")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
The Relationship Between Non-HDL-C /HDL-C Ratio (NHHR) and Vitamin D in Type 2 Diabetes Mellitus
Authors Zhen R , Ban J, Jia Z, Liu Y, Li Z, Chen S
Received 31 March 2023
Accepted for publication 19 August 2023
Published 31 August 2023 Volume 2023:16 Pages 2661—2673
DOI https://doi.org/10.2147/DMSO.S414673
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Konstantinos Tziomalos
Ruoxi Zhen,1,2 Jiangli Ban,2,3 Zhuoya Jia,1,2 Yanhui Liu,2,3 Zelin Li,1,2 Shuchun Chen1,2,4
1Graduate School, Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China; 2Department of Endocrinology, Hebei General Hospital, Shijiazhuang, Hebei, People’s Republic of China; 3Graduate School, Hebei North University, Zhangjiakou, People’s Republic of China; 4Hebei Key Laboratory of Metabolic Diseases, Shijiazhuang, Hebei, People’s Republic of China
Correspondence: Shuchun Chen, Department of Endocrinology, Hebei General Hospital, 348 Heping West Road, Shijiazhuang, Hebei, 050051, People’s Republic of China, Tel +86 31185988406, Fax +86 31185988406, Email [email protected]
Purpose: The objective of this research was to examine the relationship between non-HDL cholesterol/HDL cholesterol ratio (NHHR) and vitamin D in type 2 diabetes mellitus (T2DM).
Patients and Methods: This study enrolled 617 T2DM participants. Participants were separated into two groups: no vitamin D deficiency and vitamin D deficiency. Participants were split into two categories: individuals who had a high NHHR and those with a low NHHR, with the median NHHR serving as the cut-off. Eventually, the study participants were classified into two groups by gender, which were further classified into vitamin D deficient and non-vitamin D deficient groups.
Results: NHHR values were substantially greater in vitamin D deficient group than in the non-deficient group in both male and female T2DM patients (P< 0.05). The high NHHR group displayed substantially lower vitamin D levels than the low NHHR group [16.21 (12.55,21.35) vs 19.05 (14.59,24.07), P< 0.001]. NHHR was discovered to be negatively and independently associated with vitamin D levels, and there was no sex difference.
Conclusion: For the first time, our research revealed a negative relationship between NHHR and vitamin D in patients with T2DM.
Keywords: vitamin D, diabetes, type 2 diabetes, lipid ratio, non-HDL-C /HDL-C
Introduction
Diabetes has become one of the most general health problems of the 21st century, with an estimated 9.3% of the world’s adult population suffering from the disease.1 Among the macrovascular and microvascular problems that diabetic patients frequently experience are coronary heart disease, hypertension, diabetic nephropathy, retinopathy, and peripheral neuropathy.2 There are two primary types of vitamin D, a nutrient necessary for many bodily functions. Ergocalciferol, also known as vitamin D2, is a nutrient that can be acquired through dietary sources of vegetables and oral supplements. Cholecalciferol, also known as vitamin D3, is mainly created when skin is exposed to ultraviolet B (UVB) radiation from daylight.3 Vitamin D supplementation is essential because there are few natural sources of vitamin D in food, the diet does not provide adequate vitamin D for the majority of people, and conditions of inadequate daylight exposure contribute to vitamin D deficiency in 25% or more of patients worldwide.4 The European Society for Endocrinology’s Vitamin D Working Group’s clinical practice recommendations classify a critical level of vitamin D inadequacy as being 20 ng/mL (50 nmol/L).5 Vitamin D is a fat-soluble steroid which is required for the regulation of many vital bodily functions, including bone turnover, cell proliferation, and immune regulation.6 In addition, vitamin D is strongly related with the risk of T2DM and its low blood 25(OH)D levels impair pancreatic β-cell function and contribute to insulin resistance.7 In addition, vitamin D is strongly correlated with the risk of T2DM and its complications.
Non-HDL cholesterol/HDL cholesterol ratio (NHHR) is a newly combined indicator of atherogenic lipids.7 Non-HDL-C, which measures the atherosclerotic cholesterol levels, is computed by removing HDL-C from total cholesterol.8 There are Studies have found NHHR acts as both a standalone risk factor for carotid plaque and a lipid indicator for early plaque avoidance.9 Kim SW claims10 that NHHR has a higher diagnostic value than other traditional lipid indicators in predicting insulin resistance and metabolic syndrome. Furthermore, NHHR has been shown as a more potent predictor of non-alcoholic fatty liver disease (NAFLD).11 Some recent research have found that vitamin D deficiency increases the risk of dyslipidemia, and that vitamin D supplementation affects serum lipid levels, lowering total cholesterol, triglycerides, and LDL cholesterol while increasing HDL cholesterol.12 Vitamin D3 supplementation reduces lipid production, oxidative stress, and apoptosis in diabetic mice and has been demonstrated to drastically lower plasma triglyceride and LDL cholesterol levels.13 Furthermore, a number of research on NHHR and the risk of developing T2DM have been published7,14 However the relationship between NHHR and vitamin D in T2DM has not been studied. Therefore, the aim of our current research was to figure out: 1) the relationship between NHHR and vitamin D in T2DM, whether there were gender differences; 2) Whether NHHR is an independent influencing factor for vitamin D.
Materials and Methods
Research Subjects
The Department of Endocrinology at Hebei General Hospital carried out this research from December 2021 to September 2022. Participants in the study had to meet the 1999 World Health Organization diagnostic criteria for diabetes mellitus. The following individuals were excluded from this study: those with type 1 diabetes or acute diabetic complications, pregnant women, those with hepatic or renal impairment, tumors, those with thyroid diseases, those with hyperparathyroidism, and those using medications that may influence vitamin D. All participants endorsed an informed consent form before to registration, and this research was authorized by the medical ethics committee of the Hebei General Hospital. The Declaration of Helsinki was followed during the study’s execution.
Information and Biochemical Measurements
A questionnaire was filled out by all participants to provide general information covering age, gender, medical history, menopause history, smoking and alcohol consumption. A professional took two measurements of the participants’ height, weight, body mass index (BMI), and systolic and diastolic blood pressure, recording the mean values. Subjects had blood specimens collected after an 8-hour fasting to measure vitamin D, triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), albumin (Alb), alanine aminotransferase (ALT), aspartate aminotransferase (AST), urea nitrogen (BUN), creatinine (SCr), uric acid (UA), glomerular filtration rate (GFR); fasting blood glucose (FBG) and glycosylated hemoglobin (HbA1c). Laboratory doctors in the Department of Nuclear Medicine, Hebei General Hospital, tested 25-hydroxyvitamin D3 using the electrochemiluminescence method. NHHR was computed as non-HDL-C [mmol/L]/HDL-C [mmol/L]. TC [mmol/L] − HDL-C [mmol/L] equals non-HDL-C [mmol/L].
Statistical Analysis
The analyses in this research were carried out using SPSS 26.0 for data processing. The Kolmogorov–Smirnov test was employed to examine normal distributions. Data which were not normally distributed were presented as median values (25th-75th interquartile range), while continuous variables that followed a normal distribution were expressed as mean standard deviation. Numbers are used to express data for categorical variables (percentages). The Student’s t-test or the Mann–Whitney test was employed to compare clinical parameters between groups. Using the χ2 test, categorical variables were compared. To examine the relationship between each indicator and the NHHR, Spearman or Pearson correlation analysis was utilized. The independent relationship between NHHR and vitamin D levels was examined using multiple linear regression analysis. P-values <0.05 were considered statistically significant.
Results
Clinical Characteristics of All Participants
This study comprised a total of 617 type 2 diabetes patients, including 216 males and 401 females. The average BMI was 26.20 kg/m2, the average age was 59.24 years, and the average DM duration was 10 years. The mean FBG and the mean percentage of glycosylated hemoglobin were both 7.61 mmol/L and 8.60%, respectively. Of the total subjects, metformin was used by 375 (60.78%), insulin was applied by 345 (55.92%) and statins by 376 (60.94%). The average vitamin D level was 17.80 ng/mL, and 378 subjects (61.3%), who had 25(OH)D levels below 20 ng/mL. With a mean NHHR value of 3.29, 310 patients overall (50.24%) had high NHHR values (Table 1).
 |
Table 1 Clinical Characteristics of All Participants |
Clinical Features of All Patients with T2DM with and without Vitamin D Deficiency
As shown in Table 2, patients with vitamin D deficiency had considerably higher NHHR and HbA1c levels in comparison with subjects who had no vitamin D insufficiency (P<0.001). When compared with those who were not vitamin D deficient, patients in the vitamin D deficiency group had considerably lower levels of age, albumin, AST, HDL, and non-HDL (P<0.05). In contrast, fasting blood glucose levels, total cholesterol, triglycerides, and LDL were considerably higher in vitamin D deficient patients (P<0.05). In terms of gender, BMI, and length of diabetes, there were no appreciable variations between two groups. In addition, in the vitamin D deficient group, the number of people on metformin, insulin and statins was comparable to the non-vitamin D deficient group. Figure 1 illustrates the difference in NHHR between the group with vitamin D insufficiency and the group without one.
 |
Table 2 Clinical Features of All Patients with T2DM with and without Vitamin D Deficiency |
 |
Figure 1 Comparison of NHHR in non-vitamin D deficient and vitamin D deficient groups in all participants. *Denotes significance at a P value of <0.05. |
Clinical Features of All T2DM Patients in the High and Low NHHR Groups
There was no discernible distinction in age between two groups, however compared to the high NHHR group, the low NHHR group included noticeably more male patients (P<0.05). Both diastolic and systolic blood pressure levels were noticeably higher in individuals with high NHHR when contrasted to those with low NHHR (P=0.049, P<0.001), whereas the length of diabetes was noticeably shorter in the high NHHR group. FBG, TC, TG, LDL, non-HDL and HbA1c levels were significantly higher in the high NHHR group compared to the low NHHR group (p < 0.001), while HDL levels were significantly lower in the low NHHR group (P < 0.001). Vitamin D deficiency was more prominent in the high NHHR group. When contrast to the low NHHR group, the high NHHR group had significantly lower levels of vitamin D (P <0.001) (Table 3). The proportion of metformin and insulin use was significantly higher in the high NHHR group than in the low NHHR group (P < 0.001). However, there was no significant difference in statins use between the two groups (P=0.387). Figure 2 illustrates the prevalence of low vitamin D levels and vitamin D insufficiency in individuals who have high NHHR levels to those with low levels of NHHR.
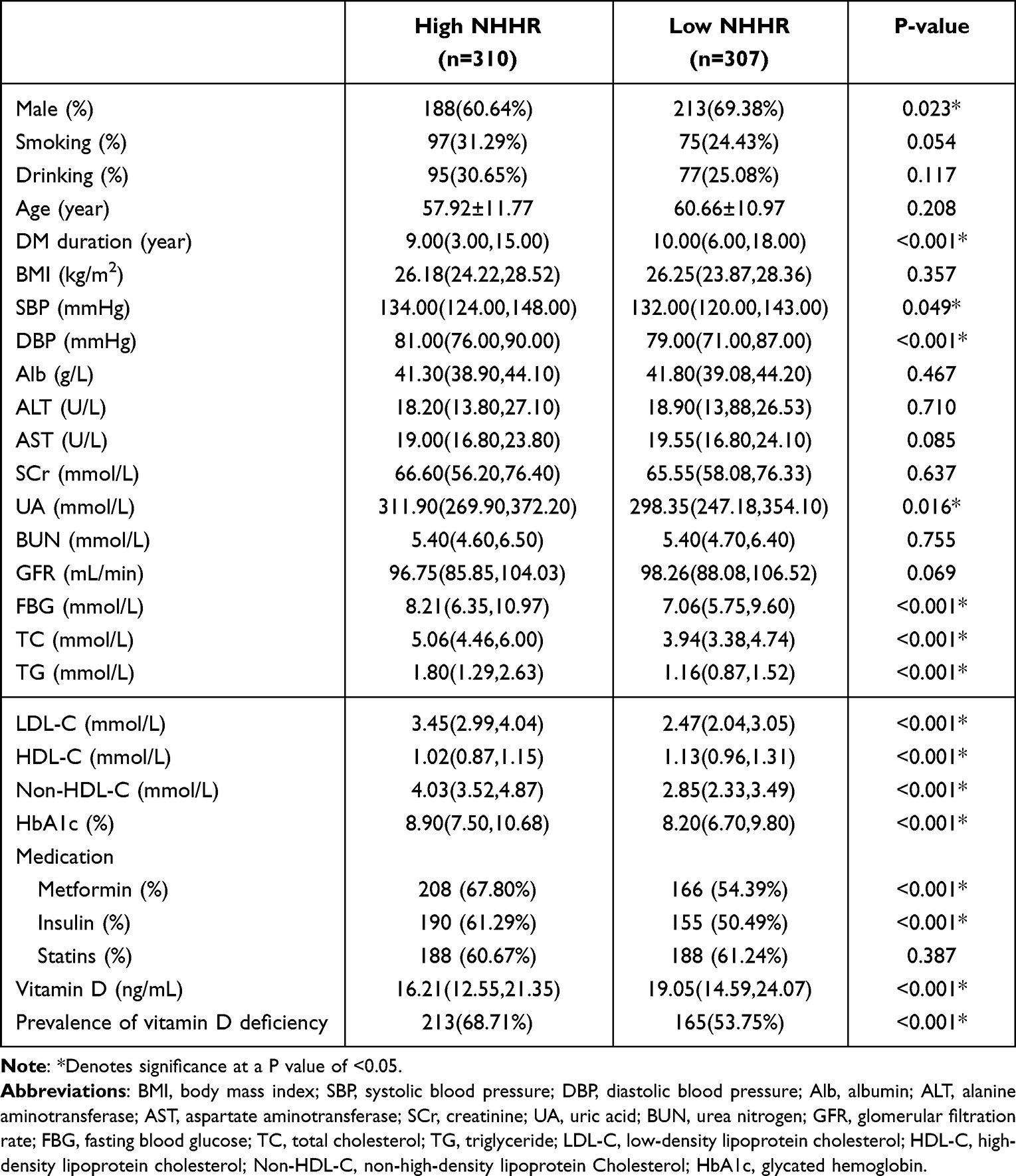 |
Table 3 Clinical Features of All T2DM Patients in the High and Low NHHR Groups |
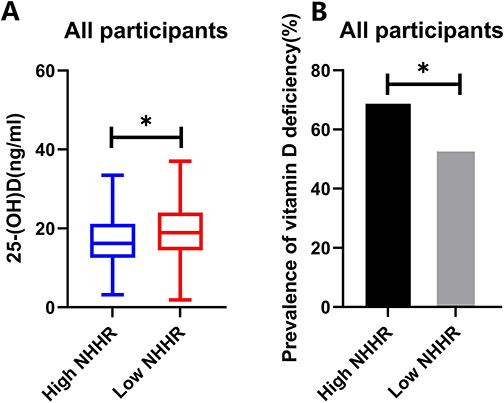 |
Figure 2 Comparison of 25(OH)D levels and prevalence of vitamin D deficiency in the High NHHR and Low NHHR groups for all participants (A) Comparison of 25(OH)D levels in the high NHHR and low NHHR groups for all participants. (B) Comparison of prevalence of vitamin D deficiency in the high NHHR and NHHR groups for all participants. * Denotes significance at a P value of <0.05. |
Clinical Features of Male and Female Patients with T2DM with and without Vitamin D Deficiency
Male patients with vitamin D insufficiency had considerably higher NHHR values than male patients without vitamin D deficiency in contrast to vitamin D deficient group (P<0.001). In comparison to female patients without vitamin D insufficiency, female patients with vitamin D insufficiency exhibited substantially higher NHHR values (P<0.001) (Table 4). Figure 3 illustrates the variations in NHHR and vitamin D levels between the male and female groups.
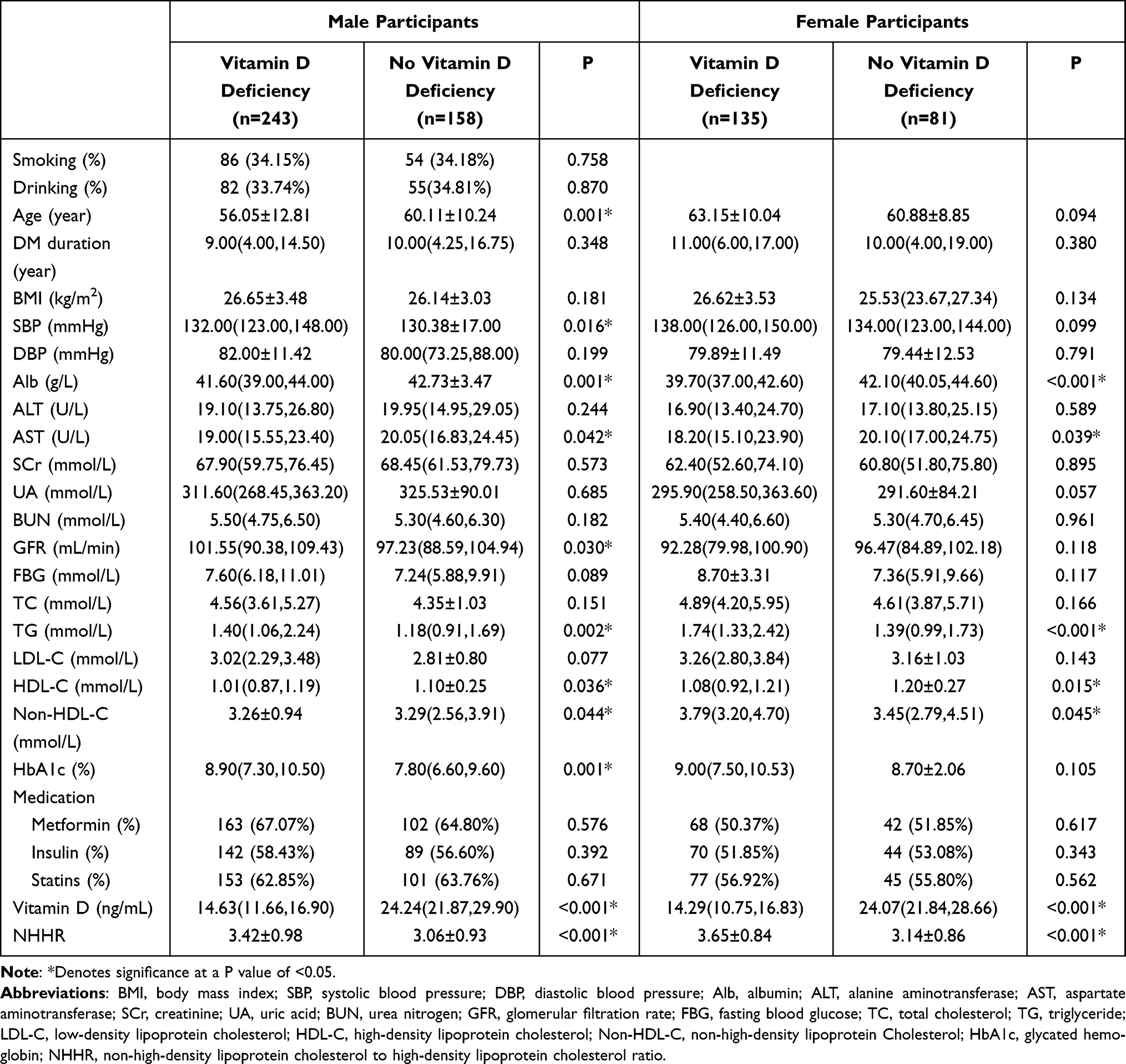 |
Table 4 Clinical Features of Male and Female Patients with T2DM with and without Vitamin D Deficiency |
 |
Figure 3 Comparison of NHHR levels and vitamin D levels in female and male participants (A) Comparison of NHHR between the vitamin D deficient group and the no vitamin D deficiency group in male participants. (B) Comparison of NHHR between the vitamin D deficient and no vitamin D deficient groups in female participants. (C) Comparison of vitamin D in the High NHHR and Low NHHR groups among male participants. (D) Comparison of vitamin D in the High NHHR and Low NHHR groups among female participants. * Indicates significance at p-value < 0.05. |
Association Between Vitamin D and NHHR in T2DM Patients
As Table 5 and Figure 4 illustrate, Vitamin D was detected to be inversely linked with NHHR (r =−0.202, P< 0.001) in all research subjects, and it was also inversely linked with NHHR in male Participants (r =−0.166, P=0.001) and female participants (r =−0.263, P<0.001).
 |
Table 5 Correlation Between Vitamin D and Other Factors in Patients with T2DM |
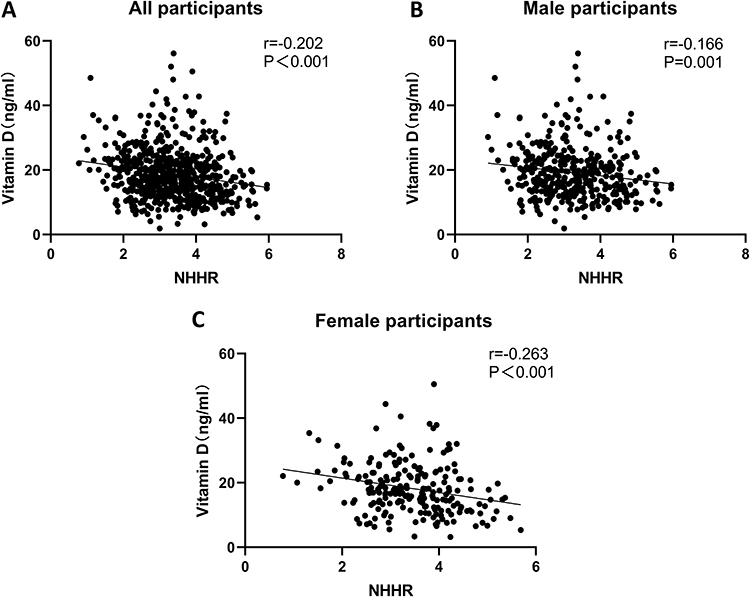 |
Figure 4 Correlation between vitamin D and NHHR levels (A) Correlation between vitamin D and NHHR levels in all participants. (B) Correlation between vitamin D and NHHR levels in male participants. (C) Correlation between vitamin D and NHHR levels in female participants. |
Multivariate Linear Regression Analysis of Vitamin D and NHHR in T2DM
In all subjects, Vitamin D had a negative correlation with NHHR in crude model 1 (β=−0.196, P<0.001), model 2 (adjusted for age, BMI and DM duration) (β=−0.200, P<0.001), model 3 (adjusted for age, BMI, DM duration, Alb, SBP, HbA1c) (β=−0.178, P<0.001) and model 4 (adjusted for age, BMI, DM duration, Alb, SBP, HbA1c, Scr, UA, BUN, GFR) (β =−0.175, P<0.001) (Table 6).
 |
Table 6 Correlation Between Vitamin D with NHHR in All T2DM Patients |
In spite of whether the model is adjusted or not, NHHR was found to be inversely related with vitamin D in female participants with T2DM (model 1: =−0.271, P<0.001; model 2: =−0.274, P<0.001; model 3: =−0.243, P<0.001; model 4: =−0.230, P=0.001) (Table 7). In the same way, NHHR was also found to be adversely related with vitamin D in male participants with T2DM (model 1: =−0.155, P=0.002; model 2: =−0.127, P=0.017; model 3: =−0.103, P=0.044; model 4: =−0.103, P=0.047), in spite of whether the model is adjusted or not (Table 8).
 |
Table 7 Correlation Between Vitamin D and NHHR in Female Patients with T2DM |
 |
Table 8 Correlation Between Vitamin D and NHHR in Male Patients with T2DM |
Discussion
Vitamin D deficiency is becoming a very common disorder worldwide and is estimated to occur in approximately one billion people worldwide due to the compromised bioavailability of vitamin D as a result of human lifestyle, diet and the use of sun protection.15,16 Vitamin D that has been absorbed is attached to celiac particles, which are taken up by the lymphatic system and delivered into the bloodstream. Vitamin D2 and D3 from the diet and vitamin D3 from skin manufacturing are linked to albumin and vitamin D binding protein (DBP). Vitamin D (where D stands for D2 or D3) is delivered to the liver, where it is converted by 25-hydroxylase into 25 (OH) D, the main circulating form of vitamin D; In the kidney, it is converted to 1,25 (OH) 2D by 1A-hydroxylase. 1,25 (OH)2D binds to DBP, enters the circulation, reaches effector tissue cells, binds to vitamin D receptor (VDR) in cells, performs various physiological functions and regulate biological metabolism. VDRs are distributed in practically all tissues and cells in the body, despite the fact that they are primarily found in tissues that control calcium and phosphorus homeostasis. And there is increasing proof that vitamin D functions outside of the skeleton.4 Vitamin D can perform a wide range of biological functions owing to the widespread distribution of VDR in tissue cells, including controlling cell differentiation and proliferation, cellular immunity, obstructing angiogenesis, and stimulating the secretion of insulin and renin.6 Vitamin D insufficiency accelerates the evolution of type 2 diabetes and its complications by an unknown mechanism, but many studies suggest that it is closely linked to insulin resistance, disturbances in glucose metabolism and oxidative stress.17,18 Vitamin D deficiency promotes the development and progression of microvascular and macrovascular complications of T2DM,15,16 including peripheral neuropathy (DPN), retinopathy (DR), diabetic nephropathy (DN) and coronary atherosclerosis. In addition, vitamin D deficiency can lead to an increased risk of non-alcoholic fatty liver disease, bladder cancer, colorectal cancer and other diseases.11,19,20 Vitamin D plays a wide range of roles and is essential for physical fitness and health, therefore early discovery of vitamin D deficiency is particularly important in preventing the development of diabetes and its complications.
Diabetic patients typically have atherosclerotic lipid disorders, which are identified as raised levels of non-HDL-C, TG, and decreased concentrations of HDL-C. It has been shown that atherosclerotic lipid disorders are a distinct risk factor for diabetes.21 NHHR is a comprehensive lipid index that includes information on all atherogenic and anti-atherogenic lipid microparticles. In this study, we found that patients with T2DM with higher NHHR levels were more likely to develop vitamin D deficiency and that NHHR values were significantly and independently negatively correlated with vitamin D levels. Therefore, we suggest that high NHHR is a risk factor for the development of vitamin D deficiency in patients with type 2 diabetes. Our analysis may be related to the following mechanisms. Firstly, non-HDL-C covers a greater proportion of atherogenic cholesterol that is transported to peripheral cells, including low-density lipoprotein-C, very low-density lipoprotein (VLDL-C), medium-density lipoprotein (IDL-C), celiac particles and their TG-rich lipoprotein residues9,22 NHHR represents the balance of cholesterol transport. A higher NHHR index indicates a greater tendency for peripheral cholesterol deposition, elevated distribution of blood cholesterol to peripheral cells may lead to insulin resistance or islet beta-cell dysfunction, and cholesterol deposition in peripheral cells, which may increase peroxisome proliferator-activated receptor-γexpression23, thereby increasing peripheral insulin resistance, leading to vitamin D deficiency. This may lead to inhibition of vitamin D binding to its receptor, which may exacerbate insulin resistance and affect glucose metabolism, among other things. Secondly, vitamin D regulates the immune response of macrophages and monocytes, thereby reducing the production of inflammatory factors and reducing the inflammatory response,24 while HDL is involved in the reverse cholesterol transport (RCT) pathway, which transports excess peripheral cholesterol to the liver for metabolism. HDL-C has anti-inflammatory and antioxidant biological functions and may prevent the development of vitamin D deficiency by inhibiting endoplasmic reticulum stress and β-cell apoptosis, thereby preventing the development of vitamin D deficiency. In an analysis of 48,703 Korean individuals, Kim S.W. discovered that NHHR helped identify persons who were more likely to develop the metabolic syndrome and insulin resistance.10 As a result, it was discovered that NHHR had good diagnostic capability for identifying insulin resistance, and the integration of non-HDL-C and HDL-C was considerably more precise in predicting disorders related with the probability of developing diabetes than traditional lipid measurements.25 According to this study’s findings, vitamin D insufficiency is linked to poor lipid metabolism. In Chinese T2DM patients, NHHR, a measure of the lipid metabolic response, is strongly correlated with vitamin D insufficiency.
All study participants were split into vitamin D deficiency and no vitamin D deficiency groups, and pertinent clinical characteristics were gathered to evaluate them. The vitamin D insufficiency group exhibited lower amounts of albumin but higher systolic blood pressure in comparison with no vitamin D deficiency group, this result is in line with Jia’s findings.26 Uncertainty about the process by which they interact, which may be caused by confounding variables like gender and age, exists. The incidence of vitamin D insufficiency in younger individuals raised the possibility that the type of labor performed by vitamin D deficient patients may be connected to vitamin D levels. Consistent with earlier investigations, fasting blood glucose and glycated hemoglobin levels were higher in vitamin D deficient group in comparison with the non-vitamin D deficient group.27 We detected variations in vitamin D values and the prevalence of vitamin D inadequacy between the two groups of patients when we separated patients based on their median NHHR index. In T2DM patients, NHHR were adversely linked with vitamin D levels. Whether to adjust the model or not, we discovered that NHHR were independently and adversely related with vitamin D levels in both male and female T2DM populations.
There are several advantages to this study. Firstly, this is the first research to certify a negative relationship between NHHR and vitamin D in the Chinese T2DM population. Secondly, NHHR can be easily calculated because it has a straightforward formula and is a biochemical indication that we frequently test. There are obviously some drawbacks to this study. This research also has some shortcomings. Firstly, we were unable to confirm a causal link between vitamin D insufficiency and NHHR because this was a cross-sectional observational study design. Secondly, we were unable to control for the effects of factors such as diet, sunlight hours, seasonal variations and different types of lipid-lowering medications on vitamin D and lipid levels. In addition, the study did not deepen the effects of smoking and drinking habits on vitamin D and lipid levels, and did not collect data such as proteinuria, but only included GFR, which did not allow a better assessment of renal function in the study population. Future studies on vitamin D levels should incorporate an in-depth analysis of all these influencing factors, taking into account the nature of the work of the study population, individual dietary habits, seasonal variations, outdoor activities, and the effects of lipid-lowering medications.
Conclusion
In summary, this study detected that high NHHR was a risk factor for vitamin D deficiency in patients with type 2 diabetes. Moreover, NHHR was independently and negatively associated with vitamin D levels in patients with T2DM, and there were no gender differences.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lovic D, Piperidou A, Zografou I, Grassos H, Pittaras A, Manolis A. The growing epidemic of diabetes mellitus. Curr Vasc Pharmacol. 2020;18(2):104–109. doi:10.2174/1570161117666190405165911
2. Demir S, Nawroth PP, Herzig S, Ekim Üstünel B. Emerging targets in type 2 diabetes and diabetic complications. Adv Sci. 2021;8(18):2100275. doi:10.1002/advs.202100275
3. Pittas AG, Jorde R, Kawahara T, Dawson-Hughes B. Vitamin D supplementation for prevention of type 2 diabetes mellitus: to D or not to D? J Clin Endocrinol Metab. 2020;105(12):3721–3733. doi:10.1210/clinem/dgaa594
4. de la Guía-Galipienso F, Martínez-Ferran M, Vallecillo N, Lavie CJ, Sanchis-Gomar F, Pareja-Galeano H. Vitamin D and cardiovascular health. Clin Nutr. 2021;40(5):2946–2957. doi:10.1016/j.clnu.2020.12.025
5. Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911–1930. doi:10.1210/jc.2011-0385
6. Yang M, Liu J, Zhou X, et al. Correlation analysis between serum vitamin D levels and lower extremity macrovascular complications in individuals with type 2 diabetes mellitus. J Diabetes Res. 2019;2019:4251829. doi:10.1155/2019/4251829
7. Sheng G, Liu D, Kuang M, Zhong Y, Zhang S, Zou Y. Utility of non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio in evaluating incident diabetes risk. DMSO. 2022;15:1677–1686. doi:10.2147/DMSO.S355980
8. Sheng G, Kuang M, Yang R, Zhong Y, Zhang S, Zou Y. Evaluation of the value of conventional and unconventional lipid parameters for predicting the risk of diabetes in a non-diabetic population. J Transl Med. 2022;20(1):266. doi:10.1186/s12967-022-03470-z
9. Wang A, Li Y, Zhou L, et al. Non-HDL-C/HDL-C ratio is associated with carotid plaque stability in general population: a cross-sectional study. Front Neurol. 2022;13:875134. doi:10.3389/fneur.2022.875134
10. Kim SW, Jee JH, Kim HJ, et al. Non-HDL-cholesterol/HDL-cholesterol is a better predictor of metabolic syndrome and insulin resistance than apolipoprotein B/apolipoprotein A1. Int J Cardiol. 2013;168(3):2678–2683. doi:10.1016/j.ijcard.2013.03.027
11. Kwok RM, Torres DM, Harrison SA. Vitamin D and nonalcoholic fatty liver disease (NAFLD): is it more than just an association? Hepatology. 2013;58(3):1166–1174. doi:10.1002/hep.26390
12. Surdu AM, Pînzariu O, Ciobanu D-M, et al. Vitamin D and its role in the lipid metabolism and the development of atherosclerosis. Biomedicines. 2021;9(2):172. doi:10.3390/biomedicines9020172
13. Lee H, Lee H, Lim Y. Vitamin D3 improves lipophagy-associated renal lipid metabolism and tissue damage in diabetic mice. Nutr Res. 2020;80:55–65. doi:10.1016/j.nutres.2020.06.007
14. Zhang N, Hu X, Zhang Q, et al. Non-high-density lipoprotein cholesterol: high-density lipoprotein cholesterol ratio is an independent risk factor for diabetes mellitus: results from a population-based cohort study. J Diabetes. 2018;10(9):708–714. doi:10.1111/1753-0407.12650
15. Pludowski P, Takacs I, Boyanov M, et al. Clinical practice in the prevention, diagnosis and treatment of vitamin D deficiency: a central and eastern European expert consensus statement. Nutrients. 2022;14(7):1483. doi:10.3390/nu14071483
16. Zakaria WNA, Mohd Yunus N, Yaacob NM, et al. Association between vitamin D receptor polymorphisms (BsmI and FokI) and glycemic control among patients with type 2 diabetes. Int J Environ Res Public Health. 2021;18(4):1595. doi:10.3390/ijerph18041595
17. Dai J, Yu M, Chen H, Chai Y. Association between serum 25-OH-vitamin D and diabetic foot ulcer in patients with type 2 diabetes. Front Nutr. 2020;7:109. doi:10.3389/fnut.2020.00109
18. Szymczak-Pajor I, Drzewoski J, Śliwińska A. The molecular mechanisms by which vitamin D prevents insulin resistance and associated disorders. Int J Mol Sci. 2020;21(18):6644. doi:10.3390/ijms21186644
19. Ekmekcioglu C, Haluza D, Kundi M. 25-hydroxyvitamin D status and risk for colorectal cancer and type 2 diabetes mellitus: a systematic review and meta-analysis of epidemiological studies. IJERPH. 2017;14(2):127. doi:10.3390/ijerph14020127
20. Zhao Y, Chen C, Pan W, et al. Comparative efficacy of vitamin D status in reducing the risk of bladder cancer: a systematic review and network meta-analysis. Nutrition. 2016;32(5):515–523. doi:10.1016/j.nut.2015.10.023
21. Tomlinson B, Patil NG, Fok M, Lam CWK. Managing dyslipidemia in patients with Type 2 diabetes. Expert Opin Pharmacother. 2021;22(16):2221–2234. doi:10.1080/14656566.2021.1912734
22. Kjeldsen EW, Nordestgaard LT, Frikke-Schmidt R. HDL cholesterol and non-cardiovascular disease: a narrative review. Int J Mol Sci. 2021;22(9):4547. doi:10.3390/ijms22094547
23. Narvaez CJ, Simmons KM, Brunton J, Salinero A, Chittur SV, Welsh JE. Induction of STEAP4 correlates with 1,25-dihydroxyvitamin D 3 stimulation of adipogenesis in mesenchymal progenitor cells derived from human adipose tissue: VITAMIN D, STEAP4 AND ADIPOGENESIS. J Cell Physiol. 2013;228(10):2024–2036. doi:10.1002/jcp.24371
24. El-Sharkawy A, Malki A. Vitamin D signaling in inflammation and cancer: molecular mechanisms and therapeutic implications. Molecules. 2020;25(14):3219. doi:10.3390/molecules25143219
25. Lin D, Qi Y, Huang C, et al. Associations of lipid parameters with insulin resistance and diabetes: a population-based study. Clin Nutr. 2018;37(4):1423–1429. doi:10.1016/j.clnu.2017.06.018
26. Jia Y, Song T, Li Z, Zhou L, Chen S. The relationship between triglyceride glucose index and vitamin D in type 2 diabetes mellitus. DMSO. 2022;15:511–525. doi:10.2147/DMSO.S348845
27. Zhao X, Deng C, Li Z, Jia Y, Chen S. Monocyte/high-density lipoprotein cholesterol ratio predicts vitamin D deficiency in male patients with type 2 diabetes mellitus. DMSO. 2022;15:2455–2466. doi:10.2147/DMSO.S376127
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.