution scores were recorded. The study demonstrated a significant relationship between video game experience and total scores. It concluded that VG players presented significantly higher baseline in virtual reality laparoscopy results than non-gamers. They also demonstrated that scoring achievement is correlated to the frequency of VG playing when virtual reality simulator is used for the first time.24 An important factor introduced by Paschold et al is the recruitment of participants with no previous surgical experience. We decided to follow their steps in order to cancel the surgical experience as a potential variable.
Previous studies conducted to validate the LASTT model were based on multiple repetitions of the exercises. A significant learning effect was observed, but its impact was reduced after the decrease of the number of repetitions allowed.20,21 We decided to only allow one try at each session to reduce the bias of the learning effect observed after the repetitions, which we considered to be able to alter the results at s2.
The scoring system developed for the LASTT is based on levels of previous exposure to gynecological laparoscopy using the classification of the European Society for Gynecological Endoscopy. It measures the LPS of the participants relative to their experience, training and group population, and calculates the score after multiple repetitions.20 Since our population falls under the category “no procedures” (score 0)21 and only one try was allowed, we had to introduce a modified scoring system that only measures performance.
Similarly to previous studies, our scoring system is based on the speed of the participant, and thus it reflects the errors and the economy of movement in the result and as such is considered to be accurate.20,21
In our study, all the participants’ performances improved from s1 to s2. Similar to the previous studies, our analysis showed that participants with previous VG experience scored significantly higher during the first session than participants with no previous VG experience. Gamers were faster and therefore committed less errors and did less useless movements than non-gamers. In addition, with no laparoscopic training, gamers were able to score higher than non-gamers during the second session 2 months later. However, the difference in the evolution ratio was not significant. Although gamers scored much higher on the second attempt than non-gamers, their skills increased at a lower speed than non-gamers.
Comparison between our two non-gamer groups, control group and intervention group, and between our three intervention sub-groups, Candy Crush, Temple Run and Crazy Balancing Game, found non-significant difference in scores during the first session. Therefore, we can consider that the baseline laparoscopic abilities of all our non-gamer groups and sub-groups are equivalent at the beginning of game.
In 2009, Badurdeen et al published a study showing a correlation between Wii (Nintendo Co, Ltd, Kyoto, Japan) gaming performance and performance of laparoscopic tasks in a simulator. Twenty participants with minimal experience with laparoscopic surgery and Wii performed three tasks on a laparoscopic simulator and three games on Wii. Participants in the top tertile of Wii performance scored higher on the laparoscopic tasks than those in the bottom tertile. This study was amongst the first to emphasize on the importance of the console used in VGs as much as the history of playing.9
To our knowledge, no study has been conducted before to find a potential correlation between smartphone gaming and laparoscopic skills. Our analysis shows that participants with no previous gaming experience in neither VGs nor SGs and who started playing on a predetermined SG present significant improvement in laparoscopic skills after 2 months of playing for 30 minutes daily compared to the control group (participants who have non previous nor actual gaming experience of any kind). In fact, intervention group got faster between s1 and s2, and showed a better evolution, in terms of speed, than the control group. Certainly, dry-box training remains necessary for the acquisition and performance of basic and complex laparoscopic skills. However, video gaming offers the surgery residents a flexible solution to improve some of their laparoscopic skills despite of their work-hours restrictions. Nowadays, video gaming is becoming practical for surgery residents, since they can practice everywhere and whenever they have free time.
Schlickum et al assessed the role of VGs’ type in 2008. Their study compared four control participants to 11 VGs players of a 3D first person shooter (FPS) game and 11 players of a 2D non-FPS game who practiced intensely for 5 weeks. The FPS group scored significantly better on the minimal invasive surgery trainer – virtual reality simulator than the other group. These findings were confirmed by the same authors in 2009, where they compared improvement scores of 15 students who played Half Life (Valve Software Corp, Bellevue, WA, USA), a FPS game, with 15 students who played Chessmaster (Ubisoft Entertainment SA, Rennes, France), a non-FPS game, with 10 control students. Under the same circumstances as the first study, both gamer groups showed a statistically significant improvement in score performance between the first and second test (Half Life group – Chessmaster group) with a greater transfer effect of Half Life group over Chessmaster group.12 In the present work, we could not find any significant difference in evolution between any of our three sub-groups. It appears that the improvement showed in the intervention group is independent from the type of game played. The significance of these results could be limited by the small sample of intervention sub-groups (sub-groups of five); therefore, a similar study conducted on a larger scale could be able to provide more reliable results concerning the role of the type of game played and the significance of the improvement shown.
Finally, we compared the evolution of the intervention group relative to every exercise separately in an attempt to find a trend in the type of laparoscopic skill acquired with SG practice. We found that intervention group got better in camera navigation while handling a pair of forceps in the dominant hand and bi-manual coordination. We also found that they got better in camera navigation while handling a pair of forceps than bi-manual coordination. Due to the small sample size, we could postulate but not confirm that SG practice improves the camera navigation skill over forceps handling. Furthermore, we were not able to assess in statistically accurate means the role of each SG in improving one laparoscopic skill over another. Further studies on a larger scale should be conducted to assess the role of SGs in improving certain skills and the characteristics that allow one SG to improve a certain laparoscopic skill. This achievement could allow the development of a smartphone application specialized in improving different laparoscopic skill.
Limitations
The male to female ratio in the study was not respected between groups since most of the male participants were gamers and most the female participants were non-gamers. However, studies show that sex is an important variable in laparoscopic skills and skill acquirement. Females usually scored less in laparoscopic tests and have a slower learning curve than males.25 Knowing that most of the gamers in the study were males and most of non-gamers were females, it is safe to consider that any randomization in terms of sex would strengthen our results.
While our sample size was very acceptable compared to previous studies, our intervention subgroups were smaller than expected. Thus, a relationship between the types of games played on smartphone and the significance of the improvement in terms of skills could not be established. The role of each type of game in improving a certain type of laparoscopic skill could not be identified.
Conclusion
Previous VG experience is a significant factor in showing better laparoscopic skills when virtual reality simulator is used for the first time, but the association between evolution without training and positive history of virtual gaming is not significant. Recent and regular SG practice significantly improves laparoscopic skills in non-gamers independently of the type of game practiced. Smartphone gaming practice appears to influence the ability to camera navigation more than the ability to handle forceps. Different SGs are able to improve different types of laparoscopic skills. Further studies should be conducted to assess the role of SGs in improving preferably some skills over others, and the games’ characteristics responsible of this discordance, therefore enabling the investment in a smartphone application, a cheap and practical tool, to improve one’s laparoscopic skills.
Acknowledgment
We would like to thank Karl Storz, Beirut, for providing the facility, materials and support needed to conduct this study.
Disclosure
Dr Zaki Sleiman is a consultant for Karl Storz. He declares that his relationship with the company has no impact upon the scientific value and the content of the submitted work. The authors report no other conflicts of interest in this work.
References
Boot WR, Kramer AF, Simons DJ, Fabiani M, Gratton G. The effects of video game playing on attention, memory, and executive control. Acta Psychol (Amst). 2008;129(3):387–398. | ||
Green CS, Bavelier D. Effect of action video games on the spatial distribution of visuospatial attention. J Exp Psychol Hum Percept Perform. 2006;32(6):1465–1478. | ||
Green CS, Bavelier D. Action video game modifies visual selective attention. Nature. 2003;423(6939):534–537. | ||
Rosser JC Jr, Lynch PJ, Cuddihy L, Gentile DA, Klonsky J, Merrell R. The impact of video games on training surgeons in the 21st century. Arch Surg. 2007;142(2):181–186; discusssion 186. | ||
Graafland M, Ten Cate O, van Seventer JP, Schraagen JM, Schijven MP. Mapping the demand for serious games in postgraduate medical education using the entrustable professional activities framework. Games Health J. 2015;4(5):381–386. | ||
Enochsson L, Isaksson B, Tour R, et al. Visuospatial skills and computer game experience influence the performance of virtual endoscopy. J Gastrointest Surg. 2004;8(7):876–882; discussion 882. | ||
Rosser JC Jr, Gentile DA, Hanigan K, Danner OK. The effect of video game “warm-up” on performance of laparoscopic surgery tasks. JSLS. 2012;16(1):3–9. | ||
Van Hove C, Perry KA, Spight DH, et al. Predictors of technical skill acquisition among resident trainees in a laparoscopic skills education program. World J Surg. 2008;32(9):1917–1921. | ||
Badurdeen S, Abdul-Samad O, Story G, Wilson C, Down S, Harris A. Nintendo Wii video-gaming ability predicts laparoscopic skill. Surg Endosc. 2010;24(8):1824–1828. | ||
Sadandanan S, Dryfhout VL, Sosnowski JP. Video games and laparoscopic surgery. J Gynecol Surg. 2008;24(2):67–74.doi:10.1089/gyn.2008.B-02295-1. | ||
Schlickum MK, Hedman L, Enochsson L, Kjellin A, Felländer-Tsai L. Transfer of systematic computer game training in surgical novices on performance in virtual reality image guided surgical simulators. Stud Health Technol Inform. 2008;132:210–215. | ||
Schlickum MK, Hedman L, Enochsson L, Kjellin A, Felländer-Tsai L. Systematic video game training in surgical novices improves performance in virtual reality endoscopic surgical simulators: a prospective randomized study. World J Surg. 2009;33(11):2360–2367. | ||
Bokhari R, Bollman-McGregor J, Kahoi K, Smith M, Feinstein A, Ferrara J. Design, development, and validation of a take-home simulator for fundamental laparoscopic skills: using Nintendo Wii for surgical training. Am Surg. 2010;76(6):583–586. | ||
Statista.com – Smartphone use for professional reasons among U.S. physicians 2012–2015. Available from: https://www.statista.com/statistics/416951/smartphone-use-for-professional-purposes-among-us-physicians/. Accessed July 24, 2018. | ||
Boulos MN, Wheeler S, Tavares C, Jones R. How smartphones are changing the face of mobile and participatory healthcare: an overview, with example from eCAALYX. Biomed Eng Online. 2011;10:24. | ||
Franko OI, Tirrell TF. Smartphone app use among medical providers in ACGME training programs. J Med Syst. 2012;36(5):3135–3139. | ||
Payne KB, Wharrad H, Watts K. Smartphone and medical related App use among medical students and junior doctors in the United Kingdom (UK): a regional survey. BMC Med Inform Decis Mak. 2012;12:121. | ||
Ozdalga E, Ozdalga A, Ahuja N. The smartphone in medicine: a review of current and potential use among physicians and students. J Med Internet Res. 2012;14(5):e128. | ||
Molinas CR, De WinG, Ritter O, Keckstein J, Miserez M, Campo R. Feasibility and construct validity of a novel laparoscopic skills testing and training model. Gynecol Surg. 2008;5:281–290. | ||
Molinas CR, Campo R. Defining a structured training program for acquiring basic and advanced laparoscopic psychomotor skills in a simulator. Gynecol Surg. 2010;7:427–435. | ||
Campo R, Reising C, Van Belle Y, Nassif J, O’Donovan P, Molina CR. A valid model for testing and training laparoscopic psychomotor skills. Gynecol Surg. 2010;7:133–141. | ||
Satava RM. Nintendo surgery. JAMA. 1992;267(17):2329–2330. | ||
Grantcharov TP, Bardram L, Funch-Jensen P, Rosenberg J. Impact of hand dominance, gender, and experience with computer games on performance in virtual reality laparoscopy. Surg Endosc. 2003;17(7):1082–1085. | ||
Paschold M, Schröder M, Kauff DW, et al. Virtual reality laparoscopy: which potential trainee starts with a higher proficiency level? Int J Comput Assist Radiol Surg. 2011;6(5):653–662. | ||
Shane MD, Pettitt BJ, Morgenthal CB, Smith CD. Should surgical novices trade their retractors for joysticks? Videogame experience decreases the time needed to acquire surgical skills. Surg Endosc. 2008;22(5):1294–1297. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.